Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Choroidal Thickness and Postural Stability in Young Adults: Exploring Ocular Contributions to Balance and Fall Prevention
Authors Althomali MM ![]() , Alkhudhair AM, Alanazi MK
, Alkhudhair AM, Alanazi MK ![]() , Alotaibi WM
, Alotaibi WM ![]() , Aldakhil S
, Aldakhil S ![]() , Alshammeri SR, Alharbi AA, Alhazmi MS
, Alshammeri SR, Alharbi AA, Alhazmi MS
Received 6 October 2025
Accepted for publication 22 January 2026
Published 10 February 2026 Volume 2026:19 566806
DOI https://doi.org/10.2147/JMDH.S566806
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Mohammed M Althomali,1,* Abdulaziz M Alkhudhair,1 Muteb K Alanazi,1 Wafa M Alotaibi,1 Sulaiman Aldakhil,2 Saleh R Alshammeri,2 Ahmad A Alharbi,1 Mohammed S Alhazmi1,*
1Optometry Department, College of Applied Medical Sciences, King Saud University, Riyadh, 11362, Saudi Arabia; 2Department of Optometry, College of Applied Medical Sciences, Qassim University, Buraydah, 51452, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Mohammed M Althomali, Optometry Department, College of Applied Medical Sciences, King Saud University, Riyadh, 11362, Saudi Arabia, Tel +966114693613, Fax +966114693536, Email [email protected]
Purpose: To investigate the relationship between choroidal thickness and postural stability in healthy young adults, focusing on the influence of refractive error and choroidal thickness distribution across quadrants.
Patients and Methods: A cross-sectional study was conducted with 24 young adults (19 men, 5 women; mean age, 22 ± 2.06 years). Refractive error was measured using an autorefractor, and choroidal thickness was assessed with optical coherence tomography. Postural stability was evaluated using a force platform under quiet stance and one-legged stance conditions. Choroidal thickness was analyzed across quadrants and rings, and its correlation with postural sway parameters was determined using univariate analyses.
Results: The mean choroidal thickness was 280 ± 77.51 μm, with the nasal quadrant being the thinnest and the inferior quadrant the thickest. Myopic participants had thinner choroids (mean, 273 ± 77.25 μm) compared to non-myopes (mean, 288 ± 77.08 μm). A positive correlation (r = 0.279, P < 0.001) was found between choroidal thickness and refractive error. In quiet stance, increased choroidal thickness was negatively correlated with anterior-posterior sway but positively correlated with medial-lateral sway. During one-legged stance, choroidal thickness was negatively correlated with most postural sway measures, except for maximum medial-lateral sway.
Conclusion: Choroidal thickness is associated with refractive error and postural stability. Regional differences in choroidal thickness may play a role in balance control, highlighting the potential relevance of ocular structural health to mechanisms underlying balance control and fall risk. Further research is needed to explore the mechanisms linking choroidal dynamics and postural control.
Keywords: balance, force platform, choroidal thickness, falls
Introduction
Maintaining postural stability involves three primary sensory systems: the visual system, which directs motion and navigates obstacles; the vestibular system, which detects angular and linear acceleration; and the somatosensory system, which senses body position, movement, and center of mass (COM) orientation.1 Postural balance is disrupted by shifts in the center of gravity or COM of the body, with the somatosensory system compensating for such displacements to prevent falls.2,3 Compensatory mechanisms, such as ankle and hip strategies, adjust body posture when significant COM displacement occurs,4,5 helping to maintain stability.6
Previous research has shown that the visual system is essential for balance control, with reduced visual acuity strongly associated with increased fall risk and postural instability.7 Specific visual functions, including binocular vision, stereoacuity, and intermediate acuity, correlate with movement control.8 Notably, multifocal lenses increase toe clearance variability. This change affects stepping patterns and increases the risk of tripping. This is likely due to image magnification and discontinuities between focal segments.9,10 Similarly, myopic and hyperopic defocus have distinct effects on stepping dynamics, with myopic defocus leading to increased vertical toe clearance.11 These findings show that postural stability depends not only on the visual function but also on the quality and reliability of retinal image processing. This suggests that understanding the role of specific ocular structures is imperative for understanding their contribution to postural control. However, the contribution of specific ocular structures on postural control remains poorly understood, particularly with respect to posterior ocular tissues.
The choroid, primarily composed of blood vessels, plays a vital role in ocular health by nourishing the outer retina and supporting the emmetropization process.12 Its thickness varies significantly based on physiological and pathological factors, including refractive error, axial length, and disease states such as diabetes and age-related macular degeneration.13,14 Additionally, choroidal thickness fluctuates with diurnal changes and environmental stimuli such as light exposure.15 Myopic eyes often have thinner choroids than emmetropic eyes, which has implications for axial elongation and scleral hypoxia.16 Optical defocus also causes localized choroidal thickening in specific regions. This suggests a targeted response to retinal image blur.17 The choroidal thickness can be measured using the Optical Coherence Tomography (OCT). This non-invasive imaging modality can be implemented in research and clinical settings. The OCT has been used safely to capture repeatable, precise images of ocular anatomy, refractive development, and disease-related structural changes. Recent advances in OCT technology have given researchers further applications, thereby strengthening the role of OCT based imaging in ophthalmic research.18
Despite growing interest in the relationship between ocular physiology and postural control, no studies to date have specifically examined the association between choroidal thickness and objective measures of postural stability. Studying this relationship in young adults allows underlying mechanisms to be explored in a population that is relatively free from age-related neurodegenerative or musculoskeletal confounders, providing insight into early ocular contributions to balance regulation.
Understanding the interaction between vision, choroidal thickness, and postural stability may improve our knowledge of postural control, which might transfer to other domains such as fall prevention strategies. Particularly for older adults and individuals with visual impairments. This study examines the effects of choroidal thickness on postural control, exploring the potential role of choroidal dynamics in balance maintenance and fall risk. To our knowledge, this is the first study to investigate the relationship between choroidal thickness and postural stability using objective force platform measurements.
Materials and Methods
Study Design, Participants, and Eligibility Criteria
This cross-sectional study initially recruited 38 healthy young adults. Participants were excluded if more than two optical coherence tomography (OCT) scans of the same type (horizontal or vertical) were unclear due to motion artifacts or poor signal strength. Based on this criterion, 14 individuals were excluded because accurate choroidal thickness measurements could not be obtained. Ultimately, 24 participants (19 men and 5 women) were included in the final analysis. Exclusion criteria also included any history of ocular pathology, ocular disease, or ocular surgery, as well as current pregnancy, given the potential influence of these conditions on choroidal structure and thickness.
Lifestyle and Temporal Covariates
Self-reported data on smoking and caffeine consumption habits were collected during the data collection process. Additionally, the time of day during which choroidal thickness was measured and the participants’ wake-up time were recorded, based on previous studies suggesting these variables influence choroidal thickness.19–21
Ocular Measurements
All participants underwent a comprehensive ocular examination prior to participation in the study. This included measurement of refractive error and visual acuity, as well as screening for ocular pathology. Participants presenting any evidence of present ocular disease or conditions known to affect choroidal structure were excluded from the study. The refractive error was measured using the TOPCON KR8800 Autorefractor-Keratometer. Choroidal thickness measurements were obtained in accordance with our previously published study,22 using the TOPCON Maestro 3D spectral-domain OCT-1. This device operates at a scanning speed of 50,000 A-scans/s, with axial and transverse resolutions of 20 µm and 6 µm, respectively. For each eye, three high-resolution horizontal and three vertical single 9-mm scans were captured at the same location, all centered on the fovea and acquired under nonmydriatic conditions. Given the known regional variation in choroidal thickness,23–25 measurements were taken across five eccentric zones (foveal, parafoveal, perifoveal, near-periphery, and periphery) and in four quadrants (superior, temporal, inferior, and nasal) extending 4.5 mm from the foveal center (Figure 1). Only scans comprising a minimum of 30 averaged B-scans were included in the analysis. Choroidal thickness was defined as the vertical distance between the outer border of the retinal pigment epithelium and the inner scleral surface. For statistical analysis, each choroidal image obtained for the measurements mentioned above was analysed separately across all regions, quadrants, and zones. These measurements were then examined in relation to postural stability outcomes by correlating subject-level choroidal thickness values with postural sway measures recorded during the various postural sway measurements.
 |
Figure 1 Representative single-line vertical OCT scans are shown as the original image (A) and the contrast-enhanced image (B), alongside horizontal scans displayed as the original image (C) and the contrast-enhanced image (D). The red lines mark the foveal pit, whereas the green and blue lines delineate the anterior and posterior borders of the choroid, respectively. (Adapted with permission from Althomali et al).22 |
Choroidal thickness was quantified using a validated MATLAB-based algorithm developed by Alonso-Caneiro et al26 and Read et al27 with contrast enhancement features applied to improve visualization of the choroidoscleral junction (Figure 2). Three trained clinicians independently evaluated all scans, and inter-rater reliability was excellent, with an intraclass correlation coefficient of 0.98 (95% confidence interval [CI]: 0.97–0.99), calculated using a two-way mixed-effects model for absolute agreement. The software produced 185 measurement points per 1 mm of lateral width, resulting in approximately 1,760 data points per OCT scan. To correct for individual differences in ocular magnification, axial length adjustments were applied to the transverse scale using a method described by Read et al.28 Final choroidal thickness values for each region were derived by averaging the corresponding data points based on predefined eccentricities.
 |
Figure 2 Analysis of optical coherence tomography (OCT) images using the OCT-Tool software of a high-quality image used for choroidal thickness evaluation. |
Posturography
Postural sway was measured using the AccuGAIT AMTI 1000 Hz force platform. This device calculates the center of pressure (COP) and the three ground reaction forces. Data were processed using VICON NEXUS software. The test conditions included quiet stance with eyes open (EO), one-legged stance test (OLST), and eyes closed (EC), with each condition repeated three times. The quiet stance condition lasted 60s, while the one-legged stance condition lasted 30s, as some participants experienced difficulty maintaining balance for 60s without moving their foot or placing the other foot on the ground. In these cases, the test was cancelled and retaken. During the tests, participants were instructed to focus on a distant target 6 meters away while standing barefoot on the force plate platform. To avoid any distractions, the examiner refrained from physical or verbal communication with participants. Data from the force platform were then analyzed using the VISUAL 3D program. The first 5 and last 5 s of the data were removed, and a low-pass Butterworth filter with a cutoff frequency of 6 Hz was applied to remove noise. Outcome measures for COP included the standard deviation, maximum, range, and cumulative path length for anterior-posterior and medial-lateral forces. The cumulative path length represents the total distance that the COP moved during the test, measured in millimeters.
Statistical Analysis
Statistical analysis was performed using SPSS software (SPSS Institute Inc., Chicago, Illinois). A univariate analysis was conducted to assess the correlations between different measures. The Kolmogorov–Smirnov test was used to assess the normality of the data. A two-tailed test was employed to determine statistical significance.
Results
A total of 24 healthy young adults participated. The cohort comprised 79.2% men (n = 19) and 20.8% women (n = 5). The mean age of the participants was 22 ± 2.06 years. The sample was divided into two groups according to their refractive error: myopes and non-myopes (Table 1). The myopic group included participants with a spherical equivalent of −0.50 D or lower, while the non-myopic group had a spherical equivalent of −0.37 D or higher.
 |
Table 1 Classification of the Sample According to Sex and Refractive Condition (Spheq = Spherical Equivalent) |
Choroidal thickness data were normally distributed (Figure 3). Thickness was analyzed according to four quadrants: nasal, superior, temporal, and inferior, and across five concentric rings: foveal, parafoveal, perifoveal, near periphery, and periphery (Figure 4).
 |
Figure 3 Normal distribution of the mean choroidal thickness observed in this study across all zones, quadrants, and participants. |
 |
Figure 4 Choroidal thickness in myopic and non-myopic groups across all quadrants and rings. |
The mean choroidal thickness for all participants was 280 ± 77.51 µm. For the non-myopic group, it was 288 ± 77.08 µm, and for the myopic group, 273 ± 77.25 µm. The nasal quadrant was the thinnest across all rings. The mean choroidal thickness was highest in the inferior quadrant (311.07 µm), followed by the superior (303.78 µm), temporal (281.10 µm), and nasal (227.34 µm) quadrants. Standard deviations ranged from 57.51 µm in the inferior quadrant to 83.09 µm in the nasal quadrant, indicating greater variability in nasal measurements. The standard errors of the mean ranged from 3.71 µm (inferior) to 5.4 µm (nasal). The 95% CI was narrowest in the inferior quadrant (303.76–318.39 µm) and widest in the nasal quadrant (216.71–237.98 µm), reflecting greater uncertainty in the nasal measurements. The nasal quadrant also exhibited the greatest range of choroidal thickness values (379.6 µm), while the smallest range was observed in the inferior quadrant (270.47 µm). Interquartile ranges were largest in the nasal quadrant (126.74 µm) and smallest in the inferior quadrant (91.26 µm), suggesting a broader distribution of values in the nasal region (Table 2). The peak choroidal thickness was observed in the subfoveal area (Ring 1) (Table 3), with thickness decreasing toward the periphery. The correlation between mean choroidal thickness and spherical equivalent for all participants was 0.279 (P < 0.001), indicating that participants with more positive spherical equivalents had thicker choroids.
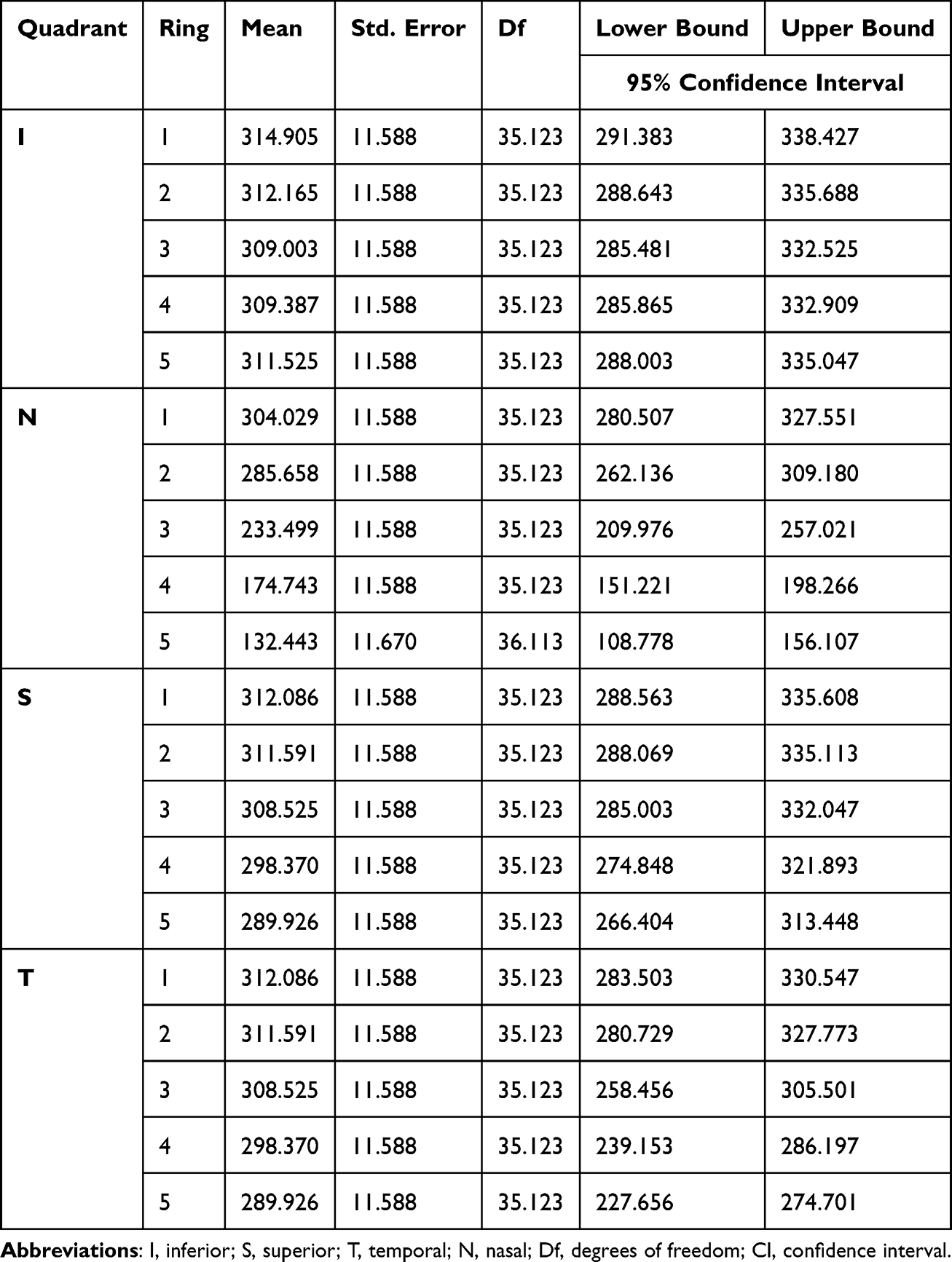 |
Table 2 Mean Choroidal Thickness in Micrometers (µm) for All Participants Represented by Quadrants and Rings |
 |
Table 3 Mean Choroidal Thickness in Micrometers (µm) for All Participants, Represented by the Rings |
To address the main study objective, the correlations between choroidal thickness and postural measures were examined using univariate regression analyses (Table 4). In the quiet stance condition, mean choroidal thickness was negatively correlated with anterior–posterior range and maximum sway (P = 0.003 and 0.001, respectively). However, it was positively correlated with medial–lateral (ML) standard deviation and range (P < 0.001 and 0.001, respectively). In the one-legged stance, mean choroidal thickness was negatively correlated with all postural sway measures except maximum sway in the ML direction (P = 0.002).
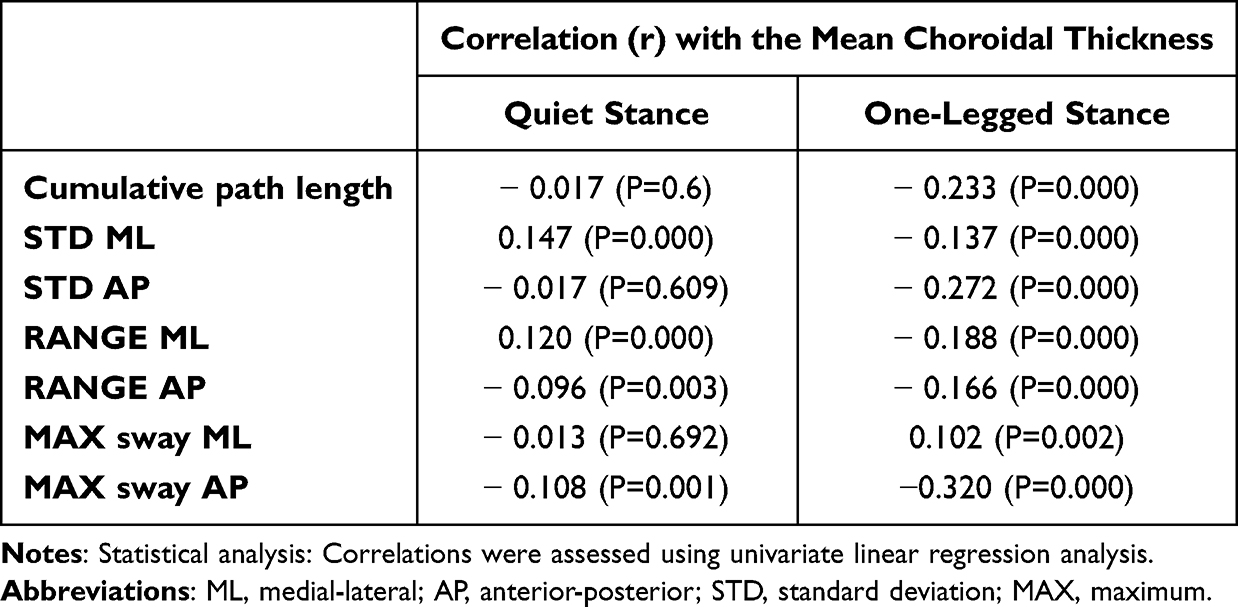 |
Table 4 Correlation Between Choroidal Thickness and Different Measures of Postural Sway |
Discussion
In this cross‐sectional study of healthy young adults, the choroidal thickness varied regionally, with the nasal quadrant being the thinnest and the inferior quadrant the thickest. Myopic participants exhibited thinner choroids compared to non‐myopes. Importantly, variations in choroidal thickness were associated with postural sway during both quiet and one-legged stance conditions, indicating a relationship between ocular structural characteristics and balance control. In quiet stance, greater choroidal thickness was linked to reduced anterior–posterior sway but increased medial–lateral variability. During one‐legged stance, thicker choroids were associated with lower sway metrics across nearly all parameters. While this study did not directly measure falls, postural sway is a known indicator of balance control and falls risk. Greater sway metrics are linked to poorer stability in older adults.29 Visual input plays a critical role in postural regulation, and impairments in visual quality, particularly those affecting the visual acuity, visual field, contrast sensitivity, and spatial awareness, have been consistently associated with increased postural instability and falls in older adults.30,31 Choroidal thickness, by influencing retinal health, perfusion, and optical quality, may therefore represent an indirect structural factor contributing to balance performance. From this perspective, the observed links between choroidal thickness and postural sway offer a clearer understanding of how the ocular structure characteristics may relate to fall risk pathways rather than direct fall outcomes.
The subfoveal choroidal thickness observed here (309 µm) (Table 3) closely mirrors values reported in a young Saudi cohort (300 ± 60 µm),22 with the thickest superior (309 ± 57 µm) and thinnest nasal (229 ± 76 µm) profiles, but differ markedly from other ethnicities.22 For comparison, Karapetyan et al found a mean subfoveal thickness of 403.6 ± 37.4 µm in White individuals, 372.47 ± 31.4 µm in Africans, and 383.6 ± 40 µm in Asian individuals.32 In contrast, a large multiethnic Asian cohort reported a much lower mean subfoveal thickness of 255.2 ± 102.6 µm.33 These discrepancies may be attributed to genetic factors, environmental influences, or measurement techniques, highlighting the importance of understanding choroidal thickness in different ethnic groups.
Myopic eyes in our sample displayed significant thinning of the choroid, supporting the well‐documented link between increasing myopia and reduced choroidal thickness.12 Mechanistically, the vasculature of the choroid supplies the outer retina and modulates scleral growth via thickness changes in response to defocus, implicating it in emmetropization and refractive development.34
Regarding regional differences in choroidal thickness, our study confirmed that the nasal quadrant had the thinnest choroid across all rings. This finding is consistent with earlier studies.14,35,36 This specific thinning in the nasal quadrant may be related to physiological or anatomical factors that are unique to that side of the eye, warranting further investigation. In terms of refractive error, our univariate linear regression analysis revealed a positive and significant correlation between choroidal thickness and spherical equivalent, suggesting that individuals with more hyperopic refractive errors tend to have thicker choroids. This finding aligns with prior research showing a relationship between higher refractive error (more positive spherical equivalent) and increased choroidal thickness.
Our study found that the myopic group had decreased choroidal thickness, with a mean subfoveal choroidal thickness of 301.77 µm. This is in line with published literature, in which myopic individuals typically exhibit thinner choroidal layers compared to non-myopes.14,35,36 For instance, in Caucasians, the mean subfoveal choroidal thickness for myopes was reported to be 307.04 µm,14 which is very similar to the value observed in our study. These findings support the hypothesis that myopia is associated with choroidal thinning, which may reflect underlying ocular adaptations to refractive error.
The visual input is critical for balance control, with impaired acuity, contrast sensitivity, and depth perception all identified as risk factors for increased sway and falls in older adults.7 Seminal work by Lee and Aronson demonstrated that visual motion signals alone can induce postural adjustments, underscoring the central role vision plays in stability.31 Here, we extend these findings by linking choroidal morphology to postural behavior. Thicker choroids were significantly protective against antero‐posterior instability but corresponded to greater medio‐lateral variability under quiet‐stance conditions. This pattern is similar to the sway differences caused by vision in people with myopia during stationary tasks. In the more challenging one‐legged stance, increased choroidal thickness correlated with reduced sway across most parameters. This supports other reports that corrected vision yields superior dynamic stability compared to myopic or eyes‐closed states.1
The choroid accounts for 85% of ocular blood flow. It nourishes the outer retina, and it adjusts its thickness in response to optical defocus, thickening with hyperopic stimuli and thinning with myopic stimuli, to guide ocular growth.12 Diurnal changes in choroidal thickness occur, with it being thicker at night and thinner during the day. These changes create variability that may affect measurements and functional outcomes, with peak thickness typically occurring between 3:00 and 9:00 AM and nadirs in the afternoon.20 As thicker choroids may enhance peripheral image quality and retinal perfusion, they could bolster the visual contributions to balance, whereas thinner choroids in myopia might exacerbate peripheral minification and spatial uncertainty,34 increasing postural sway.
Visual blur, caused by spectacle magnification or dioptric defocus, significantly changes toe-clearance control and increases the chance of tripping. Johnson et al demonstrated that older adults who wear multifocal spectacles exhibit significantly greater variability in minimum toe clearance during stair ascent than those who wear single‐distance lenses.9 Elliott and Chapman similarly reported that positive‐blur lenses led to increased vertical toe clearance, presumably as a safety adaptation, whereas negative‐blur lenses produced the opposite effect.11 Rietdyk and Rhea further showed that obstructing the lower visual field increased both lead and trail toe‐clearance variability when negotiating obstacles, highlighting the importance of unobstructed peripheral vision for precise foot trajectory regulation.37 Collectively, these findings underscore how moderate image blur can disrupt the visuomotor integration essential for stable gait, a principle that informs our exploration of choroidal influences on postural control.
The role of choroidal thickness in postural stability is an area of growing interest. Previous studies have suggested that visual acuity and refractive errors can influence postural sway and balance. Moon et al38 found that participants wearing minus lenses (myopic correction) exhibited greater sway and a higher fall risk index. Elliott and Chapman reported that myopic individuals displayed reduced toe clearance during stepping tasks.11 This can increase their risk of tripping and falling. These findings support the notion that refractive errors, particularly myopia, may lead to postural instability and a higher chance of falling.
In our study, the spherical equivalent showed a negative trend with cumulative path length in the one-legged stance. However, this association was not statistically significant. While the data suggest that more myopic individuals may show greater postural sway, this finding should be interpreted with caution. The potential role of peripheral image minification and reduced spatial awareness in myopes remains a hypothesis warranting further investigation.
Interestingly, the correlation between choroidal thickness and postural sway in our study was complex. While the mean choroidal thickness was associated with postural sway measures under certain conditions, cumulative path length did not show significant differences across the quadrants of choroidal thickness. This suggests that while choroidal thickness may relate to refractive error and potentially influence balance, other factors, such as central visual acuity or dynamic balance control mechanisms, might have a bigger impact on postural stability.
A major strength of this study is its use of high-resolution, reproducible OCT imaging to assess choroidal thickness and objective, high-frequency force platform analysis to measure postural stability. This combination ensures precise structural and functional correlations under controlled testing conditions. The cross‐sectional design of the study precludes causal inference. The findings for the young, healthy cohort may not apply to older adults or clinical populations with greater choroidal thinning or balance impairment. OCT segmentation relied on automated MATLAB algorithms. While these algorithms are efficient, they might introduce measurement bias in borderline scans.
Conclusion
This study found that individuals with myopic refractive errors, who typically have thinner choroids, exhibit greater postural sway, especially during challenging balance tasks such as the one-legged stance. Variations in choroidal thickness affected postural sway in different conditions. This might indicate that characteristics of the eye’s structure could influence balance control. These links suggest that choroidal shape may play a role in maintaining balance, possibly by affecting peripheral vision and spatial awareness. Although the study population comprised of healthy young adults, these findings may have broader implications, especially for older adults, in whom age related choroidal thinning may exacerbate balance impairments and increase fall risk.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of King Saud University (protocol code E-21-5987, 23/08/2021) for studies involving humans. Written informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Mohammed M. Althomali and Mohammed S. Alhazmi contributed equally to this work and share joint first authorship.
Funding
The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding this work through the Ongoing Research Funding Program (ORF-2026-1162).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang Z, Xiao X. Characteristics of the postural stability of the lower limb in different visual states of undergraduate students with moderate myopia. Front Physiol. 2023;13:1092710. doi:10.3389/fphys.2022.1092710
2. Okayama Y, Maekawa M, Daikuya S. Postural control strategies with alterations in visual input conditions in a standing position. Eur J Appl Physiol. 2024;125(3):707–12. doi:10.1007/s00421-024-05635-8
3. Onofrei RR, Amaricai E. Postural balance in relation with vision and physical activity in healthy young adults. IJERPH. 2022;19(9):5021. doi:10.3390/ijerph19095021
4. Jehu DA, Davis JC, Falck RS, et al. Risk factors for recurrent falls in older adults: a systematic review with meta-analysis. Maturitas. 2021;144:23–28. doi:10.1016/j.maturitas.2020.10.021
5. Salonen L, Kivelä SL. Eye diseases and impaired vision as possible risk factors for recurrent falls in the aged: a systematic review. Curr Gerontol Geriatr Res. 2012;2012:1–10. doi:10.1155/2012/271481
6. Duarte MB, da Silva Almeida GC, Costa KHA, et al. Anticipatory postural adjustments in older versus young adults: a systematic review and meta-analysis. Syst Rev. 2022;11(1):1–14. doi:10.1186/s13643-022-02116-x
7. Black A, Wood J. Vision and falls. Clin Exp Optom and Clin Exp Optom. 2005;88(4):212–222. doi:10.1111/j.1444-0938.2005.tb06699.x
8. Althomali MM, Leat SJ. Binocular vision disorders and visual attention: associations with balance and mobility in older adults. JAPA. 2018;26(2):235–247. doi:10.1123/japa.2016-0349
9. Johnson L, Buckley JG, Scally AJ, Elliott DB. Multifocal spectacles increase variability in toe clearance and risk of tripping in the elderly. IOVS. 2007;48(4):1466. doi:10.1167/iovs.06-0586
10. Beschorner KE, Milanowski A, Tomashek D, Smith RO. Effect of multifocal lens glasses on the stepping patterns of novice wearers. Gait Posture. 2013;38(4):1015–1020. doi:10.1016/j.gaitpost.2013.05.014
11. Elliott DB, Chapman GJ. Adaptive gait changes due to spectacle magnification and dioptric blur in older people. IOVS. 2010;51(2):718. doi:10.1167/iovs.09-4250
12. Nickla DL, Wallman J. The multifunctional choroid. Prog Retin Eye Res. 2010;29(2):144–168. doi:10.1016/j.preteyeres.2009.12.002
13. Chung SE, Kang SW, Lee JH, Kim YT. Choroidal thickness in polypoidal choroidal vasculopathy and exudative age-related macular degeneration. Ophthalmology. 2011;118(5):840–845. doi:10.1016/j.ophtha.2010.09.012
14. Sanchez-Cano A, Orduna E, Segura F, et al. Choroidal thickness and volume in healthy young white adults and the relationships between them and axial length, ammetropy and sex. Am J Ophthalmol. 2014;158(3):574–583.e1. doi:10.1016/j.ajo.2014.05.035
15. Read SA, Pieterse EC, Alonso-Caneiro D, et al. Daily morning light therapy is associated with an increase in choroidal thickness in healthy young adults. Sci Rep. 2018;8(1):8200. doi:10.1038/s41598-018-26635-7
16. Liu Y, Wang L, Xu Y, Pang Z, Mu G. The influence of the choroid on the onset and development of myopia: from perspectives of choroidal thickness and blood flow. Acta ophthalmologica. 2021;99(7):730–738. doi:10.1111/aos.14773
17. Hoseini-Yazdi H, Vincent SJ, Collins MJ, Read SA. Regional alterations in human choroidal thickness in response to short-term monocular hemifield myopic defocus. OPO. 2019;39(3):172–182. doi:10.1111/opo.12609
18. Płatkowska B, Kal M, Biskup M. Optical coherence tomography angiography–use in ophthalmological practice. Medical Studies. 2020;36(3):195–205.
19. Tan CS, Ouyang Y, Ruiz H, Sadda SR. Diurnal variation of choroidal thickness in normal, healthy subjects measured by spectral domain optical coherence tomography. IOVS. 2012;53(1):261. doi:10.1167/iovs.11-8782
20. Usui S, Ikuno Y, Akiba M, et al. Circadian changes in subfoveal choroidal thickness and the relationship with circulatory factors in healthy subjects. IOVS. 2012;53(4):2300. doi:10.1167/iovs.11-8383
21. Vural AD, Kara N, Sayin N, Pirhan D, Ersan HBA. Choroidal thickness changes after a single administration of coffee in healthy subjects. Retina. 2014;34(6):1223–1228. doi:10.1097/IAE.0000000000000043
22. Althomali MM, Alharbi AA, Albnayan NM, Alkhudhair AM, Alanazi MK. Choroidal thickness measurements in young Saudi adult population: a cross-sectional study. Int J Ophthalmol. 2023;16(11):1814–1819. doi:10.18240/ijo.2023.11.12
23. Hoseini-Yazdi H, Vincent SJ, Collins MJ, Read SA, Alonso-Caneiro D. Wide-field choroidal thickness in myopes and emmetropes. Sci Rep. 2019;9(1):3474. doi:10.1038/s41598-019-39653-w
24. Alanazi M, Caroline P, Alshamrani A, Alanazi T, Liu M. Regional distribution of choroidal thickness and diurnal variation in choroidal thickness and axial length in young adults. Clin Ophthalmol. 2021;15:4573–4584. doi:10.2147/OPTH.S334619
25. Alanazi MK. Within-day changes in luminal, stromal choroidal thickness, and choroidal vascularity index in healthy adults. Indian J Ophthalmol. 2023;71(1):166–173. doi:10.4103/ijo.IJO_1268_22
26. Alonso-Caneiro D, Read SA, Collins MJ. Automatic segmentation of choroidal thickness in optical coherence tomography. Biomed Opt Express. 2013;4(12):2795. doi:10.1364/BOE.4.002795
27. Read SA, Collins MJ, Vincent SJ, Alonso-Caneiro D. Macular retinal layer thickness in childhood. Retina. 2015;35(6):1223–1233.
28. Read SA, Collins MJ, Vincent SJ, Alonso-Caneiro D. Choroidal thickness in myopic and nonmyopic children assessed with enhanced depth imaging optical coherence tomography. IOVS. 2013;54(12):7578. doi:10.1167/iovs.13-12772
29. Johansson J, Nordström A, Gustafson Y, Westling G, Nordström P. Increased postural sway during quiet stance as a risk factor for prospective falls in community-dwelling elderly individuals. Age Ageing. 2017;46(6):964–970.
30. Wood JM, Killingly C, Elliott DB, Anstey KJ, Black AA. Visual predictors of postural sway in older adults. Trans Vision Sci Technol. 2022;11(8).
31. Saftari LN, Kwon OS. Ageing vision and falls: a review. J Physiol Anthropol. 2018;37(1):11.
32. Karapetyan A, Ouyang P, Tang LS, Gemilyan M. Choroidal thickness in relation to ethnicity measured using enhanced depth imaging optical coherence tomography. Retina. 2016;36(1):82–90. doi:10.1097/IAE.0000000000000654
33. Song Y, Tham YC, Chong C, et al. Patterns and determinants of choroidal thickness in a multiethnic Asian population: the Singapore epidemiology of eye diseases study. Ophthalmol Retina. 2021;5(5):458–467. doi:10.1016/j.oret.2020.08.012
34. Aldakhil S. The effect of optical defocus on the choroidal thickness: a review. Open J Ophthalmol. 2021;15(1):283–287. doi:10.2174/1874364102115010283
35. Tan CSH, Cheong KX. Macular choroidal thicknesses in healthy adults—relationship with ocular and demographic factors. IOVS. 2014;55(10):6452. doi:10.1167/iovs.13-13771
36. Tan CSH, Cheong KX, Lim LW, Li KZ. Topographic variation of choroidal and retinal thicknesses at the macula in healthy adults. Br J Ophthalmol. 2014;98(3):339–344. doi:10.1136/bjophthalmol-2013-304000
37. Rietdyk S, Rhea CK. The effect of the visual characteristics of obstacles on risk of tripping and gait parameters during locomotion. OPO. 2011;31(3):302–310. doi:10.1111/j.1475-1313.2011.00837.x
38. Moon BY, Choi JH, Yu DS, Kim SY. Effect of induced hyperopia on fall risk and Fourier transformation of postural sway. PeerJ. 2019;7(e8329). doi:10.7717/peerj.8329
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multimorbidity Patterns and Associations with Gait, Balance and Lower Extremity Muscle Function in the Elderly: A Cross-Sectional Study in Northwest China
Yang K, Yang S, Chen Y, Cao G, Xu R, Jia X, Hou L, Li J, Bi C, Wang X
International Journal of General Medicine 2023, 16:3179-3192
Published Date: 28 July 2023