Back to Journals » Advances in Medical Education and Practice » Volume 10
Case-Based Curriculum With Integrated Smartphone Applications Improves Internal Medicine Resident Knowledge Of Contraceptive Care
Authors Bachorik A, Nemer MK, Chen GL, Alexander CB, Pelletier SR, Pace LE, Shields HM ![]()
Received 28 June 2019
Accepted for publication 5 October 2019
Published 19 November 2019 Volume 2019:10 Pages 971—977
DOI https://doi.org/10.2147/AMEP.S221256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Alexandra Bachorik,1,2 Michelle K Nemer,3 Grace L Chen,4 Cristina Baseggio Alexander,1,2 Stephen R Pelletier,2 Lydia E Pace,2,4 Helen M Shields2,5
1Division of General Internal Medicine, Department of Medicine, Brigham and Women’s Hospital, Boston, MA, USA; 2Harvard Medical School, Boston, MA, USA; 3Department of Medicine, Metro Health Medical Center, Case Western Reserve School of Medicine, Cleveland, OH, USA; 4Division of Women’s Health, Department of Medicine, Brigham and Women’s Hospital, Boston, MA, USA; 5Division of Medical Communications, Department of Medicine, Brigham and Women’s Hospital, Boston, MA, USA
Correspondence: Alexandra Bachorik
Section of General Internal Medicine, Boston University School of Medicine, 801 Massachusetts Ave, 1st Fl, Boston, MA 02118, USA
Tel +12408999052
Fax +16176388096
Email [email protected]
Background: Contraception is an essential preventive service for all women. However, the literature suggests that internal medicine residents have low levels of confidence and knowledge of contraceptive care.
Objective: We designed and implemented a novel contraception curriculum promoting active, collaborative learning. We sought to evaluate whether this curriculum improved internal medicine resident knowledge of and comfort with contraceptive care through the administration of pre-/post-surveys.
Methods: Our curriculum was delivered in a two-hour session as part of the mandatory ambulatory curriculum for internal medicine interns at our institution in the academic year 2017–2018. Interns were provided with select online resources and two smartphone applications at the beginning of the session, which they then used in case-based small group work. Small group work was followed by a large group case review, co-facilitated by OB/GYN and internal medicine faculty.
Results: Thirty-eight participants completed surveys assessing knowledge of and comfort with contraceptive care immediately before and after the curriculum; 20 participants completed surveys assessing the same domains 4–6 months after the curriculum. Data from surveys administered immediately post-curriculum demonstrated significant improvements in knowledge about and comfort with counseling about, assessing medical eligibility for, and initiating multiple forms of contraception. Many of these improvements in knowledge and comfort were maintained on follow-up surveys 4–6 months following the curriculum.
Conclusion: Our case-based curriculum with integrated smartphone applications resulted in significant improvements in internal medicine resident knowledge of and comfort with the key skills of contraceptive care. In contrast to active, collaborative learning methodologies such as the flipped classroom, our methodology supports active, collaborative learning without requiring advance learner preparation, and is thus well suited to the time constraints of the graduate medical education setting. Our methodology is readily translatable to other clinical topics and residency curricula.
Keywords: reproductive health, medical education-graduate, medical education-curriculum development/evaluation, active learning, contraception
Introduction
Almost half of United States pregnancies are unintended.1 Unintended pregnancy is associated with adverse health, economic, and social consequences, particularly for women with chronic diseases who are at higher risk for maternal and fetal complications during pregnancy.2,3 As women with chronic diseases are more likely to receive primary care from internists compared to other types of providers, contraceptive care is an essential component of the care general internists provide to these patients, and to all patients seeking to avoid pregnancy.4
Despite the importance of contraceptive care in primary care and internal medicine, internal medicine residents report low levels of self-confidence and perceived competence surrounding contraceptive care.5–7 In a 2004 study, greater than 80 percent of primary care internal medicine residency program directors believed that their residents should master the prescription of oral contraceptive pills by the end of residency; however, only 10 percent believed that their residents did master this skill by the end of the residency.7 In a 2012 study at the University of Colorado, over 80 percent of residents reported perceived inadequate knowledge as a barrier to performing contraceptive counseling; greater than 20 percent of residents in this same study reported “low self-efficacy” around contraceptive counseling as a barrier to providing contraceptive counseling to patients.6
This lack of knowledge and comfort around contraceptive care perceived by both residents and by their supervisors likely results from limited curricula and training opportunities in women’s health in internal medicine residency programs.8,9 A national 2015 survey of internal medicine residency program directors demonstrated that inclusion of women’s health core competencies defined by the American Board of Internal Medicine was variable between programs nationally; contraception specifically was included in only approximately 70 percent of internal medicine residency curricula nationally.9
To address the need for improved contraceptive education among internal medicine residents, we designed, implemented and evaluated a novel contraception curriculum. In recognition of the increasing movement away from lectures in medical education and toward active, collaborative learning activities such as the flipped classroom, as well as growing use of smartphones as a portable educational and clinical resource, we employed a case-based learning design in which residents were provided with select online resources and smartphone applications for use in collaborative, case-based problem-solving.10–15
Methods
Settings And Participants
Our contraception curriculum was integrated into the ambulatory curriculum in the academic year 2017–2018 for first-year internal medicine residents (interns) at an urban tertiary academic medical center in the northeastern United States. The Partners HealthCare Institutional Review Board deemed this research exempt from further review.
Curriculum Description
Our curriculum consisted of a two-hour session facilitated by one internal medicine faculty member (L.P., H.G. and C.A.) or senior resident (A.B.) knowledgeable in reproductive health and one Obstetrics/Gynecology faculty member (K.B., D.B. and W.J.W.). We held four sessions, each with 10 participating interns. At the opening of each session, participants were provided a “toolbox” of references about contraception to guide their engagement with clinical cases, including the websites for the Center for Disease Prevention and Control (CDC) Medical Eligibility Criteria and the Reproductive Health Access Project, as well as two free smartphone applications (the CDC Contraception application and Contraception Point-of-Care application), which the participants were encouraged to download onto their phones.16–19
Participants were then split into groups of 2–3 interns and assigned one of four clinical cases to work through using the provided references, as well as any literature they located using their laptops. Each case led the participants through a clinical vignette with a series of discussion questions that covered pre-identified learning objectives for the case (see Appendix 1). Facilitators circulated during this time to assist with questions. After 20 mins of small group work, the Medicine and Obstetrics/Gynecology facilitators led an 80-min review of the cases where each group presented its case and responses to the discussion questions to the other groups, all of whom had worked on different clinical cases. During this review, participants were encouraged to ask clarifying questions about the cases, both of each other and the session facilitators.
Program Evaluation
We developed and administered anonymous written surveys to participants immediately before and after the session, as well as 4–6 months following the session (“delayed post-survey”), with the intent to: (1) describe baseline knowledge about and comfort with providing contraceptive care, and (2) assess the effectiveness of our curriculum in improving knowledge about and comfort with providing contraceptive care, both immediately post-session and over time (See Appendices 2–4). This pre-/post-survey approach to curriculum evaluation is standard in education literature as a means of assessing “changes in proficiency [that] have occurred in learners during the course of the curriculum.”20 The inclusion of a delayed post-survey is frequently used as a means of assessing whether changes in proficiency persist over time.20
To assess participant knowledge of contraceptive care, our surveys included 10 board exam-style questions with clinical vignettes, which assessed participants’ ability to match patient preferences to contraceptive method, facility with initiating a variety of contraceptive methods and knowledge of medical eligibility criteria for contraception. These questions were designed in accordance with the National Board of Medical Examiners’ guidelines for test question construction.21
Based on the literature cited above indicating low “self-efficacy” among residents as a barrier to provision of contraceptive counseling, our survey also incorporated questions about participants’ comfort with or confidence in various aspects of contraceptive care.6 Surveys included questions about participant comfort with (1) counseling about different forms of contraception, (2) initiation of contraception, and (3) assessing medical safety of contraception for patients with a range of medical conditions. Participants used a 5-point Likert scale to rate their level of comfort or confidence, ranging from “very comfortable/confident” (1) to “not at all comfortable/confident” (5). Five-point Likert scales for evaluation of comfort or confidence around clinical skills can be found elsewhere in the medical education literature, such as for the evaluation of trainee confidence or comfort with end-of-life care.22
The survey administered immediately after the session also asked participants to rate the value of the session, using another 5-point Likert scale. Similar 5-point Likert scales are used at our institution for medical education evaluation, and can be found elsewhere in the medical education literature for assessment of trainee satisfaction with educational programs.23,24
We used parametric tests for data analysis, which are appropriate for numerical data, including Likert-type data.20 We used paired t-tests to compare mean knowledge scores, as well as comfort and confidence scores, before and immediately after the curriculum. We used independent t-tests to compare the same domains between the pre- and delayed post-surveys, as the delayed post-surveys were anonymous. Participants used self-selected study identification codes for the pre- and immediate-post-surveys; most were unable to remember these identification codes for the delayed post-surveys and thus these surveys were analyzed independently. In addition to assessing and comparing global knowledge scores before and after the curriculum, we assessed and compared performance specifically in each knowledge domain (patient preference, contraceptive initiation and medical eligibility).
Results
In total, 40 interns participated in the curriculum. Thirty-nine interns completed the pre-curriculum survey, 39 completed the post-curriculum survey (for a total of 38 paired pre- and immediate post-surveys, or 95% of possible survey participants) and 20 (or 50% of possible survey participants) completed the delayed post-survey 4–6 months after the curriculum.
Baseline Knowledge Of And Comfort With Contraceptive Care
Prior to the session, the mean knowledge score (ie percent of 10 questions answered correctly) was less than 50% among all participants (Figure 1). Mean ratings of comfort and confidence around contraceptive care ranged from 3.0 for comfort with counseling about the intrauterine device (IUD) or implant to 3.6 for confidence in initiating birth control pills, patch, ring or injection (where 1= very comfortable or confident and 5= very uncomfortable) (Table 1).
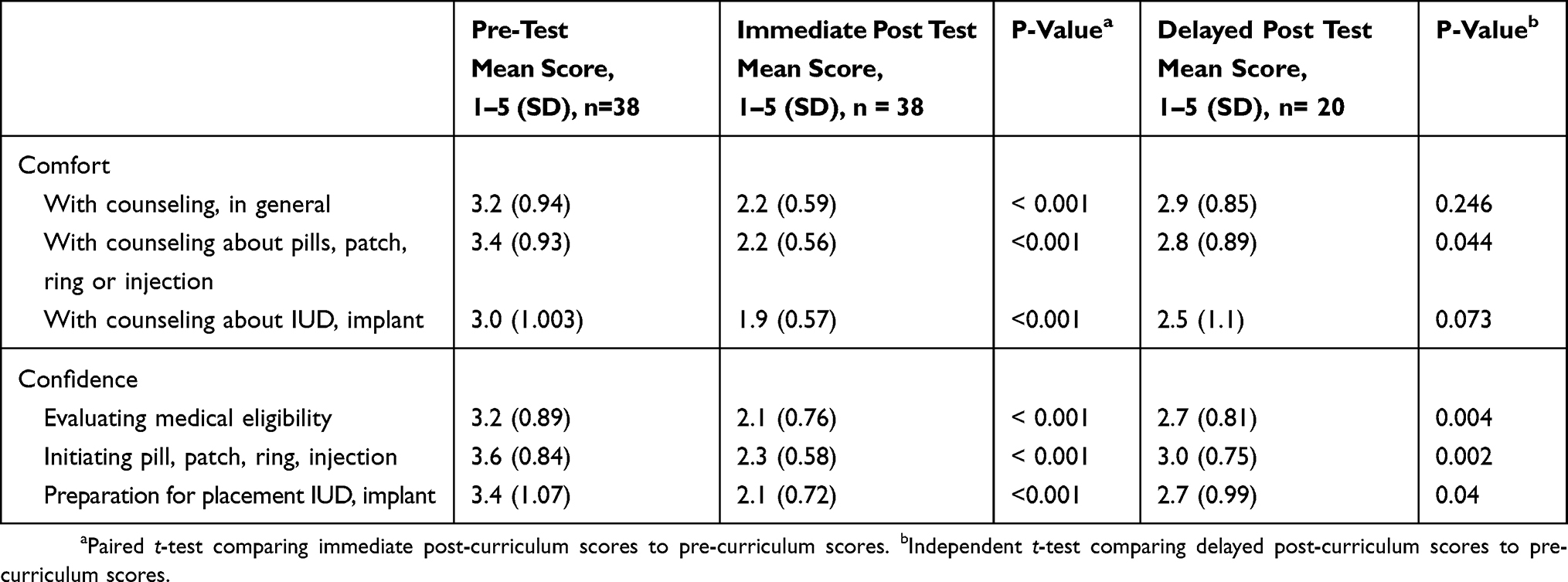 |
Table 1 Resident Comfort And Confidence With Contraceptive Counseling And Prescription Before And After Curriculum Participation (1= Very Comfortable/Confident, 5= Not At All Comfortable/Confident) |
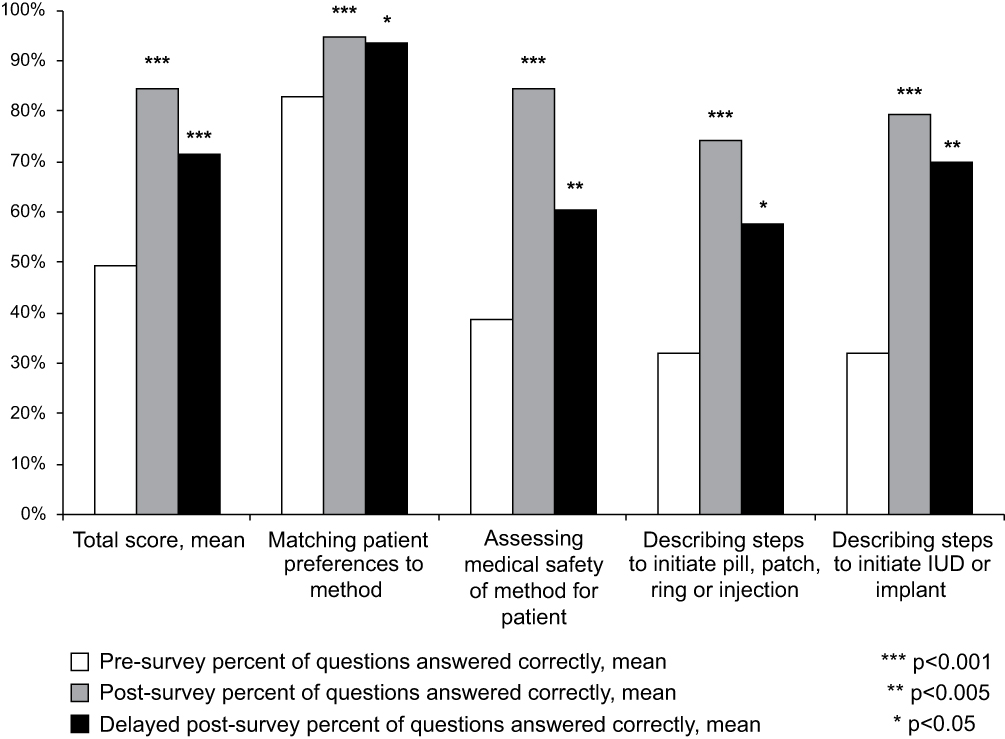 |
Figure 1 Resident performance on knowledge assessment before and after curriculum participation. Notes: Study participants completed a knowledge assessment, composed of 10 boards-style questions with clinical vignettes, immediately before, immediately after and 4–6 months after participation in the curriculum. P values to assess the statistical significance of changes between pre- and immediate post-survey data were calculated using a paired t-test; p values to assess the statistical significance of changes between pre- and delayed post-survey were calculated using an independent t-test. |
Post-Curriculum Knowledge Of And Comfort With Contraceptive Care
Immediately following the curriculum, the mean knowledge score improved significantly, nearly doubling from 49.2% correct answers on the pre-survey to 84.5% correct on the post-survey (Figure 1). Comfort and confidence scores also improved significantly across all domains (Table 1).
Many of these gains were maintained in delayed post-surveys at 4–6 months. Analysis of knowledge scores between pre- and delayed post-surveys demonstrated persistent statistically significant improvements in all knowledge domains. Compared with pre-curriculum scores there remained statistically significant gains in comfort with counseling about shorter-acting methods, confidence in assessing medically eligibility, and confidence in initiating both shorter and long-acting reversible forms of contraception, when compared to the pre-surveys (Table 1). However, improvements were no longer statistically significant around comfort with counseling in general, and comfort with counseling about the IUD or implant in particular.
Resident Feedback
Interns rated the session at a mean of 1.44 (1= very valuable, 5= not valuable at all). One participant commented, “Loved having time to download and use apps! Loved case based approach. Loved having [internal medicine] doc and GYN doc. Really excellent.”
Feasibility
This curriculum was integrated into the intern ambulatory curriculum and delivered as part of a morning of classroom-based didactics, thus ensuring access to the curriculum. Resources required for delivery of the curriculum included faculty teaching and curriculum materials. We had access to faculty from Obstetrics/Gynecology and Internal Medicine with interests in medical education and knowledge of contraceptive care. As a result of the difficulty coordinating different faculty schedules, there was no in-person faculty development session prior to curriculum facilitation; rather, faculty were provided with the curriculum materials and instructions about curriculum delivery electronically.
Discussion
Internal medicine residencies must equip their trainees to provide comprehensive women’s health care through providing training in contraception – a recommendation supported by recent policy statements by the American College of Physicians, which call for more robust training in women’s health, including contraception, at all levels of medical education.25 In this article we describe an innovative pedagogical approach, pairing active, collaborative learning activities with use of smartphone applications and online resources in “real-time,” to engage internal medicine interns and successfully improve resident knowledge and comfort around this critical clinical skillset.
The term active learning activities refers to instructional methods that promote learner engagement, including individual journaling, individual quizzes, group or paired discussion, solicitation of audience response through verbal questions or interactive audience response systems, and peer to peer teaching, among others.26–29 In general, these activities are thought to promote higher-order cognitive processes such as interpretation, application and analysis when compared to passive learning activities such as traditional lecture—and evidence from general and medical education literature indicates that active learning activities promote deeper understanding and superior recall relative to the traditional lecture.27,29
Collaborative learning activities represent a subset of active learning activities in which individual learners “work together toward a common goal and [the emphasis is on] group interactions” rather than working in isolation.29 In addition to conferring the benefits of active learning, collaborative learning activities are associated with improved quality of interpersonal interaction relative to individualistic learning.27 This is a benefit of significant value for medical trainees in an era where effective communication and functioning in interdisciplinary teams are key competencies for practicing physicians.30
In recognition of these advantages of active, collaborative learning activities, instructional methods incorporating these kinds of activities have increasingly replaced traditional lectures in medical education over the last three decades.11,12 The flipped classroom approach, in particular, has gained popularity in higher education, including medical education.11 The flipped classroom describes an educational strategy in which learners read or view content individually or in small groups prior to classroom time, and then use classroom time to engage in a guided application of concepts through a variety of active learning activities, such as problem sets.11 Though the flipped classroom model is defined by the use of classroom time for active learning activities and not necessarily collaborative ones, in practice its use in higher education and medical education has favored collaborative learning activities during classroom time, in which small groups work through clinical cases or other problem-solving activities together.11,29,31
Despite its growing popularity in medical education, implementation of the traditional flipped classroom poses unique challenges in graduate medical education settings. Specifically, resident time and motivation to research learning objectives, review content or complete assessments prior to a didactic session may be scarce or non-existent in the setting of demanding residency work hours, even on less hectic outpatient rotations. In Graham et al’s recent report on the flipped classroom, the authors note that time limitations are a major “logistical challenge” in utilizing the flipped classroom in graduate medical education.10 Emergency Medicine residents participating in a different study of the flipped classroom noted that “poor compliance” with content review and “finding time” to complete content review were weaknesses of the flipped classroom.10,32
In our model, we incorporate active, collaborative learning activities through case-based problem-solving in small and large groups without requiring advance preparation. Instead of requiring learners to review content ahead of classroom time, we provided them with curated online resources and smartphone applications to support problem-solving. This innovative approach not only addresses issues of feasibility with the flipped classroom, but also respects a tenet of adult learning by increasing the learning activity’s relevance to the learners’ professional, clinical role.33 Multiple studies demonstrate that over 50 percent of residents use smartphone applications in their clinical practice; residents also use their smartphones to access general web-based resources.13,15 Thus, by incorporating online resources and smartphone applications as problem-solving resources for our residents, we are mirroring their clinical practice and increasing the relevance of our learning activity to their daily professional tasks.
In summary, we created a curriculum that incorporates active and collaborative learning activities in a practical and highly clinically relevant manner. We received positive feedback from residents about their experience with our curriculum, and our data demonstrate its effectiveness in improving knowledge of and comfort with contraceptive care immediately following participation in the curriculum. Though our assessment of knowledge and comfort/confidence retention was limited by the anonymity and sample size of the delayed post-survey data, independent t-test analysis of these data suggests persistent knowledge and comfort gains in many domains 4–6 months following participation in the curriculum.
While there was a signal toward retention of knowledge and comfort, there was also some attrition of both between the immediate post-survey and delayed post-survey. This may indicate the need for implementation of a spaced learning strategy, either through clinical exposure as suggested above or through regular, interval review of material in a more didactic style.34
The integration of smartphone applications in our curriculum may also have a unique benefit of scaffolding this spaced learning. As we mention above, residents regularly use smartphone applications in their clinical practice, and our provision of applications relating to contraception may facilitate ongoing content review and clinical application as residents encounter opportunities for contraceptive care in their clinical practice.13,35
Our study has several limitations. Though our pre- and immediate post-survey data sample sizes represent 95 percent participation by eligible individuals (ie interns), our sample size is small. We could not conduct a paired analysis of delayed post-survey results due to participants’ inability to remember their unique identifiers. Further, since only 50 percent of curriculum participants completed delayed post-surveys, there may have been some degree of participant bias. Additionally, we did not include a control group in our study, as our pool of eligible individuals was already quite small. As a consequence, we cannot compare the results achieved with our curriculum and methods to results achieved by alternative approaches. Despite these limitations, we are able to pick up on statistically significant changes in knowledge and comfort in all domains on pre- and immediate post-surveys, and in many domains in delayed post-survey data. Finally, our survey tools assessed only self-reported comfort, without objective clinical assessment of residents’ practices around contraceptive counseling and prescribing.
Conclusion
We present a practical and translatable model for incorporating active, collaborative learning activities in the graduate medical education context without the need for advance preparation. We demonstrate our model’s success in improving knowledge of and comfort with contraceptive care. Our curriculum approach is readily translatable to other clinical topics. In ongoing research, we will develop clinically relevant strategies for evaluating trainees’ skills and patient outcomes.
Acknowledgements
Dr. Alexandra Bachorik was the 2018–2019 Sandra P. Gordon Fellow in Medical Education at the Brigham and Women’s Hospital. The authors would like to acknowledge Holly Gooding MD MSc, Deborah Bartz MD MPH, Kari Braaten MD MPH and Wan-Ju Wu MD MPH for their teaching as facilitators for the curriculum sessions. Lydia Pace and Helen Shields are co-senior authors.
Disclosure
The authors declare that no competing financial interests exist. We presented a poster covering this innovation and its results at the Harvard Medical School Medical Education Day on December 11, 2018.
References
1. Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. 2016;374(9):843–852. doi:10.1056/NEJMsa1506575
2. Campbell KH, Savitz D, Werner EF, et al. Maternal morbidity and risk of death at delivery hospitalization. Obstet Gynecol. 2013;122(3):627. doi:10.1097/AOG.0b013e3182a06f4e
3. Creanga AA, Berg CJ, Syverson C, Seed K, Bruce FC, Callaghan WM. Pregnancy-related mortality in the United States, 2006–2010. Obstet Gynecol. 2015;125(1):5. doi:10.1097/AOG.0000000000000564
4. Edwards ST, Mafi JN, Landon BE. Trends and quality of care in outpatient visits to generalist and specialist physicians delivering primary care in the United States, 1997–2010. J Gen Intern Med. 2014;29(6):947–955. doi:10.1007/s11606-014-2808-y
5. Schreiber CA, Harwood BJ, Switzer GE, Creinin MD, Reeves MF, Ness RB. Training and attitudes about contraceptive management across primary care specialties: a survey of graduating residents. Contraception. 2006;73(6):618–622. doi:10.1016/j.contraception.2006.01.014
6. Dirksen RR, Shulman B, Teal SB, Huebschmann AG. Contraceptive counseling by general internal medicine faculty and residents. J Womens Health. 2014;23(8):707–713. doi:10.1089/jwh.2013.4567
7. Spencer AL, Kern LM. Primary care program directors’ perceptions of women’s health education: a gap in graduate medical education persists. J Womens Health. 2008;17(4):549–556. doi:10.1089/jwh.2007.0473
8. Internal Medicine Training in Ambulatory Gynecology | JAMA Internal Medicine | The JAMA Network. Available from: https://jamanetwork-com.ezp-prod1.hul.harvard.edu/journals/jamainternalmedicine/fullarticle/618077.
9. Casas RS, Hallett LD, Rich CA, Gerber MR, Battaglia TA. Program directors’ perceptions of resident education in women’s health: a national survey. J Womens Health. 2016;26(2):133–140. doi:10.1089/jwh.2016.5860
10. Graham KL, Cohen A, Reynolds EE, Huang GC. Effect of a flipped classroom on knowledge acquisition and retention in an internal medicine residency program. J Grad Med Educ. 2019;11(1):92–97. doi:10.4300/JGME-D-18-00536.1
11. King AM, Gottlieb M, Mitzman J, Dulani T, Schulte SJ, Way DP. Flipping the classroom in graduate medical education: a systematic review. J Grad Med Educ. 2019;11(1):18–29. doi:10.4300/JGME-D-18-00350.2
12. Schwartzstein RM, Roberts DH. Saying goodbye to lectures in medical school — paradigm shift or passing fad? N Engl J Med. 2017;377(7):605–607. doi:10.1056/NEJMp1706474
13. Franko OI, Tirrell TF. Smartphone app use among medical providers in ACGME training programs. J Med Syst. 2012;36(5):3135–3139. doi:10.1007/s10916-011-9798-7
14. Short SS, Lin AC, Merianos DJ, Burke RV, Upperman JS. Smartphones, trainees, and mobile education: implications for graduate medical education. J Grad Med Educ. 2014;6(2):199–202. doi:10.4300/JGME-D-13-00238.1
15. Boruff JT, Storie D. Mobile devices in medicine: a survey of how medical students, residents, and faculty use smartphones and other mobile devices to find information. J Med Libr Assoc. 2014;102(1):22–30. doi:10.3163/1536-5050.102.1.006
16. Contraception Point-of-Care on the App Store. App Store. Available from: https://itunes.apple.com/us/app/contraception-point-of-care/id1212014869?mt=8.
17. Contraception on the App Store. App Store. Available from: https://itunes.apple.com/us/app/contraception/id595752188?mt=8.
18. Contraception options - the reproductive health access project. Reproductive Health Access Project. Available from: https://www.reproductiveaccess.org/key-areas/contraception/.
19. CDC - summary - USMEC - reproductive health. Available from: https://www.cdc.gov/reproductivehealth/contraception/mmwr/mec/summary.html. Published September 28, 2017.
20. Thomas PA. Curriculum Development for Medical Education: A Six-Step Approach. JHU Press; 2015.
21. Paniagua MA, Swygert KA. Constructing Written Test Questions for The Basic and Clinical Sciences. Philadephia, PA: National Board of Medical Examiners; 2016.
22. Tam V, You JJ, Bernacki R. Enhancing medical learners’ knowledge of, comfort and confidence in holding serious illness conversations. Am J Hosp Palliat Med. 2019;36(12):1096–1104. doi:10.1177/1049909119857988
23. Mody SK, Kiley J, Gawron L, Garcia P, Hammond C. Team-based learning: a novel approach to medical student education in family planning. Contraception. 2013;88(2):239–242. doi:10.1016/j.contraception.2012.07.012
24. Ottolenghi J, Athauda G, Stumbar SE, Kashan SB, Lupi C. Contraceptive pharmacology and risk communication: a case-based flipped classroom exercise. MedEdPORTAL J Teach Learn Resour. 2019;15:10790. doi:10.15766/mep_2374-8265.10790
25. Daniel H, Erickson SM, Bornstein SS; for the Health and Public Policy Committee of the American College of Physicians. Women’s Health Policy in the United States: an American College of physicians position paper. Ann Intern Med. 2018;168(12):874. doi:10.7326/M17-3344
26. Wolfley L Active learning strategies | center for excellence in teaching and learning. September 2014. Available from: https://cetl.uconn.edu/active-learning-strategies/.
27. Prince M. Does active learning work? A review of the research. J Eng Educ. 2004;93(3):223–231. doi:10.1002/j.2168-9830.2004.tb00809.x
28. Inra JA, Pelletier S, Kumar NL, Barnes EL, Shields HM. An active learning curriculum improves fellows’ knowledge and faculty teaching skills. Adv Med Educ Pract. 2017;8:359–364. doi:10.2147/AMEP.S135538
29. Hurtubise L, Hall E, Sheridan L, Han H. The flipped classroom in medical education: engaging students to build competency. J Med Educ Curric Dev. 2015;2:
30. Englander R, Cameron T, Ballard AJ, Dodge J, Bull J, Aschenbrener CA. Toward a common taxonomy of competency domains for the health professions and competencies for physicians. Acad Med. 2013;88(8):1088–1094. doi:10.1097/ACM.0b013e31829a3b2b
31. Tolks D, Schäfer C, Raupach T, et al. An introduction to the inverted/flipped classroom model in education and advanced training in medicine and in the healthcare professions. GMS J Med Educ. 2016;33(3). doi:10.3205/zma001045
32. Young TP, Bailey CJ, Guptill M, Thorp AW, Thomas TL. The flipped classroom: a modality for mixed asynchronous and synchronous learning in a residency program. West J Emerg Med. 2014;15(7):938–944. doi:10.5811/westjem.2014.10.23515
33. Merriam SB, Bierema LL. Adult Learning: Linking Theory and Practice. John Wiley & Sons; 2013.
34. Kerfoot BP, DeWolf WC, Masser BA, Church PA, Federman DD. Spaced education improves the retention of clinical knowledge by medical students: a randomised controlled trial. Med Educ. 2007;41(1):23–31. doi:10.1111/j.1365-2929.2006.02644.x
35. Wallace S, Clark M, White J. ‘It’s on my iPhone’: attitudes to the use of mobile computing devices in medical education, a mixed-methods study. BMJ Open. 2012;2(4):e001099. doi:10.1136/bmjopen-2012-001099
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.