Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Beyond The Age Limit: A Comparative Study (<70 Vs ≥70 Years) in Breast Cancer Characteristics and Surgical Management in Women
Authors Buyukasik S ![]() , Kankaya B, Altundal YE
, Kankaya B, Altundal YE ![]() , Ozgul M, Kapan S
, Ozgul M, Kapan S
Received 7 August 2025
Accepted for publication 6 December 2025
Published 12 December 2025 Volume 2025:17 Pages 1231—1246
DOI https://doi.org/10.2147/BCTT.S555684
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Suleyman Buyukasik,1 Burak Kankaya,1 Yusuf Emre Altundal,1 Mustafa Ozgul,2 Selin Kapan1
1Department of General Surgery, Faculty of Medicine, Istanbul Aydin University, Istanbul, Turkey; 2Department of Ophthalmology, Gavin Herbert Eye Institute, University of California Irvine, Irvine, CA, USA
Correspondence: Suleyman Buyukasik, Department of General Surgery, Istanbul Aydin University Faculty of Medicine, Besyol Mah, Akasya Sok. No: 4, Kucukcekmece, Istanbul, 34295, Turkiye, Email [email protected]
Purpose: This study aimed to evaluate differences in tumor characteristics, molecular subtypes, and surgical approaches between elderly (≥ 70 years) and younger (< 70 years) breast cancer patients.
Patients and Methods: This retrospective, single-center study analyzed 120 breast cancer patients (99 younger, 21 elderly) treated surgically between 2020 and 2025 at Istanbul Aydın University, Turkey. Tumor characteristics and surgical management related data were analyzed to compare two age groups. Statistical analyses included t-tests, chi-square tests, and Fisher’s exact tests.
Results: Elderly patients presented with significantly larger tumors (3.91± 0.56 vs 2.81± 0.35 cm, p< 0.05), higher T4 disease prevalence (19.05% vs 3.37%, p< 0.05), and greater metastatic burden (7.90± 6.06 vs 3.54± 4.49 metastases, p< 0.05). SLNB was performed significantly more frequently in younger patients (90.9%) compared to elderly patients (71.4%, p < 0.05). Elderly patients underwent axillary dissection in 57.1% of cases compared to 33.3% in younger patients. Advanced tumors (T3+T4) were more prevalent in elderly patients with Luminal B HER2-positive (33.3% vs 0%, p< 0.0001) and Luminal B HER2-negative (37.5% vs 8.3%, p< 0.05) subtypes. Surgical management differed significantly between groups: mastectomy was performed more frequently in elderly patients (57.14% vs 31.31%, p< 0.05), whereas breast-conserving surgery was less common (42.9% vs 67.7%, p< 0.05).
Conclusion: These findings demonstrate important differences in disease presentation and surgical management between age groups in Turkey, where breast cancer screening ends at age 69. The absence of screening detection in elderly patients, combined with their advanced disease presentation, highlights the need for further investigation with larger, multicenter cohorts to evaluate optimal screening strategies for women beyond age 69.
Keywords: breast cancer, elderly patients, tumor subtypes, surgery, age-related disparities
Introduction
Breast cancer is the most commonly diagnosed cancer in the world, with approximately 2.3 million new cases per year.1 In addition, breast cancer accounts for about 30% of all newly diagnosed cancers in women.2 In Turkey, breast cancer accounted for 23.9% of cancers recorded among women in 2020.1,3 Although age is one of the main risk factors for developing breast cancer, the global increase in life expectancy has been associated with a rise in breast cancer incidence among older women. According to Globocan 2020 data, 20% of breast cancer cases and 50% of breast cancer-related deaths occur in women over the age of 70.1 Moreover, mortality rates are higher in breast cancer cases over the age of 65, and the incidence continues to increase until the age of 80.4
International guidelines provide differing recommendations regarding breast cancer screening in women aged 70 years and above. The American Cancer Society recommends that mammographic screening should continue in women who are in good health and have a life expectancy of at least 10 years, without setting an upper age limit.5 Similarly, the American College of Radiology and the Society of Breast Imaging advise annual mammography starting at age 40 and do not advocate for a specific upper age limit.6 In contrast, in the United Kingdom, women are routinely invited for mammographic screening every three years between the ages of 50 and 71, after which they are not automatically invited but may self-refer if they wish.7 Similarly, the Dutch National Breast Cancer Screening Programme invites women aged 50–75 years for biennial mammography, with no automatic invitations beyond the age of 75.8 In Turkey, the National Breast Cancer Screening Program offers free mammography for women aged 40–69 years. The program ends at the age of 69, and no specific recommendations exist for breast cancer screening in individuals aged 70 and above.9
Research conducted in Turkey demonstrates that locally advanced breast cancer rates are substantially higher (18.4%) compared to developed countries (5%)7,10 Women aged ≥60 years show twice the rate of declining clinical examination compared to younger women.11 Furthermore, the majority of breast cancers in Turkey (67%) are detected symptomatically rather than through screening, with only 21.8% diagnosed during opportunistic mammography.7
Dr. Özmen’s analysis of 13,240 Turkish breast cancer patients found that Stage III breast cancer was diagnosed in 19% of women under 40 years of age, decreased to 13% in the 50–59 age group and 12.7% in those aged 60–69 years, then increased in patients aged 70 years and older.12 Additionally, the Turkish breast cancer screening program currently covers only 20–30% of the target population, with the majority of breast cancers being diagnosed at advanced stages.13
Cappellani et al documented that elderly breast cancer patients experience more frequent diagnostic delays and poorer outcomes related to reduced screening participation, delayed diagnosis, under-treatment, and comorbidities.14 In Turkey, where the National Breast Cancer Screening Program ends at age 69, the clinical and pathological characteristics of breast cancer in women aged 70 and older have not been systematically compared to those in younger patients.
Age-related differences in breast cancer molecular subtypes have been documented, although patterns vary across populations. Studies from different geographic regions and healthcare systems have reported divergent molecular subtype distributions with aging, suggesting that these patterns may be influenced by population-specific genetic factors, screening practices, or biological selection processes.15–17
In this comparative study, we aimed to evaluate differences in tumor characteristics, molecular subtypes, and surgical approaches between younger (<70 years) and elderly (≥70 years) breast cancer patients.
Materials and Methods
Ethics Approval
This retrospective study was conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments. The study protocol was approved by the Ethical Committee of Istanbul Aydin University (approval number: 124–2025). No interventions or changes to patient care were made for the purposes of this research.
Patient Selection and Study Design
This retrospective study included patients who underwent surgical treatment for breast cancer at the Department of General Surgery, Istanbul Aydin University Faculty of Medicine, between January 2020 and April 2025. All patients underwent clinical breast examination, radiological imaging (mammography and/or ultrasound), and core needle biopsy prior to surgery. While some patients were selected through screening mammography, the majority presented symptomatically with a palpable breast mass.
Screening procedures in our clinic consisted of clinical breast examination (CBE) followed by digital mammography using standard craniocaudal and mediolateral oblique views. For patients referred from external centers after screening mammography, the screening modality was consistently digital mammography. Patients with suspicious findings on mammography underwent supplementary breast ultrasound for further characterization.
Patients were stratified into two age groups, younger (<70 years) and elderly (≥70 years), to investigate age-associated differences in tumor characteristics and surgical management approaches.
Figure 1 presents the clinical presentation for both age groups. A total of 120 patients included 99 younger patients (<70 years) and 21 elderly patients (≥70 years). Palpable breast lump was the most common clinical presentation in both groups, presenting in 82 patients aged <70 years and 20 patients aged ≥70 years. Nipple discharge was observed in 2 younger patients and was not reported in the elderly group. Breast pain was documented in 3 patients aged <70 years and 1 patient aged ≥70 years. Among younger patients (<70 years), 12 patients were diagnosed through screening mammography, either at external centers (n=2) or at our clinic (n=10). None of the elderly patients (≥70 years) were diagnosed through screening mammography.
 |
Figure 1 Clinical presentation of breast cancer patients stratified by age group. Comparison of presenting symptoms and screening detection between patients <70 years (n=99) and ≥70 years (n=21). |
All treatment plans were reviewed in a multidisciplinary oncology board comprising specialists in general surgery, medical oncology, radiation oncology, nuclear medicine, and radiology. Patients eligible for neoadjuvant chemotherapy received it according to board recommendations; others proceeded directly to surgery based on updated clinical and radiological findings.
All surgeries were performed by the same surgical team. Depending on tumor characteristics and patient-specific factors, either breast-conserving surgery or mastectomy was performed. Sentinel lymph node biopsy (SLNB) was carried out in eligible cases, and if metastasis was detected, axillary lymph node dissection followed. In patients unsuitable for SLNB, primary axillary dissection was performed.
Data Collection and Analysis
Tumor Characteristics
Tumor diameter measurements were standardized to centimeters and validated through a systematic data cleaning algorithm to ensure consistency across measurements. Primary tumors (T stage), regional lymph nodes (N stage), and distant metastasis were evaluated according to the American Joint Committee on Cancer (AJCC) TNM classification system.
T stages were categorized as T0 (no evidence of primary tumor), Tis (carcinoma in situ), T1, T2, T3, or T4 based on clinical and pathological assessments. Advanced tumors were defined as T3 and T4 stages combined.
Lymph Node Status and Metastasis Assessment
Lymph node involvement was classified according to standard N stage definitions: N0 (no regional lymph node metastasis), N1mi (micrometastasis, approximately 0.2 mm to 2.0 mm), N1 (metastasis to 1–3 axillary lymph nodes), N2 (metastasis to 4–9 axillary lymph nodes), and N3 (metastasis to ≥10 axillary lymph nodes).
Lymph node metastatic status was additionally classified into a binary categorical variable for some analyses: “None” (including negative findings, zero positive nodes, and explicitly documented absence of metastasis) and “Metastasis” (including micrometastasis and any documented positive nodal disease).
Molecular Subtypes
Molecular subtypes were classified into five categories: Luminal A, Luminal B HER2-negative, Luminal B HER2-positive, HER2-enriched, and Triple-negative/basal-like. Classification was based on estrogen receptor (ER), progesterone receptor (PR), HER2 status, and Ki-67 expression levels determined from immunohistochemical analysis of surgical specimens.
Surgical Management Assessment
Seven key surgical management strategies were analyzed: breast-conserving surgery, mastectomy, sentinel lymph node biopsy (SLNB) performed, SLNB not stained, SLNB negative, SLNB positive, and axillary dissection. Breast-conserving surgery and axillary dissection were recorded as positive when documented as “yes” in patient records. Mastectomy was identified when the term “mastectomy” appeared in the surgery description. SLNB status was categorized as performed, not stained, negative, or positive based on specific terminology in clinical documentation.
Statistical Analysis
All statistical analyses were performed using Python 3.9 with SciPy (version 1.8.0) and pandas (version 1.4.2) libraries. Statistical significance was defined as p<0.05 throughout all analyses, with significance levels reported as p<0.05, p<0.01, or p<0.001 where appropriate.
Distribution Analysis
The distribution of continuous variables was assessed for normality using the Shapiro–Wilk test. For normally distributed data with equal variances (determined by Levene’s test), Student’s t-test was employed to compare means between groups. When normality was confirmed but variance equality was not, Welch’s t-test was utilized. For non-normally distributed data, the non-parametric Mann–Whitney U-test was applied.
Categorical Data Analysis
For categorical variables, differences in distributions between age groups were assessed using Pearson’s chi-square test. When expected cell counts were less than 5 in contingency tables, Fisher’s exact test was applied instead. For 2×2 tables, p-values were calculated using the two-sided Fisher’s exact test.
Advanced Analyses
For the molecular subtype analysis, either comparisons of metastasis counts between age groups within each subtype employed the independent t-test (for normally distributed data) or the Mann–Whitney U-test (for non-normally distributed data) based on prior normality assessment.
Advanced tumor rates were calculated as the percentage of T3+T4 tumors within each molecular subtype for both age groups. Absolute differences in rates between age groups (≥70 minus <70 years) were computed for each subtype. In addition to Fisher’s exact test, a binomial test was performed to assess whether the proportion of advanced tumors in the older age group was significantly greater than expected based on the younger age group’s rate.
For the forest plot analysis, 95% confidence intervals for the difference in proportions were calculated using the standard error formula.
Data Visualization
All visualizations were created using Python with Matplotlib (version 3.5.2) and Seaborn libraries. Figures were generated with scientific publication quality with clearly labeled axes, defined legends, and appropriate resolution for print publication.
Age groups were consistently differentiated by color and hatching patterns (light blue with circular hatching for <70 years, aquamarine with cross-hatching for ≥70 years) across all figures. Error bars representing the standard error of the mean were included where appropriate to illustrate data variability. Statistically significant differences (p<0.05) between groups were denoted with horizontal lines and corresponding p-value annotations.
Bar charts for displaying percentage distributions within TNM categories and surgical management strategies used visually distinct colors and patterns for each age group. Forest plots showing differences in advanced tumor rates between age groups included corresponding 95% confidence intervals and appropriate statistical annotations.
Missing Data Handling
Given the retrospective nature of this study utilizing surgical and pathological records, some variables had missing data. The completeness rates were as follows: age (100%, 120/120), surgical procedure (100%, 120/120), tumor size (96.7%, 116/120), T stage (91.7%, 110/120), molecular subtype (95.8%, 115/120), and axillary management procedures (100%, 120/120). We employed complete-case analysis, whereby cases with missing data for a specific variable were excluded only from analyses involving that variable.
Results
This retrospective, single-center study analyzed 120 breast cancer patients (99 younger, 21 elderly) treated surgically between 2020 and 2025 at Istanbul Aydın University, Turkey. Tumor characteristics and surgical management related data were analyzed to compare two age groups.
Table 1 summarizes the key comparative findings between age groups. Patients in the elderly group (≥70 years) had a mean age of 74.6 ± 4.7 years compared to 50.9 ± 9.7 years in the younger group (p<0.001). Elderly patients presented with significantly larger primary tumors (3.91 ± 0.56 cm vs 2.81 ± 0.35 cm, p<0.05) and a higher prevalence of T4 disease (19.05% vs 3.37%, p<0.05). Among patients with metastatic disease, the elderly group demonstrated a significantly higher mean metastasis count (7.90 ± 6.06 vs 3.54 ± 4.49, p<0.05). Surgical management patterns differed significantly between groups, with sentinel lymph node biopsy performed less frequently in elderly patients (71.4% vs 90.9%, p<0.05), while axillary lymph node dissection was more common in this group (57.1% vs 33.3%, p<0.05).
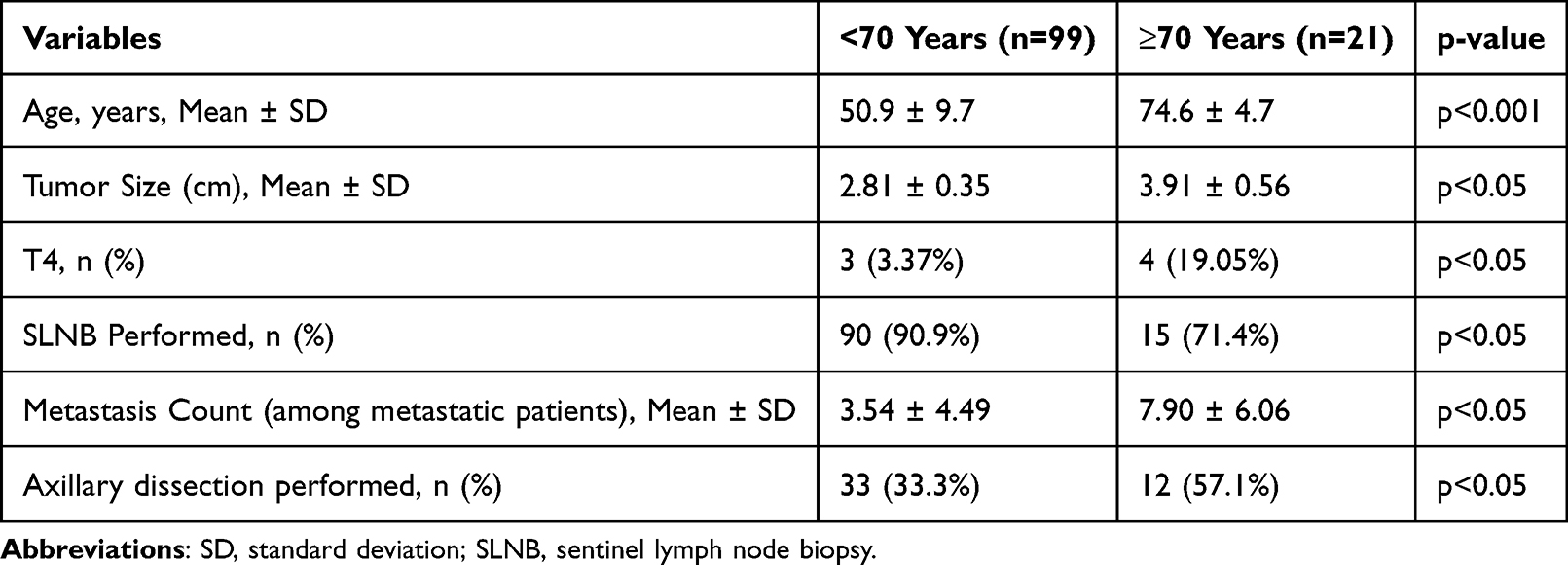 |
Table 1 Summary of Key Findings by Age Groups (<70 Vs ≥70 Years) |
Tumor Size Differences Between Age Groups
In Figure 2A, analysis of tumor size revealed significant differences between age groups. Elderly patient group (≥70 years) presented with notably larger primary breast tumors compared to younger patient group (<70 years), with mean tumor diameters of 3.91 ± 0.56 cm and 2.81 ± 0.35 cm, respectively (p < 0.05).
 |
Figure 2 Comparison of primary breast tumor size between age groups and metastatic status. (A) Mean tumor diameter (cm) comparison between younger (<70 years) and elderly (≥70 years) breast cancer patients. (B) Mean tumor diameter stratified by both age group and metastatic status. Blue bars represent patients <70 years; green bars represent patients ≥70 years. |
Relationship Between Tumor Diameter, Age, and Metastatic Status
In Figure 2B, further stratification by metastatic status demonstrated a consistent pattern of larger tumor diameters in older patients within both metastatic categories. In patients without metastasis, mean tumor diameter was 2.10 ± 0.17 cm in the younger patient group compared to 2.85 ± 0.38 cm in the elderly group. This difference was more pronounced in patients with metastasis, where mean tumor diameters were 3.76 ± 0.83 cm and 5.08 ± 1.00 cm for younger and elderly patients, respectively.
The largest disparity was observed between younger patients without metastasis and elderly patients with metastasis, with the elder patient group exhibiting tumors more than twice the diameter of the younger patient group (2.10 ± 0.17 cm vs 5.08 ± 1.00 cm, p < 0.01).
TNM Classification Analysis by Age Group
T Stage Distribution
In Figure 3A, analysis of T stage distribution revealed statistically significant differences between age groups (Fisher’s exact test, p = 0.0528). The younger group (<70 years) demonstrated a predominance of T1 (42.70%) and T2 (48.31%) tumors, which together accounted for 91.01% of cases in this age group. In contrast, the elderly group (≥70 years) showed a more varied distribution with notably higher proportions of T4 tumors (19.05% vs 3.37%, p < 0.05) and carcinoma in situ (Tis) (4.76% vs 1.12%). T2 tumors remained relatively consistent between age groups (47.62% in older vs 48.31% in younger patients). T3 tumors occurred at similar rates in both groups (4.49% in younger vs 4.76% in older patients), while T1 tumors were more common in younger patients (42.70% vs 23.81% in older patients).
 |
Figure 3 TNM classification parameters across age groups in breast cancer patients. (A) Distribution of T stage by age group. (B) Nodal status distribution by age group. (C) Box plot showing metastasis count distribution among patients with metastatic disease by age group (<70 years vs ≥70 years). Box plots display median (horizontal line), interquartile range (box), range (whiskers), and outliers (dots). |
Nodal Status
Nodal involvement patterns differed between age groups, although the difference did not reach conventional statistical significance (Fisher’s exact test, p = 0.0838) (Figure 3B). Notably, younger patients exhibited a higher proportion of N0 disease (66.33% vs 50.00% in older patients), indicating a greater likelihood of node-negative status. Micrometastasis (N1mi) was observed in 6.12% of younger patients with no corresponding cases documented in the elderly group. The elderly group demonstrated a higher prevalence of N2 disease (20.00% vs 7.14% in younger patients) and N3 disease (15.00% vs 4.08% in younger patients). N1 disease showed similar distribution between the groups (16.33% in younger vs 15.00% in older patients).
Analysis of Metastasis
Figure 3C illustrates the distribution of metastasis counts by age group among patients presenting with metastatic disease. Statistical analysis revealed a significant difference in metastatic dissemination between age groups (p < 0.05). Elderly patients (≥70 years) demonstrated higher metastatic involvement compared to younger patients (<70 years), with mean metastasis counts of 7.90 ± 6.06 and 3.54 ± 4.49, respectively.
Surgical Management Analysis by Age Group
In Figure 4, analysis of surgical management strategies revealed distinct patterns between younger (<70 years) and older (≥70 years) breast cancer patients.
 |
Figure 4 Surgical management strategies by age group. (A) Distribution of breast surgery types comparing breast-conserving surgery, mastectomy, and modified radical mastectomy between age groups. (B) Sentinel lymph node biopsy (SLNB) status showing rates of SLNB performed, not stained, negative, and positive results. (C) Axillary lymph node dissection rates. (D) Tumor laterality distribution including right, left, and bilateral cases. |
Breast Surgery Type Distribution
In Figure 4A, analysis of breast surgery types revealed statistically significant differences in surgical approach between age groups (p = 0.029). Breast-conserving surgery (BCS) was the most common procedure in both groups. BCS was performed in 68.7% (n=68) of younger patients and 47.6% (n=10) of elderly patients. Mastectomy rates remained comparable between age groups (16.2%, n=16 in younger vs 14.3%, n=3 in elderly patients). Modified radical mastectomy was performed significantly more frequently in the elderly group (38.1%, n=8) compared to the younger group (15.2%, n=15) (p = 0.029).
Sentinel Lymph Node Biopsy Status
Figure 4B demonstrates the distribution of sentinel lymph node biopsy (SLNB) procedures and outcomes across age groups. SLNB was performed significantly more frequently in younger patients (90.9%, n=90) compared to elderly patients (71.4%, n=15, p = 0.025). Among cases where SLNB was performed but lymph nodes were not stained, rates were similar between groups (6.1%, n=6 in younger vs 9.5%, n=2 in elderly patients, p = 0.628). SLNB-negative results were observed in 62.6% (n=62) of younger patients compared to 38.1% (n=8) of elderly patients (p = 0.051). SLNB-positive results were comparable between age groups (22.2%, n=22 in younger vs 23.8%, n=5 in elderly patients, p = 1.000).
Axillary Dissection Analysis
In Figure 4C, axillary lymph node dissection rates differed significantly between age groups (p = 0.049). Elderly patients underwent axillary dissection in 57.1% (n=12) of cases compared to 33.3% (n=33) in younger patients.
Tumor Laterality Distribution
Figure 4D illustrates the distribution of tumor laterality across age groups. No statistically significant differences were observed in tumor location between younger and elderly patients. Left-sided tumors were slightly more common in the elderly group (61.9%, n=13) compared to the younger group (48.5%, n=48, p = 0.338), while right-sided tumors showed the opposite pattern (48.5%, n=48 in younger vs 38.1%, n=8 in elderly patients, p = 0.473). Bilateral breast cancer was rare and observed only in younger patients (3.0%, n=3), with no cases documented in the elderly group (p = 1.000).
Distribution of Molecular Subtypes by Age Group
In Figure 5, the distribution of breast cancer molecular subtypes differed notably between age groups. In patients under 70 years of age, Luminal A was the predominant subtype (34.41%), followed by Luminal B HER2-negative (29.03%). Conversely, in the elderly group (≥70 years), Luminal B HER2-negative was the most common subtype (42.11%), representing a 13.08 percentage point increase compared to the younger group.
 |
Figure 5 Distribution of breast cancer molecular subtypes by age group. Bar chart comparing the percentage of molecular subtypes between patients <70 years (blue) and ≥70 years (green). Molecular subtyping utilized a Ki67 threshold of 14.0% for distinguishing between Luminal A and Luminal B HER2-negative categories, in accordance with current consensus guidelines. HER2: human epidermal growth factor receptor 2. |
Luminal A tumors were significantly less frequent in elderly patients (21.05% vs 34.41% in younger patients). The prevalence of Luminal B HER2-positive and HER2-overexpression subtypes was slightly higher in the younger groups (13.98% vs 10.53% and 10.75% vs 10.53%, respectively). Triple-negative breast cancers were more common in elderly patients (15.79%) compared to younger patients (11.83%).
Molecular subtyping classification utilized a Ki67 threshold of 14.0% for distinguishing between Luminal A and Luminal B HER2-negative categories, in accordance with current consensus guidelines. The observed differences in molecular subtype distribution between age groups suggest potential age-related biological variations in breast cancer, which may have implications for treatment approaches and prognosis.
Mean Metastasis Count by Molecular Subtype and Age
Figure 6 illustrates the comparison of mean metastasis counts across five major molecular subtypes (Luminal A, Luminal B HER2-, Luminal B HER2+, HER2-enriched, and Triple-negative/basal-like) stratified by age groups (<70 years vs ≥70 years). Overall, patients in the elderly group (≥70 years) demonstrated higher mean metastasis counts compared to the younger group (<70 years) in most molecular subtypes.
 |
Figure 6 Mean metastasis count by molecular subtype and age group in breast cancer patients. Bar graph comparing the average number of metastases between younger (<70 years, blue bars) and elderly (≥70 years, green bars) patients across five molecular subtypes. |
In the Luminal A subtype, elderly patients exhibited a substantially higher mean metastasis count (2.50 ± 5.00) compared to younger patients (0.42 ± 0.87, p=0.87). The Luminal B HER2- subtype showed more comparable distributions between age groups, with mean counts of 3.08 ± 5.40 in younger patients and 3.63 ± 5.68 in elderly patients (p=0.73). Notably, the Luminal B HER2+ subtype demonstrated significantly higher metastasis counts in the elderly group (9.33 ± 9.71) compared to the younger group (0.77 ± 1.54, p<0.05).
A similar pattern was observed in the HER2-enriched subtype, where elderly patients showed a mean metastasis count of 5.50 ± 3.54 compared to 0.91 ± 2.07 in younger patients. In contrast, the Triple-negative/basal-like subtype exhibited the lowest mean metastasis counts in both age groups, with comparable values between younger (0.36 ± 0.67) and elderly patients (0.33 ± 0.58, p=1.00).
Distribution of Advanced Tumors by Age Group and Molecular Subtype
In Figure 7, analysis of advanced tumor (T3+T4) distribution across molecular subtypes revealed notable age-related differences.
 |
Figure 7 Advanced tumor (T3+T4) distribution across molecular subtypes by age group. (A) Percentage of advanced-stage tumors (T3+T4) in each molecular subtype, stratified by age group (<70 years, blue bars; ≥70 years, green bars). Statistical significance is indicated where applicable (p < 0.05, p < 0.0001). (B) Forest plot displaying the difference in advanced tumor rates between age groups (≥70 minus <70 years) with 95% confidence intervals for each molecular subtype. Points to the right of zero indicate higher rates in the elderly group. Red points indicate lower rates in the elderly group. P-values are shown for each comparison. |
In Figure 7A, the percentage of advanced tumors in Luminal B HER2-negative was significantly higher in the elderly group (37.5%) compared to the younger group (8.3%, p<0.05). Similarly, Luminal B HER2+ positive showed a markedly higher rate in elderly patients (33.3%) versus younger patients (0%, p<0.0001). The HER2-enriched subtype also demonstrated a substantial difference between elderly (50.0%) and younger patients (22.2%), although this did not reach statistical significance (p=0.395). Conversely, both Luminal A and Triple-negative/basal-like subtypes showed no advanced tumors (0%) in elderly patients compared to low rates in younger patients (3.0% and 11.1%, respectively).
Figure 7B illustrates the absolute differences in advanced tumor rates between age groups (≥70 minus <70 years) with 95% confidence intervals. The most pronounced differences were observed in Luminal B HER2-positive (+0.333), Luminal B HER2-negative (+0.292), and HER2-enriched (+0.278) subtypes. Conversely, the proportion of advanced tumors was lower in elderly patients for Luminal A (−0.030) and Triple-negative/basal-like (−0.111) subtypes, with p = 1.000 for both.
Statistical analyses revealed significant age-related disparities in the prevalence of advanced tumors within specific molecular subtypes. Statistical analyses demonstrated that the proportion of advanced tumors was significantly higher in elderly patients with Luminal B HER2-negative (p < 0.05) and Luminal B HER2-positive (p < 0.0001) subtypes compared to their younger group.
Discussion
In this comparative study, we aimed to evaluate differences in tumor characteristics, molecular subtypes, and surgical approaches between younger (<70 years) and elderly (≥70 years) breast cancer patients. We found that elderly breast cancer patients (≥70 years) in Turkey present with more advanced disease, larger tumors, and higher metastatic burden than younger patients. However, Turkey’s National Breast Cancer Screening Program terminates at age 69 with no specific guidance for women aged 70 and above.
A comprehensive systematic review of global breast cancer screening guidelines demonstrates considerable variation in recommendations for women aged 70 years and above. The review analyzed over 20 international guidelines and found that many organizations recommend continued screening beyond age 70 based on individual life expectancy rather than chronological age cutoffs. Several countries, including the United States, Australia, and some European nations, emphasize shared decision-making between clinicians and patients, with continued screening recommended for women in good health with an estimated life expectancy of at least 10 years.18
The American College of Radiology and the Society of Breast Imaging recommend annual mammography starting at age 40 and do not recommend for a specific upper age limit as well as cit the mortality reduction benefits of continued screening.19 Similarly, the American Cancer Society does not propose an upper age limit for screening mammography. Instead, it recommends continued screening for healthy older women with a life expectancy of at least 10 years.5,20 In contrast, Turkey’s National Breast Cancer Screening Program ends at age 69 without guidance for women aged 70 and above, representing a more restrictive approach compared to other national guidelines.18
Our findings align with those reported by Bertozzi et al, who observed significantly different tumor characteristics in women aged ≥70 years compared to younger cohorts. Bertozzi et al found T4 tumors in 4.12% of patients aged ≥70 years versus 0.92% in those aged 45–69 years (p < 0.001), representing a 4.5-fold increase.21 Our data demonstrate both a similar pattern and a markedly higher prevalence, with T4 tumors occurring in 19.05% of elderly patients (≥70 years) compared to 3.37% in younger patients (<70 years), representing a 5.7-fold increase (p < 0.05).
Regarding axillary staging approaches, both studies document age-related disparities in sentinel lymph node biopsy utilization. Bertozzi et al reported SLNB rates of 63.57% in patients aged 45–69 years versus 59.60% in those ≥70 years.21 Our findings reveal a more pronounced disparity, with SLNB performed in 90.9% of younger patients (<70 years) compared to 71.4% of elderly patients (≥70 years, p=0.025). Furthermore, complete axillary lymph node dissection (CALND) patterns illustrate age-related surgical disparities. Bertozzi et al documented CALND rates of 36.43% in patients aged 45–69 years versus 40.40% in those ≥70 years. Our study demonstrates a larger differential, with elderly patients undergoing axillary dissection in 57.1% of cases compared to 33.3% in younger patients (p=0.049). This substantial difference representing a 23.8 percentage point increase in our elderly cohort versus a 3.97 percentage point increase in the Italian cohort, suggests that Turkish elderly patients present with more advanced nodal disease requiring extensive axillary surgery. Combined with our finding of larger primary tumors and higher T4 rates, these data show that the absence of screening after age 69 may contribute to more advanced locoregional disease requiring more axillary dissection.
Our observation of increased tumor burden in elderly patients is consistent with findings from a recent French multicenter study. In an analysis of 528 patients aged ≥70 years with triple-negative or HER2-positive breast cancer, Houvenaeghel et al reported that tumor size >50mm increased from 6.6% in the 70–74 age group to 13.3% in those >80 years (p<0.0001). Similarly, axillary lymph node macrometastases increased from 21.8% to 33.6% across these age groups (p=0.010).22 These findings parallel our results showing mean tumor diameters of 3.91 ± 0.56 cm in patients ≥70 years versus 2.81 ± 0.35 cm in those <70 years (p<0.05).
Molecular Subtype Comparison
Our findings regarding molecular subtype distribution in elderly breast cancer patients both align with and diverge from the Jenkins et al analysis. Luminal A subtype distribution increased progressively with age from 18% (ages 21–39) to 32% (ages 60–69), and peaked at 39% in elderly patients ≥70 years.17 However, our study demonstrated a converse pattern, with Luminal A prevalence decreasing from 34.41% in patients <70 years to 21.05% in patients ≥70 years.
Luminal B subtype distribution increased progressively with age from 12% (ages 21–39) to 28% (ages 60–69), and peaked at 32% in elderly patients ≥70 years.17 However, our study demonstrated a more complex pattern when stratified by HER2 status. Luminal B HER2-negative prevalence increased substantially from 29.03% in patients <70 years to 42.11% in patients ≥70 years, while Luminal B HER2-positive prevalence decreased from 13.98% in patients <70 years to 10.53% in patients ≥70 years.
HER2-enriched subtype distribution remained relatively stable across age groups, ranging from 12% to 16%, with 11% observed in elderly patients ≥70 years.17 Similarly, our study demonstrated comparable HER2 overexpression prevalence between age groups, with 10.75% in patients <70 years and 10.53% in patients ≥70 years.
Basal-like subtype distribution decreased dramatically with age from 44% (ages 21–39) to 16% (ages 60–69), reaching 9% in elderly patients ≥70 years.17 In contrast, our study demonstrated a converse pattern, with triple-negative breast cancer prevalence increasing from 11.83% in patients <70 years to 15.79% in patients ≥70 years. These contrasting and similar patterns in molecular subtype distribution in breast cancer between our Turkish cohort and the Jenkins et al study17 highlight potential population-specific differences that warrant further investigation.
In our study, none of the elderly patients (≥70 years) were diagnosed through screening mammography, compared to 12.1% of younger patients. All elderly patients presented symptomatically, predominantly with palpable breast masses (95.2%). Compared to younger patients (<70 years), elderly patients (≥70 years) presented with more advanced disease characteristics: significantly larger mean tumor sizes (3.91 cm vs 2.81 cm, p<0.05), higher proportions of T4 tumors (19.05% vs 3.37%, p<0.05), and greater metastatic burden (mean 7.90 vs 3.54 metastases, p<0.05). While multiple factors may influence presentation patterns in elderly patients, the lack of organized screening access beyond age 69 in Turkey represents a potential contributor to delayed diagnosis in this population. These findings warrant further investigation into the role of screening cessation in disease presentation among elderly patients.
Historically, radical or modified radical mastectomy was the preferred treatment for elderly patients, mainly due to uncertainties regarding their tolerance to adjuvant therapies. As a result, BCS was less frequently chosen by both patients and clinicians.23 However, recent trends show a shift toward increased use of BCS even in the elderly population.24,25 In our study, we found that mastectomy was performed more frequently in elderly patients and this was statistically significant (p<0.05). Among patients over 70 years of age, 47.6% underwent BCS, and 52.4% underwent mastectomy. All patients tolerated surgical treatment well, and there were no significant delays in initiating adjuvant therapies. In our cohort, 47.6% of elderly patients underwent BCS with good surgical tolerance, demonstrating the feasibility of both surgical approaches in this age group.
Limitations
This study has several important limitations that should be considered when interpreting the findings. First, the retrospective single-center design limits the generalizability of results to broader populations with different healthcare systems and sociodemographic characteristics. The relatively small sample size in the elderly group (n=21) may have limited statistical power to detect differences in some subgroup analyses, and the predominance of externally referred patients in this group may not fully represent the breast cancer spectrum in elderly women in community.
Detailed screening history data were not systematically available in our retrospective surgical database. This includes individual screening frequency (annual vs biennial), adherence to screening protocols, and intervals between screenings prior to diagnosis. For patients referred from external centers, we had no access to their individual-level screening histories or compliance patterns.
Second, detailed geriatric assessment data, including comorbidity profiles, functional status, cognitive function, and estimated life expectancy, were not systematically collected in our retrospective surgical database. The absence of standardized geriatric assessment tools, such as the Comprehensive Geriatric Assessment (CGA), Activities of Daily Living (ADL) scales, or the G8 screening tool, represents an important limitation.
Third, several potentially important confounding variables, including tumor grade, socioeconomic status, educational level, distance to healthcare facilities, and psychosocial support systems, were not systematically evaluated. These factors may independently influence both disease presentation and treatment choices.
Fourth, long-term outcome data, including overall survival, disease-free survival, and quality of life measures, were not available. Therefore, we cannot assess whether the different surgical approaches employed across age groups resulted in different clinical outcomes or patient satisfaction.
Fifth, our study was not designed to evaluate screening effectiveness or address the important issue of overdiagnosis, which requires population-level longitudinal data as demonstrated by Bleyer and Welch.26
Sixth, the retrospective nature of our surgical database limited available demographic data to age and sex. The absence of socioeconomic variables (education, income, insurance status) and other demographic factors that may influence cancer presentation and surgical management decisions represents an important limitation.
Seventh, the low rates of missing data (<10% for all variables) and we acknowledge this as a limitation in our study. Despite these limitations, this study provides valuable insights into the clinical characteristics and management patterns of elderly breast cancer patients in Turkey and highlights the need for reconsideration of age-based screening cutoffs.
Future Directions
Future research should address these limitations through prospective, multicenter studies incorporating comprehensive geriatric assessments and long-term follow-up data to better inform treatment guidelines for elderly breast cancer patients. Such studies should evaluate long-term outcomes including overall survival, disease-free survival, and quality of life measures.
Some international guidelines provide frameworks for population-based screening programs, most rely primarily on chronological age. The development of validated decision-making algorithms integrating chronological age, functional status, comorbidities, and life expectancy could guide individualized screening and treatment recommendations. Collaboration between surgical oncologists, geriatricians, and patient advocates will be essential to implement age-appropriate, patient-centered breast cancer care that optimizes both survival and quality of life in elderly women.
Conclusion
Our findings demonstrate important differences in disease presentation and surgical management between age groups in Turkey, where breast cancer screening ends at age 69. The absence of screening detection in elderly patients, combined with their advanced disease presentation, raises important questions about the appropriateness of age-based screening cutoffs. While acknowledging the limitations of our single-center design and small elderly cohort, these observations support the need for larger multicenter studies to evaluate optimal screening and management strategies for women beyond age 69.
Acknowledgments
The authors would like to thank the staff of the General Surgery Department and the Oncology Council at Istanbul Aydın University for their contributions to patient management and data collection. No external funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. doi:10.3322/caac.21442
3. Özmen V, Özmen T, Doğru V. Breast Cancer in Turkey; An Analysis of 20.000 patients with breast cancer. Eur J Breast Health. 2019;15(3):141–146. doi:10.5152/ejbh.2019.4890
4. Schrager S, Ovsepyan V, Burnside E. Breast cancer screening in older women: the importance of shared decision making. J Am Board Fam Med. 2020;33(3):473–480. doi:10.3122/jabfm.2020.03.190380
5. Smith RA, Andrews KS, Brooks D, et al. Cancer screening in the United States, 2017: a review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin. 2017;67(2):100–121. doi:10.3322/caac.21392
6. Monticciolo DL, Malak SF, Friedewald SM, et al. Breast cancer screening recommendations inclusive of all women at average risk: update from the acr and society of breast imaging. J Am Coll Radiol. 2021;18(9):1280–1288. doi:10.1016/j.jacr.2021.04.021
7. Ozmen V, Boylu S, Ok E, et al. Factors affecting breast cancer treatment delay in Turkey: a study from Turkish Federation of Breast Diseases Societies. Eur J Public Health. 2015;25(1):9–14. doi:10.1093/eurpub/cku086
8. RIVM. Breast cancer screening programme [homepage on the Internet]. Bilthoven (Netherlands): RIVM; 2025. Available from: https://www.rivm.nl/en/breast-cancer-screening-programme.
9. Keskinkılıc B, Gultekin M, Akarca AS, et al. Turkey Cancer Control Programme. Ankara, Turkey: Ministry of Health, Turkey Public Health Agency, Cancer Department; 2016.
10. Jassem J, Ozmen V, Bacanu F, et al. Delays in diagnosis and treatment of breast cancer: a multinational analysis. Eur J Public Health. 2014;24(5):761–767. doi:10.1093/eurpub/ckt131
11. Hayran M, Abali H, Kilickap S, et al. Socio-demographic parameters in screening for breast cancer: lessons from a population-based Women’s Health Project held in a province in Turkey. J Buon. 2010;15(4):726–731.
12. Özmen V. Breast cancer in turkey: clinical and histopathological characteristics (Analysis of 13.240 Patients). J Breast Health. 2014;10(2):98–105. doi:10.5152/tjbh.2014.1988
13. Selçuk K T, Avcı D, Dündar G Y, Mercan Y. Breast cancer screening behaviors in women aged 40 years and over in a Semi-Urban Region in Turkey. Relationships With Health Beliefs Healthcare. 2020;8(2):171.
14. Cappellani A, Vita MD, Zanghì A, et al. Prognostic factors in elderly patients with breast cancer. BMC Surg. 2013;13(Suppl 2):S2. doi:10.1186/1471-2482-13-S2-S2
15. van der Meer DJ, Kramer I, van Maaren MC, et al. Comprehensive trends in incidence, treatment, survival and mortality of first primary invasive breast cancer stratified by age, stage and receptor subtype in the Netherlands between 1989 and 2017. Int, J, Cancer. 2021;148(9):2289–2303. doi:10.1002/ijc.33417
16. Acheampong T, Kehm RD, Terry MB, Argov EL, Tehranifar P. Incidence trends of breast cancer molecular subtypes by age and race/ethnicity in the US From 2010 to 2016. JAMA Netw Open. 2020;3(8):e2013226. doi:10.1001/jamanetworkopen.2020.13226
17. Jenkins EO, Deal AM, Anders CK, et al. Age-specific changes in intrinsic breast cancer subtypes: a focus on older women. Oncologist. 2014;19(10):1076–1083. doi:10.1634/theoncologist.2014-0184
18. Ren W, Chen M, Qiao Y, Zhao F. Global guidelines for breast cancer screening: a systematic review. Breast. 2022;64:85–99. doi:10.1016/j.breast.2022.04.003
19. Lee CS, Moy L, Joe BN, Sickles EA, Niell BL. Screening for breast cancer in women age 75 years and older. AJR Am J Roentgenol. 2018;210(2):256–263. doi:10.2214/AJR.17.18705
20. Oeffinger KC, Fontham ETH, Etzioni R, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American cancer society. JAMA. 2015;314(15):1599. doi:10.1001/jama.2015.12783
21. Bertozzi S, Londero AP, Diaz Nanez JA, et al. Breast cancer care for the aging population: a focus on age-related disparities in breast cancer treatment. BMC Cancer. 2025;25:492. doi:10.1186/s12885-025-13893-8
22. Houvenaeghel G, Cohen M, Gonçalves A, et al. Triple-negative and Her2-positive breast cancer in women aged 70 and over: prognostic impact of age according to treatment. Front Oncol. 2023;13:1287253. doi:10.3389/fonc.2023.1287253
23. Bergman L, Dekker G, Van Leeuwen FE, Huisman SJ, van Dam FS, van Dongen JA. The effect of age on treatment choice and survival in elderly breast cancer patients. Cancer. 1991;67(9):2227–2234. doi:10.1002/1097-0142(19910501)67:9<2227::AID-CNCR2820670903>3.0.CO;2-0
24. Kuzan TY, Koca E, Dizdar O, et al. Breast cancer in octogenarian women: clinical characteristics and outcome. J Buon. 2013;18(2):328–334.
25. Huszno J, Kolosza Z, Mrochem-Kwarciak J, Grzybowska E. Overall survival analysis of > 65-year-old patients with breast cancer based on their molecular, clinicopathological and laboratory factors. Arch Med Sci. 2022;18(3):800–804. doi:10.5114/aoms/147736
26. Bleyer A, Welch HG. Effect of three decades of screening mammography on breast-cancer incidence. N Engl J Med. 2012;367(21):1998–2005. doi:10.1056/NEJMoa1206809
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Breast Cancer in Geriatric Patients: Current Landscape and Future Prospects
Abdel-Razeq H, Abu Rous F, Abuhijla F, Abdel-Razeq N, Edaily S
Clinical Interventions in Aging 2022, 17:1445-1460
Published Date: 28 September 2022
Breast Cancer Management in the Era of Covid-19; Key Issues, Contemporary Strategies, and Future Implications
Prodhan ASU, Islam DZ, Khandker SS, Jamiruddin MR, Abdullah A, Godman B, Opanga S, Kumar S, Sharma P, Adnan N, Pisana A, Haque M
Breast Cancer: Targets and Therapy 2023, 15:51-89
Published Date: 27 January 2023
Psychosocial Problems of Rural Indian Women Practising Breast Self-Examination – a Community-Based Study from Southern India
Balaiah Mehanathan P, Arthur Edwards Dennison A, Vikramathithan Panchapooranam A, Kandasamy S, Subbiah P, Velappan L, Kalyanaraman S
Breast Cancer: Targets and Therapy 2023, 15:263-270
Published Date: 17 April 2023
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Innovative Surgical Approaches That Improve Individual Outcomes in Advanced Breast Cancer
Luțenco V, Rebegea L, Beznea A, Tocu G, Moraru M, Mihailov OM, Ciuntu BM, Luțenco V, Stanculea FC, Mihailov R
International Journal of Women's Health 2024, 16:555-560
Published Date: 30 March 2024