Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Chromium as a Modulator of Insulin Receptor Activity: A Systematic Review of Its Role in Metabolic Syndrome and Type 2 Diabetes
Authors Babakr AT ![]() , Mukhtar MH
, Mukhtar MH ![]() , Ali ASE, Althubiti MA, Modawe GA, Fatani SH, Nasif WA
, Ali ASE, Althubiti MA, Modawe GA, Fatani SH, Nasif WA ![]()
Received 19 November 2025
Accepted for publication 17 April 2026
Published 15 May 2026 Volume 2026:19 581925
DOI https://doi.org/10.2147/DMSO.S581925
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Jae Woong Sull
Abdullatif Taha Babakr,1 Mohammed Hasan Mukhtar,1 Abeer Shaker Elmoursy Ali,2 Mohammad A Althubiti,1 Gad Allah Modawe,3 Sameer Hasan Fatani,1 Wesam A Nasif1,4
1Department of Biochemistry, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 2Department of Pathology, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 3Department of Biochemistry, Faculty of Medicine and Health Sciences, Omdurman Islamic University, Omdurman, Sudan; 4Molecular Biology Department, Genetic Engineering and Biotechnology Research Institute, Sadat City University, Sadat City, Egypt
Correspondence: Abdullatif Taha Babakr, Department of Biochemistry, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia, Tel +966-25270000/ 4322, Fax +966-25270000/4319, Email [email protected]
Abstract: Metabolic syndrome (MetS) is a complex interplay of interrelated metabolic derangements, including insulin resistance, dyslipidemia, central adiposity, and hypertension, thereby markedly amplifying the predisposition to type 2 diabetes mellitus (T2DM) and cardiovascular morbidities. Chromium (Cr), an indispensable trace element, has garnered scientific interest for its putative role in augmenting insulin sensitivity and modulating glucose metabolism. Chromium deficiency has been linked with insulin resistance and diabetes mellitus. A cycle of low chromium, defective glucose metabolism, and further loss of chromium is documented. Chromium supplementation has been associated with encouraging improvements in insulin sensitivity. It may enhance insulin signaling, regulate lipid metabolism, and mitigate obesity-related dysfunctions. However, its therapeutic efficacy remains debated due to inconsistent clinical outcomes and study variations. This comprehensive review delves into the implications of chromium supplementation, particularly chromodulin, in the context of MetS and its associated pathological sequelae. In conclusion, chromium (Cr) enhances insulin sensitivity by directly activating the insulin receptor kinase, which lowers the required insulin concentration for maximal cellular response and improves glucose uptake and storage. Synthesis of the evidence shows that Chromium (Cr) supplementation significantly benefits individuals with chromium deficiency or diabetes, improving glucose homeostasis and insulin sensitivity. This highlights the importance of baseline metabolic status in the effectiveness of Cr as a treatment, indicating that targeted interventions may be needed for optimal results in those with metabolic disturbances.
Keywords: insulin resistance, chromium, metabolic syndrome, insulin sensitivity
Introduction
MetS is presently considered as a significant public health issue and is progressively receiving heightened scrutiny due to its escalating prevalence on a global scale. Numerous factors and conditions were associated with MetS.1 Among these factors, obesity, hyperglycemia, impaired glucose tolerance, and insulin resistance, in conjunction with dyslipidemia, markedly elevate the likelihood of developing diabetes and cardiovascular disease (CVD). The elevated CVD risk together with T2DM risk as a result of MetS creates substantial healthcare needs while impairing functional ability. Patients with MetS who receive reimbursement from healthcare systems incur 2.2 times higher medical expenses compared to those without the condition.1,2 Table 1 shows a summary of the risk Factors, diagnosis, and management of MetS.
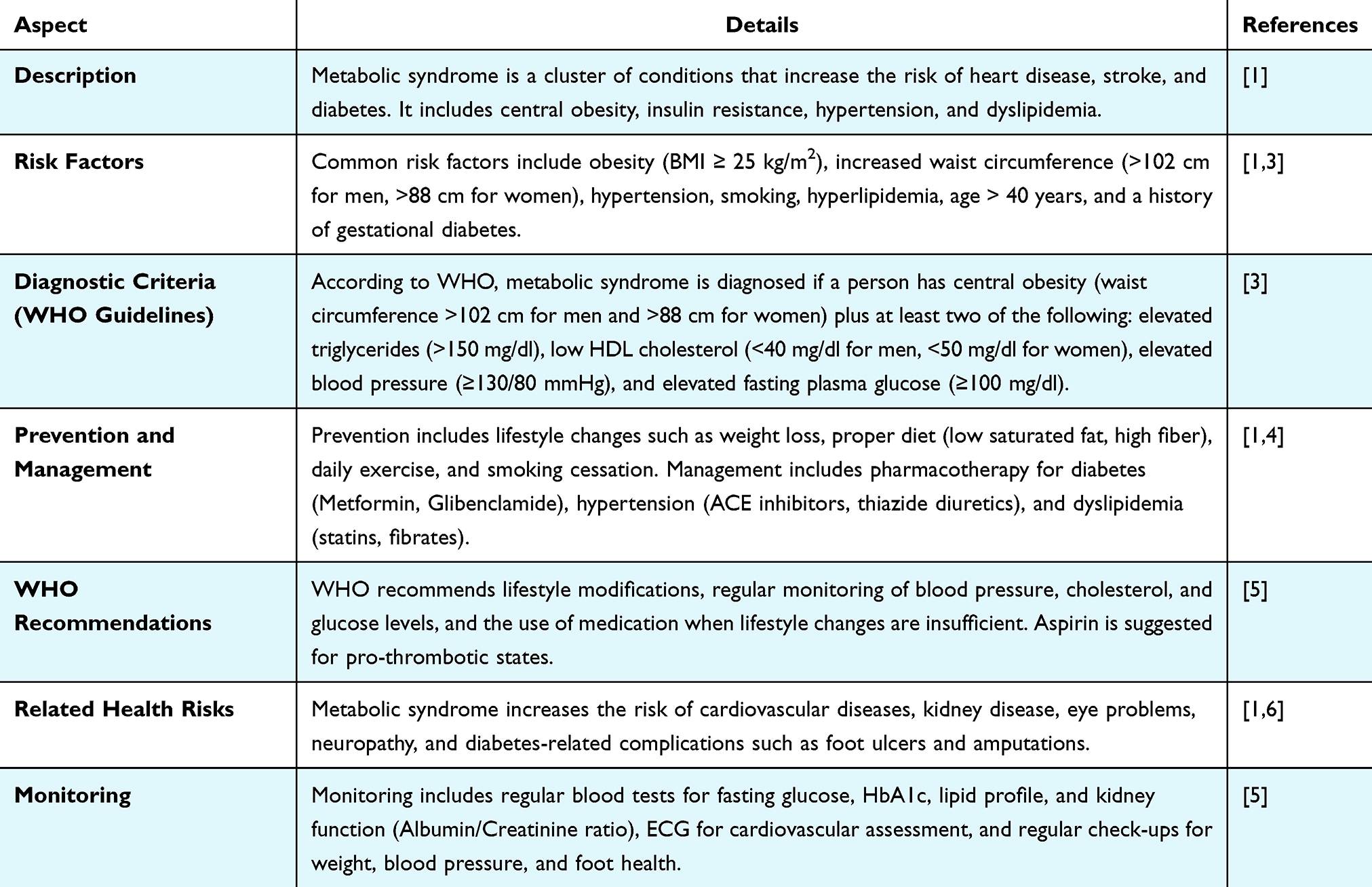 |
Table 1 Overview of Metabolic Syndrome (MetS): Risk Factors, Diagnosis, and Management |
Excessive insulin production due to insulin resistance results in hyperinsulinemia which becomes a central factor in unhealthy cholesterol development. The way the body handles fats during processing becomes impaired because of hyperinsulinemia thus increasing heart disease risks. Technically, insulin resistance causes high blood pressure yet not every person with MetS and elevated blood pressure demonstrates elevated insulin levels. In those who do, the primary mechanism behind their hypertension is heightened sodium retention by the kidneys, leading to increased blood pressure.6,7 Moreover, hypertension in individuals with MetS is closely associated with factors derived from adipose tissue, further exacerbating metabolic dysfunction. Insulin plays a complex causal role in obesity by promoting lipogenesis and inhibiting lipolysis. However, the resultant adiposity is neither the primary cause nor the direct consequence of insulin resistance. Instead, insulin resistance emerges as a downstream effect of obesity and extends beyond glucose metabolism, exerting profound influences on lipid and lipoprotein homeostasis through intricate biochemical pathways.7,8
Central obesity serves as a pivotal initiating factor in the development of MetS. While the role of insulin resistance in the onset of MetS is widely emphasized, it primarily acts as a precursor to hyperglycemia and diabetes rather than being the fundamental cause of obesity.9
Chromium (Cr), an essential trace element in human nutrition, has been linked to improved blood glucose regulation in individuals with type 1 diabetes mellitus (T1DM), T2DM, and steroid-induced diabetes. Additionally, it has been associated with an improved lipid profile in the same population groups.10 Chromium supplementation enhances insulin sensitivity and regulates glucose metabolism while also improving lipid profiles, thereby reducing the risk of both renal and cardiovascular complications. Multiple studies demonstrate positive findings, but additional clinical investigations must provide evidence and establish appropriate chromium usage and dosage. Despite over six decades of research, the therapeutic efficacy of chromium supplementation in MetS remains highly debated due to persistent inconsistencies in clinical outcomes and significant variations across studies. A critical knowledge gap exists regarding the precise impact of baseline metabolic status and chromium levels on treatment responsiveness, as many studies do not adequately assess these factors. Furthermore, the optimal dosage and specific chemical forms of chromium for targeted intervention in diverse MetS phenotypes are yet to be definitively established. While chromodulin is proposed to activate insulin receptor kinase, the exact molecular mechanisms underlying its action and the full characterization of the “cycle of loss” in varied human metabolic profiles require further elucidation. This comprehensive review aims to synthesize the current understanding of chromium supplementation, particularly chromodulin, in the context of MetS and its associated pathological sequelae, while explicitly highlighting these unresolved questions and areas requiring further rigorous investigation.
The present research employs a literature review to investigate the role of chromium in Metabolic Syndrome (MetS), emphasizing its impact on insulin sensitivity, glucose metabolism, and lipid regulation.
Methodology
This study uses a literature review to explore chromium’s role in MetS, focusing on its effects on insulin sensitivity, glucose metabolism, and lipid regulation. A systematic search was conducted, and articles were screened from databases like PubMed, Google Scholar, and Web of Science, using keywords such as “Chromium (Cr)”, “Metabolic Syndrome (MetS)”, and “Insulin Resistance”. Only studies that met the specific inclusion criteria outlined below, were included in the review.
- Intervention – Chromium supplementation, including various forms such as chromium picolinate, chromodulin, and other bioavailable chromium compounds.
- Outcomes – The outcomes generally focus on measuring glucose levels (fasting and postprandial) and insulin sensitivity, with HOMA-IR and fasting insulin levels commonly used to assess insulin sensitivity.
- Study Design – Randomized controlled trials (RCTs), observational studies, and systematic reviews evaluating chromium’s role in metabolic regulation.
- Language – Published in English.
- Publication Source – Appeared in a peer-reviewed journal.
Exclusion Criteria: Studies were excluded if they (1) had uncleared or inconsistent chromium dosages, (2) failed to measure key metabolic markers such as FPG, HbA1c, or HOMA-IR, or (3) were observational studies, animal studies, or narrative reviews without quantitative outcomes.
Chromium interventions considered in this review included dietary chromium intake, pharmacological supplementation, and clinical trials assessing chromium’s effects on insulin sensitivity, glucose metabolism, and lipid regulation, Table 2. Both short-term and long-term supplementation studies were included to analyze chromium’s sustained impact on metabolic parameters.
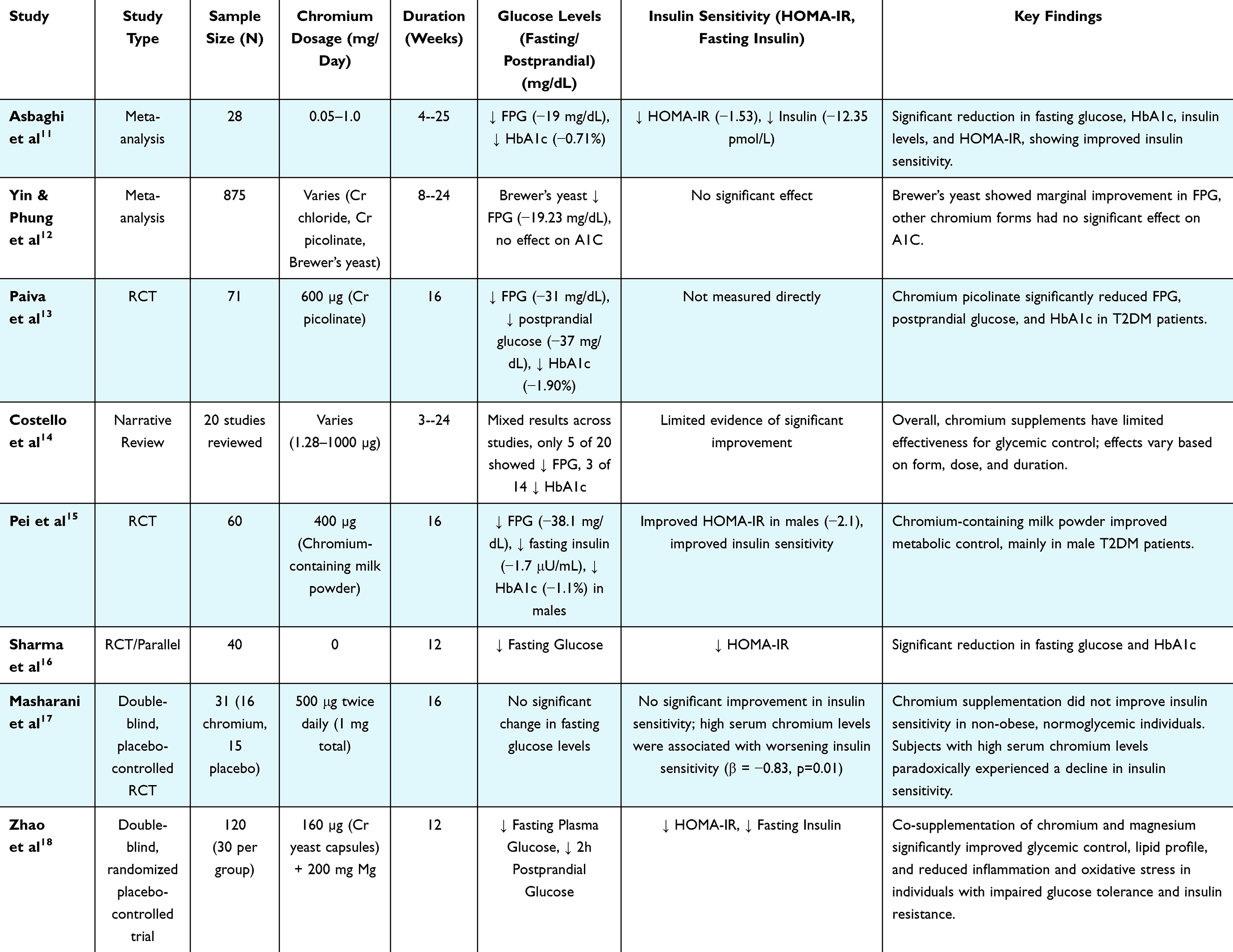 |
Table 2 Chromium Supplementation and Its Effects on Glucose Metabolism and Insulin Sensitivity |
From 1999 to 2025, a total of 299 articles were initially identified using the search term related to this study. A rigorous screening process was conducted, and 159 records were removed before screening, leaving 140 records for title and abstract review, as shown in the Sankey chart in Figure 1. Of these, 61 records were excluded for failing to meet the full inclusion criteria.
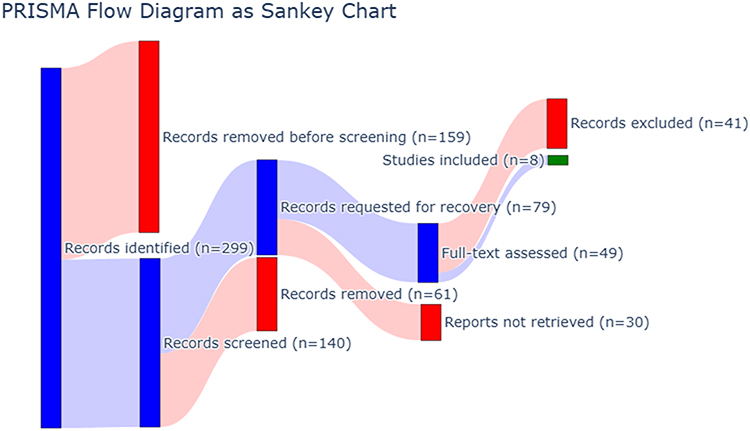 |
Figure 1 PRISMA flow diagram as Sankey chart. |
Subsequently, 79 records were requested for full-text retrieval, but 30 reports could not be obtained. Among the 49 full-text articles assessed for eligibility, 41 studies were excluded due to reasons such as lack of relevant information on chromium dosage (n=8), being review articles (n=4), non-English language (n=5), and other factors like irrelevant or incomplete data (n=24). Finally, 8 studies were included in the systematic review, Figure 2.
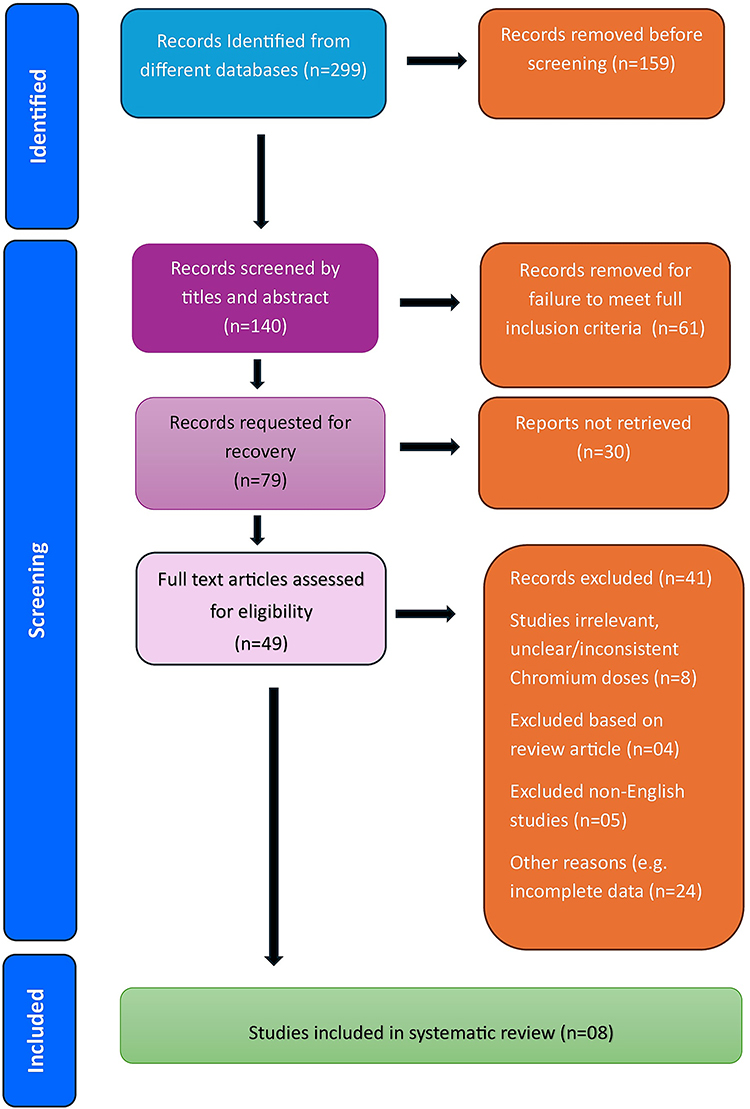 |
Figure 2 PRISMA flow diagram of the study selection process. |
Chromium’s (Cr) Role in Metabolic Syndrome (MetS): Insulin Dysregulation, Kidney Function, and Therapeutic Potential
In the early stages of MetS, the body produces too much insulin (hyperinsulinemia), but it does not work effectively, leading to various health issues. One common problem is increased protein loss in urine, which can be an early sign of kidney damage.19,20 According to the UK Prospective Diabetes Study (UKPDS), individuals with poorly controlled blood sugar are at a higher risk of developing kidney-related complications such as microalbuminuria and proteinuria, which are also associated with high blood pressure.21 This highlights the importance of glucose metabolism in MetS and suggests that chromium (Cr) may play a beneficial role due to its anti-diabetic properties. This emphasizes the importance of glucose metabolism in MetS, and why chromium (Cr) might be especially beneficial due to its anti-diabetic properties. For instance, in a study with rats, chromium supplementation helped reduce the overexpression of a protein called glucose transporter 2 (GLUT-2), which is linked to the development of diabetic microalbuminuria. This suggests that chromium could play a key role in managing MetS and its complications, including kidney issues. Additional research supports chromium’s potential in delaying the onset of diabetes and related kidney problems.22
Chromium (Cr) and Glucose Metabolism: Mechanisms, Insulin Regulation, and Therapeutic Insights
The body employs several mechanisms to maintain normal blood glucose levels. These mechanisms include the uptake of glucose by tissues such as muscle in response to insulin, the conversion of glucose into glycogen for storage in the liver and muscle, and the synthesis of glucose from non-carbohydrate sources when blood glucose levels drop.
It is well known that insulin is the primary hormone responsible for regulating blood glucose levels. It promotes glucose uptake and metabolism in insulin-sensitive tissues while inhibiting glucose production by the liver. However, the exact mechanisms by which insulin controls blood glucose is multifaceted. In vitro, studies have demonstrated that insulin primarily increases the activity of enzymes involved in glucose utilization and glycogen synthesis while simultaneously decreasing the activity of enzymes that promote gluconeogenesis. Additionally, insulin enhances the rate of gene transcription, leading to the production of more glucose-utilizing enzymes and fewer gluconeogenesis-promoting enzymes. Through these processes, the body can typically maintain normal blood glucose levels unless glucose availability or utilization is impaired.23,24
Various research papers compellingly describe Cr’s ability to lower blood glucose in different mammalian models.25–27 In both lean and genetically obese hyperglycemic mice, Cr supplementation has been shown to reduce blood glucose levels, an effect that has also been observed in Zucker rats. Studies conducted in both normal and diabetic humans, as well as in glycogen-depleted T2DM cases and non-insulin-dependent diabetic individuals, have yielded conflicting results. However, most of these studies have demonstrated that Cr supplementation can lower fasting glucose levels and improve glucose tolerance. These results were recently confirmed by a study in nonhuman primates, where Cr supplementation improved insulin sensitivity and glucose levels in a dose-dependent manner. Impaired glucose tolerance and insulin resistance are the most consistent findings associated with Cr deficiency, suggesting that these alterations may be the primary manifestation of a pathophysiological state. This hypothesis is supported by the observation in humans that the degree of glucose intolerance is the sole predictor for the later development of non-insulin-dependent diabetes. The current interest in Cr as a potential therapeutic agent for various states of insulin resistance and/or hyperglycemia emphasizes the need to unravel the precise molecular mechanisms by which Cr affects glucose metabolism.11,28,29
Chromium’s Effect on Insulin Sensitivity & Insulin Signaling Pathways
Chromium supplementation has been suggested to be beneficial in T2DM management. The main symptoms and underlying mechanisms of T2DM are well understood. Research involving both humans and animals indicates that a loss of blood sugar control occurs early in the disease’s progression. Additionally, there is now substantial evidence suggesting that impaired blood sugar control is, at least in part, due to a Cr deficiency. Data from in vitro studies, as well as several in vivo studies, indicate that Cr plays multiple roles that have the potential to influence the pathogenesis of T2DM. Further evidence from studies on T2DM patients supports the notion that Cr may have a beneficial impact on the management of the disease. However, at the molecular level, the precise mechanisms by which Cr affects T2DM progression remain largely unclear, which could limit its potential as a therapeutic option for the disease.11 Multiple studies have demonstrated that Cr supplementation in individuals with T2DM and insulin resistance can lead to improved glycemic control. This improvement is reflected in better fasting glucose levels, lower insulin levels, and reduced hemoglobin A1c levels. Cr has the strongest evidence supporting its effects on T2DM and has been shown to be comparable to oral hypoglycemic agents. A recent meta-analysis of 15 randomized controlled trials concluded that Cr supplementation significantly improves glycemic control and reduces the need for diabetes medications. Additionally, the effects of Cr on the dyslipidemic components of MetS are well-documented. Consistent data show that Cr can lower total cholesterol, triglycerides, and low-density lipoprotein (LDL) levels while increasing high-density lipoprotein (HDL) levels.30 Further details of chromium’s effect on insulin resistance and metabolic health are summarized in Table 3.
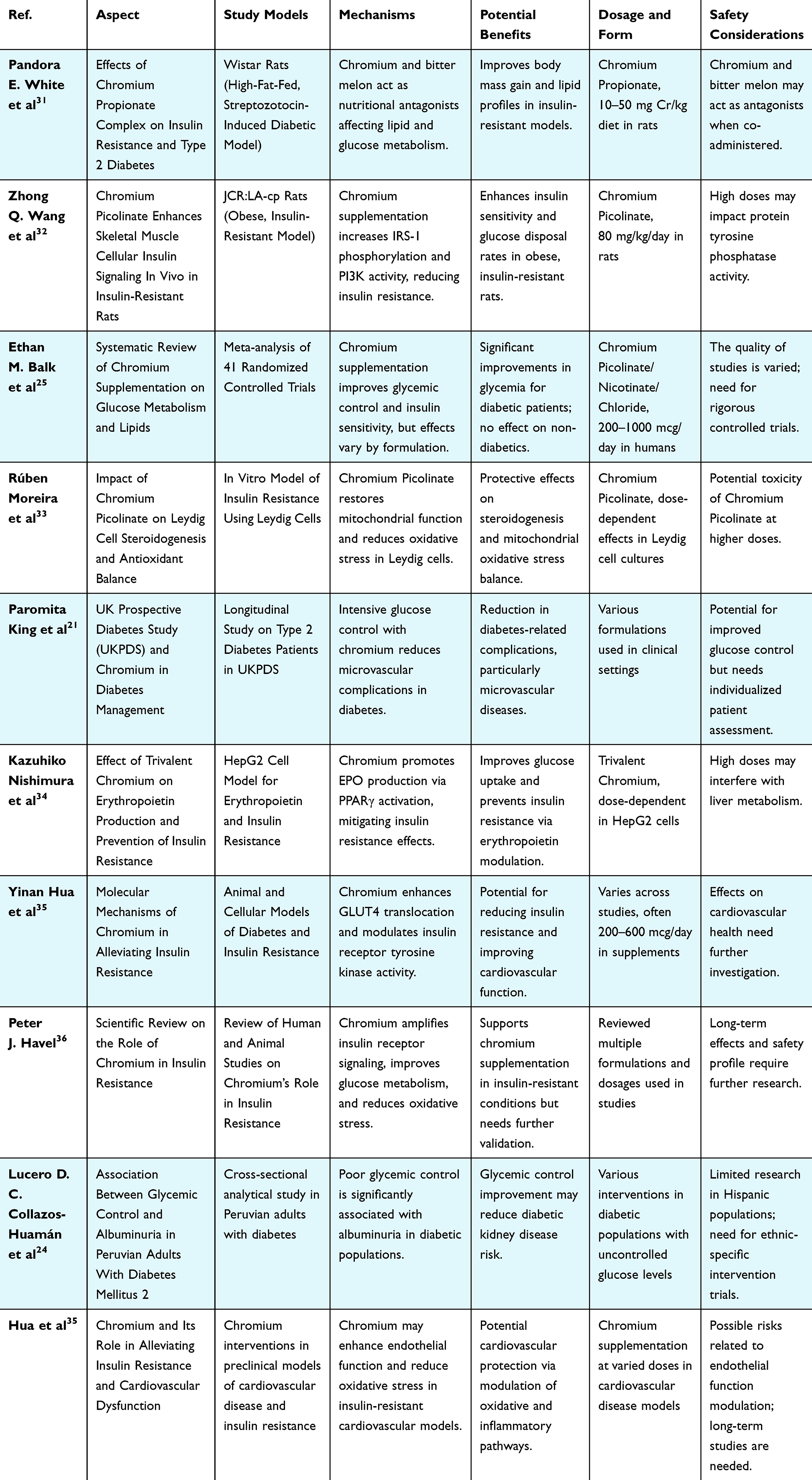 |
Table 3 Comprehensive Review of Chromium Studies: Study Models, Mechanisms, Benefits, and Clinical Insights in Metabolic Health |
Chromium primarily functions by potentiating insulin signaling. When Cr is deficient, the insulin receptor is unable to effectively interact with the insulin receptor substrate (IRS). As a result, the fat synthesis system required by adipose tissue is disrupted. This interruption ultimately disturbs the normal balance between glucose entry and storage, leading to insulin resistance. The insulin signaling cascade involves the activation of IRS, followed by phosphatidylinositol 3-kinase (PI3K), which generates the second messenger phosphatidylinositol-3,4,5-trisphosphate (PIP3). This, in turn, activates protein kinase B (Akt). Through this mechanism, Cr helps lower blood glucose levels by increasing the number of insulin receptors and transporters across the cell membrane. Consequently, this enhances insulin sensitivity, forming the core therapeutic mechanism of Cr in managing diabetes.37
For reference, in the insulin signaling cascade, insulin increases IRS activity in fat cells. The association between Cr and PI3K may stimulate tyrosine-targeted PI3K activity, leading to the production of PIP3. This process facilitates the accumulation of downstream signaling molecules, such as protein kinase B, as well as key components of normal kinase cascades, including Phosphoinositide-Dependent Kinase-1 (PDK1), in the cell plasma membrane, Figure 3. These molecules can then be activated through phosphorylation. Once protein kinase B undergoes phosphorylation, it can be directly activated by PDK1, thereby further propagating the insulin signaling pathway.38,39
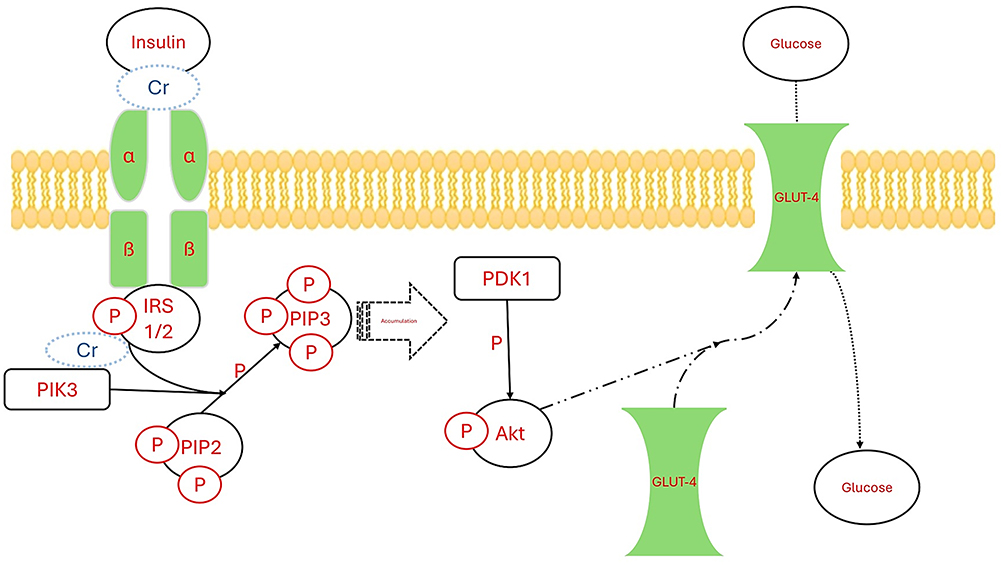 |
Figure 3 Potentiating effects of Cr over the insulin signaling pathway. The interaction between chromium (Cr) and phosphoinositide 3-kinase (PI3K) appears to enhance tyrosine-targeted PI3K activity, which subsequently promotes the synthesis of phosphatidylinositol (3,4,5)-trisphosphate (PIP3). This accumulation of PIP3 is crucial as it facilitates the recruitment and activation of downstream signaling molecules. Abbreviations: IRS, insulin receptor substrate; PDK1, Phosphoinositide-Dependent Kinase-1; Akt, protein kinase B; GLUT-4, Glucose transporter 4. |
Chromium’s (Cr) Role in Diabetes Management
Chromium’s Modulation of Insulin Signaling: Gene Expression, Receptor Activation, and Therapeutic Implications in Diabetes
Cr has been shown to influence gene expression as well as the phosphorylation of gene products involved in each major component of the insulin signaling pathway. These findings have been confirmed in various experimental systems.40 In a landmark study by Wang et al,32 rats with experimentally induced diabetes were administered Cr supplements, resulting in a threefold increase in insulin receptor mRNA, a 41% increase in insulin receptor number, and a 13-fold increase in insulin receptor kinase activity compared to diabetic animals that did not receive Cr supplementation. Additionally, the transcription of the insulin receptor gene in Cr-supplemented diabetic animals was 70% higher than in the unsupplemented diabetic group. These findings closely resemble those observed in certain models of insulin-dependent diabetes, where the downregulation of the insulin receptor is believed to contribute to impaired insulin action. This process is mediated through Cr’s ability to enhance the activity of the enzyme tyrosine kinase itself. Although further research is needed, it is reasonable to speculate that similar effects of Cr on gene expression might be observed in human diabetes, particularly in T2DM, where defects in insulin receptor kinase activity are commonly reported.32,41,42
Chromium’s Interaction with Other Molecules in Metabolic Pathways
A unified theory has been proposed regarding the role of Cr in nutrient metabolism, based on the structural similarities between low-molecular-weight chromium-binding substance (LMWCr), nutrients, and insulin-related peptide hormones and growth factors. It was concluded that Cr functions as a cofactor, enhancing the activity of all insulin-related peptide hormones and growth factors. Consequently, it amplifies the biological effects of their ligands on cell receptors, including those of insulin and insulin-like growth factor 1 (IGF-1).41,43
Impact of Chromium Deficiency on Glucose Homeostasis
Individuals with overt T2DM excrete significantly more glucose than normal in response to an oral dose of a complexing agent, possibly chromium picolinate. This effect, observed in over 40% of diabetic individuals, represents a notable metabolic abnormality. Despite variations in glucose tolerance and insulin sensitivity, the increased glucose excretion following the load appears to be independent of factors such as age, sex, diabetes severity, obesity, and dietary habits.14
Excessive glucose excretion primarily occurs in individuals with marginal or overt diabetic symptoms. Additionally, high Cr losses have been documented in a similar group of diabetic patients who were case-matched with individuals exhibiting normal and impaired glucose tolerance. Studies indicate that the response to glucose tolerance factor (GTF) in individuals with various types of disturbed carbohydrate metabolism is significantly lower, pointing to a Cr deficiency as a contributing factor to impaired glucose regulation. In at least 17 studies, dietary, blood, and urinary assessments have confirmed Cr depletion in diabetic patients, which is associated with increased glucose excretion and a subsequent reduction in biologically active Cr in the body. This depletion exacerbates insulin resistance, further impairing glucose metabolism. Clinical studies on chromium supplementation have shown that dietary intake of even small amounts of Cr has led to improvements in blood sugar control in most, though not all, T2DM patients. These findings provide strong evidence supporting the hypothesis that T2DM is associated with Cr deficiency. However, further randomized controlled trials (RCTs) are needed to establish the efficacy, optimal dosage, and long-term benefits of chromium supplementation in managing T2DM.11,14,25
Recent studies have shown that phosphoinositide 3-kinase (PI3K) activation is impaired in insulin-resistant patients, suggesting that IK fork-unresponsiveness may serve as an important molecular marker of insulin resistance. The kinase-specific protein kinase B (PKB) kinase is a 3-terminal kinase capable of phosphorylating the hydrophobic protein kinase domain of the palmitoylated TAG protein, thereby converting it into its hydrophilic structure. Protein kinase B plays a crucial role in stimulating several key components of glucose metabolism, making it an essential regulator in insulin signaling pathways.44,45
Potential Benefits of Chromium in Diabetes Management
Several hypotheses have been proposed to explain the biochemical role of chromium, particularly its function as a co-factor for insulin. Trivalent chromium (Cr3⁺) has been shown to enhance insulin activity in laboratory studies and may increase the number of insulin receptors or improve their ability to bind insulin in various experimental models. More recent evidence suggests that chromium may act as a bridging molecule, helping insulin bind more effectively to its receptors on cells, thereby improving insulin function. This hypothesis is initially based on observations that a low-molecular-weight chromium-binding substance (LMWCr) can potentiate insulin binding to erythrocytes in vitro. Subsequent studies have demonstrated the insulin-mimicking effects of LMWCr in cultured 3T3 adipocytes, along with a potentiating effect of LMWCr on the in vitro dephosphorylation of the insulin receptor. These effects are particularly significant, considering the proposed role of insulin resistance in the development of non-insulin-dependent diabetes mellitus (NIDDM). Recent reviews have examined these findings in the context of a new model for insulin-receptor interactions.35,46,47
Clinical Implications and Future Directions
Improving insulin sensitivity through Cr supplementation in individuals with MetS and impaired glucose metabolism may be associated with a reduced risk of cardiovascular morbidity and mortality. Considering that CVD is the leading cause of death in these conditions and that diabetics have a two to four-fold increase in cardiovascular mortality compared to non-diabetics, any intervention that successfully enhances insulin sensitivity and decreases blood lipid peroxidation would be expected to significantly reduce cardiovascular events.2
Although animal studies have provided intriguing insights into the long-term effects of Cr on insulin signaling, these findings have not been consistently replicated in other models. Currently, there is a lack of data on how Cr influences the insulin receptor or the conditions that precede insulin receptor substrate (IRS) recruitment and protein kinase activation.
Recent evidence suggests that Cr may enhance glucose uptake through GLUT4-independent pathways by promoting the translocation of GLUT1 to the plasma membrane.48 These effects are likely mediated through a direct action on enzymes. Furthermore, these in vitro findings align with the effects of trivalent chromium (Cr3⁺), which include an increase in the function or expression of various Cr3⁺-binding enzymes, as well as enhanced phosphorylation of several kinases at low insulin-mimetic doses. Future research investigating the impact of Cr on gene expression is expected to reinforce and expand our understanding of these mechanisms, potentially uncovering additional independent pathways through which Cr exerts its effects.35,49
Despite encouraging results from preclinical studies, research on chromium supplementation in individuals with diabetes and MetS has produced inconsistent results. Differences in study design, subjects and their glucose/insulin homeostasis status, Cr preparation and doses, and the presence of other glucose-lowering interventions have been suggested as explanations for these inconsistencies. As a result, there is a significant discrepancy in the literature regarding the dosage used, form of Cr given, duration of treatment, and varying degrees of patient glucose intolerance. Further research is needed to explicitly elucidate the effects of Cr on diabetes and MetS.50
Conclusion
The primary mechanism of Cr involves the potentiation of insulin signaling, specifically through the direct activation of the insulin receptor kinase. This activation lowers the Km of the receptor, which is non-specific, meaning that a lower concentration of insulin is required to produce a maximal cellular response. Consequently, this amplifies insulin-controlled metabolic processes. Moreover, Cr itself may function as an insulin cofactor by enhancing the binding of insulin to cells, acting as a bridging molecule between insulin and its receptor. By increasing insulin sensitivity through this mechanism, Cr effectively enhances the efficiency of glucose uptake and disposal in cells. This was identified by increased glucose disposal rates and rates of glycogen synthesis in the presence of Cr and insulin. The consequence of increasing insulin sensitivity and subsequent greater glucose and glycogen storage means there exists a lower blood glucose level. Demonstrable benefits of Cr supplementation, particularly concerning improvements in glucose homeostasis and insulin sensitivity, are observed in pre-existing chromium deficiency or overt diabetes mellitus. These populations exhibit a more pronounced response to Cr intervention. This may explain the association between Cr supplementation and lower odds of vascular dysfunction in MetS subjects. Cr also has a well-documented positive direct impact on gene expression in insulin-resistant subjects. While the essential form of Cr has not been clearly identified until now, perhaps more encouraging future research directions include developing reliable assessment tools for Cr levels as well as identifying the population groups most likely to benefit from Cr supplementation.
Data Sharing Statement
The data supporting this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors extend their appreciation to Umm Al-Qura University, Saudi Arabia for funding this research work through grant number: 26UQU4300045GSSR01.
Author Contributions
ATB: Conceptualization, Funding acquisition, Writing – original draft, Writing – review and editing.
MHM: Conceptualization, Data curation, Investigation, Resources, Visualization, Writing – original draft.
ASA: Conceptualization, Data curation, Investigation, Methodology, Resources, Supervision, Visualization, Writing – original draft, Writing – review and editing.
MAA: Data curation, Investigation, Resources, Software, Validation, Writing – original draft, Writing – review and editing.
GM: Data curation, Investigation, Resources, Validation, Writing – original draft, Writing – review and editing.
SHF: Data curation, Formal analysis, Investigation, Resources, Validation, Writing – original draft, Writing – review and editing.
WAN: Conceptualization, Data curation, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review and editing.
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research work was funded by Umm Al-Qura University, Saudi Arabia under grant number: 26UQU4300045GSSR01.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
1. Lemieux I, Després JP. Metabolic syndrome: past, present and future. Nutrients. 2020;12(11):3501. doi:10.3390/nu12113501
2. Silveira Rossi JL, Barbalho SM, de Araujo RR, Bechara MD, Sloan KP, Sloan LA. Metabolic syndrome and cardiovascular diseases: going beyond traditional risk factors. Diab Metab Res Rev. 2022;38(3):e3502. doi:10.1002/dmrr.3502
3. Onesi SO, Ignatius UE. Metabolic syndrome: performance of five different diagnostic criterias. Ind J Endocrinol Metab. 2014;18(4):496–15. doi:10.4103/2230-8210.137494
4. Pérez-Martínez P, Mikhailidis DP, Athyros VG, et al. Lifestyle recommendations for the prevention and management of metabolic syndrome: an international panel recommendation. Nutr Rev. 2017;75(5):307–326. doi:10.1093/nutrit/nux014
5. Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735–2752. doi:10.1161/CIRCULATIONAHA.105.169404
6. Nawaz SS, Siddiqui K. Plasminogen activator inhibitor-1 mediate downregulation of adiponectin in type 2 diabetes patients with metabolic syndrome. Cytokine X. 2022;4(1):100064. doi:10.1016/j.cytox.2022.100064
7. Mossberg K, Olausson J, Fryk E, Jern S, Jansson PA, Brogren H. The role of the platelet pool of Plasminogen Activator Inhibitor-1 in well-controlled type 2 diabetes patients. PLoS One. 2022;17(8):e0267833. doi:10.1371/journal.pone.0267833
8. Norton L, Shannon C, Gastaldelli A, DeFronzo RA. Insulin: the master regulator of glucose metabolism. Metabolism. 2022;129:155142. doi:10.1016/j.metabol.2022.155142
9. Kim JE, Kim JS, Jo MJ, et al. The roles and associated mechanisms of adipokines in development of metabolic syndrome. Molecules. 2022;27(2):334.
10. Khodavirdipour A, Haddadi F, Keshavarzi S. Chromium supplementation; negotiation with diabetes mellitus, hyperlipidemia and depression. J Diabetes Metab Disord. 2020;19(1):585–595. doi:10.1007/s40200-020-00501-8
11. Asbaghi O, Fatemeh N, Mahnaz RK, et al. Effects of chromium supplementation on glycemic control in patients with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Pharmacol Res. 2020;161:105098. doi:10.1016/j.phrs.2020.105098
12. Yin RV, Phung OJ. Effect of chromium supplementation on glycated hemoglobin and fasting plasma glucose in patients with diabetes mellitus. Nutr J. 2015;14:14. doi:10.1186/1475-2891-14-14
13. Paiva AN, Lima JG, Medeiros AC, et al. Beneficial effects of oral chromium picolinate supplementation on glycemic control in patients with type 2 diabetes: a randomized clinical study. J Trace Elem Med Biol. 2015;32:66–72. doi:10.1016/j.jtemb.2015.05.006
14. Costello RB, Dwyer JT, Bailey RL. Chromium supplements for glycemic control in type 2 diabetes: limited evidence of effectiveness. Nutr Rev. 2016;74(7):455–468. doi:10.1093/nutrit/nuw011
15. Pei D, Hsieh CH, Hung YJ, Li JC, Lee CH, Kuo SW. The influence of chromium chloride-containing milk to glycemic control of patients with type 2 diabetes mellitus: a randomized, double-blind, placebo-controlled trial. Metabolism. 2006;55(7):923–927. doi:10.1016/j.metabol.2006.02.021
16. Sharma S, Agrawal RP, Choudhary M, Jain S, Goyal S, Agarwal V. Beneficial effect of chromium supplementation on glucose, HbA1C and lipid variables in individuals with newly onset type-2 diabetes. J Trace Elem Med Biol. 2011;25(3):149–153. doi:10.1016/j.jtemb.2011.03.003
17. Masharani U, Gjerde C, McCoy S, et al. Chromium supplementation in non-obese non-diabetic subjects is associated with a decline in insulin sensitivity. BMC Endocr Disord. 2012;12:31. doi:10.1186/1472-6823-12-31
18. Zhao Y, Zhou M, Shang Y, et al. Effects of co-supplementation of chromium and magnesium on metabolic profiles, inflammation, and oxidative stress in impaired glucose tolerance. Diab Vasc Dis Res. 2024;21(1):14791641241228156. doi:10.1177/14791641241228156
19. Lalhriatpuii M, Chatterjee A, Dutta TK, Mohammad A, Patra AK. The effects of dietary inorganic and organic chromium supplementation on blood metabolites, hormones, and mineral composition of blood and internal organs in black Bengal goats. Biol Trace Elem Res. 2024;202(6):2547–2563. doi:10.1007/s12011-023-03856-0
20. Genchi G, Lauria G, Catalano A, Carocci A, Sinicropi MS. The double face of metals: the intriguing case of chromium. Appl Sci. 2021;11:638. doi:10.3390/app11020638
21. King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS): clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol. 1999;48(5):643–648. doi:10.1046/j.1365-2125.1999.00092.x
22. Shim K, Begum R, Yang C, Wang H. Complement activation in obesity, insulin resistance, and type 2 diabetes mellitus. World J Diab. 2020;11(1):1–12. doi:10.4239/wjd.v11.i1.1
23. Jamilian M, Foroozanfard F, Kavossian E, et al. Effects of chromium and carnitine co-supplementation on body weight and metabolic profiles in overweight and obese women with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled trial. Biol Trace Elem Res. 2020;193(2):334–341. doi:10.1007/s12011-019-01720-8
24. Collazos-Huamán LDC, Guerreros-Espino C, Herrera-Añazco P, Benites-Zapata VA. Association between glycemic control and albuminuria among Peruvian adults with diabetes mellitus 2: a cross-sectional analytical study. Sao Paulo Med J. 2022;140(6):767–774. doi:10.1590/1516-3180.2021.0448.r2.07022022
25. Balk EM, Tatsioni A, Lichtenstein AH, Lau J, Pittas AG. Effect of chromium supplementation on glucose metabolism and lipids: a systematic review of randomized controlled trials. Diab Care. 2007;30(8):2154–2163. doi:10.2337/dc06-0996
26. Vincent JB. Chapter 29 - Beneficial Effects of Chromium(III) and Vanadium Supplements in Diabetes. In: Bagchi D, Nair S, editors. Nutritional and Therapeutic Interventions for Diabetes and Metabolic Syndrome (Second Edition). Academic Press; 2018:365–374.
27. Król E, Krejpcio Z. Evaluation of anti-diabetic potential of chromium(III) propionate complex in high-fat diet fed and STZ injected rats. Food Chem Toxicol. 2011;49(12):3217–3223. doi:10.1016/j.fct.2011.09.006
28. Mozaffari MS, Abdelsayed R, Liu JY, Wimborne H, El-Remessy A, El-Marakby A. Effects of chromium picolinate on glycemic control and kidney of the obese Zucker rat. Nutr Metab. 2009;6:51. doi:10.1186/1743-7075-6-51
29. Krejpcio Z. Chapter 6 - Effects of chromium(III) supplementation on rodent models of insulin resistance and diabetes. In: Vincent JB, editor. The Nutritional Biochemistry of Chromium (III).
30. Farrokhian A, Mahmoodian M, Bahmani F, Amirani E, Shafabakhsh R, Asemi Z. The influences of chromium supplementation on metabolic status in patients with type 2 diabetes mellitus and coronary heart disease. Biol Trace Elem Res. 2020;194(2):313–320. doi:10.1007/s12011-019-01783-7
31. White PE, Król E, Szwengiel A, et al. Effects of bitter melon and a chromium propionate complex on symptoms of insulin resistance and type 2 diabetes in rat models. Biol Trace Elem Res. 2021;199(3):1013–1026. doi:10.1007/s12011-020-02202-y
32. Wang ZQ, Zhang XH, Russell JC, Hulver M, Cefalu WT. Chromium picolinate enhances skeletal muscle cellular insulin signaling in vivo in obese, insulin-resistant JCR:LA-cp rats. J Nutr. 2006;136(2):415–420. doi:10.1093/jn/136.2.415
33. Moreira R, Martins AD, Ferreira R, Alves MG, Pereira ML, Oliveira PF. Impact of chromium picolinate on leydig cell steroidogenesis and antioxidant balance using an in vitro insulin resistance model. Antioxidants (Basel). 2023;13(1). doi:10.3390/antiox13010040
34. Nishimura K, Iitaka S, Nakagawa H. Effect of trivalent chromium on erythropoietin production and the prevention of insulin resistance in HepG2 cells. Arch Biochem Biophys. 2021;708:108960. doi:10.1016/j.abb.2021.108960
35. Hua Y, Clark S, Ren J, Sreejayan N. Molecular mechanisms of chromium in alleviating insulin resistance. J Nutr Biochem. 2012;23(4):313–319. doi:10.1016/j.jnutbio.2011.11.001
36. Havel PJ. A scientific review: the role of chromium in insulin resistance. Diab Educ. 2004;2004:2–14.
37. Wang ZQ, Yu Y, Zhang XH, Komorowski J. Chromium-insulin reduces insulin clearance and enhances insulin signaling by suppressing hepatic insulin-degrading enzyme and proteasome protein expression in KKAy mice. Front Endocrinol. 2014;5:99. doi:10.3389/fendo.2014.00099
38. Kiren G, Severcan Ç, Severcan SM, Paşaoğlu H. The effect of curcumin on PI3K/Akt and AMPK pathways in insulin resistance induced by fructose. Turk J Biochem. 2024;49(4):518–524. doi:10.1515/tjb-2024-0027
39. Kearney AL, Norris DM, Ghomlaghi M, et al. Akt phosphorylates insulin receptor substrate to limit PI3K-mediated PIP3 synthesis. Elife. 2021;10. doi:10.7554/eLife.66942
40. Chirivi M, Abou-Rjeileh U, Gandy J, et al. Chromium and palmitic acid supplementation modulate adipose tissue insulin sensitivity in postpartum dairy cows. J Dairy Sci. 2025;108(1):1078–1091. doi:10.3168/jds.2024-24972
41. Kooshki F, Tutunchi H, Vajdi M, et al. A Comprehensive insight into the effect of chromium supplementation on oxidative stress indices in diabetes mellitus: a systematic review. Clin Exp Pharmacol Physiol. 2021;48(3):291–309. doi:10.1111/1440-1681.13462
42. Imanparast F, Javaheri J, Kamankesh F, et al. The effects of chromium and vitamin D(3) co-supplementation on insulin resistance and tumor necrosis factor-alpha in type 2 diabetes: a randomized placebo-controlled trial. Appl Physiol Nutr Metab. 2020;45(5):471–477. doi:10.1139/apnm-2019-0113
43. Müller GA. Insulin-like and mimetic molecules from non-mammalian organisms: potential relevance for drug discovery. Arch Physiol Biochem. 2020;126(5):420–429. doi:10.1080/13813455.2018.1551906
44. Ramasubbu K, Rajeswari VD. Impairment of insulin signaling pathway PI3K/Akt/mTOR and insulin resistance induced AGEs on diabetes mellitus and neurodegenerative diseases: a perspective review. Mol Cell Biochem. 2023;478(6):1307–1324. doi:10.1007/s11010-022-04587-x
45. Götting I, Jendrossek V, Matschke J. A new twist in protein Kinase B/Akt signaling: role of altered cancer cell metabolism in akt-mediated therapy resistance. Int J Mol Sci. 2020;21(22):8563. doi:10.3390/ijms21228563
46. Sawicka E, Jurkowska K, Piwowar A. Chromium (III) and chromium (VI) as important players in the induction of genotoxicity - current view. Ann Agric Environ Med. 2021;28(1):1–10. doi:10.26444/aaem/118228
47. Vincent JB. Mechanisms of chromium action: low-molecular-weight chromium-binding substance. J Am Coll Nutr. 1999;18(1):6–12. doi:10.1080/07315724.1999.10718821
48. Zheng H, Hu Y, Shao M, Chen S, Qi S. Chromium picolinate protects against testicular damage in STZ-induced diabetic rats via anti-inflammation, anti-oxidation, inhibiting apoptosis, and regulating the TGF-β1/Smad pathway. Molecules. 2023;28(22):7669. doi:10.3390/molecules28227669
49. Ferreira LMR, Cunha-Oliveira T, Sobral MC, Abreu PL, Alpoim MC, Urbano AM. Impact of carcinogenic chromium on the cellular response to proteotoxic stress. Int J Mol Sci. 2019;20(19):4901. doi:10.3390/ijms20194901
50. Asbaghi O, Naeini F, Ashtary-Larky D, et al. Effects of chromium supplementation on lipid profile in patients with type 2 diabetes: a systematic review and dose-response meta-analysis of randomized controlled trials. J Trace Elem Med Biol. 2021;66:126741. doi:10.1016/j.jtemb.2021.126741
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Omentin as an Independent Predictor of Metabolic Syndrome and Obesity Among Adolescents in Northeast China
Sun X, Li T, Tian Y, Ren S, Li L, Li P
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3913-3922
Published Date: 15 December 2022
The Association of HDL2b with Metabolic Syndrome Among Normal HDL-C Populations in Southern China
Chen T, Wu S, Feng L, Long S, Liu Y, Lu W, Chen W, Hong G, Zhou L, Wang F, Luo Y, Zou H
Diabetes, Metabolic Syndrome and Obesity 2024, 17:363-377
Published Date: 23 January 2024
Effect of 8-Methyl Nonanoic Acid, a Degradation By-Product of Dihydrocapsaicin, on Energy and Glucose Homeostasis in Diet-Induced Obese Mice
Keawsomnuk P, Den-Udom T, Thongin S, Wiriyakulsit N, Mukthung C, Boonthip C, Pittayakhajonwut P, Ketsawatsomkron P, Wichai U, Muta K
Journal of Experimental Pharmacology 2025, 17:555-570
Published Date: 13 August 2025
Association Between Platelet Parameters and Metabolic Syndrome in Residents of Wuhu, China: A Mediation Analysis of Insulin Resistance

Zhou L, Wu H, Wu T, Wang X, Song E, Su F, Ezeokafor CA, Wu Y, Ma X, Wang T, Wen Y
Diabetes, Metabolic Syndrome and Obesity 2026, 19:575645
Published Date: 12 February 2026
Elevated Visceral Adiposity Index is Associated with Reproductive Endocrine Characteristics, and Adverse Pregnancy Outcomes in Chinese Women with Polycystic Ovary Syndrome
Shi B, Feng J, Lu F, Guan M, Yu J, Gao Z, Wang Y, Cong J, Ma H, Han C, Yang W, Wu X, Gao J
International Journal of Women's Health 2026, 18:575900
Published Date: 17 June 2026