Back to Journals » Drug Design, Development and Therapy » Volume 19
Determining the 90% Effective Dose of Remimazolam to Prevent Physical Movement in Surgical Abortions: A Biased-Coin Up-and-Down Sequential Allocation Trial
Authors Fang F, Li H, Li L, Yan B, Yin P ![]() , Hu B
, Hu B ![]() , Zhu S
, Zhu S ![]() , Kang X
, Kang X ![]()
Received 21 August 2024
Accepted for publication 29 June 2025
Published 29 July 2025 Volume 2025:19 Pages 6379—6389
DOI https://doi.org/10.2147/DDDT.S492245
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Fuquan Fang,1,* Huiling Li,1,* Lei Li,1 Bing Yan,2 Pengfei Yin,1 Binwei Hu,3 Shengmei Zhu,1 Xianhui Kang1
1Department of Anesthesiology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Anesthesiology, The First Affiliated Hospital of Zhejiang University of Medicine, Haining Branch, Haining, Zhejiang, People’s Republic of China; 3Department of Anesthesiology, Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xianhui Kang; Shengmei Zhu, The First Affiliated Hospital, Zhejiang University School of Medicine, No. 79 Qingchun Road, Hangzhou, Zhejiang, 310003, People’s Republic of China, Email [email protected]; [email protected]
Background: Remimazolam is widely employed in surgical abortions. However, its dosing references from clinical studies such as gastrointestinal and bronchoscopic anesthesia have resulted in high incidence of physical movement.
Purpose: Determining the optimal dosage (the 90% effective dose [ED90]) for preventing physical movement during surgical abortions.
Patients and Methods: Fifty-seven individuals aged 18 to 45 undergoing surgical abortion were included. Remimazolam, combined with remifentanil, was utilized for anesthesia induction. Commencing at an initial dose of 0.25 mg/kg of remimazolam, subsequent adjustments relied on the preceding patient’s response, employing an up-down sequential allocation utilizing a biased-coin design.
Results: Patients received remimazolam doses ranging from 0.25 to 0.65 mg/kg. The estimated ED90, along with its 95% confidence interval (CI), for preventing physical movement was 0.615 mg/kg (0.398– 0.629 mg/kg). Patients maintained stable circulation, and no significant adverse events were recorded. Patients reported a satisfaction score of 4.63 ± 0.62 points. Anesthesiologists rated their satisfaction at 4.19 ± 0.61 points, and endoscopists expressed a satisfaction level of 4.53 ± 0.57 points (based on a full score of 5 points, with a minimum of 1 point).
Conclusion: The ED90 of remimazolam during surgical abortion to prevent physical movement was determined to be 0.615 mg/kg (95% CI, 0.398– 0.629 mg/kg).
Keywords: surgical abortion, 90% effective dose, remimazolam, anesthesia
Introduction
Surgical abortion is a common intervention for termination of pregnancy. The indications for the termination of pregnancy can be divided into three categories “unwanted pregnancies”, “maternal medical disorders” and “foetal reasons”.1 Surgical abortion methods include uterine aspiration, by manual or electric vacuum, and dilation and evacuation. However, uterine cervical traction and intrauterine operation during surgery can cause pain, provoke physical movement, and amplify the surgical risks.2 Moreover, the duration of the abortion procedure is short. Hence, the anesthesia must suppress physical movement while aligning with the requirements of rapid onset and recovery. Undoubtedly, this presents a challenge in the selection and dosage of anesthetics.
Remimazolam is a novel ester-benzodiazepine drug with the advantages of high clearance rate, short duration of action, rapid recovery, hemodynamic stability, and little respiratory depression.3 Based on these advantages, the use of remimazolam in gastroenteroscopy and bronchoscopy has been recognized.4–6 Studies on the application of remimazolam in abortion and hysteroscopy have emerged in the past two years and confirmed that remimazolam has better safety and efficacy than propofol and midazolam. Nevertheless, the dosages employed were based on those documented in prior studies related to gastrointestinal and bronchoscopic anesthesia. The induction and maintenance doses of remimazolam utilized for abortion and hysteroscopic surgery are reported as 0.20–25 mg/kg and 0.48–1.0 mg/kg/h, respectively.7–9 However, at this therapeutic dosage, when remimazolam was combined with remifentanil, the occurrence of physical movement ranged between 30% and 36%.7,10 Therefore, the optimal dose remains unknown. The objective of this study was to determine the optimal dose [90% effective dose (ED90)] of remimazolam to inhibit the physical movement of patients during surgical abortion.
Method
This was a prospective, double-blind, sequential-assignment study. The present study protocol was reviewed and approved by the Institutional Review Board of the First Affiliated Hospital of Zhejiang University of Medicine, Haining Branch (approval No.2023-C-001; date: 26/06/2023). Informed consent was submitted by all subjects when they were enrolled. The study was registered in the Chinese Clinical Trial Registry (ChiCTR2300076360, Principal investigator: Bing Yan, https://www.chictr.org.cn/showproj.html?proj=199813, date: 07/10/2023). This study is in accordance with the Declaration of Helsinki.
Study Population
The study was conducted at the Haining Branch of the First Affiliated Hospital of Zhejiang University School of Medicine. The patient recruitment and follow-up were conducted from 10/10/2023 to 15/12/2023. Patients aged 18 to 45 years with the American Society of Anesthesiologists (ASA) classification of I or II and Body Mass Index (BMI) between 18 and 30 kg/m2 who were scheduled for elective surgical abortion under intravenous anesthesia were eligible for inclusion in the study. The exclusion criteria were as follows: 1. Expected operative duration ≥30 minutes; 2. Patients with difficult airways; 3. History of hypertension (systolic blood pressure > 180mmHg or diastolic blood pressure > 110mmHg); 4. Hepatic and renal insufficiency; 5. Chronic lung disease with SPO2 < 95% while inhaling air; 6. Long-term use of analgesics/psychotropic drugs or long history of alcohol abuse; 7. Patients who experienced sedatives 24 hours before surgery; 8. Patients with allergies to benzodiazepines, opioids, and nonsteroidal anti-inflammatory drugs. The withdrawal criteria included: 1. Patients who failed the study due to temporary change of surgical method; 2. Emergency events such as massive bleeding or uterine perforation caused by surgical procedures; 3. Other special circumstances that resulted in the suspension of the surgical operation or the inability to conduct the study.
Perioperative Anesthesia Management
All patients were fasted for 8 hours and water for 3 hours without preoperative medication. The patients were equipped with routine electrocardiogram (ECG) monitoring, non-invasive blood pressure, oxygen saturation, and nasal inhalation of oxygen 3L/min. Patient characteristics (age, height, weight, ASA rating) were recorded. Heart rate (HR), blood pressure, pulse oxygen saturation (SpO2) and respiratory rate (RR) were recorded before induction (T0). Infusion of remifentanil was started with TCI pump, and the effective effect-site concentration (Ce) was 1.5 ng/mL.11 Subsequently, a 30mL remimazolam solution, prepared by the assistant, was administered at a consistent rate for induction (with an injection duration of 60±10s). Another anesthesiologist assessed the anesthetic effect, recording signs and any adverse events following induction (T1). The gynecologist commenced the surgical procedure when the Modified Observer’s Alertness/Sedation score was ≤2. In the case of general anesthesia abortion in this study, no additional topical analgesia was administered to each patients. Subsequent to the procedure, patients were transferred to the Post-Anesthesia Care Unit (PACU). Discharge from PACU occurred once the Aldrete score reached 10. A 24-hour post-surgery follow-up was conducted via telephone. Standardized assessment framework by telephone included Assessment Domains (Recovery Quality: consciousness, respiration, activity status, etc.; Neuropsychiatric Symptoms: dizziness, fatigue, drowsiness; GI Symptoms: nausea and vomiting; Others: open-ended questions for unexpected symptoms) and Quality Control (dual-trained research nurses conducted follow-ups; double-blind data entry system implemented). Vital signs and adverse events were monitored and documented during cervical dilation (T2), uterine aspiration (T3), the end of the operation (T4), and the time of patient discharge from PACU (T5).
If there was any physical movement observed during the procedure, an intravenous injection of 0.05 mg/kg of remimazolam was administered to mitigate it. The anesthetic effect was assessed after one minute. If adequate sedation was not achieved after three additional remimazolam interventions, intravenous administration of 1–2 mg/kg of propofol was initiated. In cases of hypotension, 200mL of lactated Ringer’s solution was intravenously administered. If this did not resolve the issue, vasoactive medications such as 6mg of ephedrine or 40ug of phenylephrine were administered. In the event of bradycardia, an intravenous injection of 0.5 mg of atropine was administered. If hypoxemia or respiratory depression occurred, steps were taken, including increasing oxygen flow, jaw support, suspending surgery, and implementing noninvasive mechanical ventilation if deemed necessary.
Remimazolam Administration
The dose of remimazolam for each patient in this study depends on the physical movement of the previous patient. Following the outcomes of the preliminary investigation and available literature, the initial predetermined dose of remimazolam for subject No. 1 was established at 0.25 mg/kg. Subsequent dosages were adjusted based on the prior patient’s reactivity. If the previous patient exhibited physical movement, the remimazolam dosage for the subsequent patient was increased by 0.05 mg/kg. Conversely, if no physical movement was observed, the remimazolam dosage for the next patient either decreased by 0.05 mg/kg or remained unchanged, as determined by a computer-generated list. The 0.05 mg/kg dose increment for remimazolam is based on pharmacokinetics, statistical validation, and prior studies. Remimazolam showed a high clearance, a small steady-state volume of distribution and a short terminal half-life.12 Regarding the use of remimazolam, the FDA recommends a minimum effective incremental dose of 0.05 mg/kg (approximately 0.25–0.30 mg for individuals weighing 50–60 kg), as stated in Section 2.4 “FDA Clinical Pharmacology Review for Remimazolam (NDA 212295)”. In addition, this step size, also used in the US gastroenteroscopy trial, ensures effective titration while maintaining safety and compliance with dosing principles.13
The preparation of remimazolam was conducted by a nurse uninvolved in anesthesia management and research. Predetermined remimazolam doses were compounded in 20 mL syringes in accordance with the aforementioned dosage assignments. A statistician generated random allocation sequence. An anesthesiology resident enrolled participants and assigned participants to interventions.
Outcomes
The primary outcome was the ED90 of remimazolam inhibiting physical movement, which was defined as visible hand/foot bending or head movement within 2 minutes after entering the uterus. The second outcome of this study was the incidence of adverse events, including hypotension (mean arterial pressure [MAP] decreased 20% from baseline for >5 minutes), bradycardia (heart rate <60 beats/min for >5 minutes), and hypoxemia (under nasal catheter oxygen inhalation, SPO2 <95% for 30 seconds). Injection pain (remimazolam), visual analogue scale (VAS), nausea, vomiting, and dizziness were also recorded. To evaluate postoperative nausea and vomiting (PONV), the Baxter scale was employed, categorizing scores as follows: 0 denoted no nausea; 2 to 4 points indicated mild nausea; 6 to 8 points signified severe nausea; a score of 10 indicated vomiting. The definition of significant nausea fell within the range of 6 to 8 on the scale.
Statistics
When determining ED90 (τ = 0.9), using the following formula: probability (B) = (1 - τ)/τ = (1–0.9)/0.9 = 0.1/0.9≈0.11. The B is the target percentage. If the patient did not show physical movement, the next patient would either receive the same dose (probability 1–11% = 89%) or a lower dose (probability 11%), which was randomly decided using a computer-generated random list prepared by a statistician who was not involved in any other part of the study. The random list was represented by 0 and −1. 0 indicates that the dose of remazolam was unchanged, and −1 indicates that the dose was reduced by one unit (0.05mg/kg). If physical movement occurred, the dose of remazolen was increased by 0.05mg/kg for the next patient. Studies found that a sequential allocation of biased coin design (BCD) was used to find the optimal anesthetic dose, requiring at least 20–40 patient target events.14–16 The trial was terminated when 45 patients experienced non-physical movement.
Measurement data with normal distribution were described as mean ± standard deviation (SD), while the non-normal distribution was expressed as median and interquartile range (IQR). Categorical variables were described as frequencies and percentages. Potential outliers were further screened using histograms and Q-Q plots. One-Way Repeated Measures ANOVA was used to compare the measurement data at different time points. Mauchly’s test was used to assess sphericity. When the assumption was violated (p < 0.05), Greenhouse-Geisser corrections were applied to adjust degrees of freedom. Post hoc pairwise comparisons were performed with Bonferroni adjustment for multiple comparisons. ED90 was determined via centered isotonic regression with a bias-corrected Morris 95% confidence interval (CI) derived by 2000 bootstrap using “dosefind” and “quickinverse” command. Adjusted response rates, following the pooled-adjacent-violators algorithm (PAVA), were estimated using the weighted isotonic regression technique.
Result
Clinical Characteristics of the Patients
The patient recruitment and follow-up were showed in Figure 1. We identified 61 eligible patients. Four were excluded: one due to age >45 years, two with a BMI <18 or >30 kg/m2, respectively, and one patient declined to participate before anesthesia. Finally, 57 patients provided informed consent and completed the study. General clinical characteristics of the patients are presented in Table 1. The Shapiro–Wilk p-values for age, height, weight, duration of abortion surgery, duration of anesthesia, time from end of surgery to eye-opening and duration of anesthesia recovery were 0.134, 0.666, 0.096, 0.257, 0.636, 0.049 and 0.246, respectively. Although the Shapiro–Wilk test for time from end of surgery indicated a statistically significant deviation from normality (p = 0.049), the histogram exhibited an approximately bell-shaped distribution. Based on the combined evaluation of graphical patterns and the conservative thresholds for skewness (0.22) and kurtosis (0.85), this variable was interpreted as adhering to the normality assumption.
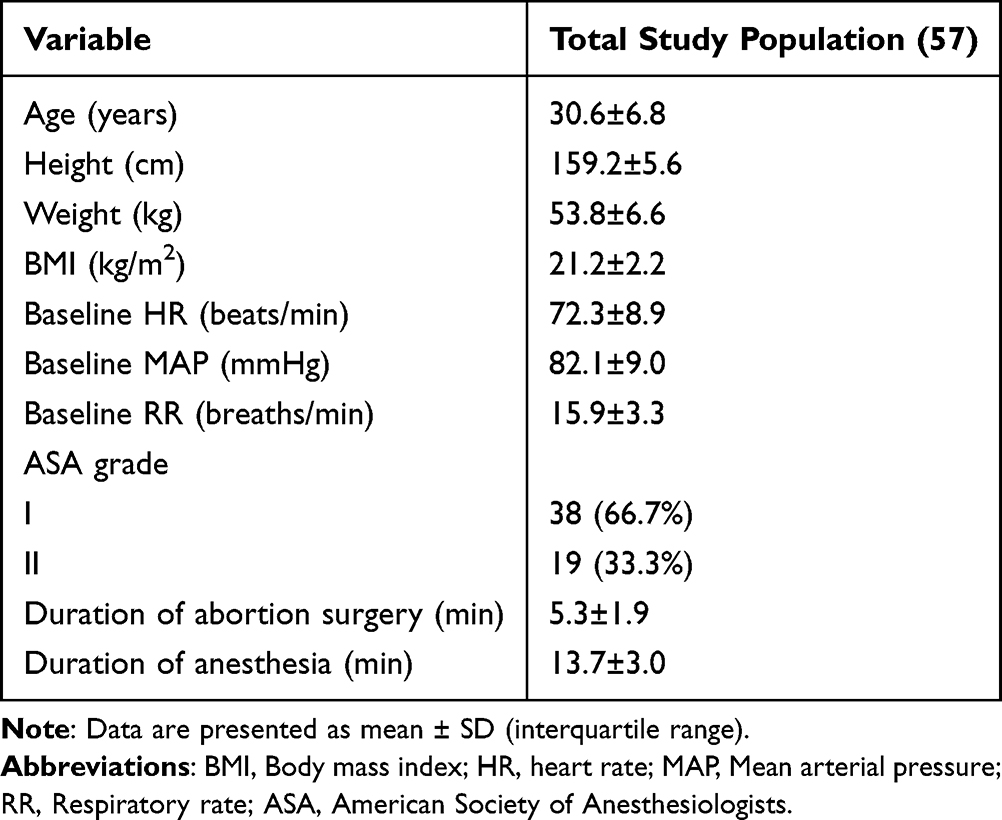 |
Table 1 Demographic and Baseline Characteristics of the Patients |
 |
Figure 1 Flow chart. Positive (+), no physical movement response; negative (-), physical movement response. |
The ED90 of Remimazolam to Inhibit Physical Movement
The up-and-down BC dose allocation sequence was shown in Figure 2. The remimazolam dose ranged from 0.25 to 0.65 mg/kg. There were 45 patients with no physical movement and 12 patients with physical movement. One patient received a dose of 0.25 mg/kg and performed a physical movement. Five patients received a dose of 0.65 mg/kg, and the anesthetic effect was satisfactory. Table 2 illustrates the positive response (no physical movement) of every patient to the administered doses of remimazolam, alongside the positive response adjusted using PAVA. The ED90, estimated through the application of centered isotonic regression, stood at 0.615 mg/kg, with a 95% CI of 0.398–0.629 mg/kg.
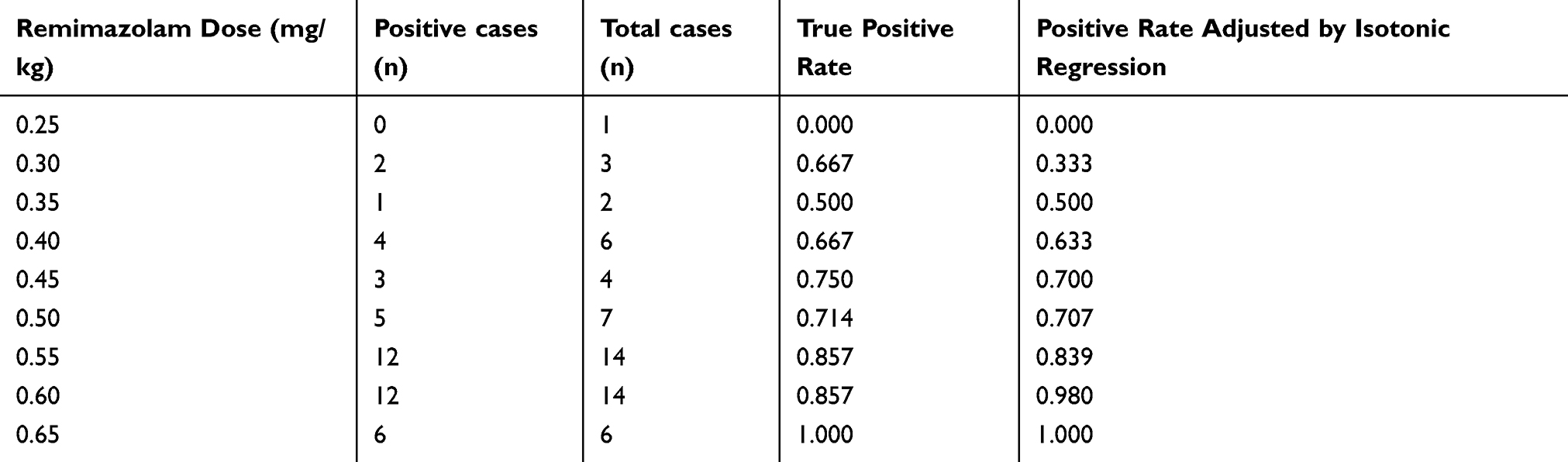 |
Table 2 The True Positive Rate of Different Remimazolam Doses and the Positive Rate Adjusted by Isotonic Regression |
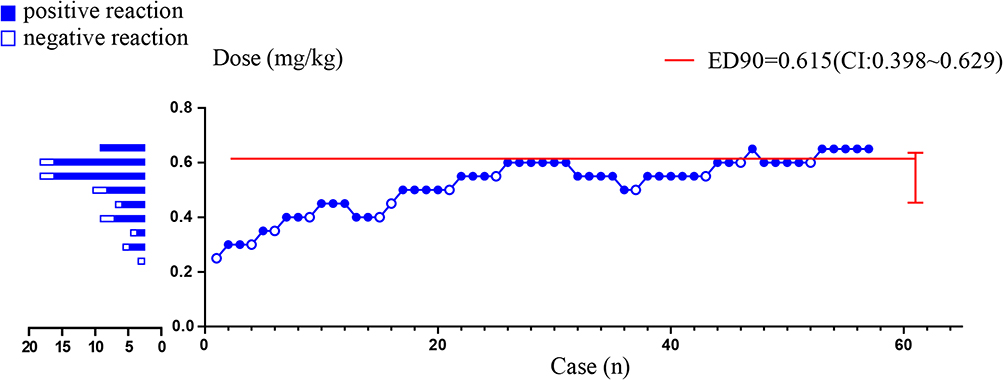 |
Figure 2 The up-down sequential response to infusion of remimazolam for preventing physical movement in surgical abortions. The initial dose was 0.25 mg/kg, with subsequent increases of 0.05 mg/kg. Successful prevention of physical movement (positive reaction) is marked by filled circles, while open circles represent unsuccessful doses (negative reaction). The red solid line (—) indicates the estimated ED90 value and its 95% confidence interval after statistical analysis. |
Adverse Events
Hypotension occurred in 8 patients. Bradycardia, nausea, vomiting, and shivers occurred in 1 case respectively. Respiratory depression occurred in 2 patients. No patient experienced injection pain and hiccups, as shown in Table 3.
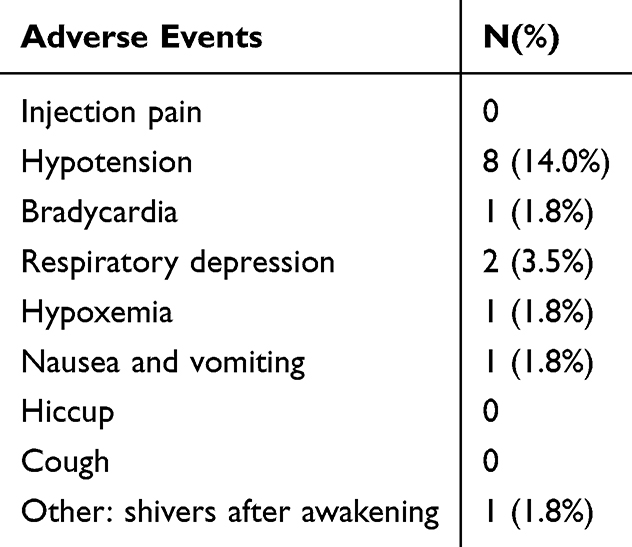 |
Table 3 The Incidence of Adverse Events |
Circulatory and Respiratory During Anesthesia
There were 6 observation time points: 1 min before induction (T0), 1 min after induction (T1), cervical dilation (T2), uterine aspiration (T3), the end of the procedure (T4) and the time of discharge from PACU (T5). Changes in MAP at each observation time point were shown in Figure 3A, with a mild decrease at T1 and T2. For MAP with the Shapiro–Wilk p > 0.05, Mauchly’s test indicated sphericity violation (W = 0.355, χ²(14) = 55.988, p < 0.001), requiring Greenhouse-Geisser correction (ε = 0.73). Time significantly affected MAP (F(3.657, 204.814) = 49.235, p < 0.001, η² = 0.46), with post hoc differences at T 1 vs 2 (p < 0.05). For HR with the Shapiro–Wilk p > 0.05, Mauchly’s test indicated sphericity violation (W = 0.163, χ²(14) = 97.996, p < 0.001), requiring Greenhouse-Geisser correction (ε = 0.66). Time significantly affected HR (F(3.335, 186.783) = 15.336, p < 0.001, η² = 0.215), with post hoc differences at T1, T2, T3, T5 (p < 0.05). But HR was still within the normal range, as shown in Figure 3B. Although RR showed non-normality for the Shapiro–Wilk p < 0.05, Mauchly’s test indicated sphericity (W = 0.663, χ²(14) = 22.211, p = 0.075). As suggested by the findings of María J. Blanca et al, repeated measures ANOVA is generally robust to non-normality when the sphericity assumption is met.17
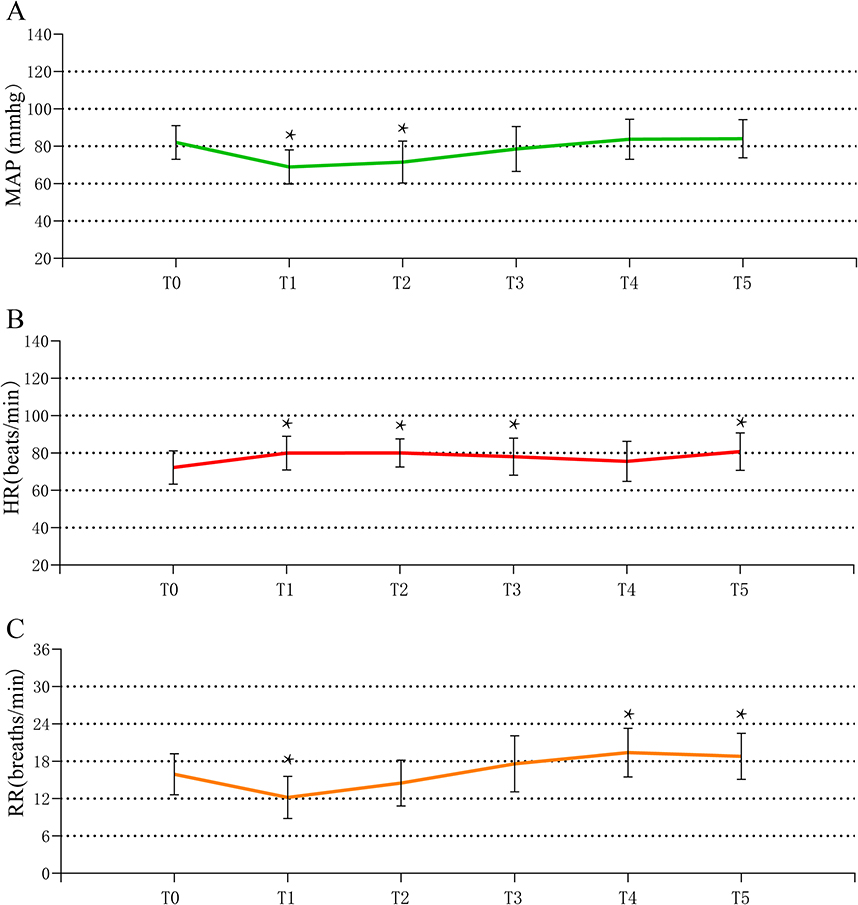 |
Figure 3 Perioperative circulatory and respiratory changes. (A) shows mean arterial pressure at different time points, (B) shows heart rate, and (C) shows respiratory rate. T0, 1 min before induction; T1, 1 min after induction; T2, cervical dilation; T3, uterine aspiration; T4, the end of the procedure; T5, the time of discharge from PACU. *The difference between the T and T0 was statistically significant (P < 0.05). |
Time significantly affected respiratory rate (F(5, 280) = 49.416, p < 0.001, η² = 0.469), with post hoc differences at T1. At T4 and T5, p < 0.001. Multivariate tests (F = 42.566, p < 0.001) supported these findings, as shown in Figure 3C. The respiratory rate fluctuated within the normal range.
Satisfaction Survey
A collective of 57 satisfaction surveys was fulfilled by patients, anesthesiologists, and surgeons, scoring within the range of 1 to 5. More specifically, patients reported a satisfaction score of 4.63±0.62, anesthesiologists rated their satisfaction at 4.19±0.61, and surgeons indicated a satisfaction score of 4.53±0.57, as outlined in Table 4.
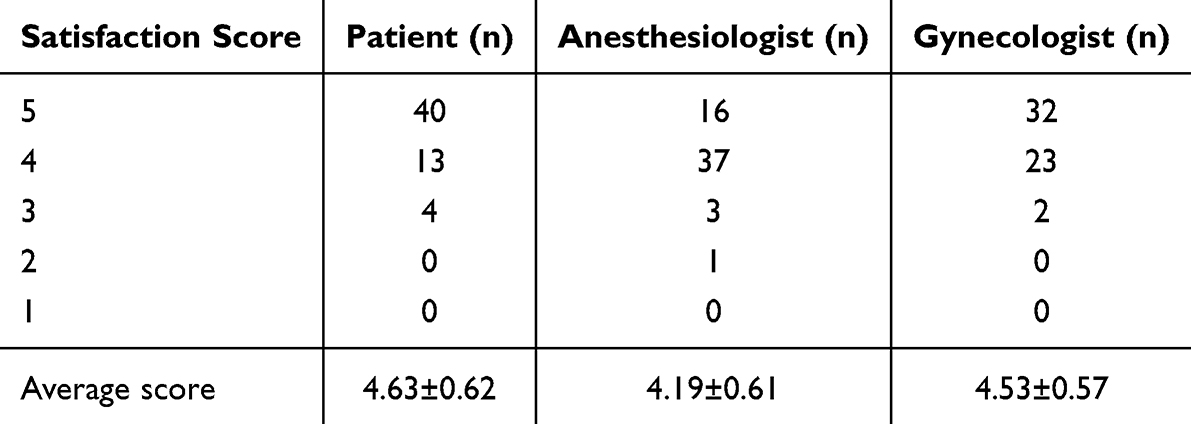 |
Table 4 Anesthesia Satisfaction Score |
Discussion
Effective anesthesia is essential for pain control and safety in surgical abortion, typically using short-acting sedatives and opioids.18 Remimazolam, a novel short-acting ester-benzodiazepine drug, has been shown to be safe and effective in abortion and hysteroscopic anesthesia. However, the dose used was based on data from Phase II and III clinical trials for gastroscopy, colonoscopy, and bronchoscopy.6,13,19 The incidence of physical movement reactions was 21% to 36% when 0.20 to 25 mg/kg remimazolam combined with remifentanil was used in abortion and hysteroscopic anesthesia.7,10,20 In this up-down sequential allocation study with BCD, the ED90 of remimazolam for physical movement prevention in patients who underwent surgical abortion was estimated to be 0.615 mg/kg (95% CI 0.398–0.629 mg/kg).
Sequential design, especially up-and-down methord (UDM), and BCD, is commonly used in anesthetic dose exploration studies.21–24 The Dixon and Mood design of the binary response experiment was designed to estimate the minimum dose, providing a 50% probability of favorable response (ED50). Effectiveness percentiles other than 50% are usually required. It is considered that 50% efficacy is an inappropriately low threshold in anesthesia and that 90% or 95% of the effective dose (ED90 or ED95) should be targeted, which is more interested for anesthesiologists.15 The UDM experiment is usually used to de determine ED50. In the UDM test, around the midpoint of the tolerance distribution, multiple mathematical models fit the observed data equally well, but at the upper tail of the distribution, the estimates of ED90 can be quite different under these mathematical models.15 Moreover, although sigmoid dose–response curves for all drugs can be well fitted by the symmetric logistic curves, they are impossible to verify, especially when dealing with small sample sizes. Based on modifying the dose allocation rules of the UDM, BCD achieves these goals.14 In the BCD test, unverifiable assumptions about sigmoid dose–response curves were avoided. In addition, the study had favorable statistical characteristics for the target-dose estimates. Thus, BCD can directly estimate ED90, avoiding the unverifiable extrapolation obtained from ED 50.15
Remimazolam is gaining attention in outpatient surgery due to its rapid onset, fast metabolism, high clearance, short half-life, and inactive metabolite.25,26 In elderly patients undergoing gastrointestinal endoscopy, when combined with 0.2 μg/kg remifentanil, the ED95 dose of remimazolam to inhibit physical movement was 0.204 (95% CI 0.175–0.389) mg/kg.27 In the published safety studies of remimazolam in surgical abortion and hysteroscopic surgery, remimazolam was used at a similar dose. The primary outcome in these studies was the incidence of adverse events (injection pain, low SpO2, bradycardia, hypotension, nausea and vomiting), which was satisfactorily low.7,10 However, the incidence of the physical movement, the secondary outcome in these studies, was as high as 21%–36%.7,10,28 Preventing physical movement is essential to facilitate a smooth abortion procedure, guaranteeing patient comfort and safety. A recent study attempted to investigate the combination of remimazolam and propofol to inhibit the physical movement, and the results showed that it could reduce the physical movement from 37.5% to 3.1%.20 Obviously, exploring the ED90 of remimazolam inhibiting the physical movement would be more beneficial to take its full advantage. Our results showed an ED90 of 0.615 mg/kg (95% CI, 0.398–0.629 mg/kg) for remimazolam to inhibit physical movement. The dosage observed in our study exceeded the findings from the mentioned gastroenteroscopy study. This variance might stem from our study’s inclusion of a non-elderly patient population. Moreover, it is plausible that the level of painful stimulation experienced during surgical abortion surpasses that of gastrointestinal endoscopic procedures.
Recent studies have also explored the intranasal administration of remimazolam.29 Pesic et al reported that intranasal remimazolam had a bioavailability of approximately 50% and an onset time of around 10 minutes in healthy adults.30 In pediatric preoperative sedation, Cai et al found that intranasal remimazolam (1.5 mg/kg) rapidly alleviated anxiety within 10 minutes though nasal.31 Long et al showed that ED95 of single nasal administration of remimazolam for effective relief of preoperative anxiety was 1.57 and 1.09 mg/kg in early childhood children and pre-school children, respectively.32 Additionally, Ni et al determined the ED50 and ED95 of intranasal remimazolam in preschool children as 0.65 mg/kg and 0.78 mg/kg, respectively, supporting its rapid sedative potential (onset within 6–9 minutes).33 Notably, the ED90 dose for intravenous administration in this study (0.615 mg/kg) was significantly lower than the effective doses reported in intranasal studies. This discrepancy may be reasonable for that intravenous administration avoids the bioavailability loss associated with the intranasal route. Nasal administration of remimazolam may be an alternative method for patients undergoing induced abortion without venous access, but this needs further research in the future.
Throughout our study, no severe adverse events were observed. In a previous multicenter, Phase 3 clinical trial focused on patients undergoing colonoscopy, and the incidence rates of bradycardia, respiratory depression, and hypotension were 1.03%, 3.09%, and 23.71%, respectively, among those who received fentanyl 1 ug/kg and remimazolam 5.0 mg for anesthesia.34 Nicholas J. Pastis et al conducted a multicenter study demonstrating satisfactory safety and efficacy using 5mg of remimazolam alongside 25–75 ug of fentanyl during fiberoptic bronchoscopy. They reported incidence rates of 4.3% for bradycardia, 2.3% for respiratory depression, and 41.9% for hypotension.6 Insun Park et al administered remimazolam at 0.4 mg/kg and remifentanil at 1.07 μg/kg during hysteroscopy, reporting incidence rates of 10.8% for bradycardia, 2.3% for respiratory depression, and 21.6% for hypotension.35 Xiaoqiang Zhang et al also reported low adverse event rates in their hysteroscopy study.7,10 In our trial, occurrences of bradycardia, respiratory depression, and hypotension were observed in patients who received a dosage of 0.4–0.6 mg/kg of remimazolam, with incidence rates of 1.8%, 3.5%, and 14.0%, respectively, aligning with the findings of the previously mentioned studies. However, Dongwoo Chae et al found that remimazolam showed steep dose–response effects on loss of consciousness and respiratory depression, with ED50/ED95 of 0.11/0.19 and 0.14/0.27 mg/kg, respectively.36 This result is obviously different from the incidence of respiratory depression reported in the above studies, which may be caused by the inconsistent definition of respiratory depression. Given the constraints of our study’s sample size, it remains imperative to enlarge the sample size further to validate the safety of the ED90 dose established in our trial.
PONV is one of the most common complications after general anesthesia.37 Major risk factors for PONV include female gender, previous history of motion sickness or PONV, nonsmoking, and postoperative opioid use.38 The incidence of PONV in women ranges from 21% to 79%.38 Na Wang et al reported an incidence of PONV as high as 50% within 24 hours after abortion and hysteroscopic surgery.39 Yuki Hari et al found that remimazolam reduced the incidence of PONV in patients undergoing gynecological laparoscopic surgery in the early postoperative period.40 In a study of 204 hysteroscopic procedures, the incidence of postoperative nausea and vomiting was 2.0% in the remmazolene group.10 The lack of PONV observed in our study might be attributed to either the limited sample size or the higher dosage of remimazolam employed. Additionally, further investigation is warranted to determine if remimazolam can effectively mitigate PONV and explore any potential correlation between the dosage of remimazolam and the occurrence of PONV.
There were certain limitations observed in our study. First, this study focused solely on female patients undergoing surgical abortion, and the determined dosage may not be directly applicable to other surgical procedures with different pain stimuli, durations, or patient populations, such as male patients or those undergoing more invasive gynecological surgeries. Second, while remifentanil was used as an adjunct opioid in this study, variations in opioid selection, dosage, or combination regimens may alter the ED90 of remimazolam. Future studies should explore whether alternative opioid regimens or multimodal anesthesia approaches can optimize sedation while minimizing adverse effects. Third, although our study identified an ED90 of 0.615 mg/kg, the sample size was relatively small, limiting the ability to assess rare adverse events, especially those related to respiratory depression or hemodynamic instability at higher doses. Even if no adverse events occurred in our cohort (0/45), this does not exclude potential risks. As highlighted by Hanley and Lippman-Hand, zero numerators require statistical interpretation.41 Applying the Rule of Three, the upper 95% confidence limit for adverse events risk is 3/45 ≈ 6.7%, indicating a plausible risk ceiling despite no observed events. The Rule of Three slightly overestimates risks in small samples, and its accuracy improves with larger sample size. Future larger cohorts could refine this estimate. Fourth, while remimazolam has been suggested to reduce postoperative nausea and vomiting (PONV), our study did not systematically evaluate its impact on PONV incidence. Future research should examine whether remimazolam at its ED90 dose provides an advantage in reducing PONV compared to other sedatives.
Conclusions
For patients undergoing surgical abortion, the ED90 of remimazolam to inhibit physical movement was determined to be 0.615 mg/kg. Additionally, adverse events such as respiratory depression and injection pain were infrequent.
Data Sharing Statement
The datasets used in the current study are available from the corresponding author (Xianhui Kang) upon reasonable request.
Ethics approval and informed consent
The protocol was approved by the Clinical Research Ethics Committee of the Haining People’s Hospital (No.2023-C-001). Participant gave written informed consent.
Consent for Publication
Written informed consent was obtained from the patients to publish.
Acknowledgments
Thе rеsеarchеrs would likе to еxprеss thеir dееpеst gratitudе to thе patiеnts participating in thе study, Haining People’s Hospital and The First Affiliated Hospital, Zhejiang University School of Medicine.
Author Contributions
All authors made a significant contribution to the work reported. Pengfei Yin, Binwei Hu and Bing Yan took part in the conception, study design, execution, acquisition of data, analysis and interpretation; Fuquan Fang took part in drafting, Lei Li and Huiling Li revised or critically reviewed the article; Shengmei Zhu gave final approval of the version to be published; Xianhui Kang have agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Zhejiang Provincial Natural Science Foundation of China (No. LQ24H010002; No. LZ24H090002) and 2023 Haining Science and Technology Project (No.2023151).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Agaoglu Z, Tanacan A, Haksever M, et al. Retrospective analysis of the indications, methods, and complications of pregnancy termination. Turk J Obstet Gynecol. 2024;21(4):273–279. doi:10.4274/tjod.galenos.2024.88886
2. Yen CF, Chou HH, Wu HM, Lee CL, Chang TC. Effectiveness and appropriateness in the application of office hysteroscopy. J Formos Med Assoc. 2019;118(11):1480–1487. doi:10.1016/j.jfma.2018.12.012
3. Kilpatrick GJ. Remimazolam: non-clinical and clinical profile of a new sedative/anesthetic agent. Front Pharmacol. 2021;12:690875. doi:10.3389/fphar.2021.690875
4. Rex DK, Bhandari R, Desta T, et al. A Phase III study evaluating the efficacy and safety of remimazolam (CNS 7056) compared with placebo and midazolam in patients undergoing colonoscopy. Gastrointest Endosc. 2018;88(3):427–437e426. doi:10.1016/j.gie.2018.04.2351
5. Yao Y, Guan J, Liu L, Fu B, Chen L, Zheng X. Discharge readiness after remimazolam versus propofol for colonoscopy: a randomised, double-blind trial. Eur J Anaesthesiol. 2022;39(12):911–917. doi:10.1097/EJA.0000000000001715
6. Pastis NJ, Yarmus LB, Schippers F, et al. Safety and efficacy of remimazolam compared with placebo and midazolam for moderate sedation during bronchoscopy. Chest. 2019;155(1):137–146. doi:10.1016/j.chest.2018.09.015
7. Zhang X, Li S, Liu J. Efficacy and safety of remimazolam besylate versus propofol during hysteroscopy: single-centre randomized controlled trial. BMC Anesthesiol. 2021;21(1):156. doi:10.1186/s12871-021-01373-y
8. Zhang S, Wang J, Ran R, Peng Y, Xiao Y. Efficacy and safety of remimazolam tosylate in hysteroscopy: a randomized, single-blind, parallel controlled trial. J Clin Pharm Ther. 2022;47(1):55–60. doi:10.1111/jcpt.13525
9. Fan S, Zhu Y, Sui C, Li Q, Jiang W, Zhang L. Remimazolam compared to propofol during hysteroscopy: a safety and efficacy analysis. Pain Ther. 2023;12(3):695–706. doi:10.1007/s40122-023-00483-4
10. Zhang X, Li S, Liu J. Remimazolam-remifentanil causes less postoperative nausea and vomiting than remimazolam-alfentanil during hysteroscopy: a single-centre randomized controlled trial. BMC Anesthesiol. 2023;23(1):199. doi:10.1186/s12871-023-02164-3
11. Minto CF, Schnider TW, Egan TD, et al. Influence of age and gender on the pharmacokinetics and pharmacodynamics of remifentanil. I. Model development. Anesthesiology. 1997;86(1):10–23. doi:10.1097/00000542-199701000-00004
12. Schuttler J, Eisenried A, Lerch M, Fechner J, Jeleazcov C, Ihmsen H. Pharmacokinetics and pharmacodynamics of remimazolam (CNS 7056) after continuous infusion in healthy male volunteers: part I. pharmacokinetics and clinical pharmacodynamics. Anesthesiology. 2020;132(4):636–651. doi:10.1097/ALN.0000000000003103
13. Borkett KM, Riff DS, Schwartz HI, et al. A Phase IIa, randomized, double-blind study of remimazolam (CNS 7056) versus midazolam for sedation in upper gastrointestinal endoscopy. Anesth Analg. 2015;120(4):771–780. doi:10.1213/ANE.0000000000000548
14. Gorges M, Zhou G, Brant R, Ansermino JM. Sequential allocation trial design in anesthesia: an introduction to methods, modeling, and clinical applications. Paediatr Anaesth. 2017;27(3):240–247. doi:10.1111/pan.13088
15. Pace NL, Stylianou MP, Warltier DC. Advances in and limitations of up-and-down methodology: a precis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
16. Zhang X, Wang J, An XH, et al. Optimum dose of spinal ropivacaine with or without single intravenous bolus of S-ketamine during elective cesarean delivery: a randomized, double-blind, sequential dose-finding study. BMC Pregnancy Childbirth. 2021;21(1):746. doi:10.1186/s12884-021-04229-y
17. Blanca MJ, Arnau J, Garcia-Castro FJ, Alarcon R, Bono R. Non-normal data in repeated measures ANOVA: impact on type I error and power. Psicothema. 2023;35(1):21–29. doi:10.7334/psicothema2022.292
18. Munro MG. Complications of hysteroscopic and uterine resectoscopic surgery. Obstet Gynecol Clin North Am. 2010;37(3):399–425. doi:10.1016/j.ogc.2010.05.006
19. Pambianco DJ, Borkett KM, Riff DS, et al. A phase IIb study comparing the safety and efficacy of remimazolam and midazolam in patients undergoing colonoscopy. Gastrointest Endosc. 2016;83(5):984–992. doi:10.1016/j.gie.2015.08.062
20. Zhang F, Chang H, Qing W, Yu R, Liao Q, Tong J. Remimazolam tosylate combined with low-dose propofol improves sedation and safety in hysteroscopy. Drug Des Devel Ther. 2022;16:4101–4108. doi:10.2147/DDDT.S390403
21. Dixon WJ, Mood AM. A method for obtaining and analyzing sensitivity data. J Am Stat Assoc. 1948;43(241):109–126. doi:10.1080/01621459.1948.10483254
22. Dixon WJ. The up-and-down method for small samples. J Am Stat Assoc. 1965;60(312):967–978. doi:10.1080/01621459.1965.10480843
23. Durham SD, Flournoy N, Rosenberger WF. A random walk rule for Phase I clinical trials. Biometrics. 1997;53(2):745–760. doi:10.2307/2533975
24. Jia N, Braun TM. The adaptive accelerated biased coin design for phase I clinical trials. J Appl Stat. 2011;38(12):2911–2924. doi:10.1080/02664763.2011.573540
25. Lee A, Shirley M. Remimazolam: a review in procedural sedation. Drugs. 2021;81(10):1193–1201. doi:10.1007/s40265-021-01544-8
26. Kilpatrick GJ, McIntyre MS, Cox RF, et al. CNS 7056: a novel ultra-short-acting Benzodiazepine. Anesthesiology. 2007;107(1):60–66. doi:10.1097/01.anes.0000267503.85085.c0
27. Ye E, Wu K, Ye H, et al. Comparison of 95% effective dose of remimazolam besylate and propofol for gastroscopy sedation on older patients: a single-centre randomized controlled trial. Br J Clin Pharmacol. 2023;89(11):3401–3410. doi:10.1111/bcp.15839
28. Yue L, Ma X, Li N, et al. Remimazolam versus propofol in combination with esketamine for surgical abortion: a double-blind randomized controlled trial. Clin Transl Sci. 2023;16(9):1606–1616. doi:10.1111/cts.13572
29. Sneyd JR. Remimazolam – current status, opportunities and challenges. Anesthesiol Perioperative Sci. 2023;1(3):25. doi:10.1007/s44254-023-00021-7
30. Pesic M, Schippers F, Saunders R, Webster L, Donsbach M, Stoehr T. Pharmacokinetics and pharmacodynamics of intranasal remimazolam-a randomized controlled clinical trial. Eur J Clin Pharmacol. 2020;76(11):1505–1516. doi:10.1007/s00228-020-02984-z
31. Cai YH, Wang CY, Fang YB, et al. Preoperative anxiolytic and sedative effects of intranasal remimazolam and dexmedetomidine: a randomized controlled clinical study in children undergoing general surgeries. Drug Des Devel Ther. 2024;18:1613–1625. doi:10.2147/DDDT.S461122
32. Long X, Wen LX, Yang H, et al. ED(95) of remimazolam in nasal administration for attenuating preoperative anxiety in children. Front Med. 2023;10:1253738. doi:10.3389/fmed.2023.1253738
33. Ni MJ, Jin YT, Wu QL, et al. Effective dose of intranasal remimazolam for preoperative sedation in preschool children: a dose-finding study using Dixon’s up-and-down method. Front Pharmacol. 2024;15:1372139. doi:10.3389/fphar.2024.1372139
34. Chen S, Wang J, Xu X, et al. The efficacy and safety of remimazolam tosylate versus propofol in patients undergoing colonoscopy: a multicentered, randomized, positive-controlled, phase III clinical trial. Am J Transl Res. 2020;12(8):4594–4603.
35. Park I, Cho M, Nam SW, Hwang JW, Do SH, Na HS. Total intravenous anesthesia induced and maintained by a combination of remimazolam and remifentanil without a neuromuscular blocking agent: a prospective, observational pilot study. BMC Anesthesiol. 2022;22(1):237. doi:10.1186/s12871-022-01779-2
36. Chae D, Kim HC, Song Y, Choi YS, Han DW. Pharmacodynamic analysis of intravenous bolus remimazolam for loss of consciousness in patients undergoing general anaesthesia: a randomised, prospective, double-blind study. Br J Anaesth. 2022;129(1):49–57. doi:10.1016/j.bja.2022.02.040
37. Ignaszak-Kaus N, Duleba AJ, Mrozikiewicz A, et al. Relationship of postoperative pain and PONV after minimally invasive surgery with the serotonin concentrations and receptors’ gene polymorphisms. J Pers Med. 2021;11(9). doi:10.3390/jpm11090833.
38. Darvall J, Handscombe M, Maat B, So K, Suganthirakumar A, Leslie K. Interpretation of the four risk factors for postoperative nausea and vomiting in the Apfel simplified risk score: an analysis of published studies. Can J Anaesth. 2021;68(7):1057–1063. doi:10.1007/s12630-021-01974-8
39. Wang N, Ding P, Zheng DY, et al. Wearable transcutaneous electrical acupoint stimulation bracelet for prevention of postoperative nausea and vomiting in patients undergoing hysteroscopic surgery: a randomised controlled trial. Br J Anaesth. 2022;129(4):e85–e87. doi:10.1016/j.bja.2022.06.028
40. Hari Y, Satomi S, Murakami C, et al. Remimazolam decreased the incidence of early postoperative nausea and vomiting compared to desflurane after laparoscopic gynecological surgery. J Anesth. 2022;36(2):265–269. doi:10.1007/s00540-022-03041-y
41. Hanley JA, Lippman-Hand A. If nothing goes wrong, is everything all right? Interpreting zero numerators. JAMA. 1983;249(13):1743–1745. doi:10.1001/jama.1983.03330370053031
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect-Site Concentration of Remimazolam by Age Groups During Target-Controlled Infusion for Total Intravenous Anesthesia: A Retrospective Comparative Study
Park J, Seo KH, Kwak J, Baek H
Drug Design, Development and Therapy 2024, 18:5149-5159
Published Date: 12 November 2024
Blood Pressure Reduction During Anesthetic Induction with Remimazolam versus Propofol in Elderly Patients: Pharmacodynamic Modeling of Remimazolam
Oh J, Kim KM, Sim JH, Lee EK, Choi BM
Drug Design, Development and Therapy 2025, 19:9571-9580
Published Date: 26 October 2025