Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Best Evidence for the Exercise-Based Management of Lower Limb Lymphedema After Gynecological Cancer: A Systematic Review and Evidence Synthesis
Authors Zhang C, Soh KL, Yubbu P, Chen J ![]() , Yang L, Chen Y, Wu J
, Yang L, Chen Y, Wu J
Received 11 December 2025
Accepted for publication 14 May 2026
Published 20 May 2026 Volume 2026:19 588181
DOI https://doi.org/10.2147/JMDH.S588181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Judith Johnson
Chaonan Zhang,1,2 Kim Lam Soh,1 Putri Yubbu,3 Jian Chen,4 Lizhi Yang,5 Yingying Chen,6 Jing Wu2
1Nursing Department, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia, Serdang, SGR, Malaysia; 2Department of Nursing, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 3Department of Pediatrics, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia, Serdang, SGR, Malaysia; 4Department of Environmental and Occupational Health, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia, Serdang, SGR, Malaysia; 5Health Medical College, Zhejiang DongFang Polytechnic, Wenzhou, Zhejiang, People’s Republic of China; 6School of Nursing, Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
Correspondence: Kim Lam Soh, Nursing Department, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia, Serdang, SGR, Malaysia, Email [email protected] Jing Wu, Department of Nursing, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China, Email [email protected]
Purpose: Lower limb lymphedema after gynecological cancer treatment significantly impairs quality-of-life, increases care needs, and escalates costs. Despite exercise benefits, evidence-based guidance on optimal interventions is lacking. This study addresses this gap by conducting a systematic review and evidence synthesis of current guidelines and high-quality studies.
Patients and Methods: A systematic search was conducted based on the hierarchical “ 6S” evidence model to retrieve high-quality evidence. Searches in PubMed, CINAHL, Embase, Web of Science, Ovid, BMJ Best Practice, UpToDate, Cochrane Library, major guideline repositories, and PEDro identified guidelines, systematic reviews, recommended practices, evidence summaries, clinical decisions, and expert consensuses on exercise therapy (inception to February 2025). Two reviewers independently screened, evaluated, extracted, and synthesized evidence using the JBI system.
Results: Seventeen publications were included. Synthesis across nine domains yielded 32 recommendations. Key findings: recommendations related to patients without active infections or lymphatic leakage only; conduct pre-exercise assessments by qualified professionals; recommend combined aerobic and resistance training. Aquatic therapy, low-impact exercises, and moderate-to-vigorous intensity exercise were beneficial/safe with individualized guidance; use appropriate compression garments during exercise; provide tailored supervision to enhance compliance. Evidence levels and grades specified.
Conclusion: This review provides a structured synthesis of the best available evidence for exercise management of lower limb lymphedema in gynecological cancer survivors, covering nine critical aspects. Findings offer a practical guide for clinicians designing interventions.
Keywords: gynecology, lower limb lymphedema, exercise, best evidence, cancer
Introduction
Gynecological cancers include cervical, ovarian and other cancers of the female reproductive organs, and represent a significant global health burden. These cancers are associated with high incidence and mortality rates, huge economic costs, psychological and social stigmatization, the impairment of reproductive function and the uneven distribution of medical resources.1 In 2022, approximately 1,473,427 new cases of gynecological cancer were reported worldwide, with an age-standardized incidence rate of 30.3 per 100,000 women.2 These cancers rank among the most common malignancies in women,3 and their incidence is projected to increase over the next two decades if current trends persist.2 Progress in screening and therapeutic approaches has led to significant gains in survival outcomes for gynecological malignancies, thus prompting increased emphasis on improving quality-of-life after treatment. Surgery, notably pelvic lymphadenectomy, remains the cornerstone of treatment for these cancers. In advanced stages, radiotherapy and chemotherapy are commonly employed; however, such interventions may impair lymphatic function, potentially resulting in lower limb lymphedema (LLL).4
LLL originates from impairment of the lymphatic system and the disruption of lymph flow, thus causing edema in one or both lower limbs due to the excessive accumulation of water, plasma proteins, extracellular blood cells, and cellular byproducts.5 Symptoms, such as edema, weightiness, discomfort, and recurrent infections, can frequently impair daily functionality and adversely affect the well-being of survivors of gynecological cancer with lower limb lymphedema.6 The timely management of LLL is crucial, as this condition can hinders a patient’ s mobility while also representing a potential risk for the development into cellulitis, ultimately reducing the quality-of-life for some patients.7 The fear of movement or exacerbating symptoms (kinesiophobia) can be a significant psychological barrier, further limiting physical activity and rehabilitation efforts. Furthermore, the management of lower limb lymphedema presents unique physiological challenges compared to upper limb involvement, primarily due to the significant influence of gravity and orthostatic pressure on lymphatic drainage in the lower extremities.
Although LLL is a chronic condition that cannot be cured, effective control can be achieved by complete decongestive therapy (CDT), including skin care, manual lymphatic drainage (MLD), exercise, and compression therapy.8 Physical activity and exercise stimulate the muscle venous pump to promote the circulation of lymphatic fluid, thus helping to alleviate swelling and enhance overall well-being.9 The latest expert consensus from the International Society of Lymphology (ISL) recommends exercise therapy for patients with cancer-related lower limb lymphedema.10
The number of research studies relating to the use of exercise for lower limb lymphedema in patients with gynecological cancer is extremely limited and there is a lack of specific exercise implementation plans for patients with lower limb lymphedema, such as exercise contraindications, exercise frequency, exercise time and exercise intensity. A evidence summary suggested that exercise may achieve slight improvements in pain, function, and the quality-of-life in patients suffering from lower limb lymphedema, although the quality of the evidence available was low and findings varied across different studies.11 Previous reviews have predominantly investigated exercise interventions for breast cancer-related lymphedema (BCRL),12,13 as this condition is more prevalent in the upper limbs when compared to other types of lymphedemas.14 However, findings from BCRL exercise studies may not be directly applicable to individuals with lower limb lymphedema, thus necessitating targeted research for this distinct patient group. Unlike previous reviews that have primarily focused on breast cancer-related lymphedema or reported general effects of exercise, this study specifically targets lower limb lymphedema in survivors of gynecological cancer. Moreover, rather than solely summarizing intervention outcomes, this study provides a structured synthesis of exercise-based management, including detailed components such as contraindications, assessment, exercise prescription, safety, and patient education, thereby translating evidence into practical guidance for clinical implementation.
In this study, we retrieved high-quality evidence focused on using exercise to manage lower limb lymphedema in patients following gynecological cancer treatment, and extracted, summarized, and analyzed the data to develop evidence-based guidelines for clinical care providers to create scientific and effective exercise regimens tailored to this group. The aim of this study was to systematically synthesize the best available evidence for the exercise-based management of lower limb lymphedema in survivors of gynecological cancer, providing a robust foundation for future clinical practice.
Materials and Methods
This review was conducted in accordance with the JBI methodology for evidence synthesis and is reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Search Strategy
A systematic search was conducted based on the hierarchical “6S” evidence model, which classifies evidence sources into six levels (Systems, Summaries, Synopses of Syntheses, Syntheses, Synopses of Studies, and Studies), to retrieve high-quality evidence. The purpose of The research question was formulated using the PIPOST framework, which includes Population, Intervention, Professionals, Outcomes, Setting, and Type of evidence.15 We screened a wide range of databases, including PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase, Web of Science, Ovid, BMJ Best practice, UpToDate, Cochrane Library, Clinical Online Network of Evidence for Care and Therapeutics (JBI CONNECT+), National Institute for Health and Care Excellence (NICE), National Guideline Clearinghouse (NGC), ECRI Guidelines TrustTM, Guideline International Network (GIN), Scottish Intercollegiate Guidelines Network (SIGN), National Comprehensive Cancer Network (NCCN), Registered Nurses’ Association of Ontario (RNAO), National Lymphedema Network (NLN), International Society of Lymphology (ISL), and the Physiotherapy Evidence Database (PEDro).
Search terms were created based on the combination of Medical Subject Headings and free terms, as follows: (gynaecolog* / gynecolog* / endometri* / cervi* / ocer* / vagina*) AND (tumor* / tumour* / cancer* / malignan* /neoplas*) AND (lymphoedem* / lymphodem* / lymph*tic / lymphedema* / swelling* / edema* / oedema*) AND (lower limb*” / “membrum inferius” / leg* / “lower extremit*) AND (exercis* / physical activit* / movement* / physical therap* / physiotherap* / strength train* / resistance train* / aerobic fitness* / weight train* / stretching exercis* / kinesiotherap* / Water Sport*). The timeframe for our literature research was from database inception to the 2nd of February 2025. Specific search terms are described in Table S1–S6.
Literature Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) patients diagnosed with lower limb lymphedema following treatment for gynecological cancers; (2) studies that included exercise interventions and provided detailed descriptions of exercise type, exercise timing, exercise protocols (including phases or steps), exercise management strategies, and exercise assessment methods; (3) the included outcome measures encompassed lymphedema symptoms, edema severity, muscle strength, and quality-of-life; (4) research types include guidelines, expert consensuses, evidence summaries, recommended practice, clinical decisions, randomized controlled trials, and systematic reviews; and (5) the articles were published in English. Consistent with the “6S” hierarchical model of evidence, this review employed a top-down selection strategy. Priority was explicitly given to pre-appraised and synthesized evidence at the apex of the pyramid, such as clinical practice guidelines, evidence summaries, and systematic reviews. Primary studies, including randomized controlled trials (RCTs), were included only when they addressed critical aspects of exercise prescription (eg., detailed parameters of frequency, intensity, time, and type) that were not sufficiently detailed or were absent in the higher-level synthesized evidence (guidelines, systematic reviews) for the population of interest.
The exclusion criteria were as follows: (1) outdated clinical practice guidelines; (2) an incomplete set of data/information; (3) evidence that did not pass quality assessment; and (4) and cases where we were unable to obtain the full text.
Study Selection and Data Extraction
LZY and YYC separately evaluated the retrieved literature based on pre-defined eligibility criteria. Any discrepancies were addressed by discussion to achieve a consensus, with a third author consulted if needed. Subsequently, both reviewers independently extracted data using a standardized data extraction form, working without knowledge of each other’s extractions. The extracted information included study attributes such as the lead author’s name and institution, the publication year, source, evidence category, and the focus of the article.
Potential overlap between included systematic reviews and directly included RCTs was assessed by comparing the primary studies included in each review with the included RCTs. Two RCTs (Abe et al, 2021; Fukushima et al, 2017) were found to overlap with the systematic review by Hsu et al (2024), while no overlap was identified with Stout et al (2020). To avoid double counting, overlapping studies were considered only once during evidence synthesis. For these studies, information was extracted directly from the original RCT reports rather than from the systematic review.
Quality Evaluation Criteria
Guideline
The quality of the included guidelines was evaluated using the Clinical practice Guideline Research and Evaluation System (Appraisal of Guidelines for Research and Evaluation, AGREE II).16 This tool consists of six domains and 23 items. The six domains include: scope and purpose, stakeholder involvement, rigor of development, clarity of presentation, applicability and editorial independence. Each item was rated on a 7-point Likert scale from 1 (strongly disagree) to 7 (strongly agree). The score for each domain was calculated with a specific formula: [(obtained score - minimum score)/(maximum score - minimum score)]*100%. Based on domain scores and expert judgement, guidelines were classified into three recommendation levels: Grade A (strong recommendation), Grade B (weak recommendation) and Grade C (not recommended). This structured evaluation ensured that we adopted a standardized and objective assessment of existing clinical guidelines.
Systematic Reviews and Expert Consensuses
The quality of the included systematic reviews and expert consensus articles was evaluated using appropriate critical appraisal tools developed by the Joanna Briggs Institute (JBI, 2016). Different tools were applied according to the type of evidence, as recommended for methodological rigor in evidence synthesis.
The JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses was used to evaluate the included systematic reviews.17 This tool comprises 11 assessment criteria, covering aspects such as the clarity of the research question, the appropriateness of the inclusion criteria, the comprehensiveness of the search strategy, and the validity of methods used to combine studies. Each criterion is rated as “yes”, “no”, “unclear”, or “not applicable”.
The JBI Critical Appraisal Checklist for Textual Evidence: Expert Opinion was used to assess expert consensus articles.18 This tool includes six criteria focusing on the credibility and trustworthiness of expert opinion, such as the clarity of the source of opinion, the expertise and authority of the author, the logical consistency of the argument, and the extent to which the opinion is supported by existing evidence. Each criterion is rated as “yes”, “no”, “unclear”, or “not applicable”.
Clinical Decision
Clinical decisions rely on high-quality evidence and directly cite this evidence. This not only improves treatment outcomes but also ensures the safety and satisfaction of patients. Through systematic retrieval, rigorous evaluation, and rational application of evidence, clinicians can make more scientific and effective decisions.
Randomized Controlled Trials
The Revised Cochrane RoB 2 tool was designed to evaluate the risk of bias in randomized controlled trials.19 This tool encompasses five domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias when measuring the outcome, and bias when selecting the reported result. Each domain is systematically assessed, and individual items are rated as having “low risk”, “some concerns”, or a “high risk” of bias. Based on these ratings, an overall judgment of the trial’s risk of bias for a specific trial can be made at the study level, thus reflecting the extent to which bias may affect the validity of its results.
Literature Quality Evaluation Process
Two researchers with a background in evidence-based nursing independently evaluated the quality of all literature by type. Disagreements were resolved by a third evidence-based nursing expert acting as an arbitrator. The inclusion principle for the evidence in this study was to prioritize evidence-based and high-quality evidence, while also considering the time at which the evidence was published.
Criteria for Determining the Levels of Evidence and Recommendation
The included studies were evaluated and assigned recommendations using the JBI Evidence and Recommendation Framework.20 Evidence was classified into tiers 1 to 5 based on study design. Furthermore, the JBI FAME criteria were used to evaluate the feasibility, appropriateness, meaningfulness, and effectiveness of the evidence; these findings allowed us to determine the strength of our recommendations, categorized as A-level (strong) or B-level (weak). These steps were conducted independently, and no composite scoring system was used to combine different appraisal results into a single metric.
Results
General Characteristics of the Included Literature
Our initial search yielded 333 records from databases including UpToDate (n=7), PEDro (n=23), NLN (n=4), NGC (n=4), NCCN (n=4), GIN (n=2), ECRI Guidelines TrustTM (n=3), JBI CONNECT+ (n=9), JBI EBP Database (n=14), NICE (n=3), BMJ Best practice (n=4), Cochrane Library (n=38), PubMed (n=44), Web of Science (n=75), Embase (n=10), Ovid (n=70), CINAHL (n=16), and ISL (n=3). Excluding duplicates and those that did not meet our requirements after reading the title, abstract and full text, a total of 13 publications were included in our final analysis. In addition, one JBI evidence summary21 was traced back to its original references, resulting in the inclusion of three guidelines, one expert consensus, and one evidence summary. Therefore, a total of 18 articles were obtained. However, as the evidence was summarized using primary research methods, the final number of articles included in the analysis was 17, consisting of 1 clinical decision support document,22 three expert consensus statements,10,23,24 seven guidelines,25–31 four randomized controlled trials32–35 and two systematic review.36,37 The study selection process is presented in Figure 1, and general information relating to the included literature is shown in Table 1.
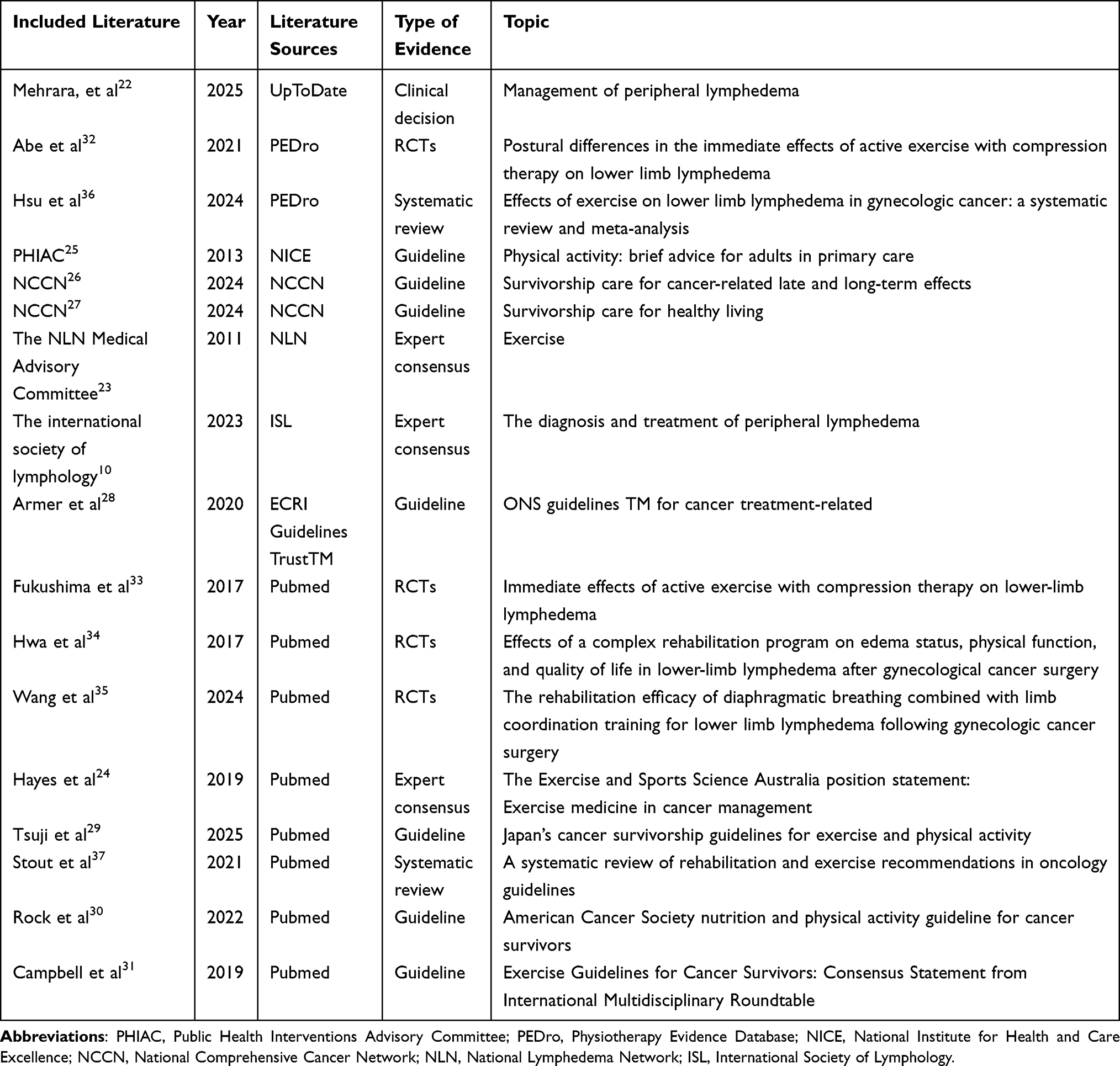 |
Table 1 General Information Extracted from the Included Literature (n = 17) |
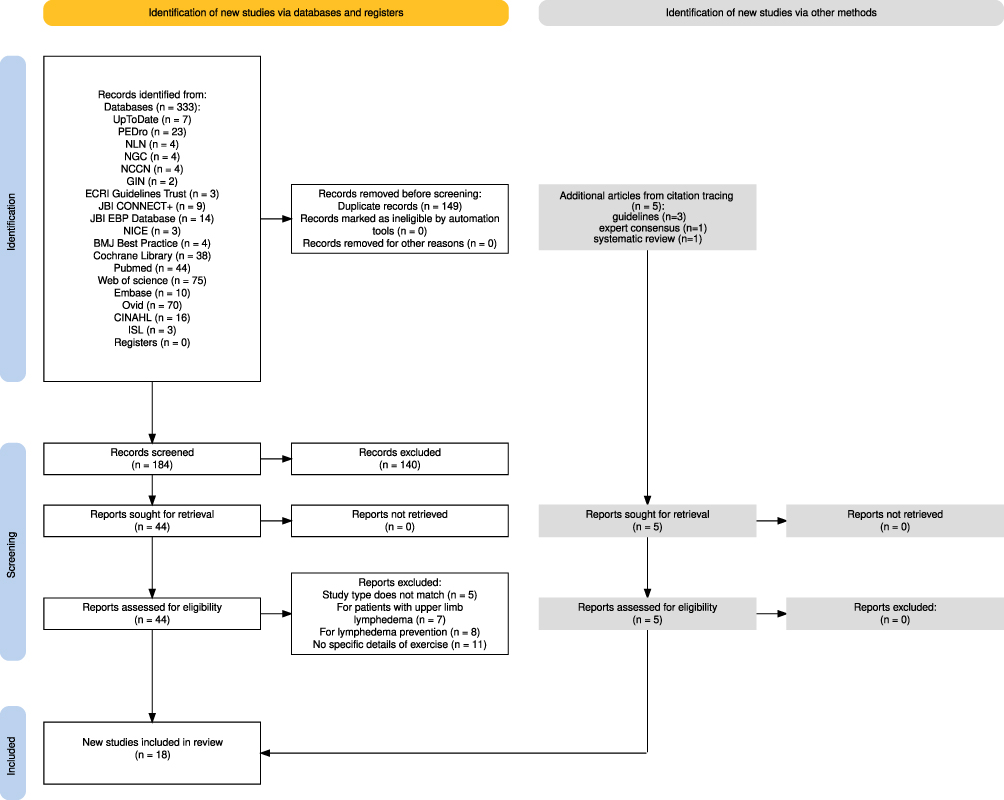 |
Figure 1 PRISMA (Preferred Reporting Items for evidence summaries) flowchart describing the study selection process. |
Quality Evaluation of the Included Literature
Quality Evaluation of the Guidelines
This review incorporated seven guidelines.25–31 Four guidelines25,29–31 achieved at least 60% compliance across six domains, earning a strong recommendation (A-level). The remaining three guidelines26–28 received a weak recommendation (B-level). Table 2 presents the compliance scores for each domain and the comprehensive quality assessment of the guidelines.
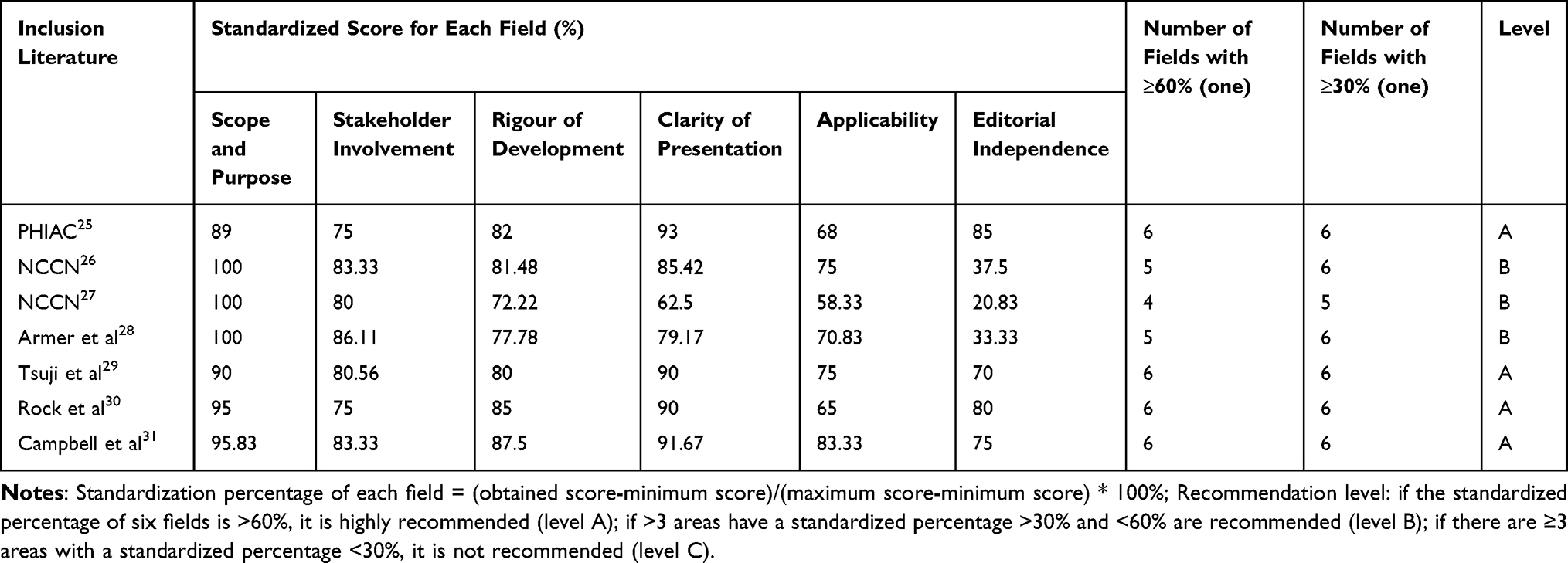 |
Table 2 Quality Evaluation of the Guidelines (n = 7) |
Quality Evaluation of Systematic Reviews
Two articles36,37 were evaluated and were approved for inclusion. Detailed quality assessment details are presented in Table S7.
Quality Evaluation results of Expert Consensuses
Three expert consensus articles10,23,24 were independently evaluated by two evaluators according to the JBI expert opinion quality evaluation tool and approved for inclusion. Detailed quality assessment details are presented in Table S8.
Quality Evaluation of Randomized Controlled Experiments
Four RCTs32–35 were evaluated in this study. Although some of the included RCTs were judged to have a high risk of bias, all eligible studies were included in the synthesis of evidence to provide a comprehensive assessment. The risk of bias was considered according to the GRADE evaluation and was reflected in the certainty of the evidence. The detailed RoB 2 risk of bias assessment results for the included RCTs are presented in Supplementary Figure S1.
Quality Evaluation of Clinical Decisions
Our analysis included one clinical decision-making article which was up-to-date and defaulted to high-level evidence.
Summary and Description of Evidence
Exercise Contraindications and Assessment
Early screening and evaluation are of great significance for exercise interventions in cases of LLL and are also the prerequisite for the management of exercise for patients. Based on our analysis, we recommend that patients with active infections (eg., cellulitis, erysipelas, or infected/scarred/inflamed skin), vascular complications (such as deep vein thrombosis, severe aneurysms, or pulmonary embolism), severe dysfunction of vital organs (heart, liver, or kidneys), lymphatic leakage, or cancer recurrence/metastasis risk, as well as those with communication or adherence difficulties, should be excluded from exercise interventions.32–35 These criteria highlight the importance of conducting systematic pre-exercise assessments and suggest the need to develop alternative rehabilitation strategies that are tailored for individuals with specific contraindications.
Health Education
Patient education is the cornerstone of self-management, yet our review found that specific educational strategies are often under-reported. Effective education must go beyond information giving; it requires empowering patients with the skills to recognize “normal” exertional responses versus pathological symptom exacerbation.24 Nurses should utilize behavioral change techniques, such as goal setting and self-monitoring (using diaries or apps), which have been shown to improve self-efficacy.10,21,24 Educational content should also frame exercise positively—focusing on improvements in strength, mood, and energy—to counteract kinesiophobia (fear of movement) common in this population.26
Exercise Precautions
While exercise can be beneficial, its implementation in patients with lymphedema should be introduced gradually and progressed with caution, as the emergence of symptoms such as pain, swelling, or discomfort may indicate physiological overload or exacerbation of the condition.23 This highlights the need for continuous symptom assessment throughout the intervention. In addition, environmental factors should not be overlooked. Exposure to temperature extremes, such as saunas or steam baths during or surrounding exercise sessions may exacerbate the symptoms of lymphedema and should be avoided.22 Moreover, while the financial burden associated with exercise interventions is generally minor, it may still become a barrier to consistent participation for some patients.29 This highlights the importance of developing cost-conscious exercise strategies and ensuring access to affordable rehabilitation programs to enhance adherence and long-term outcomes.
Findings were retrieved from the selected literature and assessed using the JBI evidence and recommendation framework, as described above. Each item of evidence was assigned a level of evidence (Levels 1–5) and a strength of recommendation (Grade A or B) based on the JBI criteria and FAME framework. Following integration of the evidence, our findings were organized into nine domains: exercise contraindications, pre-exercise assessment, exercise modality, exercise intensity, exercise prescription, exercise safety, exercise supervision and adherence, exercise education and exercise precautions for patients with gynecological cancer-related lower limb lymphedema, and 32 best evidences were formed, as presented in Table 3.
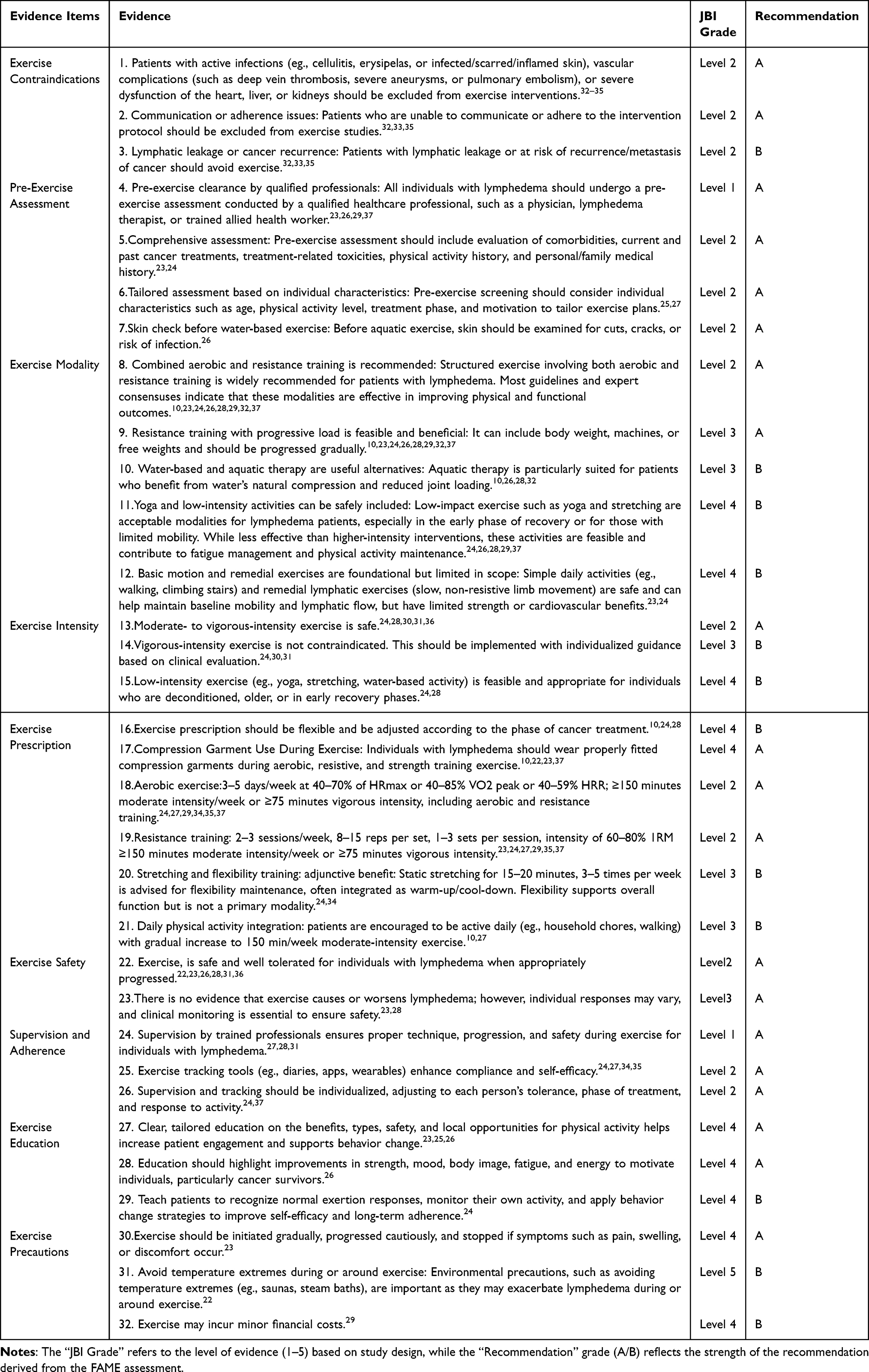 |
Table 3 Summary of Best Evidence |
Value of Summarizing Exercise Evidence for LLL Management
Lower limb lymphedema is physiologically distinct from upper limb lymphedema due to the impact of orthostatic pressure and gravity on lymphatic drainage.38 Consequently, exercise prescriptions cannot simply be extrapolated from BCRL guidelines. The active management of LLL requires a nuanced balance between muscle pump activation and gravity-dependent fluid accumulation. This review synthesizes evidence to guide clinicians in designing interventions that are not only effective but also prioritize patient safety and adherence.
Although physical activity is a key component in lymphedema, previous research indicated that women may avoid physical exercise with LLL due to concerns relating to symptom exacerbation and disease progression.39 However, a evidence summary of seven exercise interventions for lower limb lymphedema in gynecological cancer reported that three studies observed significant improvement in lymphedema-related symptoms following exercise interventions.40 Consequently, when appropriately designed and monitored, exercise is not only feasible but may also contribute positively to the management of symptoms.
The current evidence strongly supports a diverse and individualized approach to the prescription of exercise for this population. A combination of aerobic and resistance training is the most widely endorsed strategy, with multiple studies indicating improvements in strength, mobility, and overall physical function. This multimodal approach is strongly corroborated by the newly developed international consensus framework for lower limb lymphedema by Davies et al (2025).41 In their Delphi study, experts specifically advocated for a structured program that integrates resistance (eg., 2–3 sessions/week), aerobic, and flexibility exercises. The consistency between our findings and the Davies framework highlights a shifting paradigm towards more structured, multimodal exercise prescriptions.41 Aquatic therapy is particularly suited for patients who benefit from the natural compression and reduced joint loading associated with water-based activity.10,26,28,32 For individuals in earlier stages of recovery or with limited mobility, low-impact options such as yoga, stretching, or aquatic therapy, provide accessible alternatives that support lymphatic drainage, the management of fatigue, and the maintenance of physical activity.24,26,28,29,37 Basic remedial exercises and daily motion remain important for sustaining joint mobility and lymphatic flow, although their effects on strength and cardiovascular function are more limited.10,23
In addition to the type of exercise, the intensity of activity has also been shown to play a key role in clinical outcomes. Studies have consistently demonstrated that moderate to vigorous intensity exercise is safe for individuals with LLL, with no evidence of symptom aggravation when introduced cautiously and monitored regularly.24,28,30,31,36 Even vigorous-intensity activities are not contraindicated and may be appropriate when guided by clinical evaluation.24,30,31 Furthermore, lower intensity activities remain relevant and should be encouraged for those who are older, deconditioned or undergoing active cancer treatment.24,28
In terms of exercise scheduling, existing guidelines recommend aerobic exercise 3–5 days per week for a cumulative total of ≥150 minutes of moderate or ≥75 minutes of vigorous activity.2,24,29,34,35,37 Resistance training is advised 2–3 times per week, performed in sets of 8–15 repetitions at 60–80% of one-repetition maximum (1RM).23,24,27,29,35,37 Flexibility training, while supplementary, is beneficial for maintaining joint range and overall functionality, and can be implemented 3–5 times per week for 15–20 minutes, often as part of warm-up or cool-down routines.24,34 Encouraging patients to integrate light intensity movements on a daily basis, such as walking or household tasks, helps to build sustainable habits and contributes to weekly activity goals.10,27
Importantly, exercise interventions must prioritize safety and individualized monitoring. Regarding safety measures, the use of compression garments during exercise is a critical consideration. Davies et al (2025)41 emphasize this in their consensus framework, noting that sports compression gear may be a viable alternative if medical-grade garments hinder movement. However, it is noteworthy that Wittenkamp et al (2025)42 found mixed results regarding the immediate reduction of limb volume with compression during exercise. Therefore, while wearing well-fitted compression garments remains a standard recommendation to support lymphatic flow and safety,10,22,23,37 its application should be individualized based on patient tolerance and the specific exercise context to ensure long-term adherence. Supervision by trained professionals is also essential, not only for guiding safe and effective techniques, but also for ensuring the early identification of adverse symptoms and helping patients to navigate certain barriers to participation, such as determining whether an exercise method is appropriate.27,28,30 Furthermore, the integration of digital or manual tracking tools, such as apps, wearable devices, or diaries, has shown promise in enhancing compliance, motivation and self-efficacy.24,27,34,35 To be most effective, both supervision and self-monitoring strategies must be adapted to individual patient profiles, treatment phases and symptom responses.24,37 Collectively, these findings reinforce that exercise is both safe and beneficial for individuals with lower limb lymphedema, and can empower patients to engage in meaningful and long-term lifestyle changes. Notably, a recent evidence summary by Wittenkamp et al (2025) supports this conclusion.42 After analyzing 12 studies involving 367 participants, they found that exercise yields small but positive effects on health-related quality of life (HR-QOL), physical function, and pain without increasing the risk of adverse events. Although they noted high heterogeneity across studies, their findings validate the safety profile of exercise interventions in this population.
Discussion
In this study, we systematically reviewed the best evidence for the exercise-based management of LLL for survivors of gynecological cancer. Given the rising global incidence of gynecological cancers,1,2 addressing post-treatment complications like LLL is critical for enhancing survivorship quality. Despite the recognized benefits of exercise, clinical guidance has historically relied heavily on breast cancer-related lymphedema (BCRL) protocols. Our study addresses this gap by synthesizing high-quality evidence tailored specifically to the lower limb context.
Importantly, the findings of this review support the growing recognition that appropriately prescribed exercise can be safely incorporated into the management of LLL in survivors of gynecological cancer. In the past, patients with lymphedema were often advised to avoid or limit physical activity because of concerns that exercise might aggravate swelling or increase lymphatic burden. However, evidence from cancer rehabilitation and lymphedema research has gradually challenged this view, suggesting that carefully monitored exercise may help improve physical function, symptom control, and overall quality of life. Our findings further extend this understanding to the context of lower limb lymphedema following gynecological cancer treatment.
Another finding was the consistent emphasis on individualized exercise prescription and appropriate professional supervision across the included evidence sources. This may reflect the clinical complexity of LLL in survivors of gynecological cancer, as patients can differ considerably in symptom severity, treatment history, physical capacity, and comorbid conditions. Compared with generalized exercise recommendations, individualized exercise programs may be more feasible and sustainable in clinical practice while also improving adherence and safety.
When performing our analysis, we excluded several systematic reviews and clinical guidelines relating to exercise and physical activity in the management of lymphedema, as their primary studies predominantly focused on upper limb lymphedema secondary to breast cancer. Given the anatomical and physiological distinctions between upper and lower limb lymphedema, particularly in terms of lymphatic drainage and functional impairment, the findings of these studies may have limited applicability to patients with lower limb lymphedema following treatment for gynecological cancer. Furthermore, although our current analysis synthesized evidence from 17 publications, a subset of the selected articles addressed exercise interventions for cancer survivors in a broader manner, rather than specifically in those diagnosed with lower limb lymphedema. Nonetheless, the underlying principles of exercise prescription, encompassing type, frequency, and intensity, as well as specific therapeutic objectives, were deemed sufficiently relevant to support extrapolation to this population. In addition, this review included both primary studies and secondary sources, and partial overlap was identified between them. Although no quantitative synthesis was conducted across study types, the possibility of overlapping evidence may still introduce bias. Finally, given that some evidence is sourced from global literature, it is suggested that these recommended strategies should be tailored to regional settings. Additionally, this review was not pre-registered in a public registry such as PROSPERO, which represents a limitation in terms of transparency and adherence to best practices for systematic review conduct.
Conclusion
Here, we summarized the best available evidence for the management of lower limb lymphedema in survivors of gynecological cancer from nine key aspects: exercise contraindications, pre-exercise assessment, exercise modality, exercise intensity, exercise prescription, exercise safety, exercise supervision and adherence, exercise education and exercise precautions. These evidence-based recommendations can provide valuable guidance for clinical and community healthcare providers to design and implement individualized exercise programs for this population. By applying these strategies, clinical outcomes can be improved and the quality-of-life of affected women could be significantly enhanced. Despite the emergence of consensus-based frameworks, the current evidence base remains limited by methodological heterogeneity, a challenge also highlighted by Wittenkamp.42 Future research should prioritize high-quality randomized controlled trials (RCTs) that specifically test these consensus-derived exercise protocols to establish firmer cause-and-effect relationships and refine clinical guidelines for survivors of gynecological cancer.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author (Soh Kim Lam, Email: [email protected]) on reasonable request.
Acknowledgments
We sincerely thank all the participants who contributed to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was funded by Health Commission of Zhejiang Province (2023KY142), Project of Wenzhou Science and Technology Bureau (Y20220157), Project of Wenzhou Science and Technology Bureau (Y2023742) and Project of the Nursing Department of the First Affiliated Hospital of Wenzhou Medical University (HLKY202202).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Duan R, Zhang H, Yu J, et al. Temporal trends and projections of gynecological cancers in China, 2007–2030. BMC Women’s Health. 2023;23(1). doi:10.1186/s12905-023-02384-2
2. Zhu B, Gu H, Mao Z, et al. Global burden of gynaecological cancers in 2022 and projections to 2050. J Glob Health. 2024;14:04155. doi:10.7189/jogh.14.04155
3. Keyvani V, Kheradmand N, Navaei ZN, Mollazadeh S, Esmaeili S. Epidemiological trends and risk factors of gynecological cancers: an update. Med Oncol. 2023;40(3). doi:10.1007/s12032-023-01957-3
4. Caretto AA, Stefanizzi G, Garganese G, et al. Treatment of early-stage gynecological cancer-related lower limb lymphedema by lymphaticovenular anastomosis—the triple incision approach. Medicina. 2022;58(5):631. doi:10.3390/medicina58050631
5. Cucinella G, Di Donna MC, Casarin J, et al. Lower limb lymphedema after surgical staging for endometrial cancer: current insights and future directions. Taiwanese J Obstetrics Gynecol. 2024;63(4):500–13. doi:10.1016/j.tjog.2024.04.008
6. Fan X, Chen J, Weng X. Research progress in traditional Chinese medicine for the prevention and treatment of lower limb lymphedema after cervical cancer surgery/radiotherapy. Eu J Gynaecol Oncol. 2025;46(3):8. doi:10.22514/ejgo.2025.031
7. Lee J, Byun HK, Im SH, Son WJ, Roh YH, Kim YB. Risk factors for lower extremity lymphedema after surgery in cervical and endometrial cancer. J Gynecologic Oncol. 2023;34(3):e28. doi:10.3802/jgo.2023.34.e28
8. Choi JE, Chang MC. Management of lymphedema is really a matter in patients with breast cancer. World J Clin Cases. 2024;12(15):2482–2486. doi:10.12998/wjcc.v12.i15.2482
9. Mortimer PS, Pearson M, Gawrysiak P, et al. LymphActiv: a digital physical activity behavior intervention for the treatment of lymphedema and lipedema. Lymphatic Res Biol. In Press. doi:10.1089/lrb.2023.0033
10. Executive Committee of the International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2023 consensus document of the international society of lymphology. Lymphology. 2023;56(4):133–151
11. Tümkaya MN, Seven M. Interventions for prevention and management of gynecological cancer-related lower limb lymphedema: a systematic scoping review. Seminars Oncol Nurs. 2025;41(1):151781. doi:10.1016/j.soncn.2024.151781
12. Hayes SC, Singh B, Reul-Hirche H, et al. The effect of exercise for the prevention and treatment of cancer-related lymphedema: a systematic review with meta-analysis. Med Sci Sports Exercise. 2022;54(8):1389–1399. doi:10.1249/MSS.0000000000002918
13. Hasenoehrl T, Palma S, Ramazanova D, et al. Resistance exercise and breast cancer–related lymphedema—a systematic review update and meta-analysis. Support Care Cancer. 2020;28(8):3593–3603. doi:10.1007/s00520-020-05521-x
14. DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14(6):500–515. doi:10.1016/S1470-2045(13)70076-7
15. Guo Y, Miao X, Hu J, et al. Summary of best evidence for prevention and management of frailty. Age Ageing. 2024;53(2):afae011. doi:10.1093/ageing/afae011
16. Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010;182(18):E839–E842. doi:10.1503/cmaj.090449
17. Aromataris E, Fernandez R, Godfrey C, Holly C, Khalil H, Tungpunkom P. Summarizing systematic reviews: methodological development, conduct and reporting of an Umbrella review approach. Int J Evidence Based Healthcare. 2015;13(3):132–140. doi:10.1097/XEB.0000000000000055
18. McArthur A, Klugarova J, Yan H, Florescu S. Innovations in the systematic review of text and opinion. Int J Evidence Based Healthcare. 2015;13(3):188–195. doi:10.1097/XEB.0000000000000060
19. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
20. Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, editors. JBI Manual for Evidence Synthesis. JBI; 2024. doi:10.46658/JBIMES-24-01
21. Woods A. Evidence summary. cancer (adults and older adults): exercise prescription. JBI EBP Database. 2024;
22. Mehrara B, Chang EI, Ashinoff RL. Management of peripheral lymphedema. In: UpToDate. Colwell AS, Eidt JF, Mills JL, Collins KA, deputy, editors. Waltham (MA); 2025.
23. National Lymphedema Network Medical Advisory Committee. Exercise. National lymphedema network. 2011. Available from: http://www.lymphnet.org/pdfDocs/nlntreatment.pdf.
24. Hayes SC, Newton RU, Spence RR, Galvão DA. The exercise and sports science Australia position statement: exercise medicine in cancer management. J Sci Med Sport. 2019;22(11):1175–1199. doi:10.1016/j.jsams.2019.05.003
25. National Institute for Health and Care Excellence. Physical activity: brief advice for adults in primary care (NICE Guideline PH44). 2013. Available from: https://www.nice.org.uk/guidance/ph44.
26. National Comprehensive Cancer Network. Survivorship care for cancer-related late and long-term effects. NCCN Guidelines for Patients. Version 1.2024. NCCN Foundation. Available from: https://www.nccn.org/patientguidelines.
27. National Comprehensive Cancer Network. Survivorship care for healthy living. NCCN Guidelines for Patients. Version 1.2024. NCCN Foundation. Available from: https://www.nccn.org/patientguidelines.
28. Armer JM, Ostby PL, Ginex PK, et al. ONS guidelines™ for cancer treatment–related lymphedema. Oncol Nurs Forum. 2020;47(5):518–538. doi:10.1188/20.ONF.518-538
29. Tsuji K, Sasai H, Kiyohara K, et al. Japan’s cancer survivorship guidelines for exercise and physical activity. Japanese J Clin Oncol. In Press. doi:10.1093/jjco/hyae126
30. Rock CL, Thomson CA, Sullivan KR, et al. American cancer society nutrition and physical activity guideline for cancer survivors. CA A Cancer J Clin. 2022;72(3):230–262. doi:10.3322/caac.21719
31. Campbell KL, Winters-Stone KM, Wiskemann J, et al. Exercise guidelines for cancer survivors: consensus statement from international multidisciplinary roundtable. Med Sci Sports Exercise. 2019;51(11):2375–2390. doi:10.1249/mss.0000000000002116
32. Abe K, Tsuji T, Oka A, et al. Postural differences in the immediate effects of active exercise with compression therapy on lower limb lymphedema. Support Care Cancer. 2021;29(11):6535–6543. doi:10.1007/s00520-020-05976-y
33. Fukushima T, Tsuji T, Sano Y, et al. Immediate effects of active exercise with compression therapy on lower-limb lymphedema. Support Care Cancer. 2017;25(8):2603–2610. doi:10.1007/s00520-017-3671-2
34. Do J, Choi KH, Ahn JS, Jeon JY. Effects of a complex rehabilitation program on edema status, physical function, and quality of life in lower-limb lymphedema after gynecological cancer surgery. Gynecologic Oncol. 2017;147(2):450–455. doi:10.1016/j.ygyno.2017.09.003
35. Wang J, Ma J, Zhang Y, et al. The rehabilitation efficacy of diaphragmatic breathing combined with limb coordination training for lower limb lymphedema following gynecologic cancer surgery. Front Bioeng Biotechnol. 2024;12:1392824. doi:10.3389/fbioe.2024.1392824
36. Hsu Y, Nguyen TT, Chou Y, Ho C. Effects of exercise on lower limb lymphedema in gynecologic cancer: a systematic review and meta-analysis. Eur J Oncol Nurs. 2024;70:102550. doi:10.1016/j.ejon.2024.102550
37. Stout NL, Mina DS, Lyons KD, Robb K, Silver JK. A systematic review of rehabilitation and exercise recommendations in oncology guidelines. CA A Cancer J Clin. 2021;71(2):149–175. doi:10.3322/caac.21639
38. Plinsinga ML, Rye S, Jones T, et al. Mild symptoms matter: results from a prospective, longitudinal study on the relationship between symptoms, lymphedema and health-related outcomes post-gynecological cancer. Gynecol Oncol. 2024;191:158–164. doi:10.1016/j.ygyno.2024.10.011
39. Abakay H, Dogan H, Atilabey Güç A, Talay Çalış H. Association of lower extremity lymphedema with pelvic floor functions, sleep quality, kinesiophobia, body image in patients with gynecological cancers. Women Health. 2023;63(1):27–34. doi:10.1080/03630242.2022.2155900
40. Hsu -Y-Y, Liu C-Y, Ho C-L, Hsu K-F. Determinants of quality of life related to lower limb lymphedema in women with gynecological cancer surgery. Asia Pac J Oncol Nurs. 2023;10(1):100153. doi:10.1016/j.apjon.2022.100153
41. Davies LM, Koelmeyer L, Gaitatzis K, Paramanandam VS, Thompson B. Reaching consensus on exercise recommendations for individuals living with lower limb lymphoedema: a Delphi study. Disabil Rehabil. 2025;1–9. doi:10.1080/09638288.2025.2578424
42. Wittenkamp MC, Christensen J, Vinther A, Juhl CB. The effect of exercise in patients with lower limb lymphedema: a systematic review. Acta Oncol. 2025;64:484–498. doi:10.2340/1651-226X.2025.42560
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Therapeutic Potential of Ion Carrier Antibiotics in Ovarian Cancer: Mechanisms and Prospects
Feng L, Wen W, Shujuan Y
Cancer Management and Research 2026, 18:566921
Published Date: 20 January 2026