Back to Journals » Clinical Ophthalmology » Volume 20
Challenging the Treatment Threshold: Early Faricimab Prevents Vision Loss in nAMD – A Real-World Welsh Experience
Authors Swarnkar PK ![]() , Singh Bhangu J
, Singh Bhangu J ![]() , Stewart C
, Stewart C ![]() , Rifat M
, Rifat M ![]() , Khalid S, Winkworth H, Franklin-Goddard SL, Awad MH
, Khalid S, Winkworth H, Franklin-Goddard SL, Awad MH ![]() , Williams GS
, Williams GS
Received 8 March 2026
Accepted for publication 12 May 2026
Published 23 May 2026 Volume 2026:20 604687
DOI https://doi.org/10.2147/OPTH.S604687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Parinita Keshav Swarnkar,1 Jaskaran Singh Bhangu,1 Christopher Stewart,2 Mohammed Rifat,1 Sarah Khalid,1 Harry Winkworth,2 Savannah Lydia Franklin-Goddard,2 Mahmoud Husseiny Awad,1 Gwyn Samuel Williams1
1Ophthalmology Department, Singleton Hospital, Swansea Bay University Healthboard, Swansea, Wales, UK; 2Faculty of Medicine, Health and Life Science, Swansea University, Swansea, Wales, UK
Correspondence: Parinita Keshav Swarnkar, Ophthalmology Department, Singleton Hospital, Swansea Bay University Healthboard, Swansea, Wales, UK, Email [email protected]
Purpose: To compare real-world outcomes in treatment-naïve neovascular age-related macular degeneration (nAMD) patients initiated on Faricimab at early (< 0.3 logMAR) versus late (0.6– 0.7 logMAR) visual thresholds.
Methods: Retrospective, single-centre cohort study of 97 patients (53 early, 44 late) treated at a UK centre, with three monthly loading doses followed by treat-and-extend. Outcomes: BCVA change, vision loss (≥ 5 letters), stable vision at 6/12/18 months, injection intervals, extension > 8 weeks, dry macula.
Results: Baseline VA was 74 ± 3.5 letters (early) vs 54 ± 2.0 letters (late), p< 0.001. No early patient experienced sustained vision loss at 6, 12, or 18 months compared with 76.7%, 73.3%, and 75.0% of late patients, respectively (p< 0.05 for all). At the 7th injection, 67.6% of late patients lost ≥ 5 letters vs 14.9% of early patients (ARR 52.7%, p< 0.001). Cumulatively, 81.8% of late patients experienced ≥ 5-letter loss vs 41.5% of early patients (ARR 40.3%, NNT 3, p< 0.001). Mean injection intervals were similar, but the early cohort sustained extension beyond 8 weeks in > 50% of eyes from the 4th– 5th interval onward. In contrast, the late cohort exhibited a biphasic collapse, with extension rates declining from 62.2% at 6th– 7th to only 35.0% by 9th– 10th. Despite a significant baseline anatomical disadvantage (18.9% vs 50.0% dry macula, p=0.001), the early cohort achieved 100% dryness by 18 months compared with 96.7% in the late cohort, with crossover occurring by 12 months (95.8% vs 89.7%, p=0.269).
Conclusion: In this retrospective, single-centre study, early faricimab initiation was associated with preservation of high-function vision, a lower risk of clinically significant vision loss, and high rates of anatomical quiescence and durable treatment extension. These findings suggest that proactive early intervention may offer advantages over reactive treatment paradigms, although confirmation in larger, prospective, and multi-centre studies is needed.
Plain Language Summary: Why was this study done?
Wet AMD is a leading cause of sight loss in older people. In the UK, treatment usually starts after visions reaches 6/12 or below. In Wales, doctors have been starting treatment earlier, while vision is still good, to try to preserve sight rather than just slow further loss. This study compared these two approaches.
What did the researchers find?
Of 97 patients starting the drug Faricimab, 53 started early (good vision) and 44 started later (usual UK threshold).
Key findings:All Early patients kept stable vision at 6, 12, and 18 months. In contrast, about one in four Late patients lost vision.By the 7th injection, two out of three Late patients had lost vision, compared to only one in seven Early patients.Four out of five Late patients experienced vision loss, versus two out of five Early patients.Early patients achieved completely dry retinas by 18 months, even though they began with more fluid.Early patients were also better able to maintain longer gaps between injections over time.
What do these results mean?
Starting treatment early preserves high-quality vision and prevents the decline that current pathways accept. Early patients were more likely to keep their driving vision, vital for independence and quality of life. Our findings suggest that waiting for vision to drop misses a critical window. With modern anti-VEGF drugs, a proactive approach can help people with wet AMD retain useful vision longer and maintain the lifestyle they value.
Keywords: faricimab, nAMD, early intervention, treat-and-extend, real-world evidence, visual acuity
Introduction
Age-related macular degeneration (AMD) is the world’s leading cause of irreversible partial or complete central visual loss in the elderly population of higher income countries.1 With progressively ageing populations, it is expected that by 2040, up to 300 million people will be affected by AMD.2 Although the neovascular form (nAMD) accounts for only 10–15% of all AMD cases, it is responsible for approximately 90% of severe vision loss associated with the disease.3,4 nAMD is characterised by the development of choroidal neovascularisation (CNV), with intra-or sub-retinal fluid accumulation, haemorrhage, and ultimately, disciform scarring (RPE (retinal pigment epithelium) detachments) which lead to central vision loss.5
Intravitreal anti-Vascular Endothelial Growth Factor (VEGF) therapy has revolutionised nAMD treatment by reducing existing vascular permeability and inhibiting new vessel formation. However, anti-VEGF impact is limited by treatment burden (monthly or bi-monthly injections requiring hospital travel) and by patient-dissatisfaction of overall long-term effectiveness.6 As of 2024, four anti-VEGF agents are licensed for nAMD in the UK: ranibizumab (Lucentis®), aflibercept 2 mg (Eylea®), brolucizumab (Beovu®), and faricimab (Vabysmo®); bevacizumab (Avastin®) is used off-label. Recent data from the LEAVO and TANDEM trials confirm that bevacizumab is cost-effective and non-inferior to aflibercept 2 mg.7,8
Faricimab, the first-line anti-VEGF agent used for newly diagnosed nAMD in SBUHB, is a novel bispecific antibody that dually inhibits VEGF and Angiopoietin-2 (Ang-2) pathways.9 VEGF-A blockade limits neovascularisation while Ang-2 inhibition promotes vessel stabilisation, thus potentially reducing local haemorrhage. In the Phase III TENAYA and LUCERNE trials, faricimab was non-inferior to aflibercept 2 mg, with maintained vision at two years.10 Importantly, faricimab’s extended durability (up to 16-week dosing intervals in many trial patients) distinguish it from earlier agents. Compared with Ranibizumab (monthly dosing) and standard Aflibercept (8-week intervals), Faricimab offers the potential for reduced treatment burden, although comparative real-world data on interval extension beyond trial settings remain limited. A recent perspective has proposed a shift towards a “durability-centred framework” for nAMD management, emphasising sustained disease control as the primary therapeutic goal beyond short-term efficacy.11 Whether any observed benefits of early treatment are drug-specific or primarily related to the timing of intervention is therefore difficult to control for but informs the interpretation of our findings.
In 2025, an Aflibercept 2mg biosimilar (MYNZEPLI®) became available at a lower cost than the originator (£85 vs £380.19 per injection, excluding VAT).
While more affordable treatments are welcome, particularly in a National Health Service (NHS) context seeking to reduce spending without compromising care, an evidence base is essential to guide decisions, especially regarding the preservation of good baseline visual function.
A large body of observational and post-hoc trial evidence indicates that baseline visual acuity (VA) is a strong predictor of final VA in nAMD patients treated with anti-VEGF agents.12,13 Patients presenting with better initial VA tend to retain better vision over time, whereas those with poorer baseline VA often have limited functional recovery, partly due to irreversible photoreceptor damage. However, most studies have focused on outcomes after treatment initiation at conventional thresholds (eg, VA ≤6/12). Much less is known about whether initiating treatment at an even earlier stage, when patients still have high-functioning vision, confers additional benefit beyond that predicted by baseline VA alone.
This uncertainty is clinically important because early treatment might prevent vision loss that would otherwise be irreversible, but it could also lead to overtreatment of patients who would have remained stable without immediate intervention.
Current guidance from the National Institute for Health and Care Excellence (NICE) recommends offering treatment when VA falls between 6/12 and 6/96, ie, after significant functional vision loss has already occurred.14 At that stage, moderate photoreceptor loss is often irreversible, and therapy primarily aims to slow further decline rather than to restore lost vision. In Wales, clinical practice deviates from this NICE threshold: patients are offered intravitreal anti-VEGF therapy at the point of nAMD diagnosis, irrespective of their baseline best-corrected VA (BCVA). This has resulted in a treated population with substantially better mean baseline VA than that typically seen in England under NICE guidance. The Welsh approach is logically appealing, but its real-world efficacy has not been quantified. Specifically, it remains unknown whether early initiation can more effectively preserve high-functioning vision, prevent clinically significant visual decline, and enable longer, less burdensome treatment intervals compared with the standard later-initiated regimen.
Early and late cohorts were defined based on baseline BCVA at the time of first Faricimab injection. The early cohort comprised patients initiating treatment at a BCVA of <0.3 logMAR (equivalent to better than 6/12 Snellen). This threshold represents high-functioning vision and reflects the proactive treatment pathway adopted in Wales, where therapy is offered at the point of nAMD diagnosis regardless of baseline acuity.15,16 The late cohort was defined as patients starting treatment with a BCVA of 0.6–0.7 logMAR (approximately 6/24–6/30 Snellen). This range was selected for several clinically and epidemiologically relevant reasons. First, it aligns closely with the median baseline visual acuity reported in large, real-world nAMD registries and historical UK cohorts, thereby reflecting a common clinical presentation for patients with established disease.17 Second, this acuity range is characteristic of the so-called “first eye gap”, in which the initial diagnosis of nAMD is often made only after significant, irreversible vision loss has already occurred, making it an ideal benchmark for delayed presentation and missed opportunities for earlier intervention. Third, the selection of these cohorts is further justified by the distinct statistical and functional dynamics at each threshold. The early cohort represents patients at the “functional ceiling”, where the primary therapeutic objective is the preservation of high-acuity vision rather than significant letter gain. Conversely, the late cohort captures patients approaching a “functional floor” regarding independence. As noted by Rasmussen et al (2017), once visual acuity reaches the 0.7 LogMAR mark, vision typically declines to a level that prohibits reading. This transition marks a critical clinical pivot where treatment goals shift from the restoration of sight to the preservation of remaining vision and the slowing of further irreversible deterioration.
Based on these definitions, we tested the hypothesis that early treatment (initiated at <0.3 logMAR) is associated with superior preservation of visual acuity, reduced risk of vision loss, better anatomical outcomes, and more durable treatment intervals compared with late treatment (initiated at 0.6–0.7 logMAR). The primary objective of this retrospective, single-centre cohort study was therefore to compare real-world outcomes in treatment-naïve nAMD patients started on Faricimab at these two different visual thresholds, while acknowledging that our observational design can support association not causation, and that observed differences may reflect baseline prognostic factors rather than timing per se. By comparing outcomes between the early and late cohorts, this study evaluates the real-world consequences of delaying treatment until after significant vision loss has become established, relative to a strategy of proactive early intervention.
Methods
Study Design
This was a retrospective, comparative non-randomised cohort study of treatment-naïve patients with nAMD treated with Faricimab at Singleton Hospital, Swansea Bay University Health Board (SBHUB) between March 2023 and August 2025. Demographic and clinical data were collected from clinical notes and electronic health records (Welsh Clinical Portal (WCP) and OpenEyes®). Due to the retrospective nature, the requirement for informed consent was waived. All patients received a standardised loading phase of three-monthly injections followed by a treat-and-extend protocol.18 Extension decisions were based on standardised criteria: absence of new haemorrhage, stable or improved BCVA, resolution of fluid on OCT, and ≤50μm increase in CMT. Re-treatment criteria included: new macular haemorrhage, ≥5-letter vision loss attributable to nAMD, or recurrence of IRF/SRF.
Patients were stratified into two cohorts based on baseline BCVA at treatment initiation:
- Early cohort: BCVA <0.3 logMAR (better than 6/12 Snellen)
- Late cohort: BCVA 0.6–0.7 logMAR (6/24 – 6/30 Snellen)
Patient Selection
Inclusion Criteria
- Newly diagnosed (with optical coherence tomography (OCT) and/or fundus fluorescein angiography (FFA)) with treatment-naïve nAMD;
- First-line intravitreal anti-VEGF therapy with Faricimab;
- Completed at least five Faricimab injections with complete follow-up data at the third and fifth injection visits;
- Spectral-domain optical coherence tomography (SD-OCT) imaging at all timepoints.
Exclusion Criteria
- Co-existing or previous retinal pathologies affecting VA (eg, diabetic retinopathy, retinal vein occlusion, etc);
- Prior retinal surgery or intravitreal therapy;
- Significant media opacity precluding imaging;
- Fewer than five Faricimab injections received at time of analysis;
- Patients with missing data at both the third and fifth injection visits were excluded;
- Patients explicitly excluded for safety/reason (eg, “Notes lost”, “Not on Faricimab”, “Patients notes unavailable”, “Faricimab used as second-line treatment in refractory to first-line therapy”) were removed.
Data Collection
Two independent investigators PKS and CS manually extracted the following variables from electronic patient records and clinical notes, with discrepancies resolved by senior author GW. From an initial pool of 134 eligible eyes, 97 met all inclusion criteria and were included in the final analysis (53 in the Early treatment cohort, 44 in the Late treatment cohort). To maintain independence of observations and avoid inter-eye correlation issues common in ophthalmic research, only one eye per patient was included in the analysis (eyes from 97 individual subjects).19 No further statistical adjustment for potential within-patient correlation was therefore required, as each patient contributed a single eye. The most common reasons for exclusion were fewer than five Faricimab injections received (n=23), use of Faricimab as second-line therapy (n=8), and missing key timepoint data (n=6).
Imaging parameters (IRF, SRF, pigment epithelial detachment [PED]) were assessed from spectral-domain OCT images obtained at each visit by technicians independent of the treating clinical team. No formal interobserver agreement analysis (eg, Cohen’s kappa) was conducted, which is acknowledged as a limitation.
All patients underwent standardised assessment at each visit, including:
Baseline Characteristics (Pre-treatment) (Table 1):
- Demographics: Sex, Age, Ethnicity, Smoking Status
- BCVA measured using Early Treatment Diabetic Retinopathy Study (ETDRS) charts and converted to logMAR for analysis
- OCT parameters: presence of IRF (yes/no), SRF (yes/no), PED (yes/no)
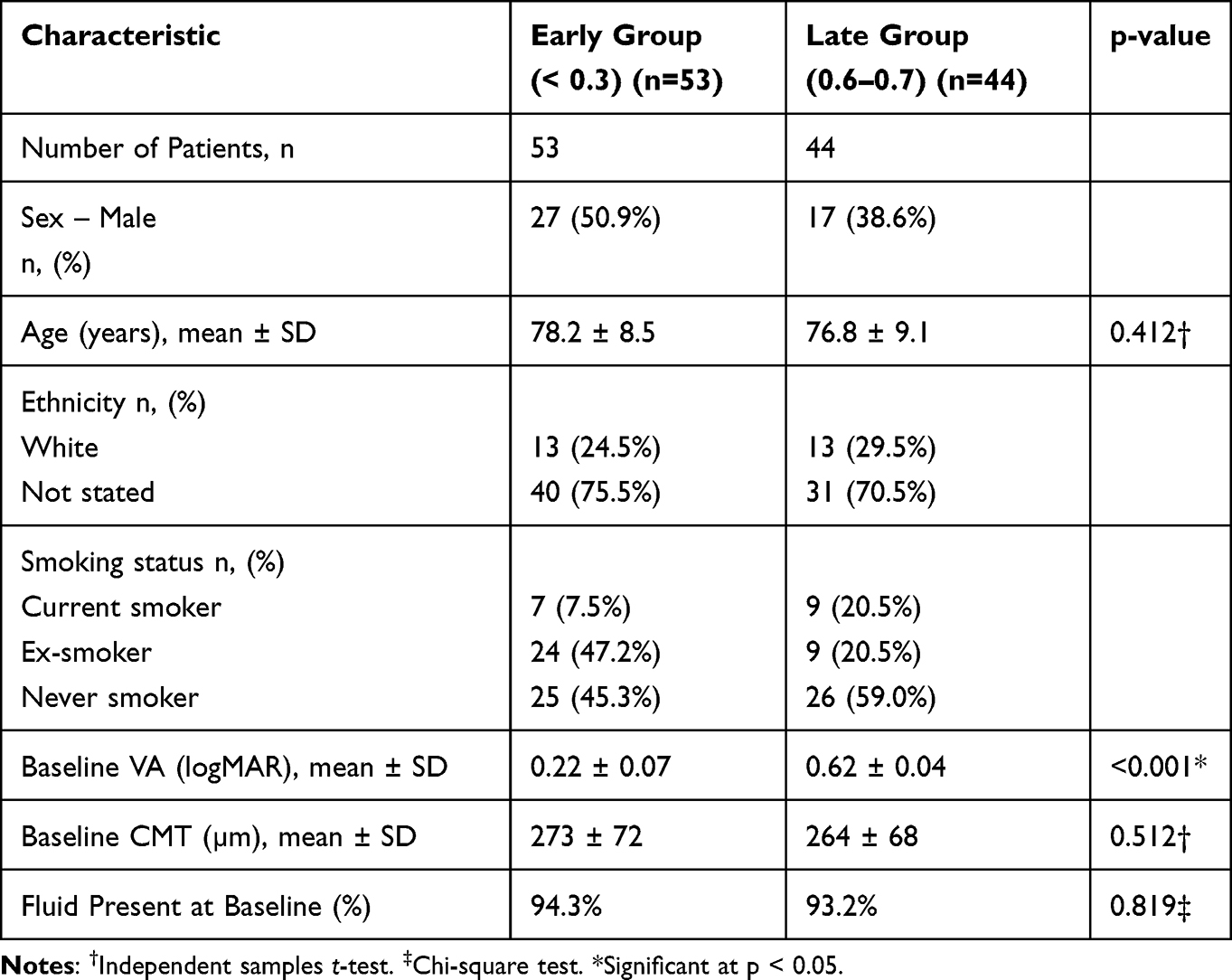 |
Table 1 Baseline Characteristics |
Follow-up data (at third, fifth, seventh, and tenth injection visits):
- BCVA, IRF, SRF, PED, and haemorrhage status
- Treatment data: injection dates, intervals, and number of injections
Outcomes:
- Visual outcomes:
- Mean change in BCVA: Change from baseline in ETDRS letters (converted from logMAR) at each injection visit (4th through 10th) - independent t-test.
- Clinically significant vision loss: Proportion of eyes losing ≥5 ETDRS letters (equivalent to ≥0.1 logMAR increase) from baseline at each injection visit - absolute risk reduction (ARR), number needed to treat (NNT), risk ratio (RR) with 95% confidence interval.
- Sustained vision stability: Proportion of eyes maintaining stable vision (defined as <5 letters lost from baseline) at landmark timepoints of 6, 12, and 18 months - RR (95% CI).
- Cumulative vision loss: Proportion of eyes experiencing at least one episode of ≥5-letter loss during follow-up - ARR and NNT.
- Response consistency: Coefficient of variation (CV) of letter change at each timepoint.
- Treat‑and‑Extend Outcomes:
- Mean injection intervals (weeks) between injections for each treatment cycle (3rd–4th through 9th–10th) - independent t-test.
- Extension rates: proportion of eyes achieving treatment intervals ≥8 weeks at each cycle - independent t-test.
- Interval stability: Mean change in interval duration (Δ weeks) between successive cycles, and proportion of eyes requiring interval shortening (“relapse rate”) at each transition - independent t-test.
- Anatomical outcomes:
- Fluid resolution rates: proportion of eyes achieving a dry macula (absence of IRF and SRF) at 6, 12, and 18 months - independent t-test.
Follow-Up Duration and Long-Term Outcomes
Follow-up extended to 18 months and approximately ten injections, which is adequate to capture short- to medium-term functional and anatomical outcomes, as well as treatment interval dynamics within a treat-and-extend framework. Mean follow up was 64 and 82 weeks for Early and Late cohorts, respectively.
Statistical Analysis
Statistical analysis was performed using SPSS version 30.0 (IBM Corp, Armonk, NY). Continuous variables were expressed as mean ± standard deviation (SD) and compared using independent t-tests or Mann–Whitney U-tests as appropriate based on distribution. Categorical variables were expressed as frequencies and percentages and compared using chi-square or Fisher’s exact tests. Within-group changes from baseline were analysed using paired t-tests.
For binary outcomes, absolute risk reduction (ARR) and number needed to treat (NNT) were calculated directly from 2×2 contingency tables. ARR was defined as the difference in the proportion of events between the Late and Early cohorts (Late – Early). NNT was calculated as 1 / ARR (rounded up to the nearest integer). Relative risks (RR) with 95% confidence intervals were estimated using the Cochran-Mantel-Haenszel method. All tests were two-tailed with p < 0.05 considered statistically significant.
No formal power calculation was performed due to the retrospective and exploratory nature of the study; the sample size (97 eyes) was based on available eligible cases during the study period. Consequently, the study may be underpowered to detect smaller differences, particularly for secondary endpoints or later timepoints, and some clinically relevant but statistically non-significant trends should be interpreted cautiously.
Adjustment for confounding: Given the non-randomised, observational design, baseline differences between early and late cohorts (eg, age, comorbidities, baseline anatomical features) may confound observed outcomes. No multivariable adjustment or regression modelling was undertaken. Therefore, the reported associations should not be interpreted as causal, and residual confounding by indication (including differences in prognosis, clinician decision-making, and access to care) remains a significant limitation.
Ethical Considerations
Data were anonymised and stored securely according to SBUHB GDPR policies. The retrospective nature waived the need for informed consent.
Results
Demographics
A total of 97 eyes from 97 patients were included: 53 in the Early group (baseline visual acuity [VA] 0.22 ± 0.07 logMAR) and 44 in the Late group (baseline VA 0.62 ± 0.04 logMAR). (Table 1). The groups were well-matched in age (78.2 ± 8.5 vs 76.8 ± 9.1 years, p=0.412) and baseline central macular thickness (273 ± 72 vs 264 ± 68 μm, p=0.512). As expected by design, baseline VA differed significantly between groups (p<0.001). The proportion of eyes with fluid present at baseline was similarly high in both groups (94% vs 93%, p=0.819).
Visual Acuity
The Early group demonstrated significantly better visual preservation at multiple timepoints compared to the Late group (Table 2). Following the 5th injection, the Early group lost a mean of 0.1 ± 3.0 letters, whereas the Late group lost 4.4 ± 7.7 letters, representing a mean difference of 4.3 fewer letters lost with early treatment (95% CI 1.7–6.9, p = 0.001). Similarly, after the 6th injection, the Early group lost 1.0 ± 4.4 letters compared to a gain of 2.7 ± 9.1 letters in the Late group (mean difference +3.7 letters, 95% CI 0.4–7.0, p = 0.028). Trends favouring early treatment were observed after the 4th injection (3.6 fewer letters lost, p = 0.064) and 7th injection (3.2 fewer letters lost, p = 0.063), though these did not reach statistical significance. From the 8th to 10th injections, no significant differences were observed between groups, although early treatment continued to show numerically less vision loss.
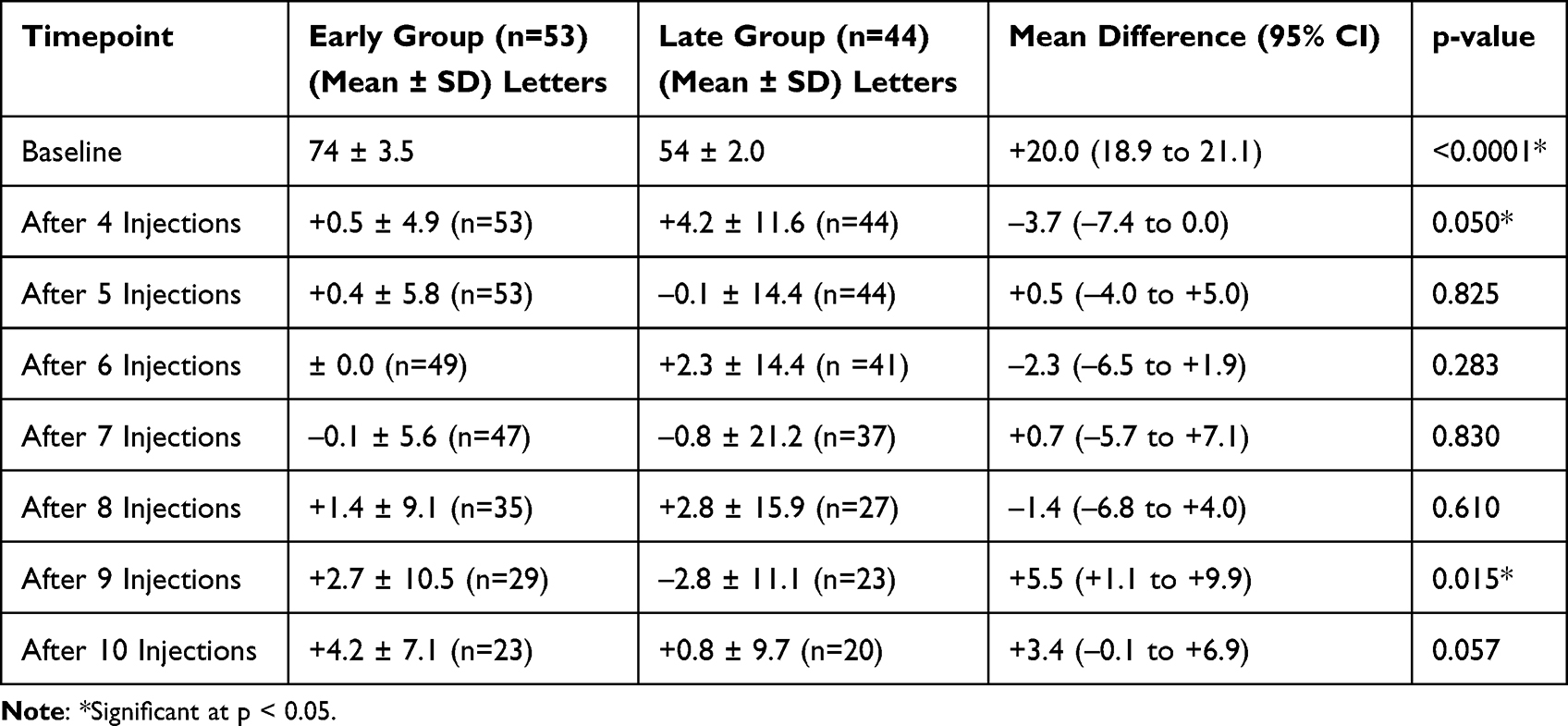 |
Table 2 Mean Change in BCVA (ETDRS Letters) from Baseline |
Analysis of the coefficient of variation (CV) revealed marked differences in the consistency of treatment response between groups (Table 2). The Early group demonstrated a progressive reduction in relative variability over time, with CV decreasing from 980% after the 4th injection to 169% after the 10th injection, indicating increasingly consistent letter gains as treatment progressed. In contrast, the Late group exhibited persistently high relative variability throughout the treatment course, with CV values exceeding 500% at most timepoints and reaching 1213% after the 10th injection. This high variability reflects inconsistent and unpredictable visual outcomes in eyes receiving later treatment. The single exception was at the 6th injection, where the Late group showed a mean gain with moderate variability (CV 626%), though this was not sustained.
A significantly higher proportion of eyes in the Early group maintained stable vision at 6, 12, and 18 months (Table 3). At 6 months, 100% (40/40) of Early group eyes maintained vision compared to 76.7% (33/43) in the Late group (RR 1.30, 95% CI 1.12–1.52, p=0.001). This difference persisted at 12 months (100% vs 73.3%, RR 1.36, 95% CI 1.14–1.63, p=0.003) and 18 months (100% vs 75.0%, RR 1.33, 95% CI 1.06–1.68, p=0.040).
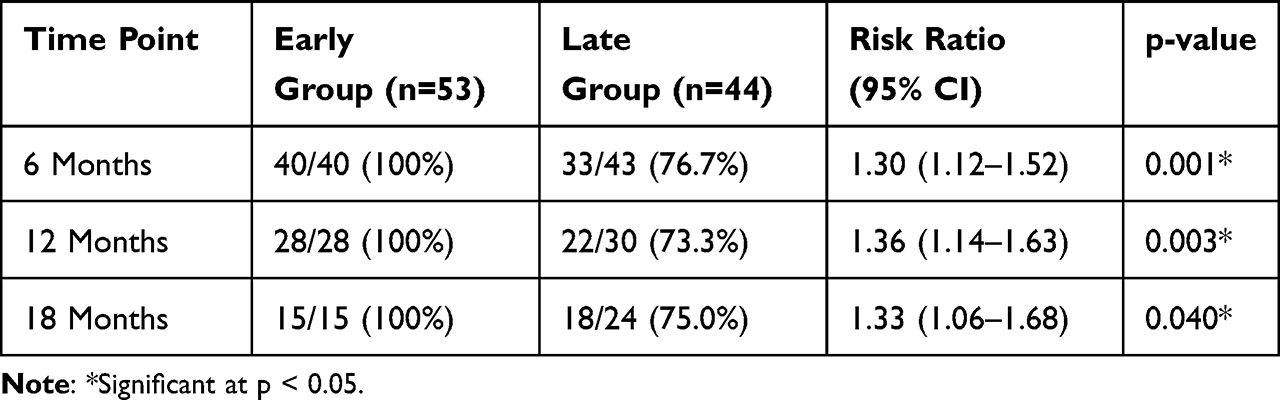 |
Table 3 Proportion of Eyes Maintaining Stable Vision at Key Timepoints |
The proportion of eyes experiencing clinically significant vision loss (≥5 ETDRS letters from baseline) was assessed at each injection from the 4th through the 10th (Figure 1 and Supplementary Table 1). In the Early cohort, the rate remained consistently low, ranging from 5.7% at the 5th injection to a peak of 22.0% at the 6th injection, then declining to 8.0% by the 10th injection. The Late cohort showed a distinctly different pattern: after an initial rate of 18.2% at the 4th injection, the proportion rose sharply to 36.4% at the 5th injection and peaked at 62.5% at the 7th injection, before declining to 29.2% at the 10th injection. The difference between cohorts was most pronounced at the 5th and 7th injections. At the 5th injection, 5.7% of Early patients lost ≥5 letters versus 36.4% of Late patients (ARR 30.7%, NNT 4, 95% CI 3–7, p<0.001). At the 7th injection, 14.9% of Early patients experienced such deterioration compared to 67.6% of Late patients (ARR 52.7%, NNT 2, 95% CI 2–3, p<0.001). A significant difference was also observed at the 10th injection (8.0% vs 35.0%, ARR 27.0%, NNT 4, 95% CI 3–22, p=0.049). No significant differences were observed at the 4th, 6th, 8th, or 9th injections, although rates consistently favoured the Early group.
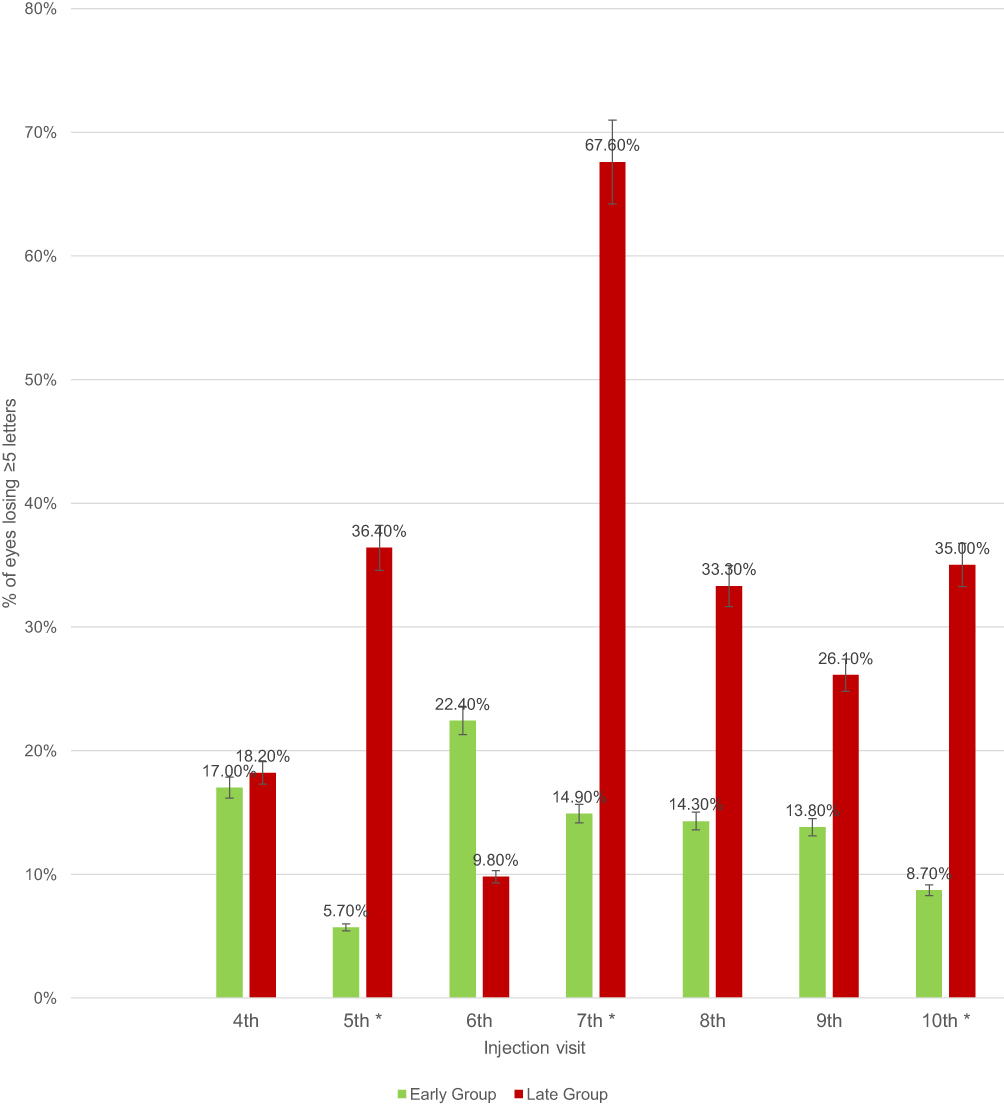 |
Figure 1 Percentage of eyes losing ≥5 ETDRS letters from baseline at each injection visit. *Significant at p < 0.05. |
Cumulatively, 41.5% (22/53) of Early patients experienced at least one episode of ≥5-letter loss during follow-up, compared to 81.8% (36/44) of Late patients, an absolute risk reduction of 40.3%. This corresponds to a number needed to treat (NNT) of 3 (95% CI 2–4), meaning that treating three patients at an early threshold prevents one additional patient from ever experiencing clinically significant vision loss.
Treat and Extend
Analysis of injection intervals revealed a biphasic treatment response between groups (Table 4 and Figure 2). In the early treatment phase (3rd to 5th injections), the Early group maintained significantly shorter intervals than the Late group (eg, 4th to 5th: 7.8 ± 2.8 vs 9.2 ± 3.9 weeks, p = 0.034), reflecting more proactive initial treatment. The mean injection intervals for each treatment cycle, along with the number of patients contributing data at each interval, are presented in Table 5.
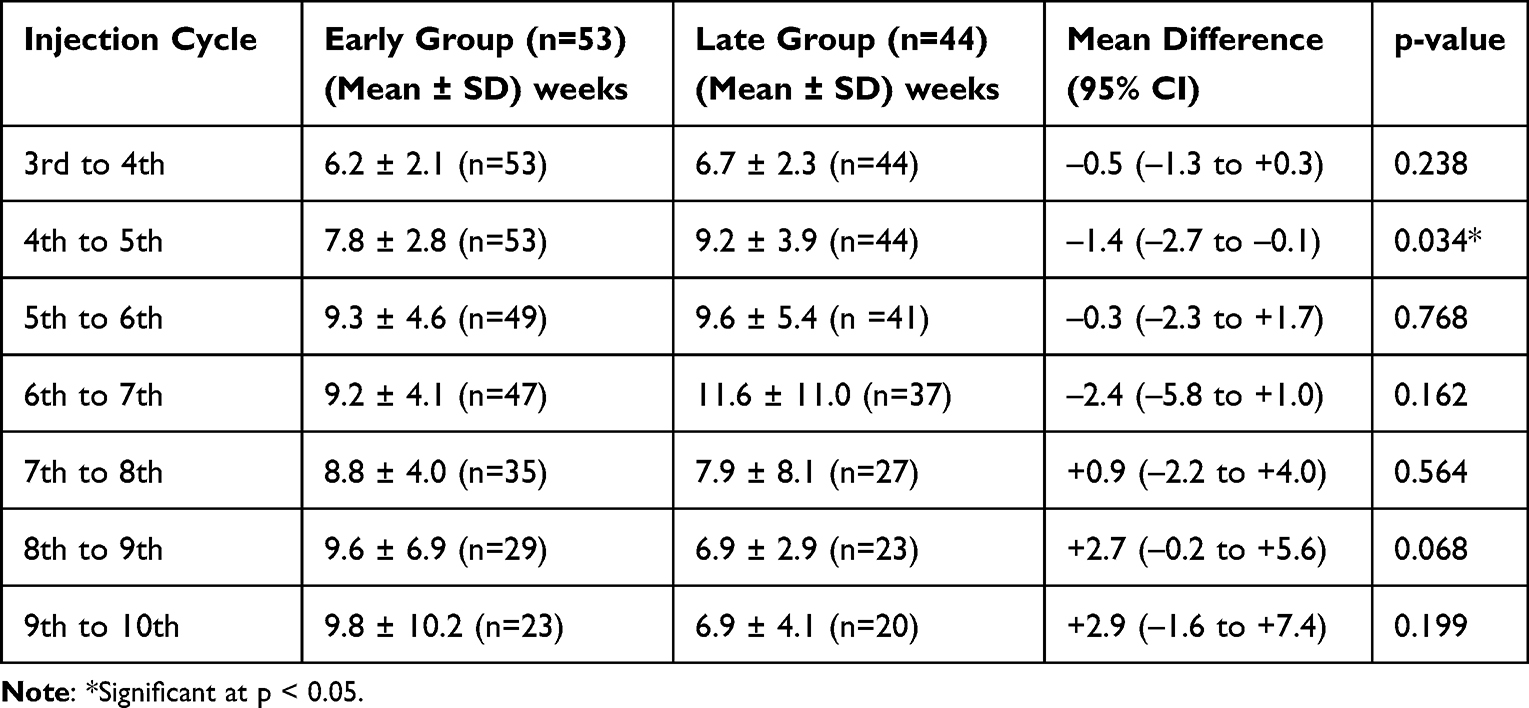 |
Table 4 Mean Injection Intervals Achieved in T&E (Weeks) |
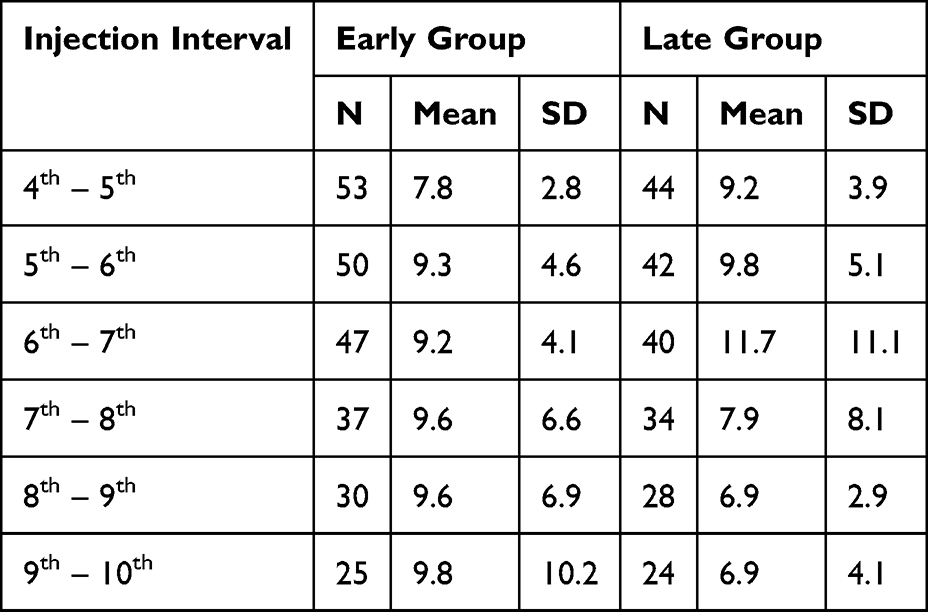 |
Table 5 Mean Injection Intervals (Weeks) from 4th to 10th Injections |
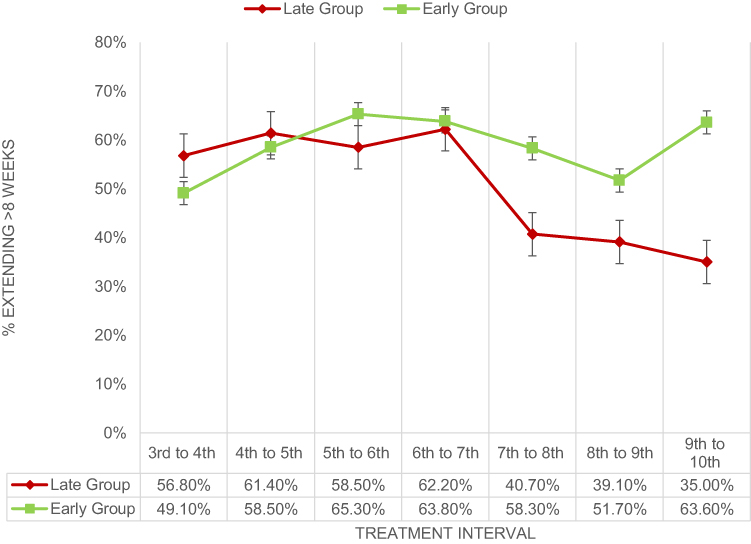 |
Figure 2 Proportion of Eyes Achieving Treatment Interval Extension Beyond 8 Weeks Over Successive Treatment Cycles. |
During the middle phase (5th to 7th injections), both groups extended their intervals, with no significant differences. However, from the 7th injection onward, a divergent pattern emerged. The Early group maintained or gradually extended intervals through the 10th injection (9.8 ± 10.2 weeks), with >50% of intervals exceeding 8 weeks throughout.
In contrast, the Late group exhibited a biphasic collapse: after peaking at 11.6 ± 11.0 weeks (6th to 7th), intervals shortened progressively to 6.9 ± 4.1 weeks by the 9th to 10th cycle. The proportion of Late group intervals >8 weeks fell sharply from 62.2% at 6th–7th to only 35.0% by 9th–10th (vs 63.6% in Early group).
Examining the proportion of intervals exceeding 8 weeks revealed a divergence in treatment durability (Figure 2). The Early group exhibited stable disease control, with extension rates consistently above 50% throughout all cycles (range 49.1–65.3%). Conversely, the Late group demonstrated progressive instability, as the proportion of eyes achieving extended intervals dropped markedly from 62.2% at the 6th–7th cycle to only 35.0% by the 9th–10th cycle.
Analysis of interval-to-interval changes revealed no significant differences between groups in treatment stability (Table 6). Mean interval changes were close to zero across all transitions in both cohorts, indicating no sustained trend toward progressive lengthening or shortening of treatment intervals over time.
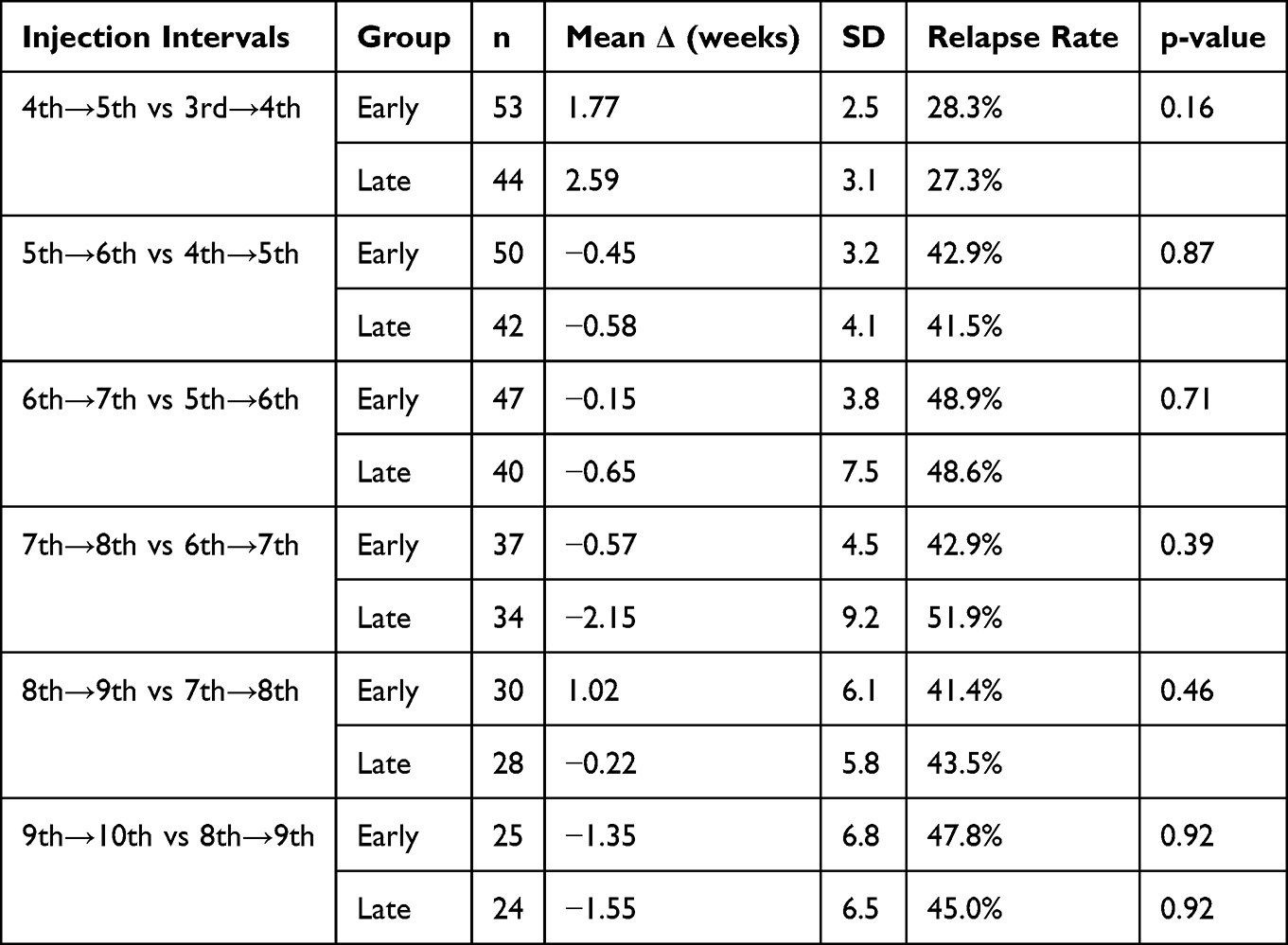 |
Table 6 Interval Stability |
Relapse rates, defined as the proportion of eyes requiring interval shortening at each transition, ranged from 27–52% across all cycles and were similar between groups at every transition. Rates peaked at the 6th–7th transition in both the Early (48.9%) and Late (48.6%) groups, coinciding with the point at which absolute intervals began to diverge.
Although the Late group exhibited a numerically higher relapse rate at the 7th–8th transition (51.9% vs 42.9%), this difference was not statistically significant (p = 0.39). No significant between-group differences in mean interval change were observed at any transition (all p > 0.05).
Anatomical
At 6 months, 75.5% of eyes in the Early group had achieved a dry macula compared to 90.5% in the Late group (p = 0.028). By 12 months, dry macula rates were 95.8% vs 89.7% (p = 0.269), and by 18 months, 100% vs 96.7% (p = 1.000) (Figure 3). Mean average CMT at end of follow up was 239 µm and 210 µm, for Early (−14.8%) and Late (−27.6%) cohorts, respectively.
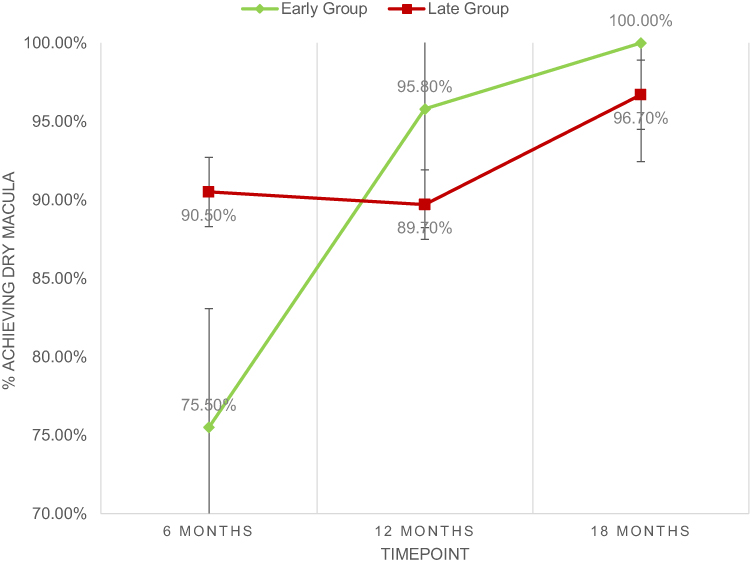 |
Figure 3 Proportion of Eyes Achieving Dry Macula (No IRF/SRF) at 6, 12, and 18 Months. All eyes had active fluid at baseline (0% dry) by inclusion criteria. |
Discussion
This real-world study provides the first direct comparison of early versus conventional late treatment initiation with Faricimab in treatment-naïve nAMD. Initiating therapy before substantial visual decline (BCVA <0.3 logMAR) preserved superior and more consistent visual function, prevented sustained vision loss, and enabled more durable treatment intervals than delaying treatment until vision had fallen to 0.6–0.7 logMAR. These findings extend the efficacy and durability observed in the TENAYA and LUCERNE trials by demonstrating that treatment timing critically determines whether real-world outcomes approach trial benchmarks or deteriorate into a “durability ceiling”.10
Visual Acuity
Our results reinforce a principle established in pivotal trials such as VIEW 1 and 2 and HARBOR: baseline visual acuity is the strongest predictor of final visual outcome.12,13 The early cohort preserved a mean of ~74 letters through ten injections, while the late cohort, despite equivalent anatomical control by 18 months, remained at a functional ceiling of ~54 letters. This ceiling effect has real-world impacts: the early cohort’s mean outcome (0.18 logMAR, ~20/32) exceeds the UK driving standard (≤0.3 logMAR), whereas the late cohort initiated treatment already below that threshold and never recovered driving-eligible vision. The current NICE guideline effectively accepts vision loss to the point of driving ineligibility as inevitable; our data suggest this is a policy choice rather than a biological necessity.20
Early treatment prevented sustained ≥5-letter loss entirely at landmark visits (NNT = 4 to prevent one case). Moreover, the early group demonstrated progressively consistent responses (coefficient of variation decreasing from 980% to 169%), while the late group’s outcomes remained unpredictably variable (CV up to 1213%). This consistency benefit, an underappreciated aspect of treatment timing, has direct implications for patient counselling and clinical decision-making. The temporal pattern of vision loss across injection visits further illustrates the advantage of early treatment. In the early cohort, the rate of ≥5-letter loss from baseline never exceeded 22% at any injection, and by the 10th injection only 8% of eyes had lost ≥5 letters. This low and declining rate suggests that any episodic vision loss in early-treated eyes was largely transient and recoverable, consistent with the observation that no early patient had sustained loss at landmark timepoints. In contrast, the late cohort exhibited a biphasic pattern: rates rose progressively to a peak of 62.5% at the 7th injection, coinciding with the period when their ability to extend treatment intervals beyond 8 weeks collapsed (from 62.2% at the 6th-7th cycle to 35.0% by the 9th–10th cycle). This temporal alignment supports a mechanistic link between incomplete disease control, recurrent exudation, and cumulative vision loss. Similar associations between fluid recurrence and visual instability have been reported in analyses by Chakravarthy et al.21
Beyond ophthalmology, preserving driving-eligible vision carries broader health economic benefits: visual impairment doubles fall risk, and AMD patients have a three-fold higher age-standardised incidence of falls, with falls costing the NHS an estimated £2.3 billion annually.22 The low NNTs (2–4) observed here suggest that early treatment strategies warrant inclusion in future cost-utility analyses that incorporate non-ocular morbidity.
Treat and Extend
Analysis of injection intervals revealed a biphasic pattern. Both groups achieved comparable intervals through the 6th-7th cycle (~11-12 weeks) but diverged thereafter. The early cohort sustained extension rates above 50% through all cycles, matching the durability reported in the TENAYA and LUCERNE trials.10 In contrast, the late cohort exhibited a biphasic collapse.
Interval-to-interval stability (relapse rates, mean interval changes) was similar between groups, indicating that delayed treatment does not produce a more “unstable” disease phenotype. Instead, the late cohort experienced a sustained inability to achieve progressive extension, a “durability ceiling” rather than episodic instability. This mechanistic insight aligns with the proposed durability-oriented framework for nAMD management, which prioritises engineering sustained disease quiescence over episodic short-term gains.11
Anatomical Outcomes and Fluid Resolution
Despite a baseline anatomical advantage favouring the late cohort (50.0% dry macula at presentation vs. 18.9% in the early cohort), complete convergence occurred by 18 months (100% vs. 96.7% dry). Importantly, the early cohort achieved this level of control faster (12 months vs. 18 months). At the end of follow-up, mean CMT decreased by 14.8% in the early cohort (to 239 µm) and by 27.6% in the late cohort (to 210 µm). This greater anatomical response in the late cohort, despite their functionally inferior outcomes, highlights a dissociation between structural and functional recovery, consistent with irreversible photoreceptor damage in delayed treatment.
Sustained fluid resolution is increasingly recognised as a critical determinant of long-term outcomes. A post-hoc analysis of the HAWK/HARRIER trials demonstrated that more fluid-free visits after loading were associated with superior visual acuity and retinal stability at 96 weeks.12 Our findings extend this observation by showing that early treatment initiation determines the likelihood of achieving sustained fluid quiescence. The bispecific mechanism of faricimab (VEGF-A/Ang-2 inhibition) likely enabled rapid drying, and this pharmacological advantage was maximised when initiated prior to irreversible anatomical remodelling.
Limitations
This study has several limitations that must be considered when interpreting the findings. First, the study’s design is non-randomised, single-centre, and has a modest sample size. Follow-up was limited to the tenth injection or 18 months for most patients; therefore, longer-term outcomes beyond this period, including fibrosis development, durability beyond two years, and the need for treatment switching, require further investigation. Second, the cohorts were not matched for age or baseline comorbidities. While we adjusted for available covariates, residual confounding cannot be excluded. Furthermore, patients with other macular pathologies (eg, retinal vein occlusion, diabetic macular oedema, etc.) were excluded to enhance internal validity, but limits generalisability beyond nAMD. Consequently, our cohort data and conclusions cannot be considered for those in which such pathologies commonly coexist. Third, we acknowledge substantial attrition over time, which may introduce bias if patients who discontinued follow-up differed systematically from those who remained. Similarly, there is potential selection bias in which patients were treated earlier versus later in the study period. Relatedly, the early and late treatment groups may differ systematically in ways directly linked to prognosis, follow-up behaviour, service access, or clinician treatment decisions. Fourth, the non-randomised design prevents causal inference. Patients treated earlier versus later likely differ in ways beyond simply the timing of treatment, which are still directly related to prognosis, clinician decision-making, or access to care. These systematic differences mean that any observed outcome differences may be due to baseline patient characteristics or treatment selection rather than to the timing of faricimab initiation itself. Our analysis cannot separate these effects; randomised trials or methods such as instrumental variable analysis would be required to support causal conclusions about treatment timing. Finally, the results of this study cannot be extrapolated to other anti-VEGF agents as only treatment-naïve (and therefore initiated on faricimab) patients were included.
In summary, while our findings provide useful real-world data on faricimab, they should be interpreted as hypothesis-generating. Future multi-centre, matched, or prospectively designed studies with broader inclusion criteria and longer follow-up are needed to confirm and extend these results.
Conclusion
The primary goal of nAMD therapy shifts depending on baseline BCVA, a proxy for disease status at initiation. Our study data demonstrates that the anti-VEGF agent, Faricimab, is effective at preserving good vision in nAMD patients when treated early. The delay in treatment allows for the development of an exudative process culminating in haemorrhage, scarring and fibrosis. Eyes with established disease likely display scarring and loss of RPE and photoreceptor cells.23 By delaying treatment until BCVA deteriorates to 0.6 logMAR, we may be missing a critical window in which therapy could preserve high-function vision and enable more flexible dosing. In an era of increasingly effective and durable agents like Faricimab, proactive rather than reactive treatment should be considered in patients with good baseline vision.
In conclusion, our real-world study confirms our hypothesis that NHS Wales’ standard practise of initiating anti-VEGF therapy, Faricimab, in nAMD patients at an earlier stage with good baseline vision (≤0.3 logMAR) successfully preserves visual function, achieves superior anatomical control and enables longer intervals between injections. The visual decline observed in a Late cohort underscores that the benefits of therapy are maximised when initiated early, prior to irreversible damage. These findings support a paradigm shift towards early intervention with high-efficacy agents to maintain long-term visual health and quality of life.
Ethical Considerations
This project was approved as an audit of current practice by the Clinical Audit Department at Swansea Bay University Health Board (SBUHB). The study was reviewed by the Joint Study Review Committee (JSRC) of SBUHB and Joint Clinical Research Facility (JCRF) at Swansea University and was formally ratified as non-research. As such, NHS Research Ethics Committee (REC) approval and a formal R&D application were not required; a permit / reference number is not given. All procedures were conducted in accordance with the principles of the Declaration of Helsinki. Patient confidentiality was strictly maintained, and all data were anonymised prior to analysis.
Acknowledgments
In line with STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Roche Products Ltd. supported with funding for the article submission charges by a hands-off grant. Roche Products Ltd. did not have any involvement in the preparation, drafting or editing of this manuscript or in the choice of authors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kulkarni AD, Kuppermann BD. Wet age-related macular degeneration. Adv Drug Deliv Rev. 2005;57(14):1994–15. doi:10.1016/J.ADDR.2005.09.003
2. Vyawahare H, Shinde P. Age-related macular degeneration: epidemiology, pathophysiology, diagnosis, and treatment. Cureus. 2022;14(9). doi:10.7759/CUREUS.29583
3. Kokotas H, Grigoriadou M, Petersen MB. Age-related macular degeneration: genetic and clinical findings. Clin Chem Lab Med. 2011;49(4):601–616. doi:10.1515/CCLM.2011.091/XML
4. Ferris FL, Fine SL, Hyman L. Age-related macular degeneration and blindness due to neovascular maculopathy. Arch Ophthalmol. 1984;102(11):1640–1642. doi:10.1001/ARCHOPHT.1984.01040031330019
5. Hernández-Zimbrón LF, Zamora-Alvarado R, Ochoa-De La Paz L, et al. Age-related macular degeneration: new paradigms for treatment and management of AMD. Oxid Med Cell Longev. 2018;2018. doi:10.1155/2018/8374647
6. Shahzad H, Mahmood S, McGee S, et al. Non-adherence and non-persistence to intravitreal anti-vascular endothelial growth factor (anti-VEGF) therapy: a systematic review and meta-analysis. Syst Rev. 2023;12(1):92. doi:10.1186/S13643-023-02261-X
7. Foss A, Haydock R, Childs M, et al. TANDEM TRIAL: a factorial randomised controlled trial of dose and review schedule of bevacizumab (Avastin) for neovascular macular degeneration in the East Midlands. BMJ Open Ophthalmol. 2020;5(1):588. doi:10.1136/BMJOPHTH-2020-000588
8. Hykin P, Prevost AT, Sivaprasad S, et al. Intravitreal ranibizumab versus aflibercept versus bevacizumab for macular oedema due to central retinal vein occlusion: the LEAVO non-inferiority three-arm RCT. Health Technol Assess. 2021;25(38):VII–111. doi:10.3310/HTA25380
9. Roche | vabysmo (faricimab-svoa). Available from: https://www.roche.com/solutions/pharma/productid-0a6b3497-d8a2-4a5f-a2d4-b0ffa5769fea.
10. Khanani AM, Kotecha A, Chang A, et al. TENAYA and LUCERNE: two-year results from the phase 3 neovascular age-related macular degeneration trials of faricimab with treat-and-extend dosing in year 2. Ophthalmology. 2024;131(8):914–926. doi:10.1016/j.ophtha.2024.02.014
11. Menna F, L DL, Meduri A, Baldascino A, Lupo S, Vingolo EM. New clinical trials and therapeutic advances with faricimab and aflibercept 8 mg in neovascular age-related macular degeneration: a durability-oriented comparative perspective. Biomedicines. 2026;14(4):773. doi:10.3390/BIOMEDICINES14040773
12. Dugel PU, Hillenkamp J, Sivaprasad S, et al. Baseline visual acuity strongly predicts visual acuity gain in patients with diabetic macular edema following anti-vascular endothelial growth factor treatment across trials. Clin Ophthalmol. 2016;10:1103. doi:10.2147/OPTH.S100764
13. Tufail A, Margaron P, Guerin T, Larsen M. Visual benefit versus visual gain: what is the effect of baseline covariants in the treatment arm relative to the control arm? A pooled analysis of ANCHOR and MARINA. Br J Ophthalmol. 2020;104(5):672–677. doi:10.1136/BJOPHTHALMOL-2018-313682
14. Recommendations | age-related macular degeneration | guidance | NICE. Available from: https://www.nice.org.uk/guidance/ng82/chapter/recommendations.
15. Rasmussen A, Fuchs J, Hansen LH, Larsen M, Sander B, Lund-Andersen H. Neovascular age-related macular degeneration: is it worthwhile treating an eye with poor visual acuity, if the visual acuity of the fellow eye is good? Eye. 2017;31(6):978. doi:10.1038/EYE.2016.324
16. Cymru L, Government W. All wales rehabilitation framework: principles to achieve a person-centred. 2022.
17. Relton SD, Chi GC, Lotery AJ, et al. Associations with baseline visual acuity in 12,414 eyes starting treatment for neovascular AMD. Eye. 2022;37(8):1652. doi:10.1038/S41433-022-02208-X
18. Modeste D, Stewart C, Premanandhan H, Awad MH, Williams GS. Evaluating faricimab in treatment-naive neovascular age related macular degeneration: a retrospective analysis of real-world data. Clin Ophthalmol. 2024;18:2821. doi:10.2147/OPTH.S468458
19. Armstrong RA. Statistical guidelines for the analysis of data obtained from one or both eyes. Ophthalmic Physiol Opt. 2013;33(1):7–14. doi:10.1111/OPO.12009
20. Driving eyesight rules - GOV.UK. Available from: https://www.gov.uk/driving-eyesight-rules.
21. Chakravarthy U, Havilio M, Syntosi A, et al. Impact of macular fluid volume fluctuations on visual acuity during anti-VEGF therapy in eyes with nAMD. Eye. 2021;35(11):2983. doi:10.1038/S41433-020-01354-4
22. Tsang JY, Wright A, Carr MJ, et al. Risk of falls and fractures in individuals with cataract, age-related macular degeneration, or glaucoma. JAMA Ophthalmol. 2024;142(2):96–106. doi:10.1001/JAMAOPHTHALMOL.2023.5858
23. Miller JW. Age-related macular degeneration revisited - piecing the puzzle: the LXIX edward Jackson memorial lecture. Am J Ophthalmol. 2013;155(1):1–35.e13. doi:10.1016/j.ajo.2012.10.018
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Short-Term Treatment Outcomes of Brolucizumab in Patients with Neovascular Age-Related Macular Degeneration: A Multicentre Indian Real-World Evidence Study
Chakraborty D, Thakkar M, Venkatesh R, Roy S, Bhavsar M, Karcher H
Clinical Ophthalmology 2023, 17:2295-2307
Published Date: 10 August 2023
Real-World Efficacy of Intravitreal Faricimab for Macular Edema Secondary to Retinal Vein Occlusion: Short-Term Outcomes and Optical Coherence Tomography Biomarker Analysis
Inokuchi S, Mizuki Y, Kamata A, Onishi J, Hayashi T, Mizuki N
Clinical Ophthalmology 2025, 19:3669-3679
Published Date: 4 October 2025