Back to Journals » International Medical Case Reports Journal » Volume 19
Gastrointestinal Basidiobolomycosis Mimicking Adhesive Bowel Disease and Ileocaecal Malignancy in an Adult HIV Patient: A Case Report Highlighting a Diagnostic Pitfall
Authors Muhumuza J ![]() , Kato J, Wanda S, Matagala N, Kagimu A, Okuku MD
, Kato J, Wanda S, Matagala N, Kagimu A, Okuku MD
Received 23 March 2026
Accepted for publication 28 May 2026
Published 3 June 2026 Volume 2026:19 611308
DOI https://doi.org/10.2147/IMCRJ.S611308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xudong Zhu
Joshua Muhumuza,1,2 Joseph Kato,2 Steven Wanda,3 Noah Matagala,4 Anthony Kagimu,1,4 Maxwel Dancan Okuku1,4,5
1Department of Surgery, Kampala International University Western Campus, Bushenyi, Uganda; 2Department of surgery, Virika Hospital, Fortportal, Uganda; 3Department of Surgery, Kabarole Hospital, Fortportal, Uganda; 4Department of Surgery, Fortportal Regional Referral Hospital, Fortportal, Uganda; 5Department of surgery, Mountains of the Moon University, Fortportal, Uganda
Correspondence: Joshua Muhumuza, Department of surgery, Kampala International University Western Campus, PO. Box 70 Ishaka, Bushenyi, Uganda, Tel +256779223560, Email [email protected]
Introduction: Fungi cause gastrointestinal basidiobolomycosis (GIB). It often presents with features that are difficult to differentiate from other gastrointestinal disorders such as malignancy and inflammatory bowel disease. This results in a misdiagnosis and delayed initiation of appropriate treatment.
Case Presentation: We present a case of a 41-year-old female, who had been HIV positive for over 20 years on antiretroviral therapy. The patient presented with intestinal obstruction. She had experienced similar episodes over the preceding month and was managed conservatively but without complete resolution. The patient also had a history of abdominal surgery; however, the indications were unclear. Emergency laparotomy revealed a tumor-like mass at the ileocecal junction, suggestive of malignancy. Tumor resection with ileotransverse anastomosis plus adhesiolysis were performed. Histopathological examination revealed chronic granulomatous inflammation with eosinophilic infiltrates in addition to fungal spores, consistent with a gastrointestinal fungal infection. The postoperative course was complicated by surgical site infection and anemia. Following the histological diagnosis, itraconazole therapy was initiated, after which the surgical site infection rapidly improved.
Conclusion: Gastrointestinal basidiobolomycosis should be considered in patients presenting with recurrent intestinal obstruction and ileocecal masses, particularly when intraoperative findings mimic malignancy. In particular, among patients with previous surgery, gastrointestinal basidiobolomycosis should be considered among the differential diagnoses when patients present with features of intestinal obstruction, to avoid delayed intervention.
Keywords: basidiobolomycosis, fungal infection, adhesive bowel disease, ileocaecal malignancy, case report
Introduction
Gastrointestinal basidiobolomycosis (GIB) is an uncommon but increasingly recognized invasive fungal disease caused by the environmental species Basidiobolus, most frequently Basidiobolus ranarum.1 Gastrointestinal basidiobolomycosis remains an uncommon diagnosis, with literature dominated by case reports and small series. Hence, its true incidence remains unclear and is probably under-recognized, as the disease is frequently misdiagnosed as a gastrointestinal malignancy, inflammatory bowel disease, or other chronic gastrointestinal disorders.2,3
Although GIB has been reported worldwide, it appears to be more prevalent in tropical and subtropical regions including Africa and the Middle East.4 In the year 2020, a case series was published in Sudan, with all the cases having widely varying presentations and clinical diagnoses including colonic carcinoma, lymphoma, rectal mass, and appendicitis.5 Gastrointestinal basidiobolomycosis (GIB) primarily affects healthy individuals. Many cases are commonly observed in the pediatric and young adult populations.1 Clinically, it is characterized by vague abdominal complaints such as chronic abdominal pain accompanied by weight loss, nausea, vomiting, constipation, and a palpable abdominal mass.6
To the best of our knowledge, this is the first reported case of gastrointestinal basidiobolomycosis (GIB) in Uganda in the indexed literature. In this case, the symptoms of the immunocompromised patient initially mimicked adhesive bowel disease, causing a delay in diagnosis. Despite these challenges, the patient was managed successfully in a resource-limited setting. This work has been reported according to SCARE criteria.7
Case Presentation
A 41-year-old female living with an HIV infection and receiving antiretroviral therapy for over 20 years presented with abdominal pain, vomiting, abdominal distension, and an inability to pass stool. She had experienced six episodes of such symptoms within the preceding month; all were managed conservatively with some improvement, and the symptoms were thought to be due to adhesive bowel disease. This was mainly because the patient had a history of abdominal surgery. However, the time since surgery, indication, and operative findings from the previous surgery were unclear due to a lack of documentation.
On physical examination, the abdomen was distended, with hyperactive bowel sounds. The patient was diagnosed with acute intestinal obstruction. An erect abdominal radiograph revealed distended bowel loops centrally located with multiple air fluid levels, as commonly seen in small bowel obstruction due to adhesive bowel disease (Figure 1). Eosinophilia (4230 cells per microliter) and thrombocytosis (610,000 platelets per microlite) were noted on CBC. Hemoglobin was 12.5 g/dl, CD4 count, 1286 cells/µL; serum electrolytes, renal function tests, and liver function tests were unremarkable. Advanced imaging was not done, mainly due to the resource limitation coupled with the emergency nature of the case which made referral of the patient for more investigations not an appropriate option.
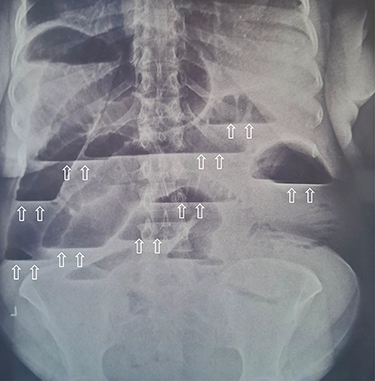 |
Figure 1 An erect abdominal Xray with distended bowel loops, centrally located with multiple air fluid levels (arrows). |
Conservative management was initiated, but this did not yield significant improvement, and emergency laparotomy was performed by a general surgeon. Intraoperatively, multiple intra-abdominal adhesions were found that were released, and a hard, irregular mass at the ileocecal junction with enlarged lymph nodes was identified. Resection was performed, followed by ileotransverse anastomosis. The specimen was sent for histopathological examination.
The postoperative period was complicated by surgical site infection and anemia requiring two blood transfusions. The wound was opened and managed with daily dressing. Histopathological examination with Hematoxylin and Eosin staining revealed chronic granulomatous inflammation with marked eosinophilic infiltration, microabscess formation, and fungal spores (Figure 2). The spores were eosinophilic, round to oval and located on the periphery of the abscess at the margin of the viable and dead tissues. All lymph nodes were reactive and no malignant changes were observed. No malignancies were identified. These findings were consistent with those of gastrointestinal basidiobolomycosis.
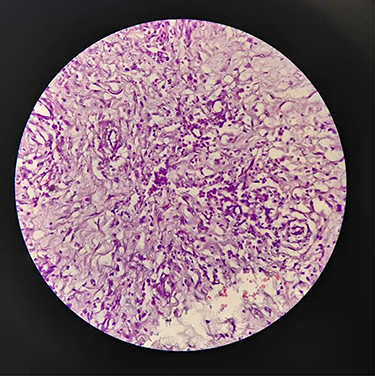 |
Figure 2 Histopathology section showing chronic granulomatous inflammation with marked eosinophilic infiltrates, micro-abscess formation and fungal spores using Hematoxylin and Eosin staining. |
Oral itraconazole therapy was initiated based on the histopathological results. Following the initiation of antifungal therapy, the surgical site infection began to improve rapidly, and wound healing accelerated (Figure 3). Secondary wound closure was then performed. It was thought that fungal infection could have contributed to the surgical site infection; however, this was not confirmed microbiologically. The patient recovered well, and was discharged. The patient was completely well, with no complaints 12 weeks post-surgery.
 |
Figure 3 Healing wound. |
Discussion
Gastrointestinal basidiobolomycosis (GIB) is a rare fungal infection caused by Basidiobolus ranarum, an environmental saprophyte that belongs to the order Entomophthorales.1 This organism is typically found in soil, decaying vegetation, and the gastrointestinal tract of amphibians and reptiles. Human infection is thought to occur through the ingestion of contaminated food or soil.1 Although basidiobolomycosis classically presents as a subcutaneous infection, gastrointestinal involvement is being increasingly recognized.2,3
Although GIB has been reported worldwide, it appears to be more prevalent in tropical and subtropical regions including Africa and the Middle East.4 In East Africa, fungal infections remain an under-recognized cause of abdominal pathology, particularly in resource-limited settings, where advanced microbiological and histopathological diagnostic facilities may not be readily available.8 Many resource-limited settings, such as Uganda, face challenges in diagnosing rare fungal infections. Thus, doctors rely on histological results that are usually obtained only after surgery.
Gastrointestinal basidiobolomycosis is believed to occur when fungal spores that subsequently invade the gastrointestinal wall are swallowed.1 Owing to the body’s immune system, inflammatory reactions often result in eosinophil infiltration, fibrosis, and abscess formation.9 This is evidenced by the eosinophilic infiltrate seen on histology in this patient, suggestive of an immune response to the fungus.9 This inflammatory reaction and fibrosis often result in the formation of a mass that can be confused with a malignant tumor as seen in six of the seven cases reported in the Sudanese case series.5
The typical presentation of GIB is nonspecific, with symptoms, such as abdominal pain, abdominal mass, weight loss, fever, and clinical features suggestive of intestinal obstruction.6 The patient presented with recurrent intestinal obstruction (IO). These IO episodes were initially thought to arise from postoperative adhesions following previous abdominal surgery. It is important to note that adhesive bowel disease is the leading cause of intestinal obstruction in patients with previous abdominal surgery, and is seen in up to 75% of cases.10 Therefore, IO symptoms were initially attributed to adhesions. Similarly, one of the seven cases in the Sudanese series presented with intestinal obstruction.5
The presence of a tumorlike mass during surgery highlights the diagnostic challenge that arises from basidiobolomycosis. Several studies have reported that basidiobolomycosis often mimics malignancy.2,4,11 This confusing presentation often results in extensive surgeries that are usually reserved for malignant tumors. This is evidenced in the case series that included seven cases in Sudan, where a clinical diagnosis of colon cancer was made in four of the seven cases, with all of them undergoing some form of colectomy.5
Although basidiobolomycosis has traditionally been reported to occur in individuals with normal immunity, some studies have suggested that it also occurs among those with compromised immunity.1 HIV infection may impair immune responses and increase susceptibility to fungal infections.8 However, it is interesting to note that, many of the basidiobolomycosis cases have been reported in individuals whose immunity was normal.9–11 This suggests that immunity alone may not determine susceptibility. The patient described in this report had been on ART for over 20 years and had a normal CD4 count, suggesting a controlled infection. It is therefore safe to assume that HIV status may have not played a role in the occurrence of basidiobolomycosis. However, long-standing HIV infection may have contributed to the altered immune responses and susceptibility to infection. This paradox requires further evaluation to elucidate any association between HIV and basidiobolomycosis.
This patient underwent surgical resection mainly because she presented with intestinal obstruction but also because during surgery, the mass had features suggestive of malignancy. In the management of basidiobolomycosis, surgery has been reported to be necessary for tissue diagnosis and management of complications such as obstruction.11 Nonetheless, it is important to note that surgery alone is not sufficient for a definitive treatment. Treatment with antifungal medications has been reported to be the cornerstone of treatment, with itraconazole being the preferred first-line treatment.11 The patient described in this report was treated with itraconazole immediately after histological diagnosis was obtained. This is similar to what was done in the Sudanese case series where all the seven patients underwent some form of surgery in addition to voriconazole in four of the cases.
It is important to note that rapid improvement in surgical site infection was observed following the initiation of itraconazole. It is our hypothesis that fungal infections may have contributed to impaired wound healing. The literature shows that fungal infections also cause surgical site infections (SSI), but are underrecognized, especially in immunocompromised patients,12 with Candida species being the most common culprit.12 In this patient, the rapid improvement in the SSI after initiation of itraconazole treatment made it plausible for a hypothesis of fungal infection contributing to the SSI, although this was not confirmed by culture. This calls for further studies on the role of fungi, specifically basidiobolomycosis, in SSI.
The literature suggests that histopathology is the most reliable method for diagnosing GIB mainly because fungal cultures are often unreliable in clinical practice. This is because tissue culture often returns negative results, mainly because the fungus is often located deep in the tissues, but also because at times, there are difficulties in the transport and growth of the fungus due to technical challenges in resource-limited settings.6 Nonetheless, tissue culture is appropriate for precise identification of the organism. Histologically, GIB characteristically exhibits granulomatous inflammation, eosinophilic infiltration, and fungal elements.9 These features were also observed in this case.
This case highlights several important clinical and surgical challenges, including the ability of GIB to mimic adhesive bowel disease and malignancy, its occurrence in patients with HIV infection, its association with prior abdominal surgery, and the potential contribution of fungal infections to postoperative surgical site infections.
Limitations
This report was limited in several ways that we would like to acknowledge. Firstly, there was no fungal culture, molecular confirmation or Periodic acid–Schiff (PAS) staining. Secondly, advanced imaging was not done, mainly due to the resource limitation coupled with the emergency nature of the case which made referral of the patient for more investigations not an appropriate option. Also, the details regarding the patient’s prior surgical history were not available in addition to not being able to confirm the link between fungal infection and surgical site infection. The findings are inherently limited by the design of this study as a case report.
Conclusion
Gastrointestinal basidiobolomycosis should be considered to be among the possible causes in patients presenting with recurrent intestinal obstruction and ileocecal masses, particularly when presentation mimics malignancy. This may be helpful in avoiding some surgical interventions, even in resource limited settings. In particular, among patients with previous surgery, gastrointestinal basidiobolomycosis should be considered among the differential diagnoses when patients present with features of intestinal obstruction, to avoid delayed intervention.
Ethical Approval
This case report was exempt from ethical approval by the Research and Ethics Committee.
Consent for Publication
Written informed consent was obtained from the patient for publication and for any accompanying images. A copy of the written consent form is available for review by the Editor-in-Chief of this journal upon request.
Acknowledgment
We acknowledge the staff of Virika Hospital, for their contribution to the care of the patient.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This case report did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sector.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dhayhi NS, Aljarbou AZ, Alhazmi AH, et al. Pediatric gastrointestinal basidiobolomycosis: descriptive bicenteric retrospective study. Sci Rep. 2025;15(1):27211. doi:10.1038/s41598-025-13098-w
2. Rizk RC, Yasrab M, Weisberg EM, Fishman EK. Gastrointestinal basidiobolomycosis masquerading as cancer. Radiol Case Rep. 2024;19(3):944–6. doi:10.1016/j.radcr.2023.11.043
3. Meeralam Y, Basfar AM, Alzanbagi A, et al. Gastrointestinal basidiobolomycosis: a case series. Cureus. 2024;16(2):e55008. doi:10.7759/cureus.55008
4. Mirmoosavi S, Salehi M, Fatahi R, et al. Gastrointestinal basidiobolomycosis – a rare fungal infection: challenging to diagnose yet treatable – case report and literature review. IDCases. 2023;32:e01802. doi:10.1016/j.idcr.2023.e01802
5. Mohammed SA, Abdelsatir AA, Abdellatif M, et al. Challenging presentations of seven cases of gastrointestinal basidiobolomycosis in Sudan: clinical features, histology, imaging, and recommendations. J Lab Physicians. 2020;12(4):281. doi:10.1055/S-0040-1721149
6. Abulhamail AS, Alsubaie MA, Bahawi YO. Atypical presentation for a gastrointestinal basidiobolomycosis and rare side effect of Voriconazole: a case report and literature review. Med Mycol Case Rep. 2025;49:100719. doi:10.1016/j.mmcr.2025.100719
7. Sohrabi C, Mathew G, Maria N, Kerwan A, Franchi T, Agha RA. The SCARE 2023 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int J Surg Lond Engl. 2023;109(5):1136. doi:10.1016/j.ijsu.2018.10.028
8. Kwizera R, Bongomin F, Lukande R. Deep fungal infections diagnosed by histology in Uganda: a 70-year retrospective study. Med Mycol. 2020;58(8):1044–1052. doi:10.1093/mmy/myaa018
9. Mohammed M, Albishri A, Alabbas A, et al. Gastrointestinal basidiobolomycosis in pediatric cases with multiple-site involvement: a case series. Cureus. 2024;16(12):e76451. doi:10.7759/cureus.76451
10. Singh A, Paruthy SB, Kuraria V, et al. Unusual triggers of acute intestinal obstruction in surgical emergencies: a series of five cases. Cureus. 2024;16(5). doi:10.7759/cureus.60848
11. Vikram V, Hallur V, Samal S, et al. Basidiobolomycosis of right colon mimicking as carcinoma of colon. ACG Case Rep J. 2021;8(5):e00573. doi:10.14309/crj.0000000000000573
12. Shirani K, Seifi A, Assadi A, Mortazavi A, Seyed Alinaghi SA. A review on fungal surgical site infections: epidemiology, risk factors, main fungal agents, and prevention. Iran J Microbiol. 2025;17(4):516. doi:10.18502/ijm.v17i4.19225
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Case Report on Gastrointestinal Basidiobolomycosis Mimicking Inflammatory Bowel Disease: Insights and Review of Saudi Literature
Garatli S, Alharbi H, Alghamdi GS, Zaidi ARZ, AlSheef M
International Medical Case Reports Journal 2026, 19:569596
Published Date: 14 July 2026