Back to Journals » Journal of Inflammation Research » Volume 18
Bowel Urgency in Ulcerative Colitis is Independently Associated with Histologic Inflammation and Stool Form Despite Endoscopic Remission
Authors Wei ZH, Chen TD ![]() , Chou JW, Lin SH
, Chou JW, Lin SH ![]() , Huang TY, Chang CW, Chiu CT, Chen CM
, Huang TY, Chang CW, Chiu CT, Chen CM ![]() , Kuo T, Su MY, Pan YB
, Kuo T, Su MY, Pan YB ![]() , Le PH
, Le PH ![]()
Received 25 June 2025
Accepted for publication 10 September 2025
Published 8 October 2025 Volume 2025:18 Pages 13897—13906
DOI https://doi.org/10.2147/JIR.S549513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Nadia Andrea Andreani
Zih-Hao Wei,1 Tai-Di Chen,2,3 Jen-Wei Chou,4– 6 Shih-Hua Lin,3,4,7 Tien-Yu Huang,4,8 Chen-Wang Chang,4,9– 11 Cheng-Tang Chiu,3,4,12– 14 Chien-Ming Chen,3,15 Tony Kuo,3,4,13 Ming-Yao Su,3,4,7,14 Yu-Bin Pan,16 Puo-Hsien Le3,4,12– 14,17
1Department of Medical Education, Taichung Veterans General Hospital, Taichung, Taiwan; 2Department of Pathology, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, Taiwan; 3Chang Gung Inflammatory Bowel Disease Center, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan; 4Taiwan Association for the Study of Intestinal Diseases (TASID), Taoyuan City, Taiwan; 5Center for Digestive Medicine, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan; 6School of Chinese Medicine, China Medical University, Taichung, Taiwan; 7Division of Gastroenterology and Hepatology, Department of Internal Medicine, New Taipei Municipal Tucheng Hospital, Tucheng, New Taipei City, Taiwan; 8Division of Gastroenterology and Hepatology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan; 9Division of Gastroenterology, Department of Internal Medicine, MacKay Memorial Hospital, Taipei, Taiwan; 10MacKay Junior College of Medicine, Nursing and Management, Taipei, Taiwan; 11College of Medicine, MacKay Medical College, New Taipei City, Taiwan; 12Chang Gung Microbiota Therapy Center, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan; 13Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan; 14College of Medicine, Chang Gung University, Taoyuan, Taiwan; 15Department of Medical Imaging and Interventions, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, Taiwan; 16Biostatistical Section, Clinical Trial Center, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan; 17Chang Gung Liver Research Center, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
Correspondence: Puo-Hsien Le, Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou Branch, 5, Fu-Hsin Street, Guei-Shan District, Taoyuan City, 33305, Taiwan, Tel +886 3 3281200 ext 8101, Fax +886 3 3272236, Email [email protected]
Background: Bowel urgency (BU) is a distressing symptom in patients with ulcerative colitis (UC), yet its associations with disease activity and patient-reported outcomes remain unclear. This study aimed to provide the first comprehensive evaluation of these relationships.
Materials and Methods: Between September 2024 and March 2025, we enrolled 100 patients with UC. Patients were stratified into two groups based on the Urgency Numeric Rating Scale (NRS): bowel urgency–active (BU-A; NRS > 1) and bowel urgency–remission (BU-R; NRS ≤ 1). Clinical parameters including the partial Mayo score, Mayo endoscopic subscore (MES), Nancy Index (NI), Bristol Stool Form Scale (BSFS), and IBD Disk score were evaluated. Logistic regression analyses were performed to identify independent predictors of active BU.
Results: 50 patients were in BU-A, and 50 in BU-R. Endoscopic remission (MES=0) occurred in 14% of BU-A and 34% of BU-R; Histological remission (NI = 0) in 10% and 36%, respectively. Stool consistency was predominantly normal (Bristol types 3– 5) in both groups (60% of BU-A, 72% of BU-R); however, type 6– 7 stools were significantly more frequent in the BU-A group (36% vs 6%, P < 0.001). The BU-A group also had significantly higher partial Mayo scores, MES, NI, and total IBD Disk scores (25.3 ± 20.0 vs 12.0 ± 14.9, P < 0.001). In multivariate analysis, higher NI (OR: 1.874; 95% CI: 1.277– 2.750; P < 0.001) and BSFS score (OR: 1.499; 95% CI: 1.052– 2.137; P = 0.025) were independently associated with active BU.
Conclusion: Histological inflammation and loose stool form were identified as independent predictors of BU. BU may persist despite endoscopic or histological remission and normal stool form, warranting targeted evaluation beyond traditional marker of disease activity.
Plain Language Summary: Summarize the established knowledge on this subjectBowel urgency (BU) is a frequent, distressing symptom of ulcerative colitis (UC) that markedly impairs quality of life.The precise links between BU, objective disease activity, and patient-reported outcomes remain unclear.
What are the significant and/or new findings of this study?Active histological inflammation and loose stool form are independent predictors of BU.BU can persist despite simultaneous endoscopic and histological remission and normal stool consistency, revealing a symptom burden not captured by conventional indices.Recognising BU as an independent treatment target supports more personalised, patient-centred management strategies and may translate into measurable gains in quality of life.
Keywords: ulcerative colitis, bowel urgency, patient-reported outcomes
Introduction
Ulcerative colitis (UC) is a chronic, relapsing inflammatory disorder of the gastrointestinal tract that frequently manifests with symptoms such as rectal bleeding, increased stool frequency, and bowel urgency (BU).1 BU, also referred to as fecal urgency, is defined as a sudden or immediate need to defecate.2 Among the various symptoms of UC, BU is considered one of the most distressing, with profound impacts on patients’ quality of life and psychosocial well-being.3–6
The majority of patients with UC, including those undergoing treatment, report experiencing BU.7 Previous cross-sectional and observational studies have shown that over 80% of UC patients experience BU.2,7–10 Moreover, BU is a major contributor to treatment dissatisfaction and is among the symptoms patients most wish to see improved.4,8,11 Despite its substantial clinical burden, BU is frequently underreported by patients, often due to embarrassment, and may be insufficiently addressed by clinicians because of limited familiarity with validated assessment instruments or an underestimation of its clinical significance.4,8,11,12
Although several studies have suggested associations between BU and disease activity, quality of life, psychological burden, clinical outcomes, and inflammatory biomarkers in UC,3,13–15 the methods used to assess BU have been inconsistent and largely unvalidated. The recent development of the Urgency Numeric Rating Scale (NRS) has introduced a standardized and reliable tool to quantify BU severity in UC patients.16 Nonetheless, comprehensive evaluations of BU in relation to a broad spectrum of clinical and patient-reported outcomes (PRO) remain scarce.
To address this gap, the present study aimed to investigate the associations between BU and multiple clinical parameters in patients with UC, including disease activity indices, endoscopic and histological findings, stool patterns, and health-related quality of life assessed by the validated IBD Disk. In addition, we examined the correlations between Urgency NRS and the Bristol Stool Form Scale (BSFS), clinical disease activity, and IBD Disk scores.
Materials and Methods
Study Design and Participants
We conducted a questionnaire-based study in adult patients with a confirmed diagnosis of UC. Participants were recruited from the Chang Gung Inflammatory Bowel Disease Center between September 2024 and March 2025. Eligible patients were those receiving regular follow-up care at the center. Regular follow-up was defined as outpatient visits scheduled according to disease activity and the treating physician’s clinical assessment, typically every 1–2 months for patients with active UC and every 2–6 months for those in remission, with shorter intervals when warranted by symptom changes or treatment modifications. Patients with incomplete questionnaires or a history of colorectal cancer surgery were excluded. Trained IBD nurse coordinators provided personalized instructions to patients in the outpatient department to facilitate questionnaire completion. The average time required to complete the questionnaire was 15–20 minutes, yielding a completion and return rate of over 90%.
Data Collection
Demographic and clinical data, including age, sex, body mass index (BMI), and disease extent (classified according to the Montreal classification), were collected. Disease activity was evaluated using the partial Mayo score, the Mayo endoscopic subscore (MES), and the Nancy Index (NI). Sigmoidoscopy or colonoscopy was performed to determine the MES of the rectosigmoid colon. The questionnaire was completed within one month of the endoscopic examination, which served as the index date for clinical correlation.
Histological activity was assessed from rectal biopsy specimens. When endoscopic inflammation was evident, targeted biopsies were obtained from the most severely inflamed rectal areas; if no visible inflammation was present, random biopsies were taken from the rectum. Endoscopic activity (MES) and histological activity (NI) were evaluated solely on rectal findings, irrespective of proximal colonic involvement.
Clinical remission was defined as a partial Mayo score ≤ 1, with no individual subscore > 1. Endoscopic remission was defined as a MES of 0, indicating normal or inactive mucosa. Histological remission was defined as a NI of 0, reflecting the absence of both acute and chronic inflammatory infiltrates. Laboratory data, including serum albumin and C-reactive protein (CRP) levels, were collected.
Current medication use was documented, including 5-aminosalicylic acid (5-ASA), immunosuppressants, corticosteroids, biologics, topical therapies, and treatments for irritable bowel syndrome (IBS). Duration of clinical follow-up was recorded. Immunosuppressant therapy consisted of azathioprine. Biologic therapies included anti–tumor necrosis factor agents (infliximab, adalimumab), an anti-integrin agent (vedolizumab), and an anti–interleukin-12/23 agent (ustekinumab). Topical treatments comprised 5-aminosalicylate enemas and hydrocortisone enemas. For patients with IBS, pharmacologic management included antispasmodics (eg, mebeverine) for abdominal pain and bloating, and osmotic (eg, polyethylene glycol) or bulk-forming laxatives for constipation-predominant symptoms, when clinically indicated.
Stool consistency was assessed using the BSFS, which categorizes stool into seven types.17 BU severity was quantified using the validated NRS, an 11-point scale ranging from 0 (no urgency) to 10 (worst possible urgency).16 Quality of life (QoL) and functional status were evaluated using the IBD Disk, a validated PRO instrument,18 which encompasses 10 domains: abdominal pain, regulation of defecation, interpersonal interactions, education and work, sleep, energy, emotions, body image, sexual function, and joint pain.
Statistical Analysis
Continuous variables were reported as means ± standard deviation (SD) and compared using Student’s t-test. Categorical variables were presented as counts and percentages, with comparisons made using the chi-square test or Fisher’s exact test, as appropriate. Logistic regression analysis was performed to identify independent predictors of BU. Variables with a P value < 0.05 in univariate analysis were included in a multivariate model. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. A P value < 0.05 was considered statistically significant. All analyses were conducted using SPSS software, version 26 (IBM Corp., Armonk, NY).
Results
Baseline Characteristics
Our study enrolled 100 UC patients at Chang Gung Memorial Hospital, Linkou, between September 2024 and March 2025. The mean age of participants was 44.8 years, and 66% were male. The mean duration since UC diagnosis was 77 months, and nearly half of the patients (47%) had pancolitis (Montreal E3). None of the enrolled patients had undergone colorectal surgery. Participants were categorized into two groups based on their Urgency NRS scores: an active BU group (BU-A; NRS > 1, n = 50) and a BU remission group (BU-R; NRS ≤ 1, n = 50).16,19 The mean Urgency NRS was significantly higher in BU-A than in BU-R (4.2 ± 2.0 vs 0.2 ± 0.4, P < 0.001). Disease activity indicators, including the partial Mayo score, MES, and NI, were significantly higher in BU-A compared to BU-R. Overall, 24 patients achieved endoscopic remission (MES = 0), comprising 7 patients (14%) in the BU-A group and 17 (34%) in the BU-R group. Similarly, histological remission (NI = 0) was observed in 23 patients, including 5 patients (10%) in BU-A and 18 (36%) in BU-R. Stool consistency also differed significantly between the two groups: the mean BSFS was 4.7 ± 1.5 in BU-A versus 3.6 ± 1.3 in BU-R (P < 0.001). Both groups predominantly had normal stool form (Bristol types 3–5), accounting for 60% of BU-A and 72% of BU-R. However, the BU-A group had a higher proportion of type 6–7 stools, indicating a greater tendency toward diarrhea. Baseline characteristics of the two groups are summarized in Table 1, and the stool pattern distribution is illustrated in Figure 1.
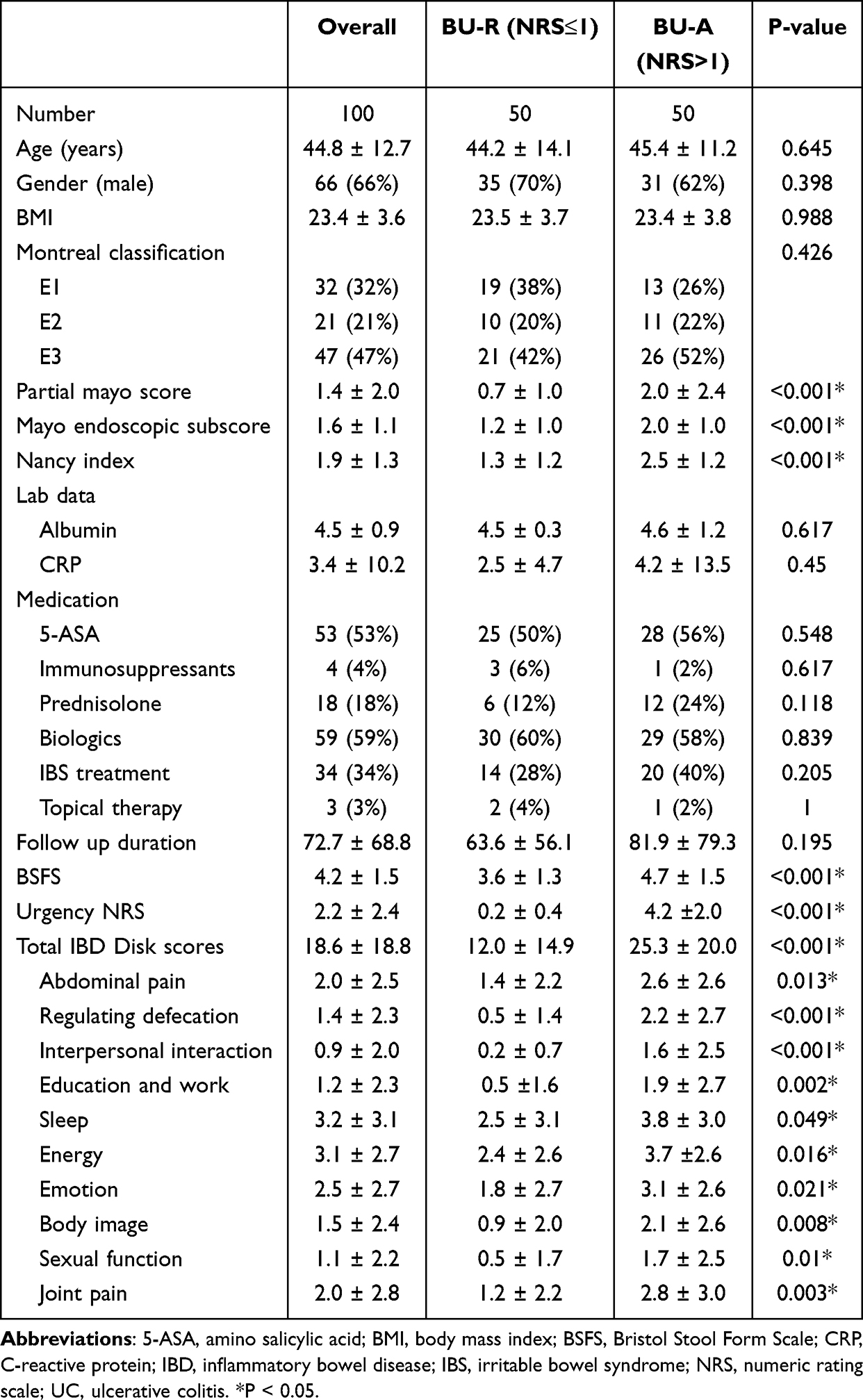 |
Table 1 Baseline Characteristics of UC Patients with BU Remission (BU-R) Versus BU Active (BU-A) |
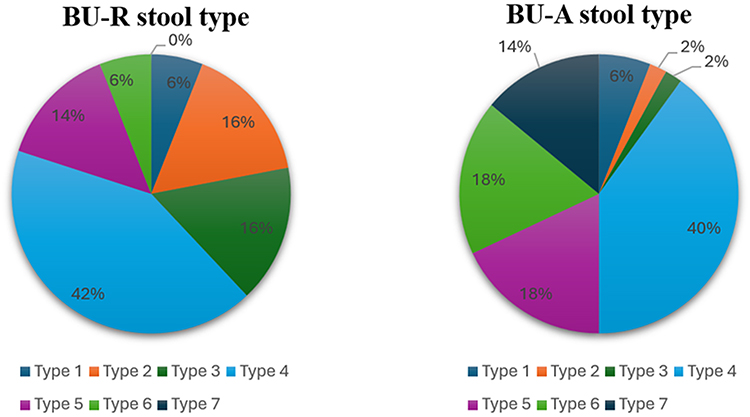 |
Figure 1 Stool Pattern Distribution in BU-R and BU-A Groups, Categorized by Bristol Stool Form Scale. Pie charts show the percentage distribution of Bristol Stool Form Scale types among patients in the BU-R and BU-A groups. |
IBD Disk Scores
Patients in the BU-A group had significantly higher total IBD Disk scores than those in the BU-R group (25.3 ± 20.0 vs 12.0 ± 14.9, P < 0.001), reflecting greater impairment in quality of life. The distribution of total IBD Disk scores for both groups is shown in Figure 2. Analysis of IBD Disk components revealed marked differences between the groups: the BU-A group scored higher in abdominal pain (2.6 ± 2.6 vs 1.4 ± 2.2, P = 0.013) and in the regulating defecation domain (2.2 ± 2.7 vs 0.5 ± 1.4, P < 0.001). Similar trends were observed in other domains, including interpersonal interactions, sleep, energy, emotion, body image, sexual function, and joint pain, where BU-A patients consistently had worse outcomes (P < 0.05 for all). These findings underscore the association between BU and impairments across multiple quality-of-life domains.
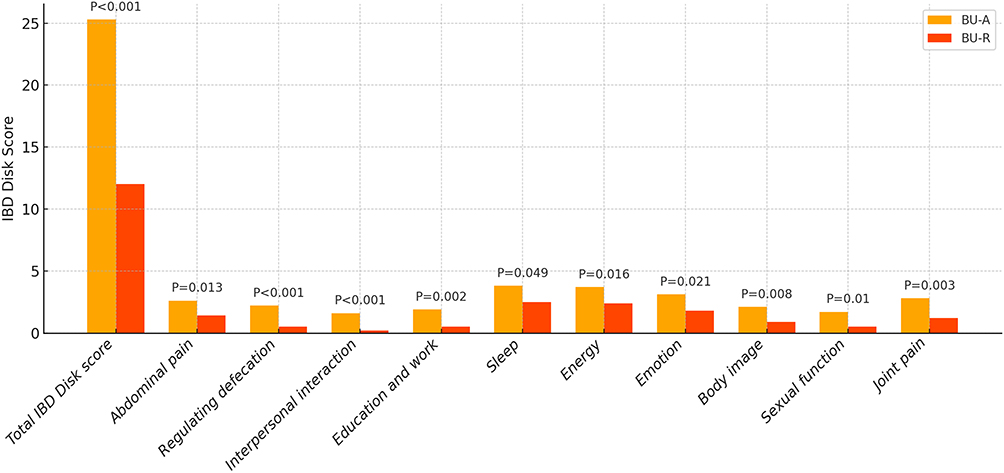 |
Figure 2 Comparison of Total IBD Disk Scores and Component Domain Scores Between BU-R and BU-A Groups. The bar graph demonstrates that the BU-A group exhibited significantly higher total IBD Disk scores, as well as elevated scores across multiple individual domains, compared with the BU-R group (P < 0.001). |
Independent Factor of BU
To identify independent factors associated with BU, variables with P < 0.05 in the univariate analysis were entered into a multivariate logistic regression. This analysis identified the NI (OR = 1.91, 95% CI: 1.319–2.764, P < 0.001) and stool pattern (OR = 1.499, 95% CI: 1.052–2.137, P = 0.025) as independent predictors of BU. Detailed results of the univariate and multivariate analyses are presented in Table 2.
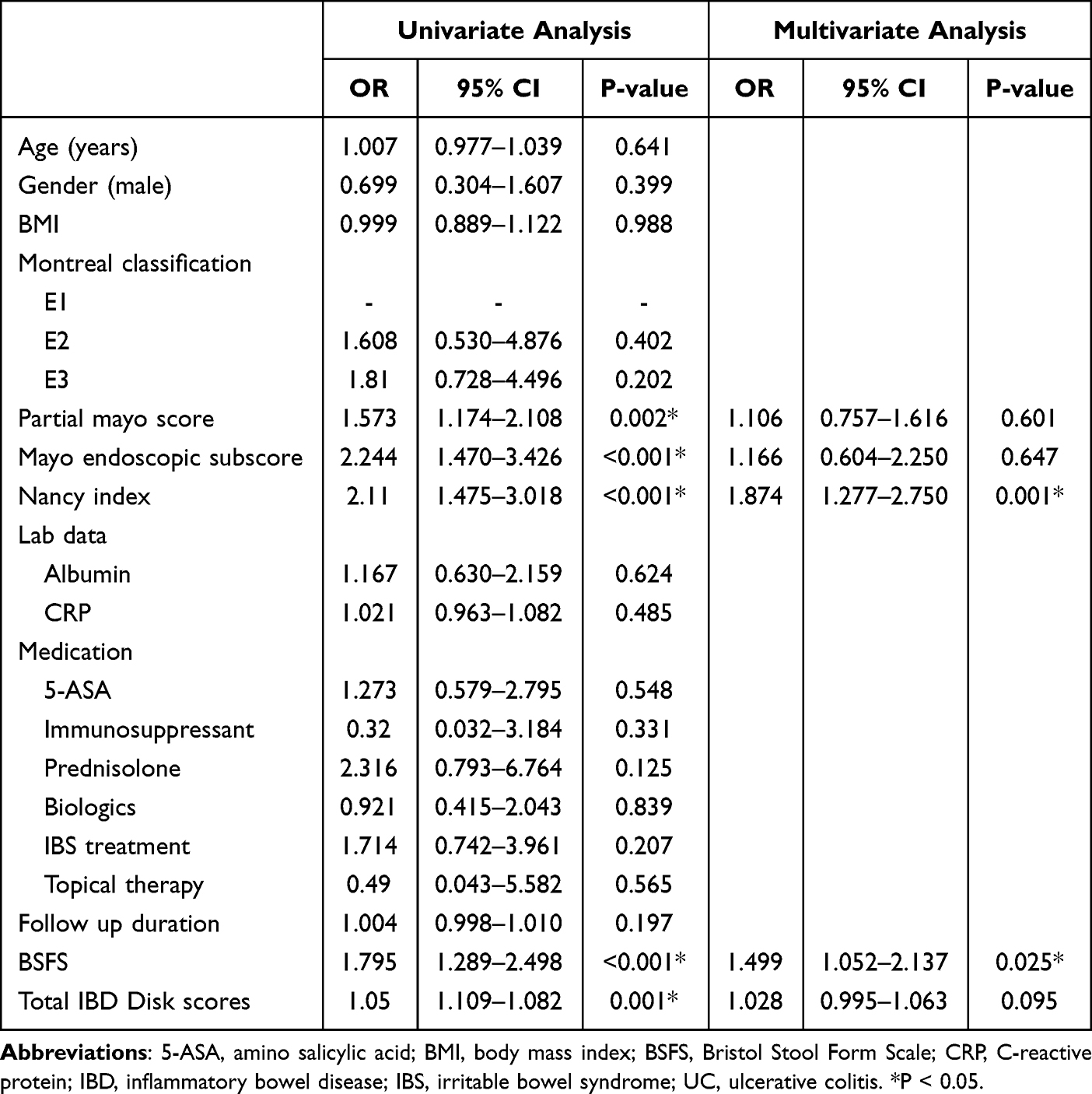 |
Table 2 Independent Factors of Bowel Urgency in UC Patients |
Discussion
BU is defined as a sudden or immediate need for a bowel movement2 and is one of the most distressing symptoms for patients with UC, significantly affecting their quality of life and psychosocial well-being.3–6 BU and urgency-related fecal incontinence have also been associated with a higher risk of colectomy, increased corticosteroid use, and a greater likelihood of hospitalization.3 Nevertheless, the assessment of BU has not been formally recommended as an endpoint in UC clinical trials or real-world studies, and it remains frequently overlooked during drug approval and registration processes.6 Furthermore, BU is not included in most UC disease activity indices, despite being a symptom with considerable impact on patients’ daily lives.20,21
A principal finding of our study was the strong association between histological inflammation and BU. Histologic remission was achieved in 34% of patients in the BU-R group but in only 10% of those in the BU-A group. Furthermore, histological activity, rather than endoscopic or clinical indices, emerged as an independent predictor of BU in our multivariate analysis. These findings are consistent with prior evidence underscoring a close link between intestinal inflammation and the presence of urgency.16 Active inflammation leads to rectal hypersensitivity, which accelerates transit through the sigmoid colon and disrupts normal rectal motility. In addition, impaired rectal wall function and reduced distensibility lower rectal capacity. As a result, even small volumes of stool can raise intrarectal pressure and trigger the sensation of urgency.22,23 Chronic inflammation may cause thickening of the muscularis mucosae and increased submucosal fibrosis, which can impair rectal wall compliance and contribute to the development of BU.24 Although previous studies have suggested that achieving BU remission may be associated with endoscopic remission,25 our findings indicate that histologic remission may better reflect true resolution of inflammation at the tissue level and thus serve as a more reliable marker for symptom control. Although current treatment guidelines, such as STRIDE-II, define endoscopic remission as the primary therapeutic target,26 emerging evidence suggests that histological remission is associated not only with improved clinical outcomes in UC27 but also with a reduction in BU, thereby enhancing patients’ quality of life. As such, histological remission may represent a meaningful future therapeutic target.
Stool form also played an important role in the expression of BU. Patients in the BU-A group had significantly looser stools than those in the BU-R group (mean BSFS 4.7 ± 1.5 vs 3.6 ± 1.3, P < 0.001), paralleling a higher inflammatory burden (mean NI 2.5 ± 1.2 vs 1.3 ± 1.2, P < 0.001). In active inflammation, stool consistency becomes looser and stool weight increases, likely due to exudation from the inflamed epithelium, increased mucus secretion, and reduced fluid and electrolyte absorption.28 Looser stool forms often reflect shorter colonic transit times and higher water content, which can overwhelm rectal capacity, especially in inflamed or hypersensitive mucosa, thereby triggering urgency.8,17,28,29 Monitoring stool type may therefore be a valuable tool in assessing the presence and severity of BU.
Importantly, our data revealed that BU can persist despite histological remission and normal stool patterns. Notably, 60% of patients in the BU-A group had normal stools (Bristol types 3–5),30 and a small subset even met histologic remission criteria. This disconnect suggests that the pathogenesis of BU involves factors beyond inflammation and stool form. Potential contributors include residual low-grade inflammation, altered rectal compliance, anorectal hypersensitivity, and psychosocial influences, which may account for the persistence of BU despite formed stools.
The potential contribution of topical therapy in these patients also warrants further investigation. A prospective study found that both active and quiescent UC patients have reduced rectal compliance compared to healthy controls.31 This finding implies that UC may be a progressive condition and that decreased rectal compliance might not fully normalize even after inflammation is controlled, although effective disease management could potentially improve compliance. Another possible explanation is that anal sphincter fatigability and altered brain-gut signaling may persist after inflammatory control is achieved.32–34 These observations challenge the paradigm that resolution of inflammation alone is sufficient to alleviate all UC symptoms and underscore the need for a broader evaluation of persistent symptoms like BU.
The persistence of BU despite remission further highlights the importance of psychosocial and functional factors. Negative emotions such as anxiety and stress may exacerbate BU by heightening visceral sensitivity through the brain-gut axis—a complex, bidirectional system involving interactions between neuroendocrine pathways, the autonomic nervous system, and the gastrointestinal tract.32,34 Prior studies have shown that BU causes significant embarrassment, fear of incontinence, and avoidance of social activities, compounding the psychosocial burden of UC.34 Recently, the IBD Disk has been shown to correlate with depression and anxiety and to identify patients at risk of adverse outcomes at IBD diagnosis.35 In our cohort, patients in the BU-A group had significantly higher IBD Disk scores across nearly all dimensions, including abdominal pain, defecation control, sleep, energy, emotion, body image, and interpersonal relationships. A decline in quality of life may contribute to anxiety or depression, which in turn can indirectly worsen BU via the brain-gut axis. The IBD Disk appears to capture much of this impact and may serve as a surrogate marker of urgency-related disability. This raises the possibility that the Urgency NRS could be integrated into future versions of the IBD Disk or other PRO instruments.
This study has several strengths and limitations. To our knowledge, this is the first study to comprehensively investigate the associations between BU and multiple clinical parameters in patients with UC, including clinical disease activity, endoscopic and histologic findings, stool patterns, and health-related quality of life assessed using the validated IBD Disk. The integration of endoscopic and histologic assessments, combined with validated instruments such as the Urgency NRS, IBD Disk, and BSFS, strengthens the validity and reliability of our findings. Moreover, the balanced distribution of BU-A and BU-R groups, together with the application of standardized evaluation methods, further enhance the robustness of the results.
Several limitations should also be acknowledged. First, rectal compliance and anorectal function were not objectively assessed (eg, via manometry or defecography), which may limit our understanding of functional contributors to urgency. Second, although the IBD Disk provided valuable patient-centered data, urgency-specific patient-reported outcome measures (such as deferral time, leakage anxiety, or urgency frequency) were not included; incorporating such tools in future studies may yield additional insights. Third, fecal calprotectin data were not routinely available, as the test is not covered by national health insurance and requires self-payment, which reduced sample availability and may have limited our ability to evaluate correlations between fecal calprotectin and BU. Finally, this was a single-center study with a relatively small sample size, which may restrict the generalizability of our findings to the broader UC population and real-world clinical settings.
Recently, BU has been increasingly recognized as a key symptom in UC and is being recommended as a core outcome measure in clinical trials,20,36 including incorporation into PRO assessments.37 Clinical trials of mirikizumab have also included BU as an important endpoint for evaluating patient outcomes in UC.38 Emerging evidence suggests that intestinal ultrasound may aid in detecting subtle, chronic alterations in rectal wall morphology—such as increased thickness or vascularity—providing a non-invasive method to assess transmural involvement that could contribute to persistent symptoms.39
In this study, histological inflammation and loose stool form were identified as independent predictors of BU. Notably, a substantial proportion of patients continued to experience BU despite achieving histological remission or having normal stool form, indicating a multifactorial origin beyond inflammation alone. These findings underscore the need of recognizing BU as a key PRO in UC and incorporating its assessment into routine clinical practice to optimize patient care.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board (IRB) of the Chang Gung Medical Foundation (approval number: 202400030B0). All study procedures involving human participants complied with the ethical standards of the institutional or national research committee and the principles of the Declaration of Helsinki.
Consent for Publication
Written informed consent was obtained from all participants for inclusion in the study. No identifiable personal data, images, or recordings are included in this manuscript.
Acknowledgments
We gratefully acknowledge the support and contributions of the members of the Chang Gung IBD Center.
Author Contributions
All authors made substantial contributions to the work reported, including, but not limited to, the conception and design of the study, execution, data acquisition, analysis, and interpretation. All authors participated in drafting, revising, or critically reviewing the manuscript; approved the final version for publication; agreed on the target journal for submission; and accepted responsibility for the integrity and accuracy of all aspects of the work.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no financial disclosures or conflicts of interest in this work.
References
1. Perler BK, Ungaro R, Baird G, et al. Presenting symptoms in inflammatory bowel disease: descriptive analysis of a community-based inception cohort. BMC Gastroenterol. 2019;19. doi:10.1186/s12876-019-0963-7
2. newton L, Randall JA, Hunter T, et al. A qualitative study exploring the health-related quality of life and symptomatic experiences of adults and adolescents with ulcerative colitis. J Patient-Reported Outcomes. 2019;3:1–13. doi:10.1186/s41687-019-0154-x
3. Sninsky JA, Barnes EL, Zhang X, Long MD. Urgency and its association with quality of life and clinical outcomes in patients with ulcerative colitis. Am J Gastroenterol. 2022;117:769–776. doi:10.14309/ajg.0000000000001685
4. Hibi T, Ishibashi T, Ikenoue Y, Yoshihara R, Nihei A, Kobayashi T. Ulcerative colitis: disease burden, impact on daily life, and reluctance to consult medical professionals: results from a Japanese Internet Survey. Inflamm Intest Dis. 2020;5:27–35. doi:10.1159/000505092
5. Dubinsky MC, Irving PM, Panaccione R, et al. Incorporating patient experience into drug development for ulcerative colitis: development of the urgency numeric rating scale, a patient-reported outcome measure to assess bowel urgency in adults. J Patient-Reported Outcomes. 2022;6:31. doi:10.1186/s41687-022-00439-w
6. Pakpoor J, Travis S. Why studying urgency is urgent. Gastroenterol Hepatol. 2023;19:95.
7. Teich N, Schulze H, Knop J, Obermeier M, Stallmach A. Novel approaches identifying relevant patient-reported outcomes in patients with inflammatory bowel diseases—LISTEN 1. Crohn’s Colitis 360. 2021;3:otab050. doi:10.1093/crocol/otab050
8. Petryszyn PW, Paradowski L. Stool patterns and symptoms of disordered anorectal function in patients with inflammatory bowel diseases. Adv Clin Exp Med. 2018;27:813–818. doi:10.17219/acem/68986
9. Lonnfors S, Vermeire S, Greco M, Hommes D, Bell C, Avedano L. IBD and health-related quality of life -- discovering the true impact. J Crohns Colitis. 2014;8:1281–1286. doi:10.1016/j.crohns.2014.03.005
10. Dulai PS, Jairath V, Khanna R, et al. Development of the symptoms and impacts questionnaire for Crohn’s disease and ulcerative colitis. Aliment Pharmacol Ther. 2020;51:1047–1066. doi:10.1111/apt.15726
11. Dubinsky MC, Watanabe K, Molander P, et al. Ulcerative colitis narrative global survey findings: the impact of living with ulcerative colitis-patients’ and physicians’ view. Inflamm Bowel Dis. 2021;27:1747–1755. doi:10.1093/ibd/izab016
12. Camarillo GF, Goyon EI, Zuniga RB, Salas LAS, Escarcega AEP, Yamamoto-Furusho JK. Gene expression profiling of mediators associated with the inflammatory pathways in the intestinal tissue from patients with ulcerative colitis. Mediators Inflamm. 2020;2020:9238970. doi:10.1155/2020/9238970
13. Ghosh S, Sanchez Gonzalez Y, Zhou W, et al. Upadacitinib treatment improves symptoms of bowel urgency and abdominal pain, and correlates with quality of life improvements in patients with moderate to severe ulcerative colitis. J Crohns Colitis. 2021;15:2022–2030. doi:10.1093/ecco-jcc/jjab099
14. Dawwas GK, Jajeh H, Shan M, Naegeli AN, Hunter T, Lewis JD. Prevalence and factors associated with fecal urgency among patients with ulcerative colitis and Crohn’s disease in the study of a prospective adult research cohort with inflammatory bowel disease. Crohn’s Colitis 360. 2021;3:otab046. doi:10.1093/crocol/otab046
15. Kulyk A, Shafer LA, Graff LA, et al. Urgency for bowel movements is a highly discriminatory symptom of active disease in persons with IBD (the Manitoba living with IBD study). Aliment Pharmacol Ther. 2022;56:1570–1580. doi:10.1111/apt.17241
16. Dubinsky MC, Shan M, Delbecque L, et al. Psychometric evaluation of the Urgency NRS as a new patient-reported outcome measure for patients with ulcerative colitis. J Patient Rep Outcomes. 2022;6:114. doi:10.1186/s41687-022-00522-2
17. Blake MR, Raker JM, Whelan K. Validity and reliability of the Bristol Stool Form Scale in healthy adults and patients with diarrhoea-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2016;44:693–703. doi:10.1111/apt.13746
18. Ghosh S, Louis E, Beaugerie L, et al. Development of the IBD disk: a visual self-administered tool for assessing disability in inflammatory bowel diseases. Inflamm Bowel Dis. 2017;23:333–340. doi:10.1097/MIB.0000000000001033
19. Danese S, Dignass A, Matsuoka K, et al. Early and sustained symptom control with Mirikizumab in patients with ulcerative colitis in the phase 3 LUCENT programme. J Crohns Colitis. 2024;18:1845–1856. doi:10.1093/ecco-jcc/jjae088
20. Rubin DT, Sninsky C, Siegmund B, et al. International perspectives on management of inflammatory bowel disease: opinion differences and similarities between patients and physicians from the IBD GAPPS survey. Inflamm Bowel Dis. 2021;27:1942–1953. doi:10.1093/ibd/izab006
21. Casellas F, Herrera-de Guise C, Robles V, Navarro E, Borruel N. Patient preferences for inflammatory bowel disease treatment objectives. Dig Liver Dis. 2017;49:152–156. doi:10.1016/j.dld.2016.09.009
22. Rao SS, Read NW, Davison PA, Bannister JJ, Holdsworth CD. Anorectal sensitivity and responses to rectal distention in patients with ulcerative colitis. Gastroenterology. 1987;93:1270–1275. doi:10.1016/0016-5085(87)90255-1
23. Krugliak Cleveland N, Torres J, Rubin DT. What does disease progression look like in ulcerative colitis, and how might it be prevented? Gastroenterology. 2022;162:1396–1408. doi:10.1053/j.gastro.2022.01.023
24. Gordon IO, Agrawal N, Willis E, et al. Fibrosis in ulcerative colitis is directly linked to severity and chronicity of mucosal inflammation. Aliment Pharmacol Ther. 2018;47:922–939. doi:10.1111/apt.14526
25. Dubinsky MC, Clemow DB, Hunter Gibble T, et al. Clinical effect of mirikizumab treatment on bowel urgency in patients with moderately to severely active ulcerative colitis and the clinical relevance of bowel urgency improvement for disease remission. Crohn’s Colitis 360. 2023;5:otac044. doi:10.1093/crocol/otac044
26. Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: an update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) initiative of the International Organization for the Study of IBD (IOIBD): determining therapeutic goals for treat-to-target strategies in IBD. Gastroenterology. 2021;160:1570–1583. doi:10.1053/j.gastro.2020.12.031
27. Bryant RV, Winer S, Travis SP, Riddell RH. Systematic review: histological remission in inflammatory bowel disease. Is ‘complete’ remission the new treatment paradigm? An IOIBD initiative. J Crohns Colitis. 2014;8:1582–1597. doi:10.1016/j.crohns.2014.08.011
28. Greig E, Sandle GI. Diarrhea in ulcerative colitis. The role of altered colonic sodium transport. Ann N Y Acad Sci. 2000;915:327–332. doi:10.1111/j.1749-6632.2000.tb05260.x
29. Nordin E, Hellstrom PM, Brunius C, Landberg R. Modest conformity between self-reporting of bristol stool form and fecal consistency measured by stool water content in irritable bowel syndrome and a FODMAP and gluten trial. Am J Gastroenterol. 2022;117:1668–1674. doi:10.14309/ajg.0000000000001942
30. Dale HF, Hagen M, Malmstrom GH, et al. Assessing hard and loose “endpoints”: comparison of patient and expert Bristol Stool Scale scoring of 2280 fecal samples. F1000Res. 2024;13:833. doi:10.12688/f1000research.152496.2
31. Krugliak Cleveland N, Rai V, El Jurdi K, Rao SS, Giurcanu MC, Rubin DT. Ulcerative colitis patients have reduced rectal compliance compared with non-inflammatory bowel disease controls. Gastroenterology. 2022;162:331–333e1. doi:10.1053/j.gastro.2021.09.052
32. Tanaka Y, Kanazawa M, Fukudo S, Drossman DA. Biopsychosocial model of irritable bowel syndrome. J Neurogastroenterol Motil. 2011;17:131–139. doi:10.5056/jnm.2011.17.2.131
33. Papathanasopoulos AA, Katsanos KH, Tatsioni A, Christodoulou DK, Tsianos EV. Increased fatigability of external anal sphincter in inflammatory bowel disease: significance in fecal urgency and incontinence. J Crohns Colitis. 2010;4:553–560. doi:10.1016/j.crohns.2010.05.002
34. Peppas S, Pansieri C, Piovani D, et al. The brain-gut axis: psychological functioning and inflammatory bowel diseases. J Clin Med. 2021;11:10. doi:10.3390/jcm11010010
35. Rimmer P, Stoica V, Ibrahim M, et al. P0401 The IBD-disk accurately assesses disability and psychological burden at IBD diagnosis and predicts adverse outcomes in both UC and Crohn’s disease during the first year of treatment. J Crohn’s Colitis. 2025;19:i897–i898. doi:10.1093/ecco-jcc/jjae190.0575
36. Sandborn WJ, Feagan BG, Hanauer SB, Lichtenstein GR. The guide to guidelines in ulcerative colitis: interpretation and appropriate use in clinical practice. Gastroenterol Hepatol. 2021;17:3.
37. Collaborators C-I, Ma C, Hanzel J, et al. CORE-IBD: a Multidisciplinary International Consensus initiative to develop a core outcome set for randomized controlled trials in inflammatory bowel disease. Gastroenterology. 2022;163:950–964. doi:10.1053/j.gastro.2022.06.068
38. Dubinsky MC, Lee SD, Panaccione R, et al. S0682 absence of bowel urgency is associated with significantly improved inflammatory bowel disease related quality of life in a Phase 2 trial of mirikizumab in patients with ulcerative colitis. Official J Am Coll Gastroenterol. 2020;115:S341.
39. Pal P, Mateen MA, Pooja K, et al. Role of intestinal ultrasound in ulcerative colitis: a systematic review. World J Meta-Analysis. 2024;12.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exploring Disease Remission and Bowel Urgency Severity Among Adults with Moderate to Severe Ulcerative Colitis: A Qualitative Study
Dubinsky MC, Newton L, Delbecque L, Hunter T, Guobyte A, Naegeli AN, McFadden S, Donaldson J, Symonds T, Lewis JD
Patient Related Outcome Measures 2022, 13:287-300
Published Date: 22 December 2022