Back to Journals » Clinical Ophthalmology » Volume 20
Encircling Laser Prophylaxis for Retinal Detachment in Stickler Syndrome: The Impact on Visual Field
Authors Fletcher DC, Schuchard RA, Morris RE ![]() , Kuhn F
, Kuhn F
Received 27 January 2026
Accepted for publication 2 July 2026
Published 14 July 2026 Volume 2026:20 599194
DOI https://doi.org/10.2147/OPTH.S599194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Supplementary video of “Encircling laser prophylaxis for retinal detachment” [599194].
Views: 20
Donald C Fletcher,1,2 Ronald A Schuchard,3 Robert E Morris,4 Ferenc Kuhn4,5
1Envision Low Vision Rehabilitation Center, Wichita, KS, USA; 2University of Kansas Medical Center, Department of Ophthalmology, KU Eye Center, Kansas City, KS, USA; 3Biotechnical Contract Consultant, Wichita, KS, USA; 4Helen Keller Eye Research Foundation, Birmingham, AL, USA; 5Department of Ophthalmology, University of Pécs, Pécs, Hungary
Correspondence: Robert E Morris, Helen Keller Eye Research Foundation, 2208 University Blvd., Suite 101, Birmingham, AL, 35233, USA, Tel +1 659 297 5577, Email [email protected]
Purpose: It is our purpose to address concerns regarding visual field loss as a barrier to optimal performance of encircling laser retinopexy as a prophylaxis for retinal detachment, especially when extended posteriorly, as in prophylaxis for retinal detachment in Stickler syndrome (SS).
Methods: We retrospectively analyzed visual field and visual acuity changes after encircling laser prophylaxis extending to the posterior edge of the vortex vein ampullae (ora secunda cerclage/Stickler syndrome, OSC/SS) in our first four SS patients who underwent such prophylaxis. We then used disability tables and validated patient questionnaires to characterize the extent of visual disability and/or symptoms resulting from such encircling prophylaxis.
Results: The reduction in peripheral visual field from OSC/SS posterior prophylaxis (to an average diameter of approximately 100 degrees in five treated eyes) was a far smaller percentage impairment (0– 21% by various estimations) than the 85% impairment from loss of both visual acuity and visual field after RD in the primary eye of a typical SS patient prior to fellow eye prophylaxis. Turano and NEI VFQ-25 Questionnaires both indicated that everyday mobility and travel visual tasks were not significantly affected by the laser prophylaxis.
Conclusion: Encircling laser retinopexy, extending posteriorly to and between the vortex vein ampullae, did not cause significant visual disability or any symptomatic visual field loss in an initial cohort of four patients with SS. Nor did we encounter any symptomatic visual field loss in 22 patients so treated subsequently. OSC/SS encircling laser prophylaxis safety and effectiveness is now being prospectively studied in a larger clinical trial (NCT07146516).
Keywords: 360-degree laser prophylaxis, retinal detachment prevention, Stickler syndrome, rhegmatogenous retinal detachment, ora secunda cerclage/Stickler syndrome, encircling laser prophylaxis
Introduction
Rhegmatogenous retinal detachment (RD) is the most common cause of sudden vision loss in seemingly normal eyes. It is usually caused by retinal tears from vitreous traction occurring in normal appearing peripheral retina (Figure 1). Encircling laser retinopexy applied to the peripheral retina by indirect ophthalmoscope (IDO) delivery (Video S1) increases retinal resistance to vitreous traction by 3-to-5-fold, protecting against such causative retinal tears.1
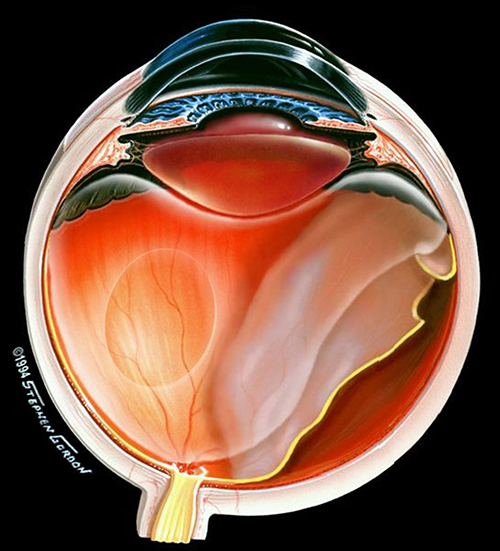 |
Figure 1 RD caused by a vitreous traction tear in normal appearing peripheral retina. Used with permission from Stephen Gordon © 2006. |
In 2008, we described uniform IDO laser grid treatment of the entire peripheral retina as an RD prophylaxis to create in effect a “second ora” (ora secunda) at the posterior edge of retinopexy. “Ora secunda cerclage” extended from the ora serrata approximately halfway to the vortex vein ampullae to prevent tears at the posterior vitreous base in non-syndromic fellow eyes.2
In January 2021, we described a successful protocol for IDO delivery of encircling laser retinopexy to prevent RD in Stickler syndrome (ora secunda cerclage/Stickler syndrome, OSC/SS).3 SS is the highest risk condition known to predispose eyes to retinal detachment, with a lifetime risk of more than 60% in affected individuals, usually involving both eyes.4
In SS, retinal detachment is often caused by multiple retinal tears occurring quite posteriorly (Supplementary Video 2).3,5 Thus, OSC/SS extends more posteriorly than had ever been described previously for encircling laser prophylaxis of RD, to and between the vortex vein ampullae (Figure 2).
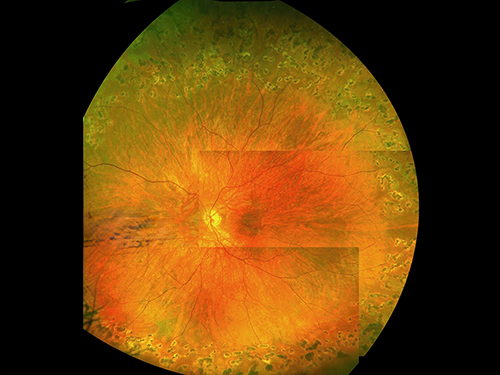 |
Figure 2 Montage image of OSC/SS encircling laser retinopexy, three months postoperative. One burn width grid spacing and moderate intensity burns are seen. The STQ vortex vein ampulla seen at 2 o’clock on the posterior edge of retinopexy is a landmark for the equator. The long ciliary nerve at 3 o’clock is spared treatment. Used with permission from Retina Specialists of Alabama, LLC. |
All encircling retinopexy prophylaxis involves a trade-off between an inevitable reduction in the peripheral visual field and increased security for the more important central visual field. However, there has been no previous analysis of the extent of such visual field reduction or its associated subjective symptoms. Here, we discuss in detail the effects of encircling laser prophylaxis on the visual field in this trade off (especially as it is extended posteriorly in SS) in a small initial sample pending results of our larger clinical trial (NCT07146516).
Consideration of the potential benefits versus the vision loss incurred is key to the general applicability of our recommendation of more posterior laser prophylaxis in Stickler syndrome. Is the sacrifice of peripheral visual field (from approximately 120-degrees to 100-degrees diameter, on Goldmann kinetic perimetry)3 warranted in exchange for the additional protection OSC/SS prophylaxis affords, against a substantial decrease in central vision or even the loss of all vision due to RD?
Methods
Herein, we performed a detailed analysis of the visual acuity and visual field changes in five eyes of the first four SS patients treated with the OSC/SS protocol and reported in less detail in our “technique” article in January 2021.3 The patients were a 53 year old father (genetically verified as SS type 2) and his three affected children whose ages were 22 years, 26 years, and 28 years when prophylactically treated. The father and the two youngest children each had suffered RD in one eye.
This retrospective case series study was determined to be exempt by the WCG Institutional Review Board, and was conducted in accordance with the tenets of the Declaration of Helsinki for research involving human subjects. Patients provided written informed consent for their case details to be published.
Corrected visual acuities were measured with a refraction performed within one year of testing, using a Snellen visual acuity chart. Postoperative visual fields were measured with a Marco Goldmann perimeter, using a 3-4-e stimulus, by a senior technician with more than 20 years’ experience in performing Goldmann kinetic perimetry; and myopia was corrected with a contact lens prescribed within one year of the examination.
Since the visual field implications of such posterior prophylaxis in SS were unknown, we initially divided prophylactic treatment into two sessions, first with anterior retinopexy protecting against giant retinal tears (GRT) at the ora that cause almost half of SS detachments. We then continued posteriorly in a second session months later if the initial laser treatment had been asymptomatic and the patient chose posterior extension in an attempt to achieve maximal protection. All patients were asymptomatic, and all chose maximal protection via second stage treatment.
Total treatment was typically between 1500 and 2500 burns in a one-burn-width grid extending to approximately the posterior edge of the vortex vein ampullae, while sparing the ampullae themselves (Figure 2). Laser application by IDO afforded stereopsis, wide angle observation, and dynamic scleral depression, enabling uniform treatment of the entire peripheral retina.
To demonstrate the value of prophylaxis versus the natural course of retinal detachment that occurs in the majority of untreated SS eyes,4 we analyzed the visual acuity and visual field changes attributable to OSC/SS prophylaxis in the fellow eye of a single patient typical of the cohort, compared to the changes in these parameters after retinal detachment repair in the primary eye. We then calculated the visual disability corresponding to the postoperative visual acuity and visual field in each eye of this patient using the American Medical Association (AMA) “Guides to the Evaluation of Permanent Impairment.”6
We also analyzed visual difficulties in mobility activities using validated questionnaires administered to all four initially treated SS patients. The questionnaires were administered by a professional with extensive experience and skills in gathering information from these surveys, who was blinded to the purpose of the study.
The instruments chosen were the Turano Questionnaire (Appendix A) and the NEI VFQ-25 Questionnaire (Appendix B).7,8 These validated questionnaires have been widely used in numerous vision-related, self-performance rating studies. The Turano Questionnaire consists of 35 ratings of mobility situations for assessment of mobility in people having visual impairments related to visual field loss. In addition, there are five questions on general impact of vision loss on travel situations.
It is understood that this first study of visual field changes due to encircling laser retinopexy is from a representative sample and does not imply statistical significance that awaits more robust data collection and analysis in our larger clinical trial (NCT07146516).
Results
In an analysis of the visual field loss associated with encircling laser prophylaxis versus the benefit, the experience gained from the four initially treated SS patients is particularly instructive.3
For our comparison of successful prophylaxis eyes and RD eyes, we used the daughter whose visual field and fundus images after OSC/SS prophylaxis are shown in Figure 3. She is typical of patients who have received OSC/SS laser prophylaxis for a fellow eye in Stickler syndrome after suffering RD in the first eye.9 And of the five initially treated eyes, her prophylaxis extended most posteriorly.
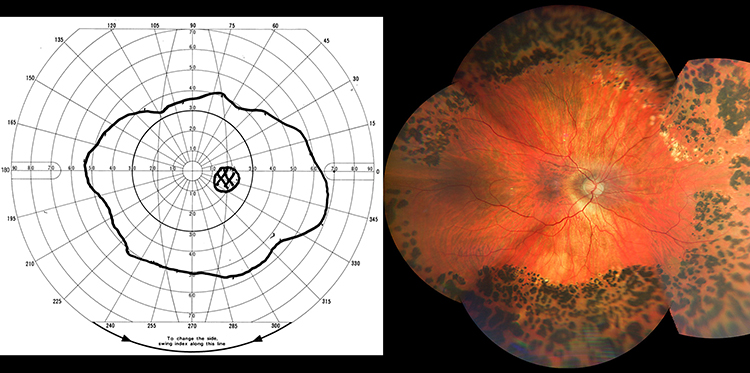 |
Figure 3 Visual field and fundus image of the fellow right eye post OSC/SS laser prophylaxis. Inferior retinopexy extends more centrally to treat posterior lattice degeneration. The 3 o’clock and 9 o’clock ciliary nerves are less intensley treated. Visual acuity is 20/30, as preoperatively, corrected with a refraction of −20.35 + 3.75 × 091. |
Her younger brother and father each had similar visual acuity and visual field findings in their fellow eyes after prophylaxis, and in their primary eyes after RD repair. All three patients of the cohort who developed RD in one eye in the absence of prophylaxis had suffered redetachment due to proliferative vitreoretinopathy before final reattachment, sustaining loss of visual acuity to a range of 20/125 to 6/200.
In the prophylactically treated right eye, she retained good visual acuity with correction, with a concentric, moderate constriction of the visual field to an approximate average of 100 degrees diameter on Goldmann kinetic perimetry.
Her left eye, status post RD repair, had corrected visual acuity of 20/125 and an even more constricted visual field with the expected fundus abnormalities (Figure 4). It is common for eyes not receiving prophylaxis and having a repaired RD in the primary eye to lose visual acuity and visual field to this level or worse in SS patients.9
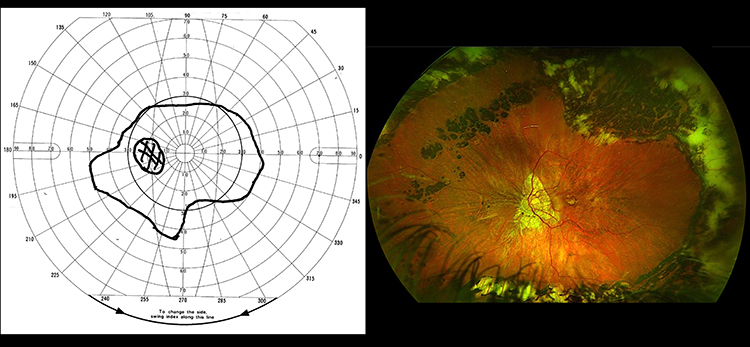 |
Figure 4 Visual field and fundus image of the primary left eye after retinal reattachment surgery. |
Disability Tables
Use of the AMA guides provides this comparison of each eye of the daughter (Figure 3):6
OSC/SS Eye
- Visual acuity corrected to 20/25 before prophylaxis is unchanged
- 105 degrees of lost peripheral visual field versus normal equates to 21% impairment of the affected eye attributable to prophylaxis
- (105-degree loss of a total possible 500 degrees of field along 8 meridians)
- 21% total impairment of the eye attributable to prophylaxis
RRD Eye
- 20/125 corrected visual acuity for distance and near equates to 74% impairment of the eye on the basis of visual acuity
- 210 degrees of lost peripheral visual field equates to 42% impairment of the eye on the basis of visual field
- (210-degree loss of a total possible 500 degrees of field along 8 meridians)
- Visual acuity and visual field combined for an 85% total impairment of the eye
Surveys
The four treated patients each participated in surveys with validated questionnaires as described in methods to provide their self-perceived difficulties with mobility tasks. Each of the four patients responded to all 40 questions in the Turano Questionnaire, making a total of 160 responses from the Turano Questionnaire. One hundred twenty of the 140 mobility items (35 of the 40 items) were assessed as “1” - no difficulty. Twelve of the 140 mobility items were assessed as “2” – a little difficulty. Eight of the 140 mobility items were rated as “3” – moderate difficulty. No items were rated as “4” or “5” (a lot of difficulty and extreme difficulty).
Individuals with typical age matched normal vision would provide responses of “1” or “2”. Two of the four patients rated all 35 of the mobility items as having no difficulty. In the significantly older of the other two patients, the “3” responses were consistently related to lighting changes (which is likely to not be related to the Stickler condition or the treatment). Research into vision and aging has demonstrated that as people age, they usually retain good high contrast, high illumination visual acuity but display loss of low-contrast, low-luminance acuity. The normal aging process would account for these scores.10
For the final patient, the “3” responses were consistently related to travel issues of avoiding obstacles, people or cars in open public spaces. There was no other consistent pattern of responses rated as moderate difficulty (eight responses) by the two patients. In addition, the responses to the five travel items indicated no impact of their vision loss on travel activities and no need for additional assistance (mobility aid or other people) to accomplish travel activities.
The NEI-VFQ 25 Questionnaire gave consistent responses indicating “no difficulty” to “limited difficulty” to the survey of problems which involve their vision and “none of the time” or “a little of the time” regarding feelings that their vision condition had affected their quality of life. In addition, little to no dissatisfaction with quality of life was reported for either questionnaire.
The list of NEI VFQ-25 questions that are relevant to doing everyday mobility and travel visual tasks related to peripheral vision are listed in the appendices. The answers to the mobility and travel related VFQ-25 items provided answers that were consistent to the Turano Questionnaire answers.
Discussion
The peripheral retina, most susceptible to development of retinal tears, is fortunately the area least important to vision. In eyes at high risk for retinal tears occurring predominately in normal appearing retina,2 peripheral encircling laser retinopexy (beyond focal retinopexy to visible predisposing lesions) is a logical procedure to increase security for the more important central retina.
A reduction in the peripheral visual field is an inevitable consequence of such prophylaxis. It is our purpose here to provide an initial analysis of concerns regarding visual field loss as a barrier to optimal performance of encircling laser prophylaxis, especially when extended posteriorly, as in OSC/SS prophylaxis. Additional analysis is part of an ongoing clinical trial (NCT07146516) of this encircling laser prophylaxis. In the absence of existent retinal tears, complications of encircling retinopexy are otherwise minimal if treatment is carefully performed.2,11,12
Encircling laser prophylaxis was largely ignored as a stand-alone prophylaxis for decades.2,13 However, through the successful SS experience,14 it has now become an important elective option (beyond observation or focal laser prophylaxis) for consideration by patients who are determined to be at high risk for retinal detachment, whatever the predisposing condition.15
Our “standard” laser prophylaxis technique is termed “Ora Secunda Cerclage” (OSC) because it produces in effect a “second ora” posterior to the vitreous base.11 It employs a grid of laser burns accurately spaced and powered with IDO delivery (Supplementary Video 1), strengthening chorioretinal adhesion by 3-to-5-fold throughout normal appearing peripheral retina.1
In SS, the resultant “ora secunda” is located even more posteriorly than standard OSC, to also prevent multiple tears that commonly occur more posteriorly than in non-syndromic eyes (OSC/SS, Figure 2).3,5 The vortex vein ampullae approximating the equator are landmarks for treatment of the entire pre-equatorial retina. In our 14-year OSC/SS experience, using this posterior treatment landmark has been sufficient to prevent the occurrence of any vitreous traction tear in 42 treated SS eyes (one atrophic defect with localized RD occurring in untreated retina).16 Focal treatment of predisposing lesions seen more posteriorly can also be considered.
Linton et al, warning of visual field loss from such posterior encircling retinopexy, limited prophylaxis to the ora serrata region to mimic the pioneering Cambridge encircling cryopexy treatment.4,17 Their shared goal was to prevent giant retinal tears (GRT) at the ora serrata that cause almost half of SS detachments.17 GRT detachments were completely eliminated and the RD rate was substantially reduced; however, laser treated eyes still suffered a 9% detachment rate, during an average 6.1 years of follow-up, from smaller tears more posteriorly, similarly to the Cambridge experience.4
A trend in all recent reports of SS encircling laser prophylaxis has been a lower failure rate (from 9% to 2.4%) as encircling retinopexy has been extended posteriorly.3,4,16–19 And it is likely that prophylaxis failure rates in SS eyes from tractional tears behind prophylaxis limited to the anterior periphery will increase significantly over decades of life expectancy beyond the brief follow-up periods currently reported.4,17 Nevertheless, encircling laser prophylaxis remains controversial as it is extended posteriorly.17,20
The AMA disability numbers reported above would indicate that the loss of peripheral field from OSC/SS posterior prophylaxis (Figure 2) is a far smaller impairment than the loss of visual acuity and reduction in visual field from RD in the absence of prophylaxis.6 This illustrates the value of prophylaxis in eyes determined to have an especially high risk of RD.
However, the AMA tables may actually overstate the functional impact of peripheral field loss from applying laser retinopexy to the entire pre-equatorial retina. If the patient’s visual field impairment from OSC/SS is rated using the Estermann 100-unit scoring grids,21 the resultant 100-degree diameter field seen in Figure 3 would score as a 0% impairment.
Thus, as reflected in Estermann scoring, peripheral visual field loss has far less functional significance than visual impairment of the central visual field.21 This assessment has recently been corroborated by Alexander Lam et al, using a virtual reality simulation system.22 Moreover, the first author has seen over 35,000 low vision patients in 39 years of full-time work in low vision rehabilitation. It has also been his observation that very few people with good visual acuity (better than 20/70) present seeking rehabilitation services before they have a concentric visual field constriction to less than a 30-degree diameter.
For example, many patients with advanced glaucoma or retinitis pigmentosa have no functional complaints with almost all daytime activities of daily living (ADL) until they have less than a 30-degree diameter field.23,24 As the visual field slowly constricts, affected patients learn compensatory strategies such as searching eye movements to scan their projected path, and function in almost all mobility tasks without incident.
Additionally, from the survey questionnaire findings and the fact that all four of the OSC/SS treated patients are driving with no accidents or citations on their driving records, it appears that there has not been a significant disruption of ADL that might be related to visual field constriction due to the more posterior laser prophylaxis treatment for SS.
In the absence of such prophylaxis, had any of the three RD-affected family members suffered a fellow eye retinal detachment with a functional result similar to their primary eye, they could easily have reached the legally blind impairment level. Not only did this not occur, but questionnaire responses indicate that the effect of having severely impaired vision in the primary eye from RD was largely masked by the remaining good vision in the OSC/SS treated fellow eye.23
In fact, several studies have shown that the better functioning eye has a stronger relationship with quality of life (QOL) than the worse seeing eye.23,25,26 This illustrates the critical need to effectively prevent retinal detachment in the fellow eye of SS patients who otherwise have an 80% chance of fellow eye RD at a young age, occurring at a median of only four years after first eye RD.4
Finally, the overwhelming importance of the central visual field versus the peripheral field may be further appreciated in that the macular region, despite corresponding to only the central 10 degrees of the human visual field, inputs to ~60% of the area of the visual cortex (whereas the peripheral 90 degrees of field inputs to ~40%), and hence is inordinately important for vision‑related QOL.23
Conclusion
Substantial retrospective evidence has accumulated during the last five years indicating that encircling laser retinopexy delivered by IDO is an effective prophylaxis for retinal detachment in SS.14,16 Our findings in this small but representative cohort indicate that the visual field loss from such encircling laser prophylaxis is typically minimal and asymptomatic, even when extended to the posterior margins of the vortex vein ampullae. Accordingly, we subsequently treated 37 additional eyes in 22 SS patients with OSC/SS, and we encountered no symptomatic visual field loss.16
The American Academy of Ophthalmology endorsed such “360-degree” (encircling or “cerclage”) laser prophylaxis for the first time in 2025, for genetically verified Stickler syndrome.27 A clinical trial is now underway at ten centers in the United States (NCT07146516) to prospectively document the extent to which OSC/SS prophylaxis prevents RD in type 1 and type 2 Stickler syndrome and to detect and document any instances of symptomatic visual field loss or treatment complications.
Because all rhegmatogenous retinal detachments share the predominate pathogenesis of peripheral vitreous traction tears, we expect that encircling laser retinopexy will ultimately gain ever wider acceptance as a safe and effective preventive option for other eyes determined to be at high risk, regardless of the predisposing condition.15,28–32 Moreover, by increasing peripheral retinal resistance to vitreous traction, it can enable the subsequent use of minimally invasive vitrectomy to reduce vitreous traction itself in selected cases.33
Abbreviations
IDO, Indirect ophthalmoscope; SS, Stickler syndrome; OSC/SS, ora secunda cerclage in Stickler syndrome; RD, retinal detachment; AMA, American Medical Association; GRT, giant retinal tear; ADL, activities of daily living; EMP, epimacular proliferation; QOL, quality of life.
Acknowledgments
The authors thank Dewayne Conn, senior technician at Retina Specialists of Alabama LLC, for performing all visual fields, and Terri Fletcher for decades of support in the field of vision rehabilitation research.
Funding
Partial funding was provided by the Helen Keller Eye Research Foundation, Birmingham, Alabama. The funding organization had no role in the design or conduct of this research.
Disclosure
The authors declare that they have no competing interests.
References
1. Zauberman H. Tensile strength of chorioretinal lesions produced by photocoagulation, diathermy, and cryopexy. Br J Ophthalmol. 1969;53(11):749–9. doi:10.1136/bjo.53.11.749
2. Morris RE, Kuhn F, Oltmanns MH, et al. A historical review of encircling laser retinopexy as a prophylaxis for rhegmatogenous retinal detachment; and a commentary on recent progress in Stickler syndrome. Clin Ophthalmol. 2026;20:588688. doi:10.2147/OPTH.S588688
3. Morris RE, Parma ES, Robin NH, et al. Stickler Syndrome (SS): laser prophylaxis for retinal detachment (Modified Ora Secunda Cerclage, OSC/SS). Clin Ophthalmol. 2021;15:19–29. doi:10.2147/OPTH.S284441
4. Alexander P, Fincham GS, Brown S, et al. Cambridge prophylactic protocol, retinal detachment, and Stickler syndrome. N Engl J Med. 2023;388(14):1337–1339. Mc2211320. PMID: 37018499. doi:10.1056/NEJ
5. Hagler WS, Crosswell HH. Radial perivascular chorioretinal degeneration and retinal detachment. Trans Am Acad Ophthalmol Otolaryngol. 1968;72(2):203–216. PMID 5659901.
6. Blais BG. AMA guides to the evaluation of ophthalmic impairment and disability. Am Med Assoc. 2011.
7. Turano KA, Geruschat DR, Stahl JW, et al. Perceived visual ability for independent mobility in persons with retinitis pigmentosa. Invest Ophthalmol Vis Sci. 1999;40(5):865–877.
8. Mangione CM, Lee PP, Gutierrez PR, et al. Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol. 2001;119(7):1050–1058. doi:10.1001/archopht.119.7.1050
9. Reddy DN, Yonekawa Y, Thomas BJ, et al. Long-term surgical outcomes of retinal detachment in patients with Stickler syndrome. Clin Ophthalmol. 2016;10:1531–1534. doi:10.2147/OPTH.S111526
10. Brabyn JA, Haegerstrom-Portnoy G, Schneck M, et al. Visual impairments in elderly people under everyday viewing conditions. J Visual Impairment Blindness. 2000;94(12):741–755. doi:10.1177/0145482X0009401202
11. Morris RE, Kuhn F, Richardson C. Preventing retinal detachment: the encircling laser retinopexy technique. Clin Ophthalmol. 2023;17:1505–1513. doi:10.2147/OPTH.S406337
12. Xie B, Lin Y, Lin C, et al. Epiretinal membrane formation following laser photocoagulation for peripheral retinal degeneration: incidence and risk factors. Eye. 2025;39(15):2768–2773. doi:10.1038/s41433-025-03945-5
13. Flaxel CJ, Adelman RA, Bailey ST, et al. Posterior vitreous detachment, retinal breaks, and lattice degeneration preferred practice pattern®. Ophthalmology. 2020;127(1):P146–P181. doi:10.1016/j.ophtha.2019.09.027
14. Camp DA, Bakhsh SR, Torkashvand A, et al. Laser prophylaxis for retinal detachment in Stickler syndrome: a systematic review and meta-analysis. Acta Ophthalmol. 2025;103(6):e364–e373. doi:10.1111/aos.17509
15. Morris RE, Kuhn F, Sipos T. Preventing retinal detachment: where are we? Implications from Stickler syndrome. Clin Ophthalmol. 2022;16:4315–4321. doi:10.2147/OPTH.S388631
16. Morris RE, Kuhn F, West MR, et al. RE: Camp DA, Bakhsh SR, Torkashvand A, et al. Laser prophylaxis for retinal detachment in Stickler syndrome: a systematic review and meta-analysis. Acta Ophthalmologica. 2025. PMID: 40370211. doi:10.1111/aos.17509
17. Linton E, Jalil A, Sergouniotis P, et al. Laser prophylaxis in Stickler syndrome: the Manchester Protocol. Retina. 2023;43(1):88–93. doi:10.1097/IAE.0000000000003634
18. Khanna S, Rodriguez SH, Blair MA, et al. Laser prophylaxis in patients with Stickler syndrome. Ophthalmol Retina. 2022;6(4):263–267. doi:10.1016/j.oret.2021.11.001
19. Naravane AV, Belin PJ, Pierce B, et al. Risk and prevention of retinal detachments in patients with Stickler syndrome. Ophthalmic Surg Lasers Imaging Retina. 2022;53(1):7–11. doi:10.3928/23258160-20211213-02
20. Berracol AM, Chang P. Diagnosing and managing Stickler syndrome, panel discussion. Retina Times. 2019.
21. Estermann B. Grid for scoring visual fields. II. Perimetry. Arch Ophthalmol. 1968;79(4):400–406. doi:10.1001/archopht.1968.03850040402007
22. Lam AKN, To E, Weinreb RN, et al. Use of virtual reality simulation to identify vision-related disability in patients with glaucoma. JAMA Ophthalmol. 2020;138(5):490–498. doi:10.1001/jamaophthalmol.2020.0392
23. Daruka R, Kuzhuppilly NIR, Dev S, et al. Correlation of central field index (10-2 visual field analysis) and activity limitation with increasing severity of glaucoma using glaucoma activity limitation-9 questionnaire. Indian J Ophthalmol. 2018;66(8):1098–1103. doi:10.4103/ijo.IJO_295_18
24. Sumi I, Matsumoto S, Okajima O, et al. The relationship between visual disability and visual scores in patients with retinitis pigmentosa. Jpn J Ophthalmol. 2000;44(1):82–87. doi:10.1016/s0021-5155(99)00171-9
25. Wandell PE, Lundström M, Brorsson B, et al. Quality of life among patients with glaucoma in Sweden. Acta Ophthalmol Scand. 1997;75(5):584–588. doi:10.1111/j.1600-0420.1997.tb00154.x
26. Sawada H, Fukuchi T, Abe H. Evaluation of the relationship between quality of vision and visual function in Japanese glaucoma patients. Clin Ophthalmol. 2011;5:259–267. doi:10.2147/OPTH.S16989
27. Kim SJ, Bailey ST, Kovach JL, et al. Posterior vitreous detachment, retinal breaks, and lattice degeneration preferred practice pattern®. Ophthalmology. 2025;132(4):P163–P196. doi:10.1016/j.ophtha.2024.12.023
28. Wallsh JO, Langevin ST, Kumar A, et al. Fellow-eye retinal detachment risk as stratified by hyaloid status on OCT. Ophthalmology. 2023;130(6):624–630. doi:10.1016/j.ophtha.2023.02.004
29. Morris RE, Kuhn F, West MR, et al. Re: Wallsh et al: fellow-eye retinal detachment risk as stratified by hyaloid status on OCT (Ophthalmology. 2023;130:624-630). Ophthalmology. 2023;130(12):e44–e45. doi:10.1016/j.ophtha.2023.08.014
30. Curran CD, Adams OE, Vagaggini T, et al. Prophylactic treatment of lattice degeneration in fellow eyes after repair of uncomplicated primary rhegmatogenous retinal detachment. Retina. 2024;44(1):63–70. doi:10.1097/IAE.0000000000003908
31. Morris RE, Kuhn F, Baxter CR, et al. Correspondence. Retina. 2025;45(12):e94–e95. doi:10.1097/IAE.0000000000004562
32. Morris RE, Sapp MR, Conn DR, et al. Can laser retinopexy prevent retinal detachment in asymptomatic, high-risk eyes? Clin Ophthalmol. 2025;19:4011–4015. doi:10.2147/OPTH.S537281
33. Morris RE, Kuhn F, Sapp MR, et al. Vitrectomy as a prevention for retinal detachment in high-risk eyes. Clin Ophthalmol. 2025;19:3249–3253. doi:10.2147/OPTH.S530665
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preventing Retinal Detachment: The Encircling Laser Retinopexy Technique

Morris RE, Kuhn F, Richardson C
Clinical Ophthalmology 2023, 17:1505-1513
Published Date: 30 May 2023
Can Laser Retinopexy Prevent Retinal Detachment in Asymptomatic, High-Risk Eyes?

Morris RE, Sapp MR, Conn DR, Chawla H, Kuhn F
Clinical Ophthalmology 2025, 19:4011-4015
Published Date: 29 October 2025
A Historical Review of Encircling Laser Retinopexy as a Prophylaxis for Rhegmatogenous Retinal Detachment; and a Commentary on Recent Progress in Stickler Syndrome

Morris RE, Kuhn F, Oltmanns MH, West MR, Baxter CR, Sapp MR, Chawla H
Clinical Ophthalmology 2026, 20:588688
Published Date: 19 April 2026