Back to Journals » International Journal of Women's Health » Volume 18
Bidirectional Associations Between Circulating Polyunsaturated Fatty Acids and Female Reproductive Endocrine-Related Diseases: A Mendelian Randomization Study
Received 22 January 2026
Accepted for publication 17 June 2026
Published 9 July 2026 Volume 2026:18 598204
DOI https://doi.org/10.2147/IJWH.S598204
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
YiLian Pan,1– 3,* Jilan Jiang,1– 3,* Feng Sun1– 3
1Department of Gynecology & Obstetrics, International Peace Maternity & Child Health Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Shanghai Key Laboratory of Embryo Original Diseases, Shanghai, People’s Republic of China; 3Shanghai Municipal Key Clinical Specialty, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feng Sun, Department of Gynaecology & Obstetrics, International Peace Maternity & Child Health Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China, Email [email protected]
Objective: Polyunsaturated fatty acids (PUFAs) are hypothesized to modulate female reproductive endocrine disorders, yet their causal relationships remain elusive. We employed Mendelian randomization (MR) to investigate bidirectional causality between circulating PUFAs (omega-3/6 subtypes, docosahexaenoic acid [DHA], linoleic acid) and endometriosis, infertility, polycystic ovary syndrome (PCOS), premenstrual syndrome, and premature ovarian insufficiency (POI).
Materials and Methods: In this two-sample MR study, exposure data from a GWAS of 115,006 Europeans were analyzed against outcome data (FinnGen and other large-scale GWAS). Forward MR assessed PUFA effects on disorders; reverse MR evaluated disorder-driven PUFA alterations. Sensitivity analyses (MR-Egger, MR-PRESSO, leave-one-out) ensured robustness.
Results: Elevated linoleic acid and total omega-6 levels increased endometriosis (OR=1.127, P=0.039; OR=1.123, P=0.037) and infertility risks (OR=1.155, P=0.019), while higher PUFA-to-total fatty acid ratios conferred protection (endometriosis: OR=0.857, P=0.017). PCOS genetically reduced DHA and total omega-3 levels while elevating omega-6/3 ratios (P< 0.05). No reverse effects were observed for other disorders.
Conclusion: Our findings implicate linoleic acid and omega-6 PUFAs as potential risk factors for endometriosis and infertility, whereas balanced PUFA ratios may be protective. PCOS disrupts omega-3 homeostasis, suggesting bidirectional metabolic interplay. These results highlight PUFAs as modifiable targets for nutritional and therapeutic strategies in reproductive health, warranting further mechanistic and clinical validation.
Keywords: two-sample mendelian randomization, endometriosis, infertility, polycystic ovary syndrome, polyunsaturated fatty acids, omega-3 fatty acids
Introduction
Female reproductive endocrine disorders, including endometriosis, infertility, polycystic ovary syndrome (PCOS), premenstrual syndrome (PMS), and premature ovarian insufficiency (POI), are among the most prevalent and debilitating conditions affecting women of reproductive age worldwide.1 Collectively, these disorders impact an estimated 10–20% of women globally, posing significant challenges to fertility, mental health, and overall quality of life.2 Endometriosis alone is associated with an annual economic burden exceeding $12,000 per patient in direct healthcare costs.3 Similarly, PCOS is associated with an increased risk of metabolic syndrome, type 2 diabetes, and cardiovascular disease, reflecting the broader systemic implications of these disorders.4 Despite advances in diagnostic and symptomatic management strategies, the underlying etiologies of these conditions remain incompletely understood, involving complex interactions between genetic predisposition, endocrine dysregulation, immune dysfunction, and environmental factors.5–7 There is an urgent need to identify modifiable biomarkers that could pave the way for novel prevention and therapeutic strategies.
Polyunsaturated fatty acids (PUFAs), comprising omega-3 (eg., docosahexaenoic acid [DHA]) and omega-6 (eg., linoleic acid) subtypes, are emerging as key modulators in reproductive physiology and pathophysiology.8 Omega-3 PUFAs are known to exert anti-inflammatory effects by inhibiting cyclooxygenase-2 activity and reducing prostaglandin E2 synthesis, mechanisms that may limit the proliferation of ectopic endometrial tissue in endometriosis.9,10 Conversely, omega-6 PUFAs serve as precursors for pro-inflammatory eicosanoids such as leukotrienes and thromboxanes, which may exacerbate ovarian hyperandrogenism and insulin resistance in PCOS.11 Observational studies have highlighted inverse associations between dietary omega-3 intake and endometriosis risk, with a pooled odds ratio (OR) of 0.78 (95% confidence interval [CI]: 0.65–0.94) in meta-analyses.12 However, the evidence for omega-6 PUFAs remains inconclusive, with some studies suggesting null or even protective effects. These discrepancies underscore the need for robust methodologies that can disentangle causality from confounding. Although several clinical trials have demonstrated that supplementation of PUFAs (such as omega-3s) can alleviate PMS, the dose and durations of supplementation varied.13,14 In contrast, another study from Houghton et al suggested that individual PUFAs were not associated with risk of PMS.15 And to best of our knowledge, there was no study have investigated the relationship between PUFAs and POI.
Importantly, circulating PUFA levels should not be interpreted simply as direct surrogates of dietary intake. Although plasma and erythrocyte PUFA concentrations provide objective biomarkers of PUFA status and partially reflect habitual dietary intake, they are also influenced by endogenous metabolic processes, including intestinal absorption, hepatic lipid metabolism, fatty acid desaturation and elongation, β-oxidation, adipose tissue storage and mobilization.16–20 Meanwhile, body mass index (BMI) has been reported to determine the plasma long-chain PUFA response to dietary fat manipulation.21 Since the widely acknowledged association between BMI and metabolic dysfunction with female reproductive endocrine disorders,22,23 conventional observational studies are vulnerable to confounding by metabolic factors. In addition, reliance on self-reported dietary intake introduces recall bias and measurement error, while correlations between self-reported PUFA intake and circulating PUFA biomarkers are often only moderate, indicating substantial uncertainty in traditional nutritional epidemiology.24,25
In addition, candidate-gene and polymorphism association studies, such as recent evidence on ADIPOQ variants in PCOS, suggest that sequence variations may contribute to PCOS-related phenotypes, although reported SNP–disease associations remain heterogeneous across populations and genetic loci.26
To address these limitations, Mendelian randomization (MR) represents a robust epidemiological approach that employs genetic variants as instrumental variables (IVs) to proxy lifelong exposure levels.27 By mimicking the principles of randomized controlled trials, MR reduces the influence of confounding and reverse causation, enabling robust causal inference.28
The validity of MR findings hinges on three core assumptions: (1) the IVs are robustly associated with the exposure (F-statistic > 10); (2) the IVs are independent of confounders of the exposure-outcome relationship; and (3) the IVs influence the outcome exclusively through the exposure, with no horizontal pleiotropy.29,30 MR has been instrumental in elucidating causal links between lipid traits and cardiometabolic outcomes,31 yet its application to reproductive endocrine disorders is still in its infancy. To date, no MR study has comprehensively evaluated the bidirectional causal relationships between circulating PUFA subtypes and female reproductive disorders, leaving critical mechanistic gaps unaddressed. This study seeks to fill these gaps through a two-sample MR design, integrating data from large-scale genome-wide association studies (GWAS) on circulating PUFAs and female reproductive disorders. Specifically, we aim to provide novel insights into the role of PUFAs as mediators of reproductive pathophysiology, advancing our understanding of their potential as modifiable targets for intervention. By addressing key limitations in prior observational research and leveraging robust statistical frameworks, this work has the potential to inform precision nutrition and lifestyle interventions tailored to high-risk populations.
Materials and Methods
Study Design
This study employed a two-sample Mendelian randomization (MR) design to examine the causal effects of circulating polyunsaturated fatty acids (PUFAs) on female reproductive endocrine disorders (Figure 1).
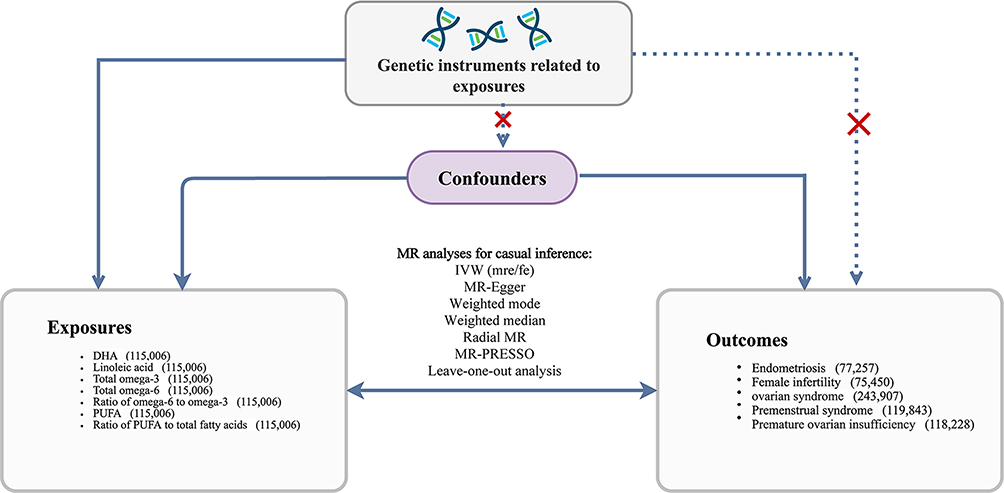 |
Figure 1 Directed acyclic graph illustrating the bidirectional Mendelian randomization framework between circulating polyunsaturated fatty acid-related traits and female reproductive endocrine disorders. Solid arrows indicate assumed causal pathways, and the double-headed arrow indicates the bidirectional MR design. Red cross symbols indicate that genetic instruments should not be associated with confounders or directly affect outcomes except through exposures. Bold text denotes the main analytical components. Abbreviations: IVW, inverse-variance weighted; MR, Mendelian randomization; DHA, docosahexaenoic acid; PUFA, polyunsaturated fatty acid. |
By employing genetic variants as instrumental variables (IVs), the MR approach provides a robust method to infer causality, addressing limitations inherent in observational studies, such as residual confounding and reverse causation. The validity of MR relies on three key assumptions. First, the relevance assumption requires that the selected IVs are strongly associated with the exposure of interest, ensuring that genetic variants significantly predict circulating PUFA levels. Second, the independence assumption mandates that IVs are not associated with any confounders of the exposure-outcome relationship, which is generally supported by the random allocation of alleles during meiosis. Third, the exclusion restriction assumption specifies that IVs influence the outcome only through their effects on the exposure, with no alternative pathways such as horizontal pleiotropy. These assumptions were rigorously evaluated and validated to ensure reliable causal inference.
Data Sources
Exposure Data
Genetic associations for circulating PUFA levels were sourced from a large-scale genome-wide association study (GWAS) of 115,006 individuals of European ancestry. This GWAS dataset provided comprehensive coverage of PUFA-related traits, including docosahexaenoic acid (DHA), linoleic acid, total omega-3 fatty acids, total omega-6 fatty acids, the ratio of omega-6 to omega-3 fatty acids, total PUFAs, and the ratio of PUFAs to total fatty acids. These data were sourced from the European Bioinformatics Institute (EBI) database, with relevant summary statistics published under GWAS Catalog IDs ranging from ebi-a-GCST90092816 to ebi-a-GCST90092941. The high-quality data from this large cohort provided a robust foundation for exploring the genetic determinants of PUFA levels and their subsequent effects on health outcomes.
Outcome Data
The outcome data were derived from GWAS datasets representing European ancestry populations from the FinnGen biobank analysis round 5. Specifically, endometriosis was examined in 77,257 participants (of whom 8,288 were cases),32 female infertility in 75,450 participants, polycystic ovarian syndrome in 220,609 individuals, premenstrual syndrome in 111,878 participants, and premature ovarian insufficiency in 118,228 participants. These datasets were selected for their large sample sizes, comprehensive genomic coverage, and rigorous phenotypic characterization, which together maximize statistical power and enhance the reliability of causal estimates. All data are publicly available at https://gwas.mrcieu.ac.uk/.
Selection of Instrumental Variables (IVs)
Instrumental variables were selected from the PUFA GWAS based on genome-wide significance thresholds ( ) to ensure strong associations with PUFA levels, satisfying the relevance assumption. To maintain independence between selected variants, clumping procedures were applied to remove linkage disequilibrium (LD) using an
) to ensure strong associations with PUFA levels, satisfying the relevance assumption. To maintain independence between selected variants, clumping procedures were applied to remove linkage disequilibrium (LD) using an  threshold of 0.001 within a 10,000 kilobase window. Palindromic single nucleotide polymorphisms (SNPs) with intermediate allele frequencies were excluded to minimize strand ambiguity and ensure consistency in allele alignment across datasets. These rigorous criteria ensured that the selected SNPs were robustly associated with circulating PUFA levels while minimizing potential bias introduced by LD or technical errors.
threshold of 0.001 within a 10,000 kilobase window. Palindromic single nucleotide polymorphisms (SNPs) with intermediate allele frequencies were excluded to minimize strand ambiguity and ensure consistency in allele alignment across datasets. These rigorous criteria ensured that the selected SNPs were robustly associated with circulating PUFA levels while minimizing potential bias introduced by LD or technical errors.
Horizontal Pleiotropy Assessment
The potential influence of horizontal pleiotropy, where IVs affect outcomes through pathways independent of the exposure, was assessed using multiple approaches. MR-Egger regression was employed to detect directional pleiotropy, with the intercept term providing a quantitative measure of deviation from the exclusion restriction assumption. A significant intercept term ( ) indicated the presence of pleiotropy. To address this, sensitivity analyses were conducted using methods robust to pleiotropy, including the weighted mode and weighted median approaches, which provide valid estimates even when a portion of the IVs are invalid. Additionally, MR-PRESSO (Pleiotropy Residual Sum and Outlier) was used to detect and correct for outliers that might bias causal estimates. Harmonization of SNPs across exposure and outcome datasets ensured consistent alignment of alleles, further reducing the risk of pleiotropic bias.
) indicated the presence of pleiotropy. To address this, sensitivity analyses were conducted using methods robust to pleiotropy, including the weighted mode and weighted median approaches, which provide valid estimates even when a portion of the IVs are invalid. Additionally, MR-PRESSO (Pleiotropy Residual Sum and Outlier) was used to detect and correct for outliers that might bias causal estimates. Harmonization of SNPs across exposure and outcome datasets ensured consistent alignment of alleles, further reducing the risk of pleiotropic bias.
Strength of Instruments
The strength of the selected IVs was evaluated using the  -statistic and the proportion of variance in the exposure explained by the IVs (
-statistic and the proportion of variance in the exposure explained by the IVs ( ).33 The
).33 The  -statistic was calculated using the formula:
-statistic was calculated using the formula:

where  is the sample size,
is the sample size,  is the number of IVs, and
is the number of IVs, and  represents the proportion of exposure variance explained by the IVs.34 An
represents the proportion of exposure variance explained by the IVs.34 An  -statistic exceeding 10 was used to define strong instruments, minimizing the risk of weak instrument bias and ensuring robust causal inference.
-statistic exceeding 10 was used to define strong instruments, minimizing the risk of weak instrument bias and ensuring robust causal inference.
Causal Effect Estimation
Causal effects were estimated using the inverse variance-weighted (IVW) method, the primary approach for two-sample MR analyses. Both multiplicative random-effects and fixed-effects models were applied, with random-effects results prioritized in the presence of heterogeneity. Sensitivity analyses complemented the primary IVW approach, including the weighted median method, which provides robust estimates when up to 50% of IVs are invalid, and the MR-Egger regression, which accounts for pleiotropy under the Instrument Strength Independent of Direct Effect (InSIDE) assumption. MR-PRESSO was used to identify and correct for outlier SNPs, while Radial MR was implemented to detect influential SNPs and assess small-sample bias. To further evaluate the robustness of causal estimates, a leave-one-out analysis was conducted by systematically excluding individual SNPs from the analysis.
Heterogeneity Testing
Heterogeneity among SNP-specific causal estimates was assessed using Cochran’s  statistic, which quantifies the deviation of individual SNP effects from the overall IVW estimate. Significant heterogeneity, indicated by
statistic, which quantifies the deviation of individual SNP effects from the overall IVW estimate. Significant heterogeneity, indicated by  , prompted the use of random-effects models, which account for between-SNP variability. The presence of heterogeneity was considered when interpreting results, as it may reflect biological differences in SNP effects or potential violations of MR assumptions.
, prompted the use of random-effects models, which account for between-SNP variability. The presence of heterogeneity was considered when interpreting results, as it may reflect biological differences in SNP effects or potential violations of MR assumptions.
Reverse Causality Testing
To examine the potential for reverse causation, the MR-Steiger test was conducted, evaluating whether the genetic variants explained more variance in the exposure than in the outcome. This approach ensured the validity of causal directionality, distinguishing exposure-driven effects from outcome-driven genetic associations.
Sensitivity Analyses and Statistical Significance
Sensitivity analyses included the consistency of results across multiple MR methods, such as IVW, MR-Egger, weighted median, and weighted mode. Results were considered robust if causal estimates were consistent in direction and magnitude across methods. Statistical significance was defined at a two-sided  , with findings contextualized within biological plausibility and prior literature. All analyses were conducted using the TwoSampleMR R package and related statistical tools, ensuring transparency and reproducibility in the analytical process.
, with findings contextualized within biological plausibility and prior literature. All analyses were conducted using the TwoSampleMR R package and related statistical tools, ensuring transparency and reproducibility in the analytical process.
Results
Overview of Data and Outcomes
An additional file summarizes the GWAS data sources for the PUFA-related traits and the five female reproductive endocrine disorders investigated (Table S1). The exposures, including circulating levels of DHA, linoleic acid, total omega-3, total omega-6, the omega-6/omega-3 ratio, PUFA, and the PUFA to total fatty acids ratio, originate from a European population GWAS (N=115,006).The outcomes of interest were endometriosis, female infertility, PCOS, premenstrual syndrome, and POI, each obtained from distinct large-scale GWAS consortia or FinnGen releases. This dataset provides a comprehensive foundation for forward Mendelian randomization (MR) analyses to test the causal roles of circulating PUFA phenotypes, as well as for reverse MR to explore the potential impact of these disorders on PUFA levels.
Instrument Selection
In the forward MR, each exposure was instrumented by SNPs that reached genome-wide significance ( ). An additional file details the number of original, LD-pruned, and palindromic-removed SNPs, along with the resultant F-statistics and proportion of variance explained (
). An additional file details the number of original, LD-pruned, and palindromic-removed SNPs, along with the resultant F-statistics and proportion of variance explained ( ) (Table S2). For instance, 34–43 SNPs were retained for DHA, each set explaining roughly 4.09% to 4.14% of the phenotypic variance, with F-values above 100 in most cases, suggesting robust instruments. Similarly, 41–46 instruments were identified for linoleic acid (
) (Table S2). For instance, 34–43 SNPs were retained for DHA, each set explaining roughly 4.09% to 4.14% of the phenotypic variance, with F-values above 100 in most cases, suggesting robust instruments. Similarly, 41–46 instruments were identified for linoleic acid ( ) and 49–57 instruments for total omega-6 (
) and 49–57 instruments for total omega-6 ( ). This table also indicates if any outlier SNPs were detected by MR-PRESSO or Radial MR, such as rs115478735 for linoleic acid, total omega-6, and PUFA in the endometriosis analysis. No substantial issues with weak instrument bias were observed, as all F-statistics exceeded the conventional threshold of 10.
). This table also indicates if any outlier SNPs were detected by MR-PRESSO or Radial MR, such as rs115478735 for linoleic acid, total omega-6, and PUFA in the endometriosis analysis. No substantial issues with weak instrument bias were observed, as all F-statistics exceeded the conventional threshold of 10.
Horizontal Pleiotropy, Heterogeneity, and Directionality Testing
Before estimating causal effects, we checked for potential pleiotropy and heterogeneity among the genetic instruments. Table 1 reports the MR-Egger intercept for each exposure–outcome pair (to detect horizontal pleiotropy), the MR-Steiger direction test, and Cochran’s Q statistics for both MR-Egger and IVW models (to evaluate between-SNP heterogeneity). In nearly all comparisons, the MR-Egger intercept did not reach statistical significance, implying that unbalanced horizontal pleiotropy was not a major issue. The MR-Steiger tests consistently confirmed the hypothesized direction of causality (exposure → outcome). However, Cochran’s Q test revealed notable heterogeneity among the instrumental variables (IVs) for DHA, Total omega-3, Total omega-6, the ratio of omega-6 to omega-3, and PUFA with respect to Polycystic Ovarian Syndrome. This finding prompted the use of a multiplicative random-effects IVW model rather than a fixed-effects model.
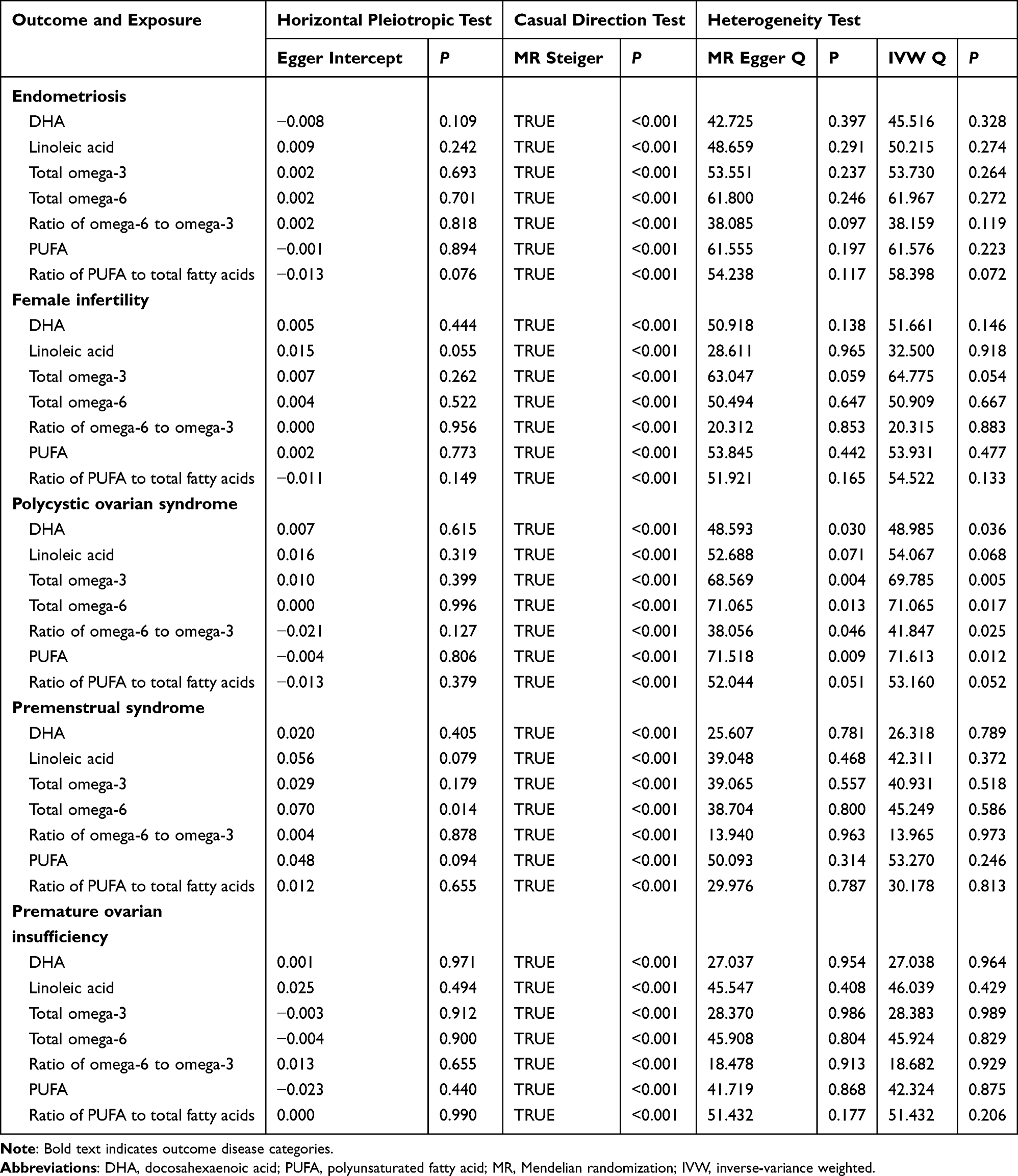 |
Table 1 The Pleiotropic and Heterogeneity Test |
Subsequently, we focused on outlier SNP detection as detailed in Table 2. In the MR-PRESSO and Radial MR tests, several outlier SNPs (eg., rs115478735) were identified. Where necessary, these outlier SNPs were removed to correct for potential horizontal pleiotropy. Importantly, the corrected analyses generally did not drastically alter the magnitude or direction of the causal estimates. For example, the causal relationships between Linoleic acid, Total omega-6, and PUFA with Endometriosis remained statistically insignificant even after the exclusion of the outlier SNPs (as shown in Table 1 and Table 2), thereby supporting the robustness of the main finding.
 |
Table 2 The MR-PRESSO and Radial Test in Forward MR |
MR Results
The primary MR analyses, based on IVW estimates (both fixed-effects and multiplicative random-effects), evaluated the relationships between PUFA-related exposures on various female endocrine disorders (Table 3). The visualization of Mendelian randomization showed stable results, further confirming the reliability of our study findings. Graphical representations, including forest plots (Figure 2) and scatter plots (Figure 3), were used to illustrate these associations.
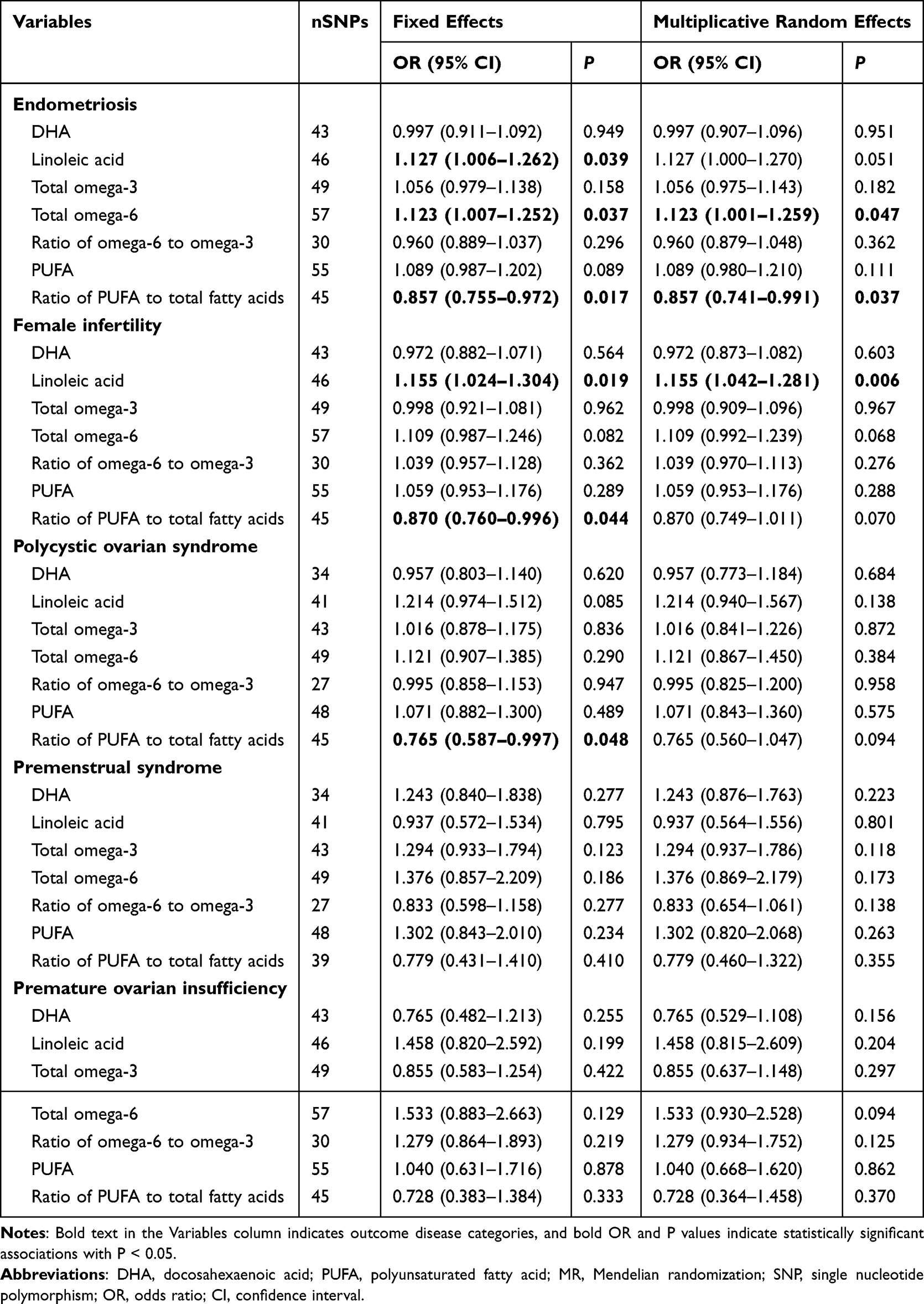 |
Table 3 The MR Results of Exposures and Outcomes |
 |
Figure 2 Forest plot of the forward Mendelian randomization analysis using fixed-effect IVW and multiplicative random-effect IVW models. The left and right panels show estimates from the fixed-effect IVW and multiplicative random-effect IVW models, respectively. Dots represent OR estimates, horizontal bars represent 95% CIs, and the vertical dashed line indicates OR = 1. Orange and blue text indicate statistically significant risk and protective effects, respectively, while black text indicates non-significant associations. Bold text indicates grouped PUFA-related exposure categories, and indented non-bold text indicates the corresponding outcome traits. Abbreviations: IVW, inverse-variance weighted; MR, Mendelian randomization; OR, odds ratio; CI, confidence interval; SNP, single nucleotide polymorphism; DHA, docosahexaenoic acid; PUFA, polyunsaturated fatty acid. |
 |
Figure 3 The scatter plots for different Mendelian randomization (MR) methods show consistent β values. (A) Total omega-6 to Endometriosis. (B) Linoleic acid to Endometriosis. (C) Linoleic acid to Female infertility. (D) Ratio of PUFA to total fatty acids to Polycystic ovarian syndrome. (E) Ratio of PUFA to total fatty acids to Endometriosis. (F) Ratio of PUFA to total fatty acids to Female infertility. |
A notably consistent finding was the positive association of genetically predicted linoleic acid levels with both endometriosis and female infertility. In the fixed-effects IVW analysis, linoleic acid exhibited an odds ratio (OR) of approximately 1.127 for endometriosis and 1.155 for female infertility (Figure 2); the random-effects models yielded similar or slightly stronger estimates. These results suggest that elevated circulating linoleic acid may increase susceptibility to these gynecological conditions (Figures 3B and C).
Total omega-6 also demonstrated a significant positive causal association with endometriosis, with an OR near 1.123 in the fixed-effects IVW analysis (Figure 2). The random-effects analysis was marginally significant as well, indicating that higher total omega-6 levels might contribute to an increased risk of endometriosis (Figure 3A).
In contrast, an intriguing inverse association was observed for the ratio of PUFA to total fatty acids (TFAs). This ratio appeared protective against endometriosis, female infertility, and polycystic ovarian syndrome. Specifically, for endometriosis, the fixed-effects IVW analysis showed an OR of roughly 0.857 (Figure 2), with similar trends observed under random-effects modeling. For female infertility and PCOS, protective effects were apparent under fixed-effects, although these associations were less robust in the random-effects models (Figure 3D–F) visually depict how higher values of this ratio align with lower disease risk).
Additionally, leave-one-out analysis validated the stability of the results, with no single SNP significantly altering the causal estimates (see Figure S1–S6). These sensitivity analyses collectively affirm the robustness of our MR results.
Furthermore, no definitive causal relationships were consistently identified for DHA, total omega-3, the ratio of omega-6 to omega-3, or total PUFA with respect to most outcomes (including premenstrual syndrome and premature ovarian insufficiency). Although some secondary or sensitivity analyses (eg., MR-PRESSO results for DHA and endometriosis) suggested minor trends, these findings were not supported by the primary IVW analyses.
Overall, the IVW results indicate that increased circulating levels of linoleic acid and total omega-6 may elevate the risk of endometriosis and, in the case of linoleic acid, female infertility, whereas a higher ratio of PUFA to total fatty acids may confer a protective effect against endometriosis, female infertility, and polycystic ovarian syndrome. Additional analyses using weighted median and weighted mode methods are provided in supplementary materials (Table S3).
Reverse MR Analyses
We additionally tested whether reproductive endocrine disorders—endometriosis, female infertility, PCOS, premenstrual syndrome, and POI—causally affect circulating PUFA traits. In these reverse models, the MR Egger intercept tests generally indicated minimal horizontal pleiotropy and the Cochran’s Q tests suggested little heterogeneity. However, for PCOS, evidence of horizontal pleiotropy was detected by the MR-Egger intercept test for SNPs associated with circulating PUFA, the ratio of PUFA to total fatty acids, total omega-6, and linoleic acid, whereas Cochran’s Q test continued to show no significant heterogeneity (Table S4).
Among all reverse analyses, polycystic ovarian syndrome showed the strongest potential to influence certain PUFA measures. Specifically, genetic liability to PCOS was associated with decreased levels of the ratio of PUFA to total fatty acids, total omega-3, and DHA, and a potential increase in the ratio of omega-6 to omega-3. Although the effect sizes were modest, the directions of these associations were consistent across both fixed-effects and multiplicative random-effects IVW models (Table 4) and Figure 4 visually depicts an inverse association for PCOS with the ratio of PUFA to total fatty acids, total omega-3, and DHA (all below unity), as well as a positive shift in the ratio of omega-6 to omega-3 in certain analyses.
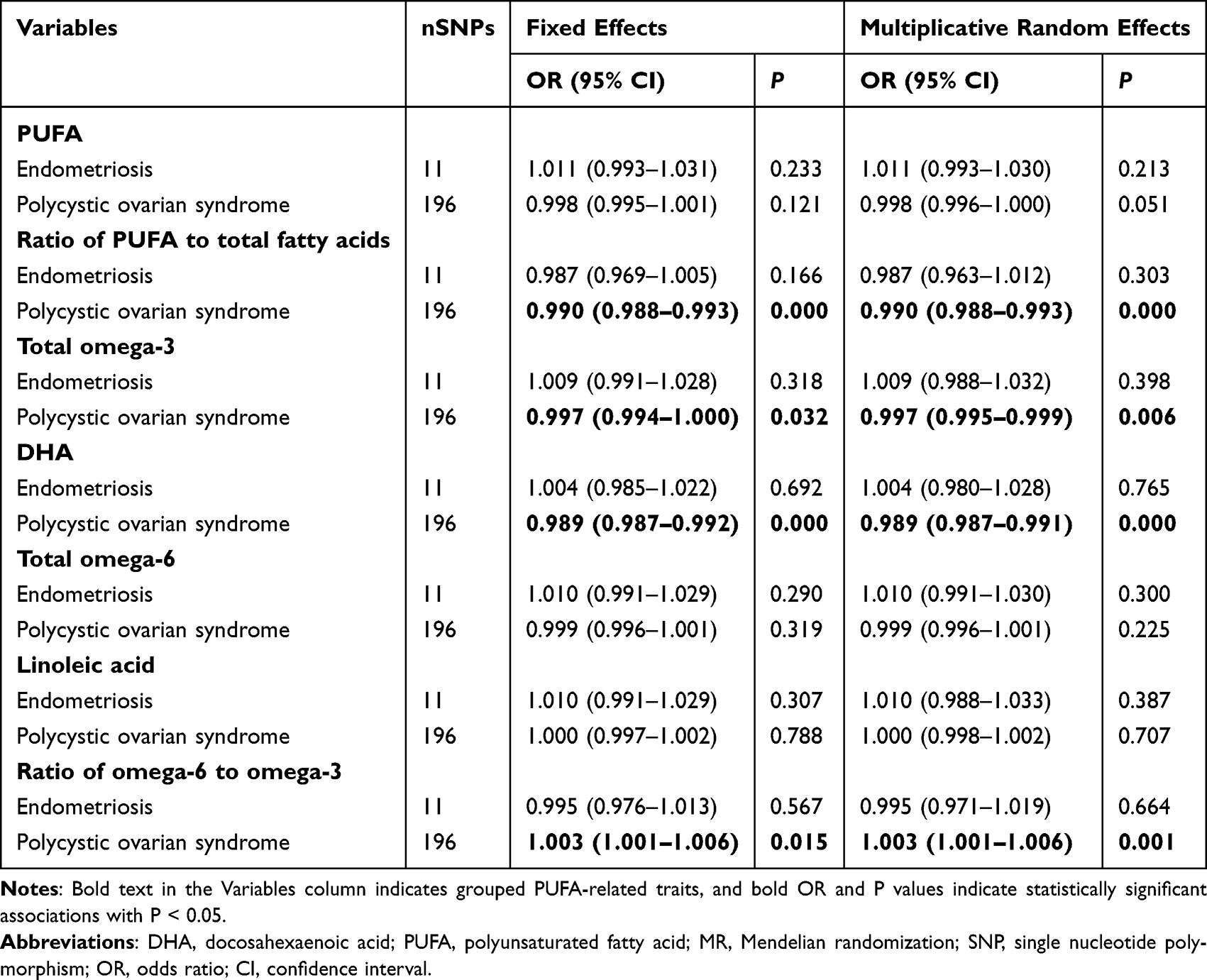 |
Table 4 The Reverse MR Results of Exposures and Outcomes |
 |
Figure 4 Forest plot of the reverse Mendelian randomization analysis using fixed-effect IVW and multiplicative random-effect IVW models. The left and right panels show estimates from the fixed-effect IVW and multiplicative random-effect IVW models, respectively. Dots represent OR estimates, horizontal bars represent 95% CIs, and the vertical dashed line indicates OR = 1. Orange and blue text indicate statistically significant positive and negative associations, respectively, while black text indicates non-significant associations. Bold text indicates grouped reproductive disorder categories, and indented non-bold text indicates the corresponding PUFA-related traits. Abbreviations: IVW, inverse-variance weighted; MR, Mendelian randomization; OR, odds ratio; CI, confidence interval; SNP, single nucleotide polymorphism; DHA, docosahexaenoic acid; PUFA, polyunsaturated fatty acid. |
In contrast, endometriosis, female infertility, premenstrual syndrome, and POI did not exhibit robust causal effects on the measured PUFA phenotypes. Across multiple tests, most estimates were centered around null values, providing no strong evidence that these conditions directly alter fatty acid profiles in circulation.
Summary of the Experimental Results
Graphical representations of the forward MR results (Figure 2) illustrate that the slope of the fitted lines—whether estimated via IVW or MR-Egger—remains consistent with the statistical findings. Our analysis indicates that elevated levels of linoleic acid or total omega-6 are implicated in an increased risk of several reproductive disorders. Conversely, a higher PUFA-to-TFA ratio is linked to a protective effect against these conditions.In contrast, Figure 4, which presents the reverse MR scenario through forest plots, confirms that PCOS is consistently linked with lower levels of beneficial PUFA fractions, including DHA, total omega-3, and the ratio of PUFA to total fatty acids, while also showing an increased ratio of omega-6 to omega-3.
Collectively, these analyses indicate that elevated circulating linoleic acid and total omega-6 may raise the risk of endometriosis—and, in the case of linoleic acid, female infertility—while a higher ratio of PUFAs to TFAs may protect against endometriosis, female infertility, and PCOS. Conversely, reverse MR analyses suggest that genetic liability to PCOS may reduce beneficial PUFA-related measures and shift the balance towards a more pro-inflammatory state by increasing the ratio of omega-6 to omega-3. These findings underscore the importance of monitoring specific fatty acid subtypes in women’s health and suggest that interventions targeting the balance between omega-6 and omega-3 could potentially mitigate the burden of endometriosis, infertility, and other reproductive conditions in susceptible populations.
Discussion
This study applied a two-sample Mendelian randomization (MR) framework to examine the causal relationships between circulating PUFA traits and female reproductive endocrine disorders—including endometriosis, female infertility, PCOS, PMS and POI.
By leveraging both forward and reverse MR analyses, our study addresses the inherent limitations of traditional observational studies, such as unmeasured confounding and reverse causation, thereby strengthening the evidence for causal conclusions.
In the forward MR analyses, elevated levels of linoleic acid and total omega-6 were positively associated with endometriosis and female infertility, with linoleic acid showing the strongest and most consistent effects. It could be explained by the role of omega-6-related lipid metabolism in reproductive tract inflammation.35 Linoleic acid is the parent omega-6 PUFA and can be metabolically connected to downstream omega-6 pathways, including arachidonic acid-derived eicosanoid production.36 Arachidonic acid serves as a precursor for prostaglandins and leukotrienes, which are central mediators of inflammatory signaling.36 On the other hand, prostaglandins and leukotrienes could be directly involved in reproductive physiology and pathology. In endometriosis, endometriotic lesions show increased COX-2 expression and COX-2-derived PGE2 biosynthesis compared with normal endometrium.37 COX-2/PGE2 axis promotes inflammatory activation, lesion survival, angiogenesis, pain sensitization, and local estrogen production, thereby supporting the inflammatory microenvironment required for lesion persistence.37 Leukotrienes, generated through the 5-lipoxygenase pathway, may further amplify inflammatory cell recruitment, vascular permeability, and peritoneal inflammatory responses.36 For female infertility, PUFA-derived prostaglandin signaling may also influence reproductive physiology by regulating prostaglandin synthesis, steroid metabolism, ovulation, endometrial receptivity, and implantation.35 Conversely, a higher ratio of PUFAs to TFAs appeared to be protective against endometriosis, female infertility, and PCOS. This protective effect likely reflects the anti-inflammatory role of omega-3 PUFAs, which counteract omega-6-mediated inflammation by producing mediators such as resolvins and protectins.38 Notably, the ratio of omega-6 to omega-3, an established marker of inflammatory balance39 did not show significant causal associations, suggesting that overall PUFA balance may be more critical than their relative proportions.
Reverse MR analyses further revealed that genetic liability to PCOS might lead to systemic changes in lipid profiles, specifically by reducing total omega-3 and DHA levels and increasing the ratio of omega-6 to omega-3. Although the effect sizes were modest, these findings suggest that PCOS may shift the PUFA profile toward a more pro-inflammatory state, potentially exacerbating the condition. One possible explanation involves the FADS1–FADS2 desaturase pathway. The FADS gene cluster has been associated with PCOS susceptibility, and FADS2 encodes Δ6 desaturase, a key enzyme involved in the endogenous conversion of essential fatty acid precursors, including α-linolenic acid and linoleic acid, into their long-chain PUFA metabolites.40,41 Because omega-3 and omega-6 precursors share desaturase and elongase enzymes, reduced FADS2 expression or activity could create a metabolic bottleneck that limits the conversion of α-linolenic acid toward long-chain omega-3 species, including DHA, while favoring a higher omega-6 to omega-3 balance under conditions of abundant omega-6 substrate availability.42,43
In addition to the FADS1–FADS2 pathway, hormonal imbalance may also partly explain the reverse associations between PCOS and altered PUFA profiles. Female reproductive endocrine disorders are characterized by distinct endocrine disturbances, including hyperandrogenism and ovulatory dysfunction in PCOS, estrogen-dependent inflammatory activity in endometriosis, impaired follicular development in female infertility, cyclic ovarian steroid fluctuations in PMS, and estrogen–gonadotropin dysregulation in POI.44–46 These hormonal abnormalities may influence lipid metabolism, inflammatory mediator production, and circulating PUFA levels. Moreover, PCOS and other inflammatory reproductive disorders are closely linked to immune-inflammatory dysregulation, including altered interleukin and cytokine signaling, which may further connect endocrine disturbance with PUFA-related inflammatory metabolism.47–49
This study has several notable strengths. First, the use of both forward and reverse MR analyses minimizes biases from confounding and reverse causation, offering robust causal inferences. Second, the utilization of large-scale GWAS datasets provided comprehensive genetic coverage and statistical power, particularly for European populations. Third, extensive sensitivity analyses—including MR-Egger, weighted median, and MR-PRESSO—bolstered the credibility of our findings by addressing potential horizontal pleiotropy and weak instrument bias.
However, certain limitations should be acknowledged. The absence of individual-level data restricted our ability to perform more detailed analyses on the causal relationships between specific circulating PUFA traits and reproductive disorders. Because this study was based on publicly available GWAS summary-level data, we could not directly control the original inclusion and exclusion criteria of the recruited participants, such as disease severity, age distribution, or other cohort-specific clinical characteristics. Also, similar studies in non-European and multi-ethnic populations are warranted for the validation. Meanwhile, as this study was based on summary-level genetic data, the exploration of specific biological mechanisms underlying the observed associations could be interesting in the future. Finally, because our study was based on genetic data from individuals of European descent, the findings may not be generalizable to other ethnic groups, which could have differing genetic architectures and dietary patterns.
Overall, our findings have important implications for public health and clinical practice. The identification of elevated linoleic acid and total omega-6 levels as potential risk factors for endometriosis and infertility suggests that dietary interventions aimed at reducing omega-6 intake and promoting omega-3 consumption could be beneficial. Additionally, the protective association observed with a higher ratio of PUFAs to TFAs highlights the potential of maintaining a balanced PUFA profile to improve reproductive health. Future research should aim to validate these findings in more diverse populations and explore gene-diet interactions that may further influence these associations, as well as elucidate the underlying biological mechanisms through experimental studies.
Conclusion
In summary, our two-sample Mendelian randomization study provides genetic evidence supporting a potential causal association between circulating polyunsaturated fatty acid profiles and female reproductive endocrine disorders. Genetically predicted higher circulating linoleic acid and total omega-6 levels were associated with increased risks of endometriosis and female infertility, whereas a higher genetically predicted ratio of PUFAs to total fatty acids was associated with lower risks of these conditions and PCOS. Reverse MR analyses further suggested that PCOS may influence circulating lipid profiles, which may partly reflect altered endogenous lipid metabolism and inflammatory regulation. Therefore, our findings suggest that PUFA-related metabolic pathways may contribute to the pathophysiology of female reproductive endocrine disorders, while the potential benefits of dietary or therapeutic modulation of PUFA profiles require further validation in mechanistic studies, randomized trials, and diverse populations.
Abbreviations
CI, Confidence interval; DHA, Docosahexaenoic acid; GWAS, Genome-wide association study; IV, Instrumental variables; IVW, Inverse variance weighting; LD, Linkage disequilibrium; MR, Mendelian randomization; MR-PRESSO, Mendelian randomization-pleiotropy residual sum and outlier; OR, Odds ratio; PCOS, Polycystic ovary syndrome; POI, Premature ovarian insufficiency; PUFA, Polyunsaturated fatty acid; SNP, Single nucleotide polymorphism; TFA, Total fatty acids; WM, Weighted mean.
Data Sharing Statement
All data are available within the article and its supplementary materials.
Ethics Approval and Consent to Participate
Since this study exclusively utilized de-identified, publicly available summary-level data from GWAS database, and no individual-level data were involved, additional ethical approval was not required. The original studies have obtained approval from their respective ethics committees.This study is exempt from ethical review by the Institutional Review Board of the International Peace Maternity & Child Health Hospital based on national legislation guidelines, such as Article 32 of the Measures for Ethical Review of Research Involving Human Biological Sciences and Medical Research, China. This study was performed according to the principles expressed in the Declaration of Helsinki.
Consent for Publication
The FinnGen was approved by the Coordinating Ethics Committee of the Hospital District of Helsinki and Uusimaa (HUS/990/2017). Written informed consent was obtained from all participants before their participation in the survey.
Acknowledgments
Thanks for the support from the Medicine and Engineering Interdisciplinary Research Fund of Shanghai Jiao Tong University [YG2023QNB27] and Fundamental Research Funds for the Central Universities [YG2023QNA47]. All these funding bodies played no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by IPMCH (Grant No. YN201805) and the Fundamental Research Funds for the Central Universities [YG2023QNA47].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Selander-Han M, McGee S, Lo K. Female reproductive endocrine disorders. Prim Care. 2024;51(3):431–18. doi:10.1016/j.pop.2024.04.002
2. Zaks N, Batuure A, Lin E, et al. Association between mental health and reproductive system disorders in women: a systematic review and meta-analysis. JAMA Netw Open. 2023;6(4):e238685. doi:10.1001/jamanetworkopen.2023.8685
3. Darba J, Marsa A. Economic implications of endometriosis: a review. Pharmacoeconomics. 2022;40(12):1143–1158. doi:10.1007/s40273-022-01211-0
4. Zhu T, Cui J, Goodarzi MO. Polycystic ovary syndrome and risk of type 2 diabetes, coronary heart disease, and stroke. Diabetes. 2021;70(2):627–637. doi:10.2337/db20-0800
5. Schjenken JE, Green ES, Overduin TS, Mah CY, Russell DL, Robertson SA. Endocrine disruptor compounds-a cause of impaired immune tolerance driving inflammatory disorders of pregnancy? Front Endocrinol. 2021;12:607539. doi:10.3389/fendo.2021.607539
6. Popescu M, Feldman TB, Chitnis T. Interplay between endocrine disruptors and immunity: implications for diseases of autoreactive etiology. Front Pharmacol. 2021;12:626107.
7. Wang J, Yin T, Liu S. Dysregulation of immune response in PCOS organ system. Front Immunol. 2023;14:1169232. doi:10.3389/fimmu.2023.1169232
8. Szczuko M, Kikut J, Komorniak N, Bilicki J, Celewicz Z, Zietek M. The role of arachidonic and linoleic acid derivatives in pathological pregnancies and the human reproduction process. Int J Mol Sci. 2020;21(24):9628. doi:10.3390/ijms21249628
9. Pazderka CW, Oliver B, Murray M, Rawling T. Omega-3 polyunsaturated fatty acid derived lipid mediators and their application in drug discovery. Curr Med Chem. 2020;27(10):1670–1689. doi:10.2174/0929867325666180927100120
10. Murray M. Omega-3 polyunsaturated fatty acid derived lipid mediators: a comprehensive update on their application in anti-cancer drug discovery. Expert Opin Drug Discov. 2024;19(5):617–629. doi:10.1080/17460441.2024.2340493
11. Phelan N, O’Connor A, Kyaw Tun T, et al. Hormonal and metabolic effects of polyunsaturated fatty acids in young women with polycystic ovary syndrome: results from a cross-sectional analysis and a randomized, placebo-controlled, crossover trial. Am J Clin Nutr. 2011;93(3):652–662. doi:10.3945/ajcn.110.005538
12. Sienko A, Cichosz A, Urban A, Smolarczyk R, Czajkowski K, Sienko J. The effect of two anti-inflammatory dietary components, omega-3 and resveratrol, on endometriosis. Ginekol Pol. 2024;95(7):573–583. doi:10.5603/gpl.97573
13. Sampalis F, Bunea R, Pelland MF, Kowalski O, Duguet N, Dupuis S. Evaluation of the effects of Neptune Krill Oil on the management of premenstrual syndrome and dysmenorrhea. Altern Med Rev. 2003;8(2):171–179.
14. Rocha Filho EA, Lima JC, Pinho Neto JS, Montarroyos U. Essential fatty acids for premenstrual syndrome and their effect on prolactin and total cholesterol levels: a randomized, double blind, placebo-controlled study. Reprod Health. 2011;8:2. doi:10.1186/1742-4755-8-2
15. Houghton SC, Manson JE, Whitcomb BW, et al. Intake of dietary fat and fat subtypes and risk of premenstrual syndrome in the Nurses’ Health Study II. Br J Nutr. 2017;118(10):849–857. doi:10.1017/S0007114517002690
16. Ooi EMM, Ng TWK, Watts GF, Barrett PHR. Dietary fatty acids and lipoprotein metabolism: new insights and updates. Curr Opin Lipidol. 2013;24(3):192–197. doi:10.1097/MOL.0b013e3283613ba2
17. Sun Q, Ma J, Campos H, Hankinson SE, Hu FB. Comparison between plasma and erythrocyte fatty acid content as biomarkers of fatty acid intake in US women23. Am J Clin Nutr. 2007;86(1):74–81. doi:10.1093/ajcn/86.1.74
18. Schoeler M, Caesar R. Dietary lipids, gut microbiota and lipid metabolism. Rev Endocr Metab Disord. 2019;20(4):461–472. doi:10.1007/s11154-019-09512-0
19. Gonzalez-Soto M, Mutch DM. Diet regulation of long-chain pufa synthesis: role of macronutrients, micronutrients, and polyphenols on δ-5/δ-6 desaturases and elongases 2/5. Adv. Nutr. 2021;12(3):980–994. doi:10.1093/advances/nmaa142
20. Dyall SC, Balas L, Bazan NG, et al. Polyunsaturated fatty acids and fatty acid-derived lipid mediators: recent advances in the understanding of their biosynthesis, structures, and functions. Prog Lipid Res. 2022;86:101165
21. Chouinard-Watkins R, Conway V, Minihane AM, Jackson KG, Lovegrove JA, Plourde M. Interaction between BMI and APOE genotype is associated with changes in the plasma long-chain-PUFA response to a fish-oil supplement in healthy participants. Am J Clin Nutr. 2015;102(2):505–513. doi:10.3945/ajcn.114.103507
22. Schon SB, Cabre HE, Redman LM. The impact of obesity on reproductive health and metabolism in reprodu ctive-age females. Fertil Steril. 2024;122(2):194–203. doi:10.1016/j.fertnstert.2024.04.036
23. Zhang Y, Alzahrani M, Dambaeva S, Kwak-Kim J. Dyslipidemia and female reproductive failures: perspectives on lipid m etabolism and endometrial immune dysregulation. Semin Immunopathol. 2025;47(1):18. doi:10.1007/s00281-025-01043-y
24. Marklund M, Leander K, Vikstrom M, et al. Polyunsaturated fat intake estimated by circulating biomarkers and risk of cardiovascular disease and all-cause mortality in a population-based cohort of 60-year-old men and women. Circulation. 2015;132(7):586–594. doi:10.1161/CIRCULATIONAHA.115.015607
25. Lanier K, Wisseman B, Strom C, et al. Self-reported intake and circulating epa and dha concentrations in us pregnant women. Nutrients. 2023;15(7):1753. doi:10.3390/nu15071753
26. Taşkin E, Eroğlu S. Adiponectin gene polymorphisms rs1501299 and rs17300539 are not associated with polycystic ovary syndrome. Rev Assoc Med Bras. 2025;71(12):e20250864. doi:10.1590/1806-9282.20250864
27. Power GM, Sanderson E, Pagoni P, et al. Methodological approaches, challenges, and opportunities in the application of Mendelian randomisation to lifecourse epidemiology: a systematic literature review. Eur J Epidemiol. 2024;39(5):501–520. doi:10.1007/s10654-023-01032-1
28. Sanderson E, Glymour MM, Holmes MV, et al. Mendelian randomization. Nat Rev Meth Primers. 2022;2.
29. Lee K, Lim CY. Mendelian randomization analysis in observational epidemiology. J Lipid Atheroscler. 2019;8(2):67–77. doi:10.12997/jla.2019.8.2.67
30. De Leeuw C, Savage J, Bucur IG, Heskes T, Posthuma D. Understanding the assumptions underlying Mendelian randomization. Eur J Hum Genet. 2022;30(6):653–660. doi:10.1038/s41431-022-01038-5
31. Zeng H, Lin C, Wang S, Zheng Y, Gao X. Genetically predicted body composition in relation to cardiometabolic traits: a Mendelian randomization study. Eur J Epidemiol. 2021;36(11):1157–1168. doi:10.1007/s10654-021-00779-9
32. Kurki MI, Karjalainen J, Palta P, et al. FinnGen provides genetic insights from a well-phenotyped isolated population. Nature. 2023;613(7944):508–518. doi:10.1038/s41586-022-05473-8
33. Wang Y, Gao L, Lang W, et al. Serum calcium levels and parkinson’s disease: a mendelian randomization study. Front Genet. 2020;11:824. doi:10.3389/fgene.2020.00824
34. Burgess S, Thompson SG. Bias in causal estimates from Mendelian randomization studies with weak instruments. Stat Med. 2011;30(11):1312–1323. doi:10.1002/sim.4197
35. Wathes DC, Abayasekara DRE, Aitken RJ. Polyunsaturated fatty acids in male and female reproduction. Biol Reprod. 2007;77(2):190–201. doi:10.1095/biolreprod.107.060558
36. Innes JK, Calder PC. Omega-6 fatty acids and inflammation. Prostaglandins Leukot Essent Fatty Acids. 2018;132:41–48. doi:10.1016/j.plefa.2018.03.004
37. Lai -Z-Z, Yang H-L, Ha S-Y, et al. Cyclooxygenase-2 in Endometriosis. Int J Biol Sci. 2019;15(13):2783–2797. doi:10.7150/ijbs.35128
38. Kwon Y. Immuno‐resolving ability of resolvins, protectins, and maresins derived from omega‐3 fatty acids in metabolic syndrome. Mol Nutr Food Res. 2019;64(4).
39. Jeong HY, Moon YS, Cho KK. ω-6 and ω-3 polyunsaturated fatty acids: inflammation, obesity and foods of animal resources. Food Sci. Anim. Resour. 2024;44(5):988–1010. doi:10.5851/kosfa.2024.e65
40. Tian Y, Zhang W, Zhao S, et al. FADS1-FADS2 gene cluster confers risk to polycystic ovary syndrome. Sci Rep. 2016;6:21195. doi:10.1038/srep21195
41. Brown KM, Sharma S, Baker E, Hawkins W, van der Merwe M, Puppa MJ. Delta-6-desaturase (FADS2) inhibition and omega-3 fatty acids in skeletal muscle protein turnover. Biochem Biophys Rep. 2019;18:100622. doi:10.1016/j.bbrep.2019.100622
42. Banaszak M, Górna I, Drzymała-Czyż S. Fatty acid profile and desaturase activity in obesity: roles, mechanisms, and clinical relevance. Metabolites. 2025;15(9):595. doi:10.3390/metabo15090595
43. Mumford SL, Browne RW, Kim K, et al. Preconception plasma phospholipid fatty acids and fecundability. J Clin Endocrinol Metab. 2018;103(12):4501–4510. doi:10.1210/jc.2018-00448
44. Velez LM, Seldin M, Motta AB. Inflammation and reproductive function in women with polycystic ovary syndrome†. Biol Reprod. 2021;104(6):1205–1217. doi:10.1093/biolre/ioab050
45. Zondervan KT, Becker CM, Koga K, Missmer SA, Taylor RN, Viganò P. Endometriosis. Nat Rev Dis Primers. 2018;4(1):9. doi:10.1038/s41572-018-0008-5
46. Huang Y, Liu Z, Geng Y, et al. The risk factors, pathogenesis and treatment of premature ovarian insufficiency. Jovarian Res. 2025;18(1):134. doi:10.1186/s13048-025-01714-2
47. Oală IE, Mitranovici MI, Chiorean DM, et al. Endometriosis and the role of pro-inflammatory and anti-inflammatory cytokines in pathophysiology: a narrative review of the literature. Diagnostics. 2024;14:3. doi:10.3390/diagnostics14030312
48. Granda D, Szmidt MK, Kaluza J. Is premenstrual syndrome associated with inflammation, oxidative stress and antioxidant status? a systematic review of case–control and cross-sectional studies. Antioxidants. 2021;10(4):604. doi:10.3390/antiox10040604
49. Regidor P-A, Mueller A, Sailer M, Gonzalez Santos F, Rizo JM, Moreno Egea F. Chronic Inflammation in PCOS: the Potential Benefits of Specialized Pro-Resolving Lipid Mediators (SPMs) in the Improvement of the Resolutive Response. Int J Mol Sci. 2021;22(1):384. doi:10.3390/ijms22010384
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Plasma and Peritoneal Fluid Annexin A2 Levels in Patients with Endometriosis
Zygarowicz M, Kacperczyk-Bartnik J, Sierdzinski J, Wojtyla C, Pierzynski P, Manka G, Kiecka M, Spaczynski RZ, Piekarski P, Banaszewska B, Jakimiuk A, Issat T, Rokita W, Mlodawski J, Szubert M, Sieroszewski P, Raba G, Szczupak K, Kluz T, Kluza M, Lipa M, Warzecha D, Wielgos M, Koc-Zorawska E, Zorawski M, Laudanski P
Journal of Inflammation Research 2023, 16:5959-5969
Published Date: 7 December 2023
The Improved-EFI Score: A Multi-Omics-Based Novel Efficacy Predictive Tool for Predicting the Natural Fertility of Endometriosis Patients
He Q, Zhang C, Hu Y, Deng J, Zhang S
International Journal of General Medicine 2025, 18:881-895
Published Date: 19 February 2025
A Mendelian Randomization Study of the Association Between Polycystic Ovary Syndrome and Serum Urea Levels
Wang T, Qi Z, Zhao S, Lian F
International Journal of Women's Health 2025, 17:1807-1814
Published Date: 17 June 2025
Global Burden of Polycystic Ovary Syndrome: A Systematic Analysis of Pre- and Post-Pandemic Trends from the 2021 Global Burden of Disease Study (1990–2021)
Guo Y, Du Y, Zhang L, Xu H, Liu J, Li S, Xu Z, Yan J, Chen J, Wang H
International Journal of Women's Health 2026, 18:583951
Published Date: 31 March 2026
The Impact of Endometriosis on Ovarian Reserve: A Systematic Review
Christina NLL, Tjahyadi D, Anwar R, Rachmawati A, Rafi MA
International Journal of Women's Health 2026, 18:604715
Published Date: 26 May 2026