Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Behavioral Interventions for the Patient–Caregiver Unit in Patients with Chronic Heart Failure: A Systematic Review of Caregiver Outcomes
Authors G S, Tan WA ![]() , Lee ARYB
, Lee ARYB ![]() , Chen MZ
, Chen MZ ![]()
Received 5 January 2022
Accepted for publication 20 April 2022
Published 29 April 2022 Volume 2022:15 Pages 921—939
DOI https://doi.org/10.2147/JMDH.S357179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Suthershinii G,1,* Weiling Amanda Tan,2,* Ainsley Ryan Yan Bin Lee,2 Matthew Zhixuan Chen3
1Department of Biological Sciences, National University of Singapore, Singapore, Singapore; 2Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore; 3Division of Geriatric Medicine, Department of Medicine, National University Hospital, Singapore
*These authors contributed equally to this work
Correspondence: Matthew Zhixuan Chen, Division of Geriatric Medicine, Department of Medicine, National University Hospital, 1E Kent Ridge Road, Tower Block, Level 10 Department of Medicine, 119228, Singapore, Tel +65 6779 5555, Email [email protected]
Background: Chronic heart failure (CHF) is a debilitating condition that affects millions worldwide. It is accompanied by a myriad of adverse consequences, such asdiminishing of quality of life and deterioration of mental health. Caregivers play a pivotal role in helping CHF patients manage their conditions and symptoms, as a result the physical, mental and emotional state of caregivers have a direct impact on CHF patients and the management of this condition.
Purpose: This systematic review aims to synthesize data about the effectiveness of behavioral interventions targeted at patients with chronic heart failure (CHF) and/or informal caregivers of CHF patients to improve overall management and treatment of CHF in the population.
Patients and Methods: Three databases were searched for published studies and studies that included evaluated outcomes of interventions that targeted CHF patients or informal caregivers. All randomized controlled trials, trials of either experimental or quasi-experimental design were included. Studies that only involved formal caregivers, patient populations of adolescents/young adults and patients with non-chronic conditions were excluded.
Results: Across the 21 included studies, no study reported a significant improvement in all three domains of quality of life (QoL), depression and loneliness of caregivers while only three studies reported a significant improvement in two outcomes. Within each domain, heterogeneity in measures limited quantitative pooling.
Conclusion: This review provides data on the efficacy of interventions targeted at CHF patients and/or informal caregivers. It also highlights successful interventions and its features. Following this, additional resources need to be invested and directed towards implementing these interventions.
Keywords: caregiver burden, chronic care, multidisciplinary care, psychosocial
Introduction
Chronic heart failure (CHF) is a debilitating condition that affects close to 26 million people worldwide. There is a dramatic increase in prevalence, especially in developed countries and amongst older adults.1,2 CHF usually manifests symptoms such as shortness of breath, weakness in limbs, fatigue, which worsens over time in periodic stages.3–5 With the advent of technology and medical advancements, pharmacological agents and non-pharmacological agents such as the implantation of intra-cardiac defibrillators (ICD) and cardiac resynchronization therapy have markedly improved clinical outcomes of patients with CHF.6–9 However, CHF remains associated with high mortality rates, high hospitalization rates and poor quality of life outcomes.1
Additionally, it has been found that increased burden on the caregivers of CHF patients adversely affects patient outcomes. Caregivers play a pivotal role in CHF disease management by helping patients cope with symptoms, providing emotional support, and aiding in decision-making.10 Being a chronic debilitating condition, there can be a significant toll on informal caregivers,11 increasing the incidence and severity of loneliness, depression, and poor quality of life amongst caregivers.12 Such adverse caregiver outcomes are strongly associated with poor patient outcomes such as increased mortality and hospital readmissions. Many studies have shown that behavioral interventions that target caregivers and patients alike have benefited patient–caregiver dyads. However, there is significant heterogeneity among such studies, with varying interventions and qualitative and quantitative ways of evaluating outcomes and results. Therefore, this systematic review aims to synthesize data from varying studies to identify effective interventions that could alleviate patient and caregiver outcomes, improving CHF care and management in the population.
Methods
The systematic review was reported according to the Preferred Reporting Items of Systematic Reviews and Meta-Analyses (PRISMA) guidelines.13 Searches of three databases (PubMed, Embase and CENTRAL) were conducted for studies published from the date of inception to June 2021.
Search Strategy
Literature search was performed using search strategy for each database using the search strategy in Supplementary Table 1 and other sources retrieved 16,953 results. References were imported into EndNote X9 and 2477 duplicates were identified and removed. Of 14,476 titles and abstracts screened, 14,384 were excluded. After screening the full-text studies, 21 were included in the review. The screening process is detailed in the PRISMA flowchart in Figure 1.
 |
Figure 1 PRISMA flowchart. Notes: The PRISMA figure is available from: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. Creative Commons CC BY 4.0.40 |
Study Selection
Studies evaluating outcomes of interventions that are targeted at the patient or informal caregivers were included. We included all randomized controlled trials, and trials of either experimental or quasi-experimental design according to the PICOS (population, intervention, comparison, outcomes) inclusion and exclusion criteria. We included studies that involved patients formally diagnosed with heart failure of any stage and their informal caregivers implementing any behavioral intervention, which could be educational, psychoeducational or counseling delivered through synchronous or asynchronous means.
Outcomes of interest included caregiver-related psychosocial outcomes, spanning domains including caregiver burden, stress, self-efficacy and confidence, loneliness, depression and quality of life. To be included, studies should measure and report outcomes of informal caregivers of patients. Only controlled prospective studies were included in this review.
We subsequently excluded other types of studies: studies that only involved formal caregivers, studies where the patient population consisted of adolescents/young adults or patients with non-chronic conditions, studies with small sample sizes of less than 10, and studies that did not report on any form of caregiver outcome.
Two reviewers independently screened citations and abstracts to identify studies potentially meeting the inclusion criteria. For those studies, full-text versions were retrieved and independently screened by two reviewers to determine whether they met inclusion criteria. Disagreements about whether the inclusion criteria were met were resolved through consensus with a third senior reviewer.
Data Extraction
Data extraction of relevant study information for studies meeting inclusion criteria was performed independently by two reviewers. Disagreements were resolved through discussion.
Quality Assessment
The Jadad score was used to assess the quality of included studies and consists of three items: randomisation (0–2 points), blinding (0–2 points) and participant dropout and withdrawal (0–1 points). The final score ranges from 0 to 5 points with higher scores indicating better quality. Studies rated to have a score of 2 or less were considered to be of low quality and those with a score of 3 or more were considered to be of high quality. Supplementary Table 2 reports methodological quality of all retained studies using the Jadad scale to assess risk of bias in all trials regardless of design. Quality assessment of each included study was performed by two reviewers independently with any discrepancies resolved by consensus.
Results
Description of Studies
Of the 21 studies, eight were conducted in the Asia-Pacific Region, with three studies in countries with Chinese culture. Another seven studies were conducted in the United States (US), and one study was conducted in the United Kingdom (UK). All studies did not target any specific racial or ethnic group. However, one of the studies14 conducted in the US unintentionally contains a less diverse sample due to their recruitment method. There was also no particular socio-economic group targeted by any of the studies.
Fourteen studies were randomized controlled trials, four were quasi-experimental, while one study was a single-arm pilot clinical trial, one was a mixed comparative study, and one was a mixed model study.
Types of Outcomes
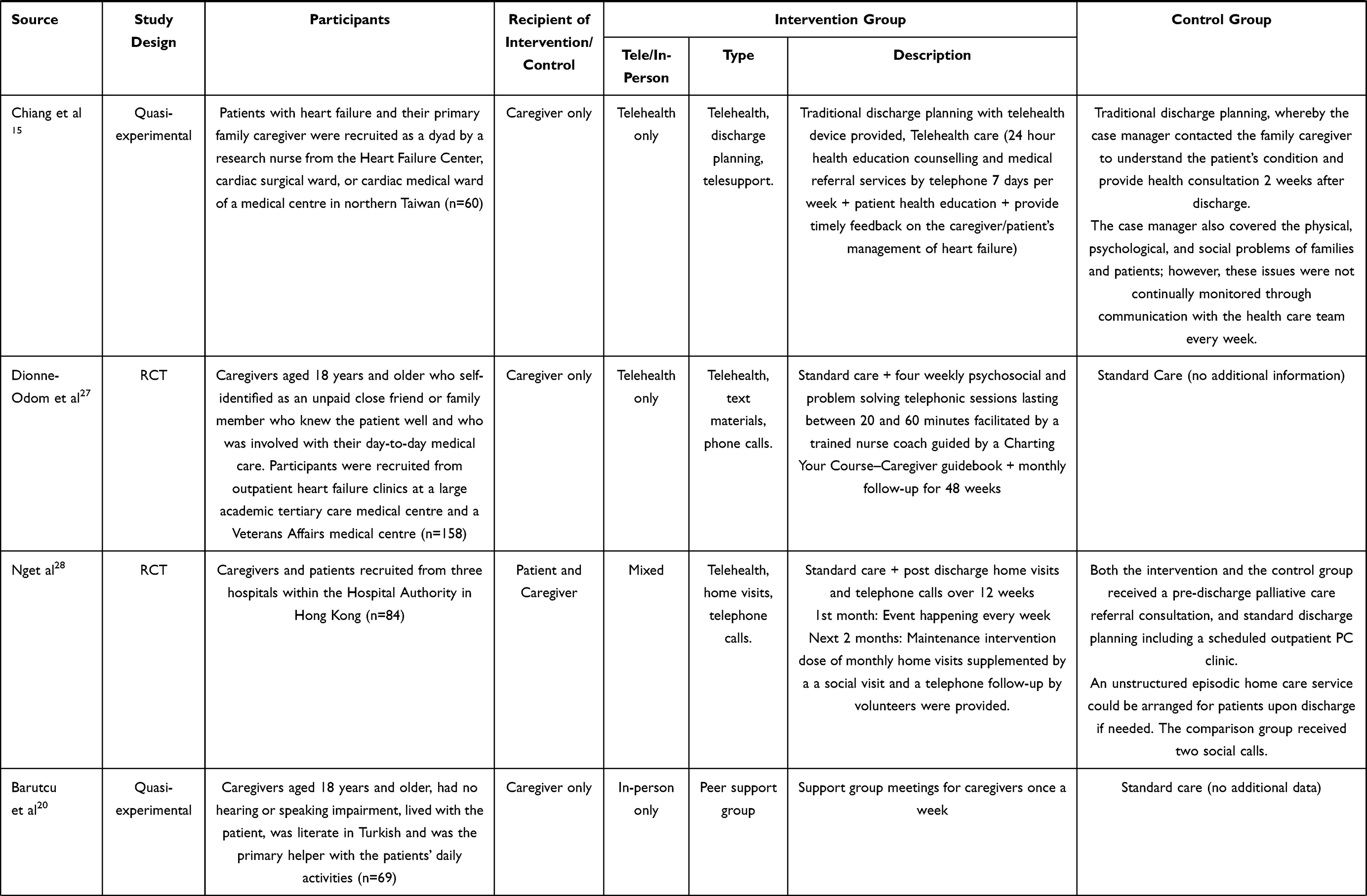
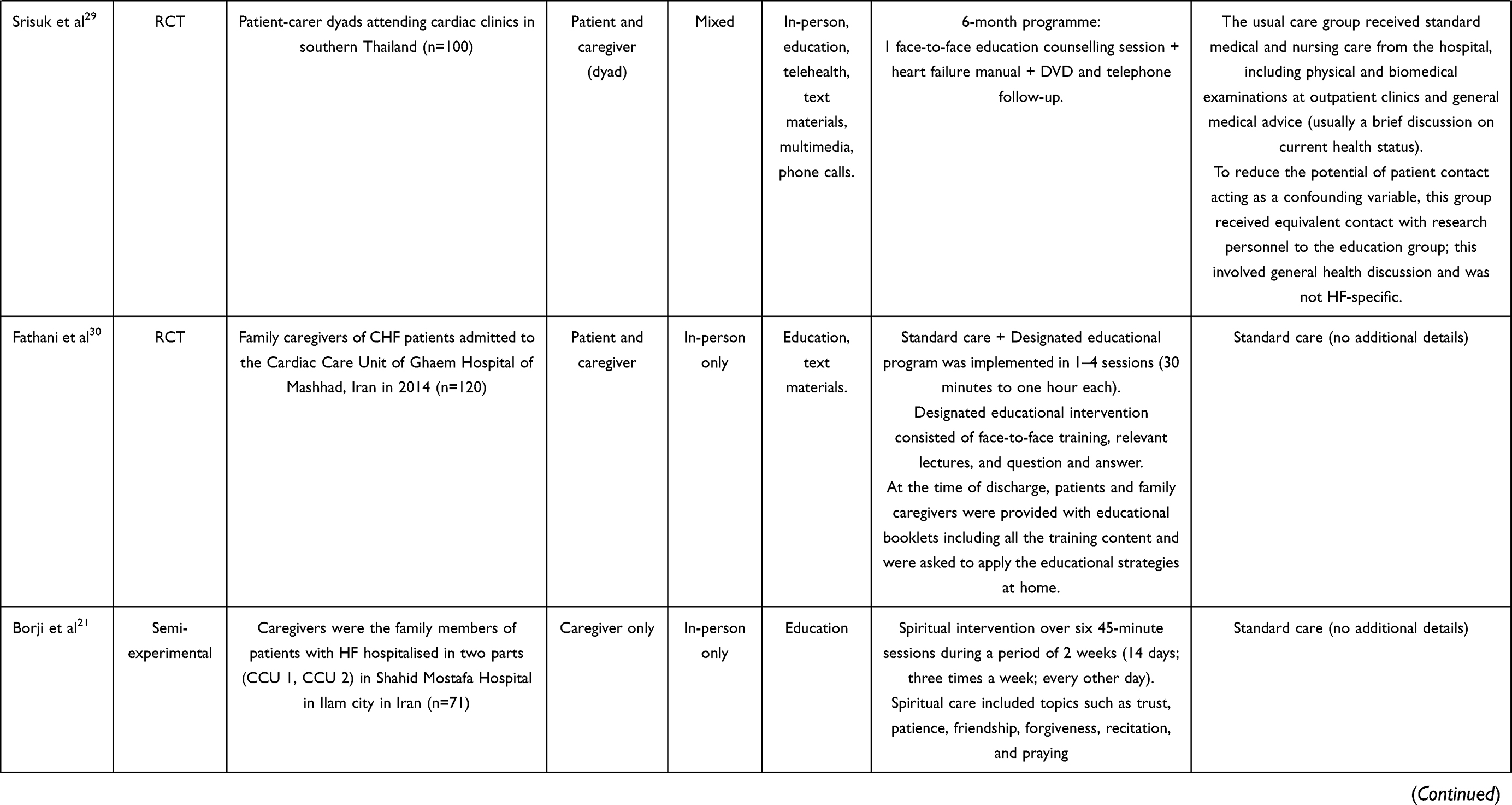
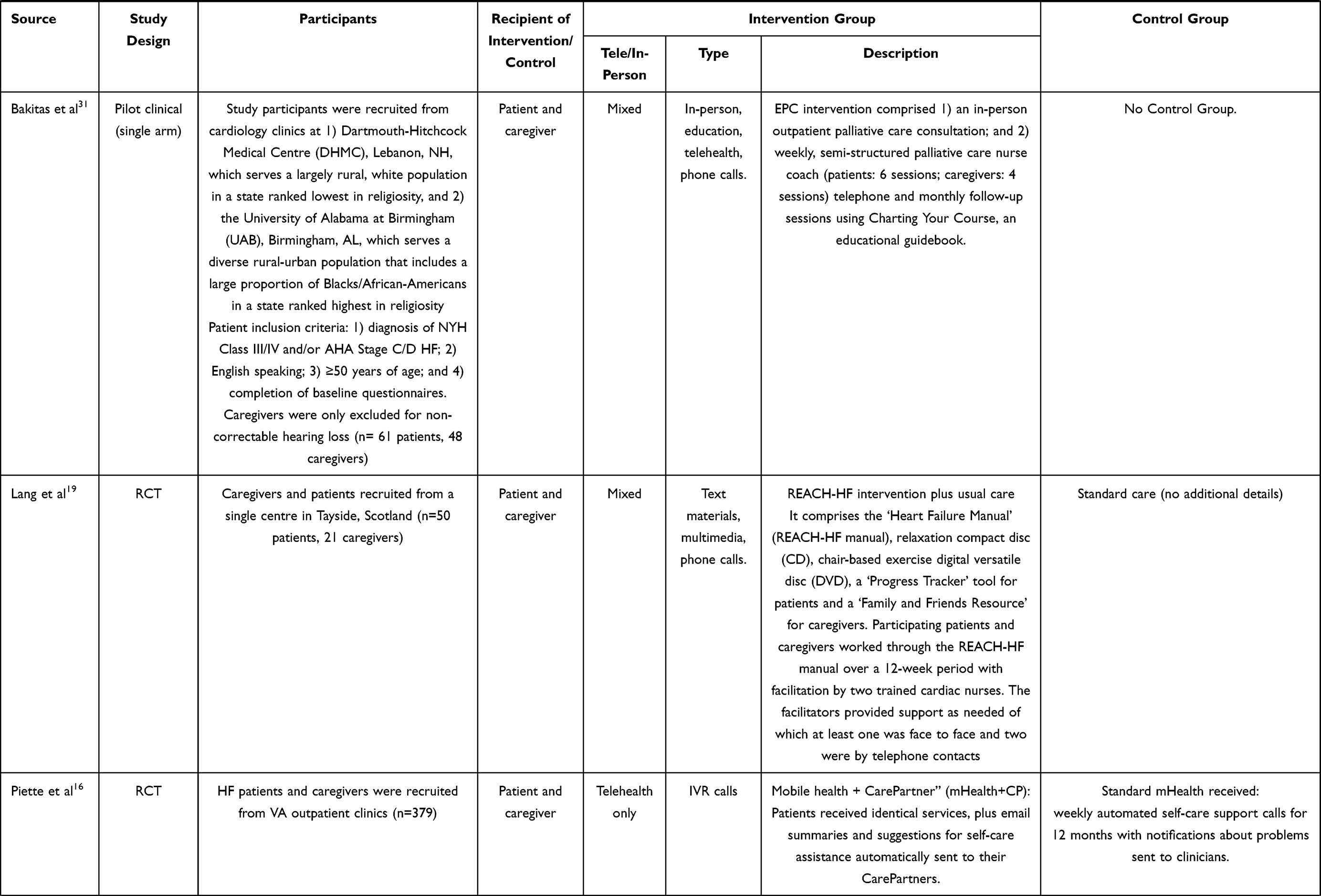
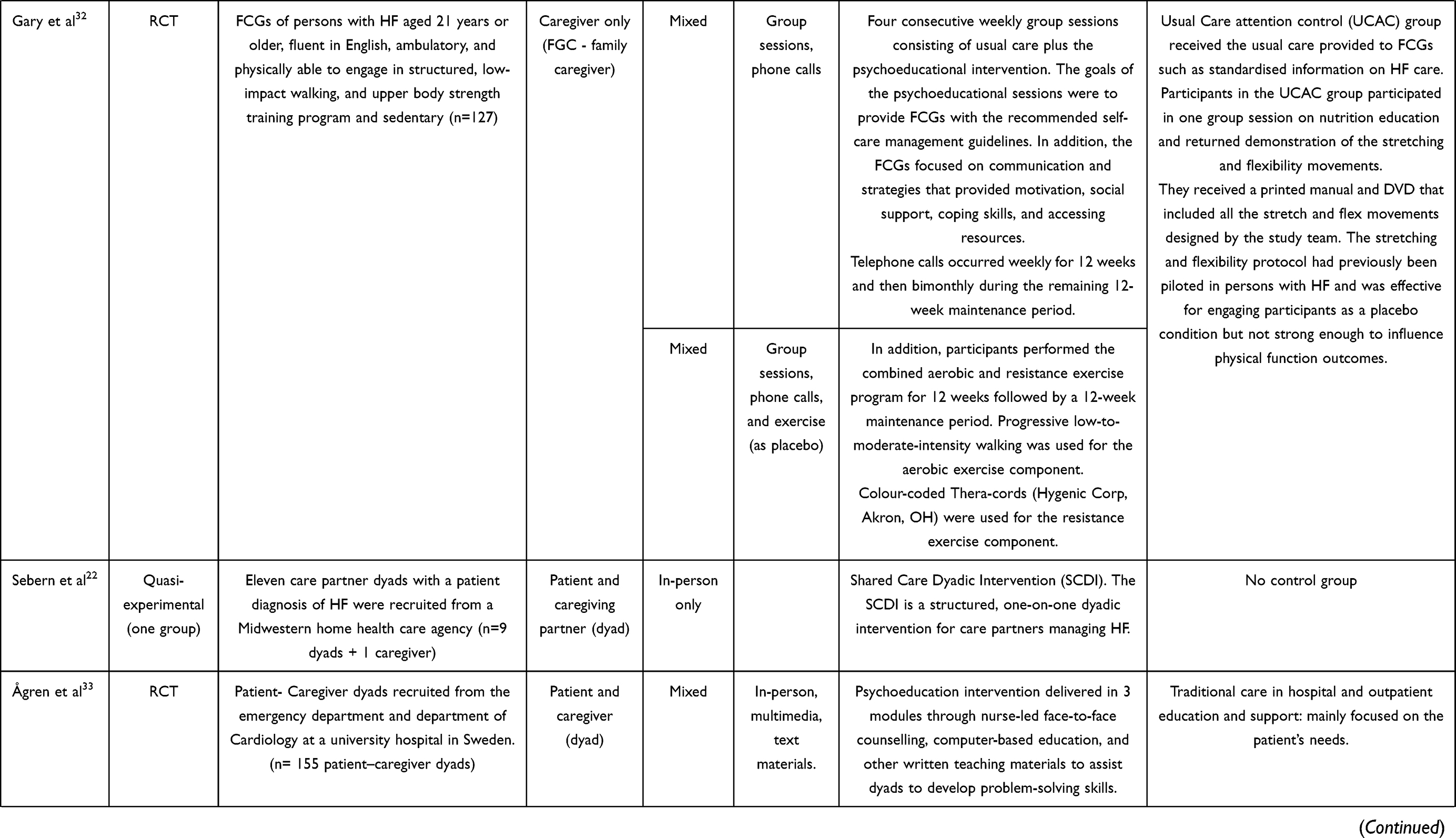
Across the 21 studies, three primary outcomes were identified as measures of caregiver burden, namely 1) Quality of Life (QoL), 2) Depression, Anxiety and 3) Loneliness. Twenty studies provided data on quality of life, 14 studies provided data on depression, two studies provided data on anxiety and three studies provided data on loneliness. Heterogeneity was noted in the measures of effect used for each domain across studies. However, each questionnaire used had prior validation before use in the study. Table 1 provides a summary of characteristics of all included studies, while Table 2 provides a summary of the outcomes and scales used in all included studies.
 |
 |
 |
 |
 |
 |
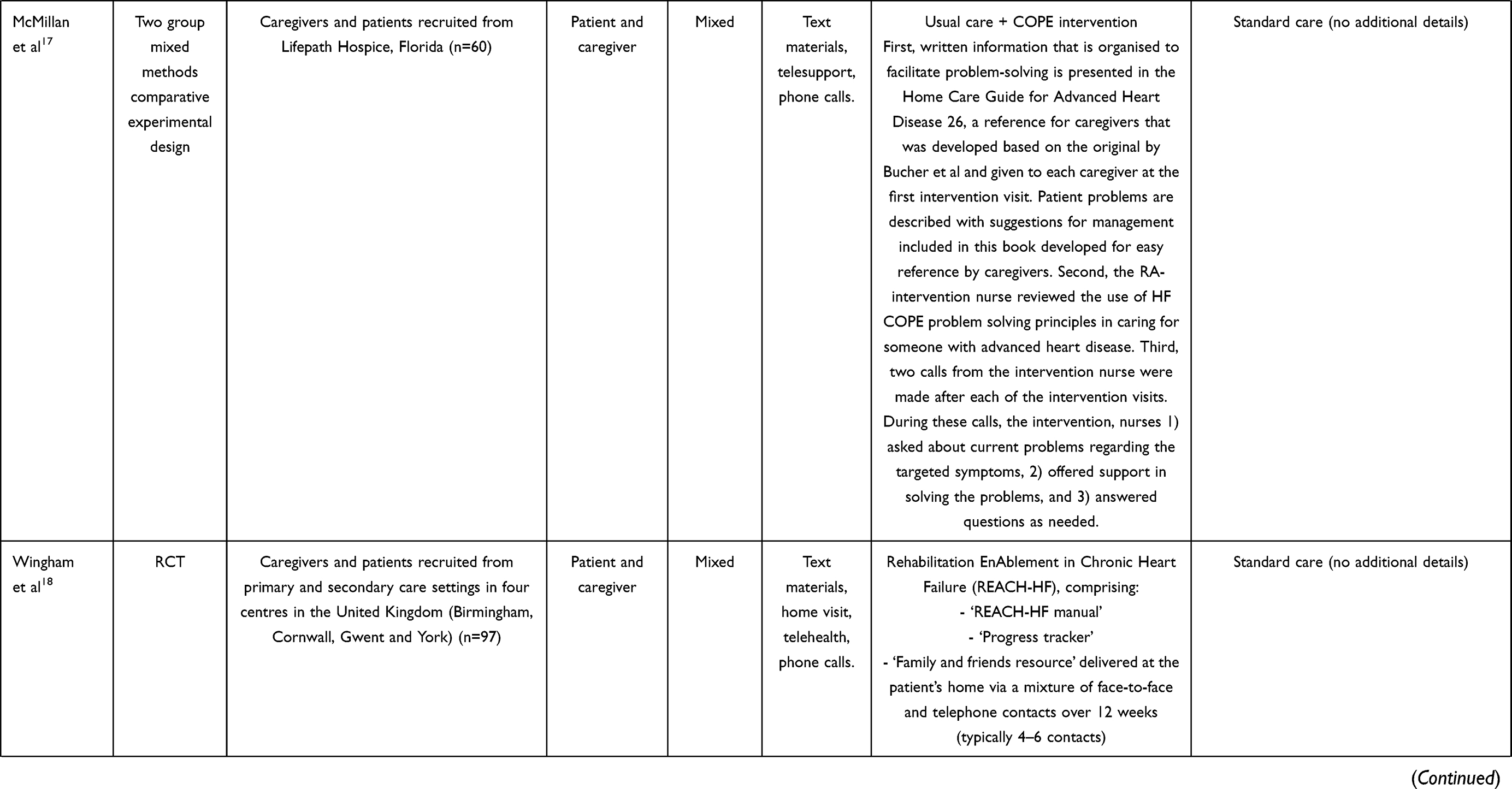 | Table 1 Summary of Interventions |
 |  |  |
Table 2 Summary of Outcomes |
Types and Features of Interventions
Across the 21 studies, three main types of interventions were identified: 1) Education, 2) Psychoeducation and 3) Counseling. Table 1 provides a detailed overview of the characteristics of included studies.
Overall, the three main types of interventions were found to be delivered either synchronously, asynchronously or both. Asynchronous delivery methods did not involve real-time interaction between caregivers and educators. Caregivers were usually provided with educational material and resources that they could contend with at their own times and own targets and as such learning is carried out independently and flexibly. Synchronous delivery methods involve real-time interaction between caregivers and educators who are usually health care professionals.
The targets of most interventions were both the patient and their caregiver, with 10 interventions involving both parties. Four studies were dyadic, involving the patient and their caregiver or partner as a dyad and seven studies involved only the caregiver.
Education
Among the 21 studies, five studies,14–18 incorporated only education as a main type of intervention, whereby education entailed the dissemination of information related to heart failure. This includes symptom and risk factor management, dietary and lifestyle advice.
Three of the studies15,16,18 delivered the educational intervention asynchronously, while two of the studies14,17 had both synchronous and asynchronous delivery. One of the studies15 involved a device that tracked the symptoms of the patient, which allowed easier management and monitoring of symptoms, creating lower caregiver burden (p=0.382), higher stress mastery and better family function. Another study16 involved a telehealth application that automatically e-mails summaries and suggestions for self-care to the patient’s caregiver/partner. This reduced caregiving strain at both six and 12 months (both p≤0.03) and improved depressive symptoms among caregivers/partners who reported greater burden at baseline (p≤0.03). Wingham et al used a program manual, progress tracker and ‘family and friends’ resource delivered in-person and over phone calls over 12 weeks, improving confidence of caregivers’ self-management.
The two studies14,17 that used both synchronous and asynchronous delivery of educational materials involved text materials, telehealth support and phone calls. These caused no significant effect in McMillan et al, while Piamjariyakul et al saw significantly improved caregiver confidence and social support scores, and caregiver depression was significantly lower.
Two studies14,16 used a dyadic intervention for patient and caregiver, with Piette et al being a Self-Care Dyadic Intervention, which improved emotional wellbeing for caregivers (effect size=0.51), while Piamjariyakul et al used telephone coaching, caregiving guides, list of local support organizations, a resource book, low-sodium booklet and a daily pill organizer. Piamjariyakul et alʹs resource-rich approach was found to lower caregiver depression significantly (M-Wz=−2.4, p=0.01) while increasing caregivers’ social support (M-Wz=2.4, p=0.01).
Psychoeducation
One study19 incorporated only psychoeducational intervention and support as the main intervention, which was delivered asynchronously. Psychoeducation includes the teaching of coping and self-care strategies, like stress and anxiety management. Lang et al involved text materials, multimedia and phone calls, with a cardiac nurse facilitating the completion of the manual with the patient and caregiver over 12 weeks. This improved caregiver depression and alleviated caregiver burden.
Counseling
Four studies20–23 incorporated synchronous counseling as the main intervention. Counseling encompasses a health professional helping caregivers to find, cope, work through and manage the problems they face. Counseling also entails the provision of a platform for caregivers to communicate and discuss their concerns and issues in relation to their role as a caregiver, which can be done through peer-support groups, forums and dyadic interventions. One study20 involved the implementation of support group meetings that promoted discussions about caregiver problems and solutions, which reduced caregiver burden scores (p<0.05) in all dimensions except objective personal care. Caregiver depression scores remained the same (p>0.05). Another study21 incorporated a spiritual approach that provided spiritually guided strategies and advice to cope with problems, such as teaching about trust, patience, forgiveness, friendship, recitation and praying which reduced the anxiety level (p=0.001) of caregivers of patients with HF.
Two studies22,23 implemented a dyadic intervention that involved both caregiver and patient, delivered through face-to-face sessions between dyads and a multidisciplinary team. Sebern et alʹs dyads were invited to discuss situations that cause stress and talk about the possible effects on their relationship and their mutual need for support. This did not show any significant changes in caregiver burden measured by CBS and DOBI (p varying from 0.08 to 0.99). Agren et alʹs intervention teaches and supports caregiver problem solving by provision of a reference book, review of the use of problem-solving principles by an intervention nurse, two calls made by an intervention nurse to discuss and review problems and possible solutions and intervention visits. However, this also did not improve caregiver depression (POMS mean=8.4 baseline, 8.9 at three weeks, 9.9 at four weeks) and caregiver quality of life (CQOL mean=43.2 baseline, 40.8 at three weeks, 40.2 at four weeks) significantly enough. These two dyadic interventions that integrated counseling did not produce significantly positive results on caregiver burden, caregiver depression and quality of life.
Combination of Interventions
Eleven studies24–34 incorporated either two or three main types of interventions. Two studies25,29 incorporated both education and counseling, while seven studies24,26,27,30–32,34 incorporated both education and psychoeducation.
Two studies28,33 incorporated education, counseling and psychoeducation. Ng et al involved regular home visits and telephone calls, while Agren et al involved face-to-face sessions with professionals and telephone visits. These lowered caregiver burden in Ng et al (p=0.024), while in Agren et al, there was no significant difference found (p varying from 0.08 to 0.99).
Impact of Interventions
Across the 21 studies, none of the studies reported a significant improvement in all three outcomes of (i) Quality of Life, (ii) Depression and Anxiety, and (iii) Loneliness, while only three studies16,22,25 reported a significant improvement in two outcomes. Eight studies14,15,20,21,24,28,30,32 reported a significant improvement in only one outcome.
Quality of Life
Quality of life amongst caregivers was measured as an outcome by 20 of the 21 studies. Across the 20 studies, 20 different scales were used to measure the outcome of QOL, with most studies using more than one type of scale to do so.
Of the 20 studies that measured QOL, nine studies15,16,20,22,24,25,28,30,32 reported a significant improvement in caregiver burden and overall QOL post-intervention. Additionally, three other studies18,19,31 reported moderate improvements in QOL after the intervention.
Depression and Anxiety
Depression amongst caregivers was measured as an outcome by 14 of 21 studies. Out of which, five studies used the Hospital Anxiety and Depression Scale (HADS), three studies used the Centre for Epidemiology Depression Scale (CESDP), three studies used the Beck Depression Inventory (BDI). The remaining three studies used the Profile of Mood States (POMS) Scale, Beck Anxiety and State Trait Anxiety Scale. Of the 14 studies, five studies14,16,21,22,25 reported a significant improvement in depressive symptoms, three studies18,19,31 reported moderate to slight improvements in depressive symptoms, and six studies17,20,26,27,33,34 reported no significant improvement in depressive symptoms post-intervention.
Anxiety amongst caregivers was measured by two of 21 studies, one of which used the Beck Anxiety Inventory (BAI) and the other used the State Anxiety Scale. One of the studies21 reported a significant decrease in anxiety levels amongst caregivers post-intervention, while the other study22 did not report any changes in anxiety levels in caregivers at baseline and post-intervention.
Loneliness
Loneliness amongst caregivers was measured as an outcome by three of 21 studies.23,26,33 All three studies used the Caregiver Burden Scale-22 (CBS-22) to measure loneliness. All three studies found that loneliness amongst caregivers was not significantly improved by the interventions.
Discussion
Caregiver Burden and Quality of Life
The ten interventions that caused a significant improvement in caregiver burden and QOL involved education, psychoeducation, peer-support groups and professional tele-support. However, the seven studies that did not report significant changes in caregivers’ QOL also involved the same interventions, with four of them having a dyadic structure.
This suggests that although education and psychoeducation may significantly improve caregiver QOL, the method of intervention delivery is also important. Text materials were not correlated with improved QOL, while phone calls and multimedia proved to be more effective. Delivery methods such as text materials are not correlated with improved QOL, while phone calls and multimedia proved to be more effective. On top of that, dyadic interventions seem to have little to no effect on improving caregiver burden and QOL, as seen in the four studies with dyadic interventions. Studies that produced positive results were also generally from the Asia-Pacific region, which suggests that other factors such as culture may also influence the effectiveness of such interventions.
Depression and Anxiety
The five interventions that reported improvements involved education, peer-support groups and professional tele-support. The other six studies that did not report any significant changes or improvements in depressive symptoms employed psychoeducation, dyadic psychosocial interventions, education and professional tele-support. There are no specific intervention modalities that are consistently correlated with improvement in depressive symptoms, hence external factors such as context and patient attitudes may be the cause of inconsistent results. It seems that disease education, tele-support and peer-support groups can reduce depression amongst caregivers; however, the effectiveness of these interventions may depend on methods of delivery and other factors. It could also be possible that these interventions influenced the caregiving burden, which in turn influenced the caregiver’s depression, hence the correlation is unclear.
As for anxiety, only one study21 that employed a spiritually driven intervention reported significant improvements in anxiety, while the other study22 involving a dyadic intervention did not report any significant changes in anxiety levels. It could be suggested that spiritual care alleviates anxiety; however, such generalised conclusions may be premature, considering that the study focused on Islam-related spiritual care. Hence, other religious domains and faiths have to be studied to conclude consistency across religions. In the study22 that did not report any significant changes in anxiety, it must be noted that caregivers’ baseline anxiety levels were already low to begin with; hence, the employment of a dyadic intervention may not have had much of an effect. Other intervention modalities could be trialed to assess efficacy in alleviating anxiety in caregivers with high baseline anxiety levels.
Loneliness
The three studies that measured loneliness as an outcome did not include peer-support groups in their intervention. Two of these studies involved dyads of patient and caregiver, which could be seen as a form of social support, however the patient and caregiver were known to each other before the study, hence widening of the caregiver’s social circle with new social contacts has not been studied.
Loneliness could also see little improvement due to the limitations in CBS in measuring caregiver’s loneliness. As all three studies used CBS to measure this outcome, this is a potential mismatch of scale to outcome, which weakens the correlation between the interventions and caregivers’ loneliness.
Limitations of Review
A limitation of our review is the heterogeneity in measures of effect, such as questionnaires employed in each study. Inter-study variability is introduced as a result.
The findings of studies also need to be contextualized to the country and community. It is suggested that each study can be conducted on the background of different pre-existing support schemes and resources, so as to take into account important factors like cultural acceptance and availability of social support.
While evaluating interventions based on their results, the availability of resources such as time and manpower have to be evaluated too, as these enable the intervention to be implemented successfully. Certain countries could have deficits in resources or manpower, which led to difficulty in implementing interventions or limitations in the quality of interventions provided. On top of that, the generalizability of the results should also be tested, as an intervention may not be effective when applied to other countries, cultures and demographics. This would require even more resources, which would be a limitation for lower-developed countries, which may already be those with the highest needs.
The evaluation of interventions was narrowed by focusing on three main outcomes alone while other domains of analysis (eg, Self-Care) were excluded. As such, interventions that may not have yielded promising results as per our analysis may potentially be effective in improving other outcomes and vice versa.
Lastly, the methodology of our study was limited as only studies available in English were included. While grey literature was not considered in order to ensure the rigour of included studies, the breadth of studies would be limited.
Recommendations
The effectiveness of interventions is substantially dependent on the mode of its delivery; synchronous or asynchronous. Both synchronous and asynchronous delivery methods have a fair share of advantages and disadvantages. For instance, asynchronous methods tend to be more cost and resource effective, it can transcend temporal and geographical barriers, but at the same time it reduces caregiver-physician real-time interaction.35
Apart from weighing out such advantages and disadvantages of asynchronous and synchronous delivery methods before deciding on a delivery method for an intervention, other factors should also be considered. Factors such as attitudes of both physicians and caregivers towards asynchronous and synchronous delivery methods, competencies of physicians and caregivers in navigating through such methods,36 age and even the type of outcome being targeted must also be considered.
It has been found that asynchronous and synchronous delivery methods tend to be more effective for specific types of outcomes. When it comes to outcomes such as self-care and disease management, asynchronous delivery methods have been cited to be more effective while for outcomes such as quality of life, a combination of synchronous and asynchronous methods have been cited to be more effective.37 For outcomes such as depression, asynchronous methods are less commonly deployed since improvement in clinical outcomes like depression may require factors such as establishment of a therapeutic patient-physician alliance38 can only be offered through asynchronous interventions. However, a growing number of literature have suggested that asynchronous methods are efficacious in improving mental health outcomes such as depression, though more RCTs need to be conducted to further ascertain this claim.35 In all, it is important to evaluate the pros and cons of both delivery methods to choose a suitable one for an intervention. On top of that, other factors such as the demographics of the caregivers, type of outcome being targeted must also be taken into consideration to ensure that an intervention yields promising results.
Next, a holistic approach in the implementation of interventions can be adopted. Naturally, there are many factors that influence the effectiveness of interventions. For instance, individual preferences and ingrained cultural practices may influence perceptions and attitudes towards an intervention.39 This can perhaps be addressed by including incentives or by involving community leaders who may be better positioned to help change attitudes and perceptions towards interventions. As such, recognizing the nuanced needs of subpopulations would allow interventions to be tailored and personalized accordingly to ensure optimal effectiveness.
Conclusion
Patients with congestive cardiac failure often necessitate dedicated care and support. Patients often suffer debilitating effects on health and have to integrate both lifestyle and medical management into their daily lives. Patients themselves are often plagued with stress and depression coping with their condition.
The difficulties of informal caregivers, likewise, are often overlooked in their struggle of caring for patients. To ameliorate the various psychosocial stressors of caregivers would require a multi-faceted approach, often involving education, support and counseling. This review has outlined the various programs and interventions implemented in communities around the world in efforts to improve psychosocial outcomes in caregivers.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Savarese G, Lund LH. Global public health burden of heart failure. Card Fail Rev. 2017;3(1):7–11. doi:10.15420/cfr.2016:25:2
2. Bragazzi NL, Zhong W, Shu J, et al. Burden of heart failure and underlying causes in 195 countries and territories from 1990 to 2017. Eur J Prev Cardiol. 2021;28:1682–1690. doi:10.1093/eurjpc/zwaa147
3. Watson RD, Gibbs CR, Lip GY. ABC of heart failure. Clinical features and complications. BMJ. 2000;320(7229):236–239. doi:10.1136/bmj.320.7229.236
4. Malik A, Brito D, Chhabra L. Congestive heart failure. In: StatPearls. Treasure Island (FL): StatPearls PublishingCopyright © 2021, StatPearls Publishing LLC.; 2021.
5. Inamdar AA, Inamdar AC. Heart failure: diagnosis, management and utilization. J Clin Med. 2016;5(7):62. doi:10.3390/jcm5070062
6. Schranz D, Akintuerk H, Esmaeili A, Latus H, Apitz C. Heart failure therapy based on interventricular mechanics and cardio-vascular communications. Cardiovasc Diagn Ther. 2021;11(4):1080–1088. doi:10.21037/cdt-20-347
7. Lombardi CM, Cimino G, Pellicori P, et al. Congestion in patients with advanced heart failure: assessment and treatment. Heart Fail Clin. 2021;17(4):575–586. doi:10.1016/j.hfc.2021.05.003
8. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
9. Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137–e61. doi:10.1161/CIR.0000000000000509
10. Niño de Guzmán Quispe E, Martínez García L, Orrego Villagrán C, et al. The perspectives of patients with chronic diseases and their caregivers on self-management interventions: a scoping review of reviews. Patient. 2021;14:719–740. doi:10.1007/s40271-021-00514-2
11. Hwang B, Fleischmann KE, Howie-Esquivel J, Stotts NA, Dracup K. Caregiving for patients with heart failure: impact on patients’ families. Am J Crit Care. 2011;20(6):
12. Kitko L, McIlvennan CK, Bidwell JT, et al. Family caregiving for individuals with heart failure: a scientific statement from the American Heart Association. Circulation. 2020;141(22):e864–e78. doi:10.1161/CIR.0000000000000768
13. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
14. Piamjariyakul U, Werkowitch M, Wick J, Russell C, Vacek JL, Smith CE. Caregiver coaching program effect: reducing heart failure patient rehospitalizations and improving caregiver outcomes among African Americans. Heart Lung. 2015;44(6):466–473. doi:10.1016/j.hrtlng.2015.07.007
15. Chiang LC, Chen WC, Dai YT, Ho YL. The effectiveness of telehealth care on caregiver burden, mastery of stress, and family function among family caregivers of heart failure patients: a quasi-experimental study. Int J Nurs Stud. 2012;49(10):1230–1242. doi:10.1016/j.ijnurstu.2012.04.013
16. Piette JD, Striplin D, Marinec N, Chen J, Aikens JE. A randomized trial of mobile health support for heart failure patients and their informal caregivers: impacts on caregiver-reported outcomes. Med Care. 2015;53(8):692–699. doi:10.1097/MLR.0000000000000378
17. McMillan SC, Small BJ, Haley WE, Zambroski C, Buck HG. The COPE intervention for caregivers of patients with heart failure: an adapted intervention. J Hosp Palliat Nurs. 2013;15(4):196–206. doi:10.1097/NJH.0b013e31827777fb
18. Wingham J, Frost J, Britten N, et al. Caregiver outcomes of the REACH-HF multicentre randomized controlled trial of home-based rehabilitation for heart failure with reduced ejection fraction. Eur J Cardiovasc Nurs. 2019;18(7):611–620. doi:10.1177/1474515119850011
19. Lang CC, Smith K, Wingham J, et al. A randomised controlled trial of a facilitated home-based rehabilitation intervention in patients with heart failure with preserved ejection fraction and their caregivers: the REACH-HFpEF Pilot Study. BMJ Open. 2018;8(4):e019649. doi:10.1136/bmjopen-2017-019649
20. Barutcu CD, Mert H. Effect of support group intervention applied to the caregivers of individuals with heart failure on caregiver outcomes. Holist Nurs Pract. 2016;30(5):272–282. doi:10.1097/HNP.0000000000000164
21. Borji M, Mousavimoghadam SR, Salimi E, Otaghi M, Azizi Y. The impact of spiritual care education on anxiety in family caregivers of patients with heart failure. J Relig Health. 2019;58(6):1961–1969. doi:10.1007/s10943-018-0689-9
22. Sebern MD, Woda A. Shared care dyadic intervention: outcome patterns for heart failure care partners. West J Nurs Res. 2012;34(3):289–316. doi:10.1177/0193945911399088
23. Ågren S, Strömberg A, Jaarsma T, Luttik ML. Caregiving tasks and caregiver burden; effects of an psycho-educational intervention in partners of patients with post-operative heart failure. Heart Lung. 2015;44(4):270–275. doi:10.1016/j.hrtlng.2015.04.003
24. Etemadifar S, Bahrami M, Shahriari M, Farsani AK. Family caregivers’ experiences of caring for patients with heart failure: a descriptive, exploratory qualitative study. J Nurs Res. 2015;23(2):153–161. doi:10.1097/JNR.0000000000000076
25. Hu X, Dolansky MA, Su Y, Hu X, Qu M, Zhou L. Effect of a multidisciplinary supportive program for family caregivers of patients with heart failure on caregiver burden, quality of life, and depression: a randomized controlled study. Int J Nurs Stud. 2016;62:11–21. doi:10.1016/j.ijnurstu.2016.07.006
26. Liljeroos M, Ågren S, Jaarsma T, Årestedt K, Strömberg A. Long-term effects of a dyadic psycho-educational intervention on caregiver burden and morbidity in partners of patients with heart failure: a randomized controlled trial. Qual Life Res. 2017;26(2):367–379. doi:10.1007/s11136-016-1400-9
27. Dionne-Odom JN, Ejem DB, Wells R, et al. Effects of a telehealth early palliative care intervention for family caregivers of persons with advanced heart failure: the ENABLE CHF-PC randomized clinical trial. JAMA Netw Open. 2020;3(4):e202583. doi:10.1001/jamanetworkopen.2020.2583
28. Ng AYM, Wong FKY. Effects of a home-based palliative heart failure program on quality of life, symptom burden, satisfaction and caregiver burden: a randomized controlled trial. J Pain Symptom Manage. 2018;55(1):1–11. doi:10.1016/j.jpainsymman.2017.07.047
29. Srisuk N, Cameron J, Ski CF, Thompson DR. Randomized controlled trial of family-based education for patients with heart failure and their carers. J Adv Nurs. 2017;73(4):857–870. doi:10.1111/jan.13192
30. Fathani M, Afzal Aghaee M, Tadayonfar M. Evaluation of the effect of designated educational intervention on the improvement of quality of life in caregivers of patients with chronic heart failure. J Babol Univ Med Sci. 2016;18(5):20–25.
31. Bakitas M, Dionne-Odom JN, Pamboukian SV, et al. Engaging patients and families to create a feasible clinical trial integrating palliative and heart failure care: results of the ENABLE CHF-PC pilot clinical trial. BMC Palliat Care. 2017;16(1):45. doi:10.1186/s12904-017-0226-8
32. Gary R, Dunbar SB, Higgins M, et al. An intervention to improve physical function and caregiver perceptions in family caregivers of persons with heart failure. J Appl Gerontol. 2020;39(2):181–191. doi:10.1177/0733464817746757
33. Ågren S, Evangelista LS, Hjelm C, Strömberg A. Dyads affected by chronic heart failure: a randomized study evaluating effects of education and psychosocial support to patients with heart failure and their partners. J Card Fail. 2012;18(5):359–366. doi:10.1016/j.cardfail.2012.01.014
34. Löfvenmark C, Saboonchi F, Edner M, Billing E, Mattiasson AC. Evaluation of an educational programme for family members of patients living with heart failure: a randomised controlled trial. J Clin Nurs. 2013;22(1–2):115–126. doi:10.1111/j.1365-2702.2012.04201.x
35. O’Keefe M, White K, Jennings JC. Asynchronous telepsychiatry: a systematic review. J Telemed Telecare. 2021;27(3):137–145. doi:10.1177/1357633X19867189
36. Hilty DM, Torous J, Parish MB, et al. A literature review comparing clinicians’ approaches and skills to in-person, synchronous, and asynchronous care: moving toward competencies to ensure quality care. Telemed e-Health. 2021;27(4):356–373. doi:10.1089/tmj.2020.0054
37. Verhoeven F, Tanja-Dijkstra K, Nijland N, Eysenbach G, van Gemert-pijnen L. Asynchronous and synchronous teleconsultation for diabetes care: a systematic literature review. J Diabetes Sci Technol. 2010;4(3):666–684. doi:10.1177/193229681000400323
38. Palylyk-Colwell E, Argáez C. Telehealth for the Assessment and Treatment of Depression, Post-Traumatic Stress Disorder, and Anxiety: Clinical Evidence. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2018.
39. Bulthuis SE, Kok MC, Raven J, Dieleman MA. Factors influencing the scale-up of public health interventions in low- and middle-income countries: a qualitative systematic literature review. Health Policy Plan. 2020;35(2):219–234. doi:10.1093/heapol/czz140
40. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi:10.1136/bmj.n71
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.