Back to Journals » Clinical Ophthalmology » Volume 19
Vitrectomy as a Prevention for Retinal Detachment in High-Risk Eyes
Authors Morris RE ![]() , Kuhn F, Sapp MR, Chawla H
, Kuhn F, Sapp MR, Chawla H
Received 26 March 2025
Accepted for publication 28 July 2025
Published 5 September 2025 Volume 2025:19 Pages 3249—3253
DOI https://doi.org/10.2147/OPTH.S530665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Morris.
Views: 269
Robert E Morris,1– 3 Ferenc Kuhn,1,4 Mathew R Sapp,1– 3 Harshvardhan Chawla1– 3
1Helen Keller Eye Research Foundation, Birmingham, AL, USA; 2Retina Specialists of Alabama, Birmingham, AL, USA; 3Department of Ophthalmology, University of Alabama at Birmingham, Birmingham, AL, USA; 4Department of Ophthalmology, University of Pécs Medical School, Pécs, Hungary
Correspondence: Robert E Morris, Helen Keller Eye Research Foundation, 2208 University Blvd. Suite 101, Birmingham, AL, 35233, USA, Tel +1 205 936-0704, Email [email protected]
Abstract: Rhegmatogenous retinal detachment (retinal detachment, RD) is the most common cause of spontaneous vision loss in aging eyes that were seeing normally until the moment of its occurrence. Causative retinal breaks usually occur in the form of peripheral tears at the vitreous base, resulting from traction exerted by the aging vitreous as it detaches posteriorly. Peripheral encircling laser retinopexy increases retinal resistance to vitreous traction in high-risk eyes. To achieve maximal lifetime prophylaxis, we show that in selected high-risk cases the vitreous can thereafter be removed by advanced vitrectomy techniques, reducing vitreous traction itself.
Plain Language Summary: Retinal detachment (RD) is a separation of the retinal layer from the back eye wall by passage of fluid through a retinal tear. It is analogous to wallpaper separating from a wall, and it is noticed as a sudden dark curtain developing in the field of vision. RD is the most frequent cause of spontaneous visual loss in aging eyes that have enjoyed normal vision until the moment of its occurrence.
This Perspective article and its supplementary case series describe a method of reducing RD risk in selected eyes by surgery (vitrectomy) to remove the mobile, aging vitreous gel (see Figure 1) that moves with body motion, causing retinal tears. We show that the risk of such a vitrectomy has plummeted from almost 40% in the 1970’s to less than 1% today. Along with prior laser “welding”, it thereafter results in an eye with the lowest possible lifetime risk of RD.
Keywords: retinal detachment, retinal detachment prevention, vitrectomy prophylaxis, encircling laser prophylaxis, iatrogenic retinal tears
Perspectives
Elective Vitrectomy
For five decades pars plana vitrectomy has been considered a risk factor for rhegmatogenous retinal detachment (retinal detachment, RD), resulting primarily from the complication of iatrogenic retinal tears. Retinal tears were reported to occur in 37% of cases during the 1970s,1 and vitrectomy was typically performed only for otherwise blinding injuries and disease.2
Because of this high risk of iatrogenic tears, elective (by choice or optional) vitrectomy, although now commonplace, only very gradually developed. For example, in 1980 Clarkson et al recommended performance of elective vitrectomy for a vitreous hemorrhage only if it failed to clear in six months.3
The most common indication for elective vitrectomy is macular pucker. A PubMed search recently garnered only seven reports of macular pucker surgery published during the entire decade of the 1970s. During the 1990s, approximately 167 such reports were published, and now more than that number are published annually, coinciding with a continued decrease in the iatrogenic tear complication (Figure 2).
 |
Figure 1 Vitrectomy prophylaxis following encircling laser prophylaxis. Preoperative, Intraoperative, and Postoperative. |
 |
Figure 2 Graphic display of publication chronology for elective macular pucker vitrectomy. |
By 1990, the iatrogenic tear rate had been reduced to approximately 5%.4 And after small gauge, cannulated vitrectomy became standard, the iatrogenic tear rate fell further to 1–2%.5 Moreover, wide field viewing systems made possible microscopic examination under anesthesia (mEUA) of the peripheral retina.6 Thus, both increasingly rare iatrogenic tears and existent predisposing lesions could be predictably discovered and treated by endolaser retinopexy.
Development of Vitreous Opacity Vitrectomy (VOV)
With this background in mind, we long ago became convinced that the suffering of patients with extensive, symptomatic vitreous opacities (“floaters”, 95% associated with posterior vitreous detachment, PVD)7 was real, substantial, and curable by vitrectomy.8 But elective vitrectomy for this then controversial indication required an iatrogenic tear rate as close to zero as possible.9
Thus began our assiduous quest to completely eliminate retinal traction and iatrogenic tears during vitreous removal;10 and to optimize discovery and prophylactic intraoperative treatment of existent predisposing conditions.11
We now pursue this ideal while performing vitreous opacity vitrectomy (VOV)8 using 27-gauge cannulated entry that protects the vitreous base, ultra-high speed cutting, a small aspiration port, minimal suction, vitreous staining as needed, and by avoiding proximity to the retina (vitreous base shaving) during vitreous removal.12 Our goal is to have all surgical traction end in the vitreous, never reaching the peripheral retina.
Immediately upon entry, the surgeon performs microscopic examination of the retina with endoillumination to identify previously undetected predisposing lesions. Meticulous, 360-degree peripheral retinal examination by the entire surgery team is repeated under high magnification at vitrectomy conclusion. Endoillumination and dynamic scleral depression are used to detect even microscopic defects, now in a vented eye that maintains set pressure even during scleral depression.13
Our intraoperative examination of the peripheral retina is better than was possible in the clinic preoperatively, and better than it will ever be postoperatively, enabling reliable discovery and retinopexy prophylaxis for predisposing lesions. Moreover, vitrectomy permanently reduces the vitreous mass and thus its lifetime traction potential. Intracameral antibiotic administration, reported to reduce the risk of endophthalmitis seven-fold to 0.03% in phacoemulsification, is a final safety measure for consideration in VOV vitrectomy.14
Vitrectomy Prophylaxis After Encircling Laser Prophylaxis
Two major research themes of the Helen Keller Eye Research Foundation have been refining encircling laser prophylaxis against retinal detachment (Figure 3), recently endorsed by the American Academy of Ophthalmology for Stickler syndrome,15–18 and as described above, developing vitreous opacity vitrectomy (VOV) as the safest possible curative procedure for extensive symptomatic vitreous opacities.8
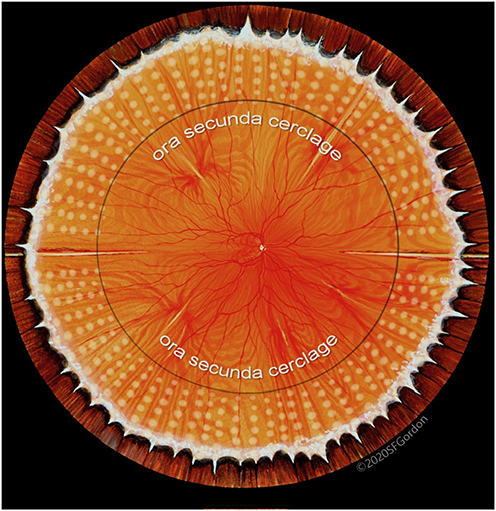 |
Figure 3 Encircling laser prophylaxis via the ora secunda cerclage technique. |
Serendipitously, these themes have now coalesced in the use of these same vitrectomy techniques,8 in selected pseudophakic eyes already having mature encircling laser prophylaxis and PVD, to reduce the lifetime risk of retinal detachment to an absolute minimum by eliminating vitreous traction in so far as safely possible (prophylactic vitrectomy, Figure 1). Although prophylactic vitrectomy can also be performed in eyes without PVD, one then assumes the risk associated with natural vitreous detachment at an earlier age than would otherwise occur; and if PVD is created, the obligation to accomplish PVD with less risk than would otherwise occur spontaneously.
Elective vitrectomy prophylaxis is highly dependent on individual patient preference and may include fellow eyes when the primary eye has previously lost macular function; or eyes of patients with Stickler syndrome in whom bilateral involvement is up to 80%.19 Such patients are usually quite knowledgeable of potential risks based on prior surgical experience and counseling. They are further counseled that our goal is achieving least possible lifetime risk, although the actual amount of RD risk reduction remains to be determined.
In effect, therefore, the techniques of vitreous opacity vitrectomy and prophylactic vitrectomy are identical. They share one goal and only one goal – to remove the central mass of vitreous as safely as possible – but for different reasons. In the former, it is to remove aging vitreous that has opacified. In the latter, it is to remove the mobile aging vitreous as a source of traction. From concept through execution, an imperative in both is to achieve a risk level as close to zero as possible in every step of surgery.
Conclusion
Unlike most vitrectomies in which vitreous removal is only a prelude to the main goal of retinal treatment, in prophylactic vitrectomy it is the “main act”, and it is performed accordingly. There is no intention to treat the retina. In fact, the opposite is true – the intention is to leave the retina undisturbed – although existent retinal breaks and lattice degeneration are diligently sought and strengthened while the opportunity to do so is uniquely available. Indeed, it is now finally possible to adopt intraoperative RD risk reduction as a secondary goal in “deep eye surgery”- reversing the long-standing fear of iatrogenic tears as the primary obstacle to the use of pars plana vitrectomy as an elective procedure.
The amount of RD risk reduction achievable by prophylactic vitrectomy remains to be determined. Zero risk for RD is unattainable, but the goal of prophylactic vitrectomy is to reduce the lifetime risk of RD relative to the same eye without vitrectomy, with an ancillary benefit of eliminating vitreous opacities. After 50 years of technological evolution, we have reached an inflection point, such that vitrectomy can now be considered as a selective prophylaxis addition after encircling retinopexy, rather than only as a risk factor for retinal detachment. A case series of prophylactic vitrectomy in high-risk eyes accompanies this article (supplement), each case with follow-up of at least five years. Included within the supplement is a video for Case 3 (Video S1) and Case 4 (Video S2).
Abbreviations
RD, rhegmatogenous retinal detachment; PVD, posterior vitreous detachment; VOV, vitreous opacity vitrectomy; mEUA, microscopic evaluation under anesthesia.
Consent for Publication
Each patient provided consent for the use of their unidentifiable medical information used in the supplemental case series. In addition, the figures were used with permission from artists Stephen Gordon and David Fisher, and from Retina Specialists of Alabama, LLC.
Acknowledgments
The authors thank Christina Sullivan MHA, Linda Laney RN, and Jessica Haynes for technical and clerical assistance.
Author Contributions
The concept of vitrectomy as a prophylaxis for RD was initiated by Drs. Morris and Kuhn in response to a call by organizers of the 2025 Vail Vitrectomy Symposium for completely novel presentations on pars plana vitrectomy, fifty years after its introduction by Dr Robert Machemer. It was presented by Dr Kuhn on February 8, 2025, to audience acclaim. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Partial funding was provided by the Helen Keller Eye Research Foundation.
Disclosure
The authors report no conflicts of interest with respect to this work.
References
1. Michels RG, Ryan SJ. Results and complications of 100 consecutive cases of pars plana vitrectomy. Am J Ophthalmol. 1975;80(1):24–29. PMID: 1155545.
2. Young PW, Shea M. Pars plana vitrectomy. Can J Ophthalmol. 1977;12(2):106–113. PMID: 880509.
3. Clarkson JG, Flynn HW, Daily MJ. Vitrectomy in Terson’s syndrome. Am J Ophthalmol. 1980;90(4):549–552. PMID: 7424753. doi:10.1016/s0002-9394(14)75027-5
4. Carter JB, Michels RG, Glaser BM, et al. Iatrogenic retinal breaks complicating pars plana vitrectomy. Ophthalmology. 1990;97(7):848–53; discussion 854. PMID: 2381696. doi:10.1016/s0161-6420(90)32492-2
5. Chen GH, Tzekov R, Jiang FZ, et al. Iatrogenic retinal breaks and postoperative retinal detachments in microincision vitrectomy surgery compared with conventional 20-gauge vitrectomy: a meta-analysis. Eye. 2019;33(5):785–795. PMID: 30560911; PMCID: PMC6707291. doi:10.1038/s41433-018-0319-5
6. Morris RE. Floater stories: assessing the potential benefits of vitrectomy. Clin Ophthalmol. 2024;18:1651–1654. PMID: 38855015; PMCID: PMC11162631. doi:10.2147/OPTH.S460876
7. Morris RE, Witherspoon CD, Kimble J, et al. Vitreous Opacity Vitrectomy (VOV) for Degenerative Vitreous Syndrome (DVS) – let’s talk about floaters.
8. Morris RE. Vitreous Opacity Vitrectomy (VOV): safest possible removal of “Floaters”. Clin Ophthalmol. 2022;16:1653–1663. PMID: 35673347; PMCID: PMC9167598. doi:10.2147/OPTH.S361557
9. Cohen MN, Rahimy E, Ho AC, et al. Management of symptomatic floaters: current attitudes, beliefs, and practices among vitreoretinal surgeons. Ophthalmic Surg Lasers Imaging Retina. 2015;46(8):859–865. PMID: 26431302. doi:10.3928/23258160-20150909-11
10. Ng E, Masalkhi M, Steel DH, et al. Twenty-seven-gauge vitrectomy: a consecutive, single-centre case series with exclusive use over a 4-year period. BMC Ophthalmol. 2023;23(1):518. PMID: 38129776; PMCID: PMC10734045. doi:10.1186/s12886-023-03265-w
11. Foos RY. Tears of the peripheral retina; pathogenesis, incidence and classification in autopsy eyes. Mod Probl Ophthalmol. 1975;15:68–81. PMID: 1160919.
12. Texeira A, Chong LP, Matsuoka N, et al. Vitreoretinal traction created by conventional cutters during vitrectomy. Ophthalmology. 2010;117(7):1387–1392.e2. PMID: 20176400. doi:10.1016/j.ophtha.2009.11.004
13. Witherspoon CD, Morris RE, Goggans WE. Automated regulation of fluid infusion pressure during vitrectomy. Arch Ophthalmol. 1986;104(10):1551. doi:10.1001/archopht.1986.01050220145044
14. Vieira IV, Boianovsky C, Saraiva TJ, et al. Safety and efficacy of intracameral moxifloxacin injection for prophylaxis of endophthalmitis after phacoemulsification. Arq Bras Oftalmol. 2017;80(3):165–167. PMID: 28832735. doi:10.5935/0004-2749.20170040
15. Kim SJ, Bailey ST, Kovach JL, et al; American Academy of Ophthalmology Preferred Practice Pattern Retina/Vitreous Committee. Posterior vitreous detachment, retinal breaks, and lattice degeneration preferred practice pattern®. Ophthalmology. 2025;132:P163–P196. PMID: 39918519. doi:10.1016/j.ophtha.2024.12.023
16. Morris RE, Parma ES, Robin NH, et al. Stickler Syndrome (SS): laser prophylaxis for retinal detachment (Modified Ora Secunda Cerclage, OSC/SS). Clin Ophthalmol. 2021;15:19–29. PMID: 33447008; PMCID: PMC7802593. doi:10.2147/OPTH.S284441
17. Morris RE, Kuhn F, Sipos T. Preventing retinal detachment: where are we? Implications from stickler syndrome. Clin Ophthalmol. 2022;16:4315–4321. PMID: 36583093; PMCID: PMC9793794. doi:10.2147/OPTH.S388631
18. Morris RE, Kuhn F, Richardson C. Preventing retinal detachment: the encircling laser retinopexy technique. Clin Ophthalmol. 2023;17:1505–1513. PMID: 37273500; PMCID: PMC10239236. doi:10.2147/OPTH.S406337
19. Fincham GS, Pasea L, Carroll C, et al. Prevention of retinal detachment in Stickler syndrome: the Cambridge prophylactic cryotherapy protocol. Ophthalmology. 2014;121(8):1588–1597. PMID: 24793526. doi:10.1016/j.ophtha.2014.02.022
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preventing Retinal Detachment: The Encircling Laser Retinopexy Technique

Morris RE, Kuhn F, Richardson C
Clinical Ophthalmology 2023, 17:1505-1513
Published Date: 30 May 2023
Can Laser Retinopexy Prevent Retinal Detachment in Asymptomatic, High-Risk Eyes?

Morris RE, Sapp MR, Conn DR, Chawla H, Kuhn F
Clinical Ophthalmology 2025, 19:4011-4015
Published Date: 29 October 2025