Back to Journals » International Journal of Nanomedicine » Volume 21
Biomaterial-Based Strategies for Gout Therapy: Recent Advances, Current Challenges, and Future Perspectives – A Review
Authors Zhang Z, Li R, Wu X, Wang W, Chen B, Zeng H, Pan X, Wang Q, Wang H, Li Y
Received 28 February 2026
Accepted for publication 9 June 2026
Published 3 July 2026 Volume 2026:21 605873
DOI https://doi.org/10.2147/IJN.S605873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. RDK Misra
Zhicheng Zhang,1 Ruiyan Li,1 Xiaohan Wu,2 Wenjie Wang,1 Bo Chen,1 Haolin Zeng,1 Xiangjun Pan,1 Qingshuai Wang,1 Hao Wang,1 Yingzhi Li,1
1Orthopedic Medical Center, The Second Hospital of Jilin University, Changchun, 130022, People’s Republic of China; 2Department of Pathology, The Second Hospital of Jilin University, Changchun, Jilin, 130022, People’s Republic of China
Correspondence: Hao Wang; Yingzhi Li, Orthopedic Medical Center, The Second Hospital of Jilin University, Changchun, 130022, People’s Republic of China, Email [email protected]; [email protected]
Abstract: Gout is a complex and progressive inflammatory disease caused by the deposition of monosodium urate (MSU) crystals. Recent research on the application of biomaterials in gout treatment has shown promising potential. Biomaterials, with their unique biocompatibility, controlled release properties, and targeted delivery capabilities, offer significant advantages in enhancing drug solubility and bioavailability, reducing systemic adverse effects, and enabling more precise and stage-specific therapeutic intervention. In this review, we systematically categorize the various biomaterials applied in gout therapy over the past five years, including nano-drug delivery systems, microneedle drug delivery systems, and novel biomaterial-based therapeutics for gout treatment. We highlight the design principles, construction strategies, and mechanisms of action associated with each type of biomaterial. By comparatively analyzing the functions of different biomaterial platforms, this review further summarizes their potential therapeutic roles, relative advantages, and current limitations in gout management. In addition, we discuss currently used gout-related animal models and their relevance to preclinical evaluation, and synthesize emerging therapeutic targets that may guide future biomaterial design. Overall, this review highlights both the opportunities and the translational challenges of biomaterial-based strategies for gout therapy, providing insights for the development of more targeted, effective, and clinically relevant therapeutic approaches.
Keywords: gout, hyperuricemia, gouty arthritis, gout animal models, drug delivery systems
Introduction
Gout is an inflammatory disease characterized by hyperuricemia and monosodium urate (MSU) crystal deposition.1,2 Although current therapies, including urate-lowering agents,3–5 anti-inflammatory drugs(NSAIDs),6 targeted inhibitors of inflammatory pathways,7 and uricase-based therapies,8,9 can partially control gout, their clinical utility is often limited by low bioavailability, poor specificity, systemic adverse effects, enzyme instability, immunogenicity, and short circulation half-life.10 These limitations have prompted growing interest in biomaterial-based strategies for gout treatment. Owing to their biocompatibility, biodegradability, and tunable delivery properties, biomaterials can improve targeting efficiency, prolong drug release, and reduce systemic toxicity, thereby offering a promising platform for gout therapy.11–14
Biomaterials offer significant benefits in the non-surgical management of gout, particularly in drug delivery and inflammation control. Biomaterials, when used as carriers for drug delivery, can effectively target and control the release of drugs at the site of pathology, thereby enhancing drug bioavailability and minimizing the side effects associated with high systemic doses of conventional oral medications.15,16 In recent years, various biomaterial-based platforms, including nanoparticles, liposomes, hydrogels, microneedles, and bioactive scaffolds, have been explored for gout treatment due to their abilities to improve drug stability, enhance tissue targeting, and enable sustained or stimuli-responsive drug release. The modifiability and material specificity of biomaterials also allow them to exert intrinsic bioactive effects, such as regulating inflammatory responses, promoting MSU crystal dissolution, or inhibiting crystal formation, thereby reducing inflammation and preventing gout flares.17–19 For example, nanomaterials can enhance the intracellular delivery of anti-inflammatory agents, while injectable hydrogels provide localized and sustained therapeutic effects within affected joints. Overall, biomaterial-based systems represent a promising therapeutic strategy for gout treatment due to their abilities to improve drug delivery efficiency, regulate inflammatory responses, and enable multifunctional therapeutic effects. Continued development of these systems may provide new opportunities for improving the clinical management of gout.
The development and validation of biomaterials typically depend on animal models of relevant diseases to assess their efficacy and safety. Currently, gout-related animal models mainly include hyperuricemia models and MSU-induced acute arthritis models, which help replicate key pathological features of gout and assess the in vivo therapeutic effects and biosafety of biomaterials. Recent reviews have provided valuable insights into the application of nanomaterials, hydrogels, liposomes, and other delivery systems for improving anti-inflammatory and urate-lowering therapies in gout.20 These studies have provided valuable perspectives on the therapeutic potential of biomaterial-based approaches and have helped advance this emerging field. Existing review articles have provided important summaries of biomaterial-based drug delivery strategies and therapeutic outcomes in gout. In this context, the present review aims to provide a more integrated perspective by linking the pathological progression of gout with the characteristics of currently available animal models and recent advances in biomaterials for gout treatment. In addition to summarizing drug delivery strategies, mechanisms of action, and therapeutic efficacy, this review also discusses current limitations and translational challenges of biomaterial-based therapies, including biosafety, targeting efficiency, and the insufficient clinical relevance of existing animal models. Finally, we propose future directions for optimizing animal model construction and accelerating the clinical translation of biomaterial-based therapeutics for gout.
Pathogenesis of Gout
Gout typically follows a progressive course, with patients often experiencing minimal discomfort in the early stages of the disease. The onset and progression of gout can be broadly divided into four stages21 (Figure 1), and early intervention is critical to prevent disease progression. The first stage of gout is asymptomatic hyperuricemia (Figure 1A), characterized by sustained serum uric acid levels ≥420 μmol/L,22 without overt clinical symptoms.23 Hyperuricemia results from increased uric acid production or impaired urate excretion, which is primarily regulated by renal and intestinal urate transport systems.
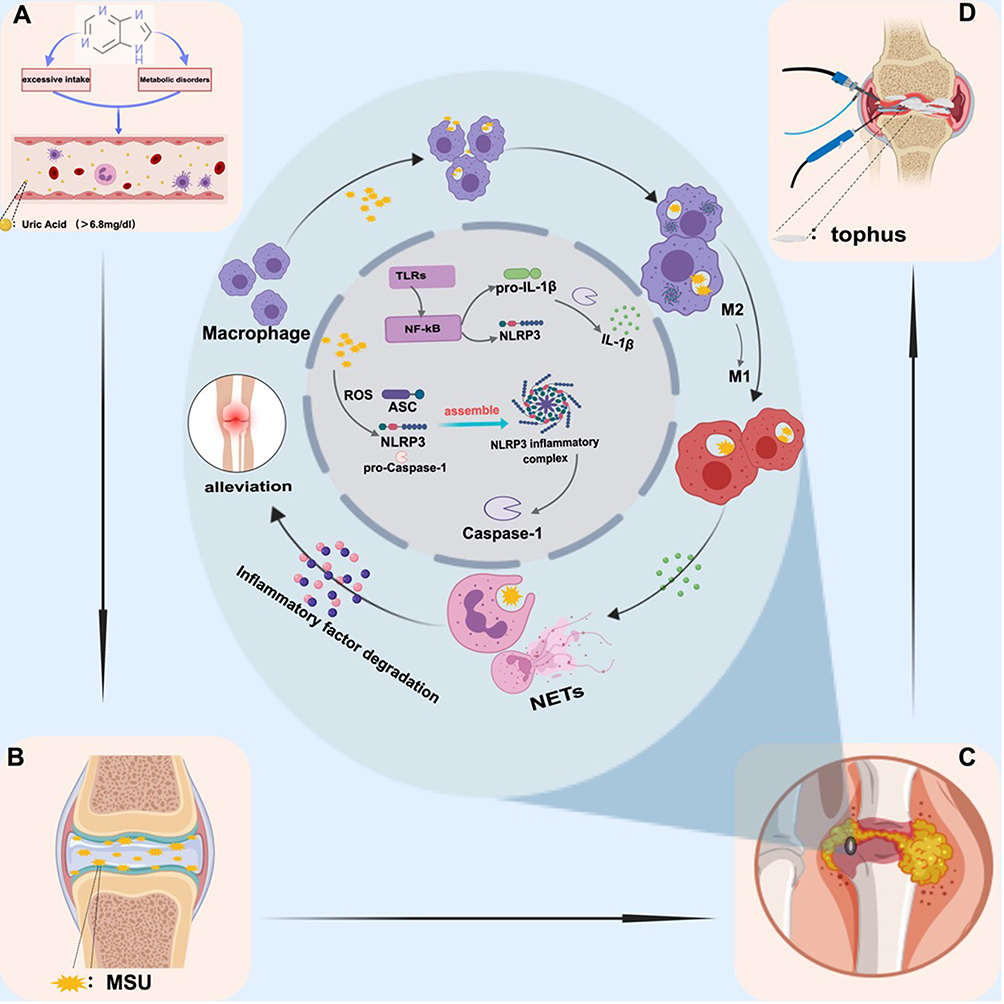 |
Figure 1 The four stages of gout development. (A) Hyperuricemia; (B) Abnormal deposition of MSU in joints; (C) The inflammatory phase and pathogenesis of gout involve the activation of the NF-κB inflammatory signaling pathway. The first signal is triggered by TLRs (Toll-like receptors), and the second signal is activated by monosodium urate (MSU) crystals. These dual signals lead to the assembly of the NLRP3 inflammasome, initiating an inflammatory response mediated by inflammatory cells such as macrophages and neutrophils; (D) Advanced-stage gout and treatment. |
The second stage of gout onset is the asymptomatic deposition of MSU crystals (Figure 1B). Due to persistently elevated uric acid levels in the body, excessive deposition of MSU crystals occurs in the joints or extra-articular tissues, with the lower limb joints being more commonly affected. However, the exact cause of MSU crystal deposition remains unclear24 and may be influenced by factors such as temperature, pH, sodium ion concentration, and the unique structure of the synovial membrane.25 During this stage, although MSU crystals are abnormally deposited, no significant inflammatory response is yet present.
The third stage of gout onset is the acute inflammatory phase, during which the inflammatory response is activated through a dual signaling pathway (Figure 1C). The first signal is initiated by Toll-like receptors (TLRs),1,26 which activate the NF-κB signaling pathway.27 Activation of NF-κB promotes the recruitment of neutrophils and other inflammatory cells, induces the formation of the NLRP3 inflammasome, and promotes the generation of pro-IL-1β.28 The second signal is triggered by MSU crystals. After macrophages and monocytes engulf MSU crystals, mitochondrial reactive oxygen species (ROS) generation and potassium efflux jointly promote the assembly of the NLRP3 inflammasome. The NLRP3 inflammasome also plays an important role in regulating macrophage polarization from the M2 anti-inflammatory phenotype to the M1 pro-inflammatory phenotype,29 Subsequently, the activated NLRP3 inflammasome recruits ASC and Caspase-1, leading to Caspase-1 activation and the maturation of pro-IL-1β into active IL-1β, IL-1β is a key inflammatory cytokine in gout. It promotes vasodilation, induces the recruitment of neutrophils and other immune cells, and stimulates the release of additional inflammatory mediators such as TNF-α and IL-8,30 thereby amplifying local inflammation. Persistent IL-1β signaling can further induce matrix-degrading enzymes, leading to local cartilage and bone destruction and explaining why chronic gout may result in irreversible joint damage. The inflammatory response in gout is generally self-limited, and its resolution is closely associated with the formation of neutrophil extracellular traps (NETs).31,32 NETs help suppress inflammation by degrading inflammatory cytokines, although the regulatory mechanisms underlying NET formation remain unclear.
The fourth stage is chronic tophaceous gout (Figure 1D), characterized by tophus formation, progressive joint destruction, and increased risk of complications such as renal impairment and nephrolithiasis.33 Understanding these pathological stages provides an important basis for developing targeted biomaterial-based strategies for gout treatment.
Methods for Constructing Animal Models of Gout
Current animal models for gout are primarily categorized into hyperuricemia models and gouty arthritis models. Hyperuricemia models can be established by intraperitoneal injection of potassium oxalate solution in experimental animals,34 or by inducing hyperuricemia through a high-fat diet35 or a high-fat, high-purine diet.36 Acute gouty arthritis models can be developed by directly injecting MSU crystals into the joint cavity or peritoneal cavity.37–40 However, the hyperuricemia models created by these methods often fail to accurately replicate the joint swelling, pain, and intra-articular inflammation observed in gout patients. Additionally, the presence of Urate Oxidase (UOX) in many experimental animals, which breaks down uric acid, makes it difficult to establish a stable hyperuricemia model and challenges the simulation of the progressive stages of gout development.41 Similarly, acute gout models generated by direct injection of MSU into the joint or peritoneal cavity fail to mimic the characteristic recurrent attacks of gout and its gradual disease progression. Recent studies have developed improved modeling techniques that more closely resemble the clinical manifestations of gout in humans (Figure 2A).
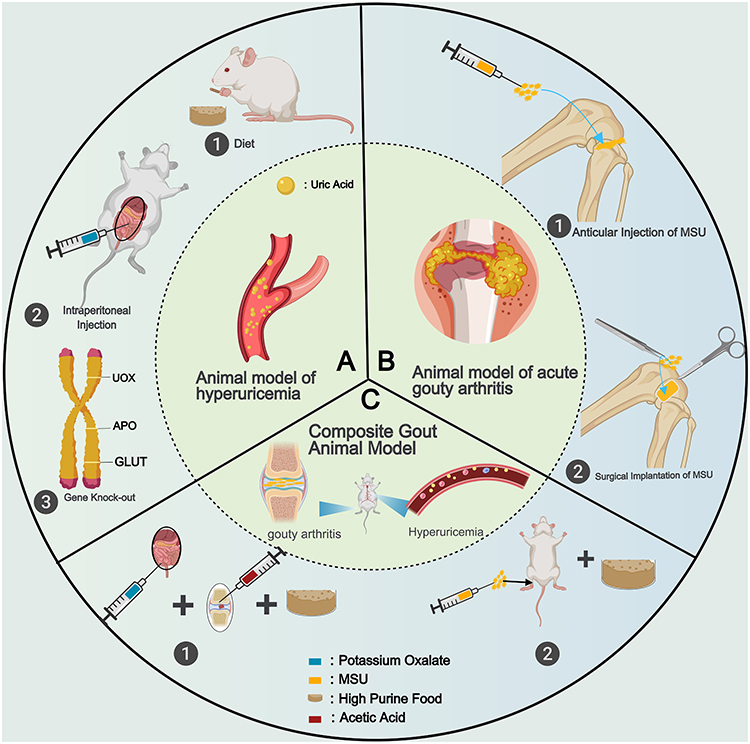 |
Figure 2 Construction methods for gout animal models. The circular schematic is divided into three sectors labeled (A–C) at the center of each sector. (A) Strategies for establishing hyperuricemia animal models, including dietary intervention, intraperitoneal injection, and gene knockout approaches. (B) Strategies for establishing acute gouty arthritis animal models, including intra-articular injection of monosodium urate (MSU) crystals and surgical implantation of MSU crystals. (C) Strategies for establishing combined animal models exhibiting both hyperuricemia and gouty arthritis, including the integration of intraperitoneal injection or dietary intervention with modification of the intra-articular microenvironment, as well as the combination of dietary intervention with intra-articular MSU injection. The numbered labels (1–3) indicate different model-construction approaches shown within each pane. |
Gene Knockout and Gene Mutation Animal Models of Hyperuricemia
Currently, rodents are widely used as experimental animal models; however, due to the presence of UOXin rodents, which leads to the degradation of MSU, establishing a stable gout model remains challenging. To circumvent the impact of UOXon model stability, Lu Jie et al42 successfully developed a UOX-deficient mouse model by knocking out the mouse UOXgene, resulting in an animal model that spontaneously develops hyperuricemia. This model enables experimental animals to maintain a long-term hyperuricemic state, closely resembling the pathogenesis of gout in human patients. However, the absence of the UOXgene may cause pancreatic and renal dysfunction in the experimental animals, with a survival rate of approximately 40% at 62 weeks (Figure 2A).
In another study, researchers utilized the Cre/lox P recombinase system to develop a liver-specific conditional UOXknockout mouse model, achieving a survival rate of up to 90%. This novel model not only induced spontaneous hyperuricemia in the animals but also reduced the expression of the organic anion transporter (oat1), which is associated with urate reabsorption.36
Gene knockout animal models can not only establish a more stable hyperuricemia model but are also suitable for studying the pathogenesis of gout induced by hyperuricemia or the pathological damage caused by hyperuricemia.43,44 To investigate whether GLUT12 also mediates physiological urate transport, Yu et al45 constructed a GLUT12 knockout animal model, which similarly exhibited hyperuricemia. Additionally, to verify the relationship between apolipoprotein E (APOE) and hyperuricemia, an APOE knockout model was developed, demonstrating significantly higher uric acid levels compared to the control group.46
These gene knockout animal models focus on altering uric acid metabolism within experimental animals to establish spontaneous hyperuricemia models. Future research could combine gene knockout models with gouty inflammation models to develop more stable and representative models that better reflect the pathogenesis of gout.
Gene Knockout and Gene Mutation Animal Models of Hyperuricemia
Currently, rodents are widely used as experimental animal models; however, due to the presence of UOXin rodents, which leads to the degradation of MSU, establishing a stable gout model remains challenging. To circumvent the impact of UOXon model stability, Lu Jie et al42 successfully developed a UOX-deficient mouse model by knocking out the mouse UOXgene, resulting in an animal model that spontaneously develops hyperuricemia. This model enables experimental animals to maintain a long-term hyperuricemic state, closely resembling the pathogenesis of gout in human patients. However, the absence of the UOXgene may cause pancreatic and renal dysfunction in the experimental animals, with a survival rate of approximately 40% at 62 weeks (Figure 2B).
In another study, researchers utilized the Cre/lox P recombinase system to develop a liver-specific conditional UOXknockout mouse model, achieving a survival rate of up to 90%. This novel model not only induced spontaneous hyperuricemia in the animals but also reduced the expression of the organic anion transporter (oat1), which is associated with urate reabsorption.36
Gene knockout animal models can not only establish a more stable hyperuricemia model but are also suitable for studying the pathogenesis of gout induced by hyperuricemia or the pathological damage caused by hyperuricemia.43,44 To investigate whether GLUT12 also mediates physiological urate transport, Yu et al45 constructed a GLUT12 knockout animal model, which similarly exhibited hyperuricemia. Additionally, to verify the relationship between apolipoprotein E (APOE) and hyperuricemia, an APOE knockout model was developed, demonstrating significantly higher uric acid levels compared to the control group.46
These gene knockout animal models focus on altering uric acid metabolism within experimental animals to establish spontaneous hyperuricemia models. Future research could combine gene knockout models with gouty inflammation models to develop more stable and representative models that better reflect the pathogenesis of gout.
Composite Gout Animal Model
To more accurately simulate the pathogenesis of gout and develop a more stable gout animal model, researchers have combined a high-fat diet (10% yeast extract) with the injection of 1 milligram of MSU crystals into the footpad every 10 or 7 days.47,48 This composite gout model, compared to the hyperuricemia model induced solely by a high-fat diet and the acute gout model created by single MSU crystal injections, showed more severe ankle swelling in the experimental animals. Additionally, tissue sections revealed a higher infiltration of inflammatory cells (Figure 2C).
Wang et al49 combined intraperitoneal injection of potassium oxalate solution with a high-fat diet and intra-articular injection of acetic acid to promote the spontaneous formation and deposition of MSU. This model more accurately reflects joint damage caused by gout, simulating the various stages of gout development that clinical patients may experience through spontaneous MSU deposition. Compared to methods such as direct intra-articular injection of MSU, this model may be more suitable for biomaterials research.
To simulate the clinical manifestation of recurrent gouty arthritis, Xu et al50 created a 1.5mm diameter and 2mm depth cartilage defect in the femoral trochlear groove of SD rats. They then implanted 20 mg of MSU crystals into the defect. Every five days, an additional 20 mg of MSU crystals were injected into the operated joint, with each experimental animal receiving 3 to 5 injections to simulate the recurrent inflammation caused by intra-articular MSU crystal deposition. The repeated high-dose injections of MSU crystals did not cause severe extra-articular pathological damage to the experimental animals and achieved sustained MSU deposition in the animal model. The model exhibited significant neutrophil infiltration in the joints, and high expression levels of IL-1β and TNF-α were observed in the inflammatory cells. This model effectively simulated the characteristic recurrent inflammatory response caused by gout, as well as potential bone destruction and tophus formation due to MSU crystals.
Biodegradable Materials for Gout Treatment
Currently, conventional drugs used in the treatment of gout, such as allopurinol, NSAIDs, corticosteroids, colchicine, and targeted inhibitors of gout-related inflammatory pathways, often have varying degrees of side effects and liver and kidney toxicity due to their high doses.41 Moreover, these drugs are challenging to target specifically to the site of disease, leading to low bioavailability.5 To address the current challenges in gout treatment, researchers are increasingly investigating the therapeutic potential of biomaterials. For instance, a bionic meniscus embedded with Pt–CeO2 nanozymes and engineered with a gradient microporous architecture has been shown to effectively catalyze uric acid degradation while simultaneously scavenging reactive oxygen and nitrogen species,51 offering a promising strategy for personalized gout management. More broadly, biomaterials provide significant advantages in enhancing drug bioavailability and minimizing adverse effects owing to their excellent biocompatibility, controllable release profiles, and targeted delivery capabilities. By constructing effective drug delivery systems (DDS), the advantages of biomaterials can be fully utilized. Additionally, as biomaterials themselves may possess anti-inflammatory, antioxidant, and uric acid-lowering properties, they hold potential as novel gout therapeutic agents, providing more diverse treatment options for gout.
Novel Drug Delivery Systems
Nano-Composite Structured Drug Delivery Systems
The nanoparticle drug delivery system, while offering excellent biocompatibility, enables sustained drug delivery to specific sites, significantly enhancing drug utilization,52 thus addressing the adverse effects caused by the high doses or side effects of conventional drugs. Additionally, by employing drug carriers with synergistic effects alongside the encapsulated drugs, the therapeutic efficacy of the composite material can be enhanced through synergistic treatment.53,54 Moreover, by adjusting the type of biomaterial, it is possible to achieve responsive and sustained drug release from the delivery system. The nanodrug delivery systems reviewed in this section are summarized in Table 1 and their representative design mechanisms are schematically illustrated in Figure 3.
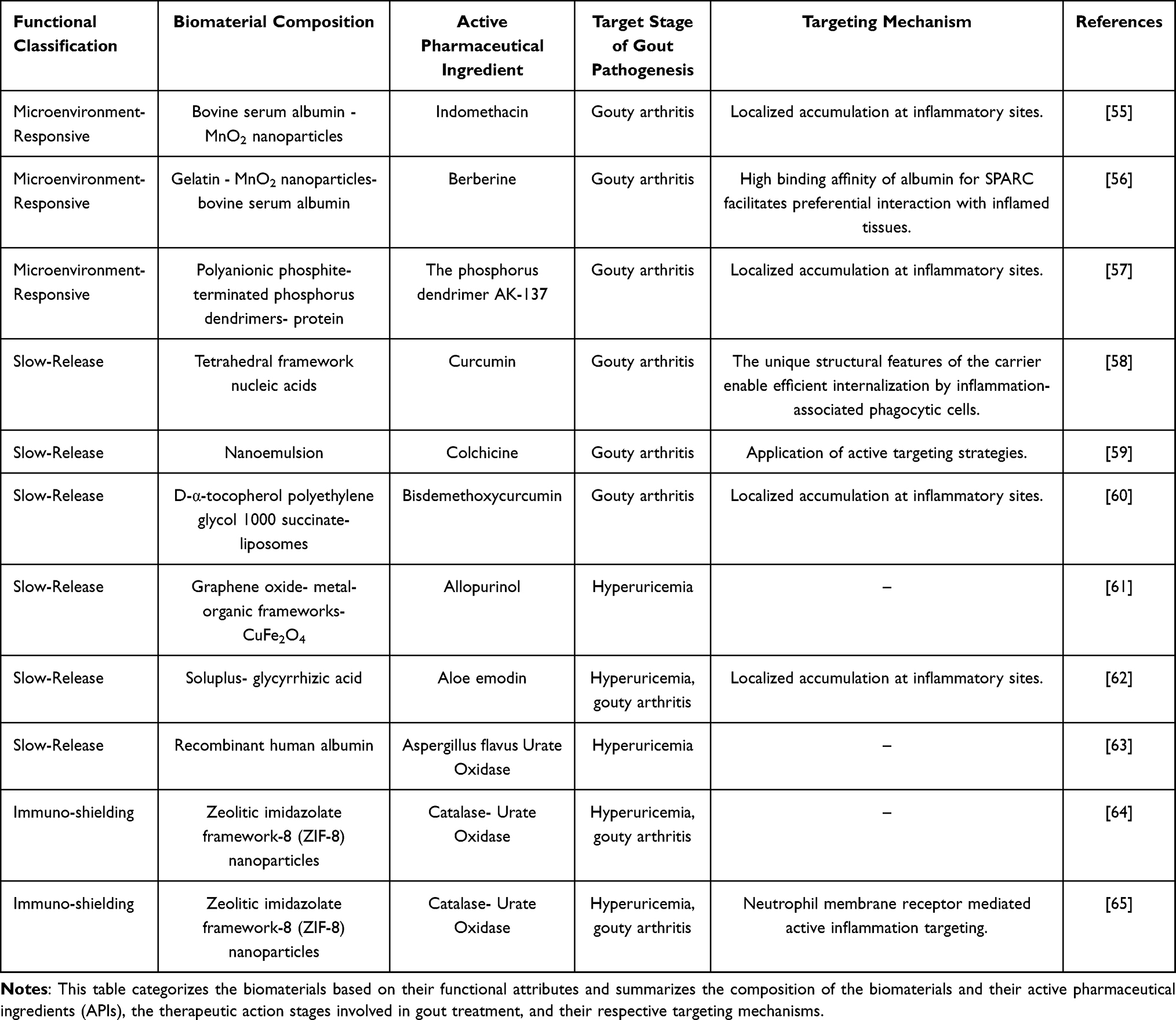 |
Table 1 Nanoparticle-Based Drug Delivery Systems for Gout Treatment |
 |
Figure 3 Construction methods and anti-gout mechanisms of nanoparticle drug delivery systems. (A) Schematic representation of BIM construction and its anti-gout mechanism, highlighting inhibition of ROS and gout-associated inflammatory factors. Reproduced with permission.59 Copyright 2023, AMER CHEMICAL SOC. (B) Diagram illustrating the construction of MAGN and its anti-gout mechanism. Reproduced with permission.65 Copyright 2023, ELSEVIER. (C) Schematic representation of Cur-TFNAs construction and characteristic images showing the reduction in inflammatory factor expression levels. Cur-TFNAs effectively decreased the expression levels of inflammatory cytokines (IL-1β and TNF-α).66 Reproduced with permission. Copyright 2022, KEAI PUBLISHING LTD. (D) Schematic illustration of UCZN preparation and its anti-gout mechanism, demonstrating urate-lowering effects along with the inhibition of inflammatory factor expression. Reproduced with permission.67 Copyright 2021, SCIENCE PRESS. (E) Mechanistic diagram of UCZR binding with red blood cells and specific SEM images showing red blood cells before and after binding.68 Reproduced with permission. Copyright 2024, WILEY. |
Microenvironment-Responsive Nanoparticle Drug Delivery System
Gout, as a metabolic inflammatory disease, is closely associated with disruptions in the local joint microenvironment, including decreased pH,55 reactive oxygen species (ROS) overload, and matrix metalloproteinase (MMP) activation. These unique pathological conditions provide opportunities for the development of microenvironment-responsive biomaterials.14,56 Studies have demonstrated that Manganese dioxide (MnO2) nanoparticles exhibit excellent catalytic capabilities,57 enabling the decomposition of ROS into water and oxygen,58 effectively alleviating oxidative stress. ROS, as one of the triggers in the inflammatory process of gout, plays a crucial role in promoting the rapid degradation of ROS to mitigate gout-related inflammation. Based on the properties of MnO2, its incorporation as a constituent of biomaterials enables effective suppression of gout flares through synergistic therapeutic effects. To achieve precise regulation of the inflammatory response in the third stage of gout pathogenesis using biomaterials while enabling microenvironment-responsive release of therapeutic agents, researchers have developed a stimuli-responsive drug delivery system (BIM) based on bovine serum albumin (BSA) and MnO259 (Figure 3A). This composite material inherits the excellent biocompatibility of BSA, while the presence of MnO2 nanoparticles prevents the burst release of the encapsulated drug, offering remarkable pH-responsive release properties. These properties depend on the degradation rate of MnO2 nanoparticles. The study found that at pH 6 in a weakly acidic environment, 50% of indomethacin was released over 12 hours, whereas at pH 7.4 (neutral environment), only 30% of indomethacin was released. An acute gouty arthritis animal model was constructed by injecting MSU crystals into the joints of mice, simulating the third stage of gout pathogenesis. The study demonstrated that MnO2 nanoparticles can effectively degrade ROS, improving the oxidative stress response caused by MSU crystal deposition in joints, while the release of indomethacin downregulated the expression of cyclooxygenase-2 (COX-2). This microenvironment-responsive drug delivery system effectively inhibited the expression of pro-inflammatory cytokines through synergistic effects, while also suppressing macrophage polarization to the M1 pro-inflammatory phenotype and inhibiting the migration of neutrophils and other inflammatory cells to the site of inflammation. This study establishes an innovative therapeutic strategy for targeted gout treatment through a synergistic triple-action mechanism encompassing ROS scavenging, anti-inflammatory effects, and immunomodulation.60,61 While BIM shows effective ROS scavenging and anti-inflammatory effects, its responsiveness is limited primarily to pH changes, and joint-specific targeting relies on passive accumulation rather than active sensing of inflammatory cues. Future improvements could integrate multiple microenvironmental signals (ROS, MMPs, and cytokine concentrations) to achieve more precise release control and enhanced therapeutic outcomes.
Recent studies have revealed that although berberine (an active compound in traditional Chinese medicine) exhibits notable anti-inflammatory and antioxidant properties,62 its poor aqueous solubility and rapid in vivo metabolism result in a bioavailability of less than 1%, severely limiting its application in gout management.63 Leveraging the capacity of biomaterials to enhance drug solubility, well-engineered drug delivery systems can optimize the anti-gout efficacy of berberine. However, achieving precise targeting of gout-associated inflammation and stimuli-responsive drug release remains a research challenge. Macrophages play pivotal roles in gout inflammation, where during their specific inflammatory response, they secrete matrix metalloproteinase-2 (MMP-2). Functioning as a gelatinase, MMP-2 disrupts synovial membrane integrity and accelerates inflammatory cell infiltration.64 Concurrently, it potently degrades gelatin, providing a strategic rationale for developing stimuli-responsive drug delivery systems. Based on the capacity of biomaterials to enhance drug solubility, researchers have developed drug delivery carriers to increase the bioavailability of berberine, thereby improving control of the third stage of gout pathogenesis. They successfully constructed a nanogel drug delivery system (MAGN) composed of MnO2 nanoparticles, gelatin, and BSA65 (Figure 3B). This biomaterial utilizes the affinity of BSA for secreted protein acidic and rich in cysteine (SPARC) to achieve targeted accumulation in the joint synovium. MAGN is capable of modulating its degradation rate in the joint synovium by sensing changes in the local MMP-2 concentration, allowing for the responsive release of the loaded berberine and MnO2 nanoparticles. Based on the release of its loaded compounds, this biomaterial also demonstrates anti-inflammatory and antioxidant stress capabilities. Similarly, by intra-articular injection of MSU crystals, an acute gouty arthritis animal model was established. MAGN effectively reduced ankle swelling in the animal model and significantly lowered the expression of ROS and inflammatory cytokines IL-6, IL-1β, and TNF-α within the joint. Compared with simpler MnO2-based systems, MAGN improves joint-specific accumulation and responsiveness to MMP-2, yet its sensitivity to dynamic microenvironmental changes remains limited, potentially reducing efficacy in heterogeneous inflammatory states. Future design strategies may focus on multi-stimuli responsive nanogels integrating pH, ROS, and cytokine sensing, along with optimized biodegradability and controlled release kinetics, to achieve more precise and personalized gout therapy. Microenvironment-responsive biomaterials, including MnO2-based carriers and MMP-sensitive nanogels, offer promising strategies for gout treatment through combined ROS scavenging, anti-inflammatory, and immunomodulatory mechanisms. However, current systems face limitations in sensitivity, targeting specificity, and dynamic response control. Continued mechanistic studies of gout pathogenesis and joint microenvironment heterogeneity are expected to inform the next generation of biomaterials with improved translational potential.
Slow-Release Nanoparticle Drug Delivery Systems
Based on the excellent tunable properties of biomaterials, slow-release DDS can be constructed by adjusting the composition and binding methods of biomaterials. The slow-release function not only allows for the sustained release of encapsulated drugs, achieving long-lasting therapeutic effects, but also avoids the side effects caused by the explosive release of drugs. Such DDS can significantly improve the bioavailability of the encapsulated drugs while reducing the occurrence of liver and kidney toxicity and other side effects. Biomaterials with controlled release capabilities should possess excellent biocompatibility and structural stability, such as tetrahedral framework nucleic acids (TFNAs), liposomes, and nanoemulsions, which have garnered extensive attention in recent years. TFNAs, constructed through the self-assembly of single-stranded DNA, exhibit outstanding biocompatibility and are readily absorbed by cells. Additionally, due to the structural stability of the tetrahedral nucleic acid framework, which can be maintained for nearly 48 hours within cells, studies have found that these can serve as carriers for small molecule drugs, increasing their bioavailability and reducing the potential cytotoxicity caused by burst drug release.69,70 To improve the solubility, stability, tissue absorption, and low bioavailability of the anti-inflammatory component curcumin, Zhang et al chose TFNAs as the delivery vehicle.66 This nanocarrier system (Cur-TFNAs) presents a discrete spherical profile with a size of approximately 20 nanometers, and its curcumin encapsulation efficiency reaches nearly 92.08 ± 0.89%, enabling controlled release of curcumin. Compared to non-carrier transport, the use of the tetrahedral nucleic acid framework reduced the degradation rate of curcumin in the body by 40%, and increased the drug uptake rate by RAW264.7 cells under both inflammatory and normal conditions by more than sixfold. Due to these factors, this biomaterial effectively inhibited the activation of the NF-kB signaling pathway and reduced the expression of reactive oxygen species (ROS) and gout-related inflammatory cytokines (IL-6, IL-1β, and TNF-α) (Figure 3C). In an acute gouty arthritis animal model, constructed by injecting MSU crystals into mouse ankles, the curcumin-loaded drug delivery system exhibited lower ankle swelling, less inflammatory cell infiltration, and reduced production of inflammatory cytokines and reactive oxygen species compared to the colchicine treatment group. Cur-TFNAs provide an efficient delivery strategy for the anti-gout application of curcumin through enhanced solubility, sustained release, and targeted delivery mechanisms. Although Cur-TFNAs show significant improvements in drug bioavailability and anti-inflammatory efficacy, their responsiveness is primarily passive, relying on cellular uptake and slow release rather than dynamically sensing inflammatory microenvironment cues. Future designs could integrate stimuli-responsive elements, such as ROS or pH-sensitive linkers, to achieve on-demand drug release in response to active gout flares, improving therapeutic precision.
Nanoemulsions, a new type of drug delivery system, have received widespread attention in recent years due to their ability to prevent particle aggregation, ensuring uniform drug distribution. Their structural stability also enables the enhancement of poorly soluble drug dissolution, thus improving drug bioavailability,71 achieving equivalent therapeutic effects at lower doses. As a carrier for colchicine,72 nanoemulsions significantly increased colchicine bioavailability and efficacy at the same dose. Moreover, due to their slow degradation and lower drug dose, nanoemulsions can effectively alleviate the side effects and organ toxicity caused by high doses of colchicine. Nanoemulsions improve drug stability and reduce toxicity; however, they offer limited targeting specificity and lack the ability to actively respond to microenvironmental changes in inflamed joints.
Liposomes are among the most commonly used nanoparticle DDS. By adjusting their physicochemical properties and surface functionalities, liposomes can enhance vascular permeability and target inflammatory cells.73 One study utilized liposomes as a carrier for the anti-inflammatory agent bisdemethoxycurcumin (BDMC) and successfully prepared a specific liposomal drug delivery system via the thin-film hydration method.74 This biomaterial is modified with D-α-tocopherol polyethylene glycol 1000 succinate (TPGS), which serves as a scavenger of reactive oxygen species (ROS) and can be effective in the third stage of gout pathogenesis, inhibiting the activation of the second signal of gout inflammation. Additionally, TPGS enhances the stability of liposomes, resulting in a superior sustained-release effect and increasing the bioavailability of BDMC by tenfold. Despite high drug-loading and ROS-scavenging capabilities, this liposomal system has not yet been validated in gout animal models, limiting conclusions about in vivo efficacy. Future studies should evaluate functionalized liposomes in acute gout models to confirm therapeutic effects and optimize surface modifications for improved joint targeting.
Furthermore, appropriately altering the composition of biomaterials can achieve a larger specific surface area, thereby improving the drug-loading capacity of drug delivery systems. By combining graphene oxide (GO) and metal-organic frameworks, researchers have successfully developed a drug delivery system with a high specific surface area. This system achieved a 90% encapsulation rate for allopurinol and, due to its sustained-release capabilities, allowed for up to four days of continuous release of allopurinol,75 simultaneously avoiding potential hepatic and renal damage caused by the metabolism of the same dose of allopurinol in the body.76 In their hyperuricemia rat model induced by a high-fructose diet, this biomaterial demonstrated excellent uric acid-lowering effects, potentially offering a novel therapeutic option for the initial stage of gout pathogenesis. Although (GO)-metal-organic framework carriers achieve prolonged drug release and high encapsulation, their biocompatibility and long-term safety in vivo remain concerns for clinical translation. Future research should investigate biodegradable frameworks and integrate stimuli-responsive release mechanisms to improve both safety and therapeutic precision.
Aloe emodin (AE) possesses multiple pharmacological actions, including antimicrobial and anti-inflammatory effects, but its hydrophobic nature results in low bioavailability, preventing it from fully exerting its pharmacological benefits.77 To improve its bioavailability and to validate the potential anti-gout efficacy of AE as an anti-inflammatory agent, Shi, Feng, and others successfully prepared mixed micelles composed of Soluplus® (polyvinyl caprolactam-polyvinyl acetate-polyethylene glycol graft copolymer) and glycyrrhizic acid(GA) using the thin-film hydration method.78 The AE encapsulation efficiency in this biomaterial reached 90.3 ± 1.08%, a high rate due to GA’s excellent solubilizing ability for AE. The controlled release capabilities of this biomaterial increased the bioavailability of AE by 3.09 times, enhancing the drug’s half-life and maximum plasma concentration. In their hyperuricemia and acute gouty arthritis animal model, induced by diet and MSU injection, AE effectively reduced the blood uric acid levels by inhibiting the activity of xanthine oxidase (XOD) and suppressed the expression of inflammatory cytokines IL-1 and IL-6, alleviating joint swelling and the inflammatory response in gout-afflicted animals. While AE micelles improve solubility and anti-inflammatory effects, their responsiveness to fluctuating disease states or local joint microenvironment signals is limited, potentially reducing efficiency during acute flares.
Current research focuses on modulating sustained-release drug delivery systems through optimized carrier composition and structural design to enhance drug delivery performance. However, limitations in targeting precision and unpredictable drug release environments pose significant clinical translation challenges. The intermittent and episodic nature of gout flares further complicates therapeutic management, as most sustained-release systems lack dynamic modulation capabilities responsive to disease state transitions. Consequently, future studies must improve targeting specificity and intelligent responsiveness to advance the clinical application of sustained-release delivery systems in gout therapy. Overall, slow-release nanoparticle DDS provide enhanced bioavailability, reduced toxicity, and improved therapeutic effects. However, current systems largely rely on passive release and lack microenvironmental responsiveness. Integrating multi-stimuli responsive mechanisms, optimizing in vivo targeting, and validating long-term safety will be critical for translating these systems into precise, clinically effective gout therapies.
Immuno-Shielding Nanoparticle Drug Delivery Systems
UOXhas been widely employed for the treatment of hyperuricemia due to its exceptional urate-lowering efficacy. However, its inherent antigenicity and immunogenicity often result in minimal bioavailability of active UOX, thereby limiting its therapeutic potential.79,80 Developing drug delivery systems with immunogenicity-masking capabilities can prevent unnecessary UOXdegradation and enhance its bioavailability. Recent studies have successfully constructed composite nanoparticles by co-loading UOXand catalase (CAT) into zeolitic imidazolate framework-8 (ZIF-8) nanoparticles,67 followed by encapsulating the composite structure with purified neutrophil membranes (NM). Neutrophil membranes retain the surface antigens and functional properties of neutrophils, effectively shielding the encapsulated enzymes from immune attacks. Additionally, due to the inherited cell membrane functionality, the biomaterial can recognize inflammatory factors such as IL-1β, TNF-α, and IL-6, enabling targeted delivery to gout inflammation sites (Figure 3D). The neutrophil membrane’s specific functions also allow the material to neutralize inflammatory factors, alleviating gout-related inflammation. UOXand CAT encapsulated in ZIF-8 nanoparticles can efficiently degrade uric acid and eliminate hydrogen peroxide (H2O2) through biocatalysis, thereby suppressing inflammation during gout flares.This innovative biomaterial demonstrated its efficacy in reducing ankle swelling and inflammatory responses in animal models of acute gouty arthritis induced by intra-articular injection, while significantly lowering uric acid levels in hyperuricemia models established through intragastric administration. By targeting both the first and third stages of gout pathogenesis, this biomaterial exhibits dual therapeutic effects.
Similarly, Li et al co-loaded UOXand CAT into ZIF-8 nanoparticles but innovatively employed UCZ as nano-building blocks and tannic acid as interparticle ligands to assemble the nanoparticles onto the surface of red blood cells68 (Figure 3E). This approach not only conferred immunosuppressive capabilities to the nanoparticles but also preserved the inherent functions of red blood cells. Owing to the excellent circulatory performance and immune evasion properties of red blood cells, the nanoparticles exhibited prolonged retention in vivo, significantly enhancing the bioavailability and efficacy of the gout-specific enzymes they carried. Another study utilized red blood cells directly as carriers for UOXand employed an innovative injection technique to avoid unnecessary UOXdegradation.81 Compared with red blood cell-based immune-shielding systems, neutrophil membrane-coated nanoparticles may offer stronger inflammation-homing capacity and additional cytokine-neutralizing effects because they retain membrane proteins involved in inflammatory recognition. These features may make neutrophil membrane-based systems more advantageous in the acute inflammatory phase of gout. In contrast, red blood cell-based platforms exhibit superior circulation time and immune evasion capacity, which may be more suitable for sustained systemic urate-lowering therapy. However, their active targeting to inflamed joints appears relatively weaker than that of neutrophil membrane-coated systems. Therefore, different immune-shielding strategies may be appropriate for different therapeutic goals, with neutrophil membrane camouflage being more favorable for acute flare control and red blood cell-based systems being potentially better suited for long-acting metabolic regulation.
Drug delivery systems employing immune-shielding strategies have successfully overcome the clinical limitations of urate oxidase (UOX) through biomimetic camouflage. However, critical challenges remain, including how to enhance targeting specificity and minimize off-target effects—an unresolved imperative. In addition, issues such as membrane source standardization, large-scale manufacturing, storage stability, and batch-to-batch consistency may further limit clinical translation of these biomimetic delivery systems. The integration of immune-shielding strategies with microenvironment-responsive release or sustained-release functions may further improve therapeutic precision and broaden their applicability across different stages of gout pathogenesis. With continued technological innovation, immune-shielded delivery systems hold transformative potential for advancing gout therapeutics.
Transdermal Microneedle Drug Delivery Systems
Microneedles (MNs) are biomaterials with sufficient mechanical strength to effectively penetrate the stratum corneum of the skin, with lengths ranging from 200 to 1000 micrometers.82 They also possess certain degradable properties. Microneedle-based DDS, which meet these criteria, can release the loaded drugs in the epidermal or dermal layers of the skin, where they are absorbed through capillaries, enabling precise drug administration while avoiding the first-pass elimination effect associated with oral drugs. This approach enhances the bioavailability of the drug.83,84 Due to their micron-sized dimensions, microneedles do not cause significant pain or discomfort when inserted into the skin, and they also avoid the risk of accidental injury that may occur with conventional hypodermic needles, such as damage to skin nerve endings and blood vessels. This not only enhances the safety of injections but also significantly reduces patient pain and other discomforts, thereby improving patient compliance.85 Given the excellent characteristics of transdermal microneedles, recent studies have introduced various types of microneedles for the treatment of gout. These biomaterials are primarily divided into two stages: one targeting the hyperuricemia phase during the pathogenesis of gout and the other addressing the inflammation caused by urate crystal deposition. Table 2 summarizes recent advances in microneedle-based systems for gout therapy, detailing carrier materials, incorporated drug types, and categorization of primary mechanisms of action.
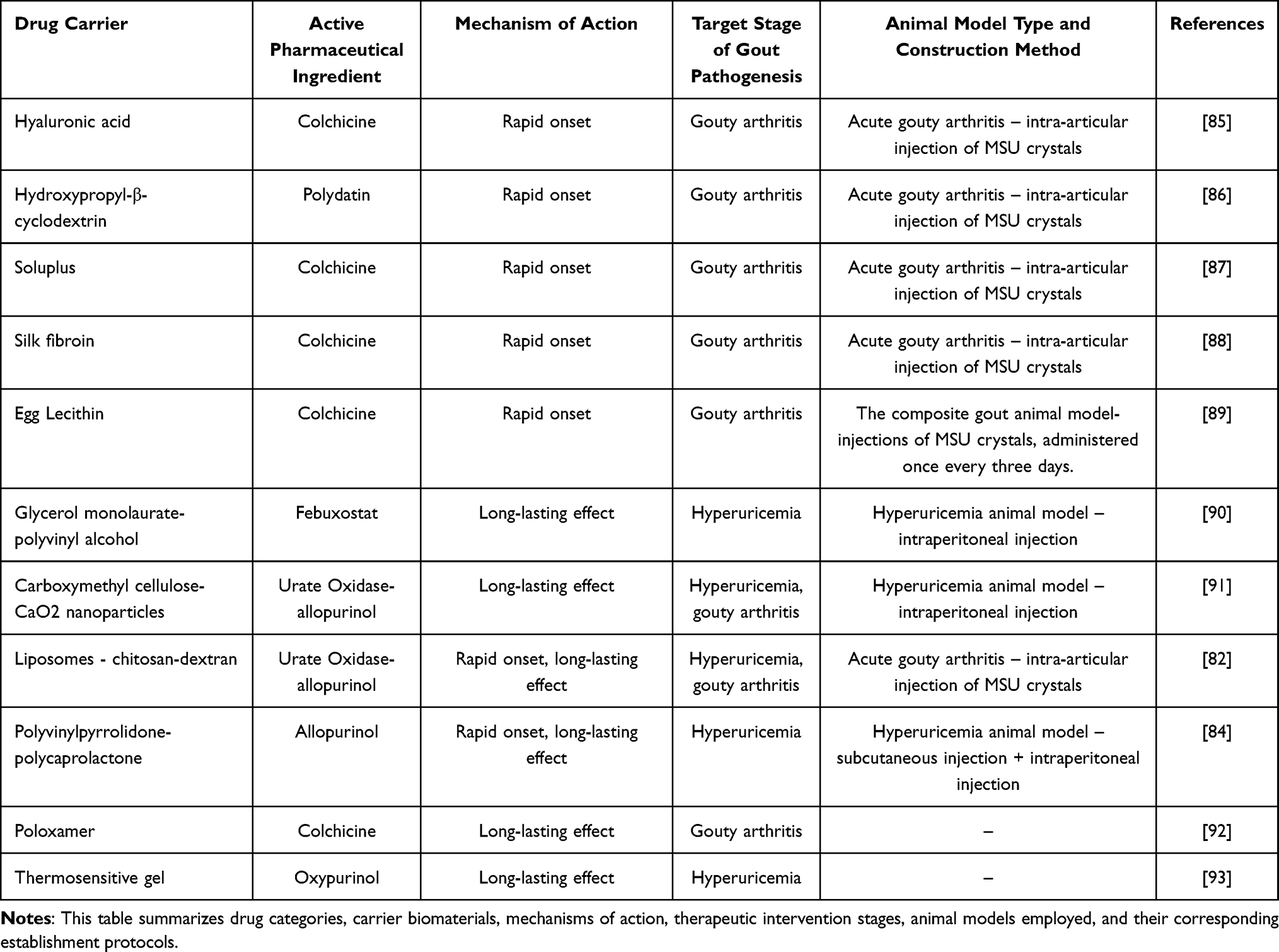 |
Table 2 Microneedles for Gout Treatment |
Rapid-Acting Anti-Inflammatory Microneedles
Targeting the third stage of gout pathogenesis, rapid onset is crucial for alleviating inflammatory responses. Prompt action can effectively relieve symptoms caused by acute inflammation and prevent irreversible intra-articular bone damage resulting from prolonged inflammation.86,87 To achieve rapid and precise anti-inflammatory effects, Liu et al developed water-soluble hyaluronic acid microneedles loaded with colchicine.88 These composite microneedles demonstrated excellent biocompatibility, solubility, and degradability. In their study, the hyaluronic acid microneedles efficiently penetrated the skin without causing significant damage. Compared to non-microneedle gels, the microneedles enhanced colchicine penetration by 3.36 times. In an acute gouty arthritis animal model induced by monosodium urate (MSU) injection, the microneedles provided rapid relief of acute ankle inflammation. While achieving the same therapeutic efficacy, the colchicine dosage in the gel group was 4.35 times higher than that in the microneedle group. Additionally, microneedle delivery achieved anti-inflammatory effects comparable to oral administration while avoiding gastrointestinal side effects associated with oral colchicine.
To further enhance rapid anti-inflammatory effects, another study developed fast-dissolving microneedles capable of complete dissolution within 5 minutes of skin insertion89 (Figure 4A). These microneedles enabled the rapid release of the anti-inflammatory agent polydatin. To improve its solubility, hydroxypropyl-β-cyclodextrin was employed as a carrier, increasing polydatin solubility by 10.59 times and its permeability by 8.6 times. Using an MSU-induced acute gout model, drug delivery via microneedles loaded with 1.6 mg of polydatin achieved therapeutic efficacy equivalent to oral colchicine (0.5 mg/kg), attributed to the rapid onset of action. To evaluate potential adverse effects, an acute gouty arthritis model was established by intra-articular MSU injection, and changes in animal body weight were monitored as a validation metric.90 Results indicated that the microneedles exhibited gout-therapeutic efficacy similar to colchicine without significant changes in animal body weight.
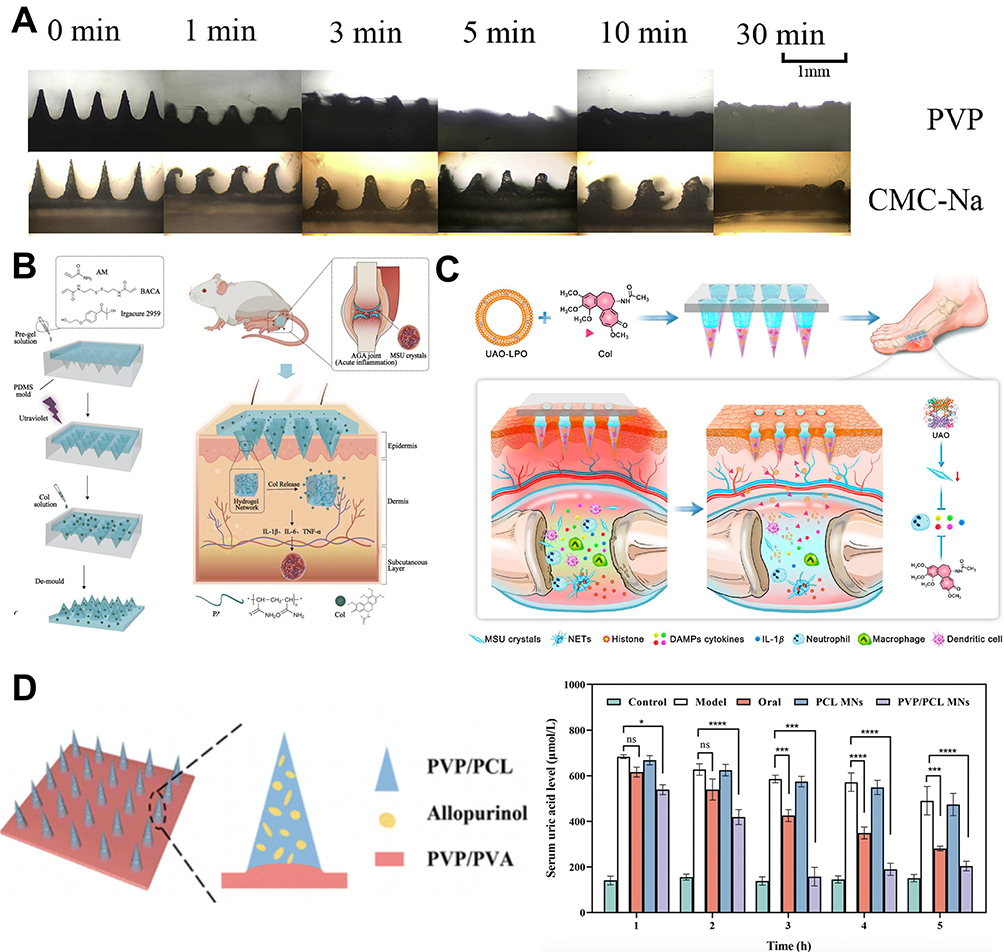 |
Figure 4 (A) Rapid dissolution performance of water-soluble microneedles.89 Copyright 2020, ELSEVIER. (B) Schematic of the construction and anti-inflammatory pathway of Col-HMNs.92 Reproduced with permission. Copyright 2023, ROYAL SOC CHEMISTRY. (C) Schematic illustration of the construction method of UAO-LPO/Col-MNs.94 Reproduced with permission. Copyright 2023, INST MATERIA MEDICA, Chinese ACAD MEDICAL SCIENCES. (D) Schematic of allopurinol-loaded composite microneedles and their uric acid-lowering efficacy.95 The “*” symbol indicates a statistically significant difference between groups (p< 0.05 (*), 0.01 (**), 0.001 (***) and 0.0001 (****). Reproduced with permission. Copyright 2023, ROYAL SOC CHEMISTRY. |
In another approach, colchicine was utilized as a delivery component to achieve rapid anti-inflammatory effects. By combining Soluplus with colchicine through freeze-drying technology, researchers fabricated water-soluble microneedle tips. Leveraging Soluplus’s excellent solubility, the microneedles dissolved completely within 3 hours, releasing approximately 74% of the colchicine within 24 hours.91 Jiang et al focused on increasing the drug-loading capacity of microneedles and providing appropriate carriers for rapid dissolution and action.92 Their study successfully synthesized hydrogel microneedles capable of swelling up to 2.7 times upon injection (Figure 4B). This remarkable swelling capacity resulted in over 95% colchicine encapsulation efficiency, with each microneedle delivering 1 mg of colchicine. These microneedles exhibited sustained drug-release capabilities. In an MSU-induced acute gout inflammation model, a single microneedle treatment achieved therapeutic efficacy comparable to oral colchicine (0.5 mg/kg), significantly suppressing inflammatory cytokines IL-1β, IL-6, and TNF-α. By utilizing microneedles, the required drug dosage for managing acute gout inflammation was significantly reduced, minimizing side effects and organ damage associated with high-dose treatments. Collectively, these rapid-acting anti-inflammatory microneedles demonstrate distinct but complementary advantages. Water-soluble hyaluronic acid microneedles exhibit excellent biocompatibility and efficient colchicine delivery, whereas fast-dissolving polydatin microneedles provide a more rapid dissolution profile and may reduce the adverse effects associated with colchicine exposure. In contrast, swelling hydrogel microneedles offer markedly improved drug-loading capacity and partial sustained-release behavior; however, their relatively slower dissolution may somewhat compromise the immediate-response advantage required during acute gout flares. Therefore, although all three systems exhibit significant anti-inflammatory efficacy, rapidly dissolving formulations appear more suitable for acute symptom relief, whereas swelling or partially sustained-release platforms may be advantageous when prolonged local drug retention is desired.
The rapid-acting anti-inflammatory microneedles are designed to rapidly dissolve at the site of inflammation,93 enabling precise and timely modulation of gout flare-ups. Recent studies have achieved significant breakthroughs in this area. Nevertheless, most currently reported systems still rely primarily on passive dissolution mechanisms rather than active responsiveness to inflammatory cues such as pH, reactive ROS, or cytokine levels. Future research is therefore expected to integrate ultra-rapid dissolution with microenvironment-responsive release mechanisms, enabling on-demand and precision regulation of acute gout inflammation while better matching drug release kinetics to fluctuating inflammatory intensity.
Long-Acting Uric Acid-Lowering Microneedles
Given the staged characteristics of gout pathogenesis, achieving long-term urate-lowering effects during the first stage, hyperuricemia, is crucial for mitigating disease progression. As hyperuricemia patients often lack noticeable clinical symptoms, their treatment adherence is typically poor. Developing a rational, long-acting composite microneedle system could address this issue and better prevent the advancement of gout. Patel et al developed non-allopurinol cubic drug vesicles by combining glycerol monolaurate (GMO) with polyvinyl alcohol (PVA) as components.96 Using the Quality by Design (QbD) approach, they prepared cubic vesicles with a size of approximately 157 nm and excellent drug loading capabilities, with the drug content constituting about 97.28%. By mixing these cubic vesicles with PVA and lactose, they successfully formulated long-acting uric acid-lowering microneedles.
Similarly, to achieve sustained urate-lowering effects, another study designed a layered microneedle drug delivery system.97 The outer layer consisted of carboxymethyl cellulose (CMC) loaded with allopurinol (AP), while the inner layer comprised a composite of uricase (UOX), calcium peroxide (CaO2) nanoparticles, and polyvinylpyrrolidone (PVP K30). The microneedles, approximately 800 µm in height, leveraged the excellent solubility of CMC to dissolve immediately upon insertion into the skin, releasing the outer-layer allopurinol for rapid urate-lowering effects. Subsequently, the decomposition of UOXand CaO2 nanoparticles enabled long-term urate degradation. Interestingly, UOXactivity was regulated by oxygen levels; CaO2 nanoparticles hydrolyzed in skin tissues to release oxygen, enhancing UOXactivity. Additionally, CaO2 acted as an oxidizing agent to directly oxidize uric acid, further facilitating its rapid degradation. The layered microneedles demonstrated encapsulation efficiency and loading capacity of 62.41% and 39.4%, respectively. In a hyperuricemia animal model established via intraperitoneal injection of hypoxanthine, the layered microneedles successfully penetrated the skin and reduced serum uric acid levels to 142 μmol/L within 3 hours. The effect was sustained for up to 12 hours and, compared to oral administration, caused no significant liver or kidney tissue damage. Compared with cubic vesicle-based microneedles, layered microneedles provide a more sophisticated therapeutic design by integrating immediate allopurinol release with prolonged enzymatic urate degradation. Such a dual-stage strategy may be more suitable for patients requiring both rapid and sustained urate control. However, the increased structural complexity and incorporation of multiple active components may also create challenges in formulation stability, manufacturing reproducibility, and quality control. In contrast, cubic vesicle-based microneedles appear simpler in formulation and may therefore offer advantages in scalability, although their functional versatility and biological responsiveness remain relatively limited. Future long-acting urate-lowering microneedles should not only prolong therapeutic duration, but also improve release predictability, enzymatic stability, and formulation simplicity. Incorporating disease-responsive elements may further enable these systems to better adapt to metabolic fluctuations and individual variability during gout progression.
Composite Functional Microneedles
Multifunctional microneedles capable of achieving multiple therapeutic effects have become a research focus in recent years. For instance, Yang et al developed a multilayered microneedle system to achieve both anti-inflammatory and urate-lowering effect94 (UAO-LPO/Col-MNs) (Figure 4C). This microneedle consists of three layers: a needle tip layer, a separation layer, and a base layer. The needle tip layer is composed of uricase (UOX) encapsulated in liposomes (LPO), colchicine, chitosan, and low-molecular-weight dextran. The liposomes enhance the stability and enzymatic activity of UOXwhile improving the solubility of colchicine, enabling a 5µg increase in colchicine loading per microneedle. Chitosan prevents burst drug release, facilitating sustained drug delivery, while dextran provides the composite microneedle with sufficient mechanical strength to penetrate the skin. The separation layer, made of PVP K90, dissolves rapidly upon insertion, allowing the needle tip layer to remain in the skin for the sustained release of colchicine and UOX. The base layer serves as a support platform for the composite microneedles. In a gout animal model induced by monosodium urate (MSU) crystal injection, the microneedles demonstrated excellent local targeting and sustained drug release capabilities, effectively reducing the required drug dosage for gout treatment and lowering the associated costs. By delivering dual anti-gout drugs, the microneedles not only degrade uric acid but also effectively inhibit the activation of the NLRP3 inflammasome, suppressing the release of inflammatory cytokines IL-1β, TNF-α, and IL-8. Moreover, by inhibiting the RANK/RANKL pathway, the microneedles prevent osteoclast maturation, thereby mitigating joint bone destruction caused by gout.
To achieve both rapid onset and sustained urate-lowering effects, Wang et al successfully developed biodegradable microneedles using polyvinylpyrrolidone (PVP) and polycaprolactone (PCL) as base materials, capable of carrying 0.2 mg of allopurinol95 (Figure 4D).The rapid degradation of PVP enables the microneedles to release approximately 80% of the encapsulated allopurinol within 15 minutes. Additionally, PVP’s fast degradation accelerates the subsequent breakdown of PCL after insertion, allowing the remaining 20% of allopurinol to be released gradually. In hyperuricemia animal models established by subcutaneous and intraperitoneal injection, the microneedles achieved urate-lowering effects comparable to oral allopurinol at the same dose. Furthermore, the slow degradation of PCL ensured that the urate-lowering effects lasted for over 5 hours, while avoiding liver and kidney tissue damage associated with oral administration. This improved drug safety, dosing intervals, and bioavailability. These composite functional microneedles represent two distinct design philosophies. The multilayer UAO-LPO/Col-MNs system is more comprehensive, simultaneously targeting uric acid metabolism, inflammation, and bone destruction, and may therefore be more suitable for complex or advanced gout conditions. However, its structural and compositional complexity may increase manufacturing costs and translational barriers. By contrast, the PVP/PCL biodegradable microneedles adopt a comparatively simpler design and effectively combine rapid and sustained urate-lowering release, potentially facilitating formulation reproducibility and large-scale production. Nevertheless, their therapeutic scope remains relatively narrower because they mainly focus on urate reduction rather than simultaneously modulating inflammatory and osteolytic pathways. Future multifunctional microneedles may benefit from combining simplified structural designs with multi-target therapeutic functions, thereby balancing therapeutic breadth, manufacturability, and translational feasibility. In particular, integrating microenvironment-responsive release mechanisms with dual- or multi-drug delivery may further improve efficacy across different stages of gout pathogenesis.
Transdermal MNs drug delivery systems have emerged as a highly promising strategy for the treatment of chronic diseases such as gout, owing to their superior drug delivery efficiency and excellent patient compliance. Recent advances have led to the development of a diverse array of MNs platforms, which can be broadly classified into rapid-acting, sustained-release, and multifunctional types. These platforms enable precise therapeutic interventions at various stages of gout pathogenesis, including acute inflammatory flares, asymptomatic hyperuricemia, and inflammation-associated molecular targets. Among them, rapid-acting anti-inflammatory MNs demonstrate fast onset and effective symptom control during acute gout attacks, while significantly reducing drug dosage and associated adverse effects. Sustained-release MNs for urate-lowering therapy provide prolonged and stable control of serum uric acid levels, thereby potentially improving medication adherence in asymptomatic patients and delaying disease progression. Multifunctional MNs, which co-deliver anti-inflammatory and urate-lowering agents, further optimize therapeutic outcomes by addressing both acute symptoms and long-term disease management in a synergistic manner. Despite these promising advancements, several challenges remain in the clinical translation of MNs systems. First, further improvements in drug loading efficiency and controlled-release precision are necessary. Additionally, in advanced gout cases complicated by tophi-induced skin ulceration, the safety and efficacy of MNs penetration require further investigation. Moreover, MNs platforms applied in gout management still present several inherent limitations. For instance, insufficient penetration may occur in patients with severely thickened or damaged skin at inflamed joints, which may reduce drug delivery efficiency. In addition, current MNs systems depend primarily on passive dissolution mechanisms, which can limit their ability to adjust dosing in response to dynamic changes in inflammatory activity during recurrent gout flares. These limitations highlight the need for more adaptable and clinically validated microneedle platforms. Future research should focus on integrating intelligent, stimuli-responsive biomaterials with disease-targeting capabilities to enable dynamic control over microneedle dissolution, drug release kinetics, and responsiveness to the inflammatory microenvironment. Overall, different microneedle systems exhibit distinct therapeutic advantages. Rapid-dissolving anti-inflammatory microneedles are more suitable for acute gout flares, long-acting urate-lowering microneedles are better adapted for chronic metabolic regulation, and multifunctional microneedles provide broader intervention across multiple pathological pathways. However, trade-offs still exist between rapid drug release, sustained therapeutic efficacy, structural complexity, and translational feasibility.
In summary, transdermal microneedle systems offer a novel and versatile approach for gout treatment and hold significant potential for advancing personalized and precision medicine strategies in clinical practice. Future studies should therefore focus not only on improving therapeutic efficacy, but also on clarifying the optimal clinical application scenarios of different microneedle platforms, simplifying manufacturing processes, and strengthening long-term in vivo safety validation to facilitate clinical translation.
Other Types of Drug Delivery Systems
Approximately one-third of total uric acid excretion occurs via the gastrointestinal (GI) tract, primarily mediated by uric acid transporters located in intestinal epithelial cells. The uric acid concentration in the gut may influence the activity of these transporters, making long-term regulation of intestinal uric acid transporter function a potential new direction for controlling gout progression. To achieve targeted regulation of local intestinal uric acid transporter activity and enhance uric acid excretion through the GI tract, Tang et al developed a core-shell hydrogel microsphere (UPA)98 (Figure 5A). The microspheres consist of a core of uricase and dopamine, encapsulated in a calcium alginate shell, with an average size of 205.9 ± 8.2 µm. Due to the protective calcium alginate shell, the microspheres can remain stable for over 6 hours in acidic simulated gastric fluid but degrade rapidly within 1 hour under simulated intestinal fluid conditions, enabling targeted drug release in the intestine. The targeted intestinal degradation of the microspheres allowed rapid release of uricase and dopamine within 1–2 hours. Uricase effectively decomposed uric acid in the intestine, generating hydrogen peroxide (H2O2) during the process, which created a locally oxygen-rich environment. This environment facilitated the polymerization of dopamine into polydopamine. Moreover, the adhesion of uricase to polydopamine prolonged its functional activity, reducing treatment costs. Uricase-mediated uric acid breakdown also activated the expression of intestinal uric acid transporters ABCG2 and GLUT9 (Figure 5B), enhancing the transport of uric acid into the intestinal lumen and increasing intestinal uric acid excretion by 27.6%. Interestingly, the polymerization of dopamine consumed local reactive oxygen species (ROS), effectively suppressing acute inflammatory responses associated with gout. In hyperuricemia and acute gouty arthritis animal models, the application of these hydrogel microspheres increased intestinal uric acid excretion by 27.6%, reduced serum uric acid levels by 71%, and significantly alleviated inflammation and joint swelling caused by monosodium urate (MSU) crystals. Intestinal microbiota, another key contributor to intestinal uric acid excretion, may also play a role in gout pathogenesis. Notably, the use of hydrogel microspheres reduced the abundance of gut bacteria commonly found in gout patients without disrupting the overall homeostasis of normal gut microbiota. These findings further validated the hydrogel microspheres’ exceptional anti-gout efficacy through multiple synergistic pathways.
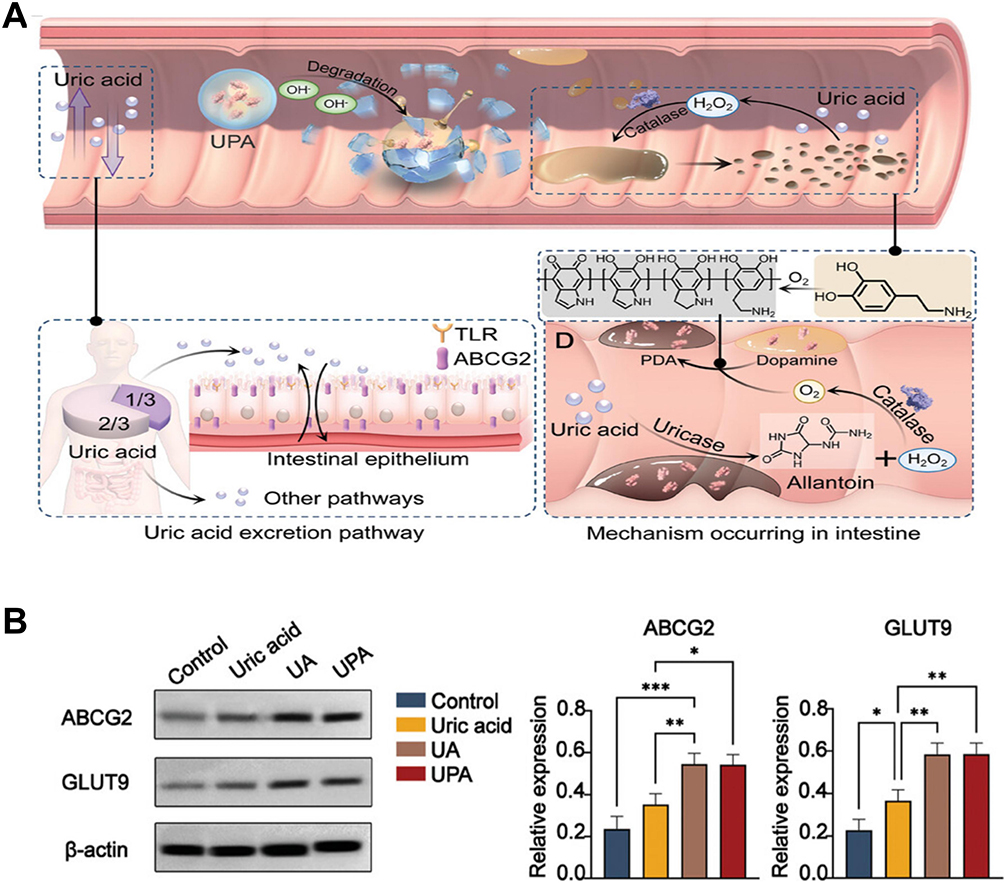 |
Figure 5 The schematic diagram of the mechanism of action of UPA and its effects. (A) UPA microspheres release their contents in the small intestine, enabling the in situ polymerization of dopamine within the intestinal mucosa. This facilitates the immobilization of UOXin the small intestine, thereby significantly enhancing the activity of uric acid transport proteins in intestinal epithelial cells. (B) The regulatory effects of UPA on intestinal uric acid transporters (GLUT9 and ABCG2) were demonstrated.98 The “*” symbol indicates a statistically significant difference between groups (p< 0.05 (*), 0.01 (**), 0.001 (***). Reproduced with permission. Copyright 2024, WILEY-V CHVERLAG GMBH. |
Fish collagen has many advantageous properties, such as non-toxicity, high absorbability, low cost, biodegradability, and excellent biocompatibility with human cells and tissues.99 Recent studies have combined fish scale collagen with carrageenan to create hydrogel microspheres capable of loading allopurinol.100 The combination of fish scale collagen and carrageenan retains the superior biocompatibility of fish scale collagen while inheriting the excellent hydrophilicity of carrageenan, enhancing the water solubility of the composite delivery system. The hydrogen bonds formed between the components endow the system with excellent pH-responsive properties, enabling controlled release of allopurinol in response to environmental changes, thus improving drug utilization. The drug loading capacity of these hydrogel microspheres for allopurinol is approximately 40%, and drug release in different simulated body fluids increased by 1.6 to 6.7 times. However, the study lacks an assessment of the therapeutic efficacy in vivo for hyperuricemia treatment. More importantly, these emerging delivery systems also reveal several common challenges. For intestinal-targeted microspheres, maintaining enzyme stability during gastrointestinal transit, ensuring reproducible intestinal release, and clarifying long-term effects on gut microbiota remain essential issues. For collagen-based or other biopolymer microspheres, the absence of in vivo efficacy data and insufficient validation of disease-targeting capability limit current conclusions regarding their therapeutic potential. Future studies should therefore place greater emphasis on improving targeting precision, evaluating long-term biosafety, and validating therapeutic performance in clinically relevant animal models.
In this section, we systematically summarize the distinct characteristics of various emerging drug-delivery platforms developed for gout therapy. Nanocomposite drug-delivery systems exhibit excellent biocompatibility and controllable release properties, enabling targeted administration while markedly improving drug utilization efficiency. Systems based on MnO2, ZIF-8, liposomes, or DNA frameworks can be applied during both chronic and acute phases of gouty arthritis to achieve anti-inflammatory and urate-lowering effects. Their major advantages include prolonged pharmacological activity and reduced adverse effects; nevertheless, limitations such as suboptimal targeting precision and restricted stimulus-responsive behavior remain. Microneedle-based delivery systems provide a minimally invasive, precise, and patient-compliant administration route and can be categorized into rapid-acting, long-acting, and multifunctional types. Rapid-acting microneedles are suitable for controlling inflammation during acute gout flares, long-acting microneedles help maintain serum urate levels, and multifunctional microneedles enable synergistic anti-inflammatory and urate-lowering therapy. Their primary constraints involve optimizing drug-loading capacity and penetration depth. Intestinal-targeted hydrogel microspheres regulate uric acid metabolism through interactions with the physiological gastrointestinal environment and are suitable for long-term management of hyperuricemia. Compared with nanocarrier-based and microneedle-based systems, these delivery platforms are still relatively limited in number and remain less mature in terms of mechanistic validation and translational evaluation. Nevertheless, they provide valuable alternative strategies by exploiting nontraditional therapeutic routes, particularly the gastrointestinal pathway, for urate regulation. Their major strengths lie in physiological compatibility and the potential for long-term metabolic intervention, whereas their current weaknesses mainly involve insufficient in vivo evidence, unclear targeting specificity, and limited standardization for clinical translation. Overall, nanocarrier-based systems are advantageous for chronic management, microneedle platforms are well suited for individualized and non-invasive therapy, and stimulus-responsive systems align more closely with the precise regulation required during acute inflammatory episodes, collectively providing diverse strategies for stage-specific, precision treatment of gout. Future research should further clarify the optimal clinical application scenarios of these emerging platforms and promote the integration of intestinal targeting, stimuli responsiveness, and improved biosafety evaluation. Such efforts may facilitate the development of more effective and clinically translatable delivery systems for stage-specific and precision treatment of gout.
Novel Biomaterial-Based Drugs for Gout Treatment
Carbon Dots
Carbon dots (CDs) are a class of novel biocompatible materials composed of carbon nanoparticles with diameters smaller than 10 nm. They offer several advantages, including excellent structural stability, low biological toxicity, cost-effective synthesis, and remarkable biocompatibility.101 In recent years, carbon dots have been investigated as active components for the treatment of gout, and studies have also explored their use in chemically modifying UOXto reduce its side effects.102 Additionally, carbon dots have been employed in the detection of uric acid levels.103,104 As a key enzyme in uric acid production, inhibiting xanthine oxidase (XOD) activity can help reduce uric acid levels in the body, thus achieving therapeutic effects in gout treatment.105 In a study by Wang et al, kudzu root (Pueraria lobatae Radix) was used as the precursor to prepare a new type of water-soluble bio-carbon dot (PLR-CDs) using pyrolysis and freeze-drying techniques.106 The size of the carbon dots was approximately 3–10 nm (Figure 6A). The carbon dots demonstrated excellent biocompatibility. In hyperuricemia and acute gouty arthritis animal models induced by intraperitoneal injection of high-purine compounds and intra-articular injection of monosodium urate (MSU) crystals, a comparison of the therapeutic efficacy of bio-carbon dots, allopurinol, and colchicine revealed that bio-carbon dots achieved urate-lowering effects similar to those of allopurinol and colchicine. This effect was achieved by inhibiting xanthine oxidase activity, and no significant side effects were observed. (Figure 6B).
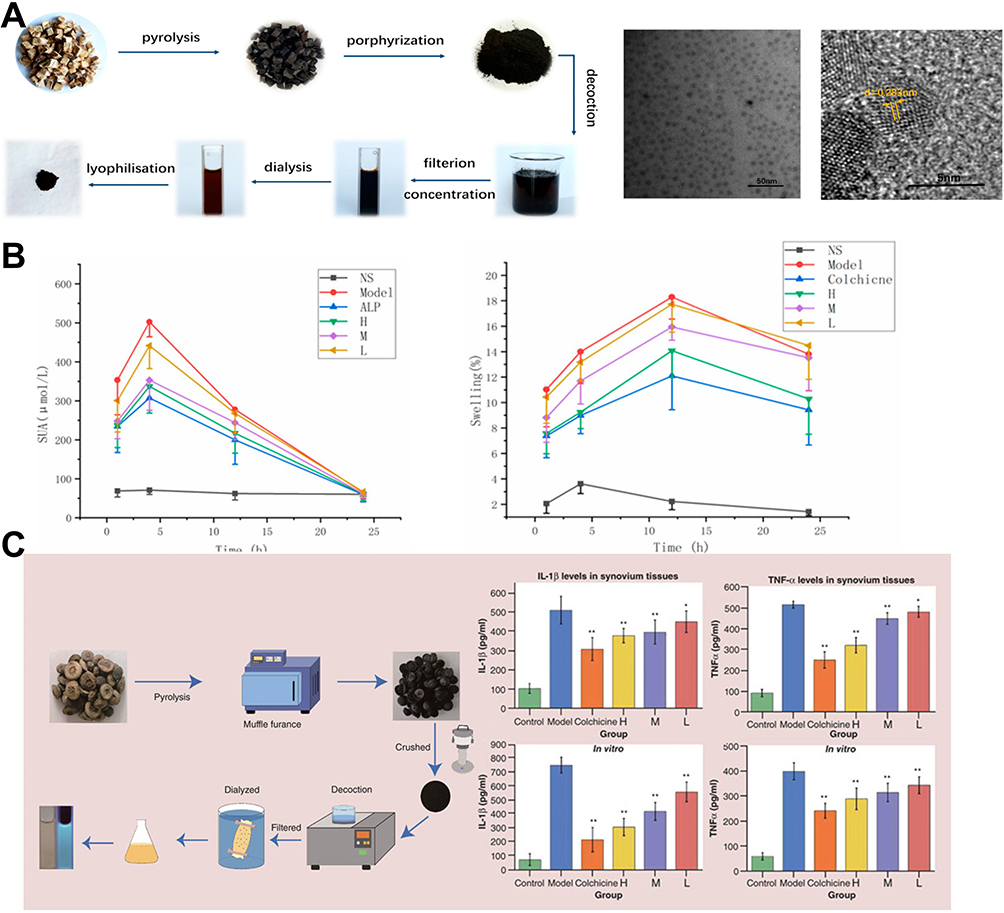 |
Figure 6 The preparation process and functional effects of different carbon dots. (A) Preparation process of PLR-CDs and their transmission electron microscopy (TEM) images. (B) Uric acid-lowering effect of PLR-CDs and their ability to reduce ankle swelling in gout animal models (H, M, L represent different doses of PLR-CDs).106 Reproduced with permission. Copyright 2019, MDPI. (C) Schematic of AFIC-CDs preparation process and their inhibitory effect on inflammatory cytokines. Reproduced with permission.107 The “*” symbol indicates a statistically significant difference between groups (p< 0.05 (*), 0.01 (**). Copyright 2019, FUTURE MEDICINE LTD. |
Another study utilized immature bitter orange (Aurantii Fructus Immaturus, AFI) as the active substance for gout treatment, which was processed by pyrolysis, concentration, and purification to produce carbon dots derived from AFI (AFIC-CDs).107 These carbon dots had a spherical structure with sizes ranging from 1.1 to 4.4 nm. They were easy to prepare, cost-effective, and exhibited the ability to reduce serum uric acid levels by inhibiting XOD activity in both serum and liver. Furthermore, AFIC-CDs alleviated gout-induced inflammation by suppressing the production of inflammatory cytokines, IL-1β and TNF-α (Figure 6C). Recent research suggests that different types of carbon dots may provide an effective approach to treating gouty arthritis. Carbon dots also possess the advantage of being easily surface-modified,104 which could allow for more precise therapeutic effects or reduce potential adverse reactions through targeted surface modifications in future studies. Although both PLR-CDs and AFIC-CDs demonstrated promising urate-lowering and anti-inflammatory effects, current studies mainly emphasize phenotypic efficacy rather than clearly defining the structure–activity relationship of the carbon dots themselves. In particular, because these materials are derived from complex natural precursors, the specific active surface groups responsible for XOD inhibition and inflammation suppression remain insufficiently characterized. Compared with conventional small-molecule drugs, carbon dots may offer better biocompatibility and surface tunability, but their pharmacodynamic consistency, metabolic fate, and long-term biosafety still require more rigorous evaluation.
Metal Nanomaterials
Research has demonstrated the formation of gold nanoclusters (AuNCs) with a size of approximately 2.88 nm through the combination of lysozyme and free gold ions. Subsequently, folic acid (FA) was used to form hydrogen bonds with AuNCs, resulting in the creation of folic acid-modified lysozyme-protected gold nanoclusters (FLA) with a diameter of 4.5 nm (Figure 7A).108 The gold nanoclusters exhibit a specific recognition function for urate salts, conferring a certain degree of targeting ability to the composite nanoclusters. To improve the biocompatibility and mitigate liver and kidney toxicity, folic acid, known for its excellent biocompatibility, was incorporated into the composite nanoclusters. This modification accelerated the renal metabolic efficiency of FLA without causing significant nephrotoxicity. Due to the remarkable anti-inflammatory and antioxidative stress properties of gold nanoclusters, they effectively inhibited the production of inflammatory cytokines such as IL-1β and TNF-α (Figure 7B) after being phagocytized by macrophages and eliminated excessive ROS (Figure 7C). In an animal model of acute gouty arthritis induced by direct MSU crystal injection, FLA significantly alleviated pain, inhibited inflammation, and reduced cartilage damage caused by MSU crystal deposition. The outstanding anti-inflammatory properties of FLA present a novel approach to treating gout.
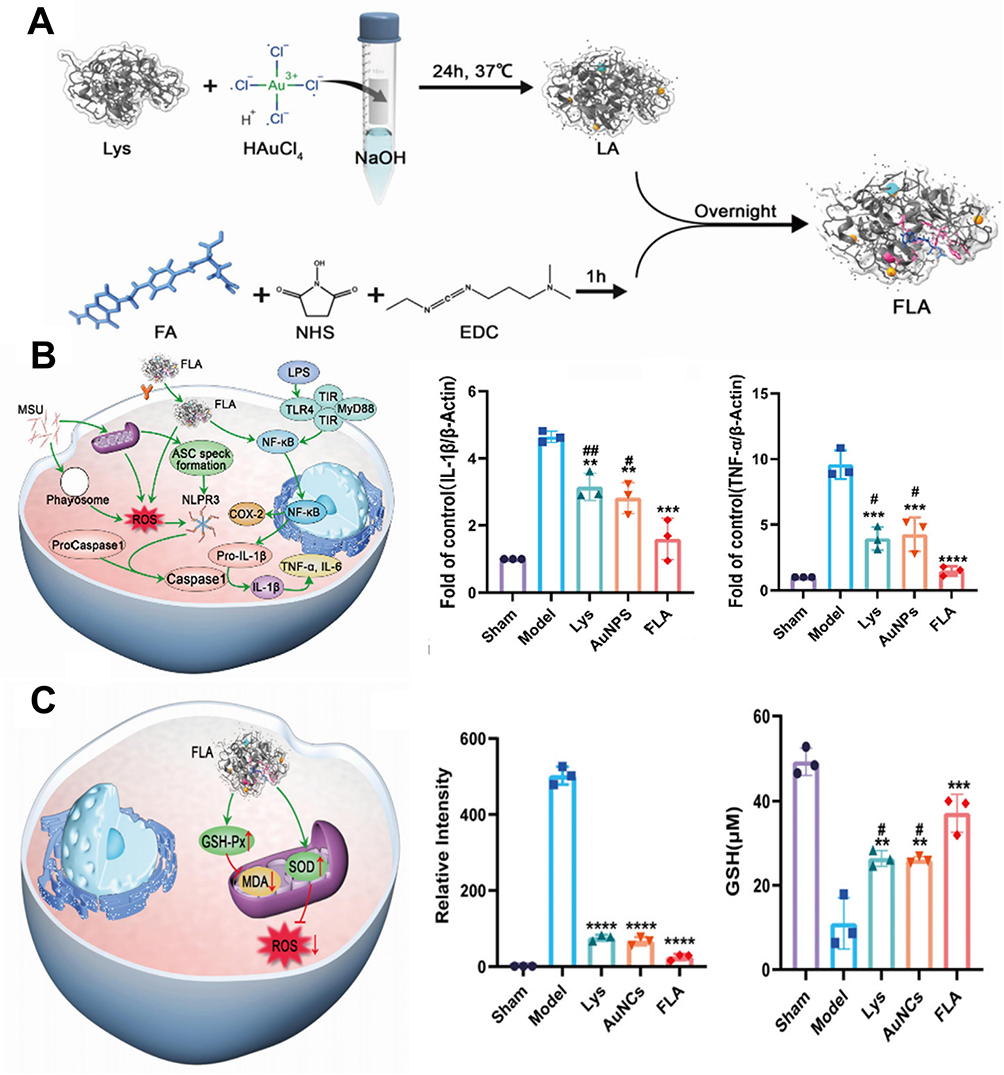 |
Figure 7 The schematic diagram of the preparation process and mechanism of action of FLA, as well as the anti-inflammatory experimental results of FLA. (A) Schematic of the FLA construction process. (B) Schematic of FLA’s anti-inflammatory pathway and its effect on inhibiting inflammatory cytokines. (C) Schematic of FLA’s antioxidative stress pathway and its therapeutic efficacy.108 The “*” indicates a significant difference compared with the model group, while “#” indicates a significant difference compared with the FLA group (*p < 0.05, **p < 0.01, ***p < 0.001, **p < 0.0001; #p < 0.05, ##p < 0.01). Reproduced with permission. Copyright 2022, ELSEVIER SCI LTD. |
Nanometal oxide particles, compared to their non-nano counterparts, exhibit superior biocompatibility and lower cellular toxicity. In recent years, these particles have been used in the treatment of various diseases. Some studies have shown that nanometal oxides, due to their unique anti-inflammatory and antioxidative properties, can treat gout flare-ups and effectively reduce serum uric acid levels and the inflammation caused by urate crystal deposition.109 Kiyani et al investigated the effects of different types of nanometal oxide particles on gout, discovering that copper oxide nanoparticles110,111 and zinc oxide nanoparticles112 can reduce oxidative stress responses in experimental animals, effectively decreasing the joint inflammation caused by urate crystals. Ingesting low concentrations of iron oxide nanoparticles113 did not cause significant liver or kidney toxicity but effectively reduced uric acid levels, achieving therapeutic outcomes. Their most recent research found that silver oxide nanoparticles114 exhibit similar effects to the aforementioned nanometal oxides. However, the efficacy of nanometal oxide particles has not been significantly superior to current allopurinol-based drugs, and the specific mechanisms of action regarding uric acid reduction and inflammation suppression remain unclear. With further research, nanometal oxide particles may become a rational therapeutic option for the treatment of gouty arthritis in the future. Compared with metal oxide nanoparticles, folic acid-modified gold nanoclusters exhibit a more clearly defined design rationale, including urate-related recognition, renal clearance optimization, and anti-inflammatory activity, and therefore appear to have stronger translational potential. By contrast, although various nanometal oxides have shown anti-inflammatory and urate-lowering effects, their mechanisms remain less well defined, and their therapeutic efficacy has not been clearly superior to existing urate-lowering drugs. Moreover, despite the nanostructured form improving biocompatibility relative to bulk metals, concerns regarding long-term accumulation, off-target effects, and biosafety cannot yet be neglected.
Gene-Encoded Antigout Drugs
In recent years, genetic engineering has emerged as a research hotspot and has been widely applied in the construction of biomaterials, drug screening, and the study of disease mechanisms.115–117 Interleukin-1 receptor antagonists (IL-1Ra) have demonstrated excellent efficacy in treating gout-related inflammation. However, their low bioavailability limits their clinical application. To extend the half-life of IL-1Ra and improve its effective utilization, Zhang et al engineered a chimeric protein consisting of the IL-1Ra sequence and a peptide with 72 lysine-rich residues.17 To prevent potential inactivation of the chimeric protein caused by covalent assembly, the chimeric protein’s positive charge was used to electrostatically adsorb the negatively charged PEG-COO-, resulting in the successful preparation of spherical nanoparticles with an average diameter of 180 nm. The incorporation of the IL-1Ra sequence into the nanoparticles enhanced the inhibition of the IL-1β signaling pathway, increasing its effect by eight times compared to the control group. Furthermore, the bioavailability of IL-1Ra was increased by sevenfold. Due to the sustained-release properties of the nanoparticles, the drug administration interval could be extended up to 72 hours, effectively reducing the cost of gout treatment. Notably, compared to free IL-1Ra, the half-life of IL-1Ra in the nanoparticles was increased by four times, possibly due to the random coil structure of the protein secondary conformation carried by the chimeric protein. In an acute gout model established by injecting MSU crystals into the rat ankle joint, the nanoparticles exhibited superior anti-inflammatory and anti-swelling effects compared to commonly used gout treatments, such as indomethacin. Gene-encoded anti-gout therapeutics provide a highly specific biological strategy, particularly for directly modulating inflammatory signaling pathways. In comparison with small-molecule or inorganic nanomaterial-based approaches, this strategy may offer stronger mechanistic precision and better biological potency. However, the currently reported IL-1Ra-based system mainly targets gout-associated inflammation rather than upstream urate metabolism, and therefore may be more suitable for acute inflammatory control than long-term metabolic management. In addition, issues such as immunogenicity, production complexity, storage stability, and protein degradation in vivo remain major barriers to broader application. Future studies should explore whether gene-encoded therapeutics can be extended beyond anti-inflammatory pathways to simultaneously regulate urate metabolism and inflammatory cascades. Combining genetically engineered proteins with biomaterial-based stabilization or targeting strategies may further improve their translational feasibility.
Enzyme-Driven Functional Nanotherapeutic Platforms
In recent years, intelligent nanomaterials powered by enzymatic catalysis have demonstrated strong microenvironment-modulating and self-enhancing capabilities in gout therapy,18 enabling uricase (UOx) to function beyond passive urate degradation and instead achieve more efficient and safer precision treatment through externally controlled or self-propelled mechanisms.
Zheng et al developed a magneto-responsive cyclic cascade nano-hybrid enzyme (NUOx) for precise gout therapy.118 By applying an alternating magnetic field, the Fe3O4 nanorings generate localized magnetothermal effects that enhance their catalase-like activity, thereby enabling on-demand activation of the covalently immobilized UOx and establishing a controllable UOx/CAT cascade system. This design effectively addresses the hypoxic milieu of the gouty joint cavity and mitigates the risks associated with continuous urate degradation. With a core–shell structure composed of Fe3O4 nanorings and surface-anchored UOx, NUOx exhibits high magnetic-thermal conversion efficiency, reversible enzymatic regulation, and favorable joint retention. In vitro, NUOx markedly improves urate degradation and monosodium urate (MSU) crystal dissolution under magnetic stimulation while maintaining dynamic urate homeostasis. In an acute gout model, NUOx combined with magnetic field stimulation significantly reduces intra-articular urate levels, alleviates inflammation and pain, repairs cartilage, and ameliorates local hypoxia, outperforming free UOx and demonstrating highly controllable and safe therapeutic potential. Liu et al designed a Urate Fuel-Driven Self-Propelling Nanomotor (AHMSNs@UOx@SC) that exploits endogenous urate at the lesion site to initiate autonomous motion.119 The nanomotor is constructed from asymmetric amine-functionalized hollow mesoporous silica nanoparticles (AHMSNs) with a single large opening, enabling ionic diffusiophoretic propulsion. UOx is covalently immobilized on the particle surface, followed by electrostatic loading of sodium citrate (SC), forming a “urate degradation–H2O2 scavenging” self-cascade system. UOx catalyzes urate decomposition to generate ionic gradients that propel the nanomotor, while SC simultaneously removes the cytotoxic H2O2 by-product and produces O2, which further enhances UOx catalysis through positive feedback. Moreover, SC elevates local pH, improves urate solubility, and suppresses MSU crystallization. This nanomotor demonstrates efficient urate degradation, H2O2 elimination, and enhanced intra-articular dispersion, resulting in substantial alleviation of inflammation, oxidative damage, and joint destruction in both acute and recurrent gout models. Compared with conventional UOx-based formulations, these enzyme-driven nanotherapeutic platforms represent a more advanced design paradigm because they not only degrade urate but also actively remodel the pathological microenvironment. The magneto-responsive NUOx system offers high controllability and may be particularly advantageous when external regulation is desired, whereas the urate-fuel-driven nanomotor exhibits stronger autonomy and lesion-adaptive behavior. However, these sophisticated functions are accompanied by increased structural complexity, which may complicate manufacturing, reproducibility, and regulatory evaluation. In addition, the clinical applicability of external magnetic stimulation or self-propelled nanomotion in human joints remains to be fully validated. Future development of enzyme-driven functional nanoplatforms should focus on simplifying material architecture while preserving microenvironment-responsive behavior. Greater attention should also be paid to large-scale preparation, long-term biosafety, and the feasibility of real clinical operation in deep or complex joint cavities.
Traditional Chinese Medicine and Extracts from Plants and Animals
Traditional Chinese medicine (TCM) has long been recorded as a treatment for gout. In recent years, an increasing number of active components from TCM have been identified as novel drugs for gout treatment.63,120 TCM can inhibit various inflammatory factors involved in the development of gout and effectively reduce serum uric acid levels. Research indicates that the primary mechanisms of TCM in treating gout include promoting uric acid excretion, enhancing immune function, and blocking peripheral nerve sensation.121 Curcumin and its analogs exhibit excellent anti-inflammatory bioactivity,122 as they can inhibit the formation of the NLRP3 inflammasome. This mechanism is of practical significance for gout therapy because NLRP3 inflammasome activation is a central event in monosodium urate (MSU)-induced inflammatory cascades. Therefore, curcumin-based interventions may be particularly valuable for controlling acute gouty inflammation and reducing the amplification of IL-1β-driven inflammatory responses. In recent years, increasing evidence has demonstrated their potential to effectively suppress the inflammatory response in gouty arthritis, thereby achieving therapeutic effects. Various other inhibitors targeting gout-related inflammatory pathways,123 plant extracts,124 animal extracts,125 and alkaloids90 have also been extensively studied in gout treatment. Compared to existing therapies, these agents show higher specificity, lower biotoxicity, and fewer side effects, offering promising alternatives for future gout treatment. These agents may offer promising alternatives or adjuncts to existing therapies because of their multitarget pharmacological activities and relatively favorable biosafety profiles. However, despite these encouraging findings, the current evidence for curcumin and many other natural extracts remains largely limited to anti-inflammatory activity demonstration and preliminary efficacy evaluation. Their practical therapeutic roles in gout have not yet been fully clarified, particularly with respect to whether they are most suitable for acute flare control, long-term urate regulation, or adjunctive therapy in combination with existing drugs. In addition, many natural products are characterized by complex compositions, variable source quality, and insufficient standardization, which complicate mechanistic interpretation and reproducibility across studies. For curcumin in particular, poor aqueous solubility, limited bioavailability, rapid metabolism, and insufficient tissue targeting remain major barriers to achieving consistent in vivo efficacy.
Among the five major categories of emerging anti-gout therapeutics, each exhibits distinct strengths and limitations. Carbon dots show favorable biocompatibility, tunable surface properties, and dual anti-hyperuricemic and anti-inflammatory activities, although their long-term in vivo safety and metabolic fate remain unclear. Metal nanomaterials display strong antioxidative, ROS-scavenging, and anti-inflammatory effects, but concerns regarding metal accumulation and biosafety may limit their translational potential. Gene-encoded anti-gout agents offer direct advantages in urate degradation and metabolic regulation; however, immunogenicity and poor in vivo stability remain major challenges. Traditional Chinese medicines and plant- or animal-derived extracts are widely accessible and generally associated with low toxicity, with the capacity to modulate both inflammation and urate metabolism through multiple pathways. Nevertheless, their complex composition and unstable pharmacological performance often require biomaterial-assisted delivery to improve solubility and bioavailability. In addition, enzyme-driven functional nanotherapeutic platforms provide emerging opportunities for microenvironment modulation and precise intervention in gout. Collectively, these biomaterial-based strategies may serve complementary roles in future integrated gout therapy. To facilitate cross-category comparison, Table 3 summarizes the major biomaterial categories discussed in this review, together with their representative platforms, therapeutic roles, advantages, limitations, and future directions.
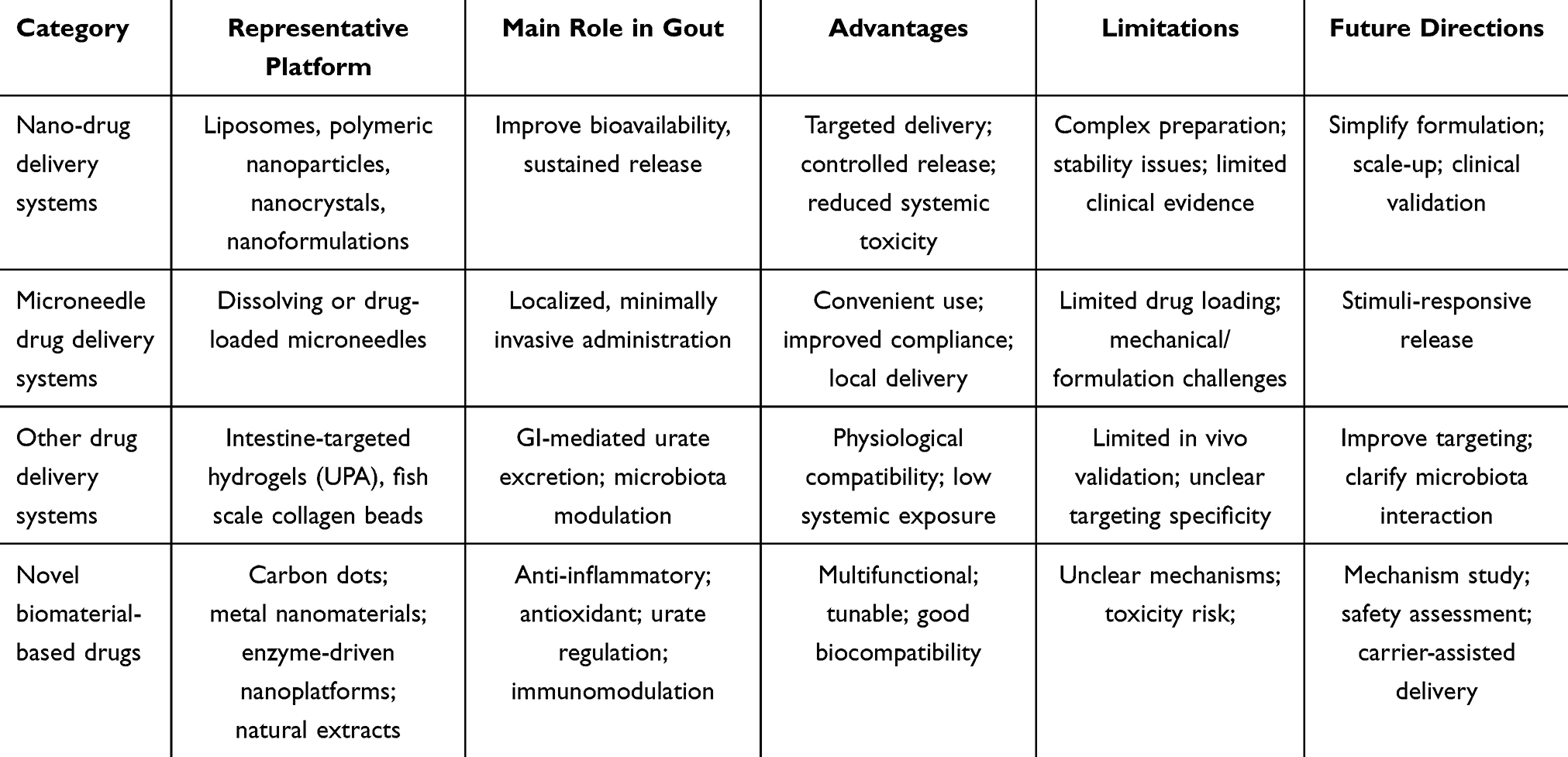 |
Table 3 Comparative Summary of Major Biomaterial Categories for Gout Therapy Based on the Classification Framework of This Review |
Potential Therapeutic Targets of Future Biomaterials
Uric Acid Transporters
Dysregulation of urate excretion is a common cause of gout, with uric acid transporters playing a crucial role in this process. Among the various urate transporters involved in urate excretion, three dominate: glucose transporter 9 (GLUT9), urate transporter 1 (URAT1), and ABCG2.126 GLUT9 and URAT1 are primarily located in the proximal tubules of the kidneys, mediating renal reabsorption of urate.127 ABCG2 mainly facilitates urate excretion in the intestines.128 Dysfunction of these transporters can lead to hyperuricemia and subsequent gout attacks, and potentially cause severe renal impairment due to abnormal urate accumulation in the kidneys.129 Research indicates that targeting uric acid transporters can yield satisfactory therapeutic outcomes for gout.130 Future biomaterial development may focus on these transporters as potential therapeutic targets, exploring new biomaterials specifically designed to inhibit uric acid transporters or developing targeted DDS carrying transporter inhibitors. This could provide more therapeutic options for gout treatment.
Non-Coding RNA
Long non-coding RNAs (lncRNAs) and microRNAs are two types of non-coding RNAs that play roles in regulating gene expression. Recent research indicates that microRNAs and lncRNAs may be involved in various stages of gout development. For instance, a decrease in microRNA-223 may exacerbate gout-related inflammation,131,132 highlighting the diverse roles of these small molecules in disease progression. Unlike the regulation of protein translation, non-coding RNAs such as microRNAs and lncRNAs can directly modulate the transcriptional levels of coding genes.133 MicroRNAs and lncRNAs primarily influence the inflammatory process through signal transduction pathways,134 such as microRNA-146a and microRNA-302b.135,136 Additionally, these non-coding RNAs can regulate inflammation caused by urate crystals,137 thus participating in the modulation of hyperuricemia and gouty inflammation. These non-coding RNAs hold promise as potential therapeutic targets for biomaterials aimed at treating gout.
Gut Microbiota
Gut microbiota refers to the collective microorganisms residing in the human gastrointestinal tract, playing key roles in host metabolism, immune regulation, and digestion. Under normal conditions, they form a relatively stable ecosystem with the host. Recently, gut microbiota has become a novel research hotspot for exploring disease mechanisms.138–141 Studies suggest that gut microbiota not only participate in the breakdown of urate in the intestines but also play roles in the inflammatory response associated with gout.142 Increasing evidence indicates a close relationship between gut microbiota and gout pathogenesis. The gut microbiota can influence urate metabolism by modulating the function of intestinal urate transporters,143 For example, A.indistinctus can alleviate hyperuricemia by enhancing the excretion of uric acid through the upregulation of the intestinal urate transporter ABCG2.144
Disruption of gut microbiota balance can lead to urate metabolism disorders, resulting in urate accumulation and subsequent gout attacks.145 Research shows significant differences in gut microbiota composition between gout patients and healthy individuals,146 with a notable decrease in the abundance of the genus Coprococcus in gout patients.147 This suggests that improving the gut microenvironment and microbiota composition in gout patients could be a potential therapeutic strategy. Current studies have found that probiotics, prebiotics, and active components of traditional Chinese medicine can modulate gut microbiota,148 effectively reversing hyperuricemia and alleviating gout-induced inflammation.149 Additionally, gut microbiota transplantation has been explored to alter the host’s gut microbiota structure and function, achieving therapeutic effects.150 Future biomaterial research could target gut microbiota as a therapeutic approach for gout, contributing to a better understanding of gout pathogenesis and more effective treatment strategies.
Conclusions and Future Directions
The onset and progression of gout involve multiple interconnected pathological processes, including dysregulated urate metabolism, monosodium MSU crystal deposition, activation of inflammatory responses, and amplification of oxidative stress. Although current clinical management, which primarily relies on urate-lowering and anti-inflammatory therapies, can control the disease to some extent, it remains difficult to simultaneously meet multiple therapeutic demands, such as rapid onset of action, sustained urate lowering, and prevention of recurrence. In this context, biomaterials have emerged as an important research direction in gout therapy because of their potential for precise drug delivery, sustained-release enhancement, and synergistic intervention across multiple pathological pathways. As illustrated in Figure 8, current biomaterial-based strategies for gout therapy can be broadly classified into four categories: nanoparticle-based drug delivery systems, microneedle-based drug delivery systems, other drug delivery systems, and novel biomaterial-based therapeutics.
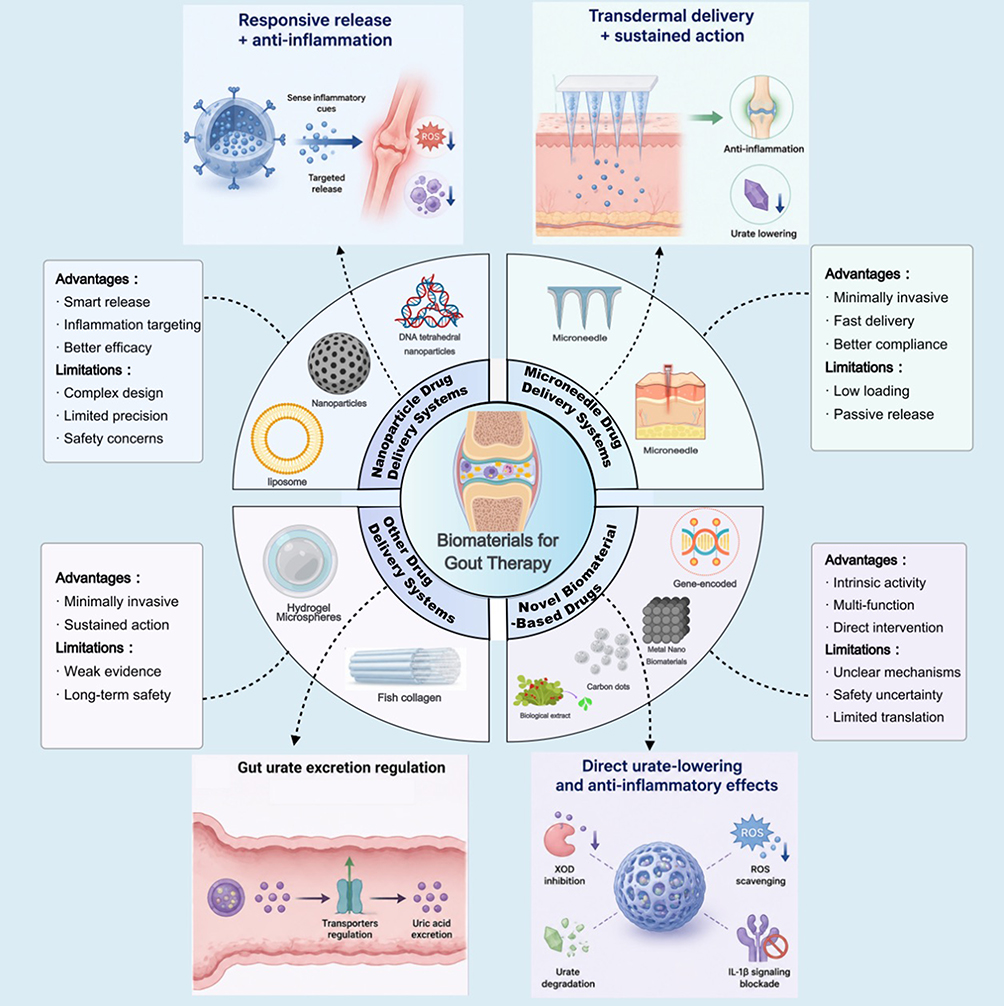 |
Figure 8 Conceptual summary of major biomaterial-based strategies for gout therapy. Different categories of biomaterials applied in gout treatment are classified and compared, with emphasis on their mechanisms of action, key advantages, and current limitations. |
Specifically, nanoparticle-based drug delivery systems offer the advantage of responsive drug release in the inflammatory microenvironment, thereby enhancing local anti-inflammatory efficacy while reducing adverse effects. However, their limitations include structural complexity and the lack of sufficient evidence regarding long-term safety. Microneedle-based drug delivery systems are characterized by minimal invasiveness, rapid onset of action, and relatively good patient compliance, making them attractive for long-term gout management. Nevertheless, their drug-loading capacity is limited, and drug release often depends largely on passive diffusion; therefore, their actual clinical benefit still requires further validation. Other drug delivery systems, particularly gut-related delivery strategies, provide new opportunities for regulating urate excretion and improving the metabolic microenvironment. To some extent, these approaches may address a key limitation of conventional therapies, namely the difficulty of tailoring treatment according to the underlying mechanisms of hyperuricemia. However, the overall evidence supporting these systems remains relatively weak, and their long-term stability and safety have not yet been adequately evaluated. In contrast, novel biomaterial-based therapeutics may function not only as carriers but also as active therapeutic agents. Through their intrinsic properties, they may directly participate in disease intervention by inhibiting xanthine oxidase, scavenging ROS, promoting urate degradation, or blocking inflammatory signaling pathways, thereby demonstrating the potential for multifunctional synergy. Even so, research in this area still lacks clear mechanistic elucidation and a solid foundation for clinical translation.
Although biomaterial-based strategies for gout therapy have shown promising potential in recent years, these approaches remain largely at the preclinical stage, and a substantial gap still exists between experimental studies and actual clinical application. Moreover, most current studies have been validated using acute inflammatory or hyperuricemia animal models. While such models can reflect certain aspects of gout pathology, they do not adequately recapitulate the chronic hyperuricemia state, recurrent attacks, and tissue dysfunction commonly observed in patients. Therefore, future research should focus more explicitly on two key priorities. The first is in vivo safety, particularly the distribution, metabolism, accumulation, immunogenicity, and risks associated with long-term administration of biomaterials. The second is therapeutic efficacy with mechanistic certainty. In other words, future studies should not only determine whether serum urate levels or inflammatory markers are improved, but also clarify whether these strategies truly target the key pathological events of gout, including excessive urate production or metabolic imbalance, MSU crystal-induced inflammation, and ROS-related tissue damage. Only after their safety and mechanisms of action have been thoroughly validated can these biomaterial-based strategies truly address the current unmet needs in gout therapy, such as precise inflammation control, sustained drug delivery, and recurrence prevention, and thereby achieve meaningful clinical translation.
Funding
This study was supported by funding from National Natural Science Foundation of China (823B2059), the Science and technology research project of Jilin Provincial Department of Education (JJKH20231219KJ), the Jilin Scientific and Technological Development Program (20240305034YY).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dalbeth N, Gosling AL, Gaffo A, Abhishek A. Gout. Lancet. 2021;397(10287):1843–32. doi:10.1016/S0140-6736(21)00569-9
2. Dalbeth N, Choi HK, Joosten LAB, et al. Gout. Nature Reviews Disease Primers. 2019;5(1):69. doi:10.1038/s41572-019-0115-y
3. Strilchuk L, Fogacci F, Cicero AF. Safety and tolerability of available urate-lowering drugs: a critical review. Expert Opin Drug Saf. 2019;18(4):261–271. doi:10.1080/14740338.2019.1594771
4. Saag KG, Becker MA, White WB, et al. Evaluation of the relationship between serum urate levels, clinical manifestations of gout, and death from cardiovascular causes in patients receiving febuxostat or allopurinol in an outcomes trial. Arthritis Rheumatol. 2022;74(9):1593–1601. doi:10.1002/art.42160
5. Tao H, Mo Y, Liu W, Wang H. A review on gout: looking back and looking ahead. Int Immunopharmacol. 2023;117:109977. doi:10.1016/j.intimp.2023.109977
6. Rashad AY, Daabees HG, Elagawany M, Shahin M, Moneim AEA, Rostom SAF. Towards the development of dual hypouricemic and anti-inflammatory candidates: design, synthesis, stability studies and biological evaluation of some mutual ester prodrugs of febuxostat-NSAIDs. Bioorg Chem. 2023;135. doi:10.1016/j.bioorg.2023.106502
7. Pillinger MH, Mandell BF. Therapeutic approaches in the treatment of gout. Semin Arthritis Rheumatism. 2020;50(3, Supplement):S24–S30. doi:10.1016/j.semarthrit.2020.04.010
8. Mikuls TR, Cheetham TC, Levy GD, et al. Adherence and outcomes with urate-lowering therapy: a site-randomized trial. Am J Med. 2019;132(3):354–361. doi:10.1016/j.amjmed.2018.11.011
9. Cho WH, Kim H, Yoo S-Y, Lee SM, Kim T, Lee J-Y. Advancements in uricase formulations: overcoming therapeutic challenges in enzyme replacement therapy. J Pharm Invest. 2025;55(4):521–556. doi:10.1007/s40005-025-00733-x
10. Bao Z, Li Q, Zhou Z, Yang J, Zhang L. Mitigating uricase immunogenicity through Zwitterionic peptide fusion for enhanced gout therapy. Langmuir. 2025;41(20):12664–12674. doi:10.1021/acs.langmuir.5c00829
11. Darnell M, Mooney DJ. Leveraging advances in biology to design biomaterials. Nature Mater. 2017;16(12):1178–1185. doi:10.1038/nmat4991
12. Luan J, Li R, Xu W, et al. Functional biomaterials for comprehensive periodontitis therapy. Acta Pharmaceutica Sinica B. 2023;13(6):2310–2333. doi:10.1016/j.apsb.2022.10.026
13. Huang H, Feng W, Chen Y. Two-dimensional biomaterials: material science, biological effect and biomedical engineering applications. Chem Soc Rev. 2021;50(20):11381–11485. doi:10.1039/d0cs01138j
14. Li J, Zhang H, Han Y, Hu Y, Geng Z, Su J. Targeted and responsive biomaterials in osteoarthritis. Theranostics. 2023;13(3):931–954. doi:10.7150/thno.78639
15. Tu Z, Zhong Y, Hu H, et al. Design of therapeutic biomaterials to control inflammation. Nat Rev Mater. 2022;7(7):557–574. doi:10.1038/s41578-022-00426-z
16. Rodrigo-Navarro A, Sankaran S, Dalby MJ, Del Campo A, Salmeron-Sanchez M. Engineered living biomaterials. Nat Rev Mater. 2021;6(12):1175–1190. doi:10.1038/s41578-021-00350-8
17. Zhang J, Sun Y, Qu Q, et al. Engineering non-covalently assembled protein nanoparticles for long-acting gouty arthritis therapy. J Mat Chem B. 2021;9(48):9923–9931. doi:10.1039/d1tb01760h
18. Lin A, Sun Z, Xu X, et al. Self-cascade uricase/catalase mimics alleviate acute gout. Nano Lett. 2022;22(1):508–516. doi:10.1021/acs.nanolett.1c04454
19. Chen R, Yang J, Wu M, et al. M2 macrophage hybrid membrane-camouflaged targeted biomimetic nanosomes to reprogram inflammatory microenvironment for enhanced enzyme-thermo-immunotherapy. Adv Mater. 2023;35(39):2304123. doi:10.1002/adma.202304123
20. Peng Z, Meng F, Deng Q, et al. Advances in drug delivery systems for the management of gout and hyperuricemia. Front Pharmacol. 2025;16.
21. Dalbeth N, Merriman TR, Stamp LK. Gout. Lancet. 2016;388(10055):2039–2052. doi:10.1016/S0140-6736(16)00346-9
22. Hansildaar R, Vedder D, Baniaamam M, Tausche A-K, Gerritsen M, Nurmohamed MT. Cardiovascular risk in inflammatory arthritis: rheumatoid arthritis and gout. Lancet Rheumatol. 2021;3(1):e58–e70. doi:10.1016/S2665-9913(20)30221-6
23. Richette P, Doherty M, Pascual E, et al. 2018 updated European League Against Rheumatism evidence-based recommendations for the diagnosis of gout. Ann Rheumatic Dis. 2020;79(1):31–38. doi:10.1136/annrheumdis-2019-215315
24. Chhana A, Lee G, Dalbeth N. Factors influencing the crystallization of monosodium urate: a systematic literature review. BMC Musculoskelet Disorders. 2015;16(1):296. doi:10.1186/s12891-015-0762-4
25. Ahn H, Lee G, Lee G-S. Lower temperatures exacerbate NLRP3 inflammasome activation by promoting monosodium urate crystallization, causing gout. Cells. 2021;10(8). doi:10.3390/cells10081919
26. So AK, Martinon F. Inflammation in gout: mechanisms and therapeutic targets. Nat Rev Rheumatol. 2017;13(11):639–647. doi:10.1038/nrrheum.2017.155
27. Efferth T, Oesch F. The immunosuppressive activity of artemisinin-type drugs towards inflammatory and autoimmune diseases. Med Res Rev. 2021;41(6):3023–3061. doi:10.1002/med.21842
28. Zhang F-S, He Q-Z, Qin CH, Little PJ, Weng J-P, Xu S-W. Therapeutic potential of colchicine in cardiovascular medicine: a pharmacological review. Acta Pharmacol Sin. 2022;43(9):2173–2190. doi:10.1038/s41401-021-00835-w
29. Shi M, Luo J, Ding L, Duan L. Spontaneous resolution of acute gout: mechanisms and therapeutic targets. RMD Open. 2023;9(3):e003586. doi:10.1136/rmdopen-2023-003586
30. Martinon F, Pétrilli V, Mayor A, Tardivel A, Tschopp J. Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature. 2006;440(7081):237–241. doi:10.1038/nature04516
31. Sil P, Wicklum H, Surell C, Rada B. Macrophage-derived IL-1β enhances monosodium urate crystal-triggered NET formation. Inflammation Res. 2017;66(3):227–237. doi:10.1007/s00011-016-1008-0
32. Chen C, Wang J, Guo Y, et al. Monosodium urate crystal-induced pyroptotic cell death in neutrophil and macrophage facilitates the pathological progress of gout. Small. 2023. doi:10.1002/smll.202308749
33. Cohen-Rosenblum AR, Somogyi JR, Hynes KK, Guevara ME. Orthopaedic management of gout. J Am Acad Orthopaed Surgeons Global Res Rev. 2022;6(11). doi:10.5435/JAAOSGlobal-D-22-00216
34. Zhang KH, Wang MQ, Wei LL, Feng CJ, Zhang YS, Teng JB. Investigation of the effects and mechanisms of Dendrobium loddigesii Rolfe extract on the treatment of gout. Evid Based Complement Alternat Med. 2020;2020. doi:10.1155/2020/4367347
35. Feng Y, Yu Y, Chen Z, et al. Effects of β-carotin and green tea powder diets on alleviating the symptoms of gouty arthritis and improving gut microbiota in C57BL/6 mice. Front Microbiol. 2022;13. doi:10.3389/fmicb.2022.837182
36. He L, Tang W, Huang L, et al. Rational design of a genome-based insulated system in Escherichia coli facilitates heterologous uricase expression for hyperuricemia treatment. Bioeng Transl Med. 2023;8(2):e10449. doi:10.1002/btm2.10449
37. Patil T, Soni A, Acharya S. A brief review on in vivo models for gouty arthritis. Metab Open. 2021;11:100100. doi:10.1016/j.metop.2021.100100
38. Li W-Y, Yang F, Chen J-H, Ren G-F. β-caryophyllene ameliorates MSU-induced gouty arthritis and inflammation through inhibiting NLRP3 and NF-κB signal pathway: in silico and in vivo. Front Pharmacol. 2021;12. doi:10.3389/fphar.2021.651305
39. Piao M-H, Wang H, Jiang Y-J, Wu Y-L, Nan J-X, Lian L-H. Taxifolin blocks monosodium urate crystal-induced gouty inflammation by regulating phagocytosis and autophagy. Inflammopharmacology. 2022;30(4):1335–1349. doi:10.1007/s10787-022-01014-x
40. Duan L, Chen J, Razavi M, et al. Alpha2B-adrenergic receptor regulates neutrophil recruitment in MSU-induced peritoneal inflammation. Front Immunol. 2019;10. doi:10.3389/fimmu.2019.00501
41. Duan Y, Jiang N, Chen J, Chen J. Expression, localization and metabolic function of “resurrected” human urate oxidase in human hepatocytes. Int J Biol Macromol. 2021;175:30–39. doi:10.1016/j.ijbiomac.2021.01.163
42. Lu J, Hou X, Yuan X, et al. Knockout of the urate oxidase gene provides a stable mouse model of hyperuricemia associated with metabolic disorders. Kidney Int. 2018;93(1):69–80. doi:10.1016/j.kint.2017.04.031
43. Yin C, Liu B, Li Y, et al. IL-33/ST2 induces neutrophil-dependent reactive oxygen species production and mediates gout pain. Theranostics. 2020;10(26):12189–12203. doi:10.7150/thno.48028
44. Lu J, He Y, Cui L, et al. Hyperuricemia predisposes to the onset of diabetes via promoting pancreatic β-cell death in uricase-deficient male mice. Diabetes. 2020;69(6):1149–1163. doi:10.2337/db19-0704
45. Toyoda Y, Takada T, Miyata H, et al. Identification of GLUT12/SLC2A12 as a urate transporter that regulates the blood urate level in hyperuricemia model mice. Proc Natl Acad Sci. 2020;117(31):18175–18177. doi:10.1073/pnas.2006958117
46. Ogura M, Toyoda Y, Sakiyama M, et al. Increase of serum uric acid levels associated with APOE ε2 haplotype: a clinico-genetic investigation and in vivo approach. Human Cell. 2021;34(6):1727–1733. doi:10.1007/s13577-021-00609-w
47. Lin X, Shao T, Wen X, Wang M, Wen C, He Z. Combined effects of MSU crystals injection and high fat-diet feeding on the establishment of a gout model in C57BL/6 mice. Adv Rheumatol. 2020;60(1):52. doi:10.1186/s42358-020-00155-3
48. Hao G, Xu X, Song J, Zhang J, Xu K. Lipidomics analysis facilitate insight into the molecular mechanisms of urate nephropathy in a gout model induced by combination of MSU crystals injection and high-fat diet feeding. Front Mol Biosci. 2023;10.
49. Wang J, Hao P, Sun X, et al. New animal model of chronic gout reproduces pathological features of the disease in humans. RMD Open. 2023;9(4):e003499. doi:10.1136/rmdopen-2023-003499
50. Xu H-L, Li S-K, Xue X-A, Chen Z-Y, Hua Y-H. Minimally invasive embedding of saturated MSU induces persistent gouty arthritis in modified rat model. Biomed Res Int. 2021;2021:6641701. doi:10.1155/2021/6641701
51. Shuai C, Hu S, Wang K, et al. Bionic menisci with integrated material–structure–functionality for gouty arthritis. Colloids Surf B. 2025;252:114672. doi:10.1016/j.colsurfb.2025.114672
52. Peng X, Li X, Xie B, et al. Gout therapeutics and drug delivery. J Control Release. 2023;362:728–754. doi:10.1016/j.jconrel.2023.09.011
53. Adepu S, Ramakrishna S. Controlled drug delivery systems: current status and future directions. Molecules. 2021;26(19). doi:10.3390/molecules26195905
54. Lou J, Duan H, Qin Q, et al. Advances in oral drug delivery systems: challenges and opportunities. Pharmaceutics. 2023;15(2). doi:10.3390/pharmaceutics15020484
55. Dou C, Li J, He J, et al. Bone-targeted pH-responsive cerium nanoparticles for anabolic therapy in osteoporosis. Bioact Mater. 2021;6(12):4697–4706. doi:10.1016/j.bioactmat.2021.04.038
56. Lombardi AF, Ma Y, Jang H, et al. AcidoCEST-UTE MRI reveals an acidic microenvironment in knee osteoarthritis. Int J Mol Sci. 2022;23(8). doi:10.3390/ijms23084466
57. Liu L, Wang C, Li YT, et al. Manganese dioxide nanozyme for reactive oxygen therapy of bacterial infection and wound healing. Biomater Sci. 2021;9(17):5965–5976. doi:10.1039/d1bm00683e
58. Wu YG, Zhou ZH, Zhang M, Li S, Sun MY, Song ZQ. Hollow manganese dioxide-chitosan hydrogel for the treatment of atopic dermatitis through inflammation-suppression and ROS scavenging. J Nanobiotechnol. 2023;21(1). doi:10.1186/s12951-023-02174-w
59. Mohapatra A, Rajendrakumar SK, Chandrasekaran G, et al. Biomineralized nanoscavenger abrogates proinflammatory macrophage polarization and induces neutrophil clearance through reverse migration during gouty arthritis. ACS Appl Mater Interfaces. 2023;15(3):3812–3825. doi:10.1021/acsami.2c19684
60. Zhang MJ, Yu TT, Li J, et al. Matrix metalloproteinase-responsive hydrogel with on-demand release of phosphatidylserine promotes bone regeneration through immunomodulation. Adv Sci. 2024;11(20). doi:10.1002/advs.202306924
61. Ding K, Liao MR, Wang YY, Lu JR. Advances in Composite Stimuli-Responsive Hydrogels for Wound Healing. Mechanisms Appl Gels. 2025;11(6). doi:10.3390/gels11060420
62. Wang KJ, Yin J, Chen JY, Ma J, Si HB, Xia DQ. Inhibition of inflammation by berberine: molecular mechanism and network pharmacology analysis. Phytomedicine. 2024;128. doi:10.1016/j.phymed.2023.155258
63. Xu X, Yi H, Wu J, et al. Therapeutic effect of berberine on metabolic diseases: both pharmacological data and clinical evidence. Biomed Pharmacother. 2021;133:110984. doi:10.1016/j.biopha.2020.110984
64. Chen J, Zheng Y, Gong S, et al. Mechanisms of theaflavins against gout and strategies for improving the bioavailability. Phytomedicine. 2023;114. doi:10.1016/j.phymed.2023.154782
65. Sun J, Liu X, Du J, et al. Manganese-doped albumin-gelatin composite nanogel loaded with berberine applied to the treatment of gouty arthritis in rats via a SPARC-dependent mechanism. Int J Biol Macromol. 2023;253:126999. doi:10.1016/j.ijbiomac.2023.126999
66. Zhang M, Zhang X, Tian T, et al. Anti-inflammatory activity of curcumin-loaded tetrahedral framework nucleic acids on acute gouty arthritis. Bioact Mater. 2022;8:368–380. doi:10.1016/j.bioactmat.2021.06.003
67. Zhang L, Zhang C, Zhuang Z-N, et al. Bio-inspired nanoenzyme for metabolic reprogramming and anti-inflammatory treatment of hyperuricemia and gout. Sci China Chem. 2021;64(4):616–628. doi:10.1007/s11426-020-9923-9
68. Li Z, Xue L, Yang J, et al. Synthetic biohybrids of red blood cells and cascaded-enzymes@ metal–organic frameworks for hyperuricemia treatment. Adv Sci. 2024;11(5):2305126. doi:10.1002/advs.202305126
69. Zhang T, Tian T, Zhou R, et al. Design, fabrication and applications of tetrahedral DNA nanostructure-based multifunctional complexes in drug delivery and biomedical treatment. Nat Protocols. 2020;15(8):2728–2757. doi:10.1038/s41596-020-0355-z
70. Liu Y, Sun Y, Li S, et al. Tetrahedral framework nucleic acids deliver antimicrobial peptides with improved effects and less susceptibility to bacterial degradation. Nano Lett. 2020;20(5):3602–3610. doi:10.1021/acs.nanolett.0c00529
71. Sutradhar KB, Amin ML. Nanoemulsions: increasing possibilities in drug delivery. Eur J Nanomed. 2013;5(2):97–110. doi:10.1515/ejnm-2013-0001
72. Aboumanei MH, Fayez H. Intra-articular formulation of colchicine loaded nanoemulsion systems for enhanced locoregional drug delivery: in vitro characterization, 99mTc coupling and in vivo biodistribution studies. Drug Dev Ind Pharm. 2021;47(5):770–777. doi:10.1080/03639045.2021.1934865
73. Chen L, Wang Y, Sun L, Yan J, Mao H-Q. Nanomedicine strategies for anti-inflammatory treatment of noninfectious arthritis. Adv Healthcare Mater. 2021;10(11):2001732. doi:10.1002/adhm.202001732
74. Wang Q, Liu J, Liu J, et al. Bisdemethoxycurcumin-conjugated vitamin E TPGS liposomes ameliorate poor bioavailability of free form and evaluation of its analgesic and hypouricemic activity in oxonate-treated rats. J Nanopart Res. 2021;23(6):122. doi:10.1007/s11051-021-05222-4
75. Mozaffari F, Razavian SMH, Ghasemzadeh MA. Encapsulation of allopurinol in GO/CuFe2O4/IR MOF-3 nanocomposite and in vivo evaluation of its efficiency. J Pharm Innov. 2023;18(1):149–163. doi:10.1007/s12247-022-09624-2
76. Zhang X, Cui J, Hou J, Wang W. Research progress of natural active substances with uric-acid- reducing activity. J Agric Food Chem. 2022;70(50):15647–15664. doi:10.1021/acs.jafc.2c06554
77. Hu Y, Huang WG, Luo Y, et al. Assessment of the anti-inflammatory effects of three rhubarb anthraquinones in LPS-Stimulated RAW264.7 macrophages using a pharmacodynamic model and evaluation of the structure-activity relationships. J Ethnopharmacol. 2021;273. doi:10.1016/j.jep.2021.114027
78. Shi F, Chen L, Wang Y, et al. Enhancement of oral bioavailability and anti-hyperuricemic activity of aloe emodin via novel Soluplus®-glycyrrhizic acid mixed micelle system. Drug Delivery Transl Res. 2022;12(3):603–614. doi:10.1007/s13346-021-00969-8
79. Schlesinger N, Lipsky PE. Pegloticase treatment of chronic refractory gout: update on efficacy and safety. Semin Arthritis Rheumatism. 2020;50(3, Supplement):S31–S38. doi:10.1016/j.semarthrit.2020.04.011
80. Kelly SJ, Delnomdedieu M, Oliverio MI, et al. Diabetes insipidus in uricase-deficient mice: a model for evaluating therapy with poly(ethylene glycol)-modified uricase. J Am Soc Nephrol. 2001;12(5).
81. Ban Z, Sun M, Ji H, et al. Immunogenicity-masking delivery of uricase against hyperuricemia and gout. J Control Release. 2024;372:862–873. doi:10.1016/j.jconrel.2024.06.042
82. Jung JH, Jin SG. Microneedle for transdermal drug delivery: current trends and fabrication. J Pharm Invest. 2021;51(5):503–517. doi:10.1007/s40005-021-00512-4
83. Waghule T, Singhvi G, Dubey SK, et al. Microneedles: a smart approach and increasing potential for transdermal drug delivery system. Biomed Pharmacother. 2019;109:1249–1258. doi:10.1016/j.biopha.2018.10.078
84. Singh P, Carrier A, Chen Y, et al. Polymeric microneedles for controlled transdermal drug delivery. J Control Release. 2019;315:97–113. doi:10.1016/j.jconrel.2019.10.022
85. Wang R, Jiang GH, Aharodnikau UE, et al. Recent advances in polymer microneedles for drug transdermal delivery: design strategies and applications. Macromol Rapid Commun. 2022;43(8). doi:10.1002/marc.202200037
86. Jamaledin R, Makvandi P, Yiu CK, et al. Engineered microneedle patches for controlled release of active compounds: recent advances in release profile tuning. Adv Ther. 2020;3(12):2000171.
87. Cam ME, Yildiz S, Alenezi H, et al. Evaluation of burst release and sustained release of pioglitazone-loaded fibrous mats on diabetic wound healing: an in vitro and in vivo comparison study. J Royal Soc Interface. 2020;17(162):20190712. doi:10.1098/rsif.2019.0712
88. Liu Y, Zhu X, Ji S, et al. Transdermal delivery of colchicine using dissolvable microneedle arrays for the treatment of acute gout in a rat model. Drug Delivery. 2022;29(1):2984–2994. doi:10.1080/10717544.2022.2122632
89. Chen Z, Han B, Liao L, et al. Enhanced transdermal delivery of polydatin via a combination of inclusion complexes and dissolving microneedles for treatment of acute gout arthritis. J Drug Delivery Sci Technol. 2020;55:101487. doi:10.1016/j.jddst.2019.101487
90. Santos PD, Vieira TN, Couto ACG, et al. Stephalagine, an aporphinic alkaloid with therapeutic effects in acute gout arthritis in mice. J Ethnopharmacol. 2022;293. doi:10.1016/j.jep.2022.115291
91. Anjani QK, Sabri AHB, Moreno-Castellanos N, et al. Soluplus®-based dissolving microarray patches loaded with colchicine: towards a minimally invasive treatment and management of gout. Biomater Sci. 2022;10(20):5838–5855. doi:10.1039/d2bm01068b
92. Jiang SP, Wang W, Ke JM, et al. A mechanically tough and ultra-swellable microneedle for acute gout arthritis. Biomater Sci. 2023;11(5):1714–1724. doi:10.1039/d2bm01937j
93. Woo MR, Kim JS, Cheon S, et al. Microneedles integrated with crystallinity control for poorly water-soluble drugs: enhanced bioavailability and innovative controlled release system. Mater Des. 2024;247. doi:10.1016/j.matdes.2024.113371
94. Yang Y, Li ZM, Huang P, et al. Rapidly separating dissolving microneedles with sustained-release colchicine and stabilized uricase for simplified long-term gout management. Acta Pharmaceutica Sinica B. 2023;13(8):3454–3470. doi:10.1016/j.apsb.2023.02.011
95. Wang R, Wang H, Jiang GH, et al. Transdermal delivery of allopurinol to acute hyperuricemic mice via polymer microneedles for the regulation of serum uric acid levels. Biomater Sci. 2023;11(5):1704–1713. doi:10.1039/d2bm01836e
96. Patel B, Thakkar H. Formulation development of fast dissolving microneedles loaded with cubosomes of febuxostat: in vitro and in vivo evaluation. Pharmaceutics. 2023;15(1). doi:10.3390/pharmaceutics15010224
97. Wang R, Sun Y, Wang H, et al. Core–shell structured microneedles with programmed drug release functions for prolonged hyperuricemia management. J Mat Chem B. 2024;12(4):1064–1076. doi:10.1039/D3TB02607H
98. Tang Y, Du Y, Ye J, Deng L, Cui W. Intestine-targeted explosive hydrogel microsphere promotes uric acid excretion for gout therapy. Adv Mater. 2024;36(3):2310492. doi:10.1002/adma.202310492
99. Pathan IB, Munde SJ, Shelke S, Ambekar W, Setty CM. Curcumin loaded fish scale collagen-HPMC nanogel for wound healing application: ex-vivo and in-vivo evaluation. Int J Polym Mater Polym Biomater. 2019;68(4):165–174. doi:10.1080/00914037.2018.1429437
100. Nguyen CT, Vu MQ, Phan TT, et al. Novel pH-sensitive hydrogel beads based on carrageenan and fish scale collagen for allopurinol drug delivery. J Polym Environ. 2020;28(6):1795–1810. doi:10.1007/s10924-020-01727-6
101. Li D, Xu K-Y, Zhao W-P, et al. Chinese medicinal herb-derived carbon dots for common diseases: efficacies and potential mechanisms. Front Pharmacol. 2022;13. doi:10.3389/fphar.2022.815479
102. Li H-L, Gao X-F, Li -J-J, Wan M-X, Zhang G-Q, Li Y-S. Characterization and immunogenicity of recombinant A. flavus Uox modified by Co/EDTA carbon dots. Current Pharm Biotechnol. 2024;25(2):230–246. doi:10.2174/1389201024666230519144615
103. Ma C, Jiang N, Sun X, et al. Progress in optical sensors-based uric acid detection. Biosens Bioelectron. 2023;237. doi:10.1016/j.bios.2023.115495
104. Sharma A, Choi H-K, Lee H-J. Carbon dots for the treatment of inflammatory diseases: an appraisal of in vitro and in vivo studies. Oxid Med Cell Longev. 2023;2023:3076119. doi:10.1155/2023/3076119
105. White WB, Saag KG, Becker MA, et al. Cardiovascular safety of febuxostat or allopurinol in patients with gout. N Engl J Med. 2018;378(13):1200–1210. doi:10.1056/NEJMoa1710895
106. Wang X, Zhang Y, Zhang M, et al. Novel carbon dots derived from Puerariae lobatae radix and their anti-gout effects. Molecules. 2019;24(22):4152.
107. Wang S, Zhang Y, Kong H, et al. Antihyperuricemic and anti-gouty arthritis activities of Aurantii fructus immaturus carbonisata-derived carbon dots. Nanomedicine. 2019;14(22):2925–2939. doi:10.2217/nnm-2019-0255
108. Sun J, Zhuang P, Wen S, et al. Folic acid-modified lysozyme protected gold nanoclusters as an effective anti-inflammatory drug for rapid relief of gout flares in hyperuricemic rats. Mater Des. 2022;217:110642. doi:10.1016/j.matdes.2022.110642
109. Zhu R, Niu Y, Zhou W, et al. Effect of nanoparticles on gouty arthritis: a systematic review and meta-analysis. Bmc Musculoskelet Disorders. 2023;24(1). doi:10.1186/s12891-023-06186-3
110. Kiyani MM, Rehman H, Hussain MA, et al. Inhibition of hyperuricemia and gouty arthritis in BALB/c mice using copper oxide nanoparticles. Biol Trace Elem Res. 2020;193(2):494–501. doi:10.1007/s12011-019-01734-2
111. Kiyani MM, Butt MA, Rehman H, et al. Evaluation of antioxidant activity and histopathological changes occurred by the oral ingestion of CuO nanoparticles in monosodium urate crystal-induced hyperuricemic BALB/c mice. Biol Trace Elem Res. 2022;200(1):217–227. doi:10.1007/s12011-021-02615-3
112. Kiyani MM, Butt MA, Rehman H, et al. Antioxidant and anti-gout effects of orally administered zinc oxide nanoparticles in gouty mice. J Trace Elem Med Biol. 2019;56:169–177. doi:10.1016/j.jtemb.2019.08.012
113. Kiyani MM, Moghul NB, Butt MA, et al. Anti-hyperuricemic effect of iron oxide nanoparticles against monosodium urate crystals induced gouty arthritis in BALB/c mice. Biol Trace Elem Res. 2022;200(4):1659–1666. doi:10.1007/s12011-021-02769-0
114. Kiyani MM, Moghul NB, Javed A, et al. In vivo effects of orally administered different concentrations of silver oxide nanoparticles in hyperuricemic mice. Biol Trace Elem Res. 2022;200(8):3677–3687. doi:10.1007/s12011-021-02960-3
115. Balico LDL, Gaucher EA. CRISPR-Cas9-mediated reactivation of the uricase pseudogene in human cells prevents acute hyperuricemia. Mol Ther Nucleic Acids. 2021;25:578–584. doi:10.1016/j.omtn.2021.08.002
116. Meng Y, Qi Z, Li Z, et al. Tailored hydrogel composite membrane for the regulated crystallization of monosodium urate monohydrate within coffee’s metabolites system. J Colloid Interface Sci. 2023;648:365–375. doi:10.1016/j.jcis.2023.05.183
117. Meng Y, Qi Z, Jiang H, et al. Restrained MSUM crystallization via hydrogel composited membrane based platform for gout prevention and control. Chem Eng J. 2022;450:138155. doi:10.1016/j.cej.2022.138155
118. Zheng L, Zhang Y, Shi R, et al. Nanohybrid urate oxidase with magnetically switchable catalytic potential for precise gout therapy. Biomaterials. 2025;320:123277. doi:10.1016/j.biomaterials.2025.123277
119. Liu L, Li X, Chen Y, et al. Gout management using uricase and sodium citrate hollow mesoporous nanomotors. Nat Commun. 2025;16(1):2339.
120. Wang X, Wang Y-G. Progress in treatment of gout using Chinese and Western Medicine. Chin J Integr Med. 2020;26(1):8–13. doi:10.1007/s11655-019-3058-y
121. Chi X, Zhang H, Zhang S, Ma K. Chinese herbal medicine for gout: a review of the clinical evidence and pharmacological mechanisms. ChinMed. 2020;15(1):17. doi:10.1186/s13020-020-0297-y
122. Bruchard M, Mignot G, Derangère V, et al. Chemotherapy-triggered cathepsin B release in myeloid-derived suppressor cells activates the Nlrp3 inflammasome and promotes tumor growth. Nature Med. 2013;19(1):57–64. doi:10.1038/nm.2999
123. Klück V, Jansen TLTA, Janssen M, et al. Dapansutrile, an oral selective NLRP3 inflammasome inhibitor, for treatment of gout flares: an open-label, dose-adaptive, proof-of-concept, phase 2a trial. Lancet Rheumatol. 2020;2(5):e270–e280. doi:10.1016/S2665-9913(20)30065-5
124. Quan NV, Anh LH, Lam VQ, et al. Anti-diabetes, anti-gout, and anti-leukemia properties of essential oils from natural spices Clausena indica, Zanthoxylum rhetsa, and Michelia tonkinensis. Molecules. 2022;27(3):774.
125. Goo B, Lee J, Park C, Yune T, Park Y. Bee venom alleviated edema and pain in monosodium urate crystals-induced gouty arthritis in rat by inhibiting inflammation. Toxins. 2021;13(9):661.
126. Eckenstaler R, Benndorf RA. The role of ABCG2 in the pathogenesis of primary hyperuricemia and gout—an update. Int J Mol Sci. 2021;22(13):6678.
127. Adomako EA, Moe OW. Uric acid transport, transporters, and their pharmacological targeting. Acta Physiol. 2023;238(2):e13980. doi:10.1111/apha.13980
128. Zhao T, Cao L, Lin C, et al. Intestinal uric acid excretion contributes to serum uric acid decrease during acute gout attack. Rheumatology. 2023;62(12):3984–3992. doi:10.1093/rheumatology/kead139
129. Pavelcova K, Bohata J, Pavlikova M, Bubenikova E, Pavelka K, Stiburkova B. Evaluation of the influence of genetic variants of SLC2A9 (GLUT9) and SLC22A12 (URAT1) on the development of hyperuricemia and gout. J Clin Med. 2020;9(8):2510.
130. Ristic B, Sikder MOF, Bhutia YD, Ganapathy V. Pharmacologic inducers of the uric acid exporter ABCG2 as potential drugs for treatment of gouty arthritis. Asian J Pharm Sci. 2020;15(2):173–180. doi:10.1016/j.ajps.2019.10.002
131. Yang Q-B, Li L-Q, Zhang Q-B, He Y-L, Mi Q-S, Zhou J-G. microRNA-223 deficiency exacerbates acute inflammatory response to monosodium urate crystals by targeting NLRP3. J Inflamm Res. 2021;14:1845–1858. doi:10.2147/jir.S307796
132. Zhang QB, Zhu D, Dai F, et al. MicroRNA-223 suppresses IL-1β and TNF-α production in gouty inflammation by targeting the NLRP3 inflammasome. Front Pharmacol. 2021;12. doi:10.3389/fphar.2021.637415
133. Xu Y-T, Leng Y-R, Liu -M-M, et al. MicroRNA and long noncoding RNA involvement in gout and prospects for treatment. Int Immunopharmacol. 2020;87. doi:10.1016/j.intimp.2020.106842
134. Yao L, Xu B, Li X. Neisseria gonorrhoeae-induced salpingitis is targeted by circular RNA EIF3K via miR-139-5p and regulating MAPK/NF-κB signaling pathway to promotes apoptosis and autophagy bacterial cells. Microb Pathogenesis. 2020;142. doi:10.1016/j.micpath.2020.104051
135. Chen X, Gao Q, Zhou L, Wang Y, Sun RR, Zhang ZY. MIR-146a alleviates inflammation of acute gouty arthritis rats through TLR4/MyD88 signal transduction pathway. Eur Rev Med Pharmacol Sci. 2019;23(21):9230–9237. doi:10.26355/eurrev_201911_19415
136. Ma T, Liu X, Cen Z, et al. MicroRNA-302b negatively regulates IL-1β production in response to MSU crystals by targeting IRAK4 and EphA2. Arthritis Res Therapy. 2018;20(1). doi:10.1186/s13075-018-1528-9
137. Galozzi P, Bindoli S, Doria A, Oliviero F, Sfriso P. Autoinflammatory features in gouty arthritis. J Clin Med. 2021;10(9). doi:10.3390/jcm10091880
138. Aron-Wisnewsky J, Vigliotti C, Witjes J, et al. Gut microbiota and human NAFLD: disentangling microbial signatures from metabolic disorders. Nat Rev Gastroenterol Hepatol. 2020;17(5):279–297. doi:10.1038/s41575-020-0269-9
139. Das TK, Ganesh BP. Interlink between the gut microbiota and inflammation in the context of oxidative stress in Alzheimer’s disease progression. Gut Microbes. 2023;15(1). doi:10.1080/19490976.2023.2206504
140. Fusco W, Lorenzo MB, Cintoni M, et al. Short-chain fatty-acid-producing bacteria: key components of the human gut microbiota. Nutrients. 2023;15(9). doi:10.3390/nu15092211
141. Koning M, Herrema H, Nieuwdorp M, Meijnikman AS. Targeting nonalcoholic fatty liver disease via gut microbiome-centered therapies. Gut Microbes. 2023;15(1). doi:10.1080/19490976.2023.2226922
142. Tong S, Zhang P, Cheng Q, et al. The role of gut microbiota in gout: is gut microbiota a potential target for gout treatment. Front Cell Infect Microbiol. 2022;12.
143. Dang K, Zhang N, Gao H, Wang G, Liang H, Xue M. Influence of intestinal microecology in the development of gout or hyperuricemia and the potential therapeutic targets. Int J Rheumatic Dis. 2023;26(10):1911–1922. doi:10.1111/1756-185X.14888
144. Xu Y-X, Liu L-D, Zhu J-Y, et al. Alistipes indistinctus-derived hippuric acid promotes intestinal urate excretion to alleviate hyperuricemia. Cell Host Microbe. 2024;32(3):366–381.e9. doi:10.1016/j.chom.2024.02.001
145. Wang Z, Li Y, Liao W, et al. Gut microbiota remodeling: a promising therapeutic strategy to confront hyperuricemia and gout. Front Cell Infect Microbiol. 2022;12. doi:10.3389/fcimb.2022.935723
146. Yang H-T, Xiu W-J, Liu J-K, et al. Gut microbiota characterization in patients with asymptomatic hyperuricemia: probiotics increased. Bioengineered. 2021;12(1):7263–7275. doi:10.1080/21655979.2021.1976897
147. Wei J, Zhang Y, Dalbeth N, et al. Association between gut microbiota and elevated serum urate in two independent cohorts. Arthritis Rheumatol. 2022;74(4):682–691. doi:10.1002/art.42009
148. Bian M, Wang J, Wang Y, et al. Chicory ameliorates hyperuricemia via modulating gut microbiota and alleviating LPS/TLR4 axis in quail. Biomed Pharmacother. 2020;131:110719. doi:10.1016/j.biopha.2020.110719
149. James A, Ke H, Yao T, Wang Y. The role of probiotics in purine metabolism, hyperuricemia and gout: mechanisms and interventions. Food Rev Int. 2023;39(1):261–277. doi:10.1080/87559129.2021.1904412
150. Han J, Wang Z, Lu C, et al. The gut microbiota mediates the protective effects of anserine supplementation on hyperuricaemia and associated renal inflammation. Food Funct. 2021;12(19):9030–9042. doi:10.1039/D1FO01884A
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Mechanistic Study on the Therapeutic Effects of Juanbi Lijieqing Formula in a Rat Model of Gouty Arthritis with Hyperuricemia
Lu Y, Lu C, Jian G, Xiong H, Shu Y
Journal of Pain Research 2025, 18:2865-2877
Published Date: 9 June 2025
Hyperuricemia Remission After Sleeve Gastrectomy in Chinese Patients and Establishment of a Preoperative Predictive Model: A Retrospective Cohort Study with a Mean Follow-Up of 20 Months
Chen X, Li Z, Wang Z, Sun Y, Shang M, Tian C, Liao Z, Lian D, Amin B, Du D, Xu G, Zhang N, Wang L
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2825-2836
Published Date: 12 August 2025
Subclinical Cardiac Dysfunction in Hyperuricemic Gout and Asymptomatic Hyperuricemia: A Comparative Echocardiographic Study
Jiang R, Wen W, Li Q, Dang W, He Y, Wang J, Liu J
International Journal of General Medicine 2025, 18:6909-6922
Published Date: 11 November 2025