Back to Journals » Advances in Medical Education and Practice » Volume 7
Bedside echo for chest pain: an algorithm for education and assessment
Authors Amini R, Stolz L, Kartchner J, Thompson M, Stea N, Hawbaker N, Joshi R, Adhikari S
Received 24 December 2015
Accepted for publication 17 March 2016
Published 21 May 2016 Volume 2016:7 Pages 293—300
DOI https://doi.org/10.2147/AMEP.S103083
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Richard Amini, Lori A Stolz, Jeffrey Z Kartchner, Matthew Thompson, Nicholas Stea, Nicolaus Hawbaker, Raj Joshi, Srikar Adhikari
Department of Emergency Medicine, University of Arizona Medical Center, Tucson, AZ, USA
Background: Goal-directed ultrasound protocols have been developed to facilitate efficiency, throughput, and patient care. Hands-on instruction and training workshops have been shown to positively impact ultrasound training.
Objectives: We describe a novel undifferentiated chest pain goal-directed ultrasound algorithm-focused education workshop for the purpose of enhancing emergency medicine resident training in ultrasound milestones competencies.
Methods: This was a cross-sectional study performed at an academic medical center. A novel goal-directed ultrasound algorithm was developed and implemented as a model for teaching and learning the sonographic approach to a patient with undifferentiated chest pain. This algorithm was incorporated into all components of the 1-day workshop: asynchronous learning, didactic lecture, case-based learning, and hands-on stations. Performance comparisons were made between postgraduate year (PGY) levels.
Results: A total of 38 of the 40 (95%) residents who attended the event participated in the chest pain objective standardized clinical exam, and 26 of the 40 (65%) completed the entire questionnaire. The average number of ultrasounds performed by resident class year at the time of our study was as follows: 19 (standard deviation [SD]=19) PGY-1, 238 (SD=37) PGY-2, and 289 (SD=73) PGY-3. Performance on the knowledge-based questions improved between PGY-1 and PGY-3. The application of the novel algorithm was noted to be more prevalent among the PGY-1 class.
Conclusion: The 1-day algorithm-based ultrasound educational workshop was an engaging learning technique at our institution.
Keywords: point-of care ultrasound, algorithm education, education, chest pain, bedside ultrasound, POCUS
Introduction
Point-of-care ultrasound (POCUS) continues to expand in all aspects of medicine. POCUS is a useful bedside diagnostic tool that can decrease the time to diagnosis and help determine a patient’s disposition.1–3 Goal-directed ultrasound protocols have been developed to facilitate efficiency, throughput, and patient care.1,4–7 These protocols are taught at numerous institutions and the most prevalent is the focused assessment with sonography for trauma, which is a ubiquitously used, goal-directed ultrasound protocol for assessment of an hypotensive patient after blunt abdominal trauma.8
This increasing use of POCUS was the impetus that drove the Accreditation Council for Graduate Medical Education to require emergency medicine (EM) residents to demonstrate competency in bedside ultrasound.9–11 As a result, majority of the EM residency programs now integrate ultrasound training into the resident curriculum.12–14 One of these requirements is training in bedside echocardiography; however, there is no standard format for education or assessment.12 It is known that ultrasound hands-on instruction and training workshops have been demonstrated to positively impact ultrasound training. We describe a novel undifferentiated chest pain goal-directed ultrasound algorithm-focused education workshop for enhancement of the EM resident’s training in ultrasound milestones.
Methods
Study design and setting
This was a single-center cross-sectional study conducted at an academic medical center. The study participants were 40 EM residents (postgraduate year [PGY]-1 to PGY-3) with varying ultrasound experience. Participation in the study was voluntary. This study was reviewed and approved by the University of Arizona institutional review board authority. Informed consent from participants was not required as per IRB. Data were collected from August 2014 to September 2014.
Algorithm-based ultrasound education
A 1-day educational workshop focusing on POCUS was integrated into one of the weekly EM residency didactic sessions. The educational theme for the ultrasound workshop was “The evaluation of patients with undifferentiated chest pain.” During these educational sessions, a novel goal-directed ultrasound algorithm was used as a model for teaching and learning the sonographic approach to a patient with undifferentiated chest pain (Figure 1). This workshop was developed based on the recommendations made by the Council of Emergency Medicine Residency Directors and the Academy of Emergency Ultrasound regarding the ultrasound competency skills necessary to evaluate and care for patients with undifferentiated chest pain.9 Instructors for this course were EM faculty, fellows, and residents with expertise in POCUS.
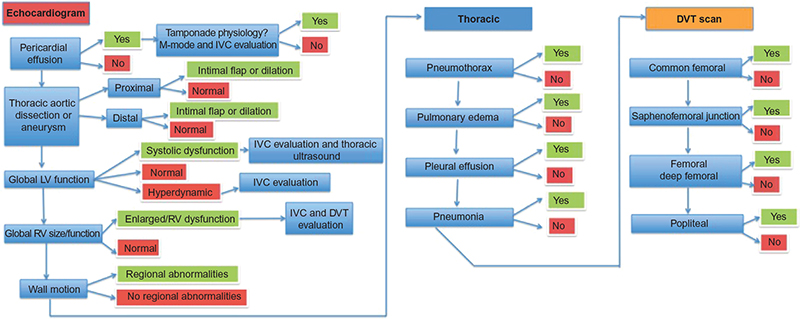 | Figure 1 Undifferentiated chest pain sonographic algorithm. |
Educational curriculum
Prior to the ultrasound workshop, the residents were provided asynchronous learning assignments that included the novel goal-directed ultrasound algorithm, reading materials, video lectures, and information regarding other educational websites. The educational tools selected for asynchronous learning describe or demonstrate the POCUS applications relevant to patients with undifferentiated chest pain. The sonographic algorithm guided the instruction provided during the workshop. For example, during the cardiac ultrasound station, students were taught to look for sonographic signs consistent with pericardial effusion, aortic root dissection or aneurysm, ventricular size irregularities, global cardiac function, and ventricular wall motion irregularities. Trained actors were used as human models for the skill stations described in Table 1. This workshop was designed as a tool to improve ultrasound milestone education; during the different stations, residents were reminded that a normal echocardiogram does not rule out cardiac pathology. Residents were informed of the risks of misdiagnoses while they improve upon their echocardiography skills. Finally, residents were reminded that bedside echocardiography does not eliminate the need for patient medical history, physical examination, and blood sampling.
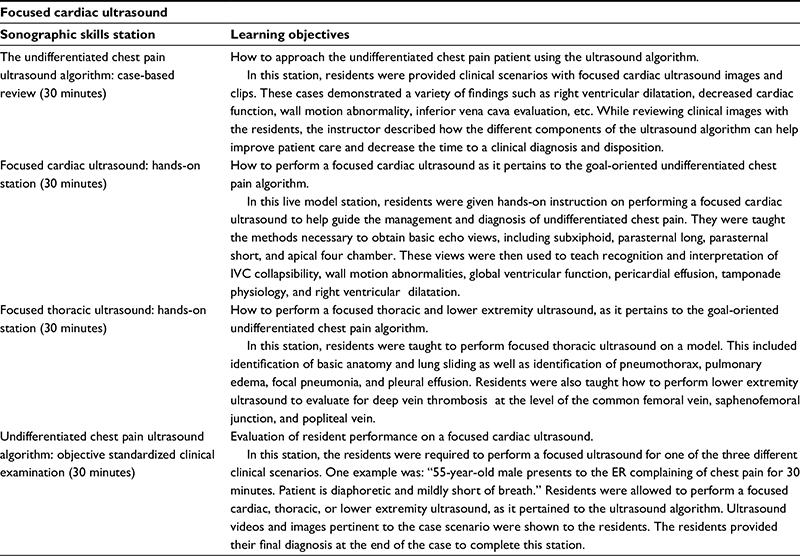 | Table 1 Skills station descriptions |
Assessment
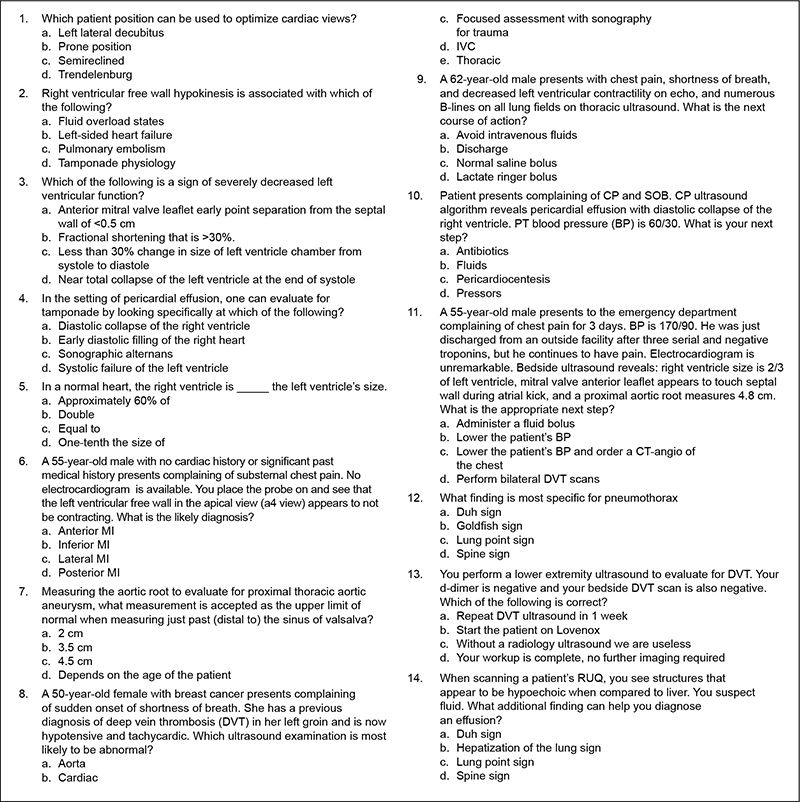
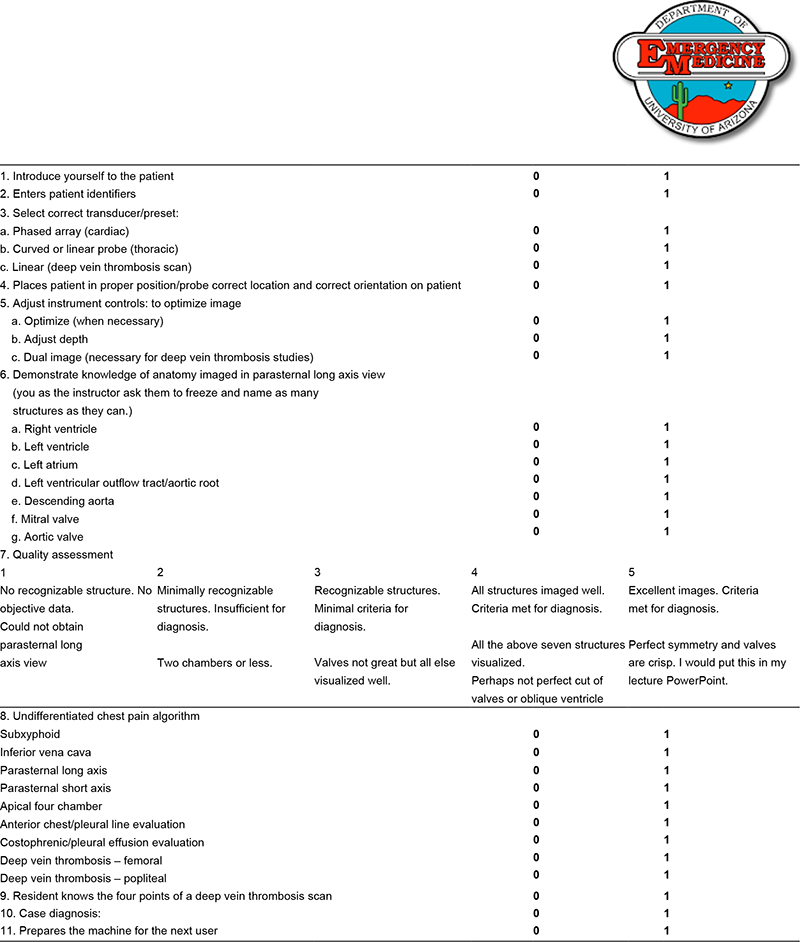
Resident assessment of the algorithm-specific skills consisted of a 14-item multiple-choice questionnaire (Figure S1) and a hands-on objective standardized clinical exam (OSCE) (Figure S2). One month after the workshop, the students were surveyed on how many times they had incorporated the algorithm into their practice (Figure S3).
Data analysis
All analyses were performed using Stata 11 (StataCorp LP, College Station, TX, USA). Data are presented as means and percentages with 95% confidence intervals (CIs) and standard deviations (SDs). Continuous variables were compared between the PGY groups using the Student’s t-test and Wilcox signed-rank test. The statistical level of significance was set at P<0.05.
Results
A total of 38 of the 40 (95%) residents who attended the event participated in the chest pain OSCE, and 26 of 40 (65%) completed the entire questionnaire. The average number of ultrasounds performed by the resident class year at the time of our study was as follows: 19 (SD=19) interns, 238 (SD=37) juniors, and 289 (SD=73) seniors. The average scores on the OSCE were 89% (SD=9) interns, 85% (SD=13) juniors, and 82% (SD=11) seniors. The average scores on the questionnaire were 70% (SD=16) interns, 82% (SD=7) juniors, and 77% (SD=15) seniors.
All the residents (100%) agreed that the undifferentiated chest pain ultrasound algorithm was useful in providing a stepwise approach to learning. Ninety-six percent (95% CI, 90%–100%) of residents agreed that the undifferentiated chest pain ultrasound algorithm was easy to understand. One student recommended that a mnemonic should be created to facilitate memorization of the algorithm.
One month after completion of the 1-day session, the residents were surveyed on how often they had incorporated the algorithm into their practice. Forty-two percent (95% CI, 22%–61%) had not used it, 42% (95% CI, 22%–61%) had used it on one to three occasions, 8% (95% CI, 0%–19%) had used in four to six times in the past month, and 8% (95% CI, 0%–19%) had used it more than six times.
Discussion
Due to the updated recommendations from the Accreditation Council for Graduate Medical Education EM milestone statement regarding ultrasound education, resident education and assessment should be adjusted accordingly.9 Whereas the assessment of most EM skills is conducted during clinical practice, ultrasound education and assessment can be restricted due to limited numbers of ultrasound-credentialed faculty at a given institution. As a result, education and assessment must be supplemented so that these new milestones can be met uniformly. Currently, there is no recommended standard for education or assessment of ultrasound milestones.12,15
The Council of Emergency Medicine Residency Directors and the Academy of Emergency Ultrasound statement includes “Undifferentiated chest pain and/or dyspnea” as one of the clinical syndromes in which EM residents are expected to display ultrasound competency.9 This is a broad and complex clinical scenario that creates a challenge with regard to training and assessing EM residents. To overcome this challenge, we created a novel, goal-directed ultrasound algorithm to serve as the central focus of training during a workshop dedicated to teach ultrasound milestones. The use of goal-directed ultrasound protocols improves emergency department flow, efficiency, and patient care.1,4–7 A patient with undifferentiated chest pain is a complex scenario that is ideal for POCUS. These patients have sizable differential diagnoses and are the literature demonstrates these patients are most likely to benefit from POCUS.1–3 Similar algorithms exist for the diagnostic differentiation of other complex clinical scenarios (BLUE protocol, RUSH protocol), but the evaluation of these protocols as educational tools has not yet been explored.6,7 For this reason, our algorithm-based workshop was conducted during resident conference/didactic time.
To our knowledge, this is the first educational workshop that is led by the milestone recommendations and uses an algorithm protocol to direct education. Previous educational documents regarding POCUS have incorporated the use of asynchronous learning, didactic lectures, hands-on practical training, and ultrasound simulation models.16,17 From these previous studies, it would appear that, to successfully engage residents during conference sessions dedicated to POCUS, a balance should be attempted between hands-on training, concept education, and assessment. For this reason, the novel algorithm was introduced at multiple stages of learning and in conjunction with a variety of different educational strategies: as a part of asynchronous learning, didactic lectures, and during practical training.
The utilization of the OSCE as an assessment measure has been previously validated.18,19 Previous studies have used the OSCE when evaluating the efficacy of the focused assessment with sonography for trauma exam as an education tool for residents, but none have studied the efficacy of using more complex algorithms (BLUE protocol, RUSH protocol) as resident teaching tools.20 Jones et al17 performed a study in which EM residents were given goal-directed echocardiography training and were then required to obtain adequate windows and identify anatomy. The use of the OSCE as an assessment tool, in the present study, not only demands the residents to obtain adequate windows and identify anatomy, but to follow a logical diagnostic sequence depending on the clinical scenario presented. The algorithm used during the educational sessions was also used as a method of assessment of resident performance.
All the residents (100%) agreed that the undifferentiated chest pain ultrasound algorithm was useful in providing a stepwise approach to learning. Ninety-six percent of residents agreed that the undifferentiated chest pain ultrasound algorithm was easy to understand. Although all residents performed well during the OSCE, our results demonstrate that the PGY-1 class performed best on the OSCE, which is unexpected given the average number of scans performed by this class was 19 (SD=19). In addition, the PGY-1 class outperformed the PGY-3 class in their ability to apply the chest pain ultrasound algorithm.
There are a few possibilities that may explain why the PGY-1 class was more proficient with the algorithm. It is possible that senior residents were less likely to benefit from a goal-oriented algorithm, as they are more proficient with cardiac ultrasound. It is also possible that senior residents may be less likely to prepare for didactic sessions and perhaps did not review the chest pain algorithm. In addition, the PGY-1 class had just completed an ultrasound boot camp and their ultrasound training was more recent than the PGY-2 and PGY-3 classes. Although the innovative algorithm was more likely to be incorporated by the younger PGY class, the knowledge-based cardiac ultrasound questionnaire scores improved across PGY class. This is expected as clinical knowledge should improve throughout residency training.
This diagnostic algorithm for the undifferentiated chest pain patient is unique and our study indicates that it can be easily learned. Unfortunately, it is possible that the complexity of such an algorithm can make it difficult to incorporate into clinical practice. During the month immediately after this workshop, residents performed 181 cardiac ultrasounds; during the previous 3 months, an average of 155 cardiac ultrasounds had been performed. Only 8% of residents stated that they had incorporated the undifferentiated chest pain algorithm into their practice more than six times. Future studies should be conducted to determine methods for improving the implementation of this goal-directed ultrasound algorithm in clinical practice as well as its impact on patient outcomes.
Limitations
This study has several limitations, including a small sample size. Furthermore, the education and assessment curriculum was neither pilot tested nor validated prior to implementation. In this study we did not conduct the necessary pretesting of residents required to fully evaluate the overall effectiveness of our novel algorithm and curriculum. Residents’ knowledge retention was assessed; however, we did not test the residents’ ability to determine pathology, as we could not replicate sonographic pathology in a standardized fashion. During assessment of the OSCE, a checklist was used, which was designed to be dichotomous and simple with the hope of eliminating any bias introduced by the evaluators. This checklist had not been previously validated. Our study was not designed to assess the overall clinical impact of this algorithm-based ultrasound workshop. Furthermore, this ultrasound workshop is not sufficiently capable of teaching all the complexities and nuances of transthoracic echocardiography, nor was the workshop designed to eliminate the need for patient medical history, physical examination, and blood sampling. Finally, the follow-up survey was conducted only 1 month after the session; as a result, the frequency of use of the chest pain algorithm may have been underrepresented.
Conclusion
The 1-day algorithm-based ultrasound educational workshop was an engaging learning technique at our institution.
Acknowledgment
This abstract was presented at the Western Society for Academic Emergency Medicine Annual National Meeting in Tucson, AZ on March 27, 2015.
Disclosure
The authors report no conflicts of interest in this work.
References
Schmidt GA, Koenig S, Mayo PH. Shock: ultrasound to guide diagnosis and therapy. Chest. 2012;142(4):1042–1048. | ||
Jones AE, Tayal VS, Sullivan DM, Kline JA. Randomized, controlled trial of immediate versus delayed goal-directed ultrasound to identify the cause of nontraumatic hypotension in emergency department patients. Crit Care Med. 2004;32(8):1703–1708. | ||
Manno E, Navarra M, Faccio L, et al. Deep impact of ultrasound in the intensive care unit: the “ICU-sound” protocol. Anesthesiology. 2012;117(4):801–809. | ||
Rose JS, Bair AE, Mandavia D, Kinser DJ. The UHP ultrasound protocol: a novel ultrasound approach to the empiric evaluation of the undifferentiated hypotensive patient. Am J Emerg Med. 2001;19(4): | ||
Volpicelli G, Lamorte A, Tullio M, et al. Point-of-care multiorgan ultrasonography for the evaluation of undifferentiated hypotension in the emergency department. Intensive Care Med. 2013;39(7): | ||
Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg Med Clin North Am. 2010;28(1):29–56, vii. | ||
Lichtenstein DA, Mezière GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest. 2008;134(1): | ||
Amini R, Stolz LA, Gross A, et al. Theme-based teaching of point-of-care ultrasound in undergraduate medical education. Intern Emerg Med. 2015;10(5):613–618. | ||
Lewiss RE, Pearl M, Nomura JT, et al. CORD-AEUS: consensus document for the emergency ultrasound milestone project. Acad Emerg Med. 2013;20(7):740–745. | ||
Noble VE, Nelson BP, Sutingco AN, Marill KA, Cranmer H. Assessment of knowledge retention and the value of proctored ultrasound exams after the introduction of an emergency ultrasound curriculum. BMC Med Educ. 2007;7:40. | ||
Kerwin C, Tommaso L, Kulstad E. A brief training module improves recognition of echocardiographic wall-motion abnormalities by emergency medicine physicians. Emerg Med Int. 2011;2011:483242. | ||
Amini R, Adhikari S, Fiorello A. Ultrasound competency assessment in emergency medicine residency programs. Acad Emerg Med. 2014;21(7):799–801. | ||
Hoyer R, Means R, Robertson J, et al. Ultrasound-guided procedures in medical education: a fresh look at cadavers. Intern Emerg Med. Epub 2015 Aug 15. | ||
Amini R, Kartchner JZ, Stolz LA, Biffar D, Hamilton AJ, Adhikari S. A novel and inexpensive ballistic gel phantom for ultrasound training. World J Emerg Med. 2015;6(3):225–228. | ||
Amini R, Kartchner JZ, Nagdev A, Adhikari S. Ultrasound-guided nerve blocks in emergency medicine practice. J Ultrasound Med. 2016;35(4):731–736. | ||
Parks AR, Atkinson P, Verheul G, Leblanc-Duchin D. Can medical learners achieve point-of-care ultrasound competency using a high-fidelity ultrasound simulator?: a pilot study. Crit Ultrasound J. 2013;5(1):9. | ||
Jones AE, Tayal VS, Kline JA. Focused training of emergency medicine residents in goal-directed echocardiography: a prospective study. Acad Emerg Med. 2003;10(10):1054–1058. | ||
Hofer M, Kamper L, Sadlo M, Sievers K, Heussen N. Evaluation of an OSCE assessment tool for abdominal ultrasound courses. Ultraschall Med. 2011;32(2):184–190. | ||
Newble D. Techniques for measuring clinical competence: objective structured clinical examinations. Med Educ. 2004;38(2):199–203. | ||
Sisley AC, Johnson SB, Erickson W, Fortune JB. Use of an Objective Structured Clinical Examination (OSCE) for the assessment of physician performance in the ultrasound evaluation of trauma. J Trauma. 1999;47(4):627–631. |
Supplementary materials
 | Figure S1 Questionnaire |
 | Figure S2 Undifferentiated chest pain objective standardized clinical exam |
 | Figure S3 Follow-up survey |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.