Back to Journals » International Medical Case Reports Journal » Volume 19
Case Report on Gastrointestinal Basidiobolomycosis Mimicking Inflammatory Bowel Disease: Insights and Review of Saudi Literature
Authors Garatli S, Alharbi H ![]() , Alghamdi GS, Zaidi ARZ
, Alghamdi GS, Zaidi ARZ ![]() , AlSheef M
, AlSheef M ![]()
Received 30 September 2025
Accepted for publication 5 June 2026
Published 14 July 2026 Volume 2026:19 569596
DOI https://doi.org/10.2147/IMCRJ.S569596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Sarah Garatli,1 Hatem Alharbi,2 Ghada Sulaiman Alghamdi,1 Abdul Rehman Zia Zaidi,3 Mohammed AlSheef1,2
1College of Medicine, Alfaisal University, Riyadh, Saudi Arabia; 2Department of Medical Specialties, King Fahad Medical City, Riyadh, Saudi Arabia; 3Department of Family and Community Medicine, College of Medicine, Alfaisal University, Riyadh, Saudi Arabia
Correspondence: Mohammed AlSheef, Department of Medical Specialties, King Fahad Medical City, Riyadh, Saudi Arabia, Email [email protected]
Abstract: Gastrointestinal basidiobolomycosis (GIB) is a rare invasive fungal infection of immunocompetent hosts that is endemic to Saudi Arabia and the wider Gulf region. Its presentation overlaps with inflammatory bowel disease (IBD), intestinal tuberculosis and malignancy, and many patients reach a definitive diagnosis only after surgery. We report a 39-year-old Saudi woman who presented with a 7-day history of right lower quadrant pain and non-bloody watery diarrhea. Initial bloods showed an elevated C-reactive protein of 21.5 mg/L, an erythrocyte sedimentation rate of 44 mm/hour and an absolute eosinophil count of 0.54 × 103/µL. Contrast-enhanced computed tomography (CT) demonstrated segmental wall thickening of the terminal ileum, cecum and proximal transverse colon, with a 3× 5 cm intramural cecal collection. Colonoscopy revealed ulcerated congested mucosa and an ileocecal stricture; targeted biopsies showed an eosinophil-rich granulomatous inflammation with broad, sparsely septate fungal hyphae demonstrating the Splendore–Hoeppli phenomenon, positive on Grocott methenamine silver and periodic acid–Schiff stains; and tissue culture grew Basidiobolus spp. Interventional radiology and surgical drainage were considered but were technically not feasible because of the intramural location, so the patient was managed medically with oral itraconazole at 200 mg every 8 hours for 3 days followed by 200 mg once daily, with monthly liver enzyme monitoring. Surgery was avoided. A repeat CT scan at 2 months showed near complete resolution of wall thickening, and follow-up colonoscopy at 5 months was normal. The patient self-discontinued itraconazole at 9 months because of symptom resolution and remained asymptomatic at follow-up 2 months later. Clinicians working in endemic regions should consider GIB in any patient with an ileocecal mass or abscess, eosinophilia and an IBD-like presentation, because early biopsy with fungal stains and prompt azole therapy can avert surgery.
Keywords: gastrointestinal basidiobolomycosis, fungal infection, immunocompetent, itraconazole, case report, Saudi Arabia, inflammatory bowel disease mimicker, Basidiobolus
Introduction
Basidiobolus ranarum is a saprophytic fungus of the order Entomophthorales that lives in soil, decaying plant matter, and the gastrointestinal contents of amphibians, reptiles and insectivorous bats.1 Human infection most commonly takes the form of a chronic subcutaneous mycosis of the limbs or trunk in healthy hosts in tropical and subtropical regions. Gastrointestinal involvement is rare but increasingly recognized, with Saudi Arabia and the southwestern USA accounting for most reported cases worldwide.2,3 Within Saudi Arabia, the southern Jazan and Asir regions remain the principal endemic foci, although adult cases from the central region around Riyadh are now well documented.2,4,5
The clinical phenotype of gastrointestinal basidiobolomycosis (GIB) is what makes it so often misread on first encounter. Patients typically present with right lower quadrant abdominal pain, a palpable or radiographically defined ileocecal mass, peripheral eosinophilia and elevated inflammatory markers. The radiological appearance of segmental bowel wall thickening with a localized mural collection further overlaps with Crohn’s disease, intestinal tuberculosis and ileocecal malignancy. In the 2001 Arizona case–control study by Lyon et al,6 longer Arizona residence and ranitidine use were the two exposures most strongly associated with GIB, with reported odds ratios of approximately 6.0 for ranitidine and 2.1 for each additional 20 years of smoking, although the small sample limits precision.6 The 2012 Mayo Clinic series by Vikram et al confirmed the surgical and antifungal management pattern and documented mortality of around 36% when diagnosis was delayed.7
These aspects matter for everyday gastroenterology practice because GIB sits inside a wider differential of inflammatory bowel disease (IBD) mimickers that clinicians in endemic regions must actively rule in or out before starting immunosuppression. Other infectious mimics include intestinal and hepatobiliary tuberculosis, which can produce identical ileocecal masses, biliary strictures and weight-loss patterns;8 endemic mycoses such as paracoccidioidomycosis, which has been reported to mimic IBD with right lower quadrant ileitis and granulomatous histopathology;9 and gastrointestinal histoplasmosis. Non-infectious mimics include drug-induced colitis, exemplified by sodium polystyrene sulfonate, mycophenolate mofetil and immune checkpoint inhibitor colitis, which can reproduce both the endoscopic and histological appearance of IBD;10 vasculitides such as eosinophilic granulomatosis with polyangiitis; and rare neoplasms such as indolent T-cell lymphoproliferative disorder of the gut.11 Misdiagnosis carries real cost: empirical corticosteroids or biologics for presumed Crohn’s disease can accelerate untreated fungal or mycobacterial disease and have been associated with disseminated infection and death.11
We describe a Saudi woman with cecal GIB whose presentation mimicked Crohn’s disease and intestinal tuberculosis. Source control by interventional radiology and surgery was attempted but not feasible because of the intramural anatomy of the collection. The patient was treated medically with itraconazole; she achieved radiological and endoscopic remission, and surgery was avoided. We also summarize the published Saudi adult and pediatric GIB literature and discuss how this case fits the IBD mimicker framework.
Case Report
A 39-year-old Saudi woman, known to have polyarteritis nodosa (not on treatment) and a history of smoking, as well as a history of liposuction, laparoscopic cholecystectomy and uncomplicated open ventral hernia repair, was referred from a private community hospital with a 7-day history of cramping right lower quadrant abdominal pain and watery non-bloody diarrhea. She denied fever, weight loss, night sweats, vomiting, cough or known tuberculosis contact, and reported no recent antibiotic or proton pump inhibitor use.
On arrival at our tertiary center she was alert, afebrile (37.0°C), normotensive (blood pressure 122/74 mmHg) and tachycardic, at 96 beats per minute. The abdomen was soft, with a tender, ill-defined mass in the right iliac fossa and no peritoneal signs. A faint reticulated rash on the lower limbs was noted, consistent with her known background of polyarteritis nodosa. Initial laboratory results from the referring hospital showed an ESR of 37 mm/hour and a CRP of 38.1 mg/L. The results of repeat laboratory testing at our center are shown in Table 1; the absolute eosinophil count was 0.54×103/µL (above the upper reference limit), with mild lymphopenia, an ESR of 44 mm/hour and a CRP of 21.5 mg/L. Liver and renal panels, serum albumin and glycosylated hemoglobin (HbA1c) were within normal limits. Stool studies for ova, cysts and parasites, Clostridioides difficile toxin and routine bacterial pathogens were negative. QuantiFERON TB Gold was negative, and screening for HIV, hepatitis B and hepatitis C was negative.
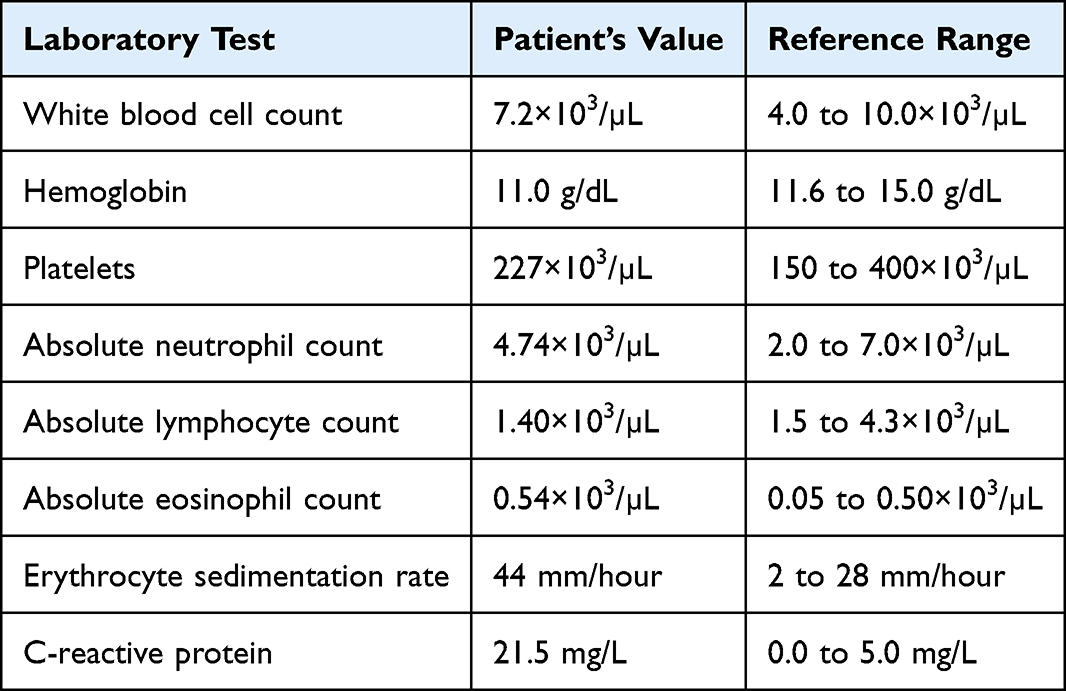 |
Table 1 Initial Laboratory Investigations at Presentation to the Tertiary Center |
A contrast-enhanced computed tomography (CT) scan of the abdomen and pelvis (Figure 1A) demonstrated long-segment circumferential wall thickening of the terminal ileum, cecum, and ascending and proximal transverse colon, with surrounding mesenteric fat stranding, free pelvic fluid and mesenteric lymphadenopathy. Within the cecum, there was a 3×5 cm intramural fluid collection consistent with an abscess (Figure 1B), without luminal obstruction or pneumoperitoneum.
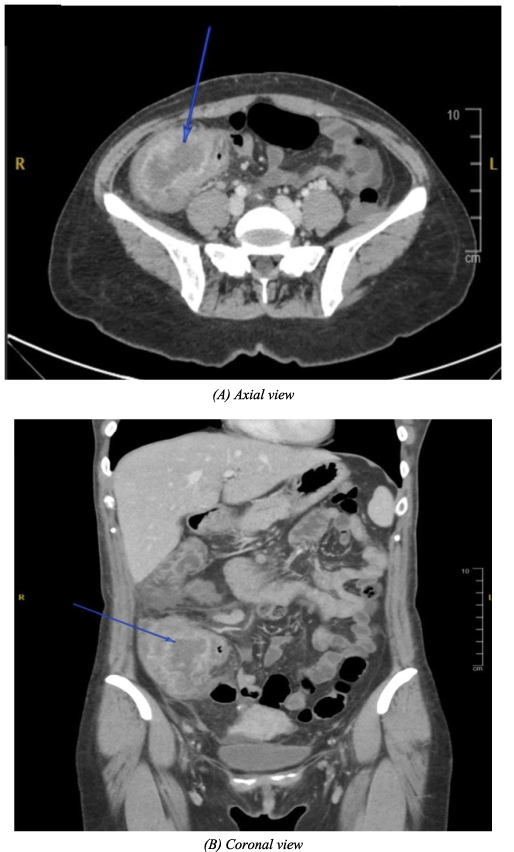 |
Figure 1 Contrast-enhanced computed tomography of the abdomen at presentation. (A) Axial image showing right body segmental circumferential wall thickening of the terminal ileum (blue arrow indicates the thickened segment). (B) Coronal image showing a 3×5 cm right body intramural fluid collection within the cecal wall (blue arrow indicates the collection). |
She was admitted for inpatient evaluation and continued on intravenous piperacillin tazobactam and metronidazole started at the referring hospital, along with intravenous metoclopramide and oral omeprazole for symptom control. The clinical differential at this point was Crohn’s disease with a phlegmon, ileocecal tuberculosis and a perforated cecal neoplasm. Colonoscopy on day 2 of admission revealed a localized area of severely congested, inflamed and ulcerated mucosa in the cecum, with a tight non-traversable stricture at the ileocecal valve (Figure 2). Multiple biopsies were taken from the cecal ulcers and the structured ileocecal valve.
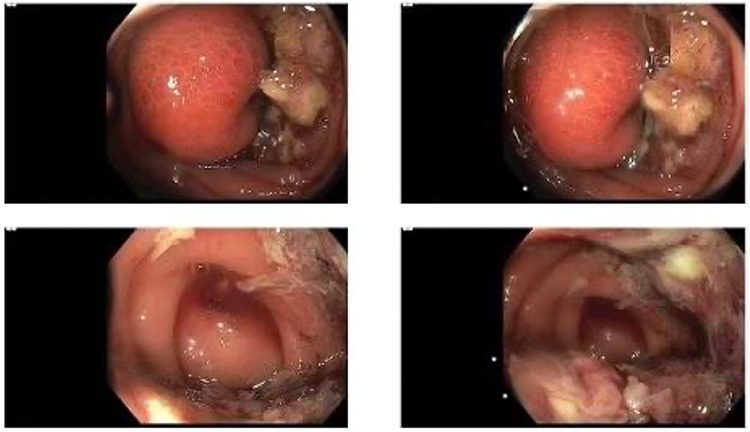 |
Figure 2 Colonoscopy at admission. Four representative images of the cecum showing a localized area of severely congested, inflamed and ulcerated mucosa with friable exudate, and a tight non-traversable stricture at the ileocecal valve. |
Histopathology, reviewed by two consultant gastrointestinal pathologists, demonstrated a dense eosinophil-rich inflammatory infiltrate of the colonic crypts and lamina propria, with crypt abscesses (Figure 3A) and broad, irregular, sparsely septate fungal hyphae with right-angled branching surrounded by eosinophilic material consistent with the Splendore–Hoeppli phenomenon (Figure 3B). The hyphae stained positively with Grocott methenamine silver (Figure 3C) and periodic acid–Schiff stains (Figure 3D). Tissue culture from the cecal biopsy grew Basidiobolus spp.; species-level identification was not performed because the genus-level diagnosis is sufficient to guide therapy and the laboratory did not have molecular identification on site. Acid-fast bacillus (AFB) stain and mycobacterial culture were negative on both biopsy and stool. Together with the negative QuantiFERON, this excluded intestinal tuberculosis; and the histopathological appearance, in particular the broad sparsely septate hyphae with right-angled branching and the Splendore–Hoeppli reaction, excluded paracoccidioidomycosis (which typically shows multiple budding ship-wheel yeasts on Grocott) and Crohn’s disease (which is characterized by non-caseating granulomas without fungal elements).9
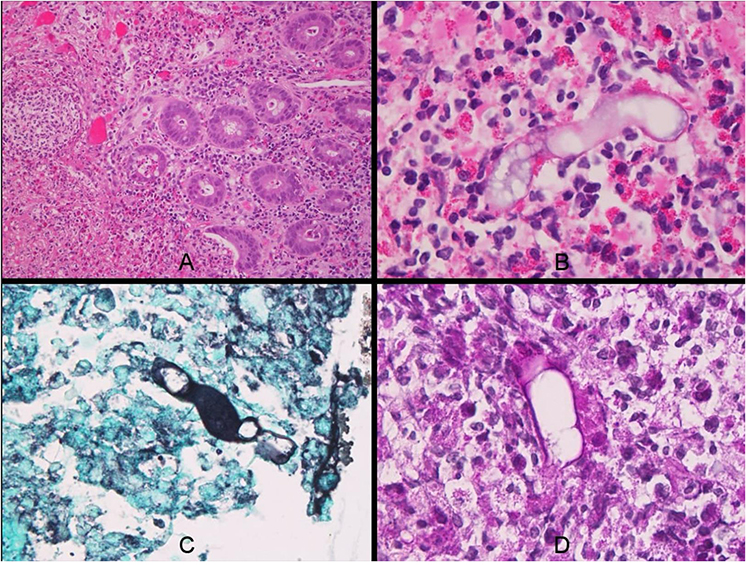 |
Figure 3 Histopathology of the cecal biopsy. (A) Dense eosinophilic infiltration of the colonic crypts and lamina propria (hematoxylin and eosin, original magnification 100×). (B) Broad, irregular, sparsely septate fungal hyphae with right-angled branching, surrounded by eosinophilic Splendore–Hoeppli material (hematoxylin and eosin, 400×). (C) Positive staining of the fungal hyphae with Grocott methenamine silver (400×). (D) Positive staining of the fungal hyphae with periodic acid–Schiff (400×). |
Interventional radiology and colorectal surgery were consulted to consider source control. Percutaneous CT-guided drainage was deemed not feasible because the collection was contained within the bowel wall itself rather than in a separate accessible cavity, and any percutaneous tract would have crossed normal bowel, with a high risk of enterocutaneous fistulization or perforation, an established limitation of intramural abscess drainage. Surgical drainage would, in effect, have required right hemicolectomy, which the patient preferred to defer pending a trial of medical therapy.
Oral itraconazole was started at 200 mg every 8 hours for the first 3 days as a loading regimen, followed by 200 mg once daily as maintenance therapy. Itraconazole was selected over voriconazole because of its established Saudi case experience in GIB,2,4,12 its reasonable activity against Entomophthorales and a more favorable side-effect profile for prolonged use. The patient was counseled on the importance of taking the capsule with food and an acidic beverage to maximize absorption, and the existing omeprazole was discontinued. Liver function tests were monitored at baseline, week 2, week 4 and monthly thereafter, and remained within normal limits throughout. Routine therapeutic drug monitoring of itraconazole trough levels was not available at our institution; the decision to continue therapy was based on clinical and radiological response. The patient was reviewed in the colorectal surgery clinic with a planned repeat CT at 2 months and repeat colonoscopy at 5 months, with surgical resection held in reserve as a rescue strategy.
A follow-up CT at 2 months showed near-complete resolution of the wall thickening in the terminal ileum, cecum and ascending colon, and resolution of the intramural collection. Follow-up colonoscopy at 5 months showed a normal cecum and a healed ileocecal valve. The patient was advised to complete a 12-month course of itraconazole but elected to self-discontinue at 9 months citing full symptom resolution and a preference to stop chronic medication. A telephone follow up at 2 months after discontinuation confirmed that she remained asymptomatic; she was discharged from clinic with instructions to return for repeat imaging and inflammatory markers if symptoms recurred.
Discussion
This case anchors three teaching points for clinicians who care for patients with IBD-like presentations in endemic regions. First, GIB can be successfully managed with antifungal therapy alone when surgical or percutaneous source control is not feasible. Second, a structured exclusion of other IBD mimickers, in particular intestinal tuberculosis, is essential before any immunosuppression is started. Third, intramural collections behave differently to free pericolic abscesses, both in terms of drainability and in terms of the antifungal response that can be expected.
The Saudi GIB literature was reviewed by searching PubMed and Google Scholar on 14 November 2025 using the terms basidiobolomycosis, Basidiobolus, Saudi Arabia and gastrointestinal, with no date restriction, supplemented by hand searching the reference lists of included articles. Reports describing adult or pediatric patients with histopathologically or microbiologically confirmed GIB diagnosed in Saudi Arabia were eligible, and we extracted age, sex, presenting symptoms, eosinophilia status, primary anatomical site, treatment and outcome. The accumulated Saudi experience is summarized in Table 2. Recurring features across these reports include male predominance (particularly in pediatric cases from the Jazan region), right lower quadrant abdominal pain, palpable abdominal mass, peripheral eosinophilia in the majority of cases, elevated ESR and CRP, and an ileocecal site of disease.2,4,5,12–14 The most recent bicentric retrospective series from Jazan and Riyadh, by Dhayhi et al in 2025, reported 42 pediatric cases over a 12-year period, and confirmed the persistent male predominance and the central role of itraconazole- or voriconazole-based regimens.15 Most adult Saudi cases have undergone surgical resection at diagnosis, but a small number have been managed medically without operation, including the 2025 report by Alsulaimi et al of a 32-year-old Saudi man with ileocecal GIB treated successfully with antifungal therapy alone.14 Our patient adds to this small but growing experience of medical management.
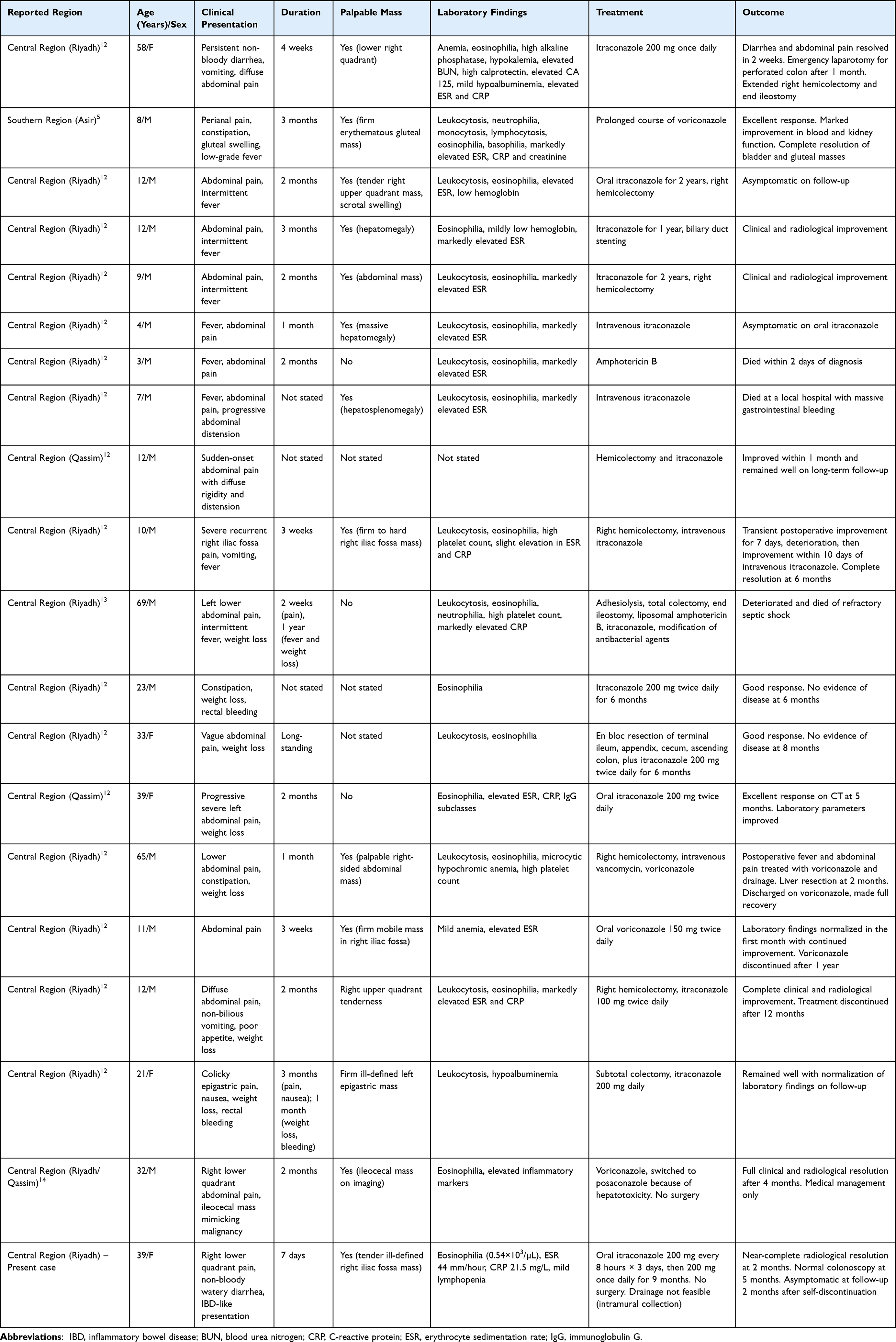 |
Table 2 Summary of Published Saudi Reports of Gastrointestinal Basidiobolomycosis |
Eosinophilia is one of the most consistent laboratories clues and was the feature that prompted us to broaden the differential beyond Crohn’s disease. Across the largest published series, peripheral eosinophilia is reported in approximately 85% of cases.3,5 In our patient, the absolute eosinophil count of 0.54×103/µL was modestly elevated above the upper reference limit, in keeping with this pattern, and tissue eosinophilia was the dominant histopathological feature. Eosinophilia is not specific, however, and overlaps with eosinophilic gastroenteritis, parasitic infection (Strongyloides in particular), eosinophilic granulomatosis with polyangiitis and hypereosinophilic syndrome, all of which were considered and excluded in our patient through stool studies, vasculitis serology and clinical evaluation.
Intestinal tuberculosis is the single most important diagnostic competitor in this clinical setting. Caseating granulomas with central necrosis and AFB-positive bacilli on biopsy distinguish tuberculosis from GIB, and a structured workup with QuantiFERON or T SPOT.TB testing, mycobacterial culture and AFB staining of biopsy material is mandatory. In our patient, QuantiFERON was negative, AFB staining was negative, mycobacterial culture grew no organisms after 6 weeks, and histopathology showed broad sparsely septate hyphae with the Splendore–Hoeppli phenomenon rather than caseating granulomas. The diagnostic overlap between intestinal and hepatobiliary tuberculosis and other infectious mimickers has been thoroughly reviewed by Esguerra-Paculan and Soldera, who emphasize that histological demonstration of Mycobacterium tuberculosis is the definitive diagnostic step.8 Paracoccidioidomycosis was also considered because it can present with right lower quadrant ileitis and granulomatous histopathology in immunocompetent hosts, although it is essentially restricted to Latin America and is morphologically distinguishable by its multiple budding yeast forms on Grocott stain.9 Drug-induced colitis from sodium polystyrene sulfonate, mycophenolate or checkpoint inhibitors was considered and excluded by medication history.10 Polyarteritis nodosa, which our patient carried as a background diagnosis, can itself cause gastrointestinal ischemia and ulceration that may mimic Crohn’s disease,11 but the absence of mesenteric arterial findings on CT, the absence of systemic flare and the presence of fungal hyphae on biopsy made this an unlikely contributor to the colonic lesion. A 2025 narrative review by Bakkaloğlu and Çelik provides a useful framework for systematically working through these IBD mimickers in clinical practice.11
The decision to manage this patient medically rather than surgically was driven by the intramural nature of the collection. Free pericolic or pelvic abscesses larger than 3–4 cm are typically drained percutaneously under CT or ultrasound guidance, with success rates above 80%, but collections contained entirely within the bowel wall are not readily accessible without traversing healthy bowel and risking perforation or fistula formation. For this anatomical subset, antibiotic and antifungal management with close radiological follow-up, or formal bowel resection, are the two principal options. Itraconazole was selected over voriconazole because the published Saudi adult experience with itraconazole-based regimens has been favorable,2,4,12 and because voriconazole carries a higher risk of hepatotoxicity, visual disturbance and skin photosensitivity during prolonged use.13 Liver function tests were monitored monthly and remained normal. Therapeutic drug monitoring of itraconazole trough levels is recommended in international guidance for invasive fungal infection because of variable oral absorption, although it was not available at our institution; the clinical and radiological response served as a pragmatic substitute. The optimal duration of therapy in GIB is uncertain, and has ranged from 6 to 12 months in published Saudi and international series.3,4,12 Our patient adhered to 9 months of therapy and remained well at short-term follow-up; longer follow-up would be needed to confirm durable remission.
Limitations
This report has several limitations. As a single case, it cannot support generalizable conclusions about medical management of intramural GIB collections. Species-level identification of the Basidiobolus isolate was not performed, so we cannot confirm Basidiobolus ranarum as the causative species, and the diagnosis rests on the genus-level culture together with the characteristic histopathology. Source control by drainage was not achieved, which complicates any direct comparison with the standard surgical literature. Treatment duration was 9 months rather than the planned 12 months, and follow-up after discontinuation has so far been limited to 2 months, so the possibility of late relapse cannot be excluded. Finally, the risk factor odds ratios mentioned in the Introduction are taken from a small case–control study with wide confidence intervals,5 and should be interpreted as hypothesis generating rather than as established causation.
Conclusion
In endemic regions, an IBD-like presentation with right lower quadrant pain, an ileocecal mass or abscess on imaging and peripheral eosinophilia should prompt early endoscopic biopsy with fungal stains and culture, and a structured exclusion of intestinal tuberculosis, paracoccidioidomycosis and drug-induced colitis before any immunosuppressive therapy is started. Early itraconazole-based antifungal therapy can avert surgery when source control is not technically feasible, as in our patient with an intramural cecal collection. The optimal duration of antifungal therapy in GIB remains uncertain, and a structured follow-up plan with symptom-triggered repeat imaging and inflammatory markers is advisable after treatment discontinuation.
Data Sharing Statement
The data and materials supporting this case report are available upon request from the corresponding author.
Ethical Approval and Consent for Publication
Institutional approval to publish the case details was obtained from the Institutional Review Board of King Fahad Medical City, Riyadh, Saudi Arabia (log number 24-582). Written informed consent for publication of the clinical details and accompanying images was obtained from the patient.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this paper.
References
1. Ribes JA, Vanover-Sams CL, Baker DJ. Zygomycetes in human disease. Clin Microbiol Rev. 2000;13(2):236–10. doi:10.1128/CMR.13.2.236
2. Nemenqani D, Yaqoob N, Khoja H, Al Saif O, Amra NK, Amr SS. Gastrointestinal basidiobolomycosis: an unusual fungal infection mimicking colon cancer. Arch Pathol Lab Med. 2009;133(12):1938–1942. doi:10.5858/133.12.1938
3. Pezzani MD, Di Cristo V, Parravicini C, et al. Gastrointestinal basidiobolomycosis: an emerging mycosis difficult to diagnose but curable. Case report and review of the literature. Travel Med Infect Dis. 2019;31:101378. doi:10.1016/j.tmaid.2019.01.013
4. Meeralam Y, Alsulami H, Aljoaid AM, et al. Basidiobolomycosis mimicking fistulizing Crohn’s disease: a case report from Saudi Arabia. Cureus. 2023;15(4):e37981. doi:10.7759/cureus.37981
5. Ghazwani SM, Arishi HM, Dhayhi NS, et al. Pediatric gastrointestinal basidiobolomycosis: a retrospective study from Jazan Province, Saudi Arabia. Infect Drug Resist. 2023;16:4667–4676. doi:10.2147/IDR.S416213
6. Lyon GM, Smilack JD, Komatsu KK, et al. Gastrointestinal basidiobolomycosis in Arizona: clinical and epidemiological characteristics and review of the literature. Clin Infect Dis. 2001;32(10):1448–1455. doi:10.1086/320161
7. Vikram HR, Smilack JD, Leighton JA, Crowell MD, De Petris G. Emergence of gastrointestinal basidiobolomycosis in the United States, with a review of worldwide cases. Clin Infect Dis. 2012;54(12):1685–1691. doi:10.1093/cid/cis250
8. Esguerra-Paculan MJA, Soldera J. Hepatobiliary tuberculosis in the developing world. World J Gastrointest Surg. 2023;15(10):2305–2319. doi:10.4240/wjgs.v15.i10.2305
9. da Cruz ER, Forno AD, Pacheco SA, et al. Intestinal paracoccidioidomycosis: case report and systematic review. Braz J Infect Dis. 2021;25(4):101605. doi:10.1016/j.bjid.2021.101605
10. Dos Santos FS, Aver GP, Paim TV, Riva F, Brambilla E, Soldera J. Sodium polystyrene sulfonate induced colitis. GE Port J Gastroenterol. 2023;30(2):153–155. doi:10.1159/000521195
11. Bakkaloğlu OK, Çelik AF. Differential diagnosis of inflammatory bowel disease. J Enterocolitis. 2025;4(Suppl 1):S20–S27. doi:10.14744/Jenterocolitis.2025.82883
12. Al Asmi MM, Faqeehi HY, Alshahrani DA, Al-Hussaini AA. A case of pediatric gastrointestinal basidiobolomycosis mimicking Crohn’s disease. A review of pediatric literature. Saudi Med J. 2013;34(10):1068–1072. doi:10.15537/1658-3175.5841
13. Alsaeed M, Mursi M, Bahloul A, et al. A rare case of fatal gastrointestinal basidiobolomycosis. IDCases. 2023;31:e01709. doi:10.1016/j.idcr.2023.e01709
14. Alsulaimi MS, Memon MY, Alyabary IM, et al. Ileocecal basidiobolomycosis mimicking malignancy successfully treated without surgery: a case report. World J Clin Cases. 2025;13(30):108566. doi:10.12998/wjcc.v13.i30.108566
15. Dhayhi NS, Aljarbou AZ, Alhazmi AH, et al. Pediatric gastrointestinal basidiobolomycosis: descriptive bicentric retrospective study. Sci Rep. 2025;15(1):27211. doi:10.1038/s41598-025-13098-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pediatric Gastrointestinal Basidiobolomycosis: A Retrospective Study from Jazan Province, Saudi Arabia
Ghazwani SM, Arishi HM, Dhayhi NS, Shami MO, Gosadi IM, Rajab M, Badedi M, Mobarki M, Alhazmi AH
Infection and Drug Resistance 2023, 16:4667-4676
Published Date: 18 July 2023
Challenges in Surgical Intervention for a Rare Case of Anterior Segment Dysgenesis: A Case Report
Aldawood A, Bakri S, Alotaibi B
International Medical Case Reports Journal 2023, 16:579-584
Published Date: 21 September 2023
Surgical Management and Antifungal Therapy for Extensive Eumycetoma of the Right Foot: A Case Report from Resource Limited Settings
Ali TA, Mahamud MA, Hassan SA, Abdullahi IM, Abdulkarim OM, Dhaqane AH, Mohamed AA, Siddig EE
International Medical Case Reports Journal 2026, 19:593386
Published Date: 10 March 2026
Gastrointestinal Basidiobolomycosis Mimicking Adhesive Bowel Disease and Ileocaecal Malignancy in an Adult HIV Patient: A Case Report Highlighting a Diagnostic Pitfall
Muhumuza J, Kato J, Wanda S, Matagala N, Kagimu A, Okuku MD
International Medical Case Reports Journal 2026, 19:611308
Published Date: 3 June 2026