Back to Journals » Clinical Ophthalmology » Volume 19
Can Laser Retinopexy Prevent Retinal Detachment in Asymptomatic, High-Risk Eyes?
Authors Morris RE ![]() , Sapp MR, Conn DR, Chawla H, Kuhn F
, Sapp MR, Conn DR, Chawla H, Kuhn F
Received 23 May 2025
Accepted for publication 26 September 2025
Published 29 October 2025 Volume 2025:19 Pages 4011—4015
DOI https://doi.org/10.2147/OPTH.S537281
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Laser retinopexy prevents retinal detachment – Video S1 [537281]
Views: 526
Robert E Morris,1– 3 Mathew R Sapp,1– 3 Dewayne R Conn,1,2 Harshvardhan Chawla,1– 3 Ferenc Kuhn1,4
1Helen Keller Eye Research Foundation, Birmingham, AL, USA; 2Retina Specialists of Alabama, Birmingham, AL, USA; 3Department of Ophthalmology, University of Alabama at Birmingham, Birmingham, AL, USA; 4Department of Ophthalmology, University of Pécs Medical School, Pécs, Hungary
Correspondence: Robert E Morris, Helen Keller Eye Research Foundation, 2208 University Blvd., Suite 101, Birmingham, AL, 35233, USA, Tel +1 659 297 5577, Email [email protected]
Abstract: Significant literature evidence of retinal detachment prophylaxis safety and effectiveness for asymptomatic but high-risk eyes has appeared during the last five years. But it is still deemed “insufficient evidence to guide management” of asymptomatic fellow eyes in the American Academy of Ophthalmology’s Preferred Practice Pattern for 2025. However, both focal and encircling prophylaxis for asymptomatic fellow eyes with lattice degeneration, and encircling laser prophylaxis for asymptomatic fellow eyes with attached posterior vitreous, now justify treatment consideration versus continued observation, based on the evidence we do have, even though it is not “level one”.
Keywords: rhegmatogenous retinal detachment, RD, retinal detachment prevention, encircling laser prophylaxis, 360-degree laser prophylaxis, retinal tear, Stickler syndrome, SS
More than fifty years after the introduction of laser retinopexy as a prophylaxis for rhegmatogenous retinal detachment (retinal detachment, RD),1 prophylactic treatment of asymptomatic but high-risk eyes remains controversial.
Predisposing conditions can be identified by history and physical examination. They include lattice degeneration, retinal breaks, myopia, pseudophakia, family history of RD, fellow eye status, impending posterior vitreous detachment (PVD), and (rarely but importantly) Stickler syndrome status. Nevertheless, because it has been difficult to identify precisely which eyes are at high risk and how high a risk they face, there have been no prospective, randomized clinical trials performed during five decades of laser retinopexy - though such trials have been frequently called for at the conclusion of retrospective articles on RD prophylaxis.2,3
The American Academy of Ophthalmology Retina/Vitreous committee in its preferred practice pattern (PPP) revision published on February 7, 2025, continues to maintain that
Sufficient evidence exists to warrant treating acute, symptomatic horseshoe tears. There is insufficient evidence for treatment of other vitreoretinal abnormalities.
Further stating that
A primary limitation of prophylactic therapy is that causative breaks leading to RRD often occur during a PVD in areas that appeared normal prior to the PVD.3
As a result, physicians and their patients in the United States continue to remain “on their own” in making preventive decisions for asymptomatic eyes with various conditions predisposing to RD.
Preventive retinopexy includes focal treatment of selected visible lesions (Figure 1); and 360-degree (encircling) grid treatment (Figure 2) - developed precisely to overcome the limitation cited in the PPP - that causative tears often occur in normal appearing (peripheral) retina.4,5
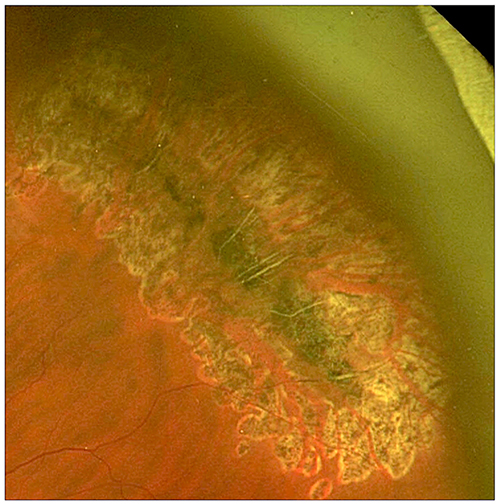 |
Figure 1 Image of coalescent laser treatment for prophylaxis of a pigmented lattice degeneration lesion. Used with permission of Retina Specialists of Alabama |
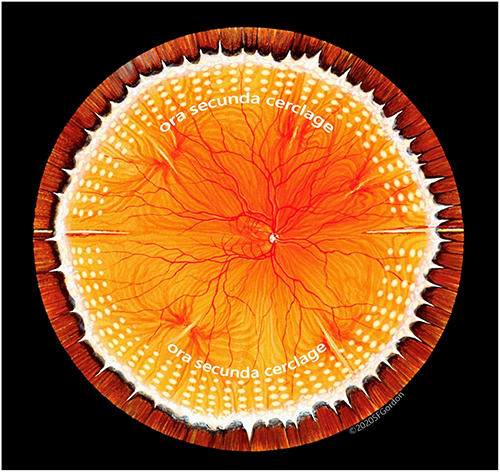 |
Figure 2 Illustration of “standard” ora secunda cerclage (OSC) that in our experience has proven successful in non-syndromic eyes for more than two decades - producing in effect a “second ora” posterior to all high-risk peripheral retina.4 Used with permission of artist Stephen F Gordon ©2020. |
The conundrum of focal versus encircling versus no prophylaxis has recently been mitigated by strong proof of safe and effective encircling retinopexy prophylaxis in asymptomatic children and adolescents with Stickler syndrome (SS), the highest risk condition known to predispose an eye to RD.6,7 Encircling laser prophylaxis reduced RD approximately five-fold, preventing not only detachments, but also giant retinal tears and the multiple smaller tears that commonly cause SS detachments.7
SS patients are definitively identifiable via genetic testing; and their high-risk level (over 50% lifetime) has been well established.6 Thus, the 2025 PPP report for the first time endorsed 360-degree (encircling) laser prophylaxis for asymptomatic, high-risk eyes - but only for genetically verified SS.3
Because SS and more common (non-syndromic) age-related RD share the ultimate pathogenesis of peripheral vitreous traction tears, it is reasonable to expect similar encircling laser prophylaxis effectiveness in both.8 In fact, we have found this to be the case since laser delivery via the indirect ophthalmoscope (IDO) was introduced in the 1990s (Video S1). Nevertheless, focal laser treatment of symptomatic retinal tears remains the only prophylaxis unequivocally endorsed for non-syndromic eyes in the 2025 PPP.3
The choice of observation versus preventive treatment for asymptomatic, high-risk eyes should not ignore the preponderance of existing evidence, even though it is less than “level one.” In the absence of clinical trials, but with additional recent evidence of prophylaxis safety and effectiveness in asymptomatic, high-risk eyes,6,7,9 it is becoming increasingly important to provide patient education regarding the evidence we do have, though it is still deemed insufficient in the 2025 PPP.3
Of particular importance is the plight of asymptomatic fellow eyes, especially when the primary eye had a poor visual outcome after RD repair. Fortunately, two author groups have recently reported significant information to better guide fellow eye prophylaxis.9,10
Wallsh et al in 2023 reported on 582 fellow eyes with attached posterior vitreous proven by optical coherence tomography (OCT), followed for an average of 5.7 years. They showed a 41.5% rate of retinal tear or retinal detachment in such eyes when PVD eventually occurred.10 Lattice degeneration was associated with a 50% increase in the rate of RD development.
Curran et al in 2024 showed a 41% rate of tear or detachment in 352 fellow eyes with lattice degeneration (83% without initial PVD), during an average follow-up of 2.95 years.9 This was reduced to a rate of 17% in 146 fellow eyes (88% without initial PVD) prophylactically treated with focal laser (Figure 1) during an average follow-up of 2.69 years. When undergoing cataract surgery, phakic fellow eyes with lattice degeneration developed tears or detachments in 31% of eyes. This was reduced to a rate of 22% in fellow eyes that had previously been treated with focal laser prophylaxis.
While citing Curran et al, the 2025 PPP still states that “a prospective trial is necessary to confirm the effectiveness of laser prophylaxis in fellow eyes;” and that “there is no level I evidence to support the use of prophylactic laser surgery to areas of lattice retinal degeneration prior to anterior segment surgery.”3
In the likely long interim awaiting results of a prospective clinical trial, we believe that both focal retinopexy and encircling prophylaxis (seeking to further reduce risk below the 17% achieved with focal prophylaxis)9 are reasonable treatments for fellow eyes with lattice degeneration, especially absent a PVD.10 And encircling laser prophylaxis is a reasonable consideration for fellow eyes with persistently attached posterior vitreous, facing a 41.5% risk at the time of PVD, especially if the primary eye lost macular function to RD.11
A complete description of a technique to achieve optimal encircling laser prophylaxis (Ora Secunda Cerclage, OSC)4 is available in our 2023 publication. For all predisposing conditions in high-risk, non-syndromic eyes, when preventive encircling prophylaxis is elected, grid treatment should extend from the ora serrata posteriorly (4 or 5 rows) so as to encompass the vitreous base.4 If the long ciliary nerves at 3 and 9 o’clock are spared, laser power is appropriately controlled, and care is taken to maintain adequate pupil dilation throughout treatment, the anterior segment is minimally affected by encircling grid laser prophyaxis.4
We extend encircling laser treatment further posteriorly in Stickler syndrome, to and between the vortex vein ampullae (approximately 9 rows).12 Our protocol (Ora Secunda Cerclage/Stickler Syndrome, OSC/SS) is now being studied in the first clinical trial (clinicaltrials.gov) of retinal detachment prevention by laser retinopexy since its introduction in 1970.1
In all encircling retinopexy prophylaxis, reduced peripheral visual field is an inevitable trade off to achieve increased lifetime security for the more important central visual field, but this is rarely symptomatic.11,12 Epimacular proliferation (EMP) is seen in 4% of cases postoperatively, but this is no higher than the incidence of EMP in untreated, elderly adults.13 And it is considerably less frequent and less significant as compared to EMP seen after treatment of retinal detachments.4
The Wallsh et al and Curran et al reports, combined with the success of encircling prophylaxis in asymptomatic SS patients,7,12 should now be part of achieving informed consent for continued observation or preventive retinopexy treatment in fellow eyes. And the informed patient’s preference should then be guiding.
While retinopexy increases retinal resistance to vitreous traction by a factor of three to five,14 it does not reduce vitreous traction itself. To do so in selected asymptomatic but especially high-risk eyes, after maturation of encircling laser retinopexy prophylaxis, “safest possible” vitrectomy, as designed for eyes with symptomatic vitreous opacities, can now also be considered to achieve maximum prophylaxis.15,16
Abbreviations
RD, retinal detachment; PPP, preferred practice pattern; OSC, ora secunda cerclage; PVD, posterior vitreous detachment; SS, Stickler syndrome; OCT, optical coherence tomography.
Acknowledgments
The authors thank Christina Sullivan, MHA and Linda Laney, RN without whom this work could not have been published in its final form. They also thank Wesley Skipper for administrative support whenever needed.
Funding
Partial funding was provided by the Helen Keller Eye Research Foundation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McDonald PR, Tasman W. Treatment of peripheral breaks: comparison of cryosurgery, diathermy, laser, and xenon photocoagulator. Int Ophthalmol Clin. 1967;7(2):451–457. PMID: 5601677. doi:10.1097/00004397-196700720-00017
2. Wilkinson CP. Interventions for asymptomatic retinal breaks and lattice degeneration for preventing retinal detachment. Cochrane Database Syst Rev. 2012;3(3):CD003170. Update in: Cochrane Database Syst Rev. 2014;(9):CD003170. doi: 10.1002/14651858.CD003170.pub4. PMID: 22419286; PMCID: PMC4730545. doi:10.1002/14651858.CD003170.pub3
3. Kim SJ, Bailey ST, Kovach JL, et al. American Academy of Ophthalmology Preferred Practice Pattern Retina/Vitreous Committee. Posterior vitreous detachment, retinal breaks, and lattice degeneration preferred practice pattern®. Ophthalmology. 2025;132(4):P163–P196. PMID: 39918519. doi:10.1016/j.ophtha.2024.12.023
4. Morris RE, Kuhn F, Richardson C. Preventing retinal detachment: the encircling laser retinopexy technique. Clin Ophthalmol. 2023;17:1505–1513. PMID: 37273500; PMCID: PMC10239236. doi:10.2147/OPTH.S406337
5. Byer N. Evidence-based analysis of prophylactic treatment of asymptomatic retinal breaks and lattice degeneration; invited commentary: against treatment. Ophthalmology. 2000;107:15–16. doi:10.1016/S0161-6420(99)00066-4
6. Fincham GS, Pasea L, Carroll C, et al. Prevention of retinal detachment in Stickler syndrome: the Cambridge prophylactic cryotherapy protocol. Ophthalmology. 2014;121(8):1588–1597. PMID: 24793526. doi:10.1016/j.ophtha.2014.02.022
7. Camp DA, Bakhsh, SR, Torkashvand, A et al. Laser prophylaxis for retinal detachment in Stickler syndrome: A systematic review and meta‐analysis. Acta Ophthalmologica, 2025;103(6):e364–e373. PMID: 40370211. doi10.1111/aos.17509
8. Morris RE, Kuhn F, Sipos T. Preventing retinal detachment: where are we? Implications from stickler syndrome. Clin Ophthalmol. 2022;16:4315–4321. PMID: 36583093; PMCID: PMC9793794. doi:10.2147/OPTH.S388631
9. Curran CD, Adams OE, Vagaggini T, et al. Prophylactic treatment of lattice degeneration in fellow eyes after repair of uncomplicated primary rhegmatogenous retinal detachment. Retina. 2024;44(1):63–70. PMID: 37536462. doi:10.1097/IAE.0000000000003908
10. Wallsh JO, Langevin ST, Kumar A, Huz J, Falk NS, Bhatnagar P. Fellow-eye retinal detachment risk as stratified by hyaloid status on OCT. Ophthalmology. 2023;130(6):624–630. PMID: 36773761. doi:10.1016/j.ophtha.2023.02.004
11. Morris RE, Kuhn F, West MR, Richardson C. Re: Wallsh et al.: Fellow-eye retinal detachment risk as stratified by hyaloid status on OCT (Ophthalmology. 2023;130:624–630). Ophthalmology. 2023;130(12):e44–e45. PMID: 37737810. doi:10.1016/j.ophtha.2023.08.014
12. Morris RE, Parma ES, Robin NH, et al. Stickler Syndrome (SS): laser prophylaxis for retinal detachment (Modified Ora Secunda Cerclage, OSC/SS). Clin Ophthalmol. 2021;15:19–29. PMID: 33447008; PMCID: PMC7802593. doi:10.2147/OPTH.S284441
13. Xie B, Lin Y, Lin C, et al. Epiretinal membrane formation following laser photocoagulation for peripheral retinal degeneration: incidence and risk factors. Eye. 2025. PMID: 40721494. doi:10.1038/s41433-025-03945-5
14. Zauberman H. Tensile strength of chorioretinal lesions produced by photocoagulation, diathermy, and cryopexy. Br J Ophthalmol. 1969;53(11):749–752. PMID: 5358520; PMCID: PMC506750. doi:10.1136/bjo.53.11.749
15. Morris RE. Vitreous Opacity Vitrectomy (VOV): safest possible removal of “Floaters”. Clin Ophthalmol. 2022;16:1653–1663. PMID: 35673347; PMCID: PMC9167598. doi:10.2147/OPTH.S361557
16. Morris RE, Kuhn F, Sapp MR, Chawla H. Vitrectomy as a prevention for retinal detachment in high-risk eyes. Clin Ophthalmol. 2025;19:3249–3253. doi:10.2147/OPTH.S530665
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preventing Retinal Detachment: The Encircling Laser Retinopexy Technique

Morris RE, Kuhn F, Richardson C
Clinical Ophthalmology 2023, 17:1505-1513
Published Date: 30 May 2023
Vitrectomy as a Prevention for Retinal Detachment in High-Risk Eyes

Morris RE, Kuhn F, Sapp MR, Chawla H
Clinical Ophthalmology 2025, 19:3249-3253
Published Date: 5 September 2025
A Historical Review of Encircling Laser Retinopexy as a Prophylaxis for Rhegmatogenous Retinal Detachment; and a Commentary on Recent Progress in Stickler Syndrome

Morris RE, Kuhn F, Oltmanns MH, West MR, Baxter CR, Sapp MR, Chawla H
Clinical Ophthalmology 2026, 20:588688
Published Date: 19 April 2026
Encircling Laser Prophylaxis for Retinal Detachment in Stickler Syndrome: The Impact on Visual Field

Fletcher DC, Schuchard RA, Morris RE, Kuhn F
Clinical Ophthalmology 2026, 20:599194
Published Date: 14 July 2026