Back to Journals » Clinical Ophthalmology » Volume 17
Preventing Retinal Detachment: The Encircling Laser Retinopexy Technique
Authors Morris RE ![]() , Kuhn F, Richardson C
, Kuhn F, Richardson C
Received 29 January 2023
Accepted for publication 11 May 2023
Published 30 May 2023 Volume 2023:17 Pages 1505—1513
DOI https://doi.org/10.2147/OPTH.S406337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Robert E Morris.
Views: 2512
Robert E Morris,1– 3 Ferenc Kuhn,2,4 Cole Richardson1– 3
1Retina Specialists of Alabama, LLC, Birmingham, AL, USA; 2Helen Keller Foundation for Research and Education, Birmingham, AL, USA; 3Department of Ophthalmology, University of Alabama at Birmingham (UAB), Birmingham, AL, USA; 4Department of Ophthalmology, University of Pécs Medical School, Pecs, Hungary
Correspondence: Robert E Morris, Helen Keller Foundation for Research and Education, 2208 University Boulevard, Suite 101, Birmingham, AL, 35233, USA, Tel +1 205 936 0704, Email [email protected]
Abstract: Encircling (360 degree) retinal detachment prophylaxis using indirect ophthalmoscope laser delivery recently achieved strong proof of safety and effectiveness by preventing the development of peripheral retinal tears and detachments in the eyes of patients with Stickler syndrome (syndromic eyes). Untreated, Stickler syndrome patients have a 65% lifetime risk of retinal detachment (half by age 20, 80% bilateral). This report describes an optimal technique of encircling laser retinopexy to also prevent the more common retinal detachments seen in aging (non-syndromic) eyes that share with Stickler syndrome the common pathogenesis of peripheral retinal tears caused by vitreous traction.
Keywords: retinal tear, retinal detachment, retinal detachment prevention, 360-degree laser retinopexy, encircling laser prophylaxis, ora secunda cerclage, Stickler syndrome
Plain Language Summary
Laser treatment to the peripheral retina has recently been shown to reliably prevent retinal tears that lead to potentially blinding childhood retinal detachment in Stickler syndrome, a rare inherited disease having the highest known risk for retinal detachment (see illustrations). Because retinal detachments in older adults (having no such known genetic predisposition) are similarly caused by peripheral retinal tears, this is strong evidence that encircling laser treatment could likely also prevent this most frequent cause of sudden sight loss in high-risk eyes of the elderly population. This article describes the details of how to optimally apply similar laser preventive treatment in (non-syndromic) adult eyes.
Introduction
Encircling laser treatment to the peripheral retina has recently been shown to reliably prevent retinal tears and retinal detachment (RD) in Stickler syndrome (SS), a rare inherited disease having the highest known lifetime risk of RD.1–6 We reviewed the history of RD prevention in a December 2022 publication, concluding that this recent SS experience constitutes the first strong proof that encircling laser retinopexy applied with the indirect ophthalmoscope (IDO laser cerclage) is a safe and effective RD prophylaxis for all high-risk eyes that share the common pathogenesis of peripheral retinal tears caused by vitreous traction.7
The current report presents the details of an optimal IDO laser cerclage technique for (non-syndromic) high risk eyes undergoing age-related vitreous traction, concluding with comments on future RD prevention.
History of Encircling Laser Prophylaxis
Indirect ophthalmoscope laser delivery was first described in 1981,8 and has been clinically available since approximately 1990.9 For the first time it enabled reliable laser treatment of the entire peripheral retina, extending anteriorly to and beyond the ora serrata. Thus, IDO laser delivery brought to treatment of the peripheral retina the same advantages the IDO had long provided in diagnosis (wide-angle viewing, stereopsis, and dynamic scleral depression).
Rhegmatogenous retinal detachment is frequently caused by tears in normal appearing peripheral retina, usually coincident with posterior vitreous detachment (PVD).10,11 The threat of such tears in high-risk fellow eyes of individuals who have already lost vision in one eye from RD, or the experience of having an eye suffer RD despite seemingly successful, earlier focal laser to an existent tear in the same eye (Figure 1), caused encircling (360 degree) laser prophylaxis to be adopted empirically. It has since probably been most frequently used as a prophylaxis against re-detachment, either by IDO or more recently by endolaser application, during vitrectomy repair of existent RD. In fact, a 2013 survey by the American Society of Retina Specialists (ASRS) showed that 40% of retina specialists once used encircling laser treatment as part of routine vitrectomy RD repair.
 |
Figure 1 Illustration of retinal detachment from a new tear in normal appearing retina in an eye that had previously received focal laser for a retinal tear elsewhere. Image ©(2005)Stephen F. Gordon. |
We became early adopters of IDO laser delivery (Supplementary video 1) and presented our experience with encircling IDO laser prophylaxis for high-risk eyes at the inaugural meeting of the ASRS in 2002. We presented our concepts subsequently in many other meeting forums; by invitation as the Cover Story in the publication Retina Today (March/April 2008);12 and elsewhere.13
Although it has been widely used, very little is reported on the technique of IDO encircling laser prophylaxis, even though both its effectiveness and its safety depend on methodology. Here we discuss the technical details of successful encircling IDO laser prophylaxis.
The Current Prophylaxis Environment
Although it has now been more than 50 years since the advent of laser retinopexy,14 and three decades since the advent of IDO laser delivery,9 the entire field of retinal detachment prophylaxis continues laboring in the absence of any randomized clinical trial on the effectiveness of either focal or encircling laser prophylaxis.15 In this “evidence-based” environment, focal treatment of symptomatic tears is accepted but the value of focal treatment of asymptomatic (non-traumatic) defects and lattice degeneration is unknown, and it is usually not recommended.16 And encircling prophylaxis receives little mention despite its ubiquity.16
However, there now exist at least fourteen retrospective, comparative publications,17 over a period of more than 30 years,of encircling IDO laser prophylaxis effectiveness, with a reported net RD risk reduction of approximately 77% in various “high-risk” retinal conditions (Supplemental Report - Table). Although one can dispute the “strength of evidence” for each of these retrospective reports, it is less convincing to ignore their totality. This is especially true in the context of the recently successful encircling laser prophylaxis in SS that provides the first strong evidence upon which similar prophylaxis in all eyes at high risk of RD from peripheral retinal tears can confidently go forward.7
Technique - Ora Secunda Cerclage (Creating a Second Ora)
Before the advent of IDO delivery, peripheral encircling laser treatment was applied with a mirrored contact lens at a slit lamp, typically leaving untreated retina anteriorly.18 RD could still occur from new defects in the untreated anterior retina (Figure 2), breaking through the posterior laser “fence” barrier.19 Especially because of its ability to more easily place treatment as anteriorly as the ora in encircling RD prophylaxis, IDO delivery has been a critically important improvement over such slit lamp delivery.
 |
Figure 2 Illustration of failed encircling laser prophylaxis as performed via a mirrored contact lens before the advent of IDO laser delivery. Image ©(2002)Stephen F. Gordon. |
To remedy the danger posed by untreated high-risk retina anteriorly, we performed encircling grid retinopexy using IDO delivery, from posterior to the vitreous base to the ora serrata in all meridians (Figure 3). In effect, we created a “second ora” or “ora secunda” more posteriorly (ora secunda cerclage, OSC),12 taking the entire high-risk retina “off the playing field.” The concept of producing a “second ora” posteriorly was also mentioned independently by Pollack et al in 1994.18 It is an important concept and terminology that continues to distinguish this approach from the “failed fence” approach shown in Figure 2, and from literature reports with little or no technique description (Supplemental Report - Quotations).20,21
 |
Figure 3 Illustration of our “standard” ora secunda cerclage (OSC) that has proven successful in non-syndromic eyes for more than two decades. Images ©(2020)Stephen F. Gordon. |
In our standard OSC encircling prophylaxis technique, coalescent treatment is first placed around visible defects and lattice degeneration, and the long ciliary nerves at 3 and 9 o’clock are demarcated for avoidance. Smooth on-and-off scleral depression protects against causing inadvertent vitreous traction. Then an encircling grid of laser applications is placed elsewhere in the periphery from approximately halfway between the vortex vein ampullae and the ora serrata, extending anteriorly to reach the ora.
Although the vortex veins exit the sclera several millimeters posterior to the equator, internally the vortex vein ampullae are located at approximately the equator, averaging 7.6 mm posterior to the ora serrata.22
In all cases, treatment should encompass the (invisible) posterior border of the vitreous base, lying on average less than 2 mm and rarely more than 3.7 mm behind the ora serrata (less than halfway between the ora serrata and the vortex vein ampullae)22,23 to protect the retina during any subsequent PVD. This usually requires four or five rows of treatment immediately posterior to the ora serrata, with one burn width separation.
But reference to “rows” is somewhat of an artificial construct since treatment is commonly placed without regard to creating distinct “rows”, although the term is frequently used in the literature for convenience of communication. And burn width is variable and only an approximation when performing IDO. More importantly, treatment should be placed with regard to spacing and extent. However placed, an OSC treatment edge lying behind the vitreous base does not present a significant risk for tearing during subsequent PVD in our experience, although in a few eyes the vitreous base can extend abnormally far posteriorly with advancing age.22
Burn Placement and Intensity
Burn placement should be meticulously controlled throughout a procedure with a suggested treatment speed set at an interval of 150 to 200 milliseconds between laser applications (Supplementary video 1). Each surgeon must find a “sweet spot” that allows as rapid “lasering” as possible but as slow as necessary to achieve a true grid pattern with moderate intensity. There is no distinction in high-speed treatment with overlapping or too intense burns, producing unintended areas of retinal necrosis and consequent atrophy. Maximal dilation ensures optimal viewing for laser placement and protects against inadvertent iris and lens burns (Figure 4).
 |
Figure 4 Postoperative images of acute burns of the iris and anterior lens cortex, associated with IDO laser treatment using normal settings of 300 mw power, 0.1 sec, but with inadequate dilation of a brown iris. Courtesy of Retina Specialists of Alabama, LLC. |
Beyond accurate burn placement, good control of laser power is critically important. The delicate neurosensory retina can develop necrotic defects when the chorioretinal complex is treated with excessive power density, weakening the retina instead of strengthening it as intended. This can itself lead to iatrogenic RD. The size of the aiming beam on the retinal surface indicates the need to adjust laser power accordingly, to avoid higher than intended power density. This can change with the laser light path through variable ocular media as complete encirclement is achieved.
An average OSC treatment with IDO, using a 28-diopter condensing lens, consists of 800 to 1400 moderate intensity applications of encircling grid laser, placed between one and two burn widths apart. It is important to spare anterior segment innervation via the long ciliary nerves in the horizontal meridians to reliably prevent the complications of internal ophthalmoplegia and neurasthenic cornea.24 In our experience, OSC not only prevents detachments emanating from tears in the periphery, but it also prevents tears themselves from occurring within properly treated peripheral retina. Optimally performed retinopexy strengthens chorioretinal adhesion by a factor of 3–5 versus untreated retina,25 to help withstand subsequent vitreous traction.
The laser power used to perform OSC is set to produce easily seen but not “chalk white” burns, approaching from a known conservative power density. Heavily pigmented eyes require reduced treatment power, and as encirclement proceeds this can vary across quadrants even within a single eye, necessitating laser power adjustments (or momentary intentional defocusing to enlarge burns, decreasing power density). Conversely, a minimally pigmented choroid cannot easily produce the grey/white retinal lesion commonly expected, and one should not mistakenly increase power density far above the usual levels trying to obtain it.
Prophylaxis against giant retinal tear/dialyses (as in SS) requires a tighter grid pattern.3–6 Slightly higher power density is also advisable. Especially in a tight grid pattern, the effort to space burns requires slower treatment speed and prevents retinal necrosis from overlapping applications. Moreover, to prevent giant tears near the ora in Stickler syndrome (OSC/SS), we have shown that the anterior edge of treatment can be extended on to the pars plana to cover the anterior vitreous base. And the posterior edge of treatment can be extended to and between the vortex vein ampullae, preventing the multiple posterior tears often seen in SS eyes,26 without causing symptomatic loss of peripheral visual field.3
Safety Considerations
The definition of “burn” is “to alter or destroy by the action of heat”.27 The distinction between altering (to produce a strengthening adhesion) and destroying (by causing necrosis) while treating the delicate neurosensory retina can be minimal (Figure 5), requiring vigilance in monitoring power density and the resultant retinal “whitening”. To encourage sensitivity to the issue of burn intensity, we routinely record not only the number of burns delivered, but also the total joules of energy used (Supplemental Report - Parameters).
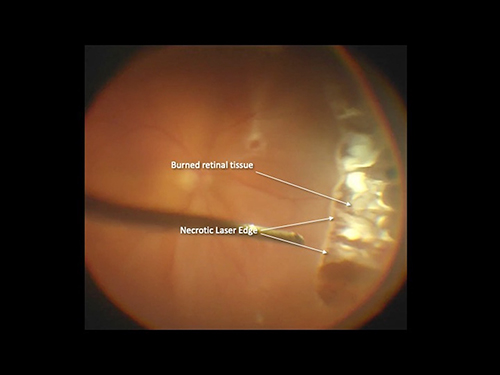 |
Figure 5 Large, oval necrotic defect in previously normal retina, extending from 2 to 5 o’clock, one week after encircling endolaser treatment during RRD repair, necessitating subsequent reoperation with application of a high external scleral buckle. Courtesy of Retina Specialists of Alabama, LLC. |
Over treatment can occur during encircling treatment with rapid IDO delivery when insufficient effort is made to achieve separated “grid” lesions of moderate intensity. It can also occur during vitrectomy with high-speed endolaser applications from a probe held too close to the retina during wide-angle viewing. Moreover, intense, and coalescent laser treatment of the choroid can leave large areas of bare sclera unavailable to produce future chorioretinal adhesions, evoking an analogy to “carpet bombing” in its final appearance (Figure 6).28
 |
Figure 6 Coalescent, intense laser applications leave a large area of atrophic choroid and injures the temporal long ciliary nerve, risking internal ophthalmoplegia and denervation of the cornea.23 Courtesy of Retina Specialists of Alabama, LLC. |
During repair of RD by vitrectomy, gas tamponade, and laser treatment of tears, if encircling laser prophylaxis is also performed, it should be accomplished with the great care and expertise befitting its importance in preventing future defects and detachment - not inadvertently producing them. After all, it is the part of the procedure that permanently changes the retina, for better or for worse, and it should not be routinely delegated to a less experienced assistant once the retina is reattached. Will it stay there? That’s determined by the quality of laser retinopexy.
Focal treatment of defects and modest lattice degeneration can usually be accomplished with the convenience of local anesthesia. But when an eye is determined to be at high risk of RD and a patient desires maximal preventive treatment via encircling retinopexy, laryngeal mask anesthesia is also justified and provides the ideal surgical conditions most conducive to accomplishing optimal prophylaxis.
Summary
So where have we been, and where are we going once an ideal encircling prophylaxis technique is established?
Encircling laser prophylaxis was once routinely applied at the conclusion of vitrectomy, especially for macular hole closure and RD repair,20 to forestall postoperative redetachments from undetected peripheral defects or iatrogenic tears that were more common and more covert (ASRS survey, 2013). But this was an era when slow cutters, large suction ports, large (non-cannulated) sclerotomies, and primitive suction control were still in use, before wide angle microscopes were routinely available to examine the peripheral retina at vitrectomy conclusion (Figure 7).29
 |
Figure 7 Image of current ultra-high speed (5000 to 20,000 cpm) 20G and 27G vitrectomy probes that have dramatically reduced the incidence of intraoperative tears during vitrectomy, obviating the need for routine encircling laser prophylaxis in most procedures. 20G instruments are now rarely used, in favor of 25G, 23G and 27G probes. Courtesy of Alcon corporation. |
With iatrogenic tears now being relatively rare and even tiny existent defects more easily discovered, most post-vitrectomy eyes are no longer “high-risk” eyes for RD.30 Consequently, if the surgeon performs microscopic examination of the peripheral retina under anesthesia (MEPRUA) when concluding vitrectomy, the need for intraoperative encircling laser as a routine prophylaxis against redetachment has greatly diminished.31 Henceforth, however, encircling laser at the conclusion of vitrectomy reattachment will always be advantageous for selected cases that warrant it in the surgeon’s judgement.- especially as an alternative to adding scleral buckles to vitrectomy reattachment surgery.32
The importance of encircling prophylaxis is apparently just beginning, however, for the prevention of RD in adults with various predisposing lesions/conditions, and in children with Stickler syndrome. Strong proof of “cause and effect” from preventively treating asymptomatic eyes in older adults has eluded research physicians for decades, because it has been difficult to show which eyes are truly at high risk, and to quantify how high a risk they face.
It has thus been almost impossible, despite 50 years of laser retinopexy, to document a substantial preventive effect of treatment to the degree of statistical certainty now required for broad acceptance of new procedures. For decades such a proof requirement has overcome both the knowledge that 360-degree laser retinopexy substantially increases retinal resistance to vitreous traction tears throughout the peripheral retina;25 and numerous retrospective comparative reports of encircling laser effectiveness (Supplemental Report - Table).
However, these difficulties are not present in Stickler children and adolescents, who are easily identifiable by genetic testing, family history, and eye examination; and whose lifetime retinal detachment risk is known to be 65%.1,2 So successful prophylaxis in SS has recently provided the first strong evidence to justify IDO laser cerclage prophylaxis for all eyes (syndromic and non-syndromic) that are at high risk from the same pathogenesis - peripheral retinal tears caused by vitreous traction.7
Conclusion
It is difficult to define “high risk” in non-syndromic adult eyes, and we do not purport to do so here. But when counseling a patient estimated to be at high risk, it is no longer acceptable practice to withhold mention of encircling prophylaxis in expectation of even stronger future proof of safety and efficacy. It is the patient who lives “under the sword of Damocles”,33 (Supplementary video 2) and who should have the right to choose prophylaxis or continued observation based on strong existent evidence.
Regardless of indication, encircling laser prophylaxis for each eye should be expertly performed and “as much as necessary, but as little as possible”. The effort to do so leaves a laser “signature” that permanently reflects the surgeon’s great effort to achieve ideal long-term prophylaxis stability.
Acknowledgments
Christina Sullivan assisted in manuscript preparation and video editing. Laura Beckwith, Dewayne Conn, and Jessica Haynes provided substantial assistance in administration and clinical care, for which we are grateful. The staff of the UAB Callahan Eye Hospital operating rooms expertly assisted us in refining our treatment techniques. Bernard Dib, MD aided with video and photography. All photographic images are courtesy of Retina Specialists of Alabama LLC, and illustrations are with permission of artist Stephen Gordon.
Funding
Support for this article was provided by the Helen Keller Foundation for Research and Education, through grants from the Hanna Charitable Trust; the Kent Companies of Midland, Texas; and the Gary Christ trust benefitting the Foundation.
Disclosure
Dr. Robert Morris is President of the Helen Keller Foundation for Research and Education, Birmingham, Alabama, USA. Dr. Ferenc Kuhn is the Foundation’s Director of Clinical Research and Chairman of the International Society of Ocular Trauma. Drs. Morris and Kuhn are vitreoretinal surgeons and longtime research collaborators in ocular trauma, macular surgery, endophthalmitis, and retinal detachment. Dr. Cole Richardson is a fellow at Retina Specialists of Alabama, Birmingham, Alabama, USA. The authors report no other conflicting interests with respect to this study.
References
1. Parma ES, Körkkö J, Hagler WS, Ala-Kokko L. Radial perivascular retinal degeneration: a key to the clinical diagnosis of an ocular variant of stickler syndrome with minimal or no systemic manifestations. Am J Ophthalmol. 2002;134(5):728–734. doi:10.1016/S0002-9394(02)01646-X
2. Fincham GS, Pasea L, Carroll C, et al. Prevention of retinal detachment in stickler syndrome. The Cambridge prophylactic cryotherapy protocol. Ophthalmology. 2014;121(8):1588–1597. doi:10.1016/j.ophtha.2014.02.022
3. Morris RE, Parma ES, Robin NH, et al. Stickler Syndrome (SS): laser prophylaxis for retinal detachment (modified Ora Secunda Cerclage, OSC/SS). Clin Ophthalmol. 2021;15:19–29. PMID: 33447008; PMCID: PMC7802593. doi:10.2147/OPTH.S284441
4. Naravane AV, Belin PJ, Pierce B, Quiram PA. Risk and prevention of retinal detachments in patients with stickler syndrome. Ophthalmic Surg Lasers Imaging Retina. 2022;53(1):7–11. PMID: 34982001. doi:10.3928/23258160-20211213-02
5. Khanna S, Rodriguez SH, Blair MA, Wroblewski K, Shapiro MJ, Blair MP. Laser prophylaxis in patients with stickler syndrome. Ophthalmol Retina. 2022;6(4):263–267. PMID: 34774838. doi:10.1016/j.oret.2021.11.001
6. Linton E, Jalil A, Sergouniotis P, et al. Laser prophylaxis in stickler syndrome: the Manchester protocol. Retina. 2022. PMID: 36165842. doi:10.1097/IAE.0000000000003634
7. Morris RE, Kuhn F, Sipos T. Preventing retinal detachment: where are we? Implications from stickler syndrome. Clin Ophthalmol. 2022;16:4315–4321. doi:10.2147/OPTH.S388631
8. Mizuno K. Binocular indirect argon laser photocoagulator. Br J Ophthalmol. 1981;65:425–428. doi:10.1136/bjo.65.6.425
9. Friberg TR. Clinical experience with a binocular indirect ophthalmoscope laser delivery system. Retina. 1987;7(1):28–31. doi:10.1097/00006982-198707010-00006
10. Benson WE, Grand MG, Okun E. Aphakic retinal detachment: management of the fellow eye. Arch Ophthalmol. 1975;93:245–249.
11. Byer NE. Evidence-based analysis of prophylactic treatment of asymptomatic retinal breaks and lattice degeneration; invited commentary: against treatment. Ophthalmology. 2000;107(1):15–16. doi:10.1016/S0161-6420(99)00066-4
12. Morris R, Witherspoon CD, Kuhn F, Sapp M. Retinal detachment laser prophylaxis (by invitation). Retina Today. 2008;2008:63–66.
13. Morris RE, Shere JL, Witherspoon DCCD, et al. Intraoperative retinal detachment prophylaxis in vitrectomy for retained cataract fragments. J Cataract Refract Surg. 2009;35(3):491–495. doi:10.1016/j.jcrs.2008.11.037
14. Little HL, Zweng HC, Peabody RR. Argon laser slit-lamp retinal photocoagulation. Trans Am Acad Ophthalmol Otolaryngol. 1970;74(1):85–97. PMID: 4985080.
15. Wilkinson CP. Evidence-based analysis of prophylactic treatment of asymptomatic retinal breaks and lattice degeneration. Ophthalmology. 2000;107(1):12–18. PMID: 10647712. doi:10.1016/s0161-6420(99)00049-4
16. American Academy of Ophthalmology Preferred Practice Pattern. Preferred practice guidelines. Posterior vitreous detachment, retinal breaks, and lattice degeneration. San Francisco, CA: American Academy of Ophthalmology; 2019. Available from: www.aao.org/ppp.
17. Ripandelli G, Rossi T, Cacciamani A, Scarinci F, Piaggi P, Stirpe M. Laser prophylactic treatment of the fellow eye in giant retinal tears: long-term follow-up. Retina. 2016;36(5):962–966. doi:10.1097/IAE.0000000000000805
18. Pollack A, Milstein A, Oliver M, Zalish M. Circumferential argon laser photocoagulation for prevention of retinal detachment. Eye. 1994;8(4):419–422. doi:10.1038/eye.1994.99
19. Bonnet M, Aracil P, Carneau F. Rhegmatogenous retinal detachment after prophylactic argon laser photocoagulation. Graefes Arch Clin Exp Ophthalmol. 1987;225(1):5–8. doi:10.1007/BF02155795
20. Koh HJ, Cheng L, Kosobucki B, Freeman WR. Prophylactic intraoperative 360° laser retinopexy for prevention of retinal detachment. Retina. 2007;27(6):744–749. doi:10.1097/IAE.0b013e318030ebd7
21. Verhoekx J, van Etten P, Wubbels R, van Meurs J, van Overdam K. Prophylactic laser treatment to decrease the incidence of retinal detachment in fellow eyes of idiopathic giant retinal tears. Retina. 2020;40(6):1094–1097. PMID: 30865062. doi:10.1097/IAE.0000000000002494
22. Sohn EH, Strohbehn A, Stryjewski T, et al. Posteriorly inserted vitreous base: preoperative characteristics, intraoperative findings, and outcomes after vitrectomy. Retina. 2020;40(5):943–950. PMID: 30883531; PMCID: PMC6697230. doi:10.1097/IAE.0000000000002482
23. Wang J, McLeod D, Henson DB, Bishop PN. Age-dependent changes in the basal retinovitreous adhesion. Invest Ophthalmol Vis Sci. 2003;44(5):1793–1800. PMID: 12714607. doi:10.1167/iovs.02-0802
24. Bouheraoua N, Hrarat L, Parsa CF, et al. Decreased corneal sensation and subbasal nerve density, and thinned corneal epithelium as a result of 360-degree laser retinopexy. Ophthalmology. 2015;122(10):2095–2102. doi:10.1016/j.ophtha.2015.06.010
25. Zauberman H, Berman ER. Measurement of adhesive forces between the sensory retina and the pigment epithelium. Exp Eye Res. 1969;8(3):276–283. PMID: 4240714. doi:10.1016/s0014-4835(69)80039-4
26. Hagler WS, Crosswell HH. Radial perivascular chorioretinal degeneration and retinal detachment. Trans Am Acad Ophthalmol Otolaryngol. 1968;72(2):203–216. PMID: 5659901.
27. Editors. “Burn” Merriam-WebsterDictionary. Available from: www.Merriam-Webster.com.
28. Editors. Carpet-Bomb “carpet bombing”. Merriam-WebsterDictionary. Available from: https://www.merriam-webster.com/dictionary/carpet-bomb.
29. TeixeiraTexeira A, Chong LP, Matsuoka N, et al. Vitreoretinal traction created by conventional cutters during vitrectomy. Ophthalmology. 2010;117(7):1387–1392. doi:10.1016/j.ophtha.2009.11.004
30. Tan HS, Mura M, De Smet MD. Iatrogeni25. c retinal breaks in 25-gauge macular surgery. Am J Ophthalmol. 2009;29(6):854–859.
31. Morris RE. Vitreous Opacity Vitrectomy (VOV): safest possible removal of “floaters”. Clin Ophthalmol. 2022;1(16):1653–1663. PMID: 35673347; PMCID: PMC9167598. doi:10.2147/OPTH.S361557
32. Falkner-Radler CI, Graf A, Binder S. Vitrectomy combined with endolaser or an encircling scleral buckle in primary retinal detachment surgery: a pilot study. Acta Ophthalmol. 2015;93(5):464–469. PMID: 25626910. doi:10.1111/aos.12663
33. Editors. The sword of damocles. Collins dictionary. Available from: https://www.collinsdictionary.com/us/dictionary/english/sword-of-Damocles.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Vitrectomy as a Prevention for Retinal Detachment in High-Risk Eyes

Morris RE, Kuhn F, Sapp MR, Chawla H
Clinical Ophthalmology 2025, 19:3249-3253
Published Date: 5 September 2025
Can Laser Retinopexy Prevent Retinal Detachment in Asymptomatic, High-Risk Eyes?

Morris RE, Sapp MR, Conn DR, Chawla H, Kuhn F
Clinical Ophthalmology 2025, 19:4011-4015
Published Date: 29 October 2025
A Historical Review of Encircling Laser Retinopexy as a Prophylaxis for Rhegmatogenous Retinal Detachment; and a Commentary on Recent Progress in Stickler Syndrome

Morris RE, Kuhn F, Oltmanns MH, West MR, Baxter CR, Sapp MR, Chawla H
Clinical Ophthalmology 2026, 20:588688
Published Date: 19 April 2026