Back to Journals » Infection and Drug Resistance » Volume 17
Carbapenem-Resistant Enterobacter cloacae Complex in Southwest China: Molecular Characteristics and Risk Factors Caused by NDM Producers
Authors Zeng Z, Wei Y ![]() , Ye C, Jiang Y
, Ye C, Jiang Y ![]() , Feng C, Guo T, Song M, Ding Y, Zhan P
, Feng C, Guo T, Song M, Ding Y, Zhan P ![]() , Liu J
, Liu J
Received 26 November 2023
Accepted for publication 12 April 2024
Published 29 April 2024 Volume 2024:17 Pages 1643—1652
DOI https://doi.org/10.2147/IDR.S447857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Zhangrui Zeng,1,* Yueshuai Wei,1,* Caihong Ye,1 Yuan Jiang,1 Chunlin Feng,1 Tongtong Guo,1 Min Song,1 Yinhuan Ding,1 Ping Zhan,2 Jinbo Liu1
1Department of Laboratory Medicine, The Affiliated Hospital of Southwest Medical University, Sichuan Province Engineering Technology Research Center of Molecular Diagnosis of Clinical Diseases, Molecular Diagnosis of Clinical Diseases Key Laboratory of Luzhou, Luzhou, People’s Republic of China; 2Department of Gynaecology, The Affiliated Hospital of Southwest Medical University, Luzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinbo Liu, Department of Laboratory Medicine, The Affiliated Hospital of Southwest Medical University, Sichuan Province Engineering Technology Research Center of Molecular Diagnosis of Clinical Diseases, Molecular Diagnosis of Clinical Diseases Key Laboratory of Luzhou, Luzhou, People’s Republic of China, Te/Fax +86 0830 3165730, Email [email protected]
Purpose: The isolation rate of carbapenem-resistant Enterobacter cloacae complex (CREC) is continuously increasing. The aims of this study were to investigate the molecular characteristics and risk factors associated with CREC infections.
Methods: Bacterial species were identified using the matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) (Bruker Daltonik GmbH, Bremen, Germany), and the hsp60 gene was utilized for further typing. Antimicrobial susceptibilities were assessed through the MicroScan WalkAway 96 Plus system (Siemens, Germany) and the microbroth dilution method. Antimicrobial resistance genes were screened through polymerase chain reaction (PCR), while the homologous relationship was assessed using multilocus sequence typing (MLST). Conjugation experiments were performed to verify whether the plasmid could be transferred. Additionally, logistic regression model was employed to analyze risk factors for CREC infections.
Results: 32 strains of CREC bacteria were isolated during the study, yet only 20 were retained for preservation. While the isolates demonstrated resistance to the majority of antibiotics, they exhibited high sensitivity to polymyxin B and tigecycline. All isolates carried the blaNDM resistance gene, including 13 blaNDM-1 isolates and 7 blaNDM-5 isolates. MLST homology analysis revealed the presence of seven known ST types and one new ST type. Conjugation experiments confirmed that 13 isolates were capable of transferring the blaNDM resistance gene to Escherichia coli strain EC600. Single-factor analysis identified multiple primary risk factors for CREC infection, but multivariate analysis did not reveal independent risk factors.
Conclusion: This study investigates the molecular characteristics and risk factors associated with CREC infections. The detection rate of CREC strains in our hospital is continuously rising and homology analysis suggested that strains might spread in our hospital, emphasizing the importance of implementing effective preventive measures to control the horizontal transmission of plasmid-mediated antimicrobial resistance genes.
Keywords: carbapenem-resistant, Enterobacter cloacae complex, antimicrobial resistance, molecular characteristics, risk factors
Introduction
Enterobacter cloacae complex (ECC), a species of the Enterobacteriaceae family, is increasingly prevalent in clinical infections. They are widespread in the environment and represent a clinically significant opportunistic pathogen.1 ECC comprises various species including Enterobacter cloacae, Enterobacter hormaechei, Enterobacter asburiae, Enterobacter kobei, Enterobacter ludwigii, Enterobacter nimipressuralis, Enterobacter mori, among others.2 The hsp60 gene typing scheme serves as a common method for distinguishing members within ECC, and it is widely adopted in practice.3 ECC strains are notorious members of the “ESKAPE” pathogens, causing diverse infections in clinical settings such as pulmonary, urinary system, and bloodstream infections.4 Recent studies have shown that this emerging multidrug-resistant (MDR) pathogen can lead to severe infections in newborns, resulting in poorer prognosis and higher treatment costs.5,6
With the increase of prevalence of clinical strains that producing extended-spectrum β-lactamase (ESBL), carbapenem antibiotics are regarded as the last line of defense against MDR bacterial infections. However, the clinical isolation rate of carbapenem-resistant Enterobacteriaceae (CRE) is gradually increasing.7 According to the report from the China Antimicrobial Resistance Surveillance System (CHINET), the resistance rate of Enterobacteriaceae to carbapenems was 2.7% in 2012. However, over the span of ten years, this rate has astonishingly risen to 9.7% in 2022. Mechanisms such as the production of carbapenemases, overexpression of efflux pumps, and mutation of porins contribute to Enterobacteriaceae resistance to carbapenem antibiotics.8 Carbapenemases production play a crucial role as the primary mechanism contributing to bacterial resistance, including enzymes such as KPC, NDM, VIM, IMP, and OXA-48.9 New Delhi metallo-β-lactamase (NDM) is an important member of class B carbapenemase, existing in various subtypes, with NDM-1 being the most common.10 The production of these enzymes renders most antibiotic treatments ineffective, posing a significant challenge to public health systems.
This retrospective study was conducted in a tertiary hospital in Southwest China with the aims of identifying the clinically isolated species of CREC strains, investigating the molecular characteristics and risk factors associated with CREC infections. The findings from this study will provide valuable insights for the hospital to control and prevent CREC infections.
Materials and Methods
Bacterial Collection
CREC was defined as Enterobacter cloacae complex strains resistant to imipenem or meropenem. From January 2020 to January 2023, a total of 32 strains of CREC bacteria were isolated, however, only 20 strains were preserved. Then, clinical isolates were identified using the matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) (Bruker Daltonik GmbH, Bremen, Germany). Because of the genetic similarity of Enterobacter cloacae complex members, amplification of the hsp60 gene was performed for the further identification of bacterial species.3 The primers were shown in Table S1.
Antimicrobial Susceptibility Testing (AST)
Antimicrobial susceptibility testing on CREC isolates was performed using the MicroScan WalkAway 96 Plus system (Siemens, Germany) and the microbroth dilution method, including Amikacin, Imipenem, Meropenem, Cefazolin, Cefuroxime, Ceftriaxone, Cefotaxime, Ceftazidime, Cefepime, Sulperazon, Ciprofloxacin, Levofloxacin, Tobramycin, Aztreonam, Ampicillin/sulbactam, Piperacillin/tazobactam, Cefoxitin, Tigecycline and Polymyxin B. The interpretation of the results followed the guidelines provided by the Clinical and Laboratory Standards Institute (CLSI). For the interpretation of tigecycline susceptibility results, the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines were employed. Escherichia coli ATCC25922 was used as the control strain, obtained from the China National Health Inspection Center.
Screening of CREC and Detection of Antimicrobial Resistance Genes
To verify whether the strain produces carbapenemases, as previously described, modified carbapenem inactivation method (mCIM) and EDTA-modified carbapenem inactivation method (eCIM) were utilized for validation.11 The phenotypic screening was conducted following the guidelines provided by the CLSI. Bacterial DNA templates were obtained through bacterial boiling, and polymerase chain reaction (PCR) was conducted to identify antimicrobial resistance genes (blaKPC, blaNDM, blaVIM, blaIMP, and blaOXA-48). Additionally, the presence of ESBL and AmpC resistance genes was also assessed. Positive samples were sent to Shenggong Biotechnology Co., Ltd. (Shanghai, China) for sanger sequencing, and the obtained sequencing results were analyzed through the NCBI BLAST database (http://www.ncbi.nlm.nih.gov/BLAST/). The primers employed to target resistance genes were referenced from the previous protocol.12 The primers were shown in Table S2.
Plasmid Conjugation Test
To validate whether the resistance genes are located on plasmids and capable of horizontal transfer, conjugation experiments were carried out. Following the previous experimental protocol with slight modifications, CREC strains carrying the blaNDM gene were used as donors, with the rifampicin-resistant Escherichia coli EC600 strain serving as the recipient. In brief, the donor and recipient strains were mixed in a ratio of 2:1 in LB broth, and the mixture was cultured overnight at 37°C. The cultures were then inoculated onto LB agar plates containing 1 μg/mL meropenem and 500 μg/mL rifampicin to select for successfully conjugated strains. To confirm the successful plasmid conjugation, the presumed conjugants were purified and subsequently validated using MALDI-TOF MS and PCR.13
Multilocus Sequence Typing (MLST)
Following the primer provided by the pubMLST website(https://pubmlst.org/ecloacae/), PCR amplification was performed on seven housekeeping genes. The positive PCR products were then sent to Shenggong Biotechnology Co. Ltd. (Shanghai, China) for sanger sequencing. The obtained sequences are submitted to the pubMLST website to determine the sequence type (ST) for each isolated strain. For the sequences that cannot be matched accurately, upload the necessary information according to the requirements of the website and wait for the assignment of a new sequence number.
Statistical Analysis
Data analysis was performed with SPSS v.26.0 software. In the assessment of risk factors, different statistical tests were employed based on the type of the data. Analysis of categorical variables utilizing either the chi-square test or Fisher’s exact test. Continuous variables were assessed by utilizing either the Student’s t-tests or Mann–Whitney U-test, the selection of which was contingent upon the normality assumption of the data distribution. In the univariate analysis, variables with P < 0.1 were included in the multivariate logistic regression analysis to determine independent risk factors for CREC infection. A statistically significant result was defined as P-value less than 0.05 (two-tailed).
Results
Basic Characteristics of the CREC Strains
Between 2020 and 2023, a total of 32 non-duplicated CREC strains were isolated in our hospital. As shown in Figure 1, they were obtained from different specimen types: sputum (n = 14, 43.8%), secretions (n = 8, 25%), urine (n = 6, 18.8%), drainage fluid (n = 2, 6.2%), pus (n = 1, 3.1%), and ascites (n = 1, 3.1%). Predominantly, departments such as burn surgery, orthopedics and neurology are the main sources. The majority of patients exhibited a positive outcome, with most achieving recovery or showing significant improvement. However, three cases (n = 3, 9.4%) resulted in death, suggesting that the CREC strains may be a low-virulence bacterium.
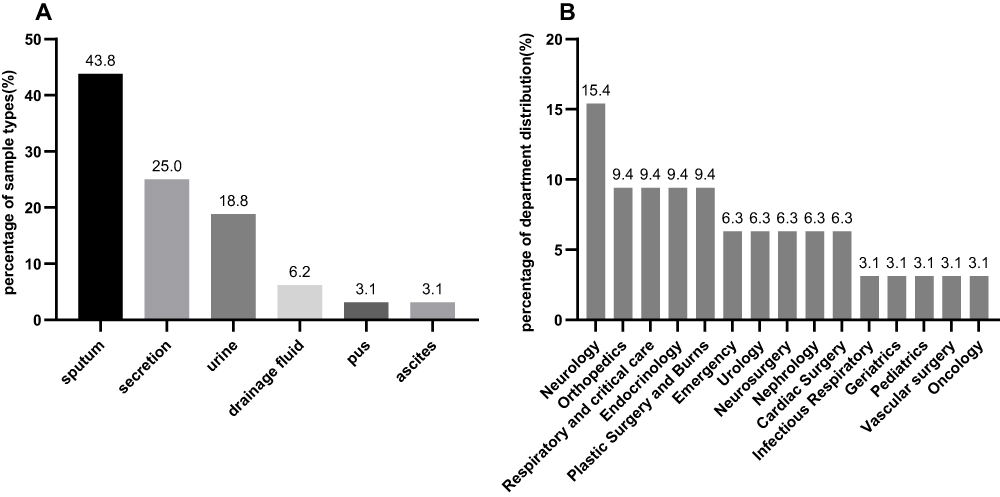 |
Figure 1 Distribution characteristics of 32 CREC isolates. (A) Sample types of 32 CREC isolates; (B) department distribution of 32 CREC isolates. |
This study compiled data on CREC isolates from the Southwest Medical University affiliated hospital over the years 2020 to 2023. In 2020, there were six isolates, followed by three isolates in 2021, seventeen isolates in 2022, and two isolates in January and February 2023. A gradual increase in the rate of CREC isolation has been observed in recent years, remaining at approximately 2% prior to 2021 but surging to 6.8% in 2022. This significant and swift escalation in isolation rates merits substantial attention.
Risk Factors of CREC Infections
In the analysis of risk factors, statistically significant differences were observed between the CREC group and the CSEC group in terms of cardiovascular diseases (P = 0.007), respiratory system diseases (P = 0.039), renal diseases (P = 0.009), gastrointestinal diseases (P = 0.026), invasive catheterization (P = 0.028) and use of aminoglycosides (P = 0.041) (Table 1). However, in the multivariate logistic regression analysis, no independent risk factors for CREC infections were identified.
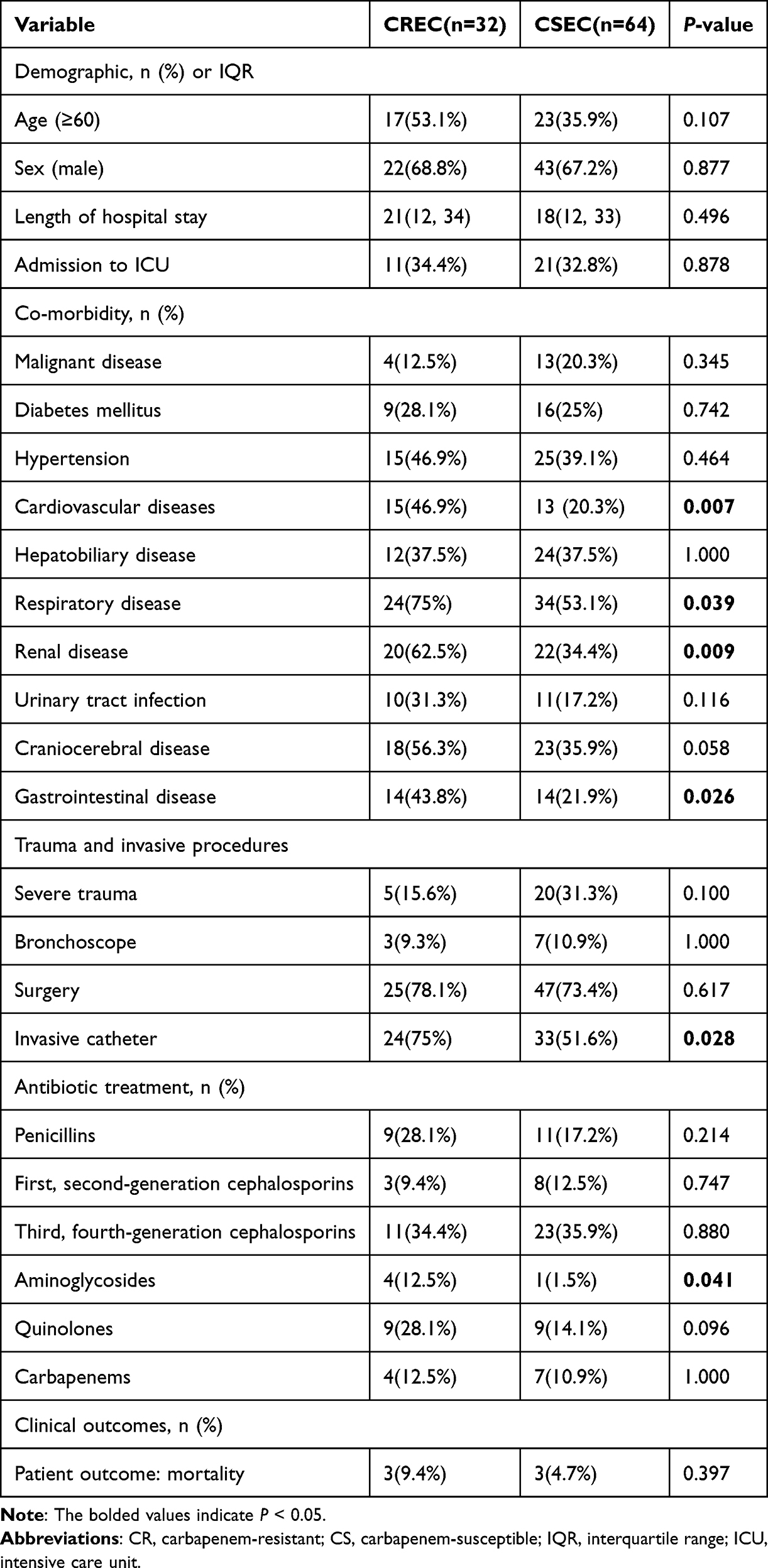 |
Table 1 Clinical Characteristics of CREC and CSEC Strains |
Species Identification of 20 CREC Strains
Seven MLST alleles were combined with the hsp60 gene, and a phylogenetic tree was constructed using Mega11.0 software with the Maximum Likelihood method. As shown in Figure 2, Enterobacter hormaechei subsp. xiangfangensis (n = 10) was the predominant strain type, followed by Enterobacter hormaechei subsp. steigerwaltii (n = 7), Enterobacter kobei (n = 2), and Enterobacter hormaechei subsp. hoffmannii (n = 1).
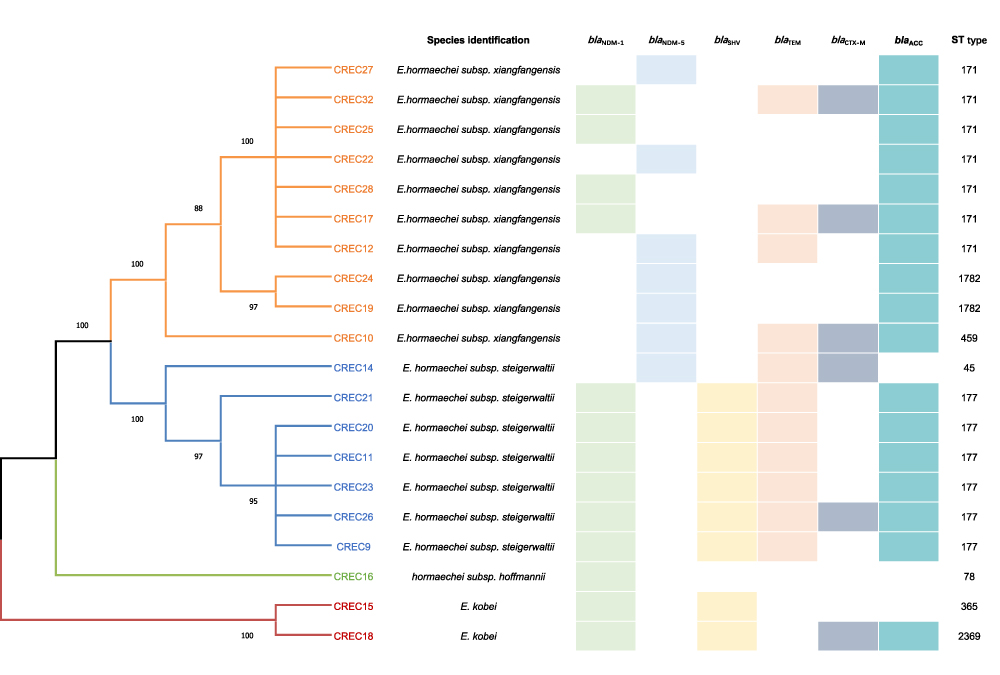 |
Figure 2 Species identification and clonal phylogenetic analysis of 20 strains of CREC. |
Antimicrobial Susceptibility Tests
All CREC strains in this study were resistant to three or more antibiotics and were defined as MDR. According to the results of antimicrobial susceptibility tests, the most sensitive antibiotics were tigecycline (100%) and polymyxin B (100%), followed by amikacin (85%). All strains showed extreme resistance to a variety of antibiotics, with 100% resistance rates to imipenem, meropenem, cefazolin, cefuroxime, ceftriaxone, cefotaxime, ceftazidime and cefepime. The antibiotic susceptibility profile was shown in Table 2.
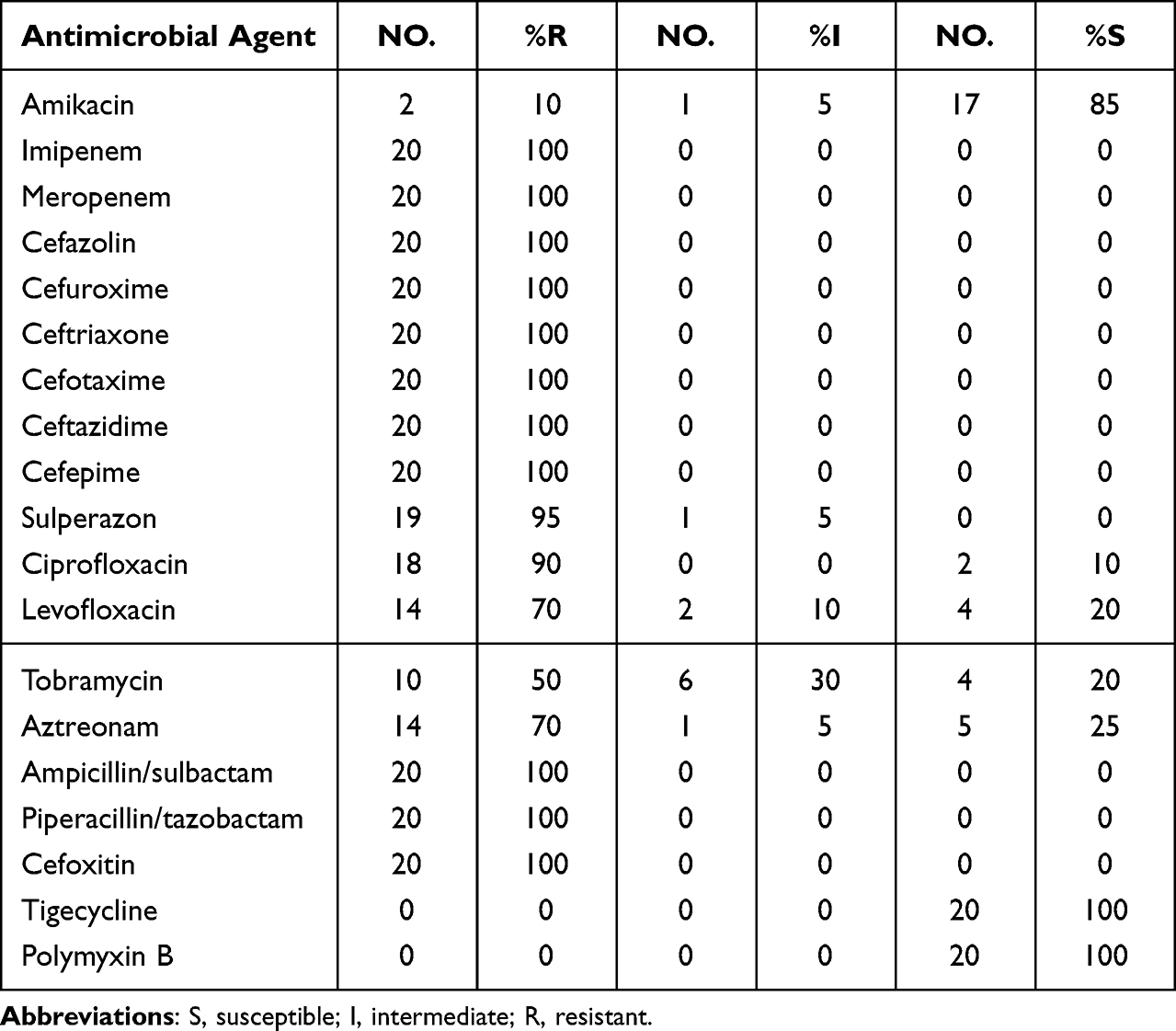 |
Table 2 Antimicrobial Susceptibility Profiles of 20 Clinical CREC Strains |
Phenotype and Genotype Analysis
As shown in Figure 2. All 20 CREC strains tested positive for both mCIM and eCIM assays, indicating the production of carbapenemases. PCR experiments revealed that all 20 CREC strains carried the blaNDM gene. Upon further sequencing analysis, it was found that 13 strains carried the blaNDM-1 gene (n = 13, 65%), while 7 strains carried the blaNDM-5 gene (n = 7, 35%). No other resistance genes were detected, suggesting that blaNDM was the predominant gene in the local area for CREC. Conjugation experiments showed that 13 CREC strains were able to transfer the resistance plasmids to recipient strains. PCR confirmation revealed that all transconjugants were positive for the blaNDM gene.
Additionally, the most frequently detected ESBL and AmpC resistance gene was blaACC (n = 17, 85%), followed by blaTEM (n = 11, 55%), blaSHV (n = 8, 40%), and blaCTX-M (n = 6, 30%).
Multilocus Sequence Typing (MLST)
A total of eight ST types were detected, including seven known ST types and one novel ST type designated as ST2369, as assigned by the pubMLST official website. The most common ST types, apart from the novel ST2369, were ST171 (n = 7) and ST177 (n = 6). Other less frequent ST types included ST1782, ST45, ST78, ST365, and ST459. It is noteworthy that the recent clinical isolates predominantly belonged to the ST171 sequence type, indicating a possible recent dissemination of this clone within our hospital. It was recommended to implement relevant measures to address this situation.
Comparison of Carbapenem Resistance Genes Carried by Different Genetic Strains
Among the 20 isolates in this study, Enterobacter hormaechei subsp. xiangfangensis (60%) was the main carrier of blaNDM-5, while other isolates mainly carried blaNDM-1. This indicated that there were differences in the types of carbapenemases carried by different subspecies of CREC strains. Additional sample sizes are required to investigate this phenomenon thoroughly.
Discussion
The infection caused by CREC has been paid more and more attention in clinical settings. As an emerging and common pathogen, CREC strains posed a serious threat to antimicrobial therapy.14 In this study, we conducted an analysis of CREC strains isolated from a teaching hospital in southwestern China. The results showed that the CREC strains exhibited high levels of resistance to most antibiotics. Molecular epidemiological studies revealed that ST171 and ST177 were the predominant sequence types, and blaNDM-1 and blaNDM-5 were the major antimicrobial resistance genes.
Enterobacter cloacae complex (ECC) includes multiple members.15 Distinguishing between these species using traditional phenotypic methods was difficult, and there was still controversy regarding the nomenclature of each member.16 For more precise molecular typing, Harald Hoffmann categorized ECC strains into 12 genetic clusters and one unstable sequence type based on the variations in the hsp60 gene.3 This classification system provided a more accurate approach to studying the classification, evolution, epidemiology, and pathogenicity characteristics of ECC strains. In this study, we classified the 20 CREC strains involved using the latest described method.2 Our research discovered that Enterobacter hormaechei was the predominant strain, with Enterobacter hormaechei subsp. xiangfangensis being the major representative, which was consistent with the findings of the majority of other studies.17,18
This study, which began in December 2020, investigated the resistance mechanisms and clinical epidemiology of CREC isolates in our hospital. The results of antibiotic susceptibility testing showed a 100% resistance rate to imipenem and meropenem, indicating a MDR phenotype. Polymyxin B and tigecycline appear to be the most effective treatments for these clinical isolates. However, there have been recent widespread reports of tigecycline-resistant CREC isolates in China, which required sufficient attention.19,20
New Delhi metallo-β-lactamase (NDM) belongs to the class B enzymes and is a type of metallo-β-lactamases (MBLs).21 In this study, the main mechanism of carbapenem resistance among the CREC strains was attributed to the production of NDM-1. And the blaNDM was identified as the only carbapenemase-encoding gene found in this study. Another research analyzing CREC strains from 11 regions in China confirmed that NDM was the predominant carbapenemase type, consistent with the findings of this study.22 Since its discovery in India in 2008, NDM has rapidly spread worldwide.23,24 Its flexible hydrolytic mechanism and increasing mutations have intensified the threat of antibiotic resistance. Extensive research has been undertaken with the objective of discovering potent inhibitors capable of reversing this prevailing condition.25,26 It has been found that the majority of blaNDM was located on plasmids, and due to the transferability of plasmids, the horizontal spread of plasmid-mediated resistance genes may occur if strict isolation measures are not taken.27 The plasmid conjugation transfer experiments in this study demonstrated that 13 CREC isolates were capable of transferring plasmids to EC600 recipient bacteria, conferring resistance and promoting the development of multidrug-resistant bacteria. This finding aligns with a study conducted in other southwestern regions of China.28 Plasmid-mediated horizontal gene transfer promotes the formation of the MDR phenotype in bacteria, further complicating the treatment of infections.
A total of eight sequence types were identified, with ST171 (n = 7) and ST177 (n = 6) being the most common. Previous research has examined the transmission of two different lineages of ST171 in the United States, highlighting ST171 as a high-risk clone with significant epidemic potential.29 However, recent studies have indicated its widespread presence across various regions.30,31 Another high-risk clone, ST78, was also identified in this study (n = 1), although it has not caused extensive outbreaks in the local region, appropriate measures should still be taken. When comparing different genetic clusters of bacteria, the blaNDM-5 gene was found to be predominantly distributed in Enterobacter hormaechei subsp. xiangfangensis, showing differences from bacteria in other genetic clusters. This phenomenon warranted further investigation. Conversely, all Enterobacter hormaechei subsp. steigerwaltii isolates carried the blaNDM-1 gene, which is significantly different from Enterobacter hormaechei subsp. xiangfangensis, suggesting variations in the enzyme types carried by different genetic clusters of bacteria. In this study, a new ST type, ST2369, was also identified. Through hsp60 gene sequencing, it was determined to be Enterobacter kobei and carried the blaNDM-1 gene. This is the first report of an ST2369 isolate of carbapenem-resistant Enterobacter kobei carrying the blaNDM-1. This newly discovered type requires further research to determine its specific characteristics and understand the spread of this clone. Its pathogenic potential should not be overlooked.
This study has some limitations. Firstly, the number of strains included in the study was relatively small, and it would be beneficial to collect more strains for future research. Secondly, the study was conducted in a single center, which limits its ability to represent the prevalence of strains in other regions. The results may have some bias due to the localized sample collection. It is important to expand the scale of the study in the future to conduct more comprehensive investigations and characterizations of CREC strains at a deeper level.
Conclusion
In this study, we described the molecular characteristics, risk factors and resistance mechanism of CREC strains in a tertiary hospital in Sichuan, China. ST171 and ST177 were the main sequence types. NDM was the predominant carbapenemase discovered and can be disseminated through plasmids, which was also the main reason for carbapenem resistance of CREC strains in our hospital. A new ST (ST2369) strain carrying the blaNDM-1 gene was detected. This research could help to better understand CREC strains and improve infection control and treatment in hospitals.
Data Sharing Statement
The data used or analyzed in this study can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study received approval from the Ethics Review Committee of the Affiliated Hospital of Southwest Medical University (KY2022267), in accordance with the principles outlined in the Declaration of Helsinki. Additionally, all patients participated by providing written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the grants from Sichuan Science and Technology Program (2022NSFSC1426, 2022ZHYZ0012, 2022YFQ0093, 2022YFS0008).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu S, Huang N, Zhou C, et al. Molecular mechanisms and epidemiology of carbapenem-resistant Enterobacter cloacae complex isolated from Chinese patients during 2004–2018. Infect Drug Resist. 2021;14:3647–3658. doi:10.2147/idr.S327595
2. Ganbold M, Seo J, Wi YM, Kwon KT, Ko KS. Species identification, antibiotic resistance, and virulence in Enterobacter cloacae complex clinical isolates from South Korea. Front Microbiol. 2023;14:1122691. doi:10.3389/fmicb.2023.1122691
3. Hoffmann H, Roggenkamp A. Population genetics of the nomenspecies Enterobacter cloacae. Appl Environ Microbiol. 2003;69(9):5306–5318. doi:10.1128/aem.69.9.5306-5318.2003
4. De Oliveira DMP, Forde BM, Kidd TJ, et al. Antimicrobial resistance in ESKAPE pathogens. Clin Microbiol Rev. 2020;33(3). doi:10.1128/cmr.00181-19
5. Girlich D, Ouzani S, Emeraud C, et al. Uncovering the novel Enterobacter cloacae complex species responsible for septic shock deaths in newborns: a cohort study. Lancet Microbe. 2021;2(10):e536–e544. doi:10.1016/s2666-5247(21)00098-7
6. Rahal A, Andreo A, Le Gallou F, et al. Enterobacter cloacae complex outbreak in a neonatal intensive care unit: multifaceted investigations and preventive measures are needed. J Hosp Infect. 2021;116:87–90. doi:10.1016/j.jhin.2021.07.012
7. Han M, Liu C, Xie H, et al. Genomic and clinical characteristics of carbapenem-resistant Enterobacter cloacae complex isolates collected in a Chinese tertiary hospital during 2013–2021. Front Microbiol. 2023;14:1127948. doi:10.3389/fmicb.2023.1127948
8. Ma J, Song X, Li M, et al. Global spread of carbapenem-resistant Enterobacteriaceae: epidemiological features, resistance mechanisms, detection and therapy. Microbiol Res. 2023;266:127249. doi:10.1016/j.micres.2022.127249
9. Jean SS, Harnod D, Hsueh PR. Global threat of carbapenem-resistant gram-negative bacteria. Front Cell Infect Microbiol. 2022;12:823684. doi:10.3389/fcimb.2022.823684
10. Li X, Wang Q, Huang J, et al. Clonal outbreak of NDM-1-producing Enterobacter hormaechei belonging to high-risk international clone ST78 with the coexistence of tmexCD2-toprJ2 and mcr-9 in China. Int J Antimicrob Agents. 2023;61(6):106790. doi:10.1016/j.ijantimicag.2023.106790
11. Zhao M, He J, Zhang R, Feng J, Deng Y, Zhang J. Epidemiological characteristics of New Delhi Metallo-β-Lactamase-producing Enterobacteriaceae in the fourth hospital of Hebei medical university. BMC Infect Dis. 2023;23(1):298. doi:10.1186/s12879-023-08242-8
12. Li Z, Ding Z, Yang J, et al. Carbapenem-Resistant Klebsiella pneumoniae in Southwest China: molecular characteristics and risk factors caused by KPC and NDM Producers. Infect Drug Resist. 2021;14:3145–3158. doi:10.2147/idr.S324244
13. Sun L, Chen Y, Qu T, et al. Characterisation of a Novel Hybrid IncFII(pHN7A8):IncR:IncN Plasmid Co-Harboring bla(NDM-5) and bla(KPC-2) from a Clinical ST11 Carbapenem-Resistant Klebsiella pneumoniae Strain. Infect Drug Resist. 2023;16:7621–7628. doi:10.2147/idr.S435195
14. Bolourchi N, Giske CG, Nematzadeh S, et al. Comparative resistome and virulome analysis of clinical NDM-1-producing carbapenem-resistant Enterobacter cloacae complex. J Glob Antimicrob Resist. 2022;28:254–263. doi:10.1016/j.jgar.2022.01.021
15. Candela A, Guerrero-López A, Mateos M, et al. Automatic discrimination of species within the Enterobacter cloacae complex using matrix-assisted laser desorption ionization-time of flight mass spectrometry and supervised algorithms. J Clin Microbiol. 2023;61(4):e0104922. doi:10.1128/jcm.01049-22
16. Wu W, Feng Y, Zong Z. Precise species identification for Enterobacter: a genome sequence-based study with reporting of two novel species, Enterobacter quasiroggenkampii sp. nov. and Enterobacter quasimori sp. nov. mSystems. 2020;5(4):e00527–20. doi:10.1128/mSystems.00527-20.
17. Oshiro S, Tada T, Watanabe S, et al. Emergence and spread of carbapenem-resistant and aminoglycoside-panresistant Enterobacter cloacae complex isolates coproducing NDM-Type Metallo-β-Lactamase and 16S rRNA Methylase in Myanmar. mSphere. 2020;5(2):e00054–20 doi:10.1128/mSphere.00054-20.
18. Zhu Z, Xie X, Yu H, et al. Epidemiological characteristics and molecular features of carbapenem-resistant Enterobacter strains in China: a multicenter genomic study. Emerg Microbes Infect. 2023;12(1):2148562. doi:10.1080/22221751.2022.2148562
19. Sun L, Xu J, He F. Draft genome sequence data of a tigecycline-resistant Enterobacter cloacae ST93 clinical strain isolated from bloodstream infection. Data Brief. 2018;21:414–418. doi:10.1016/j.dib.2018.10.004
20. Jiang Y, Yang S, Deng S, Lu W, Huang Q, Xia Y. Epidemiology and resistance mechanisms of tigecycline- and carbapenem-resistant Enterobacter cloacae in Southwest China: a 5-year retrospective study. J Glob Antimicrob Resist. 2022;28:161–167. doi:10.1016/j.jgar.2022.01.005
21. Farhat N, Khan AU. Evolving trends of New Delhi Metallo-betalactamse (NDM) variants: a threat to antimicrobial resistance. Infect Genet Evol. 2020;86:104588. doi:10.1016/j.meegid.2020.104588
22. Jin C, Zhang J, Wang Q, et al. Molecular characterization of carbapenem-resistant Enterobacter cloacae in 11 Chinese cities. Front Microbiol. 2018;9:1597. doi:10.3389/fmicb.2018.01597
23. Yan Z, Ju X, Zhang Y, et al. Analysis of the transmission chain of carbapenem-resistant Enterobacter cloacae complex infections in clinical, intestinal and healthcare settings in Zhejiang province, China (2022–2023). Sci Total Environ. 2024;920:170635. doi:10.1016/j.scitotenv.2024.170635
24. Gartzonika K, Politi L, Mavroidi A, et al. High prevalence of clonally related ST182 NDM-1-producing Enterobacter cloacae complex clinical isolates in Greece. Int J Antimicrob Agents. 2023;62(1):106837. doi:10.1016/j.ijantimicag.2023.106837
25. Palica K, Deufel F, Skagseth S, et al. α-Aminophosphonate inhibitors of metallo-β-lactamases NDM-1 and VIM-2. RSC Med Chem. 2023;14(11):2277–2300. doi:10.1039/d3md00286a
26. Li X, Wang Q, Zheng J, et al. PHT427 as an effective New Delhi metallo-β-lactamase-1 (NDM-1) inhibitor restored the susceptibility of meropenem against Enterobacteriaceae producing NDM-1. Front Microbiol. 2023;14:1168052. doi:10.3389/fmicb.2023.1168052
27. Liu H, Tu Y, He J, et al. Emergence and plasmid cointegration-based evolution of NDM-1-producing ST107 Citrobacter freundii high-risk resistant clone in China. Int J Antimicrob Agents. 2024;63(2):107069. doi:10.1016/j.ijantimicag.2023.107069
28. Hu K, Zhang J, Zou J, et al. Molecular characterization of NDM-1-producing carbapenem-resistant E. cloacae complex from a tertiary hospital in Chongqing, China. Front Cell Infect Microbiol. 2022;12:935165. doi:10.3389/fcimb.2022.935165
29. Gomez-Simmonds A, Annavajhala MK, Wang Z, et al. Genomic and geographic context for the evolution of high-risk carbapenem-resistant Enterobacter cloacae complex clones ST171 and ST78. mBio. 2018;9(3):e00542–18 doi:10.1128/mBio.00542-18.
30. Lumbreras-Iglesias P, de Toro M, Vázquez X, García-Carús E, Rodicio MR, Fernández J. High-risk international clones ST66, ST171 and ST78 of Enterobacter cloacae complex causing blood stream infections in Spain and carrying bla(OXA-48) with or without mcr-9. J Infect Public Health. 2023;16(2):272–279. doi:10.1016/j.jiph.2022.12.015
31. Hu S, Xie W, Cheng Q, et al. Molecular eidemiology of carbapenem-resistant Enterobacter cloacae complex in a tertiary hospital in Shandong, China. BMC Microbiol. 2023;23(1):177. doi:10.1186/s12866-023-02913-x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.