")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Impact of Medication Adherence on Emergency Department Visits in Patients with COPD in a Single Tertiary Hospital in Saudi Arabia
Authors Alshehri S, Alshibani M
Received 13 November 2022
Accepted for publication 27 March 2023
Published 17 April 2023 Volume 2023:18 Pages 593—598
DOI https://doi.org/10.2147/COPD.S392946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Samah Alshehri, Mohannad Alshibani
Department of Pharmacy Practice, Faculty of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Samah Alshehri, Department of Pharmacy Practice, King Abdulaziz University, P.O. Box 80200, Jeddah, 21589, Saudi Arabia, Tel +966564362332, Fax +12 9666400000. Ext. 20675, Email [email protected]
Introduction: There is a very limited information and studies on the impact of adherence to chronic obstructive pulmonary disease (COPD) medications in Saudi Arabia. We hypothesized that the adherence to COPD medication in our tertiary hospital is poor and can lead to frequent ED visits and longer hospitalization stays. The purpose of this study was to assess the impact of medication adherence in patients with COPD on emergency department (ED) visits and hospitalization.
Methods: A single-center retrospective observational study included patients with a COPD exacerbation, who were admitted to a tertiary teaching hospital in Jeddah, Saudi Arabia from October 2017 to November 2020. The primary outcome was the rate of emergency department (ED) visit in one year. Secondary outcomes were hospitalization after ED visit and total hospital length of stay. Medication adherence was evaluated by using Fixed Medication Possession Ratio (FMPR). Patients with score of ≥ 0.80 were classified as high-adherent groups while patients with ratio < 0.80 were on low-adherent groups.
Results: A total of 266 patients enrolled in the study. Of those 266 patients, 139 patients were on high-adherent group and 127 were on low-adherent group. There was a significant difference between the high-adherent group and low-adherent group in the incidence of ED visit in one year 62 (44.6%) vs 73 (57.5%); P < 0.036, and hospitalization after the ED visit 26 (18.7%) vs 42 (33.1%); P = 0.007. However, there was no significant difference between the two groups in the total hospital length of stay.
Conclusion: Among patients with COPD, there was a significant increase in ED visit per one year that leads to more hospitalization among patients with low adherence compared to patients with high adherence. This study highlights the importance of improving the medication adherence in patients with COPD.
Keywords: COPD, adherence, ED visit, inhaler
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is one of the most common chronic respiratory diseases in the world, affecting millions of people. It is the fourth leading cause of death in the world.1 It was predicted to be the third leading cause of mortality by the year 2020. As exposure to COPD predisposing factors and the aging of the population are predicted to increase in the coming decades, COPD burdens will rise.2
Treatment adherence is defined as the extent of the patient’s response to the use of medications. As a chronic disease, medication adherence in patients with COPD is one of the most important factors for achieving successful symptoms management.3 Many factors can play an important role in treatment adherence such as smoking, missing doses, side effects and improper use of inhaler devices.4 All of these factors can affect the success of treatment in patients with COPD.4
Few studies have evaluated the impact of medication adherence in patients with COPD despite the high mortality and complications reported in some published studies.5 One previous study evaluating COPD medication adherence found that adherence is poor in Turkey and Saudi Arabia and that non-adherence is associated with a reduced quality of life.6
The adherence of the general COPD population to maintenance therapy was examined in Denmark. This study found an association between adherence and the severity of COPD as defined by GOLD Criteria.7 Another study conducted in Egypt examined the adherence of asthma and COPD medication and found that most enrolled patients were non-adherent to their therapies.8
The objective of this study is to assess adherence to COPD medications and how that may affect the rate of ED visits each year. There are few studies and very limited information and on the impact of adherence to COPD medications in Saudi Arabia. We hypothesize that the adherence to COPD medication in our tertiary hospitals is poor and can lead to frequent ED visits and longer hospitalization stays.
Method
Study Design
This is a retrospective observational study which included patients with a diagnosis of COPD from the period of October 2017 to November 2020 in a tertiary teaching hospital in Jeddah, Saudi Arabia. The study was approved by the hospital Biomedical Ethics Research Committee.
Selection of Participants
In this study, we included all patients who were 40 years of age or older who got admitted to the hospital secondary to COPD exacerbation and had a history of COPD using ICD-10 codes. We excluded patients with a history of asthma or any other chronic respiratory disease and those who were deceased before we conducted the study.
Screening
A sample size of 363 COPD patients were primarily screened for inclusion in our study. Of those 363 patients, 266 met the inclusion criteria, while 76 were deceased before the study was conducted, and 21 had asthma.
Data Collection
We collected the following information for participants in this study: demographic data, rate of emergency visits in one year, rate hospitalization in one year, length of hospital stay after first hospitalization, patients on oxygen therapy, smoking status. The medications for COPD patients were obtained from the KAUH electronic database including inhaled corticosteroids (ICS), short acting muscarinic receptors agonists (SAMA), long-acting muscarinic receptors agonists (LAMA), short-acting beta 2 agonists (SABA), and long-acting beta 2 agonists (LABA). We use these medications because they are commonly used in COPD patients according to COPD guidelines.9 We included the daily scheduled medications rather than the medication prescribed as needed agents.
Medication Adherence
We calculated medication adherence using the fixed Medication Possession Ratio (FMPR) for each class of COPD medication received. We computed FMPR by dividing the total days of medication supplied by the total number of days of therapy (6 months). We calculate the FMPR based on the 6 months observation period by summing all the scheduled COPD inhalers supply for 6 months post the first admission date. The numerator was calculated by total days’ supply of all COPD schedule medications in 6 months indexed. We calculated the adherence by determining how many inhalers were prescribed and received from the pharmacy, set a daily score weighted by the number of medications to be taken each day, the sum of the scores from the 6 months period were divide by 6 months as denominator. We defined the proportion of patients having achieved a high adherence medication supply as an FMPR of 0.8 or more.
The primary outcome was to calculate the incidence of ED visits in one year among patients with COPD. Our secondary outcomes were to identify the total hospital length of stay and hospitalization after the ED visit.
Statistical Analysis
Sample Size Calculation
We used a χ2 analysis to compare the demographic characteristics between the two groups unless the sample size for a case was less than 5, and in those cases, we used a Fisher exact test. Normally distributed continuous variables were analyzed using an unpaired t-test. A P value of less than 0.05 for any of the variables was considered statistically significant.
Results
There was no difference between the two groups in the baseline characteristics. See Table 1. A total of 139 patients were in the high adherence group, while 127 were in the low adherence group. The mean age in our study was 67.32 (±11.8) years in patients with high adherence and 67.5 (±12.5) years in patients with low adherence. There was no difference between the two groups in gender. There was also no difference between the high adherence groups and low adherence groups in the percentage of smokers (75.5% vs 78.0%; P = 0.642), respectively.
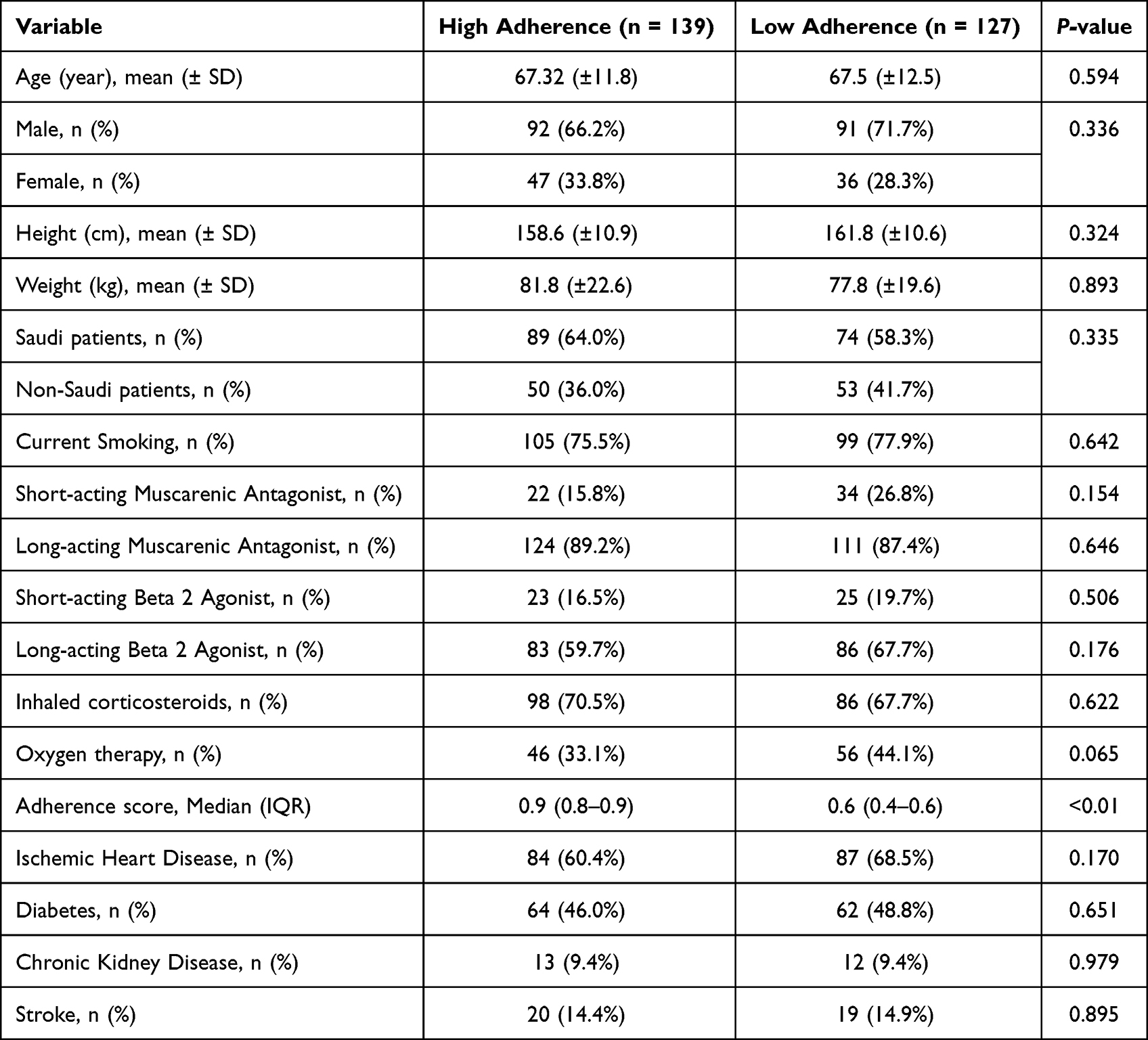 |
Table 1 Baseline Characteristics |
Regarding COPD medications, there was no significant difference between the two groups on the following most prescribed medications for COPD: SAMA, LAMA, SABA, LABA, and ICS. In addition, there was no difference between patients on oxygen therapy with high adherence (46 [33.1%]) and low adherence (56 [44.1%]).
Outcomes
The primary outcome showed that high-adherent groups had significantly low rate of ED visits in one year compared to low-adherent groups (62 [44.6%] vs 73 [57.5%]; P < 0.036).
In the secondary outcomes, the high-adherent groups had significantly lower rates of hospitalization after the ED visit (26 [18.7%] vs 42 [33.1%]; P = 0.007). On the other hand, for those patients who got hospitalized, there was no significant difference in the total hospital length of stay between the two groups (5 [3–11] vs 6 [4–9] days); P = 0.107 in high-adherent and low adherent groups, respectively (see Table 2).
 |
Table 2 Clinical Outcomes |
Discussion
To the best of our knowledge, this is the first study examining the number of ED visits related to COPD medication adherence in Saudi Arabia. We found that there was a significant difference in patients with high adherence in multiple parameters compared to patients with low adherence. The high number of ED visits per year in our study indicates the necessity to improve medication adherence for such a high-risk disease. The association between low adherence and frequent ED visits could be due to several factors such as worsening disease progression and COPD symptoms, decrease in the quality of life, increase in the number of exacerbations, and smoking. All these factors could play an essential role in improving the adherence rate and therefore reducing the complications associated with the disease.
The length of stay was less than what was previously reported in a survey in the same hospital, in which they found that the mean length of hospital stay from respiratory disease was 8.9 ± 6.3. This difference might be since respiratory disease consisted of COPD and bronchial asthma. It might also be due to the improvement of care provided to the patients in our institution.10 Moreover, our study showed no difference between groups regarding the total length of hospital stay. This might be due to the small sample size enrolled in our study. Another explanation is the long process and difficulty of finding a suitable home healthcare for discharged patients due to several complicated policies and cultural beliefs.11
Adherence to COPD medications is known to be very poor around the world including the Middle East.6–8,12 The results of our study confirm what was previously known regarding the poor adherence rates in the COPD population. Low adherence to COPD medications in prior research that measured adherence using medication possession ratios reported that 21–47% of those taking COPD medications had an average adherence of 0.8 or more.7,13,14 In our study, 52.3% of patients achieved an average adherence of 0.80 or more. Another study that examined the adherence to individual classes of COPD medication found that 54% of patients were adherent to LABA therapy while only 40% were adherent to ICS.15
This very low adherence may be because some of the patients did not want to take inhaler therapy for their COPD because of the risk of drug dependence. Another reason was the cost issue for taking some of the COPD inhalers. On the other hand, it should be noted that most patients in our hospital received COPD medications for free because it is a government hospital, and most of the eligible patients received their therapies and other services at no cost, following government policy. According to the published literature, the perception of clinician expertise in lung disease was a main factor associated with higher adherence.15 Additionally, analysis of data from the BREATHE trial suggested that the awareness of COPD disease and expectations for treatment were minimal. This finding highlighted the importance of education and effective communications between clinician and COPD patients.16 The collaborative efforts of healthcare providers regarding the disease and its treatment options are important to improving medication adherence, which may subsequently improve the clinical and economic outcomes of COPD.17
Regarding ED visits and subsequent hospitalization, our finding was supported by previous work which found that levels of adherence to COPD maintenance medications were associated with decreased risk of ED visits (hazard ratio [HR] 0.79; 95% CI 0.74, 0.83) and hospitalizations (HR 0.82; 95% CI 0.78, 0.87).18 Another study found that patients with FMPR of ≥0.80 for COPD maintenance therapy had fewer hospitalizations in comparison to patients with Medication Possession Ratios of <0.80 (RR = 0.90).13 This finding confirms the economic and clinical importance of COPD medication adherence. Moreover, another work found that the hospital admission rate secondary to COPD exacerbation were 15% and 27% in high and low adherence groups, respectively (RR 0.58 [95% CI 0.44 to 0.73, P < 0.001]). The association between adherence and hospital admission was independent of study treatment.19
Some limitations in our study should be mentioned. First, low number of patients were enrolled in our study. Second, it should be noted that this is a single-center study in a tertiary teaching hospital in Saudi Arabia, so we cannot generalize our results to other populations. Third, we could not find any information regarding pulmonary function tests, such as forced expiratory volume (FEV) and forced vital capacity (FVC) because they were not recorded in the hospital system. Moreover, since we included patient who got admitted with COPD exacerbation, many of the patients would have relatively severe COPD and data cannot be generalized to all COPD patients. Additionally, we did not assess factors influence adherence in COPD patients. Lastly, adherence was calculated by pooling the data for all COPD maintenance therapies not by the individual class of medications.
In conclusion, there was a significant increase in ED visits per year among low-adherent patients compared to high-adherent patients. This study highlights the necessity of improving medication adherence in patients with COPD in Saudi Arabia.
Data Sharing Statement
All data were retrieved from the databases and are available from the corresponding author on a reasonable request.
Ethical Approval
The Institutional Review Board at King Abdulaziz University approved the study (IRB number 660-18) before any data were collected. Participants’ consent for this study was waived because no individuals were identified. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgment
The abstract for this paper was presented at 2019 ACCP Annual Meeting, Poster number 6 available at (https://accpjournals.onlinelibrary.wiley.com/doi/full/10.1002/jac5.1204).
Funding
This project was funded by the Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah, Saudi Arabia, under Grant No. G-150-249-1442. The authors, therefore, acknowledge with thanks DSR for technical and financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
2. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
3. Tabor PA, Lopez DA. Comply with us: improving medication adherence. J Pharm Pract. 2004;17:167–181. doi:10.1177/0897190004264816
4. Osterberg L, Blaschke T. Drug therapy: adherence to medication. N Engl J Med. 2005;353:487–497. doi:10.1056/NEJMra050100
5. Van Boven JF, Chavannes NH, Van Der Molen T, et al. Clinical and economic impact of non-adherence in COPD: a systemic review. Respir Med. 2014;108(1):103–113. doi:10.1016/j.rmed.2013.08.044
6. Kokturk N, Polatli M, Oguzulgen IK, et al. Adherence to COPD treatment in Turkey and Saudi Arabia: results of the ADCARE study. Int J COPD. 2018;13:1377–1388. doi:10.2147/COPD.S150411
7. Ingebrigtsen TS, Marott JL, Nordestgaard BG, et al. Low use and adherence to maintenance medication in chronic obstructive pulmonary disease in the general population. J Gen Intern Med. 2015;30(1):51–59. doi:10.1007/s11606-014-3029-0
8. Galal I, Mohammad Y, Nada A, Mohran Y. Medication adherence and treatment satisfaction in some Egyptian patients with chronic obstructive pulmonary disease and bronchial asthma. Egyptian Journal of Broncholog. 2018;12:1.
9. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease; 2018. Available from: www.goldcopd.org.
10. Alamoudi O, Attar S, Ghabrah T, Al-Qassimi M. Pattern of common diseases in hospitalized patients at an university hospital in Saudi Arabia; A Study of 5594 Patients. JKAU Med Sci. 2009;16(4):3–12.
11. Al Shammari S. Determinants of the length of patient stay in hospital in Saudi Arabia. Saudi Med J. 1996;17(6):709–717.
12. Krauskopf K, Federman AD, Kale MS, et al. Chronic obstructive pulmonary disease illness and medication beliefs are associated with medication adherence. COPD. 2015;12(2):151–164. doi:10.3109/15412555.2014.922067
13. Simoni-Wastila L, Wei Y-J, Qian J, et al. Association of chronic obstructive pulmonary disease maintenance medication adherence with all-cause hos- pitalization and spending in a Medicare population. Am J Geriatr Pharmac. 2012;10(3):201e210.
14. Toy EL, Beaulieu NU, McHale JM, et al. Treatment of COPD: relationships between daily dosing frequency, adherence, resource use, and costs. Respir Med. 2011;105(3):435e441.
15. Cecere LM, Slatore CG, Uman JE, et al. Adherence to long-acting inhaled therapies among patients with chronic obstructive pulmonary disease (COPD). COPD J Chronic Obstr Pulm Dis. 2012;9(3):251e258.
16. Sayiner A, Alzaabi A, Obeidat NM, et al. Attitudes and beliefs about COPD: data from the BREATHE study. Respir Med. 2012;106(Suppl 2):S60–S74. doi:10.1016/S0954-6111(12)70015-X
17. Restrepo RD, Alvarez MT, Wittnebel LD, et al. Medication adherence issues in patients treated for COPD. Int J Chron Obstruct Pulmon Dis. 2008;3(3):371e384. doi:10.2147/COPD.S3036
18. Albrecht JS, Khokhar B, Huang TY, et al. Adherence and healthcare utilization among older adults with COPD and depression. Respir Med. 2017;129:53–58. PMID: 28732836; PMCID: PMC5607946. doi:10.1016/j.rmed.2017.06.002
19. Vestbo J, Anderson JA, Calverley PM, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.