Back to Journals » Drug Design, Development and Therapy » Volume 19
Blood Pressure Reduction During Anesthetic Induction with Remimazolam versus Propofol in Elderly Patients: Pharmacodynamic Modeling of Remimazolam
Authors Oh J ![]() , Kim KM
, Kim KM ![]() , Sim JH, Lee EK, Choi BM
, Sim JH, Lee EK, Choi BM ![]()
Received 15 July 2025
Accepted for publication 16 October 2025
Published 26 October 2025 Volume 2025:19 Pages 9571—9580
DOI https://doi.org/10.2147/DDDT.S553809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Juyeon Oh,1 Kyung Mi Kim,1 Ji-Hoon Sim,1 Eun-Kyung Lee,2 Byung-Moon Choi1
1Department of Anesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea; 2Department of Statistics, Ewha Womans University, Seoul, Korea
Correspondence: Eun-Kyung Lee, Department of Statistics, Ewha Womans University, 52, Ewhayeodae-Gil, Seodaemun-Gu, Seoul, 03760, Korea, Tel +82-2-3277-6857, Fax +82-2-3277-3607, Email [email protected] Byung-Moon Choi, Department of Anesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88, Olympic-Ro 43-Gil, Songpa-Gu, Seoul, 05505, Korea, Tel +82-2-3010-1704, Fax +82-2-3010-6790, Email [email protected]
Purpose: Remimazolam, a novel hypnotic agent, has demonstrated superior hemodynamic stability compared with propofol during general anesthesia, particularly in elderly patients. However, the dose-dependent reduction in blood pressure associated with remimazolam has not been quantitatively modeled in this population.
Patients and Methods: We analyzed data from 432 patients aged ≥ 65 years who underwent elective gastrectomy as part of a randomized trial comparing remimazolam with propofol. Remimazolam was administered via zero-order infusion at 6 mg/kg/h, whereas propofol was delivered using target-controlled infusion (TCI) guided by the Schnider model. Blood pressure data were transformed into fractional changes in mean arterial pressure (MBP) relative to baseline. A modified simple logistic regression model was developed to characterize the relationship between cumulative remimazolam dose and MBP reduction, with body weight evaluated as a covariate.
Results: A total of 209 patients were analyzed in each group. The modified logistic model effectively described the dose-dependent MBP reduction associated with remimazolam. Body weight was identified as a significant covariate that improved model performance. Although the remimazolam group exhibited a statistically greater MBP reduction before intubation than the propofol group (28.0 ± 9.9% vs 25.8 ± 10.1% reduction from baseline, P = 0.024), the difference was not considered clinically meaningful.
Conclusion: In elderly patients undergoing general anesthesia with remimazolam, the relationship between dose and MBP reduction during induction was well characterized using a modified logistic model, with body weight as a significant covariate. TCI may represent an effective dosing strategy for maintaining hemodynamic stability during anesthetic induction.
Trial Registration: This study was registered at the Clinical Research Information Service of the Korean National Institute of Health (CRIS, http://cris.nih.go.kr), with registration number KCT0006877, on December 27, 2021.
Keywords: remimazolam, anesthesia, hemodynamics, aged, pharmacodynamics
Introduction
Remimazolam is a relatively new hypnotic agent introduced into clinical practice, primarily for procedural sedation.1 In several countries, including South Korea, it has also received regulatory approval for use as a general anesthetic.2 Based on a Phase IIb/III clinical trial conducted in Japan,3 the Korean Ministry of Food and Drug Safety recommends a continuous infusion of remimazolam at 6–12 mg/kg/h for the induction of anesthesia.2 Several studies have consistently reported that remimazolam offers superior hemodynamic stability compared to propofol during general anesthesia and a lower incidence of hypotension.4–8 Consequently, remimazolam may be particularly advantageous for elderly patients, who are more likely to experience significant hemodynamic fluctuations during anesthetic induction.9 Furthermore, some studies have demonstrated that the incidence of postoperative delirium and the quality of recovery with remimazolam are non-inferior to those observed with propofol,10–12 suggesting that its use in elderly patients requiring general anesthesia will likely increase. However, elderly patients exhibit substantial pharmacodynamic and pharmacokinetic (PK) variability,13 which may contribute to considerable interindividual differences in blood pressure reduction during anesthesia with remimazolam. Therefore, developing a model to quantify the dose-dependent reduction in blood pressure associated with remimazolam would be valuable for achieving more stable hemodynamic control in this population.
Target-controlled infusion (TCI) is an established method of intravenous drug administration, in which the infusion rate is continuously adjusted based on PK models to maintain a user-defined target plasma or effect-site concentration in real time.14 Studies have shown that TCI provides better hemodynamic stability than conventional continuous infusion of the same agent.15 Consequently, TCI is widely used for intraoperative propofol administration in many countries, excluding the United States.16 Although PK models for remimazolam have been developed,17,18 the drug is not yet integrated into commercially available TCI pumps, making clinical implementation challenging without specialized equipment. The primary aim of this study was to develop a pharmacodynamic model to quantify the relationship between remimazolam dosing and blood pressure reduction in patients aged ≥ 65 years. Additionally, we aimed to indirectly assess the potential advantages of TCI-based administration by comparing the degree of blood pressure reduction observed during anesthetic induction using standard clinical infusion methods for remimazolam and propofol.
Materials and Methods
Study Design
This study involved a retrospective analysis of blood pressure data, dosing information, and patient characteristics collected from a previously conducted randomized controlled trial.12 The original trial compared the incidence of postoperative delirium and quality of recovery between remimazolam and propofol in patients aged ≥ 65 years undergoing elective gastrectomy.12
Ethical Considerations
The original randomized controlled trial was conducted at a single center and was approved by the Institutional Review Board of Asan Medical Center (Seoul, Korea; approval number: 2021–1668, approval date: November 25, 2021). The study was conducted in accordance with the Declaration of Helsinki. It was also registered with the International Clinical Trials Registry Platform (http://cris.nih.go.kr, KCT0006877; principal investigator: Byung-Moon Choi; registration date: December 27, 2021) prior to the enrollment of the first patient. Written informed consent was obtained from all participants. During the consent process, all patients agreed that the data collected could be used for academic purposes, with appropriate protection of personal and sensitive information.
Patient Population
Data from 432 patients who completed the original trial were included in the analysis. The inclusion and exclusion criteria and the randomization procedures are detailed in the original publication.12
Study Procedure
Upon arrival in the operating room, patients were monitored using electrocardiography, pulse oximetry, end-tidal carbon dioxide, and train-of-four (TOF) monitoring (Carescape B850; GE Healthcare, Milwaukee, Wisconsin, USA). A bispectral index (BIS™; Medtronic, Dublin, Ireland) sensor was placed on the forehead. All monitoring data were continuously recorded onto a personal computer throughout the procedure, with time synchronization based on Korean Standard Time. For patients who consented to electroencephalogram (EEG) monitoring, an 8-channel electrode montage was applied before induction, and a minimum of 5 minutes of baseline EEG was recorded before administration of anesthetic agents.19 To ensure adequate stabilization, patients remained in the supine position on the operating table for at least 10 minutes before anesthetic administration. After administration, blood pressure was measured at 1-minute intervals. Loss of consciousness was defined as the point at which the patient no longer responded to verbal commands to “open your eyes.” Following loss of consciousness, rocuronium (0.6 mg/kg) was administered. Subsequently, remifentanil was initiated via target effect-site controlled infusion using the Minto model,20 with an initial target concentration of 2 ng/mL. If systolic blood pressure was maintained above 90 mmHg, the remifentanil target concentration was increased to 3 ng/mL. Endotracheal intubation was performed once a TOF count of zero and a BIS value below 60 were confirmed. To maintain hemodynamic stability (systolic blood pressure ≥ 80 mmHg and heart rate ≥ 45 bpm), ephedrine or phenylephrine was administered as needed. Blood pressure monitors used in this study were calibrated every 6 months following hospital medical device maintenance protocols.
Administration of Anesthetic Agents
Each anesthetic agent was administered using clinically established methods, without changes to the initial dosing strategy until endotracheal intubation was completed. Remimazolam was administered as a continuous infusion at 6 mg/kg/h. Propofol was administered via TCI using the Schnider model,21,22 with a target effect-site concentration set at 3.5 μg/mL. Both agents were delivered using a commercial TCI pump (Perfusor Space; B. Braun Melsungen AG, Germany). Real-time simulations were conducted using the AsanPump TCI control software (version 2.1.5; Bionet Co. Ltd., Seoul, Korea) to obtain detailed time-stamped dosing information. The software settings were manually updated to match any adjustments made on the actual TCI pump during administration. The computer running the AsanPump software was synchronized to Korean Standard Time to ensure accurate time alignment. This procedure allowed for precise synchronization between blood pressure measurements and anesthetic dosing data, even though these data were recorded on separate computers.
Development of a Prediction Model
Blood pressure data were transformed into fractional changes relative to baseline rather than using absolute values to facilitate effective modelling and enhance clinical applicability. Baseline blood pressure was defined as 100% of the value immediately before anesthetic administration, and subsequent reductions were expressed as percentage changes. Blood pressure data up to immediately before intubation were used for modeling. For example, if the baseline mean blood pressure (MBP) was 80 mmHg and the MBP immediately before endotracheal intubation was 64 mmHg, the corresponding fractional MBP would be 80% (64/80). Given that perioperative blood pressure management primarily focuses on MBP rather than systolic blood pressure,23,24 the predictive model was developed using fractional changes in MBP.
A model that best described the fractional MBP data was selected, and a modified simple logistic regression model was employed.25 The structural model is presented in Equation (1).

Here, ϕ1 represents the horizontal asymptote range of 100 – fractional MBP as the cumulative dose (“amount”) approaches infinity; that is, ϕ1 denotes the overall range of reduction in fractional MBP. Parameter ϕ2 represents the value of the amount at which 100 – fractional MBP equals ϕ1/2, corresponding to the inflection point of the logistic curve. Parameter ϕ3 is a scale parameter that reflects the steepness of the curve and the distance on the amount axis between the inflection point and the point at which fractional MBP is approximately 100–0.73ϕ1. In this model, “amount” refers to the cumulative dose of remimazolam administered during anesthetic induction. Between-subject variability was estimated using an additive random effects model, as shown in Equation (2).

Where  is the k-th parameter for the i-th individual,
is the k-th parameter for the i-th individual,  is the typical value, and
is the typical value, and  is a random effect with a mean of zero and variance
is a random effect with a mean of zero and variance  . Within-subject variability was modeled using an additive residual error model. The Akaike Information Criterion (AIC) was used to select the final model.26 Age, sex, weight, and histories of hypertension and diabetes were evaluated as potential covariates. Model estimation was conducted using the NLMIXED procedure in SAS (version 9.4, SAS Institute Inc., Cary, NC, USA). Stochastic simulations based on the final model estimates were performed to visualize covariate effects.
. Within-subject variability was modeled using an additive residual error model. The Akaike Information Criterion (AIC) was used to select the final model.26 Age, sex, weight, and histories of hypertension and diabetes were evaluated as potential covariates. Model estimation was conducted using the NLMIXED procedure in SAS (version 9.4, SAS Institute Inc., Cary, NC, USA). Stochastic simulations based on the final model estimates were performed to visualize covariate effects.
Statistical Analysis
The primary endpoint was the development of a pharmacodynamic model describing the dose-dependent blood pressure reduction in patients aged ≥ 65 years who received remimazolam. The secondary endpoint was to indirectly assess the hemodynamic stability of TCI by comparing the degree of blood pressure reduction during anesthetic induction between remimazolam (administered via zero-order infusion) and propofol (administered via target effect-site controlled infusion). Given that the primary endpoint involved exploratory model development, a formal sample size calculation was not required. However, a sample size calculation was performed for the secondary endpoint, which involved comparing the degree of blood pressure reduction between the two groups prior to endotracheal intubation. Before conducting the original study designed to evaluate delirium incidence and quality of recovery, a pilot test was performed.19 In that study, the mean (standard deviation) reduction in blood pressure from the start of drug administration to immediately before endotracheal intubation was 26.8 ± 9.6% for remimazolam and 24.9 ± 13.4% for propofol. Based on a non-inferiority margin of 5% for the between-group difference in mean blood pressure reduction, with an alpha of 0.05 and a beta of 0.8, and accounting for a 5% dropout rate, the required sample size was calculated to be 172 patients per group.
All statistical analyses were conducted using SigmaStat version 3.5 (Systat Software, Inc., Chicago, IL, USA), R software (version 4.5.1, R Foundation for Statistical Computing, Vienna, Austria), or SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Continuous variables were summarized as mean (standard deviation) for normally distributed data or median (interquartile range) for non-normally distributed data. Categorical variables were presented as counts and percentages (n [%]). Group comparisons were performed using the two-sample t-test, Mann–Whitney U-test, or chi-square test, as appropriate.
Results
The CONSORT flow diagram for this study is presented in Figure 1. Patients with missing blood pressure, anesthetic dosing data, or inconsistent timing between these datasets were excluded from the analysis. A total of 209 patients per group were included in the final analysis. Demographic characteristics are summarized in Table 1. No statistically significant differences were observed between the two groups. Variables related to anesthetic induction, including time to endotracheal intubation, are summarized in Table 2. The difference in cumulative dose up to endotracheal intubation was attributed to the difference in potency between the two agents. The fractional change in MBP from the start of anesthetic infusion to immediately before endotracheal intubation is shown in Figure 2. In both groups, a progressive reduction in MBP was observed as infusion continued and the cumulative dose increased. Individual relative MBP values, calculated as MBP immediately before intubation divided by baseline MBP, are presented in Figure 3. Although the remimazolam group exhibited a statistically greater reduction in MBP than the propofol group (remimazolam: 72.0 ± 9.9%; propofol: 74.2 ± 10.1%; Student’s t-test, P = 0.024), this difference was not considered clinically significant. The modified logistic model adequately described the dose-dependent changes in fractional MBP. In the base model, the scale parameter  was treated as a fixed effect. When weight was included as a covariate for
was treated as a fixed effect. When weight was included as a covariate for  and
and  , the AIC decreased significantly (base model: 7412, covariate model: 7369). Other covariates, including age and sex, were not statistically significant. Parameter estimates and their standard errors for the final model are presented in Table 3. To ensure stable model estimation, body weight was centered and scaled using the transformation weightc = (weight − 40)/60, yielding values approximately between 0 and 1. Diagnostic plots for the final model are presented in Supplementary Figure S1. Results of the stochastic simulations illustrating the relationship between remimazolam dose and fractional MBP stratified by body weight are presented in Figure 4. As body weight decreased, the fractional MBP reduction at a given cumulative dose became more pronounced.
, the AIC decreased significantly (base model: 7412, covariate model: 7369). Other covariates, including age and sex, were not statistically significant. Parameter estimates and their standard errors for the final model are presented in Table 3. To ensure stable model estimation, body weight was centered and scaled using the transformation weightc = (weight − 40)/60, yielding values approximately between 0 and 1. Diagnostic plots for the final model are presented in Supplementary Figure S1. Results of the stochastic simulations illustrating the relationship between remimazolam dose and fractional MBP stratified by body weight are presented in Figure 4. As body weight decreased, the fractional MBP reduction at a given cumulative dose became more pronounced.
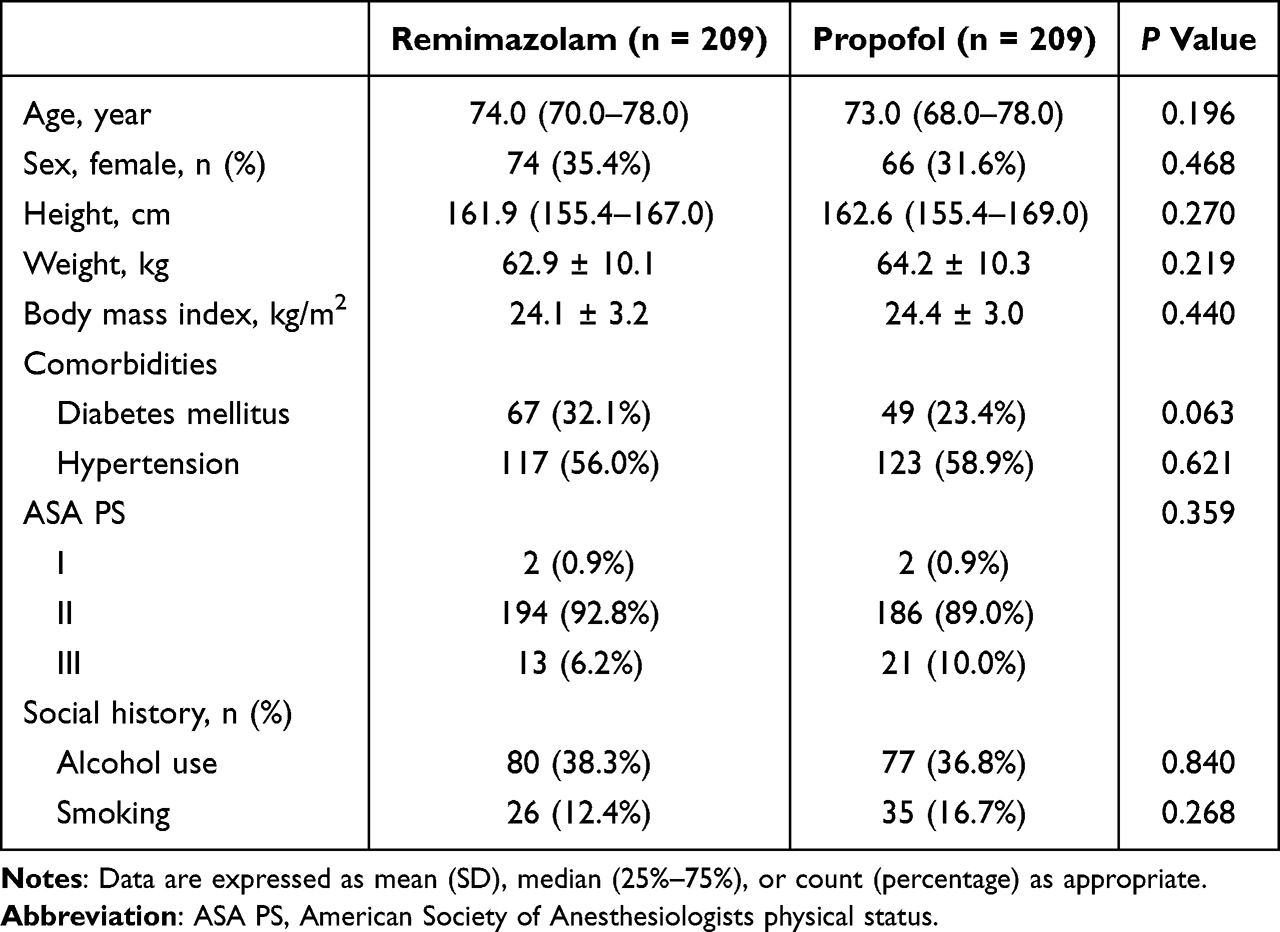 |
Table 1 Baseline Characteristics |
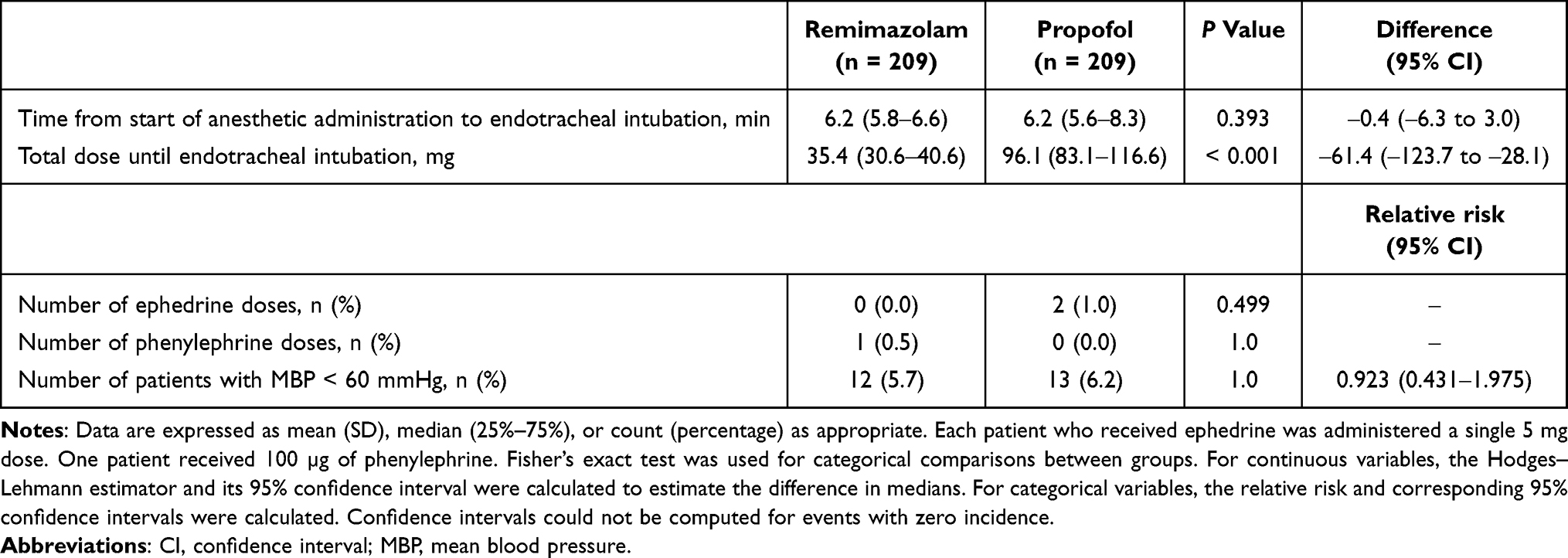 |
Table 2 Variables During Anesthetic Induction |
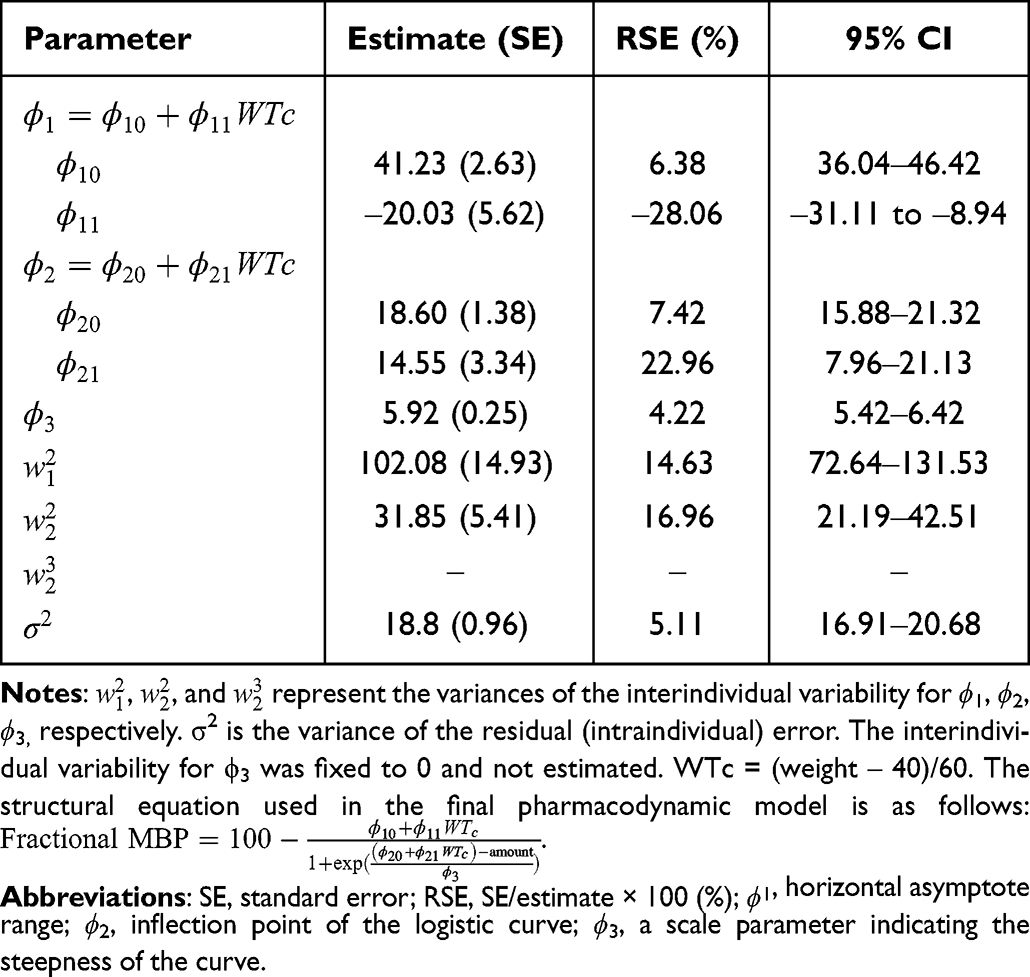 |
Table 3 Pharmacodynamic Parameter Estimates and Relative Standard Error (RSE) of the Final Pharmacodynamic Model |
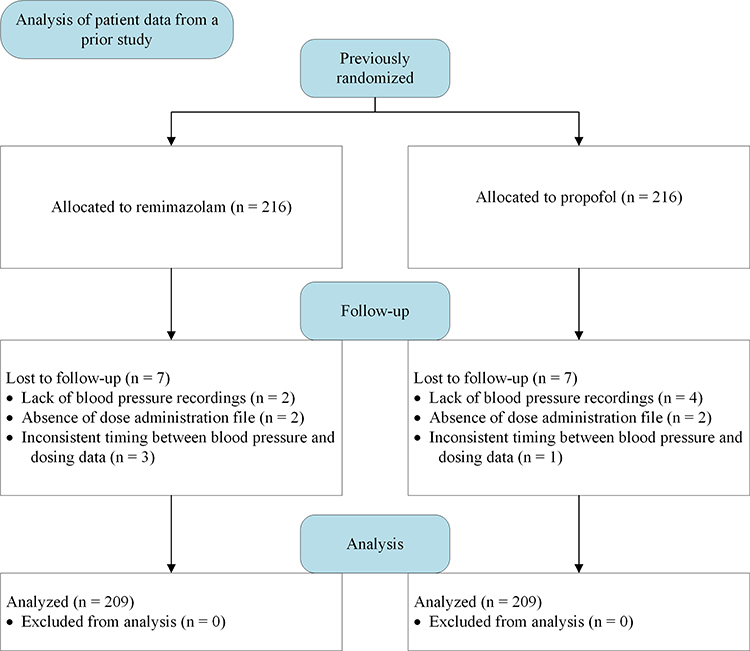 |
Figure 1 CONSORT flow diagram. This analysis was based on patient data from a previously conducted randomized controlled trial; therefore, there were no screening failures in this study. |
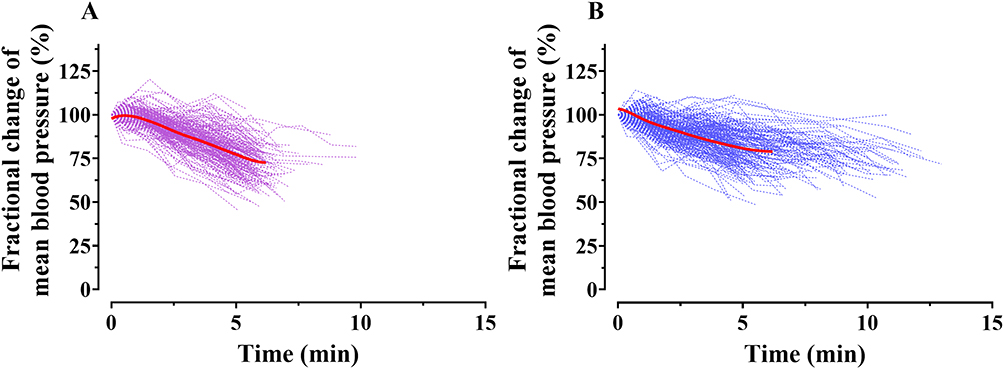 |
Figure 2 Fractional changes in mean blood pressure (MBP) following induction with remimazolam (A) and propofol (B). Each dotted line represents the fractional change in MBP (%) for an individual patient over time. The solid red line indicates the locally weighted scatterplot smoothing (LOWESS) trend. The LOWESS curve was plotted only up to the average time of endotracheal intubation during anesthetic induction with each agent. Fractional MBP was calculated by normalizing the blood pressure immediately before the administration of the anesthetic agent to 100%. |
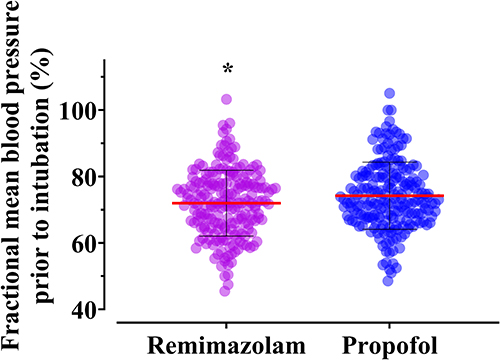 |
Figure 3 Comparison of fractional mean blood pressure (MBP) before endotracheal intubation between the remimazolam and propofol groups. Each dot represents an individual patient. The red horizontal line indicates the group mean, and the black vertical line represents the standard deviation. Fractional MBP was calculated by normalizing the blood pressure immediately before anesthetic administration to 100%. *P < 0.05 vs propofol. |
 |
Figure 4 Stochastic simulations illustrating the relationship between cumulative remimazolam dose and fractional mean blood pressure (MBP) by body weight. Panels (A–C) represent patients weighing 40 kg, 60 kg, and 80 kg, respectively. Remimazolam was simulated at an infusion rate of 6 mg/kg/h using the final model parameter estimates. A total of 1,000 simulation replicates were conducted for each weight group. The red solid line indicates the 50% prediction line, and the blue shaded area represents the 90% prediction interval. |
Discussion
In elderly patients aged ≥ 65 years, the dose-dependent reduction in MBP associated with remimazolam was well described by a modified logistic model. Body weight was identified as a significant covariate in the model. Anesthetic administration using a TCI method may offer greater hemodynamic stability than zero-order infusion.
The modified logistic regression model was particularly well suited to characterize the dose-dependent reduction in MBP, as it effectively captures the characteristic sigmoid (S-shaped) relationship between dose and hemodynamic response. In contrast to linear or simple exponential models, the logistic model accommodates a threshold effect, a steep reduction phase, and a plateau, thereby reflecting the pharmacodynamic properties of remimazolam observed in clinical settings. Furthermore, the model parameters, including the asymptote, inflection point, and steepness, provide intuitive and clinically meaningful insights into the dose-response relationship. The incorporation of random effects further enabled the model to account for inter-individual variability, enhancing its flexibility and predictive performance. The inclusion of body weight as a covariate was appropriate, as remimazolam was administered using a weight-based dosing regimen (6 mg/kg/h). Given that the infusion rate is directly dependent on patient weight, it is reasonable that body weight would influence the relationship between cumulative dose and MBP reduction.TCI is considered one of the most advanced methods of drug administration.16 Unlike conventional approaches such as constant-rate (zero-order) infusion or manually adjusted variable-rate infusion, TCI continuously calculates and adjusts the infusion rate approximately every 10 seconds based on PK models to maintain a user-defined target concentration.14 This approach allows for more precise drug delivery than manual adjustments. When covariates such as body weight or age are incorporated into the PK model, interindividual variability in PK parameters can be accounted for. Consequently, even when maintaining the same target concentration for the same duration, the actual amount of drug administered will vary according to individual patient characteristics, facilitating personalized dosing. Furthermore, general anesthetics typically exhibit a steep dose-response relationship, whereby small changes in dose can result in substantial differences in effect.27 Therefore, accurate titration is particularly important when administering these agents, and TCI offers a distinct advantage. Recent efforts have also explored the use of TCI beyond general anesthetics, including certain antibiotics,28–30 particularly in clinical scenarios where maintaining drug concentrations above the minimum inhibitory concentration is critical. In patients undergoing endoscopic procedures, the use of TCI for propofol administration has been associated with faster recovery times and a lower incidence of moderate hypotension compared with manually controlled infusion.31 These findings suggest that TCI may be an effective strategy for maintaining hemodynamic stability. In a previous study comparing zero-order infusion of remimazolam and TCI propofol administration during anesthetic induction, no statistically significant difference in MBP reduction was observed between the two groups.32 Although the small sample size (n = 20 per group) raises concerns regarding statistical power, the observation that propofol administered via TCI produced hemodynamic changes similar to those of remimazolam is consistent with the findings of the present study. If remimazolam could be administered using a TCI method, anesthetic induction is expected to be performed with even greater hemodynamic stability.This study has some limitations. First, the number of patients included in the analysis was relatively small for the development of a predictive model. Generally, the performance of predictive models improves when trained on larger and more diverse populations.33,34 For this reason, many predictive models are developed using large retrospective datasets derived from routine clinical practice.34,35 However, cumulative dosing data recorded during anesthetic induction with remimazolam are not routinely captured and must be prospectively collected in a research setting, which inherently limits the sample size. Nevertheless, because the primary objective of this study was not to develop a clinical prediction model, but rather to construct a pharmacodynamic model to quantitatively describe the dose-response relationship, the sample size was considered sufficient for this purpose. Second, when comparing blood pressure reductions between two agents, using different administration protocols introduces the possibility that the method of administration itself may act as a confounding factor. Ideally, both agents would be administered using the same method to eliminate such potential confounding. However, we believe that using administration protocols that are not routinely employed in clinical settings may limit the practical applicability of the study findings. In Korea, remimazolam is currently not available for administration via TCI because its pharmacokinetic model has not yet been incorporated into approved infusion pumps. In contrast, propofol is commonly administered using TCI in clinical practice. Therefore, rather than applying uniform administration methods solely for the purpose of standardization, we opted to reflect real-world clinical practices by using the typical administration protocol for each agent. Furthermore, the observation that propofol administered with effect site-controlled TCI produced a similar degree of blood pressure reduction to that of remimazolam administered by constant rate infusion suggests that TCI may be a useful approach for controlling hemodynamic responses during anesthetic induction. Third, the plasma concentration of remimazolam was not measured in this study, and therefore the concentration–effect relationship could not be explored. When quantifying the relationship between dose and effect, the titration paradox may arise. Measuring the actual plasma concentration would help reduce potential misinterpretation by enabling analysis of the concentration–effect relationship. However, the original study was designed to compare the incidence of postoperative delirium between propofol and remimazolam, and therefore intraoperative blood sampling for remimazolam concentrations was not performed. Nonetheless, since the current analysis incorporated a pharmacodynamic model that accounts for interindividual variability, we believe that the analytical robustness of the results remains sound.
Conclusion
In elderly patients aged ≥ 65 years undergoing general anesthesia with remimazolam, the relationship between remimazolam dose and the reduction in mean arterial pressure during anesthetic induction was well characterized using a modified logistic model. Body weight was identified as a significant covariate. When comparing the degree of mean arterial pressure reduction during induction, remimazolam administered via zero-order infusion resulted in a statistically greater decrease than propofol administered via TCI; however, this difference was not considered clinically significant.
Data Sharing Statement
The data supporting the findings of this study are available from Byung-Moon Choi upon reasonable request. Data will be shared if the request is considered appropriate.
Acknowledgments
The authors express their sincere gratitude to the patients who participated in this study. The authors also thank Jeong-Sim Yang, AS (Asan Medical Center, Korea), and Do-Yang Park, AS (Asan Medical Center, Korea), for their support as clinical research coordinators.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Hana Pharmaceutical, Co., Ltd., Seoul, Korea, which had no role in the study design, data analysis, data interpretation, or manuscript writing. Additional support was provided by the Seoul Business Agency (Grant/Award No.: BT230148).
Disclosure
The authors declare that they have no competing interests.
References
1. Hu Q, Liu X, Wen C, Li D, Lei X. Remimazolam: an updated review of a new sedative and anaesthetic. Drug Des Devel Ther. 2022;16:3957–3974. doi:10.2147/DDDT.S384155
2. Kim KM. Remimazolam: pharmacological characteristics and clinical applications in anesthesiology. Anesth Pain Med. 2022;17(1):1–11. doi:10.17085/apm.21115
3. Doi M, Morita K, Takeda J, Sakamoto A, Yamakage M, Suzuki T. Efficacy and safety of remimazolam versus propofol for general anesthesia: a multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J Anesth. 2020;34(4):543–553. doi:10.1007/s00540-020-02788-6
4. Wegner BM, Wegner GM, Spagnol LW, Costa LA, Spagnol VW, Paiva DF. Comparison between hemodynamic effects of remimazolam and propofol during general anesthesia: a systematic review and meta-analysis. Minerva Anestesiologica. 2024;90(10):901–911. doi:10.23736/S0375-9393.24.18041-8
5. Ju J-W, Lee DJ, Chung J, et al. Effect of remimazolam versus propofol on hypotension after anesthetic induction in patients undergoing coronary artery bypass grafting: a randomized controlled trial. J Clin Anesth. 2024;98:111580. doi:10.1016/j.jclinane.2024.111580
6. Koo C-H, Lee SU, Kim H-G, et al. Effect of remimazolam on intraoperative hemodynamic stability in patients undergoing cerebrovascular bypass surgery: a prospective randomized controlled trial. Korean J Anesthesiol. 2025;78(2):148–158. doi:10.4097/kja.24538
7. Li J, Liao L, Shao C, et al. Comparison of remimazolam tosylate and propofol in hemodynamic stability, postoperative cognitive function, and recovery in general anesthesia combined with regional nerve blocks: a retrospective cohort study. BMC Anesthesiology. 2025;25(1):126. doi:10.1186/s12871-025-02981-8
8. Liu X, Zhang L, Zhao L, et al. Comparison of the safety of remimazolam and propofol during general anesthesia in elderly patients: systematic review and meta-analysis. Front Med Lausanne. 2025;12:1409495. doi:10.3389/fmed.2025.1409495
9. Kawasaki S, Kiyohara C, Tokunaga S, Hoka S. Prediction of hemodynamic fluctuations after induction of general anesthesia using propofol in non-cardiac surgery: a retrospective cohort study. BMC Anesthesiol. 2018;18(1):167. doi:10.1186/s12871-018-0633-2
10. Arias JA, Wegner GRM, Wegner BFM, Silva LS, Bezerra FJL, Filardi RGM. Association of remimazolam with delirium and cognitive function: a systematic review and meta-analysis of randomised controlled trials. Eur J Anaesthesiol. 2025;42(4):285–297. doi:10.1097/EJA.0000000000002107
11. Fang PP, Hu J, Wei QF, et al. Effect of remimazolam besylate vs propofol on incidence of postoperative delirium in older patients undergoing Hip surgery: a randomized noninferiority trial. Int J Surg. 2025;111(1):1469–1472. doi:10.1097/JS9.0000000000001908
12. Sim JH, Kim KM, Lee U, Lee EK, Noh GJ, Choi BM. Incidence of postoperative delirium and quality of recovery in older patients undergoing gastrectomy under general anaesthesia with remimazolam vs. propofol: a randomised non-inferiority study. Anaesthesia. 2025;80:1370–1380. doi:10.1111/anae.16684
13. Mangoni AA, Jackson SHD. Age‐related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6–14. doi:10.1046/j.1365-2125.2003.02007.x
14. Schnider TW, Minto CF, Struys MM, Absalom AR. The safety of target-controlled infusions. Anesth Analg. 2016;122(1):79–85. doi:10.1213/ANE.0000000000001005
15. Struys MM, De Smet T, Glen JI, Vereecke HE, Absalom AR, Schnider TW. The history of target-controlled infusion. Anesth Analg. 2016;122(1):56–69. doi:10.1213/ANE.0000000000001008
16. Absalom AR, Glen JI, Zwart GJ, Schnider TW, Struys MM. Target-controlled infusion: a mature technology. Anesth Analg. 2016;122(1):70–78. doi:10.1213/ANE.0000000000001009
17. Schuttler J, Eisenried A, Lerch M, Fechner J, Jeleazcov C, Ihmsen H. Pharmacokinetics and pharmacodynamics of remimazolam (CNS 7056) after continuous infusion in healthy male volunteers: part I. Pharmacokinetic Clin Pharmacody Anesthesiol. 2020;132(4):636–651.
18. Zhou J, Leonowens C, Ivaturi VD, et al. Population pharmacokinetic/pharmacodynamic modeling for remimazolam in the induction and maintenance of general anesthesia in healthy subjects and in surgical subjects. J Clin Anesth. 2020;66:109899. doi:10.1016/j.jclinane.2020.109899
19. Kim H, Min BK, Lee U, et al. Electroencephalographic features of elderly patients during anesthesia induction with remimazolam: a substudy of a randomized controlled trial. Anesthesiology. 2024;141(4):681–692. doi:10.1097/ALN.0000000000004904
20. Minto CF, Schnider TW, Egan TD, et al. Influence of age and gender on the pharmacokinetics and pharmacodynamics of remifentanil. I. Model development. Anesthesiology. 1997;86(1):10–23. doi:10.1097/00000542-199701000-00004
21. Schnider TW, Minto CF, Gambus PL, et al. The influence of method of administration and covariates on the pharmacokinetics of propofol in adult volunteers. Anesthesiology. 1998;88(5):1170–1182. doi:10.1097/00000542-199805000-00006
22. Schnider TW, Minto CF, Shafer SL, et al. The influence of age on propofol pharmacodynamics. Anesthesiology. 1999;90(6):1502–1516. doi:10.1097/00000542-199906000-00003
23. Saugel B, Sessler DI. Perioperative blood pressure management. Anesthesiology. 2021;134(2):250–261. doi:10.1097/ALN.0000000000003610
24. Saugel B, Fletcher N, Gan TJ, et al. PeriOperative Quality Initiative (POQI) international consensus statement on perioperative arterial pressure management. Br J Anaesth. 2024;133(2):264–276. doi:10.1016/j.bja.2024.04.046
25. Pinheiro J, Bates D. Mixed-effects models in S and S-PLUS. Springer Sci Bus Media. 2000.
26. Akaike H Information theory and an extension of the maximum likelihood principle. In: Parzen E, Tanabe K Kitagawa G, editors. Selected Papers of Hirotugu Akaike. Springer; 1998; pp. 199–213.
27. Ueda I. The steep dose-response curves of anesthesia. Anesthesiology. 2002;96(1):252. doi:10.1097/00000542-200201000-00043
28. Kang HU, Kim KM, Choi JM, et al. Predictive performance of pharmacokinetic models for target concentration-controlled infusion of cefoxitin as a prophylactic antibiotic in patients with colorectal surgery. Clin Exp Pharmacol Physiol. 2022;49(10):1126–1135. doi:10.1111/1440-1681.13695
29. Lee SH, Yoon H, Park J, et al. External validation of a pharmacokinetic model for target-controlled infusion of cefazolin as a prophylactic antibiotic. Br J Clin Pharmacol. 2024;90(2):582–587. doi:10.1111/bcp.15943
30. Yi J-M, Kim KM, Lee H-J, Hong S-K, Choi B-M. External validation of a pharmacokinetic model developed for vancomycin administration via target-controlled infusion. Drug Des Devel Ther. 2025;19:2229–2241. doi:10.2147/DDDT.S507377
31. Chiang M-H, Wu S-C, You C-H, et al. Target-controlled infusion vs. manually controlled infusion of propofol with alfentanil for bidirectional endoscopy: a randomized controlled trial. Endoscopy. 2013;45(11):907–914. doi:10.1055/s-0033-1344645
32. Sekiguchi R, Kinoshita M, Kawanishi R, Kakuta N, Sakai Y, Tanaka K. Comparison of hemodynamics during induction of general anesthesia with remimazolam and target-controlled propofol in middle-aged and elderly patients: a single-center, randomized, controlled trial. BMC Anesthesiol. 2023;23(1):14. doi:10.1186/s12871-023-01974-9
33. Mukkamala R, Schnetz MP, Khanna AK, Mahajan A. Intraoperative hypotension prediction: current methods, controversies, and research outlook. Anesth Analg. 2025;141(1):61–73. doi:10.1213/ANE.0000000000007216
34. Nakanishi T, Tsuji T, Tamura T, Fujiwara K, Sobue K. Development and validation of a prediction model for acute hypotensive events in intensive care unit patients. J Clin Med. 2024;13(10). doi:10.3390/jcm13102786
35. Jo -Y-Y, Jang J-H, Kwon J-M, et al. Predicting intraoperative hypotension using deep learning with waveforms of arterial blood pressure, electroencephalogram, and electrocardiogram: retrospective study. PLoS One. 2022;17(8):e0272055. doi:10.1371/journal.pone.0272055
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect-Site Concentration of Remimazolam by Age Groups During Target-Controlled Infusion for Total Intravenous Anesthesia: A Retrospective Comparative Study
Park J, Seo KH, Kwak J, Baek H
Drug Design, Development and Therapy 2024, 18:5149-5159
Published Date: 12 November 2024
Comparison of Remimazolam versus Dexmedetomidine on Hemodynamics in Older Patients Under Lower Extremity Orthopedic Surgery with Spinal Anesthesia: A Randomized Controlled Trial
Wang D, Liu Z, Zhang W, Li S, Chen Y, Jiang C, Su N, Liu T, Li X, Bi C
Drug Design, Development and Therapy 2025, 19:6037-6046
Published Date: 14 July 2025
Determining the 90% Effective Dose of Remimazolam to Prevent Physical Movement in Surgical Abortions: A Biased-Coin Up-and-Down Sequential Allocation Trial
Fang F, Li H, Li L, Yan B, Yin P, Hu B, Zhu S, Kang X
Drug Design, Development and Therapy 2025, 19:6379-6389
Published Date: 29 July 2025
Effects of Ciprofol on Hemodynamics During Induction in Hypertensive Patients: A Prospective, Randomized, Double-Blind, Controlled Study
Xiao H, Ji M, Shi X, Sun Q, Chen Z, Dong G, Ji F
Drug Design, Development and Therapy 2025, 19:11259-11267
Published Date: 16 December 2025
Efficacy of Remimazolam for Anesthesia in Patients Undergoing Renal Allograft Transplantation: A Randomized Controlled Trial
Han M, Sun D, Lu D, Huang X, Kang F, Li J
Drug Design, Development and Therapy 2026, 20:611432
Published Date: 16 June 2026