Back to Journals » Journal of Pain Research » Volume 19
Cervical Rotation-Traction Manipulation of Different Treatment Frequency in Cervical Radiculopathy: Study Protocol for a Randomized Controlled Trial
Authors Feng T ![]() , Wang X, Sun K, Yin H, Liu A
, Wang X, Sun K, Yin H, Liu A ![]() , Li Z, Li J, Zhu L, Wei X
, Li Z, Li J, Zhu L, Wei X ![]()
Received 15 June 2025
Accepted for publication 5 February 2026
Published 24 February 2026 Volume 2026:19 547284
DOI https://doi.org/10.2147/JPR.S547284
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Tianxiao Feng,1,* Xu Wang,1,* Kai Sun,1,2 He Yin,1,2 Aifeng Liu,3 Zhenhua Li,4 Jinyu Li,5 Liguo Zhu,1,2 Xu Wei1,2
1Orthopedics and Traumatology Department, Wangjing Hospital of China Academy of Chinese Medical Sciences, Beijing, 100102, People’s Republic of China; 2Beijing Key Laboratory of Orthopedics of Traditional Chinese Medicine, Wangjing Hospital of China Academy of Chinese Medical Sciences, Beijing, 100102, People’s Republic of China; 3Orthopedics and Traumatology Department, the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, 300381, People’s Republic of China; 4Orthopedics and Traumatology Department, Affiliated Hospital of Changchun University of Chinese Medicine, Changchun, 130012, People’s Republic of China; 5Orthopedics and Traumatology Department, Dongzhimen Hospital of Beijing University of Chinese Medicine, Beijing, 100700, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xu Wei, Orthopedics and Traumatology Department, Wangjing Hospital of China Academy of Chinese Medical Sciences, 6 South Central Ring Road, Chaoyang District, Beijing, 100102, People’s Republic of China, Tel +8613488716557, Email [email protected]
Purpose: Cervical radiculopathy (CR) poses a significant challenge due to its debilitating impact. Cervical rotation-traction manipulation (CRTM) is a representative manual therapy of traditional Chinese medicine (TCM) in China, which is beneficial to improve the pain, numbness, and dysfunction of CR patients. However, the optimal treatment frequency for CRTM remains systematically underexplored in randomized controlled trials (RCTs). This clinical study aims to assess the effectiveness and safety on three sessions per week of CRTM (TSWM) compared to one session per week of CRTM (OSWM) and cervical traction (CT) in patients with CR.
Patients and Methods: This multicenter, three-arm, prospective RCT is conducted at four hospitals in China. Participants will be randomly allocated in a 1:1:1 ratio to one of the TSWM group, OSWM group, or CT group through the central randomization system. All participants will receive 4-week treatment and 16-week follow-up (total 20 weeks). The primary outcome is pain intensity of neck and arm measured by the Visual Analog Scale (VAS) at week 4. The secondary outcomes include VAS for pain intensity, VAS for numbness intensity, Neck Disability Index (NDI), Short Form 12 (SF-12), the total cost, the recurrence rate, and Expectation of Treatment and Credibility Scale (ETCS). Adverse events (AEs) will be monitored and reported throughout the trial.
Conclusion: We expect this clinical study to evaluate the optimal frequency of CRTM for CR. It will also serve as a reference and exploration for investigating the dose–response relationship of manual therapy.
Trial Registration: This clinical trial was registered at ClinicalTrials.gov (registration number: NCT06320249) on March 15, 2024.
Keywords: cervical radiculopathy, cervical rotation-traction manipulation, treatment frequency, randomized controlled trial, study protocol
Introduction
As a disabling musculoskeletal disease, cervical radiculopathy (CR) poses a significant challenge due to its debilitating impact, which imposes substantial healthcare and societal costs.1,2 It is reported that its age-adjusted annual incidence is 83.2 per 100,000 people, with higher rates in men (107.3) than women (63.5).3 As populations age, CR prevalence is projected to rapidly rise.4–6 Therefore, the evidence-based management strategies for CR patients have attracted considerable attention among researchers and patients.
Nonoperative measures are the first-line and initial treatment options for CR patients, and the majority of individuals report symptomatic improvement after a period of systematically nonsurgical intervention.7,8 The conservative therapies suggested by international clinical practice guidelines9–11 predominantly include nonsteroidal anti-inflammatory drugs, exercise therapy, patient education, manual therapy, cervical collar, and other physiotherapies. Among them, manual therapy constitutes a vital component of conservative treatment for patients with CR, frequently employed either independently or in conjunction with other therapeutic modalities. In China, based on different cultural backgrounds and healthcare policies, traditional Chinese medicine (TCM) manual therapy has developed various unique and effective manual techniques through thousands of years of clinical practice. Traditional Chinese Orthopedic Therapy was accorded prestigious national recognition as an intangible cultural treasure in 2006 (IX-6), underscoring its pivotal role as a frontline therapy for chronic musculoskeletal ailments.
Cervical rotation-traction manipulation (CRTM) is a representative physiotherapy of TCM orthopedic therapy. Previous scholars have conducted some researches elucidating its effectiveness and safety, exploring its mechanical characteristics, and probing its underlying biomechanisms.12–15 Studies have shown that CRTM outperforms cervical traction in relieving pain and dysfunction of CR patients16,17 and CRTM has also been suggested in the clinical practice guideline.18 However, on the premise that its clinical effect has been confirmed, the dose–effect relationship of the CRTM in the treatment of CR remains unclear. This has resulted in the absence of explicit dosage recommendations such as intervention frequency and duration in clinical practice guidelines.
The frequency of manipulation is a critical factor to influence study conclusion and may be related to cumulative effects. A Cochrane systematic review indicated that multiple sessions of cervical manipulation were superior to conventional medication for improving pain and function in patients with neck pain. However, a single session of cervical manipulation did not elicit clinically meaningful benefits.19 Previous studies also showed that clinical trials with negative results often had lower intervention frequencies20,21 compared to trials with positive results.22,23 CR patients often receive three sessions per week of manipulation or more16,17,23 in China, while patients have employed interventions once or twice weekly12,20,21 in many previous trials. The optimal frequency of manipulation remains unclear. Therefore, on the basis of previous clinical effect evaluation studies, we conducted the randomized controlled trial (RCT) of CR patients to compare the effectiveness and safety of three sessions per week of CRTM (TSWM) with one session per week of CRTM (OSWM).
Methods/Design
Study Design
This study outlines a protocol for a multicenter, three-arm, prospective RCT with 4 weeks of treatment and 16 weeks of follow-up for patients with CR. This study complies with the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of Wangjing Hospital, China Academy of Chinese Medical Sciences (WJEC-KT-2023-047-P002), and was registered at ClinicalTrials.gov (NCT06320249).24 This trial design will strictly follow the Statement and Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT)25 to ensure appropriate high-quality methodology and strict quality control (Supplementary Material 1). The trial flow chart and study schedule are shown in Figure 1 and Table 1.
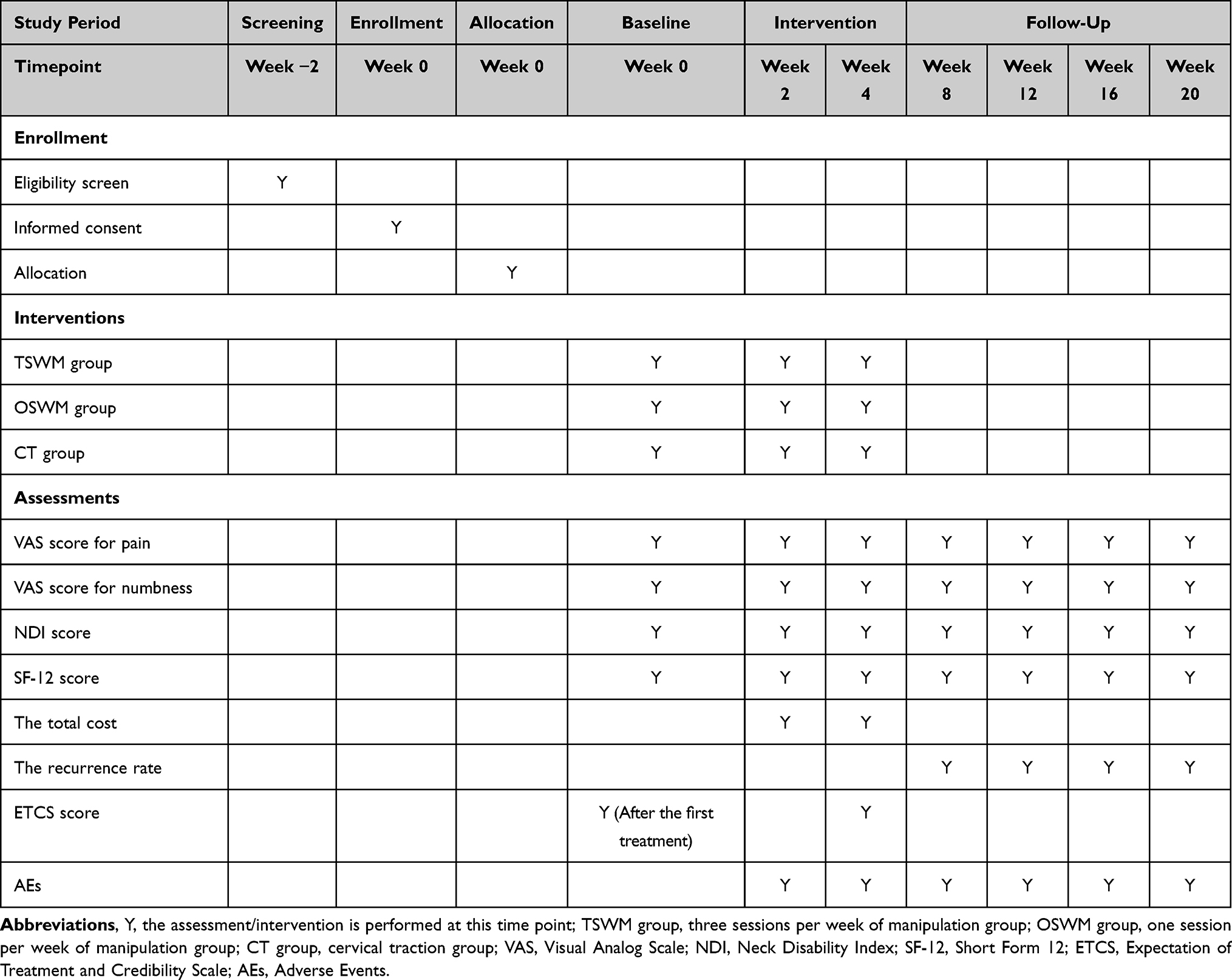 |
Table 1 The SPIRIT Schedule of Enrollment, Intervention and Assessments |
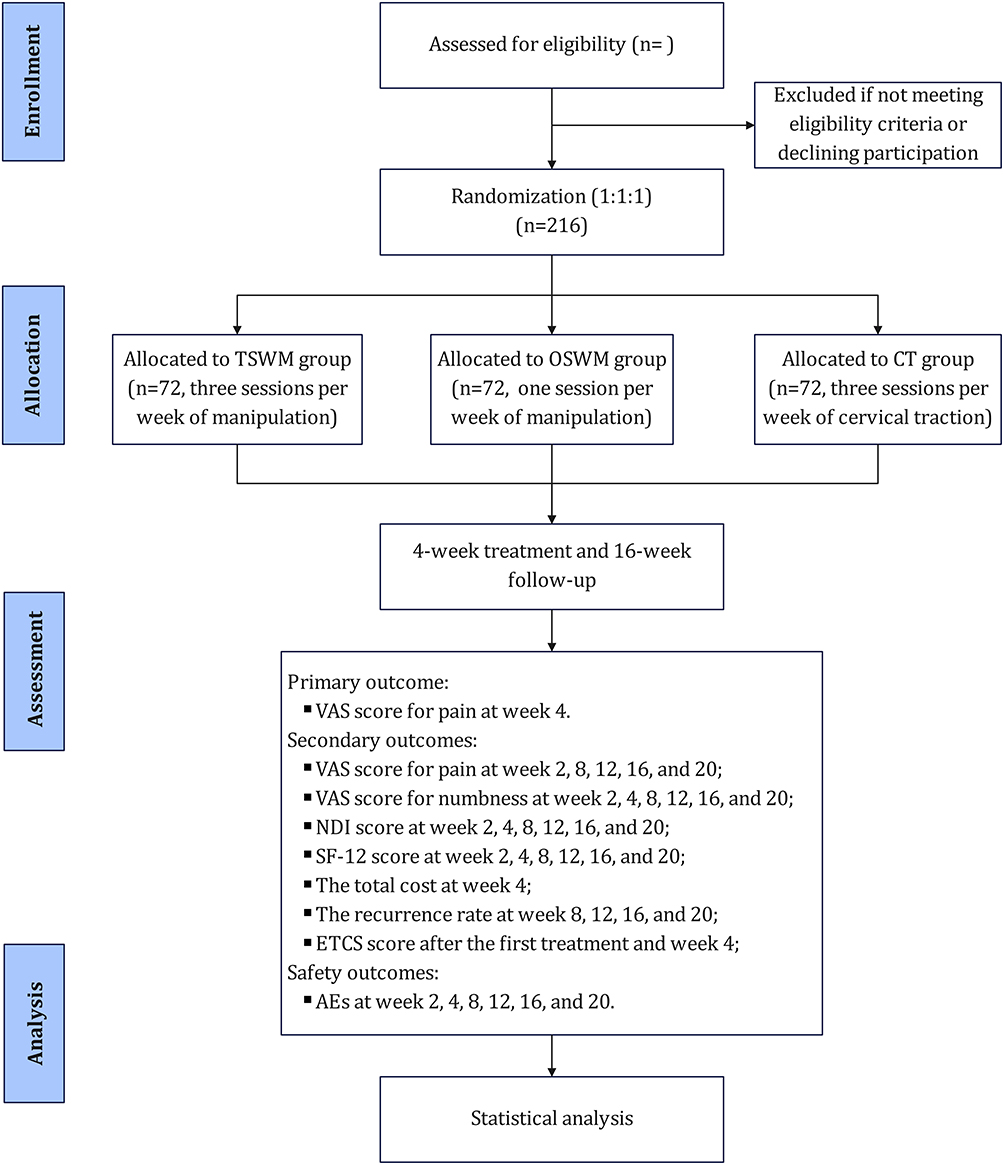 |
Figure 1 The trial flow chart. TSWM group: three sessions per week of manipulation group; OSWM group: one session per week of manipulation group; CT group: cervical traction group; VAS: Visual Analog Scale; NDI: Neck Disability Index; SF-12: Short Form 12; ETCS: Expectation of Treatment and Credibility Scale; AEs: Adverse Events. |
Participants
Diagnostic Criteria
Referring to the diagnostic criteria outlined in “An evidence-based clinical guideline for the diagnosis and treatment of cervical radiculopathy from degenerative disorders”.26 Diagnosis of CR requires alignment of patient symptoms, physical signs, and imaging findings, as outlined below: (1) Symptoms: Neck pain, stiffness, or pain radiating to the shoulder, scapular inner edge, or thoracic back. Characteristic symptoms include radiating pain and/or numbness in the upper limbs corresponding to the unilateral or bilateral distribution of cervical nerve root innervation areas. (2) Physical signs: Positive findings in the brachial plexus tension test and/or foraminal compression test. Affected nerve root distribution areas may exhibit sensory changes, muscle weakness, muscle atrophy, and diminished or absent tendon reflexes. (3) Imaging examination: X-ray or CT scans may reveal osteophyte formation or bone spur around the nerve roots due to cervical degenerative changes or manifestations of foraminal stenosis, or MRI scans may indicate nerve root compression. (4) Differential diagnosis: Exclusion of conditions primarily causing upper limb pain such as shoulder impingement syndrome, thoracic outlet syndrome, bicipital tendonitis, lateral epicondylitis, and carpal tunnel syndrome.
Inclusion Criteria
(1) Conforming to the diagnostic criteria above. (2) Aged 40–65 years. (3) VAS for pain intensity ≥4 points. (4) Disease duration ≤5 years.
Exclusion Criteria
(1) Combined with other types of cervical spondylosis. (2) Suspected or confirmed cases of cervical spine or intraspinal tumor, or intracranial tumor. (3) Patients with unclear diagnosis of spinal injury or symptoms of spinal cord injury. (4) Patients with developmental spinal canal stenosis (vertebral canal ratio = sagittal diameter of vertebral canal/sagittal diameter of vertebral body ≤ 0.75). (5) Those suffering from severe heart, lung, brain, liver, kidney, or hematopoietic system diseases. (6) Conditions such as spinal tuberculosis, osteomyelitis, and osteoporosis. (7) Individuals who have undergone cervical spine surgery and those with cervical spine deformities. (8) Pregnant, planning to become pregnant, or breastfeeding women. (9) Participants unable to complete this clinical study due to mental illness, cognitive, or emotional disorders. (10) Those who have participated in other clinical studies in the past 3 months.
Withdrawal Criteria
The following circumstances should be treated as withdrawals: (1) Participants who show poor compliance during the clinical trial, voluntarily withdraw from the study (Failure to complete ≥ 80% of the scheduled treatment sessions or interruption of treatment for more than 1 week without valid reasons). (2) Participants who experience severe adverse reactions, serious complications, or worsening conditions during the study including progressive worsening of neck pain with limb paralysis, acute cerebrovascular events, cervical fracture/dislocation, etc. (3) Participants whose treatment does not follow the protocol or whose observation data are incomplete and thus affect the assessment. (4) Participants who use other alternative treatments midway through implementing the treatment protocol.
Recruitment
The participants will be recruited across four hospitals in China, including Wangjing Hospital of China Academy of Chinese Medical Sciences, Affiliated Hospital of Changchun University of Chinese Medicine, Dongzhimen Hospital of Beijing University of Chinese Medicine, and First Teaching Hospital of Tianjin University of Traditional Chinese Medicine. The recruitment is mainly a combination form of online and offline methods through WeChat, advertisements, posters, and recruitment stations at outpatient units. Potential participants will receive detailed information about this trial, and complete doctors’ screening in the hospital based on inclusion and exclusion criteria to determine their eligibility. After checking that the eligibility criteria have been met, eligible participants will have an informed discussion with the trained researchers. Patients who have given informed consent form will be included in the study.
Randomization and Blinding
Participants will be randomly allocated in a 1:1:1 ratio to one of the three groups including TSWM group, OSWM group, and CT group through a central randomization system (Beijing Xinglin Zhicheng Technology Co, Ltd, Beijing, China) using stratified block randomization. The randomization sequence will be generated by an independent biostatistician who does not participate in the implementation or statistical analysis of this trial using SAS 9.3 software (SAS Institute, Cary, North Carolina, USA). Allocation will be performed by clinical research coordinator (CRC) who is not involved in treatment or assessment of this trial. The outcome assessors and statistical analysts are blinded to group assignment. The manual therapists and participants are not blinded because of the nature of intervention.
Interventions
Patients in the TSWM group will receive three sessions per week of CRTM, the OSWM group will undergo one session per week of CRTM, and the CT group will receive three sessions per week of cervical traction. All three groups will undergo 4-week treatment and 16-week follow-up. The procedures for CRTM and cervical traction are outlined as follows:
Cervical Rotation-Traction Manipulation
The key procedural points for CRTM are illustrated in Figure 2.27 Each session of CRTM will last approximately 10 to 15 minutes.
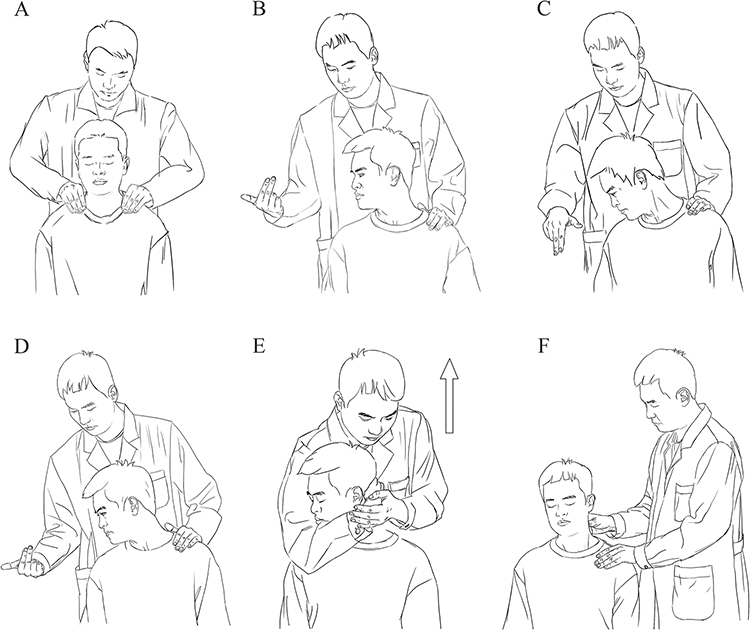 |
Figure 2 The procedure of Cervical rotation-traction manipulation. Upward arrow indicates the direction of the thrust force. (A) The patient sits in an upright position, with the neck and shoulder muscles relaxed naturally. The doctor applies massage techniques to relax the muscles around the neck area for approximately 5 to 10 minutes. (B-D) The patient is then instructed to rotate their head horizontally, flex it, and then rotate it again to its maximum limit while maintaining a sense of fixation. (E) The doctor supports the patient’s chin with their elbow and gently preloads upward for 3 to 5 seconds. The patient is then asked to fully relax, and the doctor applies a quick, short upward thrust with the elbow, which may result in audible sounds. (F) Subsequently, massage techniques are applied to further relax the muscles around the neck and shoulders. |
Cervical Traction
The procedures for cervical traction are as follows:28 The patient assumes a sitting position, and a cervical traction device with a chin strap is applied (LXZ-100E, Hangzhou Lixin Medical Equipment Co, Ltd, Zhejiang, China). The CR patient is instructed to slightly flex their head forward, approximately 10–15 degrees, based on their comfort level and symptom relief. The initial cervical traction weight starts at 3 kg and is gradually increased in increments of 0.5 kg. The maximum initial traction weight generally does not exceed 6 kg and can be further adjusted based on the patient’s tolerance. Typically, the traction weight can be maintained at 10% to 20% of the patient’s body weight. Each session of cervical traction will last approximately 10 to 15 minutes.
Outcomes
The Primary Outcome
The primary outcome is the Visual Analog Scale (VAS)29 for the neck and arm pain at week 4.
The Secondary Outcomes
The secondary outcomes include: The VAS for neck and upper limb pain at week 2, 8, 12, 16, and 20; The VAS for numbness30 at week 2, 4, 8, 12, 16, and 20; The Neck Disability Index (NDI)31 at week 2, 4, 8, 12, 16, and 20; The Short Form 12 (SF-12),32 which includes the Physical Component Summary (PCS) and the Mental Component Summary (MCS), will be assessed at week 2, 4, 8, 12, 16, and 20; The total cost at week 4: The total cost includes direct costs (registration fees, treatment fees and examination fees) and indirect costs (loss of income and transportation expenses). Record the total cost for each patient over a 4-week treatment period; The recurrence rate at week 8, 12, 16, and 20: The recurrence rate is defined as the percentage of individuals experiencing a reappearance of symptoms and signs similar to those before treatment during the follow-up period, among the total number of revisit CR patients; The Expectation of Treatment and Credibility Scale (ETCS)25 after the first treatment and week 4.
Safety Outcomes
Any adverse events (AEs) throughout this trial will be reported, and participants will be treated promptly and reasonably. Observing whether patients experience AEs such as progressive worsening of neck pain, upper limb pain, restricted neck movement, dizziness, palpitations, or serious adverse events during the study. Any AEs will be recorded diligently in the Adverse Event Record Sheet. When AEs occur, these will be reported to the relevant responsible entities and ethical committees for evaluation within 24 hours.
Sample Size
Based on the previous studies,16,34 it is anticipated that the mean pain VAS scores for patients of TSWM group, OSWM group, and CT group are 1.69, 2.45, and 3.06, respectively, with corresponding standard deviations of 1.39, 1.53, and 2.03 following a 4-week treatment period. Assuming a two-sided test with significance level of 5% and power of 80% based on an allocation ratio of 1:1:1, sample sizes of 57 per group were calculated using PASS 15 software (NCSS, LLC, Kaysville, Utah, USA). Considering the 20% dropout rate, each group will require 72 participants, totaling 216 participants.
Statistical Analysis
Statistical analyses will be performed using SPSS 26.0 software (IBM Corp., Armonk, New York, USA) and R (R Development Core Team, Vienna, Austria). Intent-to-treat analysis will be employed, with all patients included in their assigned groups receiving at least one treatment session. Missing data will be addressed using multiple imputation method. Statistical significance is set at a P value less than 0.05.
Continuous variables that conform to a normal distribution will be represented by the mean and standard deviation and variables that do not conform to a normal distribution will be represented by the median and interquartile range. Categorical variables will be described using frequencies or percentages. For primary and secondary outcomes, intervention effects will be analyzed using generalized estimating equations with baseline measurement as the covariates to account for correlation among repeated measurements. The group-by-time interaction, which indicated the difference for a given outcome between interventions overtime, will be considered our primary measure of intervention effects. Besides, the total cost and ETCS score will be examined by the One-Way ANOVA or Kruskal–Wallis test to explore differences between groups. Kruskal–Wallis test will be applied to the differences of the recurrence rate. For the safety outcomes, AEs will be analyzed by the Chi-square test or Fisher’s test. If it cannot run this analysis, we will perform descriptive analysis for presentation.
As an exploratory assessment to address potential clinical heterogeneity, predefined subgroup analyses will be conducted based on disease duration (acute less than 6 weeks, subacute 6–12 weeks, or greater than 12 weeks)10 and baseline pain intensity (moderate pain 4–6 points, severe pain 7–10 points via pain VAS score),29 using generalized estimating equations with the same covariates as the primary analysis, incorporating the interaction term (treatment group × subgroup factor × time) to test differential treatment effects (two-sided P < 0.05), and results will be presented with mean differences/relative risks and 95% confidence intervals, along with a forest plot for the primary outcome, without formal adjustment for multiple comparisons.
Data Collection and Management
The research data will be recorded on CRF initially, which will be reviewed and validated by statistical experts. Clinical Trial Electronic Data Capture System (EDC) will be applied in this trial, and the research data will be converted into the EDC system by trained and qualified investigators. If there are any uncertainties and doubts regarding the data in the EDC system, the data manager will issue an inquiry to the investigator to confirm its accuracy.
Quality Control
To ensure the successful process of this trial and the reliability of the conclusions, the clinicians directly involved in the study all hold a GCP training certificate and are trained in specific courses before the trial. Regarding intervention quality control, CRTM and cervical traction are conducted by clinicians with over 5 years of clinical experience in this field. In previous studies,35 we developed the CRTM teaching robot for researching, training, and promotion. Prior to the trial initiation, standardized CRTM operation training will be conducted. Manipulative therapists participating in this trial must pass a qualification assessment using the CRTM teaching robot. The unique feature of this robot-based training is its real-time quantification of mechanical parameters during the manipulative operation process, feedback on procedural issues, and continuous adjustment of techniques. This approach enables rapid mastery of essential technical elements (such as force magnitude, exertion timing, and direction), thereby promoting the standardization and normalization of CRTM procedures.
Discussion
The primary objective of patients with CR is to improve radicular pain, numbness, cervical dysfunction, and quality of life. CRTM has potentially beneficial effects on pain, cervical function, and quality of life. Several biomechanical studies have explored the potential mechanisms of CRTM. Wang et al12 found a significant decrease in cervical soft tissue tension in CR patients after CRTM treatment compared to before treatment using the soft tissue tension tester, and CRTM could balance the asymmetric tension between symptomatic and asymptomatic sides. An in vitro study13 showed that CRTM can significantly reduce the intradiscal pressure of intervertebral disc of human cervical spine specimens compared with cervical traction. When applying the MTS biomechanical tester to adjust thrust parameters, researchers found a discernible decrease in intradiscal pressure was observed with increasing thrust force. In addition, studies of three-dimensional finite element analysis (FEA) found that CRTM could significantly increase the area of the rotational contralateral intervertebral foramen, achieve physical decompression of the nerve roots,36 and improved the stress distribution of bilateral facet joint cartilage.37 In terms of the safety of CRTM, Zhu et al38 found that the motion ranges using the motion capture systems during CRTM were below the active range of motion reported in the literature. Furthermore, the study of FEA15 revealed that CRTM could maintain disc stress levels below the threshold for disc damage or fibrous annulus disruption, and thus demonstrated clinical safety.
In China, CRTM has gradually disseminated across many hospitals, universities, and research institutions, and this technique has garnered significant attention from medical professionals, researchers, and patient communities with the development and promotion of the CRTM teaching robot. Although the effect of the CRTM in the treatment of CR has been confirmed in previous studies, its optimal intervention frequency remains undetermined. This remains a common practical question for clinicians and patients, requiring clinical evidence to address. Based on this clinical question, we initiated the 20-week multicenter, three-arm RCT to investigate the effectiveness and safety on different frequencies of CRTM in the treatment of CR patients. In this trial, we will compare two commonly used intervention frequencies: TSWM and OSWM. Additionally, we incorporate cervical traction as the positive control, which is recommended by guidelines. All patients of three groups will receive 4-week intervention and 16-week follow-up period. For outcome measures, we select patient-reported VAS score as the primary outcome to reflect the pain intensity of CR patients. Meanwhile, the secondary outcomes mainly include the aspects of numbness, cervical function, quality of life, and recurrence rates. Furthermore, AEs throughout the 20-week trial period are comprehensively observed and documented, and health economic indicator such as the total cost during treatment is evaluated. Thus, we conduct a comprehensive assessment of the interventions across effectiveness, safety, and economic dimensions to explore the optimal frequency of CRTM for CR patients.
However, our trial has several limitations. First, the participants and manual therapists are not blinded. Due to the specific nature of the cervical manipulation and traction, it is difficult to implement blinding for both participants and manual therapists involved in the treatments, which may introduce some degree of subjective bias. In future trials, we will enhance the quality control to minimize subjective bias as much as possible. Second, we only use two common frequencies of manipulation, which seem not enough to explore the relationship between frequency and effect. Future studies may need more intervention strategies such as two or more than three sessions per week of manipulation to investigate the optimal frequency of CRTM for CR patients. Finally, the longer follow-up period has not been assessed. Further research should measure longer-term outcomes for different treatment frequencies of CRTM.
This trial will represent an important exploration of the dose–effect relationship in manual therapy, and provide clinical evidence to guide optimal frequency in treating CR with CRTM. The ultimate goal is to translate our findings into concrete recommendations to facilitate clinical choice in routine practice.
Acknowledgments
We would like to thank the anonymous reviewers for their helpful remarks. We thank the editor and the reviewers for their useful feedback.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Special Project on Evidence-based Clinical Research of Traditional Chinese Medicine in the High-level Traditional Chinese Medicine Hospital Construction Project of Wangjing Hospital, China Academy of Chinese Medical Sciences (grant number WJYY-XZKT-2023-05) and Cross Cooperation Project of Beijing Nova Program of Science and Technology (grant number 20220484228).
Disclosure
The authors declare that they have no competing interests.
References
1. Tampin B, Slater H, Briffa NK. Neuropathic pain components are common in patients with painful cervical radiculopathy, but not in patients with nonspecific neck-arm pain. Clin. J Pain. 2013;29(10):846–10.
2. Xie K, Wang Z. A predictive model for the risk of recurrence of cervical spondylotic radiculopathy after surgery. Pain Ther. 2023;12(6):1385–1396. doi:10.1007/s40122-023-00548-4
3. Radhakrishnan K, Litchy WJ, O’Fallon WM, Kurland LT. Epidemiology of cervical radiculopathy. A population-based study from Rochester, Minnesota, 1976 through 1990. Brain. 1994;117(2):325–335. doi:10.1093/brain/117.2.325
4. Buser Z, Ortega B, D’Oro A, et al. Spine degenerative conditions and their treatments: national trends in the United States of America. Global Spine J. 2018;8(1):57–67.
5. Cook C, Roman M, Stewart KM, Leithe LG, Isaacs R. Reliability and diagnostic accuracy of clinical special tests for myelopathy in patients seen for cervical dysfunction. J. Orthop Sports Phys Ther. 2009;39(3):172–178. doi:10.2519/jospt.2009.2938
6. Wei J, Yang K, Xue J, et al. Disease burden of neck pain in China from 1990 to 2021 and its prediction for 2042: the global burden of disease study 2021. J Pain Res. 2025;18:1975–1990. doi:10.2147/JPR.S516118
7. Woods BI, Hilibrand AS. Cervical radiculopathy: epidemiology, etiology, diagnosis, and treatment. J Spinal Disord Tech. 2015;28(5):E251–E259. doi:10.1097/BSD.0000000000000284
8. Thoomes EJ, Scholten-Peeters W, Koes B, Falla D, Verhagen AP. The effectiveness of conservative treatment for patients with cervical radiculopathy: a systematic review. Clin J Pain. 2013;29(12):1073–1086.
9. Kjaer P, Kongsted A, Hartvigsen J, et al. National clinical guidelines for non-surgical treatment of patients with recent onset neck pain or cervical radiculopathy. Eur Spine J. 2017;26(9):2242–2257.
10. Blanpied PR, Gross AR, Elliott JM, et al. Neck pain: revision 2017. J Orthop Sports Phys Ther. 2017;47(7):A1–A83. doi:10.2519/jospt.2017.0302
11. Expert Panel on Neurological Imaging, McDonald MA, Kirsch CFE, Amin BY, et al. ACR appropriateness criteria® cervical neck pain or cervical radiculopathy. J Am Coll Radiol. 2019;16(5):S57–S76. doi:10.1016/j.jacr.2019.02.023
12. Wang X, Jin Z, Feng T, et al. The immediate effect of cervical rotation-traction manipulation on cervical paravertebral soft tissue: a study using soft tissue tension cloud chart technology. BMC Musculoskelet Disord. 2024;25(1):184. doi:10.1186/s12891-024-07277-5
13. Han C, Feng M, Wen H, et al. Rotation-traction manipulation induced intradiskal pressure changes in cervical spine—an in vitro study. Front Bioeng Biotechnol. 2024;12:1322212. doi:10.3389/fbioe.2024.1322212
14. Lin D, He Z, Weng R, et al. Comparison of biomechanical parameters of two Chinese cervical spine rotation manipulations based on motion capture and finite element analysis. Front Bioeng Biotechnol. 2023;11:1195583. doi:10.3389/fbioe.2023.1195583
15. Huang X, Lin D, Liang Z, et al. Mechanical parameters and trajectory of two Chinese cervical manipulations compared by a motion capture system. Front Bioeng Biotechnol. 2021;9:714292. doi:10.3389/fbioe.2021.714292
16. Zhu LG, Yu J, Gao JH, et al. Observation of pain and numbness in patients with cervical radiculopathy. Chinese J Traditional Med Traumatol Orthopedics. 2009;17(4):1–3.
17. Zhu LG, Yu J, Gao JH, et al. The measurement for the range of motion of cervical spine and clinical significance. Chinese J Traditional Med Traumatol Orthopedics. 2008;16(1):1–5.
18. China Association of Chinese Medicine. Evidence-Based Practice Guideline of Traditional Chinese Medicine for Cervical Radiculopathy. China Standards Press; 2023.
19. Gross A, Langevin P, Burnie SJ, et al. Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. Cochrane Database Syst Rev. 2015;2015(9):CD004249. doi:10.1002/14651858.CD004249.pub4
20. Krauss J, Creighton D, Ely JD, Podlewska-Ely J. The immediate effects of upper thoracic translatoric spinal manipulation on cervical pain and range of motion: a randomized clinical trial. J Man Manip Ther. 2008;16(2):93–99. doi:10.1179/106698108790818530
21. Cassidy JD, Lopes AA, Yong-Hing K. The immediate effect of manipulation versus mobilization on pain and range of motion in the cervical spine: a randomized controlled trial. J Manipulative Physiol Ther. 1992;15(9):570–575.
22. Rodríguez-Sanz D, Calvo-Lobo C, Unda-Solano F, Sanz-Corbalán I, Romero-Morales C, López-López D. Cervical lateral glide neural mobilization is effective in treating cervicobrachial pain: a randomized waiting list controlled clinical trial. Pain Med. 2017;18(12):2492–2503. doi:10.1093/pm/pnx011
23. Cui X-J, Yao M, Ye X-L, et al. Shi-style cervical manipulations for cervical radiculopathy: a multicenter randomized-controlled clinical trial. Medicine. 2017;96(31):e7276. doi:10.1097/MD.0000000000007276
24. Wei X. Rotation-traction manipulation of different treatment frequency in cervical radiculopathy. ClinicalTrials.gov Identifier: NCT06320249. Accessed October 03, 2025.
25. Chan A-W, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–207. doi:10.7326/0003-4819-158-3-201302050-00583
26. Bono CM, Ghiselli G, Gilbert TJ, et al. North American Spine society. An evidence-based clinical guideline for the diagnosis and treatment of cervical radiculopathy from degenerative disorders. Spine J. 2011;11(1):64–72. doi:10.1016/j.spinee.2010.10.023
27. Feng T, Wang X, Bu H, et al. Cervical rotation-traction manipulation for cervical radiculopathy: a systematic review and meta-analysis of randomized control trials. J Pain Res. 2024;17:4055–4070. doi:10.2147/JPR.S481803
28. He SS, Fang FF. Expert consensus on traction treatment of cervical spondylosis. Chinese J Spine Spinal Cord. 2020;30(12):1136–1143.
29. Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17(1):45–56. doi:10.1016/0304-3959(83)90126-4
30. Zou T, Chen H, Wang P-C, Sun -H-H, Feng X-M. Predictive factors for residual leg numbness after decompression surgery for lumbar degenerative diseases. BMC Musculoskelet Disord. 2022;23(1):910. doi:10.1186/s12891-022-05848-y
31. Vernon H, Mior S. The neck disability index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14(7):409–415.
32. Ware JE, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
33. Devilly GJ, Borkovec TD. Psychometric properties of the credibility/expectancy questionnaire. J Behav Ther Exp Psychiatry. 2000;31(2):73–86. doi:10.1016/S0005-7916(00)00012-4
34. Wang Q, Zhu LG, Gao JH, et al. Clinical observation on rotation-traction manipulation for treatment of the cervicalspondylotic radiculopathy. J Traditional Chinese Orthopedics Traumatol. 2009;21(6):9–11.
35. Huang Y, Li S, Feng M, Zhu L. Cervical spine mechanism for reproduction of the biomechanical behaviours of the human neck during rotation-traction manipulation. Appl Bionics Biomech. 2017;2017:5829048. doi:10.1155/2017/5829048
36. Wang X, Wang HM, Chen SH, et al. Stress and morphological characteristics of intervertebral foramen of cervical rotation-traction manipulation for treating cervical spondylotic radiculopathy: a three-dimensional finite element analysis. Chin J Tissue Eng Res. 2025;29(03):441–447.
37. Bu HM, Wang X, TX F, Wang P, Zhu LG, Wei X. Influence of rotation-traction manipulation on articular cartilage stress of cervical facet under different conditions. Chinese J Traditional Med Traumatol Orthopedics. 2024;32(03):35–39+44.
38. Liguo Z, Minshan F, Xunlu Y, Shangquan W, Jie J, Vemulpad S. Kinematics analysis of cervical rotation-traction manipulation measured by a motion capture system. Evid Based Complement Alternat Med. 2017;2017(1):5293916. doi:10.1155/2017/5293916
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.