Back to Journals » Drug Design, Development and Therapy » Volume 20
Charting the Current Landscape and Future Prospects of Cancer Therapy-Related Cardiovascular Toxicity in Cancer Survivors: From Bench to Bedside
Authors Tao S ![]() , Yu L, Zhang L
, Yu L, Zhang L ![]() , Li J
, Li J ![]() , Wu J, Tan Y
, Wu J, Tan Y
Received 5 October 2025
Accepted for publication 13 February 2026
Published 3 March 2026 Volume 2026:20 572304
DOI https://doi.org/10.2147/DDDT.S572304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Leonidas D. Panos
Shiyi Tao,1 Lintong Yu,2 Lanxin Zhang,3 Jun Li,1 Ji Wu,1 Yuqing Tan1
1Department of Cardiology, Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, 100053, People’s Republic of China; 2Graduate school, Beijing University of Chinese Medicine, Beijing, 100029, People’s Republic of China; 3Department of Oncology, Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, 100053, People’s Republic of China
Correspondence: Jun Li, Email [email protected]
Abstract: Cardio-oncology represents an emerging interdisciplinary discipline focusing on optimizing oncologic efficacy while mitigating treatment-related cardiovascular complications. The advent of novel anticancer agents such as targeted therapies, immune checkpoint inhibitors, and endocrine therapies has transformed cancer care, significantly improving survival rates. Nevertheless, prolonged patient survivorship has unmasked clinically significant cardiovascular sequelae, termed cancer therapy-related cardiovascular toxicity (CTR-CVT), which manifests as acute manifestations during therapy and delayed presentations persisting years post-treatment. This dual-onset toxicity profile necessitates rigorous longitudinal cardiovascular risk stratification integrating comprehensive pre-therapeutic assessment, multi-modal imaging, and biomarker-guided surveillance to detect subclinical dysfunction, prevent premature treatment cessation, and reduce cancer recurrence and mortality risks. Future research priorities include further elucidating pathophysiological mechanisms of CTR-CVT, developing cardio-protective strategies, implementing personalized therapeutic protocols, and reducing disparities in care to advance cardio-oncology and improve patient outcomes. This review synthesizes the development of CTR-CVT, existing evidence-based CTR-CVT risk surveillance approaches, and emerging innovative early-warning strategies, and the future development prospects.
Keywords: cancer therapy-related cardiovascular toxicity, cardio-oncology, cardiotoxicity, prevention, monitoring
Introduction
Cardiovascular diseases (CVD) and cancer are the two leading chronic diseases responsible for global mortality.1 With the advancement of cancer treatment modalities, including chemotherapy, radiation therapy, targeted therapy, and immunotherapy, the survival rate of cancer patients has significantly improved.2 However, the long-term use of these therapies poses serious risks of cancer therapy-related cardiovascular toxicity (CTR-CVT), which have become a major challenge in the field of oncology.3 Cardio-oncology, an emerging interdisciplinary field combining oncology and cardiology (Figure 1), focuses on studying the cardiovascular complications caused by cancer therapies, the impact of cardiovascular diseases on cancer treatment and prognosis, and the shared pathogenic mechanisms between cancer and cardiovascular diseases.4
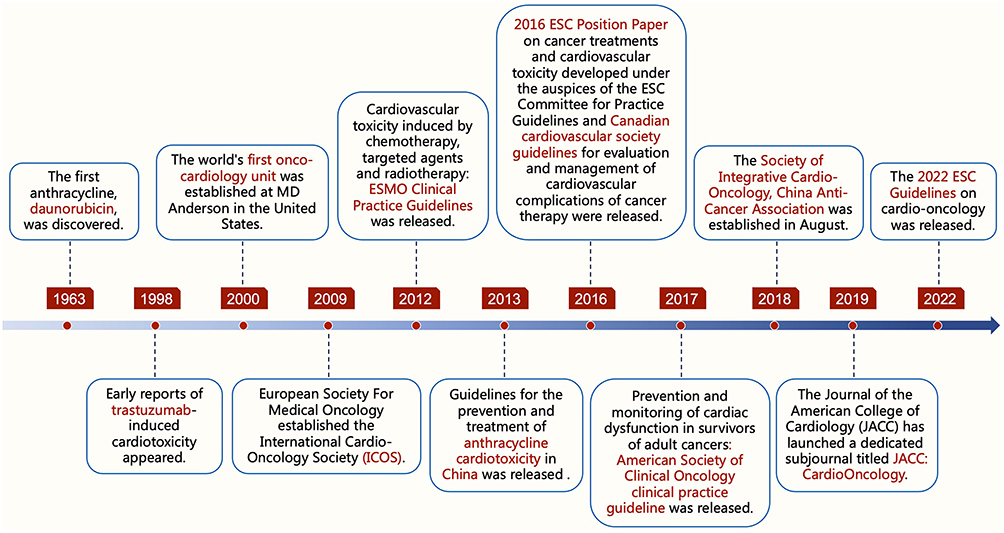 |
Figure 1 The historical development of cardio-oncology. |
CTR-CVT encompasses a spectrum of cardiovascular injuries induced by chemotherapy, radiotherapy, and targeted therapies, including coronary artery disease (CAD), cardiomyopathy, heart failure (HF), myocarditis, arrhythmias, vascular toxicities, hypertension, pericardial diseases, and valvular heart diseases (VHD), which now represent the second leading cause of morbidity and mortality among cancer survivors4 (Figure 2 and Supplementary data: Table S1). Cancer survivors face a 2- to 5-fold elevated CVD-related mortality risk relative to the general population.5 Notably, CVD constitutes the leading cause of non-oncologic mortality in this population, reducing 8-year overall survival from 81% to 60% compared to those without CVD.6 Furthermore, long-term cardiovascular complications persist across cancer survivors, including pediatric ones, with cardiotoxic manifestations frequently emerging years or even decades post-treatment.7
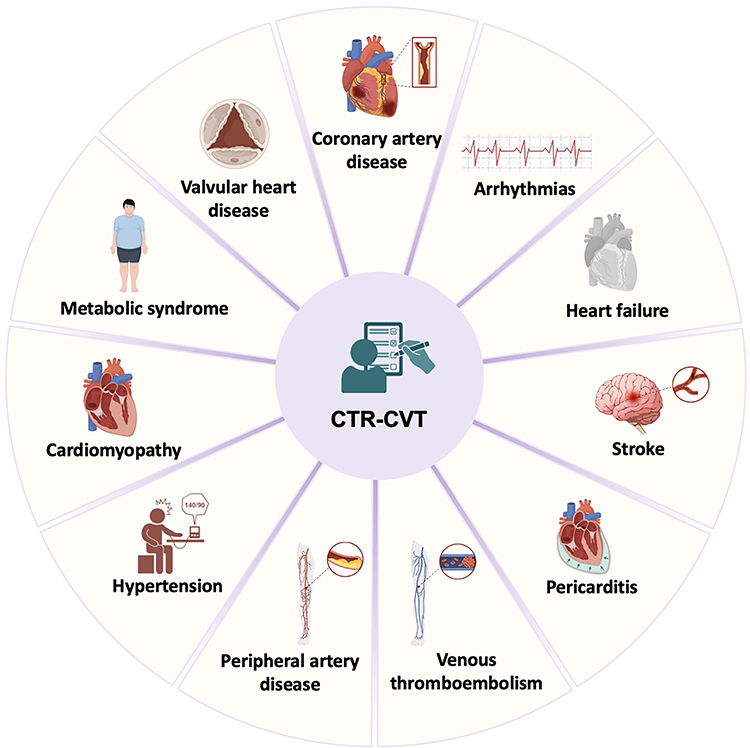 |
Figure 2 Summary of the cancer therapy-related cardiovascular diseases. Cancer therapy-related cardiovascular toxicity represents a significant clinical challenge in oncology care, encompassing a spectrum of cardiovascular pathologies including coronary artery disease, cardiomyopathy, heart failure, arrhythmias, valvular heart disease, pericarditis, peripheral artery disease, hypertension, venous thromboembolism, stroke, and metabolic syndrome. |
To address this challenge, major medical organizations have issued guidelines and consensus documents. In 2016, the European Society of Cardiology (ESC) released a position paper on cancer treatments and cardiovascular toxicity.8 The American Society of Clinical Oncology (ASCO) established clinical practice guidelines in 2017 for preventing and monitoring cardiac dysfunction in adult cancer survivors.9 A landmark milestone occurred in 2022 with the inaugural publication of the ESC Guidelines on Cardio-Oncology.4 This pivotal document marked the formal recognition of “cardio-oncology” as a distinct discipline within international cardiovascular medicine, with the term prominently featured in the title of an ESC guideline for the first time. The 2022 ESC guidelines on cardio-oncology provide detailed recommendations for monitoring, preventing, and managing cardiovascular toxicity, including multimodal and comprehensive baseline risk assessment, targeted prevention, individualized follow-up, and diagnosis and management of acute and subacute CTR-CVT.
Despite the established importance of early detection and intervention for CTR-CVT, which is facilitated by modalities such as cardiovascular imaging and biomarker detection,10,11 the field continues to face significant challenges. These include an incomplete understanding of its pathophysiological mechanisms, a lack of validated early-warning biomarkers and targeted preventive measures, and underdeveloped multidisciplinary collaboration models, all of which constrain further progress.12 Therefore, a comprehensive review of CTR-CVT and early-warning strategies is imperative, as it not only advances mechanistic understanding of cardiac toxicity pathogenesis and fosters the development of cardio-oncology but also provides evidence-based guidance for the implementation of holistic cardiovascular surveillance throughout the cancer treatment continuum, thereby enhancing patient survival rates and quality of life.13 This review aims to synthesize mechanistic insights into CTR-CVT pathogenesis and evaluate innovative early-warning strategies, including existing cardiovascular surveillance methods and artificial intelligence (AI)-enhanced early-detection system. Its significance lies in advancing cardio-oncology from reactive management to preemptive care, optimizing therapeutic decision-making through personalized risk mitigation, and ultimately improving both oncological efficacy and cardiovascular outcomes in cancer patients.
Cancer Therapy-Related Cardiovascular Toxicity
Chemotherapy‐induced Cardiotoxicity
Anthracyclines
Anthracyclines, a class of cytotoxic chemotherapeutic agents, are clinically employed in the treatment of various cancers such as breast cancer (BC), lymphomas, leukemias, and sarcomas, and are recognized as one of the most potent classes of anticancer therapeutics.4 Compounds within this class, including doxorubicin, daunorubicin, epirubicin, and idarubicin, exert their therapeutic effects through inhibiting the growth and division of tumor cells by interfering with the replication and transcription process of DNA, thus achieving antitumor effects.14 However, anthracycline therapy is associated with severe cardiotoxic effects, manifested as cardiomyopathy, HF, arrhythmias, and pericarditis, which substantially compromise cancer patient’s quality of life15 (Table 1). Anthracycline-based chemotherapeutic regimens exhibit dose-dependent cardiotoxicity, influenced by cumulative dose, age, concurrent anticancer agents, and mediastinal irradiation, with an incidence of approximately 1% for acute, ~9% for early-onset, and 0–57% for late-onset presentations.8 Long-term follow-up studies revealed that anthracycline-induced cardiac injury has surpassed tumor recurrence as the leading cause of mortality in cancer survivors.16 Notably, cardiac toxicity has been documented in up to 45.61% of pediatric patients receiving anthracycline-based chemotherapy regimens.17 Dexrazoxane and liposomal anthracyclines are currently approved in patients with high and very high CTR-CVT risk or who have already received high cumulative anthracyclines doses4 (Supplementary data: Table S2 and Table S3). Currently, approval for dexrazoxane is granted in adult patients with advanced or metastatic BC following the administration of a minimum cumulative dose of 300 mg/m2 doxorubicin or equivalent.4 Data from 2177 patients revealed that dexrazoxane lowered the risk of clinical HF and cardiac events in patients with BC undergoing anthracycline chemotherapy.18 This benefit is achieved by chelating intracellular iron to suppress oxidative stress,19 while also directly inhibiting topoisomerase IIβ to prevent DNA damage.20 Liposomal doxorubicin has been shown in a 19-trial meta-analysis to pose a lower cardiotoxic risk than the conventional form.21 Its approved uses include metastatic BC for both pegylated and non-pegylated variants, with the pegylated variant also indicated for advanced ovarian cancer, acquired immune deficiency syndrome-related Kaposi sarcoma, and multiple myeloma.4 The potential mechanisms of CTR-CVT were illustrated in Figure 3.
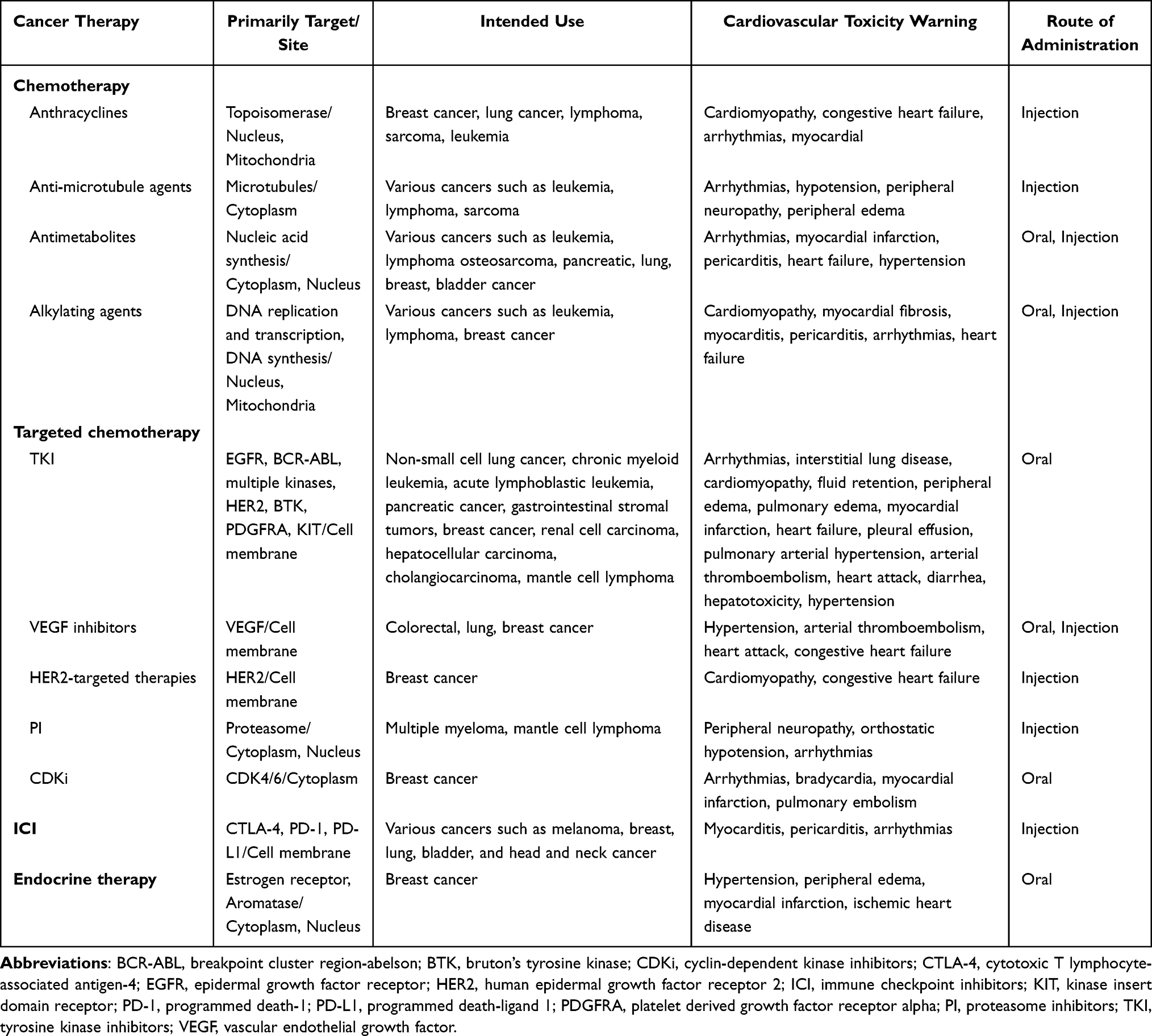 |
Table 1 Cardiovascular Toxicity Profiles of Major Cancer Therapies |
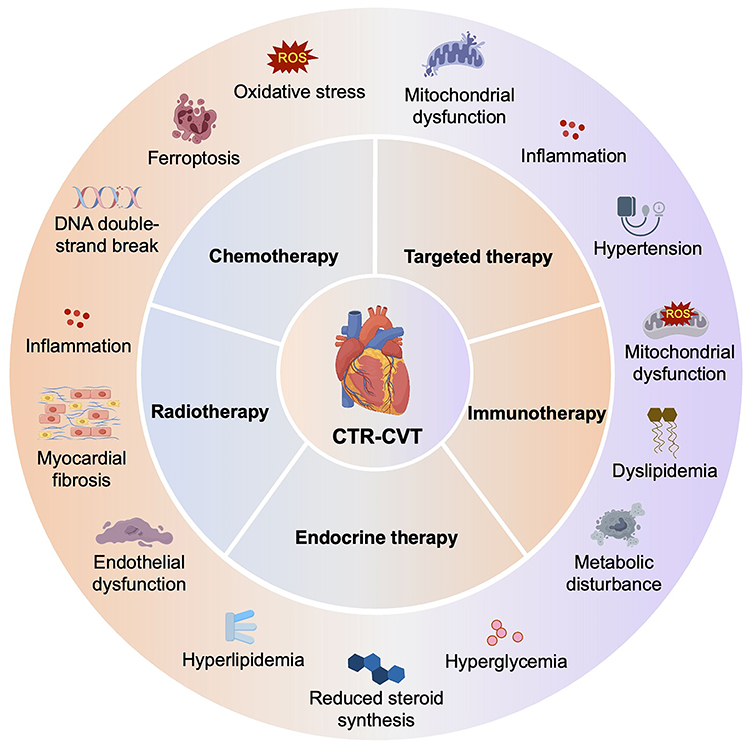 |
Figure 3 Potential mechanisms of cancer therapy-related cardiovascular toxicity. This figure delineates the possible mechanisms underlying cardiovascular toxicity across chemotherapy, targeted therapy, immunotherapy, endocrine therapy, and radiotherapy, encompassing mitochondrial dysfunction, oxidative stress, inflammation, metabolic disturbance, endothelial dysfunction, and myocardial fibrosis, highlighting their multifactorial interplay. |
Anti-Microtubule Agents
Taxanes are a class of anti-microtubule agents that impair doxorubicin clearance through pharmacokinetic interactions, leading to elevated plasma concentrations and facilitating myocardial biotransformation into cardiotoxic metabolites.22,23 Prospective longitudinal data with 30-month follow-up demonstrated that 20% of patients undergoing paclitaxel infusion developed CTR-CVT, with a median left ventricular ejection fraction (LVEF) of 48%.24 Paclitaxel demonstrates synergistic cardiotoxicity when coadministered with anthracyclines, exhibiting greater myocardial injury potential compared to docetaxel.25 Current clinical guidelines recommend sequential administration protocols prioritizing anthracycline infusion prior to paclitaxel delivery, coupled with temporal separation of cytotoxic infusions and cumulative doxorubicin dose restriction to mitigate toxicity.4 Conversely, the NSABP B-31 trial demonstrated that administering trastuzumab with paclitaxel after cyclophosphamide significantly increased incidence of CHF despite these precautions, highlighting residual risk.26 Previous reports indicated that taxanes may demonstrate a more favorable cardiac safety profile in patients with pre-existing LV dysfunction, where anthracyclines should be avoided, yet the exact cardiotoxic risks with taxanes remain incompletely characterized.27 Paclitaxel may disrupt cardiac autonomic regulation and conduction system function, predominantly manifesting as asymptomatic sinus bradycardia, while vinca alkaloid-induced cardiotoxicity is mechanistically linked to vascular endothelial dysfunction-mediated myocardial injury via impaired microvascular perfusion.28 Specifically, the cardiotoxic mechanisms of anti-microtubule agents include the induction of tubulin polymerization, inhibition of microtubule depolymerization, damage to cardiomyocytes and vascular endothelial cells, and disruption of normal cell mitosis.29 The prophylactic efficacy of renin-angiotensin-aldosterone system inhibitors and beta-blockers in anthracycline-treated patients with baseline normal cardiac function and low cardiovascular risk remains controversial, and further evidence-based studies are still needed.8
Antimetabolites
Antimetabolites, including fluoropyrimidines such as 5-fluorouracil (5-FU) and its oral prodrug capecitabine along with gemcitabine, are primarily utilized in the treatment of gastrointestinal and other malignancies. The most frequent CTR-CVT include angina pectoris, ischemia-induced electrocardiograms (ECG) abnormalities, hypertension, Takotsubo syndrome, and myocardial infarction (MI),30–32 with the rarer comprising myocarditis, arrhythmias, and peripheral arterial toxicity.33 The incidence of myocardial ischemia exhibits considerable variability, reaching up to 10%, influenced by dose-dependent, regimen-specific, and administration-route factors.34 Coronary vasospasm and endothelial injury represent primary mechanisms underlying 5-FU-induced myocardial ischemia, with chest pain and ischemic electrocardiographic alterations predominantly manifesting at rest, typically emerging within days of administration and occasionally persisting post-treatment discontinuation.35 Nevertheless, fluoropyrimidine-associated myocardial ischemia may be clinically underrecognized, with recent stress testing detecting silent ischemia in 6.9% of 5-FU-treated patients.36 A prospective study of 644 patients receiving 5-FU-based or oral capecitabine regimens confirmed that 5-FU may precipitate acute MI, necessitating heightened vigilance during fluoropyrimidine administration.37 Moreover, in alignment with ESC Guidelines for CVD prevention in clinical practice, optimization of modifiable cardiovascular risk factors is mandated throughout and post-treatment, with baseline transthoracic echocardiography (TTE) required in symptomatic CVD patients to assess pre-existing regional wall motion abnormalities or LV dysfunction.38
Alkylating Agents
Cyclophosphamide represents an antineoplastic alkylating agent and is clinically utilized in bone marrow transplantation, rheumatoid arthritis, lupus erythematosus, multiple sclerosis, neuroblastoma and other types of cancer.4 While exhibiting immunomodulatory effects at lower doses, its dose-dependent CTR-CVT predominantly manifests in patients receiving high-dose regimens (>140 mg/kg) during pre-transplant conditioning, with acute cardiotoxic manifestations emerging within days post-administration.39 The existing data indicate a 7–33% incidence of acute HF following intravenous doses exceeding 150 mg/kg, accompanied by 11–43% mortality occurring 7–21 days post-infusion.40 Moreover, alkylating agents may also induce acute and chronic pulmonary injury via DNA alkylation, oxidative and nitrosative stress, inflammation, mitochondrial dysfunction, and programmed cell death, leading to complications such as edema, fibrosis, and severe inflammation.41 Cyclophosphamide and its bioactive metabolites including acrolein, aldophosphamide, and 4-hydroxycyclophosphamide demonstrate intrinsic myocardial injury potential; of these, acrolein (an unsaturated and highly reactive aldehyde) exhibits the most pronounced cardiotoxic profile due to cardiomyocyte-selective vulnerability.42,43 Mechanistically, acrolein induces oxidative/nitrosative stress through protease adduct formation, reactive oxygen species (ROS) generation, endothelial nitric oxide synthase (eNOS) uncoupling (reduced dimer/monomer ratio), and peroxynitrite formation via nitric oxide synthase dysregulation.44,45 Other alkylating agents like cisplatin, while rarely induces direct cardiomyopathy, its nephroprotective high-volume hydration protocols may exacerbate decompensated HF in patients with preexisting cardiovascular compromise.46 Moreover, cisplatin exhibits significant vascular toxicity, inducing arterial thrombosis events through procoagulant effects and direct vascular damage, and subsequent myocardial and cerebrovascular ischemia is observed in approximately 2% of patients.47 Previous studies demonstrated that testicular cancer survivors treated with cisplatin have a higher incidence of CVD, with an absolute risk of up to 8% over 20 years.48,49
Targeted Chemotherapy‐induced Cardiotoxicity
Tyrosine Kinase Inhibitors (TKI)
Beyond conventional cytotoxic chemotherapy, molecularly targeted anticancer agents have revolutionized oncologic therapeutics through specifically targeting pathways critical for neoplastic proliferation and survival; however, while demonstrating superior selectivity and precision relative to traditional chemotherapeutic approaches, these agents are associated with cardiotoxicity.50 TKI, a class of targeted anticancer agents, competitively inhibit tyrosine kinase ATP-binding domains to attenuate neoplastic proliferation and trigger apoptosis via pro-survival pathway dysregulation, while exhibiting cardiovascular toxicities including systemic hypertension, QTc prolongation, venous thromboembolism (VTE), myocardial ischemia/infarction, and HF with reduced ejection fraction.51 A meta-analysis of 10 647 patients across 21 randomized Phase II/III trials demonstrated a significant 2.69-fold elevated risk of all-grade congestive HF (CHF) with TKI therapy versus non-TKI controls, though no significant association with severe HF incidence was observed.52 Similarly, sunitinib and nilotinib exhibit dose-dependent field potential duration prolongation, imatinib is associated with HF, whereas erlotinib demonstrates a favorable cardiac safety profile with negligible CTR-CVT.53,54
Vascular Endothelial Growth Factor (VEGF) Inhibitors
Immune-modulating and molecularly targeted therapeutics that antagonize VEGF signaling exhibit an elevated cardiovascular risk profile. As outlined in a meta-analysis, among patients on VEGF inhibitors, severe hypertension occurred in 7.4%, coronary ischemia in 1.7%, arterial thromboembolism in 1.8%, and cardiac dysfunction in 2.3% on average.55 Cabozantinib was associated with the highest number of cardiovascular events, whereas lenvatinib exhibited the strongest signal.56 The risk of developing HF during treatment with TKI inhibitors ranges from 1.5% to 4.1%, with a 5-fold increase when combined with bevacizumab.57,58 Hypertension emerges as a class-effect adverse event in VEGF inhibitor therapy, characterized by dose-dependent toxicity and risk escalation with combination therapeutic regimens.59 Studies demonstrated that VEGF inhibitor-induced vasoconstriction, a key pathogenic mechanism underlying hypertension-associated cardiotoxicity, arises potentially through reduced nitric oxide and upregulated endothelin-1 levels, driving impaired vasodilation and enhanced vasoconstriction.59 The inhibition of endothelial autocrine/paracrine VEGF signaling pathways may impair cellular viability, mediating cardiotoxic mechanisms; however, such cardiovascular adverse effects demonstrate reversibility upon therapeutic discontinuation.59,60
Human Epidermal Growth Factor Receptor 2 (HER2)-Targeted Therapies
HER2-targeted therapies, including trastuzumab, pertuzumab, trastuzumab emtansine, tucatinib, and trastuzumab deruxtecan, constitute the therapeutic cornerstone for HER2-positive invasive BC across early and metastatic disease stages, with these drugs being regulatory-approved for metastatic indications.4 Approximately 15% of BC exhibit HER2-positive status, with pathogenic HER2 overexpression recognized as a principal oncogenic driver in mammary tumorigenesis.61,62 Trastuzumab monotherapy demonstrates a clinically significant CTR-CVT risk, with cardiac dysfunction occurring in 3%-7% of patients on trastuzumab monotherapy.63 A systematic review of seven clinical trials identified trastuzumab-associated cardiotoxic events, including CHF and LVEF reduction.64 The US Food and Drug Administration (FDA) recommends a 4-week trastuzumab treatment suspension if LVEF demonstrates either a relative decline exceeding 16% from baseline or an absolute reduction ≥10%.65 As evidenced by a prior study, prophylactic beta-blocker or angiotensin-converting enzyme inhibitor initiation may mitigate trastuzumab-associated cardiotoxicity.66 Although the precise mechanisms remain incompletely characterized, preclinical evidence suggests that trastuzumab-mediated HER2 signaling inhibition in cardiomyocytes induces ROS generation, mitochondrial dysfunction, and activation of pro-apoptotic pathways, culminating in clinically evident HER2 inhibitor-induced cardiotoxicity.67,68
Proteasome Inhibitors (PI)
PI including carfilzomib, bortezomib and ixazomib, are predominantly utilized in multiple myeloma therapy, with carfilzomib demonstrating the highest incidence of cardiovascular adverse events such as hypertension, VTE, arrhythmias, LV dysfunction, and cardiomyopathy.4 A meta-analysis of 24 studies involving 2594 multiple myeloma patients identified hypertension as the most prevalent carfilzomib-associated adverse event at 12.2% incidence, followed by CHF at 4.1%.69 The ENDEAVOR trial comparing carfilzomib-dexamethasone versus bortezomib-dexamethasone in relapsed/refractory multiple myeloma demonstrated higher incidences of Grades 1–2 hypertension (16% vs 6%) and cardiac failure (Grades 1–2: 3%; Grade 3: 4% vs 1% each) in the carfilzomib arm.70 Pooled analysis of 526 patients with advanced multiple myeloma across four Phase II clinical trials demonstrated carfilzomib-associated cardiotoxicity, with arrhythmia at 13.3%, HF at 7.2%, ischemic heart disease at 3.4%, and cardiomyopathy at 1.7% incidence.71 Furthermore, clinical guidelines recommend temporary treatment discontinuation until baseline function recovery in cases of acute/chronic HF, hypertension, or LVEF reduction, as these adverse events are generally reversible upon therapy cessation and appropriate medical intervention.72 Mechanistically, proteasomes, ubiquitin-proteasome system components responsible for degrading misfolded or redundant proteins, play a critical homeostatic role in cardiomyocytes, and impairment of this proteostatic mechanism precipitates cardiac dysfunction and associated cardiovascular pathologies.73 The underlying mechanism remains incompletely elucidated but may involve PI-mediated oxidative stress within cardiomyocytes, direct proteasomal inhibition, or transient endothelial dysfunction.69,74
Cyclin-Dependent Kinase Inhibitors (CDKi)
Cyclin-dependent kinase 4/6 inhibitors (CDK4/6i), including palbociclib, ribociclib and abemaciclib, combined with endocrine therapy are approved for metastatic BC and have demonstrated improved progression-free survival with overall survival benefits in select clinical trials.4 Similarly, prior clinical trials showed that ribociclib combined with endocrine therapy significantly improved invasive disease-free survival in hormone receptor (HR)-positive/HER2-negative early-stage and advanced BC patients, with no novel toxicity signals identified during extended follow-up.75,76 However, previous studies supported that CDK4/6i, particularly ribociclib, exhibit QT interval prolongation risk, necessitating protocol-mandated electrocardiographic monitoring in Phase III clinical trials.75,77,78 Baseline electrocardiographic assessment is recommended, with serial ECG indicated at protocol-mandated intervals including day 14 of the first cycle, prior to second cycle initiation, following dose escalation, and in clinically warranted scenarios.4 Importantly, in patients with preexisting or high-risk QT prolongation, ribociclib therapy warrants multidisciplinary risk-benefit evaluation and is contraindicated with concurrent QT-prolonging agents or potent CYP3A inhibitors.4
Immune Checkpoint Inhibitors (ICI)
Immunotherapies, which augment antitumor immunity to eradicate malignant cells, comprise diverse modalities, with ICI representing the most clinically prevalent therapeutic class.79 Immune checkpoints, T cell surface proteins that modulate immune activation through ligand binding, are targeted by ICI, including cytotoxic T lymphocyte-associated antigen-4 (CTLA-4) (ipilimumab, tremelimumab), programmed death-1 (PD-1) (nivolumab, pembrolizumab, cemiplimab) and programmed death-ligand 1 (PD-L1) (atezolizumab, avelumab, durvalumab), which block checkpoint-ligand interactions to disrupt inhibitory signaling, thereby enhancing cytotoxic T cell-mediated antitumor immunity and tumor cell eradication.80 Immune-mediated cardiotoxicity may precipitate life-threatening complications including VTE, MI, cardiac dysfunction, stroke, arrhythmias, and myocarditis, often necessitating ICI discontinuation.81,82 The largest reported cohort of 122 ICI-associated myocarditis patients demonstrated early symptom onset at a median of 30 days post-ICI initiation and a mortality rate approaching 50%.83 Meta-analysis of 83,315 patients across 589 trials identified a 1.07% incidence of ICI-associated cardiotoxicities, highlighting the critical importance of early detection, ICI therapy discontinuation, immediate corticosteroid administration, and therapeutic intensification in optimizing clinical outcomes.84 Guideline-directed baseline CTR-CVT monitoring for patients receiving ICI therapy comprises ECG and troponin assay, with high-risk cohorts necessitating additional TTE evaluation.4 In addition, patients exhibiting emergent ECG abnormalities, biomarker changes, or new cardiac symptoms during therapy require immediate cardio-oncology consultation with comprehensive evaluation including TTE to quantify LVEF and global longitudinal strain.85
Endocrine Therapy
Endocrine therapy constitutes a standard therapeutic approach given that 65%-70% of early-stage and metastatic BC patients exhibit HR-positive tumor biology.86 Selective estrogen receptor modulators such as tamoxifen and toremifene, or aromatase inhibitors (AIs) including letrozole, anastrozole, and exemestane, are guideline-recommended for early-stage BC management, with therapeutic selection guided by menopausal status, comorbidities, and disease recurrence risk stratification.4 AIs combined with CDK4/6i are guideline-recommended as first- or second-line therapy for HR-positive/HER2-negative metastatic BC.4 As reported, AIs therapy is associated with elevated risks of dyslipidemia, metabolic syndrome, hypertension, HF, and MI.87 The ATAC trial demonstrated a higher cardiovascular event incidence of 2.5% in anastrozole-treated patients compared to 1.9% in tamoxifen-treated counterparts.88 Similarly, the IBIS-II trial observed a significantly higher incidence of cholesterol level elevation with anastrozole at 3% compared to tamoxifen at 1%.89 Two large meta-analyses demonstrated that extended AIs treatment duration correlated with elevated odds of CVD development in early-stage BC.90,91 Prior reports indicated that tamoxifen’s procoagulant effect aligns with the established VTE risk profile, thus contraindicating its use in thrombosis-prone patients.92,93 Toremifene and high-dose tamoxifen have demonstrated QTc interval prolongation, while no published evidence indicates CVD risk with standard-dose tamoxifen at 20 mg/day in BC patients.94 Patients should be counseled on VTE, hypercholesterolemia, and CVD risks, with acknowledgment that the absolute benefit of BC recurrence prevention generally outweighs CVD risks.87 Meanwhile, regular cardiovascular surveillance, including cholesterol level monitoring, ECG, blood pressure assessment, and vascular ultrasound evaluation, are required in patients undergoing endocrine therapy.95 Lifestyle modifications including regular physical activity and dietary optimization are recommended to mitigate obesity and hyperlipidemia, while smoking cessation is emphatically advocated to attenuate CVD risk, particularly CAD during AIs therapy and VTE in tamoxifen-treated patients.4
Radiation‐induced Cardiotoxicity
Radiotherapy, a foundational oncologic modality, utilizes high-energy radiation to target and eradicate malignant cells, frequently administered in combination with chemotherapy to optimize clinical outcomes.4 Despite the therapeutic efficacy, radiotherapy poses a significant risk of radiation-induced heart disease (RIHD), a progressive pathology with delayed manifestation characterized by a latency period extending over decades, resulting in structural cardiovascular abnormalities, conduction disturbances, and functional impairment.72 RIHD exhibits a prevalence of approximately 10% among treated patients, characterized by fibrotic and calcific involvement of the aortic root, aortic valve cusps, mitral valve annulus, and basal to mid segments of the mitral valve leaflets while sparing the distal leaflets and commissures, enabling its differentiation from rheumatic disease.96–98 A cohort study of 4414 BC survivors with a median 18-year follow-up demonstrated that combined left breast radiotherapy and cardiotoxic chemotherapy conferred the highest CTR-CVT risk, suggesting synergistic potentiation of cardiovascular toxicity.99 A case-control study of 1852 five-year Hodgkin lymphoma survivors demonstrated that cardiac valve radiation exposure correlates with a dose-dependent elevation in clinically significant VHD risk, especially exceeding thresholds of 30 Gray.100 Similarly, Hodgkin lymphoma survivors exhibit a 4- to 7-fold elevated risk of CVD compared to the general population, with cumulative CVD incidence reaching 50% at 40 years post-treatment.101 The CVD risk and associated events following chest radiotherapy are influenced by modifiable variables including anthracycline-based chemotherapy, younger age at treatment, higher radiation fractionation doses, inadequate cardiac shielding, baseline cardiovascular risk factors, and pre-existing CVD.102 Therefore, the heart is classified as a radiosensitive organ at risk during radiotherapy, necessitating rigorous minimization of cardiac dose exposure to the lowest feasible level due to the absence of a definitive threshold for radiation-induced toxicity.4 Emerging evidence identified myocardial fibrosis, endothelial dysfunction, inflammation, and vasoconstriction as key pathophysiological mechanisms driving radiotherapy-associated cardiotoxicity, with targeted modulation of these pathways offering potential to refine risk mitigation strategies and enhance clinical outcomes.103,104
Existing CTR-CVT Risk Surveillance Approaches
Serum Biomarkers
Currently, serum biomarkers such as lipids including low-density lipoprotein cholesterol and cardiac enzymes comprising cardiac troponin I (cTnI), N-terminal pro-brain natriuretic peptide (NT-proBNP), creatine kinase, and α-hydroxybutyrate dehydrogenase are commonly used for cardiovascular toxicity surveillance.105 cTnI serves as the established peripheral blood biomarker for myocardial injury, with elevated serum concentrations providing early indication of CTR-CVT. However, anthracycline administration elicits prompt cTnI elevation following initial dosing, which somewhat limits its utility in monitoring chronic cardiac dysfunction. While BNP and NT-proBNP are employed for cardiovascular risk assessment during chemotherapy, their predictive value for antineoplastic-related cardiovascular toxicity remains controversial due to susceptibility to multiple clinical variables, especially the threshold for diagnosing chemotherapy-induced cardiovascular toxicity has not been universally established.
ECG
Electrocardiography provides rapid clinical surveillance for cardiovascular toxicity, with CTR-CVT typically manifesting as nonspecific ST-segment alterations, QT-interval prolongation, T-wave abnormalities, and atrioventricular conduction disturbances. Therapeutic modification is clinically warranted only when corrected QT-interval duration exceeds 500 ms, whereas changes below 60 ms from baseline remain insignificant below this threshold.32 However, electrocardiographic assessment reflects only instantaneous cardiac status and exhibits high sensitivity but low specificity, necessitating complementary diagnostic modalities for definitive confirmation.
Cardiovascular Imaging
Cardiovascular imaging-multiple uptake gated acquisition (MUGA) and TTE represent the predominant imaging modalities using LVEF to monitor cardiac dysfunction during cancer therapy, wherein TTE offers non-invasive, radiation-free, and cost-efficient clinical accessibility for assessing LVEF and LV global longitudinal strain (GLS), while MUGA provides superior reproducibility, time efficiency, and reduced inter-individual variability, establishing it as the reference standard for LVEF quantification.106,107 Specifically, a LVEF absolute reduction exceeding 10 percentage points falling below institution-defined lower limits of normal or a GLS relative percentage decrease surpassing 15% from baseline may suggest risk of cardiotoxicity.8 Cardiac magnetic resonance imaging (CMR) demonstrates superior accuracy, precise spatial localization, and comprehensive detection capability for myocardial fibrosis, with delayed enhancement and quantitative T1 mapping serving as the reference imaging standards for fibrotic tissue characterization.108 A previous study109 indicated that the earliest doxorubicin-cardiotoxicity CMR parameter was T2 relaxation-time prolongation at week 6 in pigs and T2 mapping during treatment identifies intracardiomyocyte edema generation as the earliest marker of anthracycline-induced cardiotoxicity. Nevertheless, its implementation as routine clinical surveillance remains impractical due to limited accessibility in primary care settings, substantial cost burden, and contraindications including implanted cardiac pacemakers, ferromagnetic foreign bodies, decompensated HF, arrhythmias, and inability to tolerate supine positioning.110 Additionally, cardiac computed tomography angiography (CCTA) constitutes a widely available imaging technique for coronary anatomical and pathological evaluation, with utility in secondary prevention contexts. Given its high sensitivity in excluding CAD, CCTA is currently widely employed to rule out coronary stenosis in patients exposed to cardiotoxic anticancer therapy with newly developed reduced LVEF.111
Endomyocardial Biopsy (EMB)
EMB represents the pathohistological diagnosis method for evaluating CTR-CVT, involving transvascular catheter-based extraction of myocardial tissue for histopathological analysis, a capability unattainable by non-invasive diagnostic modalities.112 However, procedural invasiveness, requirement for substantial operator expertise, and inherent myocardial injury risks restrict its widespread clinical implementation.
Emerging Innovative Early-Warning Strategies
Testing Novel Serum Biomarkers
While existing CTR-CVT risk surveillance approaches provide partial clinical utility, their suboptimal diagnostic performance necessitates the development of precision surveillance strategies for early cardiovascular toxicity detection. Beyond the established role of cTnI and NT-proBNP in screening early cardiovascular injury, recent investigations demonstrate high-sensitivity cardiac troponin assays possess superior diagnostic sensitivity for myocardial damage.113 Additionally, emerging serum biomarkers including C-reactive protein, myeloperoxidase, galectin-3, growth differentiation factor-15, fms-like tyrosine kinase-1, cytochrome C, arginine-nitric oxide metabolites, micro-ribonucleic acids, placental growth factor, and immuno-globulin E are undergoing extensive investigation.4 Paraoxonase-1 activity may be mechanistically relevant to predicting the risk of anthracycline-induced cardiotoxicity.114 However, insufficient evidence currently exists to support routine implementation of these novel biomarkers, necessitating further investigation.
Examining Novel Hemodynamic Indicators
As stated in the 2022 ESC guidelines on cardio-oncology,4 hemodynamic monitoring is recommended for early cardiovascular toxicity surveillance in clinical cancer patients. Evidence demonstrated that non-invasive ankle-brachial index (ABI) measurement enabled early detection of nilotinib-induced progressive peripheral arterial stenosis in chronic myeloid leukemia, suggesting that routine ABI screening for diagnosing asymptomatic peripheral artery disease (PAD) may help prevent vascular adverse events.115 A systematic review and meta-analysis of 19 longitudinal and cross-sectional studies indicated that significant arterial stiffening occurred following anticancer therapy,116 and pulse wave velocity may serve as a potential approach for the early surveillance of anthracycline-induced arterial stiffening.117 Moreover, photoplethysmography is an emerging non-invasive hemodynamic monitoring technology capable of detecting arterial stiffness and endothelial dysfunction alterations to accurately evaluate cardiovascular toxicity induced by gastric cancer therapeutics.118 Thus, performing hemodynamic monitoring for cardiovascular toxicity in the early phase of antineoplastic treatment facilitates longitudinal quantification of cumulative toxicodynamic effects, precise evaluation of individual tolerance heterogeneity to therapeutic regimens, and thereby formulation of personalized intervention strategies.
Monitoring Three-Dimensional Speckle Tracking Imaging (3D-STI)
3D-STI denotes an advanced echocardiographic technique for identifying myocardial injuries at initial phases and demonstrates superior measurement reproducibility through tracking out-of-plane speckle motion.119 As multi section images within the same cardiac cycle can be obtained, evaluation time is minimized with enhanced sensitivity and detectability during early cardiotoxicity stage.120 A systematic review aggregating 22 studies involving 1991 patients demonstrated that 3D-STI may serve as a non-invasive and objective tool for assessing LV functional alterations among chemotherapy-treated cancer patients.121 In addition, 3D-STI detected initial alterations in area strain following minimal doxorubicin administration in BC patients, with early aberrations correlating to subsequent LVEF decline, demonstrating potential utility for anticipating anthracycline cardiotoxicity.122
Detecting Gene Polymorphism
Epidemiological investigations revealed substantial pharmacogenomic heterogeneity in patient tolerance to cancer therapeutic agents, wherein single-nucleotide polymorphisms in specific predisposing genetic variants closely associated with CTR-CVT.123 Candidate gene and genome-wide association studies have identified 40 candidate genes and single nucleotide polymorphisms linked to anthracycline-associated cardiac dysfunction.4 An investigation among individuals with ICI-associated myocarditis demonstrated that clonal T-cell clusters infiltrating the myocardium mirrored those detected in tumors and skeletal muscle, with RNA sequencing analyses disclosing expression of cardiac-specific genes within the tumor and proposing the compelling notion that somatic mutations intrinsic to the tumor may contribute to CTR-CVT.124 Current clinical guidelines discourage prophylactic pharmacogenetic screening for CTR-CVT risk; however, personalized genetic testing may potentially delineate oncology patients’ inherent CVD predisposition, necessitating further rigorous research.4
Developing AI-Powered CTR-CVT Risk Monitoring Methods
AI-empowered approaches encompassing machine learning (ML) and deep learning (DL) improve risk categorization, optimize therapeutic decisions, and facilitate individualized management for cancer patients with cardiovascular vulnerability.125 Within cardiac visualization methodologies, AI demonstrates enhanced capacity to substantially elevate diagnostic precision and operational efficacy.126 AI-enhanced tools have revolutionized conventional echocardiography, CMR, and positron emission tomography (PET)modalities. These technologies improve the accuracy of LVEF and GLS measurements, crucial for identifying early chemotherapy-induced myocardial injury, especially among patients treated with anthracyclines and trastuzumab.127 Integrated PET/CT systems have gained advantages through AI incorporation, allowing concurrent coronary structural evaluation and cardiac perfusion analysis.128,129 Furthermore, wearable ECG monitoring patches, biosensing devices, and AI-integrated implantable systems enable continuous cardiac surveillance and predictive modeling; these technological innovations facilitate personalized care that prioritizes cancer therapy efficacy while safeguarding long-term cardiovascular health.130,131
Challenges and Future Perspectives
This review comprehensively investigates cardiovascular toxicities associated with cancer therapies, highlighting their clinical relevance and potential screening methods for cardiotoxicity. Evidence indicates CTR-CVT represents a significant challenge in cancer patient management, encompassing CAD, cardiomyopathy, HF, arrhythmias, VHD, pericarditis, PAD, hypertension, VTE, stroke, and metabolic syndrome, which substantially affect patient prognosis and quality of life. Additionally, current CTR-CVT risk monitoring approaches and emerging innovative early detection strategies show potential for mitigating cardiovascular toxicity and enhancing patient outcomes. Despite significant advancements in this domain, several unresolved challenges persist.
Elucidation of Complex Mechanisms
The pathophysiological mechanisms underlying CTR-CVT exhibit marked complexity and variability across therapeutic modalities such as chemotherapy, targeted therapy, ICI, endocrine therapy and radiotherapy. These mechanisms manifest through diverse pathways involving mitochondrial dysfunction, oxidative stress, inflammation, metabolic disturbance, endothelial dysfunction, and myocardial fibrosis. However, current limitations stem from the absence of a cohesive mechanistic framework unifying these toxicity profiles. Future research may give priority to attempting large-scale multi-omics investigations integrating transcriptomic, metabolomic, and proteomic analyses to elucidate CTR-CVT pathogenesis and establish predictive networks.132
Current experimental modeling of CTR-CVT primarily utilizes rodent, porcine, and canine models alongside induced pluripotent stem cells (iPSCs) and other cellular platforms, with rodent models predominating due to their optimal balance of cost efficiency and biological fidelity.133 Meanwhile, the progression from 2D to 4D iPSC-based platforms has significantly enhanced the recapitulation of complex tissue and organ-level pathophysiology through improved biomimicry of in vivo microenvironments, thereby enabling high-fidelity interrogation of disease pathogenesis and therapeutic response dynamics. Future investigations integrating multi-cellular tissue models with multi-omics methodologies like sequencing may reveal the mechanisms of cardiotoxicity, thereby establishing a basis for incorporating iPSCs into preventive cardio-oncology clinical protocols. Nevertheless, developing reliable CTR-CVT models demands strategic evaluation of critical parameters. First, prioritizing model sensitivity, such as the trastuzumab’s limited murine HER2 affinity, requires myocardium-specific ErbB2-edited or iPSC-derived cardiomyocyte systems for human-relevant drug responses.134,135 Second, precise optimization of dosing regimens (route, duration) to mirror clinical cardiotoxicity, particularly anthracycline cumulative thresholds.133,136 Third, addressing interspecies biological disparities through clinical data integration to validate preclinical mechanistic insights.
Development of Personalized Risk Assessment Tools
Prior to initiating cancer therapy, a comprehensive cardiovascular evaluation should be conducted to assess the patient’s baseline cardiovascular health (Figure 4). Personalized risk assessment tools exhibit substantial promise for early detection, risk stratification, and treatment strategy of CTR-CVT. However, conventional serum biomarkers and cardiovascular imaging modalities frequently exhibit suboptimal diagnostic performance in isolation due to intrinsic limitations in capturing the pathophysiological complexity of CTR-CVT, where interindividual metabolic variability and preexisting comorbidities compromise detection accuracy, resulting in diagnostic misclassification and delayed clinical intervention. Therefore, advancing high-fidelity multiplexed biomarker signatures constitutes a critical priority, with contemporary strategies emphasizing multimodal convergence through synthesis of serum biomarkers, cardiovascular imaging, genetic screening, and electronic health records to establish holistic risk stratification profiles. Longitudinal surveillance during therapeutic intervention, integrating individualized variables including genomic susceptibility and pharmacotherapeutic protocols, optimizes prognostic precision. AI-driven analytics of patient-specific multimodal data facilitate precision risk stratification through preclinical identification of individualized risk stratification parameters, thereby enhancing the diagnostic accuracy and predictive performance of tailored risk assessment frameworks for early intervention, therapeutic surveillance, and cardiovascular outcome optimization in CTR-CVT management.137
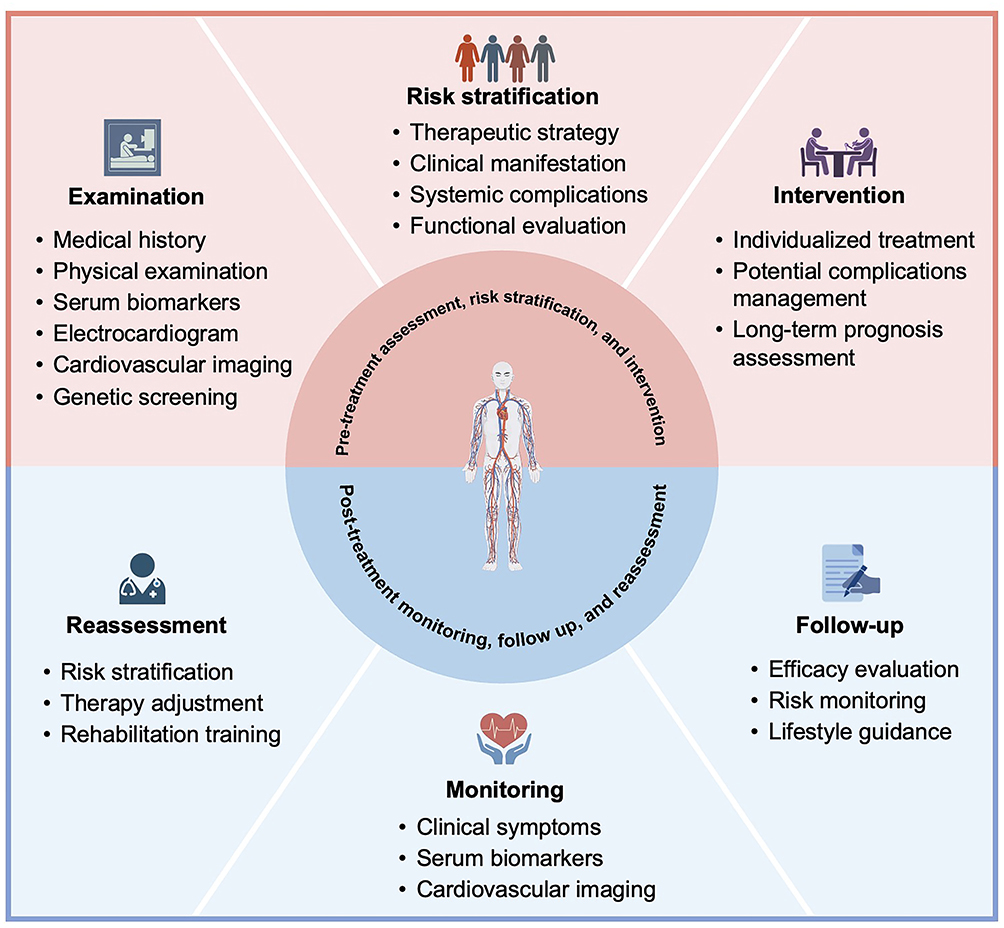 |
Figure 4 Comprehensive management of patients pre- and post-cancer therapy. Multidisciplinary risk stratification necessitates baseline cardiovascular risk profiling integrating clinical parameters, personalized treatment informed by pre-therapeutic assessment, and longitudinal surveillance with tailored rehabilitation protocols to mitigate cardiotoxicity and optimize post-cancer therapy outcomes. |
Optimization of Treatment Strategies
A primary challenge in managing CTR-CVT lies in achieving an optimal balance between oncologic efficacy and cardiovascular protection. This complexity arises from the inherent tension wherein specific interventions aimed at mitigating cardiovascular risk may inadvertently compromise cytotoxic therapeutic efficacy or disrupt systemic homeostasis. In this context, the principle of permissive cardiotoxicity has been proposed as a critical temporizing strategy, which centers on maintaining essential anticancer therapy concurrent with optimized cardiovascular management to mitigate toxicity and improve prognosis, rather than mandating treatment cessation.138 Furthermore, the pronounced heterogeneity of CTR-CVT, influenced by genetic predispositions, specific malignancy subtypes, diverse therapeutic protocols, and pre-existing metabolic conditions, complicates standardized management. While precision oncology frameworks offer a promising avenue for individualized strategies, their translation faces significant barriers, including the development of regimens tailored to dynamic metabolic profiles and therapeutic thresholds, as well as reconciling clinical efficacy with economic feasibility.3 Therefore, effective management must begin with comprehensive pre-treatment cardiovascular risk stratification, which includes thorough assessment and optimized management of modifiable factors such as hypertension, smoking, and diabetes.4 Ultimately, overcoming these challenges requires advancing mechanistic studies and establishing standardized, individualized management protocols in CTR-CVT contexts.
Improvement of Long-Term CTR-CVT Monitoring and Management
CTR-CVT exhibit latent and long-term pathological consequences that clinically manifest years to decades post-therapeutic intervention, elevating morbidity and mortality risks among survivors and highlighting the need for lifelong cardiovascular toxicity monitoring protocols. Contemporary clinical research predominantly prioritizes acute cardiovascular events during therapeutic phases, whereas comprehensive evaluations of delayed cardiovascular sequelae including metabolic disturbance, atherosclerosis, and persistent cardiac dysfunction remain understudied, hindering the development of predictive methods and targeted interventions for longitudinal cardiovascular risk mitigation. Subsequent studies should emphasize long-term follow-up studies to assess the effects of oncological interventions on cardiac well-being. Moreover, AI-powered prognostic algorithms integrating clinical data and individualized characteristics will facilitate precision risk quantification. Deployment through multinational databases and cross-specialty partnerships will refine therapeutic precision while safeguarding cardiac integrity, advancing survival metrics. Strengthened transdisciplinary integration and personalized health trajectories will optimize long-term outcomes, embedding cardiovascular preservation within oncological management.139 These approaches prove indispensable for delineating persistent sequelae of CTR-CVT and formulating targeted countermeasures for long-term risk reduction.
Conclusion
Emerging data strongly demonstrate a potential association between oncologic interventions and heightened susceptibility to CVD progression and treatment-related cardiotoxicity in cancer survivors. Clinical vigilance regarding CTR-CVT remains imperative within oncology survivorship cohorts. Research imperatives include elucidating the pathophysiological foundations of CTR-CVT in post-therapeutic cohorts and refining therapeutic efficacy. Implementation of individualized risk stratification strategies and sustained longitudinal surveillance protocols enables progression toward precision cardio-oncology and clinical outcome optimization. Collectively, investigations into CTR-CVT among cancer survivors confronts substantial challenges alongside promising prospects.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the High Level Chinese Medical Hospital Promotion Project (No. HLCMHPP2023065), the National Natural Science Foundation of China (No. 82474494), and the National Key Research and Development Program of China (No. 2022YFC3500102).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Collaborators GBDF. Burden of disease scenarios for 204 countries and territories, 2022-2050: a forecasting analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2204–19.
2. Balough E, Ariza A, Asnani A, Hoeger CW. Cardiotoxicity of Anthracyclines. Cardiol Clin. 2025;43(1):111–127. doi:10.1016/j.ccl.2024.08.002
3. Beavers CJ, Rodgers JE, Bagnola AJ, et al. Cardio-oncology drug interactions: a scientific statement from the American Heart Association. Circulation. 2022;145(15):e811–e38. doi:10.1161/CIR.0000000000001056
4. Lyon AR, Lopez-Fernandez T, Couch LS, et al. ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022;43(41):4229–4361. doi:10.1093/eurheartj/ehac244
5. Blaes A, Nohria A, Armenian S, et al. Cardiovascular considerations after cancer therapy: gaps in evidence and JACC: cardiooncology expert panel recommendations. JACC CardioOncol. 2025;7(1):1–19. doi:10.1016/j.jaccao.2024.06.006
6. Naaktgeboren WR, Linschoten M, de Graeff A, et al. Long-term cardiovascular health in adult cancer survivors. Maturitas. 2017;105:37–45. doi:10.1016/j.maturitas.2017.05.014
7. Ryan TD, Bates JE, Kinahan KE, et al. Cardiovascular toxicity in patients treated for childhood cancer: a scientific statement from the American Heart Association. Circulation. 2025;151(15):e926–e43. doi:10.1161/CIR.0000000000001308
8. Zamorano JL, Lancellotti P, Rodriguez Munoz D, et al. ESC position paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC committee for practice guidelines: the task force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(36):2768–2801. doi:10.1093/eurheartj/ehw211
9. Armenian SH, Lacchetti C, Barac A, et al. Prevention and monitoring of cardiac dysfunction in survivors of adult cancers: american society of clinical oncology clinical practice guideline. J Clin Oncol. 2017;35(8):893–911. doi:10.1200/JCO.2016.70.5400
10. Addison D, Neilan TG, Barac A, et al. Cardiovascular imaging in contemporary cardio-oncology: a scientific statement from the American Heart Association. Circulation. 2023;148(16):1271–1286. doi:10.1161/CIR.0000000000001174
11. Zaha VG, Hayek SS, Alexander KM, et al. Future perspectives of cardiovascular biomarker utilization in cancer survivors: a scientific statement from the American Heart Association. Circulation. 2021;144(25):e551–e63. doi:10.1161/CIR.0000000000001032
12. Sverdlov AL, Koczwara B, Cehic DA, et al. When cancer and cardiovascular disease intersect: the challenge and the opportunity of cardio-oncology. Heart Lung Circ. 2024;33(5):558–563. doi:10.1016/j.hlc.2023.04.301
13. Vinas-Mendieta AE, Gallardo-Grajeda A, Lopez-Fernandez T. Cardio-oncology: chances and challenges. Basic Res Cardiol. 2025;120(1):3–9. doi:10.1007/s00395-024-01080-y
14. Rawat PS, Jaiswal A, Khurana A, Bhatti JS, Navik U. Doxorubicin-induced cardiotoxicity: an update on the molecular mechanism and novel therapeutic strategies for effective management. Biomed Pharmacother. 2021;139:111708. doi:10.1016/j.biopha.2021.111708
15. Camilli M, Cipolla CM, Dent S, Minotti G, Cardinale DM. Anthracycline cardiotoxicity in adult cancer patients: JACC: cardiooncology state-of-the-art review. JACC CardioOncol. 2024;6(5):655–677. doi:10.1016/j.jaccao.2024.07.016
16. Curigliano G, Cardinale D, Dent S, et al. Cardiotoxicity of anticancer treatments: epidemiology, detection, and management. CA Cancer J Clin. 2016;66(4):309–325. doi:10.3322/caac.21341
17. Yu H, Qiu Y, Yu H, et al. Anthracycline induced cardiac disorders in childhood acute lymphoblastic leukemia: a single-centre, retrospective, observational study. Front Pharmacol. 2021;12:598708. doi:10.3389/fphar.2021.598708
18. Macedo AVS, Hajjar LA, Lyon AR, et al. Efficacy of dexrazoxane in preventing anthracycline cardiotoxicity in breast cancer. JACC CardioOncol. 2019;1(1):68–79. doi:10.1016/j.jaccao.2019.08.003
19. Kwok JC, Richardson DR. The cardioprotective effect of the iron chelator dexrazoxane (ICRF-187) on anthracycline-mediated cardiotoxicity. Redox Rep. 2000;5(6):317–324. doi:10.1179/135100000101535898
20. Lyu YL, Kerrigan JE, Lin CP, et al. Topoisomerase IIbeta mediated DNA double-strand breaks: implications in doxorubicin cardiotoxicity and prevention by dexrazoxane. Cancer Res. 2007;67(18):8839–8846. doi:10.1158/0008-5472.CAN-07-1649
21. Yamaguchi N, Fujii T, Aoi S, Kozuch PS, Hortobagyi GN, Blum RH. Comparison of cardiac events associated with liposomal doxorubicin, epirubicin and doxorubicin in breast cancer: a Bayesian network meta-analysis. Eur J Cancer. 2015;51(16):2314–2320. doi:10.1016/j.ejca.2015.07.031
22. Holmes FA, Rowinsky EK. Pharmacokinetic profiles of doxorubicin in combination with taxanes. Semin Oncol. 2001;28(4 Suppl 12):8–14. doi:10.1053/sonc.2001.26435
23. Salvatorelli E, Menna P, Cascegna S, et al. Paclitaxel and docetaxel stimulation of doxorubicinol formation in the human heart: implications for cardiotoxicity of doxorubicin-taxane chemotherapies. J Pharmacol Exp Ther. 2006;318(1):424–433. doi:10.1124/jpet.106.103846
24. Osman M, Elkady M. A prospective study to evaluate the effect of paclitaxel on cardiac ejection fraction. Breast Care. 2017;12(4):255–259. doi:10.1159/000471759
25. Floyd JD, Nguyen DT, Lobins RL, Bashir Q, Doll DC, Perry MC. Cardiotoxicity of cancer therapy. J Clin Oncol. 2005;23(30):7685–7696. doi:10.1200/JCO.2005.08.789
26. Tan-Chiu E, Yothers G, Romond E, et al. Assessment of cardiac dysfunction in a randomized trial comparing doxorubicin and cyclophosphamide followed by paclitaxel, with or without trastuzumab as adjuvant therapy in node-positive, human epidermal growth factor receptor 2-overexpressing breast cancer: NSABP B-31. J Clin Oncol. 2005;23(31):7811–7819. doi:10.1200/JCO.2005.02.4091
27. Gollerkeri A, Harrold L, Rose M, Jain D, Burtness BA. Use of paclitaxel in patients with pre-existing cardiomyopathy: a review of our experience. Int, J, Cancer. 2001;93(1):139–141. doi:10.1002/ijc.1295
28. Joshi AM, Prousi GS, Bianco C, et al. Microtubule Inhibitors and Cardiotoxicity. Curr Oncol Rep. 2021;23(3):30. doi:10.1007/s11912-021-01014-0
29. Meijers WC, Aboumsallem JP, Lyon AR, Moslehi J, de Boer RA. Forward and reverse cardio-oncology. Physiol Rev. 2026;106(1):587–644.
30. Zamorano JL, Gottfridsson C, Asteggiano R, et al. The cancer patient and cardiology. Eur J Heart Fail. 2020;22(12):2290–2309. doi:10.1002/ejhf.1985
31. Herrmann J. Vascular toxic effects of cancer therapies. Nat Rev Cardiol. 2020;17(8):503–522.
32. Herrmann J, Lenihan D, Armenian S, et al. Defining cardiovascular toxicities of cancer therapies: an International Cardio-Oncology Society (IC-OS) consensus statement. Eur Heart J. 2022;43(4):280–299.
33. Padegimas A, Carver JR. How to diagnose and manage patients with fluoropyrimidine-induced chest pain: a single center approach. JACC CardioOncol. 2020;2(4):650–654. doi:10.1016/j.jaccao.2020.06.012
34. Frickhofen N, Beck FJ, Jung B, Fuhr HG, Andrasch H, Sigmund M. Capecitabine can induce acute coronary syndrome similar to 5-fluorouracil. Ann Oncol. 2002;13(5):797–801. doi:10.1093/annonc/mdf035
35. Polk A, Vistisen K, Vaage-Nilsen M, Nielsen DL. A systematic review of the pathophysiology of 5-fluorouracil-induced cardiotoxicity. BMC Pharmacol Toxicol. 2014;15:47. doi:10.1186/2050-6511-15-47
36. Lestuzzi C, Vaccher E, Talamini R, et al. Effort myocardial ischemia during chemotherapy with 5-fluorouracil: an underestimated risk. Ann Oncol. 2014;25(5):1059–1064.
37. Kosmas C, Kallistratos MS, Kopterides P, et al. Cardiotoxicity of fluoropyrimidines in different schedules of administration: a prospective study. J Cancer Res Clin Oncol. 2008;134(1):75–82. doi:10.1007/s00432-007-0250-9
38. Visseren FLJ, Mach F, Smulders YM, et al. ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42(34):3227–3337. doi:10.1093/eurheartj/ehab484
39. Oliveira GH, Al-Kindi SG, Guha A, et al. Cardiovascular risk assessment and management of patients undergoing hematopoietic cell transplantation. Bone Marrow Transplant. 2021;56(3):544–551. doi:10.1038/s41409-020-01080-1
40. Iqubal A, MK I, Sharma S, et al. Molecular mechanism involved in cyclophosphamide-induced cardiotoxicity: old drug with a new vision. Life Sci. 2019;218:112–131. doi:10.1016/j.lfs.2018.12.018
41. Sola E, Morales-Garcia JA, Lopez-Munoz F, Ramos E, Romero A. In vivo evidence of melatonin’s protective role in alkylating-agent-induced pulmonary toxicity: a systematic review. Antioxidants. 2025;14(6):712. doi:10.3390/antiox14060712
42. Kurauchi K, Nishikawa T, Miyahara E, Okamoto Y, Kawano Y. Role of metabolites of cyclophosphamide in cardiotoxicity. BMC Res Notes. 2017;10(1):406. doi:10.1186/s13104-017-2726-2
43. Henning RJ, Johnson GT, Coyle JP, Harbison RD. Acrolein can cause cardiovascular disease: a review. Cardiovasc Toxicol. 2017;17(3):227–236. doi:10.1007/s12012-016-9396-5
44. Maeshima T, Honda K, Chikazawa M, et al. Quantitative analysis of acrolein-specific adducts generated during lipid peroxidation-modification of proteins in vitro: identification of N(tau)-(3-propanal)histidine as the major adduct. Chem Res Toxicol. 2012;25(7):1384–1392.
45. Yousefipour Z, Ranganna K, Newaz MA, Milton SG. Mechanism of acrolein-induced vascular toxicity. J Physiol Pharmacol. 2005;56(3):337–353.
46. Herrmann J. Cardiovascular toxicity with cisplatin in patients with testicular cancer: looking for something heavier than heavy metal. JACC CardioOncol. 2020;2(3):456–459. doi:10.1016/j.jaccao.2020.07.007
47. Moore RA, Adel N, Riedel E, et al. High incidence of thromboembolic events in patients treated with cisplatin-based chemotherapy: a large retrospective analysis. J Clin Oncol. 2011;29(25):3466–3473. doi:10.1200/JCO.2011.35.5669
48. Huddart RA, Norman A, Shahidi M, et al. Cardiovascular disease as a long-term complication of treatment for testicular cancer. J Clin Oncol. 2003;21(8):1513–1523. doi:10.1200/JCO.2003.04.173
49. Haugnes HS, Wethal T, Aass N, et al. Cardiovascular risk factors and morbidity in long-term survivors of testicular cancer: a 20-year follow-up study. J Clin Oncol. 2010;28(30):4649–4657. doi:10.1200/JCO.2010.29.9362
50. Ekram J, Rathore A, Avila C, Hussein R, Alomar M. Unveiling the cardiotoxicity conundrum: navigating the seas of tyrosine kinase inhibitor therapies. Cancer Control. 2024;31:10732748241285755. doi:10.1177/10732748241285755
51. Sayegh N, Yirerong J, Agarwal N, et al. Cardiovascular toxicities associated with tyrosine kinase inhibitors. Curr Cardiol Rep. 2023;25(4):269–280. doi:10.1007/s11886-023-01845-2
52. Ghatalia P, Morgan CJ, Je Y, et al. Congestive heart failure with vascular endothelial growth factor receptor tyrosine kinase inhibitors. Crit Rev Oncol Hematol. 2015;94(2):228–237. doi:10.1016/j.critrevonc.2014.12.008
53. Altrocchi C, Van Ammel K, Steemans M, et al. Evaluation of chronic drug-induced electrophysiological and cytotoxic effects using human-induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs). Front Pharmacol. 2023;14:1229960. doi:10.3389/fphar.2023.1229960
54. Trent JC, Patel SS, Zhang J, et al. Rare incidence of congestive heart failure in gastrointestinal stromal tumor and other sarcoma patients receiving imatinib mesylate. Cancer. 2010;116(1):184–192. doi:10.1002/cncr.24683
55. Abdel-Qadir H, Ethier JL, Lee DS, Thavendiranathan P, Amir E. Cardiovascular toxicity of angiogenesis inhibitors in treatment of malignancy: a systematic review and meta-analysis. Cancer Treat Rev. 2017;53:120–127. doi:10.1016/j.ctrv.2016.12.002
56. Zhang Y, Deng J, Wang J. Cardiovascular toxicities associated with vascular endothelial growth factor receptor tyrosine kinase inhibitors: a pharmacovigilance study based on FDA adverse event reporting system. Int J Clin Pharm. 2025;47(5):1467–1474. doi:10.1007/s11096-025-01962-8
57. Richards CJ, Je Y, Schutz FA, et al. Incidence and risk of congestive heart failure in patients with renal and nonrenal cell carcinoma treated with sunitinib. J Clin Oncol. 2011;29(25):3450–3456. doi:10.1200/JCO.2010.34.4309
58. Choueiri TK, Mayer EL, Je Y, et al. Congestive heart failure risk in patients with breast cancer treated with bevacizumab. J Clin Oncol. 2011;29(6):632–638. doi:10.1200/JCO.2010.31.9129
59. Touyz RM, Lang NN, Herrmann J, van den Meiracker AH, Danser AHJ. Recent advances in hypertension and cardiovascular toxicities with vascular endothelial growth factor inhibition. Hypertension. 2017;70(2):220–226. doi:10.1161/HYPERTENSIONAHA.117.08856
60. Touyz RM, Herrmann J. Cardiotoxicity with vascular endothelial growth factor inhibitor therapy. NPJ Precis Oncol. 2018;2:13. doi:10.1038/s41698-018-0056-z
61. Howlader N, Altekruse SF, Li CI, et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst. 2014;106(5). doi:10.1093/jnci/dju055.
62. Vogel CL, Cobleigh MA, Tripathy D, et al. Efficacy and safety of trastuzumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J Clin Oncol. 2023;41(9):1638–1645. doi:10.1200/JCO.22.02516
63. Telli ML, Hunt SA, Carlson RW, Guardino AE. Trastuzumab-related cardiotoxicity: calling into question the concept of reversibility. J Clin Oncol. 2007;25(23):3525–3533. doi:10.1200/JCO.2007.11.0106
64. Balduzzi S, Mantarro S, Guarneri V, et al. Trastuzumab-containing regimens for metastatic breast cancer. Cochrane Database Syst Rev. 2014;2014(6):CD006242. doi:10.1002/14651858.CD006242.pub2
65. Hamo CE, Bloom MW, Cardinale D, et al. Cancer therapy-related cardiac dysfunction and heart failure: part 2: prevention, treatment, guidelines, and future directions. Circ Heart Fail. 2016;9(2):e002843. doi:10.1161/CIRCHEARTFAILURE.115.002843
66. Guglin M, Krischer J, Tamura R, et al. Randomized trial of lisinopril versus carvedilol to prevent trastuzumab cardiotoxicity in patients with breast cancer. J Am Coll Cardiol. 2019;73(22):2859–2868. doi:10.1016/j.jacc.2019.03.495
67. Nemeth BT, Varga ZV, Wu WJ, Pacher P. Trastuzumab cardiotoxicity: from clinical trials to experimental studies. Br J Pharmacol. 2017;174(21):3727–3748. doi:10.1111/bph.13643
68. Leemasawat K, Phrommintikul A, Chattipakorn SC, Chattipakorn N. Mechanisms and potential interventions associated with the cardiotoxicity of ErbB2-targeted drugs: insights from in vitro, in vivo, and clinical studies in breast cancer patients. Cell Mol Life Sci. 2020;77(8):1571–1589. doi:10.1007/s00018-019-03340-w
69. Waxman AJ, Clasen S, Hwang WT, et al. Carfilzomib-associated cardiovascular adverse events: a systematic review and meta-analysis. JAMA Oncol. 2018;4(3):e174519. doi:10.1001/jamaoncol.2017.4519
70. Dimopoulos MA, Moreau P, Palumbo A, et al. Carfilzomib and dexamethasone versus bortezomib and dexamethasone for patients with relapsed or refractory multiple myeloma (ENDEAVOR): a randomised, Phase 3, open-label, multicentre study. Lancet Oncol. 2016;17(1):27–38. doi:10.1016/S1470-2045(15)00464-7
71. Siegel D, Martin T, Nooka A, et al. Integrated safety profile of single-agent carfilzomib: experience from 526 patients enrolled in 4 phase II clinical studies. Haematologica. 2013;98(11):1753–1761. doi:10.3324/haematol.2013.089334
72. Chang HM, Moudgil R, Scarabelli T, Okwuosa TM, Yeh ETH. Cardiovascular complications of cancer therapy: best practices in diagnosis, prevention, and management: part 1. J Am Coll Cardiol. 2017;70(20):2536–2551. doi:10.1016/j.jacc.2017.09.1096
73. Schrader J, Henneberg F, Mata RA, et al. The inhibition mechanism of human 20S proteasomes enables next-generation inhibitor design. Science. 2016;353(6299):5948. doi:10.1126/science.aaf8993
74. Gavazzoni M, Lombardi CM, Vizzardi E, et al. Irreversible proteasome inhibition with carfilzomib as first line therapy in patients with newly diagnosed multiple myeloma: early in vivo cardiovascular effects. Eur J Pharmacol. 2018;838:85–90. doi:10.1016/j.ejphar.2018.09.014
75. Im SA, Lu YS, Bardia A, et al. Overall survival with ribociclib plus endocrine therapy in breast cancer. N Engl J Med. 2019;381(4):307–316. doi:10.1056/NEJMoa1903765
76. Slamon D, Lipatov O, Nowecki Z, et al. Ribociclib plus endocrine therapy in early breast cancer. N Engl J Med. 2024;390(12):1080–1091. doi:10.1056/NEJMoa2305488
77. Slamon DJ, Neven P, Chia S, et al. Phase III randomized study of ribociclib and fulvestrant in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: MONALEESA-3. J Clin Oncol. 2018;36(24):2465–2472. doi:10.1200/JCO.2018.78.9909
78. Slamon DJ, Neven P, Chia S, et al. Overall survival with ribociclib plus fulvestrant in advanced breast cancer. N Engl J Med. 2020;382(6):514–524. doi:10.1056/NEJMoa1911149
79. Hu JR, Florido R, Lipson EJ, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors. Cardiovasc Res. 2019;115(5):854–868. doi:10.1093/cvr/cvz026
80. Zhang L, Reynolds KL, Lyon AR, Palaskas N, Neilan TG. The evolving immunotherapy landscape and the epidemiology, diagnosis, and management of cardiotoxicity: JACC: cardiooncology primer. JACC CardioOncol. 2021;3(1):35–47. doi:10.1016/j.jaccao.2020.11.012
81. Kondapalli L, Hsia J, Miller R, Flaig TW, Bonaca MP. Burden of cardiovascular disease in immune checkpoint inhibitor-treated patients: reconciling adjudicated and coded outcomes. JACC CardioOncol. 2022;4(5):649–656. doi:10.1016/j.jaccao.2022.09.003
82. O IBZ, MJ O, Nohria A. Immune checkpoint inhibitor-related myocarditis with or without concomitant myopathy: clinical findings and cardiovascular outcomes. JACC CardioOncol. 2025;7(3):252–264. doi:10.1016/j.jaccao.2025.02.005
83. Salem JE, Manouchehri A, Moey M, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study. Lancet Oncol. 2018;19(12):1579–1589. doi:10.1016/S1470-2045(18)30608-9
84. Nielsen DL, Juhl CB, Nielsen OH, Chen IM, Herrmann J. Immune checkpoint inhibitor-induced cardiotoxicity: a systematic review and meta-analysis. JAMA Oncol. 2024;10(10):1390–1399. doi:10.1001/jamaoncol.2024.3065
85. Awadalla M, Mahmood SS, Groarke JD, et al. Global longitudinal strain and cardiac events in patients with immune checkpoint inhibitor-related myocarditis. J Am Coll Cardiol. 2020;75(5):467–478. doi:10.1016/j.jacc.2019.11.049
86. Curigliano G, Lenihan D, Fradley M, et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann Oncol. 2020;31(2):171–190. doi:10.1016/j.annonc.2019.10.023
87. Okwuosa TM, Morgans A, Rhee JW, et al. Impact of hormonal therapies for treatment of hormone-dependent cancers (breast and prostate) on the cardiovascular system: effects and modifications: a scientific statement from the american heart association. Circ Genom Precis Med. 2021;14(3):e000082. doi:10.1161/HCG.0000000000000082
88. Baum M, Budzar AU, Cuzick J, et al. Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomised trial. Lancet. 2002;359(9324):2131–2139.
89. Forbes JF, Sestak I, Howell A, et al. Anastrozole versus tamoxifen for the prevention of locoregional and contralateral breast cancer in postmenopausal women with locally excised ductal carcinoma in situ (IBIS-II DCIS): a double-blind, randomised controlled trial. Lancet. 2016;387(10021):866–873. doi:10.1016/S0140-6736(15)01129-0
90. Amir E, Seruga B, Niraula S, Carlsson L, Ocana A. Toxicity of adjuvant endocrine therapy in postmenopausal breast cancer patients: a systematic review and meta-analysis. J Natl Cancer Inst. 2011;103(17):1299–1309. doi:10.1093/jnci/djr242
91. Goldvaser H, Barnes TA, Seruga B, et al. Toxicity of extended adjuvant therapy with aromatase inhibitors in early breast cancer: a systematic review and meta-analysis. J Natl Cancer Inst. 2018;110(1):31–39. doi:10.1093/jnci/djx141
92. Breast International Group. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med. 2005;353(26):2747–2757. doi:10.1056/NEJMoa052258
93. Blondon M, Bodmer A, Thouvenin L, et al. Differential impact of tamoxifen and aromatase inhibitors on thrombin generation: the prospective HEMOBREAST cohort. Blood Adv. 2022;6(9):2884–2892. doi:10.1182/bloodadvances.2021006623
94. Barber M, Nguyen LS, Wassermann J, Spano JP, Funck-Brentano C, Salem JE. Cardiac arrhythmia considerations of hormone cancer therapies. Cardiovasc Res. 2019;115(5):878–894. doi:10.1093/cvr/cvz020
95. Curigliano G, De Azambuja E, Lenihan D, Calabro MG, Cardinale D, Prevention CCM. Monitoring, and management of cardiac dysfunction in patients with metastatic breast cancer. Oncologist. 2019;24(11):e1034–e43. doi:10.1634/theoncologist.2018-0773
96. Hering D, Faber L, Horstkotte D. Echocardiographic features of radiation-associated valvular disease. Am J Cardiol. 2003;92(2):226–230. doi:10.1016/S0002-9149(03)00546-0
97. Hull MC, Morris CG, Pepine CJ, Mendenhall NP. Valvular dysfunction and carotid, subclavian, and coronary artery disease in survivors of hodgkin lymphoma treated with radiation therapy. JAMA. 2003;290(21):2831–2837. doi:10.1001/jama.290.21.2831
98. Malanca M, Cimadevilla C, Brochet E, Iung B, Vahanian A, Messika-Zeitoun D. Radiotherapy-induced mitral stenosis: a three-dimensional perspective. J Am Soc Echocardiogr. 2010;23(1):108e1–2. doi:10.1016/j.echo.2009.08.006
99. Hooning MJ, Botma A, Aleman BM, et al. Long-term risk of cardiovascular disease in 10-year survivors of breast cancer. J Natl Cancer Inst. 2007;99(5):365–375. doi:10.1093/jnci/djk064
100. Cutter DJ, Schaapveld M, Darby SC, et al. Risk of valvular heart disease after treatment for Hodgkin lymphoma. J Natl Cancer Inst. 2015;107(4). doi:10.1093/jnci/djv008.
101. van Nimwegen FA, Schaapveld M, Janus CP, et al. Cardiovascular disease after Hodgkin lymphoma treatment: 40-year disease risk. JAMA Intern Med. 2015;175(6):1007–1017. doi:10.1001/jamainternmed.2015.1180
102. Lancellotti P, Nkomo VT, Badano LP, et al. Expert consensus for multi-modality imaging evaluation of cardiovascular complications of radiotherapy in adults: a report from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur Heart J Cardiovasc Imaging. 2013;14(8):721–740. doi:10.1093/ehjci/jet123
103. Spetz JKE, Florido MHC, Fraser CS, et al. Heightened apoptotic priming of vascular cells across tissues and life span predisposes them to cancer therapy-induced toxicities. Sci Adv. 2022;8(45):eabn6579. doi:10.1126/sciadv.abn6579
104. Yi J, Yue L, Zhang Y, et al. PTPMT1 protects cardiomyocytes from necroptosis induced by gamma-ray irradiation through alleviating mitochondria injury. Am J Physiol Cell Physiol. 2023;324(6):C1320–C31. doi:10.1152/ajpcell.00466.2022
105. Zhang X, Sun Y, Zhang Y, et al. Cardiac biomarkers for the detection and management of cancer therapy-related cardiovascular toxicity. J Cardiovasc Dev Dis. 2022;9(11).
106. Printezi MI, Yousif LIE, Kamphuis JAM, et al. LVEF by multigated acquisition scan compared to other imaging modalities in cardio-oncology: a systematic review. Curr Heart Fail Rep. 2022;19(3):136–145. doi:10.1007/s11897-022-00544-3
107. Cho I, You SC, Cha MJ, et al. Cancer therapy-related cardiac dysfunction and the role of cardiovascular imaging: systemic review and opinion paper from the Working Group on Cardio-Oncology of the Korean Society of Cardiology. J Cardiovasc Imaging. 2024;32(1):13. doi:10.1186/s44348-024-00014-5
108. Thavendiranathan P, Wintersperger BJ, Flamm SD, Marwick TH. Cardiac MRI in the assessment of cardiac injury and toxicity from cancer chemotherapy: a systematic review. Circ Cardiovasc Imaging. 2013;6(6):1080–1091. doi:10.1161/CIRCIMAGING.113.000899
109. Galan-Arriola C, Lobo M, Vilchez-Tschischke JP, et al. Serial magnetic resonance imaging to identify early stages of anthracycline-induced cardiotoxicity. J Am Coll Cardiol. 2019;73(7):779–791. doi:10.1016/j.jacc.2018.11.046
110. Tamaki N, Manabe O, Hirata K. Cardiovascular imaging in cardio-oncology. Jpn J Radiol. 2024;42(12):1372–1380. doi:10.1007/s11604-024-01636-x
111. Lisi C, Catapano F, Rondi P, et al. Multimodality imaging in cardio-oncology: the added value of CMR and CCTA. Br J Radiol. 2023;96(1150):20220999. doi:10.1259/bjr.20220999
112. Baumeier C, Harms D, Aleshcheva G, Gross U, Escher F, Schultheiss HP. Advancing precision medicine in myocarditis: current status and future perspectives in endomyocardial biopsy-based diagnostics and therapeutic approaches. J Clin Med. 2023;12(15):5050. doi:10.3390/jcm12155050
113. Murtagh G, Januzzi JL, Scherrer-Crosbie M, et al. Circulating cardiovascular biomarkers in cancer therapeutics-related cardiotoxicity: review of critical challenges, solutions, and future directions. J Am Heart Assoc. 2023;12(21):e029574. doi:10.1161/JAHA.123.029574
114. Thompson EW, Demissei BG, Smith AM, et al. Paraoxonase-1 activity in breast cancer patients treated with doxorubicin with or without trastuzumab. JACC Basic Transl Sci. 2022;7(1):1–10. doi:10.1016/j.jacbts.2021.10.010
115. Sumi M, Sato K, Uematsu N, et al. Clinical characteristics of vascular adverse events and significance of peripheral artery disease as a risk factor in chronic myeloid leukemia patients treated with nilotinib. Rinsho Ketsueki. 2018;59(2):137–144. doi:10.11406/rinketsu.59.137
116. Parr SK, Liang J, Schadler KL, Gilchrist SC, Steele CC, Ade CJ. Anticancer therapy-related increases in arterial stiffness: a systematic review and meta-analysis. J Am Heart Assoc. 2020;9(14):e015598. doi:10.1161/JAHA.119.015598
117. Schneider C, Gonzalez-Jaramillo N, Marcin T, et al. Time-dependent effect of anthracycline-based chemotherapy on central arterial stiffness: a systematic review and meta-analysis. Front Cardiovasc Med. 2022;9:873898. doi:10.3389/fcvm.2022.873898
118. Kirichenko YY, Ilgisonis IS, Belenkov YN, et al. The effect of chemotherapy on endothelial function and microcirculation in patients with gastric cancer. Kardiologiia. 2020;60(2):89–95. doi:10.18087/cardio.2020.2.n908
119. Muraru D, Niero A, Rodriguez-Zanella H, Cherata D, Badano L. Three-dimensional speckle-tracking echocardiography: benefits and limitations of integrating myocardial mechanics with three-dimensional imaging. Cardiovasc Diagn Ther. 2018;8(1):101–117. doi:10.21037/cdt.2017.06.01
120. Saito K, Okura H, Watanabe N, et al. Comprehensive evaluation of left ventricular strain using speckle tracking echocardiography in normal adults: comparison of three-dimensional and two-dimensional approaches. J Am Soc Echocardiogr. 2009;22(9):1025–1030. doi:10.1016/j.echo.2009.05.021
121. Azzam M, Wasef M, Khalaf H, Al-Habbaa A. 3D-based strain analysis and cardiotoxicity detection in cancer patients received chemotherapy. BMC Cancer. 2023;23(1):760. doi:10.1186/s12885-023-11261-y
122. Piveta RB, Rodrigues ACT, Vieira MLC, et al. Early change in area strain detected by 3d speckle tracking is associated with subsequent cardiotoxicity in patients treated with low doses of anthracyclines. Front Cardiovasc Med. 2022;9:842532. doi:10.3389/fcvm.2022.842532
123. Cartas-Espinel I, Telechea-Fernandez M, Manterola Delgado C, Avila Barrera A, Saavedra Cuevas N, Riffo-Campos AL. Novel molecular biomarkers of cancer therapy-induced cardiotoxicity in adult population: a scoping review. ESC Heart Fail. 2022;9(3):1651–1665. doi:10.1002/ehf2.13735
124. Johnson DB, Balko JM, Compton ML, et al. Fulminant myocarditis with combination immune checkpoint blockade. N Engl J Med. 2016;375(18):1749–1755. doi:10.1056/NEJMoa1609214
125. Jain SS, Elias P, Poterucha T, et al. Artificial intelligence in cardiovascular care-part 2: applications: JACC review topic of the week. J Am Coll Cardiol. 2024;83(24):2487–2496. doi:10.1016/j.jacc.2024.03.401
126. Hanneman K, Playford D, Dey D, et al. Value creation through artificial intelligence and cardiovascular imaging: a scientific statement from the American Heart Association. Circulation. 2024;149(6):e296–e311. doi:10.1161/CIR.0000000000001202
127. Nechita LC, Tutunaru D, Nechita A, et al. AI and smart devices in cardio-oncology: advancements in cardiotoxicity prediction and cardiovascular monitoring. Diagnostics. 2025;15(6):787. doi:10.3390/diagnostics15060787
128. O’Driscoll JM, Hawkes W, Beqiri A, et al. Left ventricular assessment with artificial intelligence increases the diagnostic accuracy of stress echocardiography. Eur Heart J Open. 2022;2(5):oeac059. doi:10.1093/ehjopen/oeac059
129. Battisha A, Mann C, Raval R, Anandaram A, Patel B. clinical applications and advancements of positron emission tomography/computed tomography in cardio-oncology: a comprehensive literature review and emerging perspectives. Curr Oncol Rep. 2024;26(11):1442–1451. doi:10.1007/s11912-024-01598-3
130. Bayoumy K, Gaber M, Elshafeey A, et al. Smart wearable devices in cardiovascular care: where we are and how to move forward. Nat Rev Cardiol. 2021;18(8):581–599. doi:10.1038/s41569-021-00522-7
131. Sana F, Isselbacher EM, Singh JP, Heist EK, Pathik B, Armoundas AA. Wearable devices for ambulatory cardiac monitoring: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(13):1582–1592. doi:10.1016/j.jacc.2020.01.046
132. Shil S, Kumar P, Mumbrekar KD. Cancer therapy-induced cardiotoxicity: mechanisms and mitigations. Heart Fail Rev. 2025;30:1075–1092. doi:10.1007/s10741-025-10531-0
133. Asnani A, Moslehi JJ, Adhikari BB, et al. Preclinical models of cancer therapy-associated cardiovascular toxicity: a scientific statement from the American Heart Association. Circ Res. 2021;129(1):e21–e34. doi:10.1161/RES.0000000000000473
134. Kitani T, Ong SG, Lam CK, et al. Human-induced pluripotent stem cell model of trastuzumab-induced cardiac dysfunction in patients with breast cancer. Circulation. 2019;139(21):2451–2465. doi:10.1161/CIRCULATIONAHA.118.037357
135. Lewis Phillips G, Guo J, Kiefer JR, et al. Trastuzumab does not bind rat or mouse ErbB2/neu: implications for selection of non-clinical safety models for trastuzumab-based therapeutics. Breast Cancer Res Treat. 2022;191(2):303–317. doi:10.1007/s10549-021-06427-w
136. Ghigo A, Ameri P, Asnani A, et al. Update on preclinical models of cancer therapy-related cardiac dysfunction: challenges and perspectives. A scientific statement of the Heart Failure Association (HFA) of the ESC, the ESC Council of Cardio-Oncology, and the ESC Working Group on Cellular Biology of the Heart. Eur J Heart Fail. 2025.
137. Ravera F, Gilardi N, Ballestrero A, Zoppoli G. Applications, challenges and future directions of artificial intelligence in cardio-oncology. Eur J Clin Invest. 2025;55(Suppl 1):e14370. doi:10.1111/eci.14370
138. Porter C, Azam TU, Mohananey D, et al. Permissive cardiotoxicity: the clinical crucible of cardio-oncology. JACC CardioOncol. 2022;4(3):302–312. doi:10.1016/j.jaccao.2022.07.005
139. Bloom MW, Vo JB, Rodgers JE, et al. Cardio-oncology and heart failure: a scientific statement from the heart failure society of America. J Card Fail. 2025;31(2):415–455. doi:10.1016/j.cardfail.2024.08.045
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
“Technology Proficiency” in Medical Education: Worthiness for Worldwide Wonderful Competency and Sophistication
Jain S, Jain BK, Jain PK, Marwaha V
Advances in Medical Education and Practice 2022, 13:1497-1514
Published Date: 15 December 2022
Maintaining Serum Hemoglobin Levels Within the Physiological Range Prevented Bladder Tamponade Recurrence Due to Radiation-Induced Hemorrhagic Cystitis: A Case Report
Ueda N, Sato M, Matsukawa A, Oki Y, Mizuno R, Akiyama M, Tei N, Miyake O
Research and Reports in Urology 2023, 15:395-401
Published Date: 21 August 2023