Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Barriers and Facilitators to Inhaler Adherence in Elderly Individuals with Chronic Obstructive Pulmonary Disease: A Qualitative Study
Authors Liu YR, Zhang W, Huang Y, Peng X, Sun K, Wu Z, Wang H, Ji X, Wang J
Received 13 July 2025
Accepted for publication 4 November 2025
Published 27 November 2025 Volume 2025:20 Pages 3827—3838
DOI https://doi.org/10.2147/COPD.S553540
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vanesa Bellou
You-Ran Liu,1 Wenzhong Zhang,2 Yaqi Huang,3 Xiulan Peng,4 Kangming Sun,5 Zhiying Wu,6 Huadong Wang,4 Xiaomei Ji,7 Jie Wang7
1The Nethersole School of Nursing, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China; 2School of Nursing and Rehabilitation, Cheeloo College of Medicine, Shandong University, Jinan, Shandong Province, People’s Republic of China; 3School of Nursing, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China; 4Department of Respiratory Medicine, The First Affiliated Hospital of Bengbu Medical University, Bengbu, Anhui Province, People’s Republic of China; 5Nursing Department, The First Affiliated Hospital of Shandong First Medical University, Jinan, Shandong Province, People’s Republic of China; 6School of Nursing, Anhui Medical University, Hefei, Anhui Province, People’s Republic of China; 7School of Nursing, Bengbu Medical University, Bengbu, Anhui Province, People’s Republic of China
Correspondence: Jie Wang, School of nursing, Bengbu Medical University, No. 2600 Donghai Avenue, Bengbu, People’s Republic of China, Tel +86 18255208691, Email [email protected]
Background: Inhalation therapy is the mainstay of pharmacological treatment for patients with chronic obstructive pulmonary disease (COPD). Elderly individuals with COPD often face greater challenges in using inhalers, and their experiences with inhaler use significantly influence treatment adherence and outcomes. Therefore, it is imperative to understand barriers and facilitators influencing inhaler adherence among elderly COPD patients, based on their perceptions and experiences with inhaled medications.
Methods: A descriptive qualitative study was conducted using semi-structured interviews with elderly COPD patients recruited from a tertiary hospital in China. Data were analyzed through conventional content analysis with NVivo 11.
Results: A total of 20 participants (mean age: 75.9 years; 35% female) completed the interviews. Two themes with six subthemes were identified. The two themes were facilitators for inhaler adherence and barriers to inhaler adherence. Facilitators included perceived manageability of inhaler devices and perceived benefits of inhalation therapy. Barriers involved physical limitations, communication challenges between patients and health providers, forgetfulness, and inconvenient refill policies.
Conclusion: Adapting and optimizing inhaler devices to patient needs, increasing patient awareness of the benefits of inhalation therapy, and establishing continuous, effective pathways of patient-provider communication may represent promising approaches to improve inhaler adherence in elderly individuals with COPD.
Keywords: adherence, COPD, inhalation therapy, qualitative study, barriers, facilitators
Introduction
Between 2020 and 2050, chronic obstructive pulmonary disease (COPD) is projected to cause a global economic loss of approximately 4.3 trillion USD, with China bearing the largest absolute economic burden.1 As a progressive chronic disease, COPD typically includes periods of acute exacerbation and stable phases. Due to factors such as an aging population, widespread exposure to smoking, ongoing indoor and outdoor air pollution, the prevalence of COPD in China continues to rise.2 COPD is currently the fifth leading cause of death in China, posing a major public health challenge. Patients who experience three or more acute exacerbations are at the highest risk of mortality.3 COPD exacerbations are episodes of worsening respiratory symptoms,4 and are associated with serious adverse outcomes, including accelerated decline in lung function, impaired quality of life and higher mortality. Therefore, the primary goals of treatment during the stable phase of COPD are to alleviate symptoms and reduce the risk of acute exacerbations.
Pharmacological treatments can alleviate the disease symptoms of COPD, reduce the frequency and severity of acute exacerbations, and enhance overall health status.5 Inhaled therapy is the first-line approach and serves as the cornerstone of long-term COPD management.6 Compared to oral medications, inhaled drugs deliver medication directly to the affected bronchi,7 thereby minimizing systemic side effects and offering superior efficacy and safety. The Canadian Thoracic Society’s pharmacological treatment guidelines recommend earlier and more proactive initiation of maintenance inhaler therapy across all stages of COPD severity.8 Adherence to inhaled medication is a key determinant of successful COPD management, with correct inhaler technique and good compliance being essential for therapeutic effectiveness.9 Poor adherence to inhaler therapy increases the risk of COPD exacerbations by up to 40%.10 Despite efforts from both healthcare providers and patients, the correct usage rate is still low.11,12 Adherence to prescribed regimens remains a significant challenge, particularly among elderly patients.
Elderly patients with COPD often experience difficulties using inhaler devices due to impaired vision, cognitive decline, or motor dysfunction of the fingers, which can negatively impact their adherence to inhalation therapy.13 Previous findings indicated that only 15.7% of elderly Chinese COPD patients showed moderate or higher adherence to inhaler therapy,14 a proportion lower than the 25.9% reported in a study from Greece15 and the 33.6% observed in a survey conducted in Upper Austria.16 Complex medication regimens and the use of multiple inhaler devices can further compromise adherence among older COPD patients. Switching between devices may necessitate the adoption of new or multiple inhaler techniques, which can be particularly challenging for elderly individuals due to age-related physical and cognitive decline that hinders their ability to learn and retain necessary skills.17,18 Additionally, limited disease perception19 and heightened concerns about medication20 among elderly COPD patients further contribute to poor adherence to inhaled treatment regimens. Moreover, social factors such as inadequate inhaler technique training and low levels of family support have also been associated with poor adherence.21,22 Identifying these barriers is a prerequisite for developing targeted inhaler technique education strategies and improving disease management in elderly COPD patients.
Although previous studies have explored factors influencing inhaler adherence in elderly patients with COPD through questionnaires and data analysis, adherence remains a complex and subjective phenomenon. Quantitative research is limited in its ability to fully capture patients’ subjective meanings, practical challenges, and contextual factors during inhalation therapy. There is limited understanding of how patients perceive inhaler use and which factors they consider most important in supporting adherence to inhaled therapy for COPD. Qualitative research can offer a more comprehensive understanding of inhaler adherence by revealing potential barriers and facilitators through in-depth exploration of patients’ experiences with inhaled medications, thereby offering unique evidence to inform patient-centered interventions and strengthen guidance for clinical practice and policy decisions. However, studies that have been conducted have either used telephone interview methods that do not allow for observation of participants’ nonverbal responses,23 or interviews with patients with chronic respiratory diseases (including those with asthma and COPD) to explore the factors that influence the use of inhaler devices.24 There is limited qualitative data in elderly patients with COPD, particularly in populations with low education levels. Given that COPD predominantly affects older adults who face greater challenges in using inhalers, there is a critical need to understand inhaler use from their perspective for improve adherence.
Therefore, this study adopts a qualitative descriptive approach through face-to-face interviews to explore barriers and facilitators to inhaler adherence based on the perspectives and experiences of elderly COPD patients with inhaler use. The findings will be used to develop targeted strategies to improve patients’ adherence behaviors, which could promote health outcomes and long-term management of COPD patients.
Method
Study Design
A qualitative descriptive study was conducted using semi-structured interviews to explore the barriers and facilitators to inhaler use and adherence among older adults with COPD. This study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.25
Setting and Participants
Between February and May 2024, a purposive sample of elderly patients with COPD who were hospitalized in the respiratory medicine department of a tertiary hospital in Anhui Province were recruited. Inclusion criteria were: (1) age ≥60 years; (2) meeting the diagnostic criteria outlined in the Guidelines for the Diagnosis and Treatment of COPD (2021 Revision); (3) having used an inhaler device for more than 3 months prior to the study; and (4) willingness to provide informed consent. Exclusion criteria included: (1) coexisting respiratory diseases (eg, asthma, bronchiectasis); (2) having severe comorbidities involving other systems, (eg, advanced heart, liver, or kidney failure); and (3) having diagnosed mental disorders. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Bengbu Medical University (No. [2022] 106). Written informed consent was obtained from all participants prior to data collection, and the participants informed consent included publication of anonymized responses.
Data Collection
During the recruitment phase, the researchers explained the study’s purpose and procedures to hospital nurses, who then recommended eligible participants based on their familiarity with the patients from February to May 2024. The researchers approached individuals who met the inclusion and exclusion criteria and invited them to participate. For those who agreed, face-to-face semi-structured interviews were scheduled at a time convenient for the participants. All interviews were independently conducted by a master’s student in nursing to minimize interviewer-related bias. The interviewer had received formal training in qualitative research methods, including semi-structured interviewing techniques, and had prior experience in conducting qualitative studies. Interviews were carried out either in a private office of the hospital’s respiratory department or in the participant’s ward under conditions that ensured privacy. No others were present during the interviews, allowing participants to freely share their experiences and perspectives. A semi-structured interview guide was developed based on the research objectives and relevant literature, including one introductory question, several prompts to encourage participants to share their experiences, and a concluding question (Table 1). The guide was pilot-tested with the first two participants, until no modification was necessary; ultimately, 11 open-ended questions were finalized.
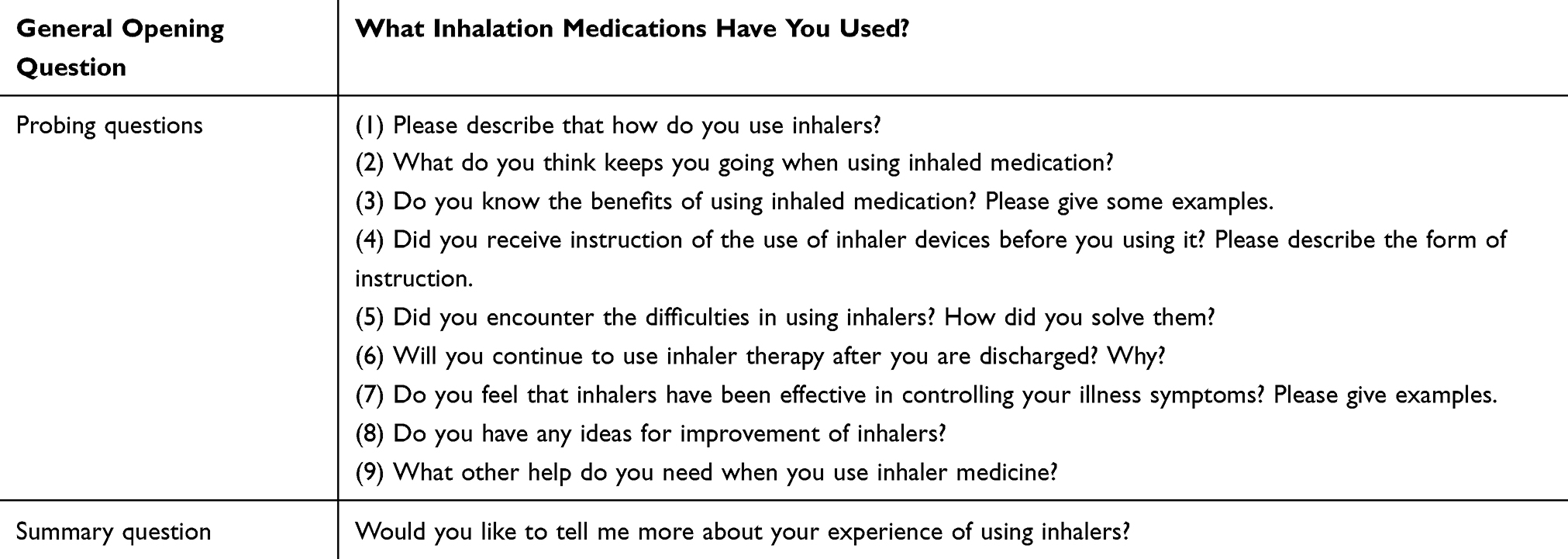 |
Table 1 Interview Guide |
Prior to the interview, the researcher explained the purpose, procedures, and content of the interview. Written informed consent was obtained from each participant. Interviews were audio-recorded using a mobile device to facilitate data preservation. The interviewer maintained a neutral stance throughout the interviews and encouraged participants to fully express their genuine thoughts and feelings. During the interviews, the interviewer listened attentively and respectfully, asked probing questions, and made suggestions where appropriate. Non-verbal cues such as tone, facial expressions, and body language were also documented in detail. Clarifications were sought in real time whenever participant responses were ambiguous. The duration of the interviews ranged from 20 to 40 minutes. Verbatim transcription of the audio recordings was completed within 48 hours of each interview. Any unclear information in the transcripts was clarified by contacting the respective participants. Throughout the qualitative study, the research team held biweekly group discussions to reflect on the interviewer’s role and positioning. This process ensured that data interpretation remained grounded in participants’ narratives and maintained rigor across data collection, transcription, and analysis. Interviews and recruitment continued until the content of the interviews no longer provided any new information.26 Saturation was considered to be reached when the information provided by new participants substantially overlapped with existing themes and no new themes emerged. After 20 participants were interviewed, no new themes emerged, suggesting that data saturation had been reached.
Data Analysis
The interview data were analyzed in this study using content analysis, a method that integrates separated information to generate content relevant to the research topic.27 All interview data were transcribed sentence-by-sentence and then the data were coded and analyzed using NVivo 11 software. Initially, a new project was created in NVivo and the textual data were imported. The transcripts were reviewed line by line, and relevant excerpts were coded by creating free nodes to capture preliminary concepts. These free nodes were subsequently organized into hierarchical tree nodes to form categories. Use the “Query” function to run the “Code Comparison” check for consistency across coders. Through iterative refinement, nodes were gradually merged into higher-order themes, and ultimately completing systematic coding. Two researchers independently read through each transcript in detail to generate initial codes. These codes were then compared and grouped into subcategories based on similarities and differences, which were subsequently organized into overarching categories reflecting common themes. Any discrepancies in coding were resolved through discussion to ensure the reliability of the analysis. All authors examined and reported the results of the study. Discrepancies were discussed by all authors until a consensus was reached.
Results
A total of 20 participants (35% female) participated in the interview. The mean age of the participants was 75.90 years (SD = 6.98), with an age range of 62 to 86 years. The mean duration of illness among participants was 15.45 years (SD = 13.62). Of the participants, 12 used a budesonide inhaler exclusively, 3 used a budesonide-formoterol powder inhaler exclusively, and 1 used an albuterol inhaler exclusively. Additionally, 2 participants used a combination of the budesonide inhaler and the budesonide-formoterol powder inhaler, while another 2 used a combination of the budesonide inhaler and the albuterol inhaler. Table 2 presents the detailed demographic characteristics of the participants.
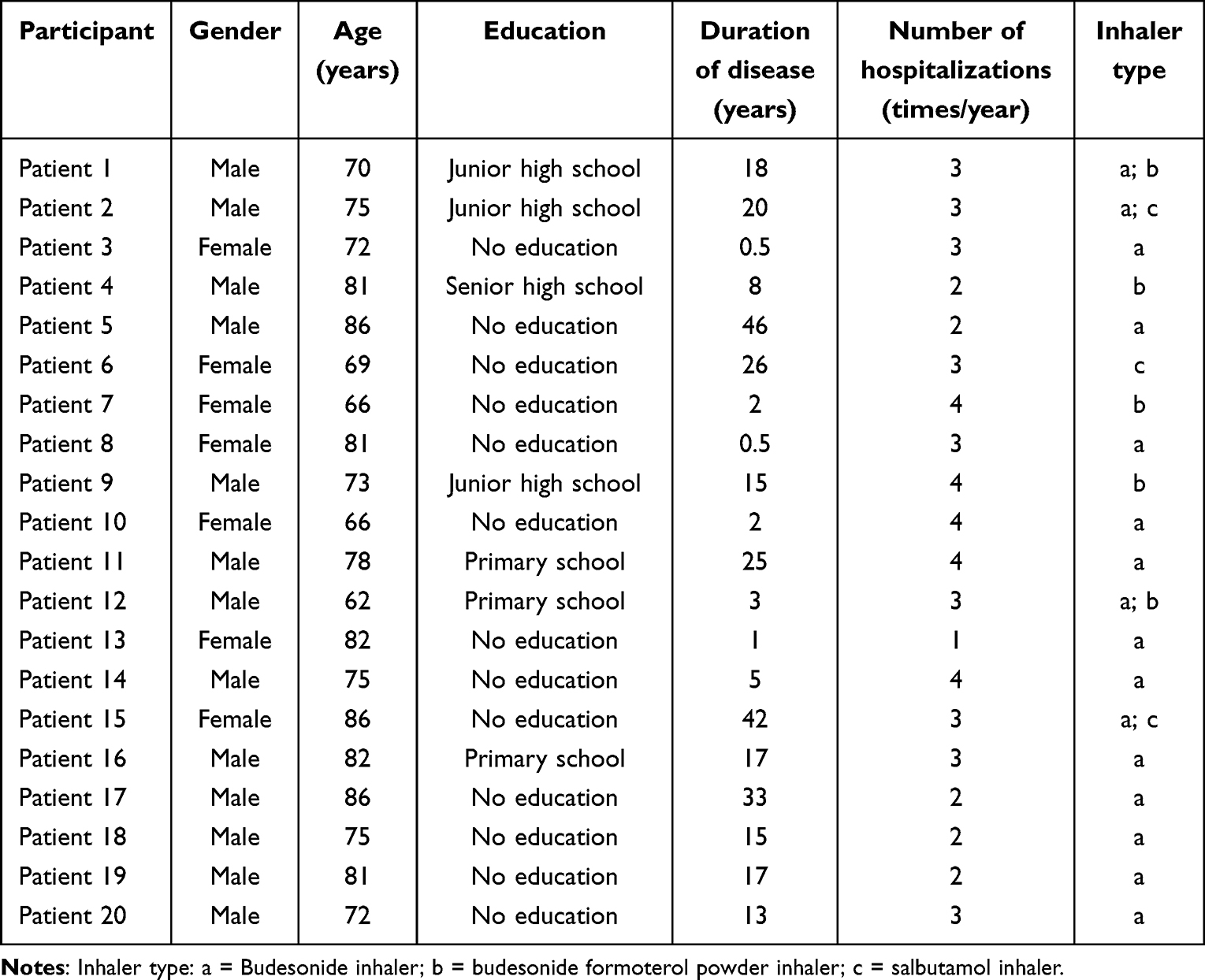 |
Table 2 Participant Demographics and Clinical Information |
Through content analysis of the qualitative data, two themes and six sub-themes that affect the adherence to inhalation therapy in older individuals with COPD were summarized: (1) Facilitators for inhaler adherence, (2) Barriers to inhaler adherence, see Table 3.
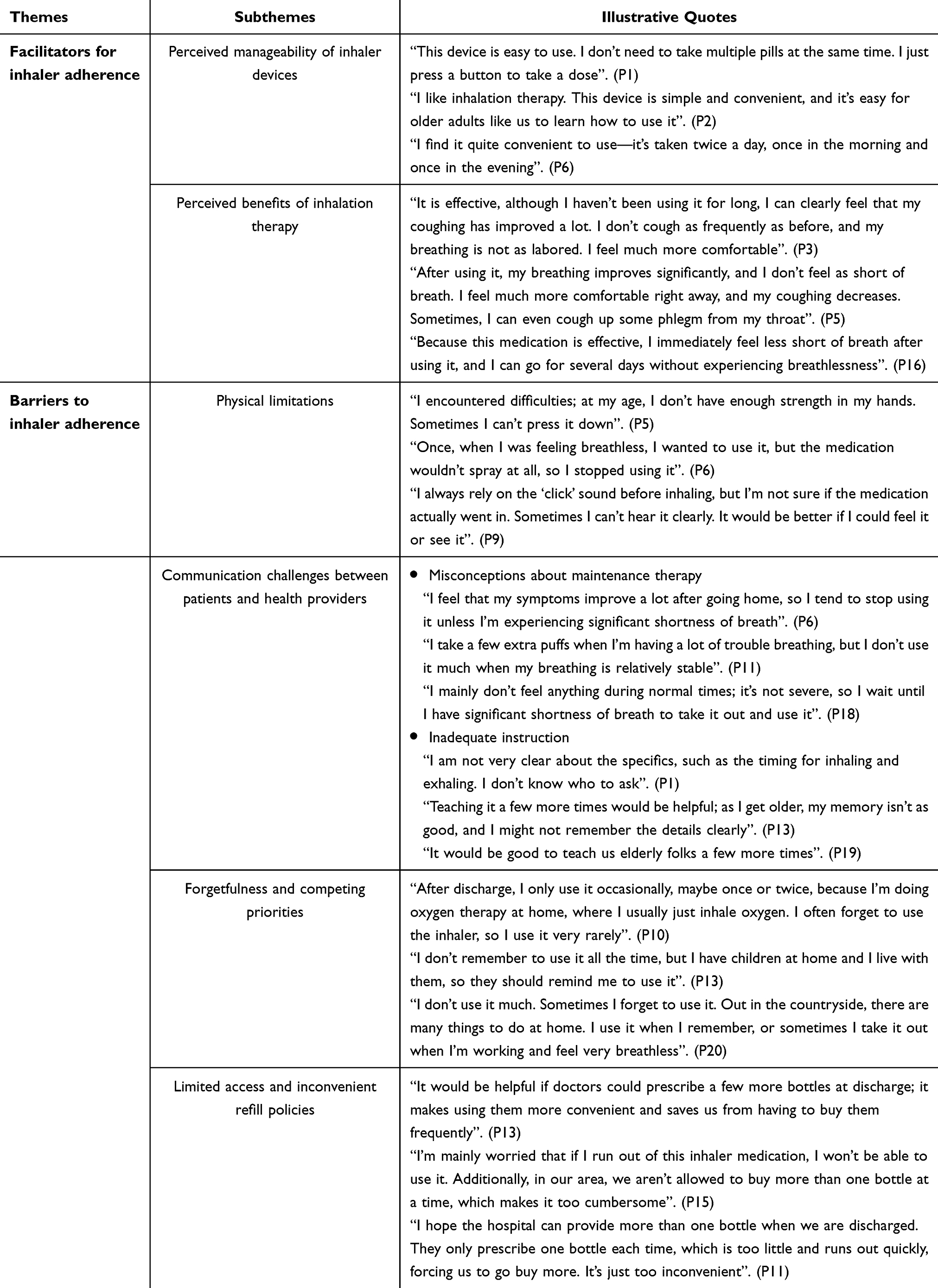 |
Table 3 Distribution of Themes and Subthemes |
Theme 1: Facilitators for Inhaler Adherence
The primary facilitators of inhaler use among individuals with COPD were participants’ perceptions of the manageability of inhaler devices and the benefits offered by the inhalation therapy, which increased their behaviors to continue therapy.
Perceived Manageability of Inhaler Devices
A prominent facilitator of inhaler adherence among participants was the perceived manageability of inhaler devices. Some participants described the inhaler device as easy to handle, requiring minimal effort or technical skill, which fostered a sense of independence and confidence of self-management. The straightforward mechanism of use, such as pressing a button, was especially valued. Furthermore, the regular dosing schedule, usually twice a day in the morning and evening, was also considered manageable and easy to integrate into daily routines.
This device is easy to use. I don’t need to take multiple pills at the same time. I just press a button to take a dose. (P1)
I like inhalation therapy. This device is simple and convenient, and it’s easy for older adults like us to learn how to use it. (P2)
I find it quite convenient to use—it’s taken twice a day, once in the morning and once in the evening. (P6)
I find it convenient to use in daily life. There’s no need to prepare the medicine — once I hear the ‘click’ sound, the medication comes up and I just inhale it. (P9)
Perceived Benefits of Inhalation Therapy
Another key facilitator to inhaler adherence was the perceived benefits of inhaler therapy. Participants consistently described significant improvements in symptoms such as coughing and breathlessness after inhaler use. Some participants noted a rapid onset of action with some experiencing immediate relief. Furthermore, the inhaler therapy was also described as providing sustained benefits, reducing the frequency and severity of symptoms over time. These positive experiences reinforced older adults’ motivation to adhere to the prescribed inhaler regimen.
It is effective, although I haven’t been using it for long, I can clearly feel that my coughing has improved a lot. I don’t cough as frequently as before, and my breathing is not as labored. I feel much more comfortable. (P3)
After using it, my breathing improves significantly, and I don’t feel as short of breath. I feel much more comfortable right away, and my coughing decreases. Sometimes, I can even cough up some phlegm from my throat. (P5)
Because this medication is effective, I immediately feel less short of breath after using it, and I can go for several days without experiencing breathlessness. (P16)
Theme 2: Barriers to Inhaler Adherence
Participants encountered various obstacles on consistent inhaler use. For some, physical limitations posed a significant challenge. Others descried poor communication of disease and treatment between patients and health providers as affecting medication-taking behaviors. Moreover, forgetfulness and restrictive medication refill policies represent additional barriers to sustained adherence to inhalation therapy among elderly patients with COPD.
Physical Limitations
Several participants encountered physical barriers related to aging that hindered effective device use. Specifically, reduced hand strength made it difficult for some to press down on the inhaler mechanism, limiting their ability to administer the medication independently.
I encountered difficulties; at my age, I don’t have enough strength in my hands. Sometimes I can’t press it down. (P5)
Once, when I was feeling breathless, I wanted to use it, but the medication wouldn’t spray at all, so I stopped using it. (P6)
Participants expressed the need for improvements to make inhalers easier to press. In addition, reliance on auditory feedback (eg, a “click” sound) was perceived as uncertain as a result of hearing loss in the elderly, and participants suggested a desire for visual indicators of medication dosage.
As I get older, I don’t have much strength in my hands. If the pressing mechanism could be improved to require less effort, it would be much better. (P5)
I always rely on the ‘click’ sound before inhaling, but I’m not sure if the medication actually went in. Sometimes I can’t hear it clearly. It would be better if I could feel it or see it. (P9)
For this budesonide-formoterol inhaler, it would be great if I could see how much is left in the device. (P12)
Communication Challenges Between Patients and Health Providers
Misconceptions About Maintenance Therapy
A key barrier to adherence was the misconception that inhalation therapy is only necessary when symptoms are present. Participants indicated that if their symptoms improved after discharge from the hospital, they were less likely to continue adhering to treatment. Some participants in the interviews indicated tended to adjust the number of times the inhalation device was used based on their disease symptoms, suggesting that there are individual misconceptions about the disease and inhalation therapy. This belief led to a reactive approach to inhaler use, that means, participants used medication only during episodes of noticeable symptoms, such as coughing and wheezing, rather than following a consistent, preventive treatment regimen.
I feel that my symptoms improve a lot after going home, so I tend to stop using it unless I’m experiencing significant shortness of breath. (P6)
I take a few extra puffs when I’m having a lot of trouble breathing, but I don’t use it much when my breathing is relatively stable. (P11)
I mainly don’t feel anything during normal times; it’s not severe, so I wait until I have significant shortness of breath to take it out and use it. (P18)
Inadequate Instruction
Inadequate instruction for inhalers use was identified as a barrier to inherence. Patients fail to grasp the steps of medication (such as the inhalation and exhalation times) when using inhaler devices but do not have a way to communicate with their medication providers. Some participants expressed that health professionals could teach the inhaler technique knowledge more often, which would make them remember it more firmly.
I am not very clear about the specifics, such as the timing for inhaling and exhaling. I don’t know who to ask. (P1)
Teaching it a few more times would be helpful; as I get older, my memory isn’t as good, and I might not remember the details clearly. (P13)
It would be good to teach us elderly folks a few more times. (P19)
Some participants indicated they would like to have channels for ongoing communication with healthcare providers regarding disease and medication-related knowledge. At the same time, participants said that providers could speak more slowly during the teaching so that they could remember more clearly.
I didn’t know much about how to inhale, hold my breath, or the need to rinse my mouth. If I forget in the future, I can always ask the doctors and nurses to learn again. (P3)
It would be helpful if you could provide more detailed instructions and speak more slowly so that we can better understand how this medication works. (P16)
Forgetfulness and Competing Priorities
Forgetfulness emerged as a common barrier to regular inhaler adherence, particularly after discharge from the hospital. Many participants reported infrequent inhaler use, often due to forgetfulness, especially when fully occupied with daily household tasks or relying more heavily on home oxygen therapy. In some cases, participants expected family members to remind them to use the inhaler, whereas such support was not always consistently available.
After discharge, I only use it occasionally, maybe once or twice, because I’m doing oxygen therapy at home, where I usually just inhale oxygen. I often forget to use the inhaler, so I use it very rarely. (P10)
“I don’t remember to use it all the time, but I have children at home and I live with them, so they should remind me to use it. (P13)
I don’t use it much. Sometimes I forget to use it. Out in the countryside, there are many things to do at home. I use it when I remember, or sometimes I take it out when I’m working and feel very breathless. (P20)
Limited Access and Inconvenient Refill Policies
Limited access to inhaler medications and restrictive refill policies emerged as practical barriers to adherence. Some participants noted that purchasing inhalers was a hassle, and they were concerned that running out of medication could negatively impact their long-term treatment. Additionally, they felt that inhalers were consumed quickly, leading to a desire for the ability to purchase more bottles at once to minimize unnecessary inconveniences.
It would be helpful if doctors could prescribe a few more bottles at discharge; it makes using them more convenient and saves us from having to buy them frequently. (P13)
I’m mainly worried that if I run out of this inhaler medication, I won’t be able to use it. Additionally, in our area, we aren’t allowed to buy more than one bottle at a time, which makes it too cumbersome. (P15)
I hope the hospital can provide more than one bottle when we are discharged. They only prescribe one bottle each time, which is too little and runs out quickly, forcing us to go buy more. It’s just too inconvenient. (P11)
Discussion
This study identified the facilitators and barriers to inhaler adherence using semi-structured interviews among elderly COPD patients in China, a population rarely addressed in previous qualitative research. Beyond correct inhaler technique, our findings emphasize the importance of enhancing patients’ understanding of the necessity of inhaled medications. Key facilitators of adherence included perceived manageability of inhaler devices and perceived benefits of inhalation therapy, while barriers encompassed physical limitations, communication challenges, forgetfulness, and inconvenient refill policies due to constraints within China’s healthcare system. These findings highlight the unique challenges faced by Chinese elderly COPD patients and extend existing knowledge. Such insights provide practical guidance for designing targeted educational and interventional strategies to improve inhaler adherence in this population.
Perceived manageability of inhaler devices, mainly tied to ease of use and convenience, was a key facilitator of adherence. A study conducted in Germany compared the popularity and preferences of various inhaler devices among patients with COPD and asthma, and the findings indicated that ease of use was the most valued factor when participants selected an inhaler.28 The ease of use of inhalers was also found to influence patients’ inhaler adherence.29 Simple device operation improved satisfaction and acceptance, both linked to better adherence.30,31 In addition, participants reported that the convenience of inhaled medication contributed to a more manageable treatment experience. Specifically, not having to remember multiple types and dosages of pills and simply pressing a button to complete the medication regimen. Since inhaled medication therapy is the use of a combination of medication and device, it may be an effective approach to improving adherence to inhaled medications by enhancing individual satisfaction and acceptability of the inhaled device.
A cross-sectional study conducted in Portugal found that COPD patients’ beliefs about the necessity of medication were associated with their ability to use inhaler therapy,32 which is consistent with the findings of this study. This study revealed that the perception of therapeutic benefits plays a crucial role in promoting adherence to inhaler use among elderly individuals with COPD in China. During the interviews, participants reported symptom relief from inhaled medications, which reinforced their perceived efficacy and promoted proactive adherence to prescribed regimens by healthcare professionals. This situation aligns with the “perceived benefits” component of the Health Belief Model,33,34 which suggests that individuals’ perceived benefits are a key factor in motivating engagement in health-related behaviors. Yet, study have shown that Chinese patients with COPD often lack clarity regarding the effectiveness of inhaled medications.35 Meanwhile, a qualitative study conducted in the United States interviewed 30 patients with COPD and found that challenges to medication adherence also included gaps in understanding the effects and benefits of the drugs.23 Therefore, health providers could further consider improving patients’ understanding of inhaled medications by providing detailed information about the medication’s effects, therapeutic benefits, and long-term benefits such as symptomatic relief, in order to improve patients’ perception of the benefits of inhaled medications, which could increase adherence to medications.
However, communication between patients and health providers needs to be improved. If there are misconceptions about patients’ understanding of maintenance inhalation therapy and inconsistent communication of instructions for inhalation device use, this can affect patients’ adherence to inhalation therapy regimens. Consistent with our finding, a qualitative study conducted in New Brunswick employed semi-structured interviews with 20 community-dwelling elderly COPD patients and revealed a strong desire for more information about COPD from healthcare providers.36 Although many studies have advocated the need to increase patients’ disease knowledge37–39 and have constructed and explored intervention strategies,40,41 they have not been widely applied in the clinic and community, and patients’ understanding of their disease and treatment still needs to be improved. In addition, there are also individuals who take the wrong steps in the medication process but are left uninstructed, which hinders the therapeutic effects of inhaled medications. Health providers play a key role in increasing patient awareness of the disease and improving inhaled medication techniques. Therefore, there should be a clear and continuous communication channel between the health provider and the patient, with regular visits to assess the patient’s technique of using the device and to ensure that the patient can correctly understand the disease process, the indicators of therapeutic efficacy, and the correct use of the medication device. Simultaneously, e-Health tools offer a promising approach to improve communication pathways and update communication methods42 to ensure continuous and effective communication between patients and health professionals.
Furthermore, the results of this study indicated that participants with COPD faced challenges in using inhalers, including physical limitations, medication forgetfulness and restricted refill policies. Consistent with the findings of Renaud et al,43 participants in this study reported that diminished muscle strength adversely affected their ability to use inhaled medications effectively. A study conducted in Germany implemented an 8-day intensive training program for older patients with COPD, consisting of daily counseling and video demonstrations, which resulted in improved inhaler technique, reduced clinical symptoms, and benefits even among those with cognitive impairments.13 Therefore, adapting and optimizing inhaler devices to the preferences of elderly patients, along with implementing appropriate intervention training, may facilitate behaviors that promote inhalation therapy adherence in elderly patients. Additionally, some participants exhibited tendencies toward medication forgetfulness, influencing them to follow the treatment regimen, similar to the findings of a systematic review.44 Patients may forget to take their medication due to a number of competing things (busy with household chores) can forget to adhere the inhalation therapy, which aligns with the findings of a study conducted in the USA.23 Therefore, health providers should encourage patients to establish medication routines while on maintenance inhalation therapy at home, such as fixing the time and place of medication taken. Inhaler adherence can also be improved through assistance from an educated family members or caregivers.45 What’s more, China’s healthcare system constraints limit patients’ ability to obtain an adequate supply of inhaled medications in a single purchase. Participants preferred larger inhaler prescriptions to better meet long-term needs. Policymakers should comprehensively consider patient preferences and other factors to develop policies enabling longer-term prescriptions and improving inhaler access to reduce patients’ burden.
Limitations
This study has several limitations. First, the severity of COPD (GOLD stage, pulmonary function tests) was not reported, which could affect COPD patients’ inhaler use experience. Future research could examine how these experiences vary with the severity of disease. Second, despite caregivers’ crucial role in COPD adherence,45 they were not interviewed; their perspectives warrant exploration to enrich understanding. Finally, this study was a single-center design with 20 participants from a tertiary hospital in China, which may affect the generalizability of the findings.
Conclusions
This study identified the barriers and facilitators for inhaler adherence among older adults with COPD based on the elderly patients’ lived experiences. To develop effective and sustainable interventions aimed at improving inhaler adherence among elderly patients with COPD, it is essential to consider the key facilitators and barriers identified in this population. Adapting inhaler devices to patient needs, increasing patient awareness of the benefits of inhalation therapy, and establishing continuous, effective pathways of patient-provider communication may represent promising approaches to improve inhaler adherence in elderly individuals with COPD.
Data Sharing Statement
To protect patient privacy, only core members of the project team have access to the data material and the data are not publicly available.
Ethics Approval
The study received approval and consent from the Ethics Committee of Bengbu Medical University.
Consent for Publication
All participants provided written informed consent. And the participants informed consent included publication of anonymized responses/direct quotes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Bengbu Medical University (2024byzd142sk).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020–50: a health-augmented macroeconomic modelling study. Lancet Glob Health. 2023;11:e1183–e1193.
2. Liang Y, Sun Y. COPD in China: current status and challenges. Arch Bronconeumol. 2022;58:790–791. doi:10.1016/j.arbres.2022.04.001
3. Soler-Cataluña J, Martínez-García MA, Román Sánchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60:925–931. doi:10.1136/thx.2005.040527
4. Lange P, Celli B, Agustí A, et al. Lung-function trajectories leading to chronic obstructive pulmonary disease. N Engl J Med. 2015;373(2):111–122. doi:10.1056/NEJMoa1411532
5. Carlin BW. Exacerbations of COPD. Resp Care. 2023;68:961–972. doi:10.4187/respcare.10782
6. Terzano C, Oriolo F. Lung characteristics in elderly males and females patients with COPD: differences and optimal use of dry powder inhalers (DPIs). Eur Rev Med Pharmacol Sci. 2017;21:1.
7. Dougall S, Bolt J, Semchuk W, Winkel T. Inhaler assessment in COPD patients: a primer for pharmacists. Can Pharm J/Revue Des Pharmaciens du Canada. 2016;149:268–273. doi:10.1177/1715163516660573
8. Kaplan A, Babineau A, Hauptman R, et al. Breaking down barriers to COPD management in primary care: applying the updated 2023 Canadian Thoracic Society guideline for pharmacotherapy. Front Med. 2024;11:1416163. doi:10.3389/fmed.2024.1416163
9. Price D, Keininger DL, Viswanad B, et al. Factors associated with appropriate inhaler use in patients with COPD – lessons from the REAL survey. Int J Chronic Obstr. 2018;Volume 13:695–702. doi:10.2147/COPD.S149404
10. Vauterin D, Van Vaerenbergh F, Grymonprez M, Vanoverschelde A, Lahousse L. Medication adherence to inhalation therapy and the risk of COPD exacerbations: a systematic review with meta-analysis. BMJ Open Resp Res. 2024;11:e001964. doi:10.1136/bmjresp-2023-001964
11. Bao LK, Khoa ND, Chi LTK, Anh NT. Prevalence and factors affecting appropriate inhaler use in elderly patients with chronic obstructive pulmonary disease: a prospective study. J Clin Med. 2023;12:4420. doi:10.3390/jcm12134420
12. Molimard M, Raherison C, Lignot S, et al. Chronic obstructive pulmonary disease exacerbation and inhaler device handling: real-life assessment of 2935 patients. Eur Respir J. 2017;49(2):1601794. doi:10.1183/13993003.01794-2016
13. Luley M-C, Loleit T, Knopf E, et al. Training improves the handling of inhaler devices and reduces the severity of symptoms in geriatric patients suffering from chronic-obstructive pulmonary disease. BMC Geriatr. 2020;20(1):1–8. doi:10.1186/s12877-020-01804-4
14. Liu Y-R, Wang Y, Chen J, et al. Developing and validating a nomogram for non-adherence to inhaler therapy among elderly chronic obstructive pulmonary disease patients based on the social ecological model. Patient Preference Adherence. 2024;Volume 18:1741–1753. doi:10.2147/PPA.S472625
15. Ierodiakonou D, Sifaki-Pistolla D, Kampouraki M, et al. Adherence to inhalers and comorbidities in COPD patients. A cross-sectional primary care study from Greece. BMC Pulm Med. 2020;20:253. doi:10.1186/s12890-020-01296-3
16. Humenberger M, Horner A, Labek A, et al. Adherence to inhaled therapy and its impact on chronic obstructive pulmonary disease (COPD). BMC Pulm Med. 2018;18:163. doi:10.1186/s12890-018-0724-3
17. Braido F, Chrystyn H, Baiardini I, et al. “Trying, but failing”—the role of inhaler technique and mode of delivery in respiratory medication adherence. J Allergy Clin Immunol Pract. 2016;4:823–832.
18. Minakata Y, Azuma Y, Sasaki S, Murakami Y. Objective measurement of physical activity and sedentary behavior in patients with chronic obstructive pulmonary disease: points to keep in mind during evaluations. J Clin Med. 2023;12. doi:10.3390/jcm12093254.
19. Liu Y-R, Wang Y, Peng X, Xie H. The impact of illness perception on medication adherence to inhaler therapy in elderly individuals with COPD. Resp Care. 2025;70:65–73. doi:10.1089/respcare.12056
20. Pattock AM, Locke ER, Hebert PL, et al. Predictors of patient-reported and pharmacy refill measures of maintenance inhaler adherence in veterans with chronic obstructive pulmonary disease. Ann Am Thoracic Soc. 2024;21(3):384–392. doi:10.1513/AnnalsATS.202211-975OC
21. Liu Y-R, Wang Y, Liu J, Xie H. Path analysis of illness perception, medication beliefs, family support on inhaler adherence in elderly COPD patients: based on triadic reciprocal determinism. Patient Educ Couns. 2025;130:108465. doi:10.1016/j.pec.2024.108465
22. Wallin M, Tagami T, Chen L, Yang M, Chan H-K. Pulmonary drug delivery to older people. Adv Drug Delivery Rev. 2018;135:50–61. doi:10.1016/j.addr.2017.11.010
23. O’Toole J, Krishnan M, Riekert K, Eakin MN. Understanding barriers to and strategies for medication adherence in COPD: a qualitative study. BMC Pulm Med. 2022;22:98. doi:10.1186/s12890-022-01892-5
24. Ma J, Sun X, Wang X, Liu B, Shi K. Factors affecting patient adherence to inhalation therapy: an application of SEIPS model 2.0. Patient Prefer Adherence. 2023;17:531–545. doi:10.2147/ppa.S395327
25. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19:349–357. doi:10.1093/intqhc/mzm042
26. Boddy CR. Sample size for qualitative research. Qual Market Res. 2016;19:426–432. doi:10.1108/QMR-06-2016-0053
27. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107–115. doi:10.1111/j.1365-2648.2007.04569.x
28. Schreiber J, Sonnenburg T, Luecke E. Inhaler devices in asthma and COPD patients–a prospective cross-sectional study on inhaler preferences and error rates. BMC Pulm Med. 2020;20:1–12.
29. Hodder R, Price D. Patient preferences for inhaler devices in chronic obstructive pulmonary disease: experience with Respimat® Soft Mist™ Inhaler. Int J Chronic Obstr. 2009;381–390. doi:10.2147/COPD.S3391
30. Chrystyn H, Small M, Milligan G, et al. Impact of patients’ satisfaction with their inhalers on treatment compliance and health status in COPD. Respir Med. 2014;108:358–365. doi:10.1016/j.rmed.2013.09.021
31. Jang JG, Lee KH, Chung JH, et al. Assessment of inhaler satisfaction and determinants of high satisfaction among Korean COPD patients. J Korean Med Sci. 2022;37:1.
32. Duarte-de-araújo A, Teixeira P, Hespanhol V, Correia-de-sousa J. COPD: misuse of inhaler devices in clinical practice. Int J Chron Obstruct Pulmon Dis. 2019;14:1209–1217. doi:10.2147/copd.S178040
33. Alyafei A, Easton-Carr R. StatPearls. StatPearls Publishing; 2024.
34. Orji R, Vassileva J, Mandryk R. Towards an effective health interventions design: an extension of the health belief model. Online J Public Health Info. 2012;4:e61050. doi:10.5210/ojphi.v4i3.4321
35. Liu Y-R, Wang Y, Wang J, Wang X. Association between illness perception and adherence to inhaler therapy in elderly Chinese patients with chronic obstructive pulmonary disease. Chron Respir Dis. 2024;21:14799731241286837. doi:10.1177/14799731241286837
36. Skerry L, Kervin E, Freeze TA, et al. “It’s a lonely battle”: a qualitative study of older adult Canadians’ experiences with chronic obstructive pulmonary disease medication adherence and support. Can Pharm J. 2023;156:32–41. doi:10.1177/17151635221140412
37. Pal A, Howarth TP, Rissel C, et al. COPD disease knowledge, self-awareness and reasons for hospital presentations among a predominately Indigenous Australian cohort: a study to explore preventable hospitalisation. BMJ Open Respir Res. 2022;9. doi:10.1136/bmjresp-2022-001295
38. Al Bshabshe A, Al Shuqayfah N, Alahmari F, et al. Awareness of chronic obstructive pulmonary disease (COPD) among the general population in Aseer Region, Kingdom of Saudi Arabia (KSA). J Family Med Prim Care. 2023;12(6):1209–1213. doi:10.4103/jfmpc.jfmpc_2462_22
39. Huang L-M, Tan C-Y, Chen X, et al. A qualitative study on illness perception and coping behaviors among patients with chronic obstructive pulmonary disease: implications for intervention. Int J Chronic Obstr. 2024;Volume 19:2467–2479. doi:10.2147/COPD.S473790
40. Odhiambo LA, Stephens PC, Cheruvu VK, Zullo MD. Enhancing disease and management knowledge among Black Americans with asthma or chronic obstructive pulmonary disease (COPD). Am J Health Promot. 2025;39:654–657. doi:10.1177/08901171241307432
41. Adida F, Pandia P, Pradana A, et al. Effectiveness of smartphone application in increasing knowledge on COPD and its non-pharmacological management in COPD patients. Narra J. 2023;3(3):e412. doi:10.52225/narra.v3i3.412
42. Xu H, Jiang X, Zeng Q, Li R. Application of e-Health tools in the assessment of inhalation therapy adherence in patients with chronic obstructive pulmonary disease: scoping review coupled with bibliometric analysis. Respir Med. 2025;236:107898. doi:10.1016/j.rmed.2024.107898
43. Renaud Y, Suter P, Grandmaison G. Patient characteristics to consider when selecting an inhaler for the treatment of chronic obstructive pulmonary disease and available assessment methods: a narrative review. Respiration. 2023;102:416–425. doi:10.1159/000530277
44. Poletti V, Pagnini F, Banfi P, Volpato E. Illness perceptions, cognitions, and beliefs on COPD patients’ adherence to treatment - a systematic review. Patient Prefer Adherence. 2023;17:1845–1866. doi:10.2147/ppa.S412136
45. Pendoni R, Albanesi B, Clari M, Pecorari G, Matarese M. Contributing to self‐care of a person with chronic obstructive pulmonary disease: a qualitative study of the experiences of family caregivers. J Adv Nurs. 2024;80:1927–1942. doi:10.1111/jan.15939
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Affecting Patient Adherence to Inhalation Therapy: An Application of SEIPS Model 2.0
Ma J, Sun X, Wang X, Liu B, Shi K
Patient Preference and Adherence 2023, 17:531-545
Published Date: 3 March 2023
Impact of Medication Adherence on Emergency Department Visits in Patients with COPD in a Single Tertiary Hospital in Saudi Arabia
Alshehri S, Alshibani M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:593-598
Published Date: 17 April 2023
The Intention of Inhaled Medication Adherence Scale (IMAS): The Development of a New Instrument for Assessing Inhaled Medication Adherence Among Patients with Chronic Obstructive Pulmonary Disease (COPD) Using Theory of Planned Behavior
Wang YH, Yang TM, Hung MS, Lin YC, Fang TP, Kuo TT, Griffiths MD, Lin CY
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1655-1664
Published Date: 2 August 2023
Effects of Adherence to an mHealth Tool for Self-Management of COPD Exacerbations
Bischoff EW, Ariens N, Boer L, Vercoulen J, Akkermans RP, van den Bemt L, Schermer TR
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2381-2389
Published Date: 1 November 2023
Mucolytic Therapy in COPD: Patient Usage and Preferences in Real-World Italian Settings
D’Antonio S, Pennisi A, Cazzola M
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:479-486
Published Date: 1 March 2025