Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Best Evidence Summary for Preconception Management in Childbearing-Age Patients with Rheumatoid Arthritis
Authors Liu S ![]() , Guo Y, Ren H, Zheng P, Lv T, Liu Q
, Guo Y, Ren H, Zheng P, Lv T, Liu Q
Received 31 October 2025
Accepted for publication 18 December 2025
Published 24 December 2025 Volume 2025:18 Pages 8197—8208
DOI https://doi.org/10.2147/JMDH.S578181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Veronica Swallow
Sanjiao Liu,1 Yifan Guo,1 Hua Ren,1 Pengyan Zheng,1 Ting Lv,2 Qingqing Liu2
1School of Nursing, Shanxi University of Chinese Medicine, Jinzhong City, Shanxi Province, 030619, People’s Republic of China; 2School of Nursing, Shanxi Medical University, Taiyuan City, Shanxi Province, 030001, People’s Republic of China
Correspondence: Hua Ren, School of Nursing, Shanxi University of Chinese Medicine, 121 University Street, Yuci District, Jinzhong City, Shanxi Province, 030619, People’s Republic of China, Email [email protected]
Background: The onset of rheumatoid arthritis (RA) most often occurs during the reproductive years. The chronic inflammatory state associated with the disease, along with the effects of therapeutic agents, contributes to a significantly higher incidence of adverse pregnancy outcomes compared to the general population. Standardized preconception management for childbearing-age patients with RA is an important prerequisite for achieving a safe pregnancy and promoting healthy offspring. However, existing evidence is scattered, and clinical practice lacks efficient evidence-based guidelines.
Objective: To identify, evaluate, and summarize the best available evidence on preconception care for childbearing age with RA, and to provide evidence-based guidance for clinical nursing practice.
Methods: A systematic search was conducted according to the “ 6S” pyramid model of evidence-based resources to identify evidence related to preconception management in childbearing-age patients with RA. Sources included clinical decision support systems, guidelines, databases, and professional association websites. The search covered all records from database inception until June 17, 2025.
Results: A total of 11 publications were included, comprising 3 guidelines, 5 expert consensuses, 2 clinical decisions, and 1 systematic review. From these sources, a comprehensive set of 23 best evidence recommendations was formed across seven key aspects: general principles, fertility risk assessment, preconception screening, pre-pregnancy medication adjustment, fertility preservation, weight and nutrition management, and psychological support. Among the evidence gathered, a strong recommendation was made for 15 items, while the remaining 8 received a weak recommendation.
Conclusion: This study provides a summary of best evidence for the preconception management of childbearing-age patients with RA, offering valuable guidance for clinical practice. To maximize patient benefits, healthcare providers should exercise careful clinical judgment when applying this evidence, taking into account the specific clinical context, individual patient circumstances, and preferences.
Trial Registration: ES20258177.
Keywords: rheumatoid arthritis, childbearing age, preconception management, fertility, evidence summary, evidence-based nursing
Introduction
Rheumatoid Arthritis (RA) is a common chronic autoimmune disease of unknown etiology, for which there is currently no cure, and continuous medication is required to maintain disease stability.1 Its incidence is rising globally, with projections indicating 31.7 million people will be affected by 2050.2 The disease shows a male-to-female ratio of approximately 3:2, with a majority of female patients being of childbearing age at onset.3
In recent years, women with RA of reproductive age (15–49 years) have garnered increased attention due to their dual roles in managing the disease and fulfilling reproductive responsibilities.4 Both RA and its treatments can influence fertility, pregnancy progression, and outcomes, thereby critically shaping reproductive decisions.5 Studies indicate that these patients face higher risks of maternal and neonatal complications compared to their healthy counterparts.6 Preconception care, through the management of modifiable risk factors (such as medication regimens and nutritional deficiencies), can effectively enhance fertility rates, reduce the incidence of maternal and perinatal complications, and decrease the risk of birth defects.7 Supporting this, a study by El Miedany et al8 demonstrated that standardized preconception management can reduce the incidence of adverse pregnancy outcomes (APO) in RA patients to a level comparable to that of the general population.Furthermore, research by Bobircă et al9 confirmed that a planned pregnancy is a protective factor against APO in RA. Their study revealed a significantly higher proportion of planned pregnancies among patients without APO (91.7%) compared to those with APO (55.9%). Therefore, implementing standardized preconception management is a crucial prerequisite for achieving safe pregnancies and ensuring the health of offspring in this patient population.
Studies indicate that standardized pre-pregnancy management should be comprehensive. It is advocated that a rheumatologist-led, multidisciplinary clinic be established to guide women with RA through pregnancy preparation.7 This clinic is responsible for facilitating communication and building consensus on several key aspects, including pre-pregnancy risk assessment, conception planning, medication guidance, disease activity monitoring, patient education, and self-management, to formulate an individualized pregnancy plan.7 Early pre-pregnancy management planning facilitates the evaluation and adjustment of medications for compatibility with pregnancy, thereby laying the groundwork for a subsequent safe gestation.3
However, existing evidence on preconception management for RA patients remains fragmented, and clinical guidelines vary in emphasis, are often lengthy, and lack consolidation. This makes it difficult for healthcare providers to efficiently retrieve and apply recommendations in practice. Therefore, this study aims to synthesize best evidence regarding preconception management for reproductive-age women with RA, offering a clear, evidence-based reference for clinical nursing.
Material and Methods
Problem Establishment
The PIPOST model was employed to formulate an evidence-based question.10 The target population (P) consisted of reproductive-age RA patients. The intervention (I) refers to preconception management strategies. The evidence implementers (P) include healthcare professionals, patients, and their families. The outcome (O) focused on pregnancy success rate, incidence of adverse pregnancy outcomes, disease flare rate during pregnancy, and fertility intentions. The evidence implementation setting (S) was healthcare institutions, communities, and households. The type of evidence (T) encompasses guidelines, expert consensuses, clinical decisions, systematic reviews, and evidence summaries.
Literature Screening Method
Evidence resources were retrieved layer by layer from high to low in accordance with the “6S” pyramid evidence resource model, including decision support systems such as Up To Date and BMJ Best Practice; platforms including the Joanna Briggs Institute (JBI), National Institute for Health and Care Excellence (NICE), Registered Nurses’ Association of Ontario (RNAO), Guidelines International Network (GIN), and MedLive; databases including Web of Science, PubMed, Cochrane Library, Embase, SinoMed, CNKI, Wanfang Database, and VIP Database; as well as professional society websites including the American College of Rheumatology (ACR), British Society for Rheumatology (BSR), European League Against Rheumatism (EULAR). The retrieval period was from the establishment of each database to June 17, 2025. The retrieval terms used were “Arthritis, Rheumatoid /rheumarthritis/rheumat* arthritis/rheumat* polyarthritis/chronic articular rheumatism” and “pregnanc* / Gravidity / Fertility / prepregnancy / preconception / gestation / fecundity” and “consensus / guideline* / clinical practices / criteria / standard / systematic review / Meta analysis /evidence summary”. An example of the PubMed search strategy is shown in Table 1.
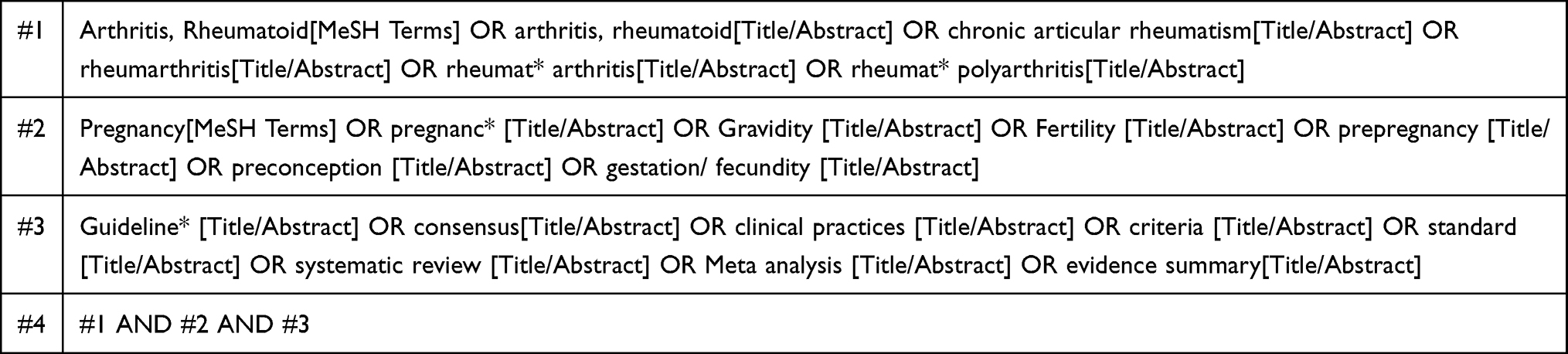 |
Table 1 PubMed Search Strategy |
Inclusion and Exclusion Criteria
Inclusion criteria: (1) Study population comprising childbearing-age RA patients; (2) Interventions or management strategies focused on preconception care for RA patients; (3) Publication types including guidelines, expert consensuses, clinical decisions, systematic reviews, and evidence summaries; (4) Articles published in either Chinese or English.Exclusion criteria: (1) Unavailable full texts or duplicate publications; (2) Interpretations or summary versions of guidelines or consensus documents; (3) Studies of poor methodological quality as assessed by the evaluation criteria.
Literature Quality Assessment Criteria and Process
Guidelines were appraised using the Appraisal of Guidelines for Research and Evaluation Instrument II (AGREE II);11 Expert consensus documents and systematic reviews were evaluated with the corresponding JBI critical appraisal tools;12,13 Clinical decisions were assessed using the Critical Appraisal for Summaries of Evidence (CASE) tool.14 The evaluation team comprised four postgraduates trained in evidence-based methodology and one evidence-based nursing specialist. While four reviewers independently assessed the guidelines, two reviewers evaluated other literature types. Any discrepancies were resolved through discussion with an additional evidence-based nursing expert.
Evidence Extraction and Summary
Two graduate students, trained in evidence-based nursing, independently extracted relevant information from the included studies. The extracted data encompassed literature sources, year of publication, subject matter, type of evidence, and specific content. This information was then cross-checked and integrated with the input of a third researcher (the corresponding author), followed by evidence summarization and synthesis, leading to the summarization and synthesis of the evidence. The principles for evidence synthesis were as follows for identical evidence, the most clearly and accessibly presented version was selected; when evidence contents were complementary, they were merged based on logical relationships; when evidence contents were independent, their original formulations were preserved; and in cases of conflicting conclusions from different sources, priority was given to evidence from authoritative literature with robust empirical support, higher study quality, and more recent publication dates.
Following evidence integration, the evidence was graded according to its source. Evidence from guidelines (which typically include pre-specified grading) was directly adopted. For evidence derived from clinical guidelines, expert consensus, and systematic reviews, the JBI Evidence Pre-Hierarchization and Recommendation System (2014 edition) was applied for grading and recommendation.15 Within this system, Level 1 represents the highest quality of evidence and Level 5 the lowest, while Grade A denotes a strong recommendation and Grade B a weak recommendation.
Result
Literature Search Results
Of the 1934 records identified through the initial search, 11 articles were included in this review following a systematic screening process. The included publications consisted of 2 clinical decision analyses,16,17 3 guidelines,18–20 5 expert consensus statements,21–25 and 1 systematic review.26 The flow diagram of the study selection process is shown in Figure 1, and the general characteristics of the included literature are presented in Table 2.
 |
Table 2 Basic Characteristics of the Included Literature (n=11) |
 |
Figure 1 The Flow Chart of Literature Screening. Abbreviations: JBI, Joanna Briggs Institute; NICE, National Institute for Health and Care Excellence; RNAO, Registered Nurses’ Association of Ontario; GIN, Guidelines International Network; ACR, American College of Rheumatology; BSR, British Society for Rheumatology; EULAR, European League Against Rheumatism. |
Results of Literature Quality Evaluation
Quality Evaluation of Clinical Decisions
Both clinical decision-making sources,16,17 which were derived from UpToDate, were included in our analysis. The quality appraisal revealed that for one source,17 all criteria were rated as “Yes” except for item 4. The other source16 was rated as “Yes” on all criteria except for item 4 and item 5. Despite these minor limitations, both sources were deemed to be of sufficient quality and were therefore included, as detailed in Table 3.
 |
Table 3 Quality Evaluation Results of Clinical Decision (n=2) |
Quality Evaluation of Guidelines
Three guidelines were included in this study.18–20 Two of these guidelines were rated as Grade A recommendations,18–20 with all domains scoring ≥60%. The guideline by Fang et al19 was rated as Grade B, as the “Independence” domain achieved a standardized percentage of only 47.92%, while all other domains scored ≥60%. Overall, the methodological quality of the guidelines was considered high, and all three were included. Detailed results are presented in Table 4.
 |
Table 4 Quality Evaluation Results of Guidelines (n=3) |
Quality Evaluation of Guidelines Expert Consensus
All five expert consensus documents21–25 satisfied all quality appraisal criteria, demonstrating high methodological quality and thus were included in the analysis. The detailed assessment is presented in Table 5.
 |
Table 5 Quality Evaluation Results of Expert Consensus (n=5) |
Quality Evaluation of of Systematic Reviews
This study included one systematic review,26 which fulfilled all quality appraisal items. It was considered to be of high quality and was retained in the final analysis.
Summary and Description of Evidence
A total of 23 evidence items were extracted, which were synthesized into best evidence for pre-pregnancy management of RA patients of childbearing age across seven domains: general principles, fertility risk assessment, pre-pregnancy screening, pre-pregnancy medication adjustment, fertility preservation, weight and nutrition management, and psychological support. The results are summarized in Table 6.
 |
Table 6 Evidence Summary of Preconception Management in Childbearing-Age Patients with RA (23 Items) |
Discussion
Adhering to Guiding Principles and Formulating a Scientific Preconception Management Plan
Evidence from items 1–4 outlines the general principles of preconception management in RA patients of reproductive age. A planned pregnancy is fundamental to reducing adverse outcomes. Preconception counseling facilitates medication review and adjustment to ensure gestational compatibility, enabling timely treatment optimization and stable disease control prior to conception.25 For RA patients not actively planning a pregnancy, effective contraception should be discussed to prevent unplanned pregnancies and potential teratogenic exposure from medications.27 Studies indicate that a multidisciplinary team approach is the most valuable source of information for family planning and reproductive choices in these patients and should be integrated into routine care.28 Therefore, rheumatologists should collaborate with gynecology, obstetrics, and nursing specialists to develop individualized preconception plans. This cooperation integrates cross-disciplinary resources, allowing for dynamic disease monitoring and comprehensive fertility assessment to ensure treatment safety and precise pregnancy timing. Furthermore, preconception management should adhere to the principle of shared decision-making, tailoring plans according to the patient’s disease activity, treatment goals, and reproductive needs. This ensures patients are fully informed and participate in decision-making, thereby safeguarding their reproductive health rights and alleviating disease- or treatment-related fertility anxieties.
Comprehensive Assessment of Fertility Risks to Optimize Pregnancy Outcomes
Comprehensive fertility risk assessment is vital for optimizing pregnancy outcomes in RA and should encompass disease activity, comorbidities, obstetric history, nutrition, anesthesia risk, and skeletal status. High disease activity elevates the risk of adverse pregnancy outcomes, and the Disease Activity Score in 28 joints (DAS28) is recommended before conception to confirm low activity or remission.7,26 As a systemic condition, RA frequently involves cardiovascular, pulmonary, and renal systems, and increases thrombosis risk, underscoring the need for preconception comorbidity screening.29,30 Obstetric history review may reveal prior miscarriage, preterm birth, stillbirth, or fetal anomalies; two or more pregnancy losses or stillbirths should prompt evaluation for antiphospholipid antibodies and gynecological disorders.22 Anesthesia and skeletal assessments are also critical, long-term glucocorticoid use and disease duration raise the risk of cervical subluxation, which can lead to paralysis or death during intubation under general anesthesia.31 Given the potential absence of symptoms, cervical spine radiography is indicated for all RA patients prior to general anesthesia, irrespective of disease duration or severity.32 Pelvic deformity may also influence delivery mode, requiring advance planning for cesarean section.22 Nutritional assessment helps reduce gestational complications and support fetal development. Future efforts should focus on developing standardized risk assessment tools incorporating individualized characteristics and dynamic monitoring are needed to guide optimal pregnancy timing.
Enhanced Preconception Screening and Early Identification of Pregnancy Risk Factors
The evidence from items 11–14 summarizes key aspects of preconception screening. Positivity for anti-Ro/SSA and anti-La/SSB antibodies represents a central risk factor for neonatal congenital atrioventricular block, which can progress from first-degree to complete block within 24 to 48 hours. In a minority of cases, timely diagnosis and initiation of treatment are achievable. Preconception screening is therefore essential, and patients with positive antibody results should be referred early to a perinatal center for multidisciplinary management.20,22 While antiphospholipid antibody positivity doubles miscarriage risk, routine screening in all women with RA is not supported due to variable reference ranges and inconsistent results,33 and testing should be considered only in those with prior miscarriage, abnormal coagulation times, or features suggestive of antiphospholipid syndrome given the low prevalence of positives.22 RA patients have a higher prevalence of thyroid dysfunction, which may impair fetal neurodevelopment,22 and the presence of hypothyroidism in anti-Ro/SSA- and anti-La/SSB-positive pregnant women further increases the risk of complete congenital heart block in offspring,34 warranting thyroid screening and specialist referral if hypothyroidism is detected. Additionally, as RA patients are at elevated risk for cervical cancer,35 cervical screening should be included in routine preconception assessment. Healthcare providers should therefore implement a standardized preconception screening checklist for this population to avoid omission of high-risk indicators.
Scientific Adjustment of Pre-Pregnancy Medication Plans to Reduce Teratogenic Risk
Evidence from items 15–18 summarizes the key considerations for preconception medication adjustment. Preconception medication management necessitates an individualized risk-benefit assessment. For women, medications with known embryotoxicity and teratogenicity (eg, methotrexate, cyclophosphamide) must be strictly avoided.21 Non-steroidal anti-inflammatory drugs (NSAIDs) are not recommended for those with infertility or recurrent pregnancy loss due to the risk of unruptured follicle syndrome. For men, a cumulative cyclophosphamide dose of ≥4000 mg/m2 poses a high risk of permanent azoospermia; therefore, fertility preservation options should be discussed prior to treatment initiation, and the drug should be discontinued at least 3 months before conception.21,36 Regarding traditional Chinese medicine, evidence suggests that Tripterygium wilfordii formulations carry reproductive toxicity.18 Based on evidence from studies on systemic lupus erythematosus,37 it is recommended that both sexes discontinue its use for at least 6 months, pending further studies to clarify this issue.20,21 Preconception treatment should be transitioned to pregnancy-compatible disease-modifying antirheumatic drugs (DMARDs) (eg, hydroxychloroquine, sulfasalazine, adalimumab). Critically, all medication adjustments must be planned 3–6 months in advance under specialist supervision, and patients must be explicitly cautioned against self-discontinuation.
Fertility Preservation Strategies for Patients Undergoing Gonadotoxic Therapy
Fertility preservation is imperative for patients exposed to gonadotoxic agents such as cyclophosphamide.38 Evidence items 19–20 outline key recommendations, include sex-specific approaches. For women with RA receiving monthly intravenous cyclophosphamide, which elevates the risk of premature ovarian insufficiency, concomitant administration of a gonadotropin-releasing hormone (GnRH) agonist is recommended to protect ovarian function. In male patients, sperm cryopreservation prior to therapy initiation is the preferred strategy to mitigate risks of infertility and long-term gonadal damage. Post-therapeutic sperm collection, if necessary, should be delayed for at least three months.20,38 For subfertile patients whose disease is stable and who test negative for antiphospholipid antibodies, assisted reproductive technology (ART) represents a viable option, as this patient selection helps mitigate the thrombotic risks associated with ovarian stimulation.20 However, a study in China highlighted significant disparities in physician awareness across specialties,39 underscoring the urgent need for enhanced professional education, streamlined referral pathways, and the promotion of multidisciplinary team (MDT) approaches to optimize fertility preservation outcomes.
Optimizing Preconception Health for Successful Pregnancy Outcomes
Evidence items 21–23 highlight the importance of preconception weight, nutrition, and psychological management for women with RA. Pre-pregnancy obesity is associated with higher risks of gestational diabetes, hypertension, cesarean delivery, and impaired initiation and duration of breastfeeding, potentially due to adiposity-related effects on prolactin and oxytocin.40 Recent guidelines also emphasize that weight control improves disease activity and prognosis in RA patients.18 Periconceptional folic acid supplementation is crucial for preventing fetal neural tube defects, often administered as part of a prenatal multivitamin;16,22 however, specific recommendations on the type, dosage, and timing of micronutrient supplementation for RA patients are lacking. As family planning can provoke anxiety and depression related to disease and parenting roles, mindfulness-based interventions have been shown to alleviate these symptoms.25 Future care models should integrate chronic disease management with preconception care, utilizing online health courses and psychological support platforms, and actively involving family members to enhance patient confidence.
Limitations
Although this study provides a comprehensive summary of evidence regarding pre-pregnancy management in women of reproductive age with RA, it only included literature published in English and Chinese, which may introduce language bias and affect the comprehensiveness and representativeness of the evidence. Moreover, due to variations in ethnicity, geographic regions, and cultural backgrounds across the included studies, the generalizability of the findings may be limited. Therefore, when applying the findings of this study into clinical practice, healthcare professionals are advised to consider the specific context, thoroughly evaluate individual patient characteristics and actual needs, and collaboratively develop safe, effective, and personalized management plans through multidisciplinary team discussions. Future research should continue to update and expand the relevant evidence to further enhance its applicability and practical guidance.
Conclusion
This study synthesizes 23 best evidence-based recommendations for preconception management in RA patients of childbearing age, constructing a comprehensive framework encompassing seven key domains: general principles, fertility risk assessment, preconception screening, pre-pregnancy medication adjustment, fertility preservation, weight and nutrition management, and psychological support. The main findings underscore the critical importance of planned pregnancy, multidisciplinary collaboration, comprehensive risk assessment, and appropriate medication adjustment in optimizing pregnancy outcomes. The findings provide a robust evidence-based foundation for standardizing preconception care. To bridge the gap between evidence and clinical practice, future efforts must integrate these recommendations with individual patient characteristics and clinical realities. This approach is essential for developing scientific and systematic preconception management strategies, thereby effectively mitigating pregnancy-related risks and optimizing maternal and fetal outcomes.
Data Sharing Statement
The data supporting the findings of this study are available within this article and are also openly available in the Fudan University Center for the Evidence-based Nursing repository at http://ebn.nursing.fudan.edu.cn, reference number ES20258177.
Ethics Statement
Ethical approval is not applicable for this study, as it is based solely on a review of publicly available literature.
Funding
This study was supported by a research grant from the Shanxi Administration of Traditional Chinese Medicine (Project No. 2023ZYYC2056). The funder had no role in the study design, data collection, analysis, or preparation of the manuscript.
Disclosure
The authors declare no conflicts of interest.
References
1. Di Matteo A, Bathon JM, Emery P. Rheumatoid arthritis. Lancet. 2023;402(10416):2019–2033. doi:10.1016/S0140-6736(23)01525-8
2. RJ Black, M Cross, LM Haile, et al. Global, regional, and national burden of rheumatoid arthritis, 1990–2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(10):e594–e610. doi:10.1016/S2665-9913(23)00211-4
3. Wang CY, Zhao L, Luo XH. Management of pregnant women with rheumatoid arthritis. Chin J Rheumatol. 2022;26(10):709–713. doi:10.3760/cma.j.cn141217-20211009-00406
4. Zi X, Yan H, Fan H, et al. OP0240-HPR GLOBAL, Regional and national burden of rheumatoid arthritis in women of childbearing age from 1990 to 2021: findings from the global burden of disease study 2021. Ann Rheum Dis. 2025;84:198–199. doi:10.1016/j.ard.2025.05.250
5. Sims C, Talabi MB. Family Planning and Rheumatoid Arthritis. Curr Rheumatol Rep. 2025;27(1):26. doi:10.1007/s11926-025-01191-y
6. Sim BL, Daniel RS, Hong SS, et al. Pregnancy Outcomes in Women With Rheumatoid Arthritis: a Systematic Review and Meta-analysis. Jcr-J Clin Rheumatol. 2023;29(1). doi:10.1097/RHU.0000000000001935
7. Saulescu IC, Panaitescu AM, Gică N, et al. Pre-Pregnancy Counselling for Women with Rheumatoid Arthritis: a Guide on Risks, Evaluations, and Multidisciplinary Approaches. J Clin Med. 2024;14(1). doi:10.3390/jcm14010114
8. El Miedany Y, Palmer D. Rheumatology-led pregnancy clinic: enhancing the care of women with rheumatic diseases during pregnancy. Clin Rheumatol. 2020;39(12):3593–3601. doi:10.1007/s10067-020-05173-6
9. Bobircă A, Simionescu AA, Mușetescu AE, et al. Outcomes of Prospectively Followed Pregnancies in Rheumatoid Arthritis: a Multicenter Study from Romania. Life-Basel. 2023;13(2):359. doi:10.3390/life13020359
10. Zhu Z, Hu Y, Xing WJ, Zhou YF, Gu Y. Composition of different types of evidence-based questions. Nurs Train J. 2017;32(21):1991–1994. doi:10.16821/j.cnki.hsjx.2017.21.025
11. Brouwers MC, Kerkvliet K, Spithoff K. The AGREE Reporting Checklist: a tool to improve reporting of clinical practice guidelines. BMJ-Brit Med J. 2016;352:i1152. doi:10.1136/bmj.i1152
12. The Joanna Briggs Institute (JBI). Checklist for text and opinion[EB/OL]. 2020. Available from: https://jbi.global/critical-appraisal-tools.
13. The Joanna Briggs Institute (JBI). Checklist for systematic reviews and research syntheses[EB/OL]. 2025. Available from: https://jbi.global/critical-appraisal-tools.
14. Foster MJ, Shurtz S. Making the Critical Appraisal for Summaries of Evidence (CASE) for evidence-based medicine (EBM): critical appraisal of summaries of evidence. J Med Libr Assoc. 2013;101(3):192–198. doi:10.3163/1536-5050.101.3.008
15. Wang CQ, Hu Y. JBI evidence pre-grading and recommendation level system (2014 version). Nurs Train J. 2015;30(11):964–967. doi:10.16821/j.cnki.hsjx.2015.11.00210.16821/j.cnki.hsjx.2015.11
16. Bermas BL. Rheumatoid arthritis and pregnancy[EB/OL]. 2025. Available from: https://www.uptodate.com/contents/zh-Hans/rheumatoid-arthritis-and-pregnancy?search.
17. Bermas BL. Effects of antiinflammatory and immunosuppressive drugs on gonadal function and teratogenicity in males with rheumatic diseases[EB/OL]. 2024. Available from: https://www.uptodate.com/contents/zh-Hans/effects-of-antiinflammatory-and-immunosuppressive-drugs-on-gonadal-function-and-teratogenicity-in-males-with-rheumatic-diseases?search.
18. National Clinical Research Center for Dermatologic and Immunologic Diseases of Peking Union Medical College Hospital. Rheumatology Physician Branch of Chinese Medical Doctor Association, Rheumatology Rehabilitation Professional Committee of Chinese Association of Rehabilitation Medicine, et al. 2024 China rheumatoid arthritis diagnosis and treatment guidelines [J]. Chin J Intern Med. 2024;63(11):1059–1077. doi:10.3760/cma.j.cn112138-20240531-00360
19. Fang LK, Huang CH, Xie Y, et al. Patient practice guideline for rheumatoid arthritis. Chin J Intern Med. 2020;59(10):772–780. doi:10.3760/cma.j.cn112138-20200807-00734
20. Sammaritano LR, Bermas BL, Chakravarty EE, et al. American College of Rheumatology Guideline for the Management of Reproductive Health in Rheumatic and Musculoskeletal Diseases. Arthritis Rheumatol. 2020;72(4):529–556. doi:10.1002/art.41191
21. Rüegg L, Pluma A, Hamroun S, et al. EULAR recommendations for use of antirheumatic drugs in reproduction, pregnancy, and lactation: 2024 update. Ann Rheum Dis. 2025;84(6):910–926. doi:10.1016/j.ard.2025.02.023
22. Tanaka Y, Murashima A, Atsumi T, et al. The management of women of childbearing age with rheumatoid arthritis: an expert report. Expert Rev Clin Immu. 2023;19(6):655–669. doi:10.1080/1744666X.2023.2197212
23. Chinese Expert Group for the Development of Off-Label Drug Use Consensus in Rheumatoid Arthritis. Chinese expert consensus on off-label drug use for rheumatoid arthritis (2022 edition). Chin Med J. 2022;102(15):1076–1085. doi:10.3760/cma.j.cn112137-20220120-00152
24. Martínez López JA, García Vivar ML, Cáliz R, et al. Recommendations for the evaluation and management of patients with rheumatic autoimmune and inflammatory diseases during the reproductive age, pregnancy, postpartum and breastfeeding. Reumatol Clin. 2017;13(5):264–281. doi:10.1016/j.reuma.2016.05.003
25. Briggs AM, Jordan JE, Ackerman IN, et al. Establishing cross-discipline consensus on contraception, pregnancy and breast feeding-related educational messages and clinical practices to support women with rheumatoid arthritis: an Australian Delphi study. BMJ Open. 2016;6(9):e012139. doi:10.1136/bmjopen-2016-012139
26. Lv J, Xu L, Mao S. Association between disease activity of rheumatoid arthritis and maternal and fetal outcomes in pregnant women: a systematic review and meta-analysis. Bmc Pregnancy Childb. 2023;23(1):724. doi:10.1186/s12884-023-06033-2
27. Ingram E, Claus L, Kolfenbach J, et al. Contraceptive Use in Women of Childbearing Ability With Rheumatoid Arthritis. Jcr-J Clin Rheumatol. 2021;27(3). doi:10.1097/RHU.0000000000001184
28. Olejárová M, Macejová Z, Gkalpakiotis S, et al. Reproductive Healthcare in Women with Rheumatoid Arthritis and Psoriatic Diseases in Routine Clinical Practice: survey Results of Rheumatologists and Dermatologists. Rheumatol Ther. 2022;9(6):1575–1586. doi:10.1007/s40744-022-00488-z
29. Misra DP. Clinical manifestations of rheumatoid arthritis, including comorbidities, complications, and long-term follow-up. Best Pract Res Cl Rh. 2025;39(1):102020. doi:10.1016/j.berh.2024.102020
30. Fazal ZA, Avina-Galindo AM, Marozoff S, et al. Risk of venous thromboembolism in patients with rheumatoid arthritis: a meta-analysis of observational studies. Bmc Rheumatol. 2024;8(1):5. doi:10.1186/s41927-024-00376-9
31. Zhu S, Xu W, Luo Y, et al. Cervical spine involvement risk factors in rheumatoid arthritis: a meta-analysis. Int J Rheum Dis. 2017;20(5):541–549. doi:10.1111/1756-185X.13096
32. Neva MH, Häkkinen A, Mäkinen H, et al. High prevalence of asymptomatic cervical spine subluxation in patients with rheumatoid arthritis waiting for orthopaedic surgery. Ann Rheum Dis. 2006;65(7):884–888. doi:10.1136/ard.2005.042135
33. El Hasbani G, Viola M, Sciascia S, et al. Antiphospholipid Antibodies in Inflammatory and Autoimmune Rheumatic and Musculoskeletal Diseases Beyond Lupus: a Systematic Review of the Available Evidence. Rheumatol Ther. 2021;8(1):81–94. doi:10.1007/s40744-020-00273-w
34. Spence D, Hornberger L, Hamilton R, et al. Increased risk of complete congenital heart block in infants born to women with hypothyroidism and anti-Ro and/or anti-La antibodies. J Rheumatol. 2006;33(1):167–170.
35. Xu M, Chen H, Tan T, et al. Exploring the causal association between rheumatoid arthritis and the risk of cervical cancer: a two-sample Mendelian randomization study. Arthritis Res Ther. 2024;26(1):35. doi:10.1186/s13075-023-03240-2
36. Huang I, Fantus RJ, Halpern JA, et al. Association of the minimal cyclophosphamide equivalent dose and outcome of microdissection testicular sperm extraction in patients with persistent azoospermia after chemotherapy. F S Rep. 2024;5(1):95–101. doi:10.1016/j.xfre.2023.11.005
37. National Clinical Research Center for Skin and Immune Diseases, et al. Chinese guidelines for the management of reproduction and pregnancy in patients with systemic lupus erythematosus. Chin J Intern Med. 2022;61(11):1184–1205. doi:10.3760/cma.j.cn112138-20220821-00612
38. Chinese Society of Fertility Preservation, Chinese Maternal and Child Health Association. Expert consensus on clinical practice of female fertility preservation in China. Chin J Reprod Contracep. 2021;41(5):383–391. doi:10.3760/cma.j.cn101441-20210228-00092
39. Song XL, Zhang XY, Zhen XM, et al. Cognitive survey and analysis of multidisciplinary clinicians on fertility preservation in China. Chin J Reprod Contracep. 2025;45(5):448–452. doi:10.3760/cma.j.cn101441-20250228-00098
40. Marchewka-Długońska J, Nieczuja-Dwojacka J, Krygowska K, et al. Effects of pre-pregnancy BMI and gestational weight gain on pregnancy and neonatal outcomes in Poland. Sci Rep-Uk. 2025;15(1):7603. doi:10.1038/s41598-025-91879-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Evidence-Based Medical Review on Promoting Gastrointestinal Function Recovery After Colorectal Cancer Surgery
Zhao CY, Shi WH, Wen ZQ, Jin YM, Shang YB, Zheng L, Li J, Chen XM
Journal of Multidisciplinary Healthcare 2024, 17:1343-1362
Published Date: 23 March 2024
Evidence Summary of Personalized Management of Peritoneal Dialysis Volume in Adults
Yu C, Sha P, Jiang Z, Wei Y, Gong B, Jiang S, Wang R
Journal of Multidisciplinary Healthcare 2025, 18:2707-2719
Published Date: 15 May 2025
An Evidence-Based Medical Review on Preoperative Exercise Prehabilitation in Lung Cancer Patients
Zhang R, Wu M, Cheng Y, Xu Y, Xia L
Journal of Multidisciplinary Healthcare 2025, 18:4849-4858
Published Date: 7 August 2025
Summary of Best Evidence for Psychosocial Interventions in Adults with Alcohol Use Disorder: An Evidence-Based Review
Yan L, Ji CF, Xia LP, Sun W, Shi JQ, Wu XD
Journal of Multidisciplinary Healthcare 2025, 18:6315-6327
Published Date: 2 October 2025
Best Evidence for Preventing Urinary Tract Infections and Optimizing Care in Adults with Indwelling Urinary Catheters
Tang J, Fan Y, Lu J, Zhang Y
Risk Management and Healthcare Policy 2025, 18:3593-3608
Published Date: 11 November 2025