Back to Journals » Journal of Pain Research » Volume 16
Bibliometric Analysis of Research Studies on Postoperative Pain Management of Cesarean Section
Authors Zhai W ![]() , Liu H, Yu Z, Jiang Y, Yang J, Li M
, Liu H, Yu Z, Jiang Y, Yang J, Li M ![]()
Received 24 January 2023
Accepted for publication 15 April 2023
Published 21 April 2023 Volume 2023:16 Pages 1345—1353
DOI https://doi.org/10.2147/JPR.S404659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Wenwen Zhai,* Huili Liu,* Zhuoying Yu, Ye Jiang, Jing Yang, Min Li
Department of Anesthesiology, Peking University Third Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Li, Department of Anesthesiology, Peking University Third Hospital, No. 49 North Garden Road, Haidian District, Beijing, 100191, People’s Republic of China, Tel +86 13522757239, Email [email protected]
Purpose: Cesarean section (C-section) is associated with moderate-to-severe postoperative pain. Many studies on pain management after C-section have been published in recent decades, many of which focused on new regional techniques. The purpose of this study is to outline the connections within the dynamic evolution of postcesarean delivery analgesia research publications using retrospective bibliometric analysis.
Patients and Methods: Published studies on postoperative pain management of C-section were retrieved from the Science Citation Index Expanded (SCI-E) of Web of Science (WOS) Core collection database. All papers published from 1978 to October 22, 2022 were searched. The research progress and growing trend were quantitatively analyzed by total publications, research institutions, journal impact factors, and author’s contribution. Total citations frequency, average citations per item and h-index were used for evaluating literature quantity. Top 20 journals with the highest number of publications were charted. The keywords co-occurrence overlay map was visualized by the VOSviewer software.
Results: From 1978 to 2022, a total of 1032 articles in postcesarean delivery analgesia research field were published, with 23,813 times cited, average citations of 23.07 per item, and an h-index of 68. The most high-yield publication year, countries, journals, authors, institutions were 2020 (n=79), the United States (n=288), Anesthesia and Analgesia (n=108), Carvalho B (n=25), and Stanford University (n=33), respectively. The United States had the most cited papers. The future research interest might be “prescription”, “quadratus lumborum block”, “postnatal depression”, “persistent pain”, “dexmedetomidine”, “enhanced recovery”, and “multimodal analgesia”.
Conclusion: By employing the online bibliometric tool and VOSviewer software, we found that studies on postcesarean analgesia had grown markedly. The focus had evolved to nerve block, postnatal depression, persistent pain, and enhanced recovery.
Keywords: postcesarean section, analgesia, bibliometric analysis, keywords analysis
Introduction
The rate of Cesarean section (C-section) has been increasing over the past decades and now exceeds 32% of births.1 C-section can cause moderate-to-severe postoperative pain in a large percentage of women.2 Poor management of acute postoperative pain can be associated with chronic postoperative pain,3 increased opioids use, delayed functional recovery, and an increase in postpartum depression.4,5 On the contrary, well-controlled postcesarean pain may improve a woman’s ability to function and mother‐child bonding.6 Previously, commonly used modalities included systemic administration of opioids, such as intramuscular injection, patient-controlled intravenous analgesia (PCIA), and neuraxial injection during regional anesthesia.6 Recent studies have focused on an opioid-saving and multimodal analgesic strategy.7,8 A number of new regional anesthesia techniques, such as transversus abdominis plane (TAP) block7 and the quadratus lumborum block,8 along with the non‐pharmacological approaches,9 have been developed. Therefore, we sought to examine the status of the research on pain interventions for C-section and to identify the popular areas and the frontiers of research on pain management after C-section. Since bibliometric analysis is a scientific method for summarizing and synthesizing literature, we aim to perform a bibliometric analysis of the reports on postcesarean delivery analgesia to find out the achievements and the development directions in this field.
Materials and Methods
Data Sources and Search Strategies
The literature data were retrieved from the Science Citation Index Expanded (SCI-E) of Web of Science (WOS) Core collection database, which was widely applied in bibliometric research using an advanced search strategy. The search query was “TS = (“cesarean section” OR “cesarean delivery” OR “cesarean” OR “C-section” OR “caesarean” OR “caesarean section” OR “caesarean delivery”) AND TS = (“postoperative” OR “postoperative periods” OR “postcesarean” OR “post cesarean” OR “postcesarean” OR “after cesarean” OR “post caesarean” OR “post-caesarean” OR “postcaesarean” OR “after caesarean”) AND TS = (“pain” OR “pain management” OR “analgesia” OR “analgesic” OR “pain control”) AND LA = (English) AND DT = (Article).” After the primary data search, two researchers screened all the manuscripts individually to confirm their relevance. The eligible study had to focus on postcesarean analgesia, and irrelevant studies were discarded. Full records of all articles were searched on October 22, 2022.
1696 publications met the inclusion criteria. Finally, 1032 articles were further assessed. The screening process is shown in Figure 1.
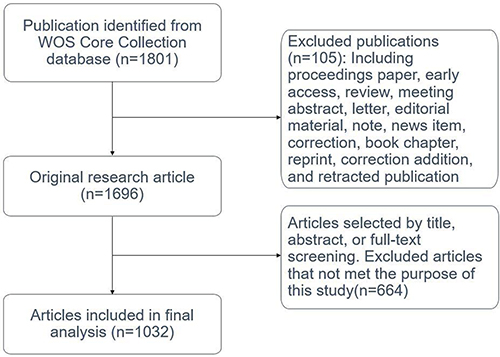 |
Figure 1 Flowchart of the methodology. |
Bibliometric Analysis
The following bibliometric information were collected including publication year, country of origin, institutional affiliations, keywords, source journal, impact factor (IF) of the journal, citation count, and authorship. No exclusion criteria were applied. The author’s keywords co-occurrence overlay map was implemented by VOSviewer, setting the minimum occurrences of a keyword to 10 times.
Results
Publications by Year
In total, 1032 articles in postcesarean analgesia research field were retrieved from the SCI-E of WOS Core Collection database from 1978 to October 22 2022, with 23,813 times cited, average citations of 23.07 per item, and an h-index of 68. As shown in Figure 2, the first article was published in 1978, and the year with the most publications (n=79) was 2020. The studies published in 2021 had the highest number of total citations (n=2522), and 2021 also had the highest average number of citations per paper (n=38).
 |
Figure 2 The annual publications and sum of times cited per year on postcesarean section analgesia. |
Top Countries
The retrieved papers were published in 58 different countries, and the top 20 countries accounted for over 80% of the total number of articles. As shown in Table 1 and Figure 3A, the United States published the largest number of articles, with 288 (16.7%), followed by China (109, 10.56%) and Turkey (85, 8.24%). The leading country by h-index was the United States (48) followed by England (29) and Canada (26). Canada had the highest average citations per article (38.16), followed by England (32.14) and Australia (31.60). As shown in Figure 3B, over the past 10 years, the number of total publications from the United States, China, Egypt, and Israel increased significantly.
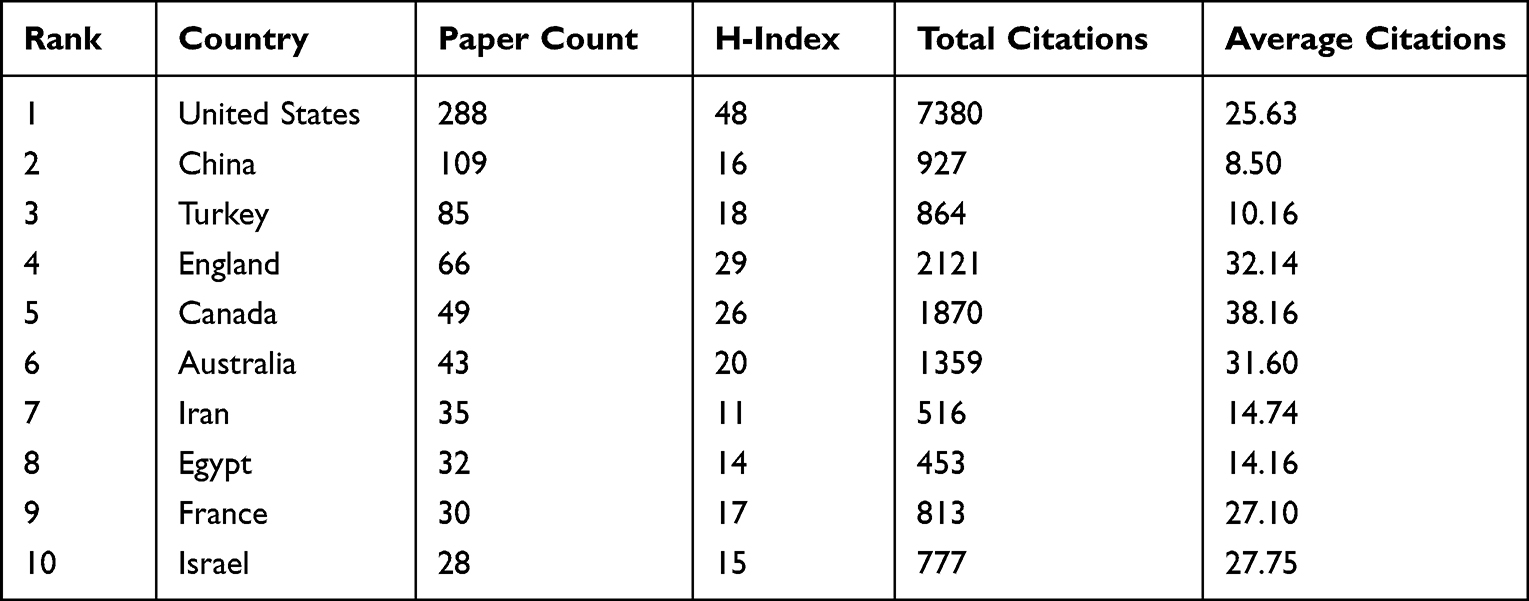 |
Table 1 Top 10 High-Yield Countries with h-Index, Total Citations, and Average Citations per Article |
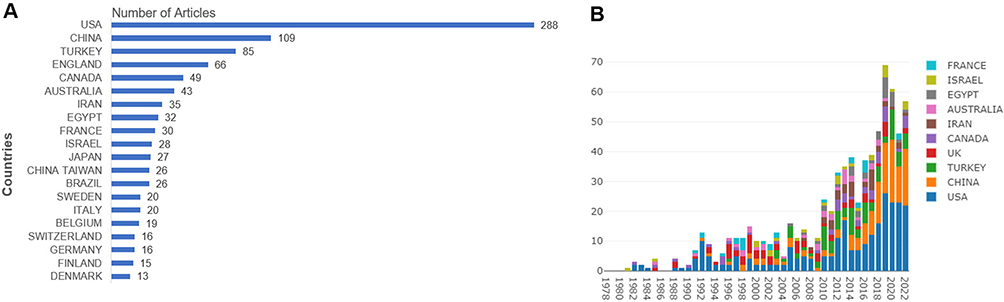 |
Figure 3 (A) Top 20 countries with the most publications on postcesarean delivery analgesia. (B) The distribution of the bibliographic records per year of the top 10 countries on postcesarean delivery analgesia. |
Leading Institutions
As shown in Table 2, among the 10 most prolific institutions, 6 came from the United States: Stanford University (n=33, 3.20%), Harvard University (n=28, 2.71%), Harvard Medical School (n=20, 1.945), Duke University (n=19, 1.84%), Brigham, and Women’s Hospital (n=18, 1.74%) and Wake Forest University (n=17, 1.65%). Other most productive institutions included Egyptian Knowledge Bank, University of Toronto, University Toronto Affiliates, and University of Western Australia.
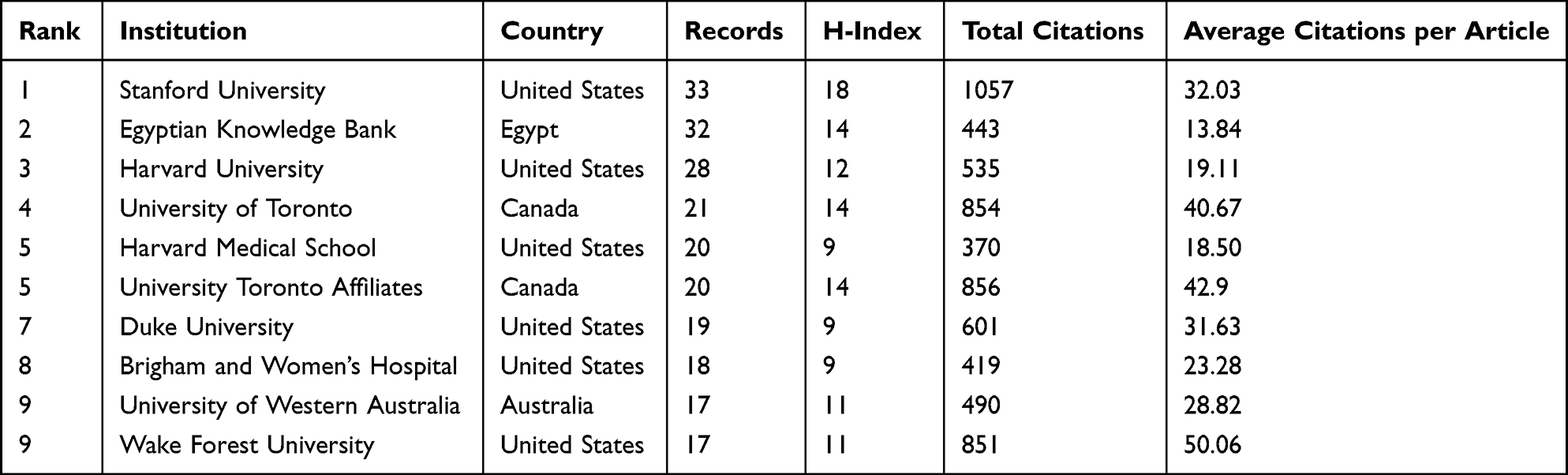 |
Table 2 The Top 10 High-Yield Institutions on Postcesarean Section Analgesia with h-Index, Total Citations, and Average Citations per Article |
Prominent Journals
Table 3 lists the top 10 journals ranked by the number of publications on postcesarean section analgesia. Nine of the top 10 journals were anesthesiology journals. The top three journals that published the greatest number of studies were Anesthesia and Analgesia (n=108, 10.47%), International Journal of Obstetric Anesthesia (n=81, 7.85%), and British Journal of Anaesthesia (n=42, 4.07%). The IFs of these 10 journals in 2022 ranged from 2.274 to 12.893.
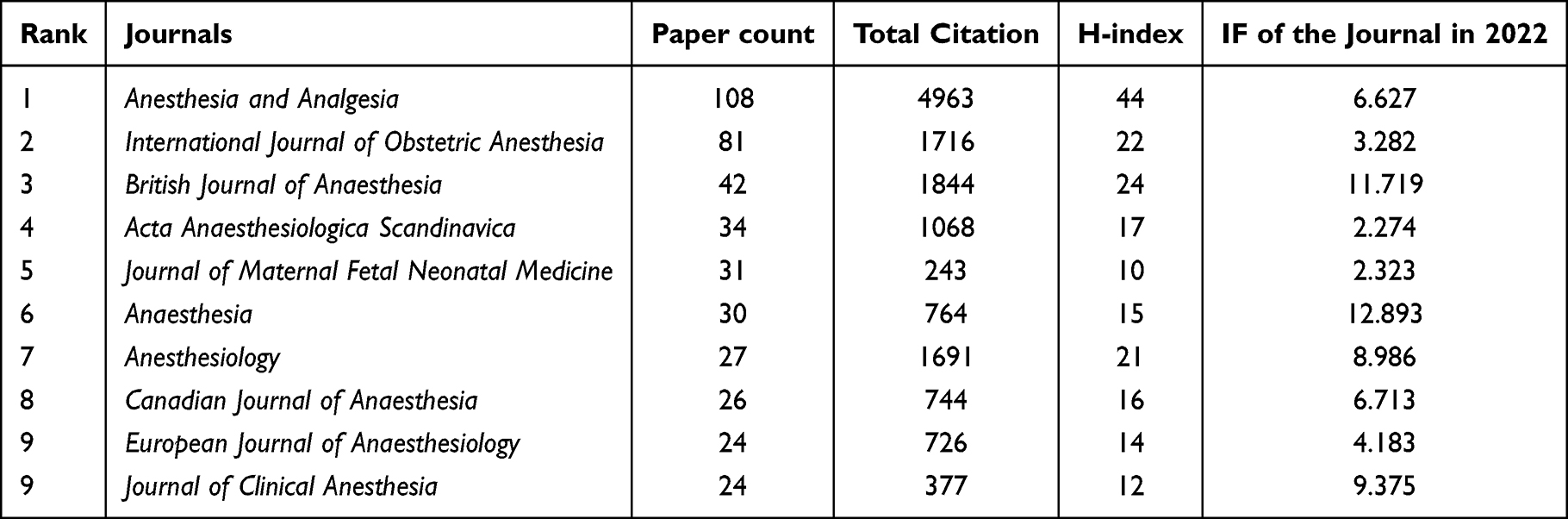 |
Table 3 Top 10 Journals for the Most Publications on Postcesarean Analgesia |
Highly Cited Papers
The 20 top-cited articles are listed in Table 4. The number of total citations for these 20 papers ranged from 122 to 381, and 13 of these papers were published in Anesthesia and Analgesia, Anesthesiology, British Journal of Anaesthesia, and Regional Anesthesia and Pain Medicine. Among the 20 top-cited studies, the most common article types were clinical trials (n=16); followed by systematic reviews or meta-analyses (n=3) and narrative reviews (n=1).
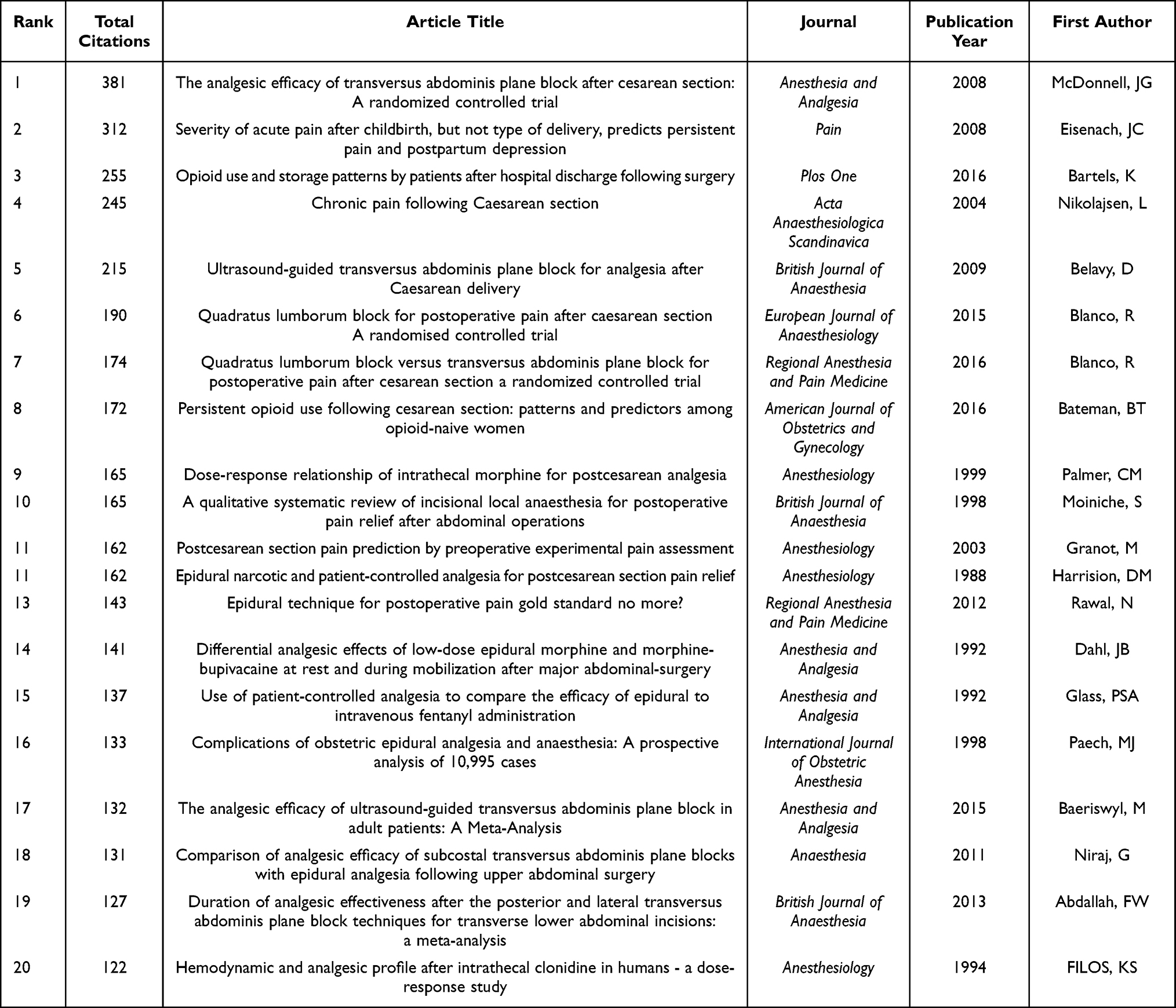 |
Table 4 Top 20 Most Cited Articles on Postcesarean Analgesia |
Co-Occurring Keywords
Terms with at least 10 occurrences in the titles and abstracts of the articles were defined as keywords, resulting in 137 extractions. The co-occurrence of these 137 terms was analyzed using the VOS viewer (Figure 4A). Among all the retrieved studies, the highest occurrence keywords were “cesarean section” with 627 occurrences (total link strength = 3426), followed by “postoperative pain” with 250 occurrences (total link strength = 1408), “analgesia” with 242 occurrences (total link strength = 1478), “morphine” with 215 occurrences (total link strength = 1455) and “pain” with 214 occurrences (total link strength = 1249).
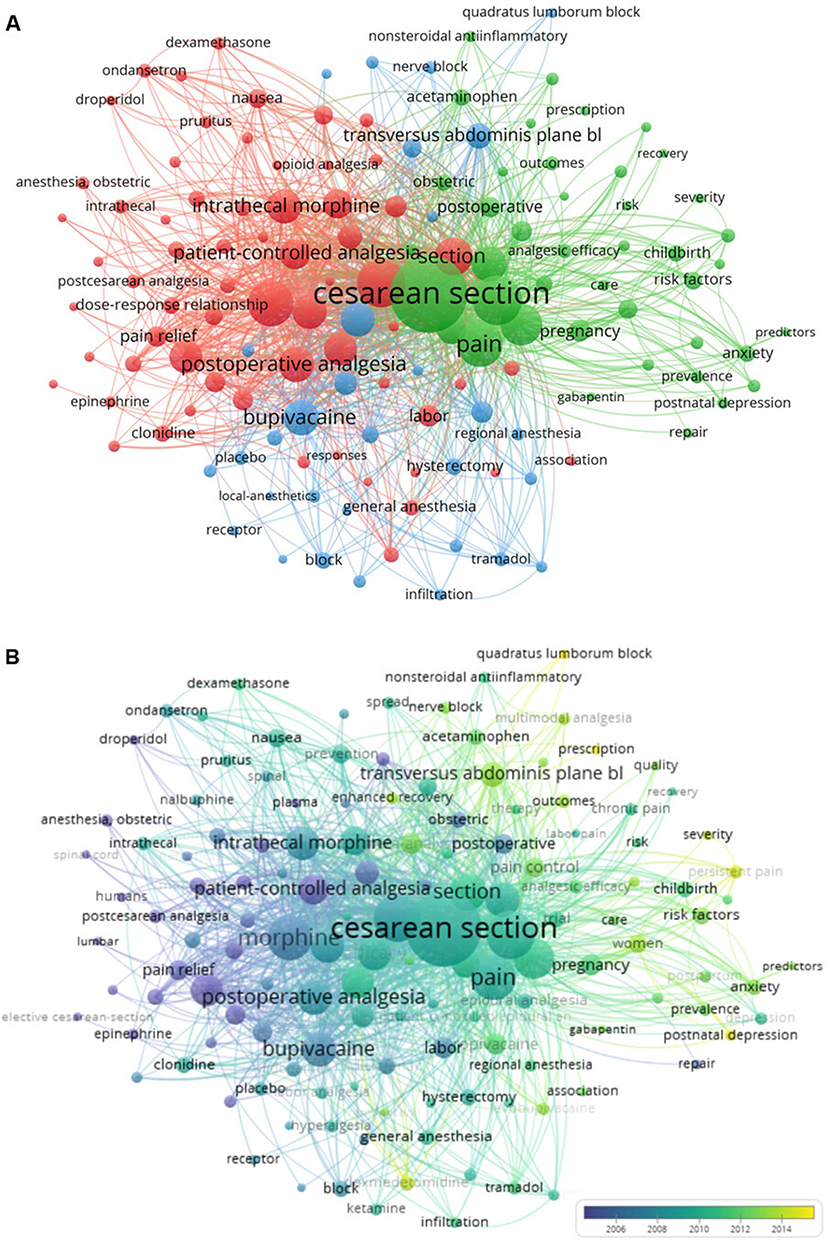 |
Figure 4 Co-occurrence analysis of 137 keywords. Each circle indicates a keyword. Items with bigger size represent more citation counts and smaller ones represent fewer citation counts. The closer distance between the two keywords represents the stronger co-occurrence. (A) Mapping of keywords in research of post cesarean pain management; 137 keywords are divided into 3 clusters. (B) Overlaid visualization map by average publication year, with violet representing earlier year and yellow representing recent year. |
The keywords were classified into three clusters, indicating that studies on postcesarean section analgesia can be categorized into three main categories: “analgesia” (cluster 1, green), “postoperative pain” (cluster 2, blue), and “nerve block” (cluster 3, red). A total of 64 items were included in the “analgesia” cluster, 42 items were included in the “postoperative pain” cluster and 31 items were included in the “nerve block” cluster.
Figure 4B shows the same co-occurrence map overlaid with different colors depending on the average publication year of the keyword, with purple representing earlier publication and yellow representing more recent publication. Overall, “prescription”, “quadratus lumborum block”, “postnatal depression”, “persistent pain”, “dexmedetomidine”, “enhanced recovery”, and “multimodal analgesia” were the latest research trends.
Discussion
This study showed that scientific research outputs involving postcesarean section pain control had significantly increased over the past years. The United States was the leading country for publications within this field. “Cesarean section”, “postoperative pain”, “analgesia”, “morphine”, and “pain” were the top five highest occurrence keywords. Moreover, “prescription”, “quadratus lumborum block”, “postnatal depression”, “persistent pain”, “dexmedetomidine”, “enhanced recovery”, and “multimodal analgesia” were the latest research trends.
The popularity of a specific topic is associated with the number of publications. The general trend for publication was upwards as shown in Figure 2. From 1978 to 1990, the average number of publications per year was less than 10. From 1991 to 2009, the number rose to around 20. There was a remarkable increase since 2012, reaching a peak of 79 in 2020. The increase in citations over the past few years also pointed to a heightened concern in this regard.
Of the top 20 most cited studies, 13 articles focused on regional anesthesia, including neuraxial techniques (n=7)10–16 (with or without morphine, fentanyl, and clonidine), incisional local anesthesia (n=1),17 and nerve blocks such as TAP block (n=6)7,18–22 and quadratus lumborum block (n=2).8,20 Low-dose intrathecal morphine was popular for postcesarean section analgesia,23 however, over the last decade, the studies had focused on reducing opioid dosage by regional block.7,8,18–22 The most-cited article entitled, “The analgesic efficacy of transversus abdominis plane block after C-section: A randomized controlled trial”, was a randomized controlled trial on TAP block.18 Of the 20 most-cited articles, two were written by Blanco, R. as first author,8,20 both focused on implementing the newly developed technologies of the regional block.
The second most frequently cited paper by Eisenach et al with 312 citations in 2008, entitled “Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression”,24 was a cohort study focusing on the relationship between postoperative acute pain and persistent pain. Since persistent pain after C-section was common25,26 and difficult to manage,27 it was crucial to identify its risk factors. In addition to postoperative acute pain, other factors such as types of anesthesia,25 history of smoking,28 preoperative anxiety, and previous persistent pain were also suggested as predictors of chronic postoperative pain after C-section.26,29
Through a co-occurrence analysis of the keywords, we discovered three major categories: analgesia, postoperative pain, and nerve block, which were the three main research directions of analgesia after C-section. In the analgesia category, we identified the terms of the most commonly used medications and methods, including “morphine”, “intrathecal morphine”, “fentanyl”, “patient-controlled analgesia”, and “opioid”. Words related to the opioid complications and their treatments, such as “nausea and vomiting”, “respiratory depression”, “pruritus”, and “ondansetron” were also included in this category. Within the category “postoperative pain”, terms such as “persistent pain”, “acute pain”, “chronic pain”, “postnatal depression”, and “risk factors” were included. This category showed a trend towards more recent studies, to be precise, 21 items in this category were after 2015, while the remaining categories had only 5 and 4, respectively. It was indicated that the research area of “postoperative pain” was currently focused on and might be the probable direction of future research. Poorly controlled postoperative pain after C-section could increase the risk of long-lasting morbidity, including chronic pain and postpartum depression.24,30 Pain and depression were complex, and future studies should investigate the relationship between them.31 In the “nerve block” category, “transversus abdominis plane block”, “wound infiltration”, “regional anesthesia”, “quadratus lumborum block” were included, as well as “double-blind” and “randomized controlled-trial”, indicating that the studies in this category might have a relatively high level of evidence.
The most recent keywords were “prescription”, “quadratus lumborum block”, “postnatal depression”, “persistent pain”, “dexmedetomidine”, “enhanced recovery”, and “multimodal analgesia”. Later, publication years were associated with lower average citation counts, and nearly all of the 10 most recent keywords had an average citation below 20, with the exception of the keyword of “enhanced recovery” (average citations, 31). Enhanced Recovery After Surgery (ERAS) has been a hot topic in a wide range of surgical procedures, including C-section in recent years.32,33
There were still some limitations of the present study. First, we only used the core collection of WOS to search literature. The more databases we use, the more information we could get and analyze. Other databases such as Scopus and MEDLINE could be considered in the future study. But WOS was the most commonly used database in scientometrics, and most bibliometric softwares could identify the format from WOS. Second, the main language of WOS was English. Articles written in other languages were excluded. Third, the more recent articles have fewer citations than the relatively older ones, and this suggested the possible weakness of bibliometric analysis in the field of innovation.
Conclusion
In this study, we searched and analyzed the literature information regarding countries, organizations, journals, high-cited papers and analyzed the thematic development and future area of interest. Our research observed the raising concern on postcesarean pain control in recent years. The future research domain might be “prescription”, “quadratus lumborum block”, “postnatal depression”, “persistent pain”, “dexmedetomidine”, “enhanced recovery”,; and “multimodal analgesia.”.
Abbreviations
C-section, Cesarean section; SCI-E, Science Citation Index Expanded; WOS, Web of Science; PCIA, patient-controlled intravenous analgesia; TAP, transversus abdominis plane; IF, impact factor; ERAS, Enhanced Recovery After Surgery.
Data Sharing Statement
The raw data can be directly obtained from the WOS Core Collection database.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Betran AP, Ye J, Moller AB, et al. Trends and projections of caesarean section rates: global and regional estimates. BMJ Glob Health. 2021;6(6):e005671. doi:10.1136/bmjgh-2021-005671
2. Granot M, Yarnitsky D, Tamir A, et al. Postcesarean section pain prediction by preoperative experimental pain assessment. Anesthesiology. 2003;98:1422–1426. doi:10.1097/00000542-200306000-00018
3. Komatsu R, Ando K, Flood PD. Factors associated with persistent pain after childbirth: a narrative review. Br J Anaesth. 2020;124(3):e117–e130. doi:10.1016/j.bja.2019.12.037
4. Sutton CD, Carvalho B. Optimal pain management after cesarean delivery. Anesthesiol Clin. 2017;35:107–124. doi:10.1016/j.anclin.2016.09.010
5. Shen D, Hasegawa-Moriyama M, Ishida K, et al. Acute postoperative pain is correlated with the early onset of postpartum depression after cesarean section: a retrospective cohort study. J Anesth. 2020;34:607–612. doi:10.1007/s00540-020-02789-5
6. Gadsden J, Hart S, Santos AC. Post-cesarean delivery analgesia. Anesth Analg. 2005;101(5S):S62–S69. doi:10.1213/01.ANE.0000177100.08599.C8
7. Baeriswyl M, Kirkham KR, Kern C, et al. The analgesic efficacy of ultrasound-guided transversus abdominis plane block in adult patients. Anesth Analg. 2015;121(6):1640–1654. doi:10.1213/ANE.0000000000000967
8. Blanco R, Ansari T, Girgis E. Quadratus lumborum block for postoperative pain after caesarean section: a randomised controlled trial. Eur J Anaesthesiol. 2015;32(11):812–818. doi:10.1097/EJA.0000000000000299
9. Zimpel SA, Torloni MR, Porfirio GJ, et al. Complementary and alternative therapies for post-caesarean pain. Cochrane Database Syst Rev. 2020;9:CD011216.
10. Palmer C, Emerson S, Volgoropolous D, et al. Dose-response relationship of intrathecal morphine for postcesarean analgesia. Anesthesiology. 1999;90(2):437–444. doi:10.1097/00000542-199902000-00018
11. Harrision DM, Sinatra R, Morgese L, et al. Epidural narcotic and patient-controlled analgesia for post-cesarean section pain relief. Anesthesiology. 1988;68(3):454–457. doi:10.1097/00000542-198803000-00025
12. Rawal N. Epidural technique for postoperative pain: gold standard no more? Reg Anesth Pain Med. 2012;37:310–317. doi:10.1097/AAP.0b013e31825735c6
13. Dahl JB, Rosenberg J, Hansen BL, et al. Differential analgesic effects of low-dose epidural morphine and morphine-bupivacaine at rest and during mobilization after major abdominal surgery. Anesth Analg. 1992;74(3):362–365. doi:10.1213/00000539-199203000-00008
14. Glass PS, Estok P, Ginsberg B, et al. Use of patient-controlled analgesia to compare the efficacy of epidural to intravenous fentanyl administration. Anesth Analg. 1992;74:345–351. doi:10.1213/00000539-199203000-00005
15. Paech MJ, Godkin R, Webster S. Complications of obstetric epidural analgesia and anaesthesia: a prospective analysis of 10 995 cases. Int J Obstet Anesth. 1998;7:5–11. doi:10.1016/S0959-289X(98)80021-6
16. Filos KS, Goudas LC, Patroni O, Polyzou V. Hemodynamic and analgesic profile after intrathecal clonidine in humans - a dose-response study. Anesthesiology. 1994;81:591–601. doi:10.1097/00000542-199409000-00011
17. Moiniche S, Mikkelsen S, Wetterslev J, et al. A qualitative systematic review of incisional local anaesthesia for postoperative pain relief after abdominal operations. Br J Anaesth. 1998;81(3):377–383. doi:10.1093/bja/81.3.377
18. McDonnell JG, Curley G, Carney J, et al. The analgesic efficacy of transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg. 2008;106:186–191. doi:10.1213/01.ane.0000290294.64090.f3
19. Belavy D, Cowlishaw PJ, Howes M, et al. Ultrasound-guided transversus abdominis plane block for analgesia after Caesarean delivery. Br J Anaesth. 2009;103(5):726–730. doi:10.1093/bja/aep235
20. Blanco R, Ansari T, Riad W, et al. Quadratus lumborum block versus transversus abdominis plane block for postoperative pain after cesarean delivery: a randomized controlled trial. Reg Anesth Pain Med. 2016;41(6):757–762. doi:10.1097/AAP.0000000000000495
21. Niraj G, Kelkar A, Jeyapalan I, et al. Comparison of analgesic efficacy of subcostal transversus abdominis plane blocks with epidural analgesia following upper abdominal surgery. Anaesthesia. 2011;66:465–471. doi:10.1111/j.1365-2044.2011.06700.x
22. Abdallah FW, Laffey JG, Halpern SH, et al. Duration of analgesic effectiveness after the posterior and lateral transversus abdominis plane block techniques for transverse lower abdominal incisions: a meta-analysis. Br J Anaesth. 2013;111(5):721–735. doi:10.1093/bja/aet214
23. Dahl JB, Jeppesen IS, Jorgensen H, et al. Intraoperative and postoperative analgesic efficacy and adverse effects of intrathecal opioids in patients undergoing cesarean section with spinal anesthesia: a qualitative and quantitative systematic review of randomized controlled trials. Anesthesiology. 1999;91(6):1919–1927. doi:10.1097/00000542-199912000-00045
24. Eisenach JC, Pan PH, Smiley R, et al. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94. doi:10.1016/j.pain.2008.07.011
25. Weibel S, Neubert K, Jelting Y, et al. Incidence and severity of chronic pain after caesarean section: a systematic review with meta-analysis. Eur J Anaesthesiol. 2016;33(11):853–865. doi:10.1097/EJA.0000000000000535
26. Nikolajsen L, Sorensen HC, Jensen TS, et al. Chronic pain following Caesarean section. Acta Anaesthesiol Scand. 2004;48(1):111–116. doi:10.1111/j.1399-6576.2004.00271.x
27. Richebe P, Capdevila X, Rivat C. Persistent postsurgical pain: pathophysiology and preventative pharmacologic considerations. Anesthesiology. 2018;129(3):590–607. doi:10.1097/ALN.0000000000002238
28. Borges NC, de Deus JM, Guimaraes RA, et al. The incidence of chronic pain following Cesarean section and associated risk factors: a cohort of women followed up for three months. PLoS One. 2020;15(9):e0238634. doi:10.1371/journal.pone.0238634
29. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625. doi:10.1016/S0140-6736(06)68700-X
30. Kainu JP, Halmesmaki E, Korttila KT, et al. Persistent pain after cesarean delivery and vaginal delivery: a prospective cohort study. Anesth Analg. 2016;123(6):1535–1545. doi:10.1213/ANE.0000000000001619
31. Lim G, Levine MD, Mascha EJ, et al. Labor pain, analgesia, and postpartum depression: are we asking the right questions? Anesth Analg. 2020;130(3):610–614. doi:10.1213/ANE.0000000000004581
32. Huang J, Cao C, Nelson G, et al. A review of enhanced recovery after surgery principles used for scheduled caesarean delivery. J Obstet Gynaecol Can. 2019;41(12):1775–1788. doi:10.1016/j.jogc.2018.05.043
33. Macones GA, Caughey AB, Wood SL, et al. Guidelines for postoperative care in cesarean delivery: Enhanced Recovery After Surgery (ERAS) Society recommendations (part 3). Am J Obstet Gynecol. 2019;221(3):247.e1–247.e9. doi:10.1016/j.ajog.2019.04.012
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bibliometric Analysis of Functional Magnetic Resonance Imaging Studies on Manual Therapy Analgesia from 2002–2022
Zhou XC, Huang YB, Liu Z, Wu HJ, Huang HZ, Tian Y, Hong SW, Hu HJ, Lv LJ, Lv ZZ
Journal of Pain Research 2023, 16:2115-2129
Published Date: 19 June 2023
Bibliometric Analysis of Research on Temporomandibular Joint and Occlusion from 2000 to 2022
Xiong X, Gao X, Zhong J, Hu S, Li Y, Zheng Y, Liu Y
Journal of Pain Research 2023, 16:2847-2860
Published Date: 16 August 2023