Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
The Intention of Inhaled Medication Adherence Scale (IMAS): The Development of a New Instrument for Assessing Inhaled Medication Adherence Among Patients with Chronic Obstructive Pulmonary Disease (COPD) Using Theory of Planned Behavior
Authors Wang YH, Yang TM, Hung MS ![]() , Lin YC
, Lin YC ![]() , Fang TP, Kuo TT, Griffiths MD
, Fang TP, Kuo TT, Griffiths MD ![]() , Lin CY
, Lin CY ![]()
Received 4 May 2023
Accepted for publication 24 July 2023
Published 2 August 2023 Volume 2023:18 Pages 1655—1664
DOI https://doi.org/10.2147/COPD.S420001
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Yin-Han Wang,1 Tsung-Ming Yang,2,3 Ming-Szu Hung,2– 4 Yu-Ching Lin,2– 4 Tien-Pei Fang,1,3 Tzu-Tzu Kuo,5,* Mark D Griffiths,6 Chung-Ying Lin7– 10,*
1Department of Respiratory Therapy, Chang Gung Memorial Hospital, Chiayi, Taiwan; 2Department of Pulmonary and Critical Care Medicine, Chang Gung Memorial Hospital, Chiayi Branch, Chiayi, Taiwan; 3Department of Respiratory Care, Chang Gung University of Science and Technology, Chiayi, Taiwan; 4Department of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan; 5Division of Respiratory Medicine, Department of Internal Medicine, E-Da Hospital, I-Shou University, Kaohsiung City, Taiwan; 6International Gaming Research Unit, Psychology Department, Nottingham Trent University, Nottingham, UK; 7Institute of Allied Health Sciences, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 8Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 9Biostatistics Consulting Center, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 10Department of Occupational Therapy, College of Medicine, National Cheng Kung University, Tainan, Taiwan
*These authors contributed equally to this work
Correspondence: Chung-Ying Lin, Institute of Allied Health Sciences, College of Medicine, National Cheng Kung University, Tainan, Taiwan, Tel +886-6-2353535 ext. 5106, Fax +886-6-2367981, Email [email protected] Tzu-Tzu Kuo, Division of Respiratory Medicine, Department of Internal Medicine, E-Da Hospital, I-Shou University, Kaohsiung City, Taiwan, Email [email protected]
Purpose: Inhaled medication adherence is an important issue for patients with chronic obstructive pulmonary disease (COPD) because adhering to inhaled medications could substantially improve their health. However, patients with COPD may not be always adhere to the prescribed inhaled medications. Therefore, understanding the underlying reasons for patients with COPD adhering to inhaled medications is important. The present study used Theory of Planned Behavior (TPB) as a theoretical framework to develop the Intention of Inhaled Medication Adherence Scale (IMAS) and assess its psychometric properties.
Patients and Methods: After reviewing papers using the TPB to design psychometric scales and the TPB scale development guidelines, 28 items were generated for expert evaluation. Eight experts reported that the 28 items all had good content validity (content validity index ranged from 0.88 to 1.00 at item-level; and from 0.981 to 0.987 at scale-level) comprising four factors. Following initial development, 235 patients with COPD (mean age 73.12 years; 93.6% males) completed the IMAS via interview with a respiratory therapist and a research assistant. The four-factor structure of the IMAS was evaluated using confirmatory factor analysis (CFA).
Results: Nine IMAS items were removed because of low factor loadings or offending estimates. The 19-item IMAS was confirmed as having a four-factor structure supported by the CFA results (comparative fit index=1.00; Tucker-Lewis index=1.00; root mean square error of approximation=0.00; standardized root mean square residual=0.06).
Conclusion: The 19-item IMAS had satisfactory psychometric properties in construct validity. The 19-item IMAS is an instrument that could help healthcare providers understand potential factors associated with adherence to inhaled medications among people with COPD.
Keywords: adherence, confirmatory factor analysis, COPD, psychometrics
Plain Language Summary
Using a psychological theoretical framework may provide helpful information for healthcare providers to develop programs to improve inhaled medication adherence among patients with chronic obstructive pulmonary disease (COPD). One of the key psychology theories in explaining human health behaviors (eg, medication adherence) is the theory of planned behavior (TPB). The TPB includes four main concepts comprising attitude (how an individual appraises and likes a behavior), subjective norm (how the environment of an individual values a behavior), perceived behavioral control (how confident an individual is in performing a behavior), and intention (whether an individual is willing to perform a behavior). However, it is not known if the TPB can be an effective framework to assess the behavior of inhaled medication adherence. Therefore, the present study designed a TPB-guided scale (the Intention of Inhaled Medication Adherence Scale; IMAS) and tested its psychometric properties. Eight experts evaluated the IMAS (28 items) and concluded that it had satisfactory content validity. Following scale development, 235 patients (220 males) with COPD (mean age=73.12 years) completed the IMAS. Confirmatory factor analysis (CFA) indicated that nine IMAS items should be deleted. The retained 19 IMAS items were again examined using CFA and had satisfactory properties. Other psychometric testing (including internal consistency, concurrent validity, and divergent validity) all supported the psychometric adequacy of the 19-item IMAS. Consequently, the IMAS can be used as an instrument help assess inhaled medication adherence among patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD), a degenerative disease, can cause severe health consequences (eg, mortality) and high levels of health burden for patients (eg, having difficulties engaging in daily activities because of breathlessness, chronic coughing, and tiredness).1–4 Additionally, the novel coronavirus disease 2019 (COVID-19) pandemic exacerbated health problems among patients with COPD, as evidenced by the increased mortality rates.5 However, patients with COPD could have good health outcomes if they adhere to inhaled medication use.6,7 More specifically, COPD symptoms (ie, breathlessness, chronic coughing, and tiredness) can be controlled and eased when patients with COPD regularly use inhaled medications according to the prescribed instructions, especially in early treatment.6–8 In contrast, patients with COPD who have poor medication adherence have been found to have ten-fold higher risk of hospitalization compared with those who have good medication adherence.9 Consequently, understanding psychological factors explaining inhaled medication adherence among patients with COPD appears to be an important issue for healthcare providers.
In order to effectively assess the psychological factors explaining inhaled medication adherence, the use of a theoretical framework is recommended.10,11 A good theoretical framework provides a fundamental basis for healthcare providers and researchers to identify the associations between studied concepts and constructs in a coherent and logical way.12 Subsequently, researchers and healthcare providers can quickly identify important psychological factors associated with successful outcomes, and then design appropriate programs to improve health behaviors for the target population (eg, inhaled medication adherence among patients with COPD in the present study). Among the best theories in explaining human health behaviors is the Theory of Planned Behavior (TPB) which is one of the most used theories with wide applications across different health behaviors, including medication adherence.13–19 However, to the best of the present authors’ knowledge, no previous studies have used the TPB to better understand inhaled medication adherence among patients with COPD. Therefore, the present study used the TPB as the theoretical framework to develop a psychometric scale assessing psychological factors explaining inhaled medication adherence among this population.
The TPB proposed by Icek Ajzen20 was an extension from the Theory of Reasoned Action.21,22 There are four primary elements (or factors) in the TPB, comprising attitude, subjective norm, perceived behavioral control, and intention which cover most of the important psychological factors explaining human behaviors.20 Attitude indicates how an individual appraises a behavior (eg, inhaled medication adherence in the present study) and whether the individual likes the behavior.20 Based on attitude, researchers can identify how an individual values or enjoys the behavior. Subjective norm indicates how an individual perceives the individuals they interact with (eg, friends, family members, acquaintances) think about the behavior.20 According to subjective norm, researchers can identify if the environment the individual lives in supports them to engage in the behavior. Perceived behavioral control indicates how confident an individual is in performing the behavior.20 Based on perceived behavioral control, researchers can identify if the individual has good self-efficacy in behavior engagement. Intention indicates how an individual intends to perform the behavior.20 Based on intention, researchers can identify if the individual is willing to perform the behavior.20
From the definitions and explanations of the four TPB elements, it can be clearly understood that the four TPB elements could be important factors in explaining inhaled medication adherence among patients with COPD. However, as aforementioned, there is a lack of psychometric instruments assessing the TPB factors in understanding inhaled medication adherence among patients with COPD. Therefore, the purpose of the present study was to develop an instrument assessing potential underlying factors associated with inhaled medication adherence among patients with COPD. Using the TPB, the instrument (ie, the Intention of Inhaled Medication Adherence Scale; IMAS) was designed taking into consideration the elements of attitude, subjective norm, perceived behavioral control, and intention. Psychometric testing was performed to examine the psychometric properties of the IMAS in terms of its reliability and validity.
Materials and Methods
Patient Participants and Data Collection
The present study was approved by the Institutional Review Board of Chang Gung Medical Foundation (approval no. 202101706B0C601) and adhered to the Declaration of Helsinki regarding the study’s procedure. Eligible participants were approached by a respiratory therapist having eight years of clinical experience to explain the present study’s purpose, procedure, and participation rights. If eligible participants agreed to participate in the study, they were asked to provide written informed consent to indicate their participation willingness. Then, they were interviewed by the respiratory therapist to complete the IMAS using Chinese content. The eligibility of the participants was identified by the respiratory therapist with the use of the following inclusion criteria. Individuals (i) had been prescribed to use at least one inhaled medication daily; (ii) had a diagnosis of COPD (based on post-bronchodilator FEV1/FVC < 70%) (ICD-10: J44-J49); and (iii) were aged 40 years or older. The exclusion criteria were that individuals (i) had refused to participate; (ii) had cognitive problems as observed by the respiratory therapist; and (iii) did not provide written informed consent. After inviting 250 participants, 235 agreed to participate (94.0% response rate). The severity of the COPD was not found to be a factor associated with the individuals’ willingness to participate. However, all participants were outpatients of a regional teaching hospital at Chiayi (a Southwestern Taiwan region). Therefore, the severity of the studied population in the present study was relatively mild (over 85% of the patients with COPD in the outpatient clinics were Groups A or B in regards to severity level). The participants’ characteristics are reported in Table 1. In brief, the participants’ mean age was 73.12 years (SD=16.7) and over 90% of them were males (n=220; 93.6%). On average, the participants had a COPD diagnosis for 4.40 years (SD=2.66).
 |
Table 1 Patient Demographics (N=235) |
Development of the Intention of Inhaled Medication Adherence Scale (IMAS)
According to the guidelines of the TPB developer (ie, Prof. Icek Ajzen)20,23 and previous studies using the TPB to design scales,13–18 the first author (an experienced respiratory therapist) worked with the last author (an expert with extensive experience in TPB research) and created 25 initial items (13 for attitude; four for subjective norm; six for perceived behavioral control; and two for intention). Then, the 25 items together with the TPB definitions were sent to eight experts (in the fields of nursing, public health, behavioral sciences, and respiratory medicine) to evaluate. One item for perceived behavioral control was deleted because it substantially overlapped the concept of another item. However, one item for perceived behavioral control was added based on the experts’ suggestion. The experts additionally suggested adding three items for intention. Therefore, 28 items reflecting the four TPB elements (see Appendix 1 for Chinese content and Appendix 2 for translated English content) were finalized for the psychometric testing (please see ‘Statistical Analysis’ section for details). For the 28-item IMAS, 13 items were designed for attitude; four items for subjective norm; six items for perceived behavioral control; and five items for intention. All the items are rated using a five-point Likert scale: 1 (completely disagree), 2 (disagree), 3 (neutral), 4 (agree), and 5 (completely agree).
After the 28 items were generated, eight experts (including experts in respiratory therapy, chest medicine, pharmacy, psychometrics) were invited to review the items to evaluate their relevance and clarity. The experts were instructed to score every item using a four-point Likert scale (1=strongly inappropriate; 2=inappropriate; 3=appropriate; and 4=strongly appropriate) to evaluate the content validity index of the IMAS (for detailed information regarding content validity index please see ‘Statistical Analysis’ section). In addition, several patients with COPD were interviewed to examine if the IMAS items could be understood by the target population.
Demographics and Clinical Characteristics Measures
The respiratory therapist collected the demographic information including age (in years), sex (male or female), smoking history (non-smoker, active smoker, or ex-smoker), family support information (solitary or caregiver), education (uneducated, elementary school, junior high school, high school, or college or above), and comorbidities (the patient verbally self-reported all the comorbid health conditions they had). The respiratory therapist additionally assessed the participants’ (i) COPD symptoms to group them into low-risk and high-risk groups, and (ii) Global Initiative for Chronic Obstructive Lung Disease (GOLD) rating to group them into mild, moderate, severe, and very severe disease severity.
Statistical Analysis
The IMAS was firstly analyzed using content validity index to examine the 28 items and the entire instrument. For each IMAS item, item content validity index was calculated for its relevance and clarity. Then, the scale content validity index was calculated using the average of the 28 item content validity indices. The content validity index was expected to be higher than 0.78 when there were six to ten experts involved in the content validity index calculation,24 and when an item had either a relevance or clarity content validity index lower than 0.78, it was deleted. Following this, descriptive statistics (including means, SDs, skewness, and kurtosis) of the IMAS items were analyzed.
A four-factor structure model was then applied to examine if the IMAS items that have content validity index larger than 0.78 fitted well with the TPB framework. More specifically, the four factors were attitude (ATT), subjective norm (SN), perceived behavioral control (PBC), and intention (IT), which correspond to the four elements in the TPB.20 Since the factor structure has a theoretical background, confirmatory factor analysis (CFA) rather than exploratory factor analysis was used to examine the IMAS structure. In the CFA, the following fit indices were used to examine if the four-factor structure fitted well with the data comprising a nonsignificant χ2, a comparative fit index (CFI)>0.9, a Tucker-Lewis index (TLI)>0.9, a root mean square error of approximation (RMSEA) <0.08, and a standardized root mean square residual (SRMR) <0.08.25,26 In addition, all the IMAS items were checked for their appropriateness in the four-factor structure with the use of their factor loading. When an IMAS item had a factor loading less than 0.5 (indicating somewhat irrelevant to its embedded construct) or larger than 0.95 (indicating offending estimates),27,28 the item was removed. After removing unsuitable items (either low loading or offending estimates), the aforementioned fit indices were used again to examine the data-model fit.
The IMAS (or the shortened IMAS if some items were deleted in the previous procedure) was then examined for its domain internal consistency, composite reliability (CR), and average variance extracted (AVE) to examine if the IMAS domains have good convergent validity. The recommended cutoffs were >0.7 for the internal consistency (using Cronbach’s α),29,30 >0.6 for CR, and >0.5 for AVE.31,32 Lastly, the IMAS was examined for its divergent validity using the comparisons between square root of AVE and the correlations between the constructs (ie, the Fornell-Larcker criterion matrix).31 When square root of the AVE for a specific domain (eg, AT) is larger than the correlations between the specific domain and other domains (ie, AT with SN, AT with PBC, and AT with IT when the specific domain is AT), divergent validity is supported.31 The statistical analyses were conducted using R software with relevant packages, including lavaan and psych.33,34
Results
The content validity of the IMAS was satisfactory given that the scale content validity index was 0.981 for relevance and 0.987 for clarity. Regarding the item content validity, all items had a value of 1, except for three items (PBC Items 1 and 2 for their relevance and clarity; IT Item 2 for its relevance) having the value of 0.88. Therefore, all IMAS items were used for the following analyses.
After ensuring all items were relevant and appropriate, item properties of the IMAS were checked and are reported in Table 2. All the IMAS items had skewness values ranging between −2.66 and 1.51, and kurtosis values ranging between −1.27 and 8.75. The CFA results showed that the initial 28-item IMAS did not have satisfactory fit indices in the proposed four-factor structure: p-value of χ2< 0.001, CFI=0.95, TLI=0.94, RMSEA=0.07, and SRMR=0.12. Several IMAS items showed relatively low factor loadings (ie, <0.4) or offending estimates (ie, >0.95). After removing the low-factor-loading and offending-estimate items, a 19-item IMAS remained and was reexamined in the four-factor structure CFA with all fit indices being satisfactory: p-value of χ2=0.93, CFI=1.00, TLI=1.00, RMSEA=0.00, and SRMR=0.06 (Table 3). Moreover, all the items had factor loadings ranging between 0.5 and 0.95 (Table 2). The 19 retained IMAS items also showed good corrected item-total correlations, ranging between 0.60 and 0.89 (Table 2). Moreover, there were nine items in the ATT domain, two in the SN domain, five in the PBC domain, and three in the IT domain.
 |
Table 2 Item Properties of the Intention of Inhaled Medication Adherence Scale (IMAS) |
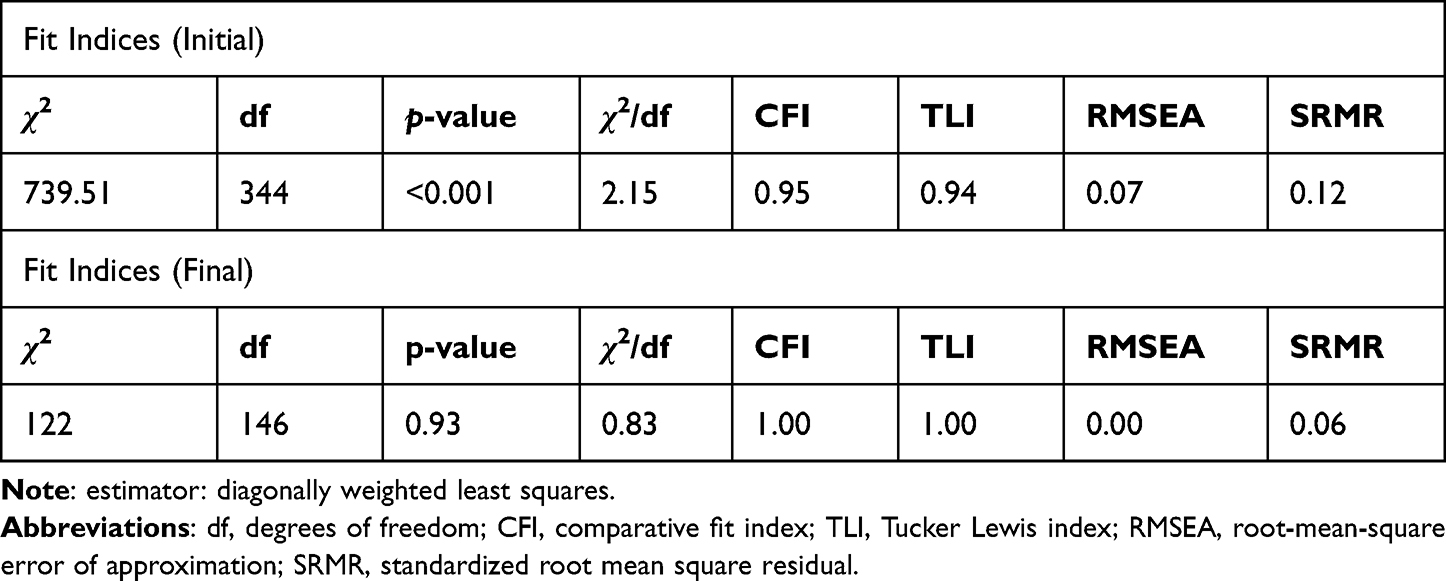 |
Table 3 Goodness-of-Fit Indices for Confirmatory Factor Analysis |
The 19-item IMAS was further examined for its domain internal consistency, domain convergent validity, and domain divergent validity. The internal consistencies of the four domains of the IMAS were very good to excellent (α=0.81 to 0.95); both CR and AVE were also higher than the suggested cutoffs (CR=0.81 to 0.94, above 0.6; AVE=0.59 to 0.77, above 0.5) (Table 4). Lastly, the divergent validity of the four domains in the IMAS was supported by the Fornell-Larcker criterion matrix. More specifically, the square root of AVE for each domain (eg, AT) was higher than the correlation coefficients of other domains with the tested domain (ie, AT with SN, AT with PBC, and AT with IT in the aforementioned example) (Table 5).
 |
Table 4 Cronbach’s α, Composite Reliability (CR), and Average Variance Extracted (AVE) in the Intention of Inhaled Medication Adherence Scale (IMAS) Constructs |
 |
Table 5 Divergent Validity of the Intention of Inhaled Medication Adherence Scale (IMAS) Using Fornell-Larcker Criterion Matrix |
Discussion
To the best of the authors’ knowledge, the present study is the first to use the TPB to design a valid instrument (ie, the IMAS) assessing attitudes, subjective norms, perceived behavioral control, and intention toward inhaled medication adherence among patients with COPD. The findings suggest that the IMAS is a valid instrument with promising psychometric properties regarding its content validity, internal consistency, convergent validity, and divergent validity. Subsequently, the present findings confirmed that the IMAS has a four-factor structure (ie, attitudes, subjective norms, perceived behavioral control, and intention) without the problem of overlapping items among the four factors.
The IMAS was first developed utilizing a standard procedure regarding TPB item generation.20 Therefore, the initial 28 items were designed with their assessed content fit within the definitions of the four TPB elements (ie, attitudes, subjective norm, perceived behavioral control, and intention). The appropriateness of each of the 28 items was verified by the experts with high content validity index across different disciplines including a respiratory therapist, a chest medicine physician, TPB experts, and psychometricians. However, some items were found to have low factor loadings in the CFA four-factor structure. Some reasons that may explain these low factor loadings are described below.
For the AT factor, Items 9 to 12 were found to have low factor loadings. This could be explained by the wording effect.35 More specifically, the retained items in AT factor shared the same item stem of “I think that using the inhaled medications…”, while Items 9 to 12 in the AT factor did not. In addition, these four items concerned negative attitudes toward inhaled medication use and this may have also resulted in low factor loadings when most of other items in the AT factor assessed positive attitudes (eight out of 13 items assessed positive attitudes). For the SN factor, the items assessing subjective norm from spouse and friends/relatives (ie, Items 1 and 2) had low factor loadings. This may be explained by the fact that patients cared less about the opinions from spouse and friends than the opinions from healthcare professionals.15 For the PBC factor, all items had strong factor loadings with one having an offending estimate. This indicates that the item (ie, Item 6) with the offending estimate highly overlapped with the content of other items.36 Therefore, the item provided little information to assess perceived behavioral control and could be removed. For the IT factor, Items 1 and 2 had low factor loadings and this may be explained by the wording effect (like the AT factor).35 More specifically, these two items assessed positive intention and the other three IT items assessed negative intention. Given that negative intention items had much stronger factor loadings than positive intention items, the negative intention items were retained with high factor loadings.
With the psychometric evidence of the IMAS demonstrated in the present study, healthcare providers who take care of patients with COPD can use the IMAS to assess potential factors affecting their inhaled medication adherence. Based on the TPB,20 inhaled medication adherence can be explained by the factors assessed using IMAS. Therefore, the IMAS can help healthcare providers further clarify which factors have strong associations with the inhaled medication adherence among their patients with COPD. In addition, the IMAS can be used as an evaluation measure to examine if any adherence improvement programs (when targeting attitudes, subjective norms, perceived behavioral control, or intention) are effective. However, when researchers or healthcare providers want to use the IMAS, they should be aware of other important factors that may affect individuals’ inhalation adherence. More specifically, level of education and knowledge in using medications by the patients is an important factor contributing to the inhalation adherence. Better educated patients are more likely to inhale properly and regularly than less educated patients.9
There are some limitations in the present study. First, the present sample had low representativeness because all participants were outpatients from a regional hospital in Taiwan. Given the low representativeness with the small sample size and use of convenience sampling, the present findings might not have good generalizability to other patient groups. Further studies are needed to replicate the present findings with the use of a larger and more representative samples (both in and outside of Taiwan). Moreover, all the participants were outpatients with relatively mild severity of COPD. Therefore, it is unclear if the present findings are generalizable to individuals with severe COPD. Second, the participants in the present study might have answered IMAS questions with a social desirability bias.37 More specifically, given that all participants were interviewed by a respiratory therapist, they were more likely to report relatively positive attitudes, subjective norms, perceived behavioral control, and intention under this circumstance. Similarly, the participants who agreed to take part in the study might have had a higher motivation and perhaps better adherence for an inhaled medication treatment than those who did not want to participate in the study. However, only 6% of all individuals who were approached did participate in the study. Third, other important psychometric properties of the IMAS were not examined, including test–retest reliability, criterion-related validity (with other relevant constructs regarding inhaled medication adherence),38 sensitivity (ie, whether the IMAS can effectively differentiate patients with different levels of attitudes, subjective norms, perceived behavioral control, and intention),39 and responsibility (ie, whether the IMAS can effectively detect the changes of attitudes, subjective norms, perceived behavioral control, and intention).40
Conclusion
The present study found that the 19-item IMAS had satisfactory psychometric properties in terms of its construct validity (ie, convergent validity and divergent validity for the four IMAS domains), internal consistency, and content validity. However, additional important psychometric properties of the IMAS need to be investigated in future studies, such as test–retest reliability and criterion-related validity. Nevertheless, the 19-item IMAS appears to be a useful instrument to help healthcare providers understand potential factors for individuals with COPD adhere to inhaled medications. More specifically, attitudes, subjective norms, perceived behavioral control, and intention of inhaled medication use can be confidently assessed using the 19-item IMAS.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, C-YL, upon reasonable request.
Ethics Approval and Informed Consent
Approval of this study was obtained from the Institutional Review Board of Chang Gung Medical Foundation under the reference number of 202101706B0C601. Moreover, the present study complies with the Declaration of Helsinki. All the participants provided written informed consent.
Consent for Publication
The present study did not report any data that could identify any specific participant. Therefore, the consent to publication is not applicable.
Acknowledgments
We thank all the participants who took part in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported in part by Chung Gung Memorial Hospital, Chiayi, Research Proposal No. CMRPG6M0051; and in part the National Health Research Institutes, Ref. No. NHRI- 11A1-CG-CO-04-2225-1.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Agustí A, Vogelmeier C, Faner R. COPD 2020: changes and challenges. Am J Physiol. 2020;319(5):L879–L883. doi:10.1152/ajplung.00429.2020
2. Blanco I, Diego I, Bueno P, et al. Geographical distribution of COPD prevalence in the Americas. COPD. 2018;15(4):317–325. doi:10.1080/15412555.2018.1481936
3. Lin W-C, Huang T-Y, Liu C-Y, Yeh M-L, C-H Y, Hwang S-L. Validation of the clinical COPD questionnaire in Taiwan. COPD. 2016;13(3):360–366. doi:10.3109/15412555.2015.1094456
4. Wold Health Organization. Chronic obstructive pulmonary disease (COPD); 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
5. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: a rapid systematic review and meta-analysis. PLoS One. 2020;15(5):e0233147. doi:10.1371/journal.pone.0233147
6. Cheng S-L, Lin C-H, Chu K-A, et al. Update on guidelines for the treatment of COPD in Taiwan using evidence and GRADE system-based recommendations. J Formosan Med Assoc. 2021;120(10):1821–1844. doi:10.1016/j.jfma.2021.06.007
7. Henrich R, Logue M. Feasibility of using the test for adherence to inhalers tool and tailoring education to the individual with chronic obstructive pulmonary disease. J Nurse Practit. 2017;13(10):e481–e483. doi:10.1016/j.nurpra.2017.07.025
8. Zhou Y, Zhong N-S, Li X, et al. Tiotropium in early-stage chronic obstructive pulmonary disease. N Engl J Med. 2017;377(10):923–935. doi:10.1056/NEJMoa1700228
9. Humenberger M, Horner A, Labek A, et al. Adherence to inhaled therapy and its impact on chronic obstructive pulmonary disease (COPD). BMC Pulm Med. 2018;18(1):1–6. doi:10.1186/s12890-018-0724-3
10. Lin C-Y, Scheerman JF, Yaseri M, Pakpour AH, Webb TL. A cluster randomised controlled trial of an intervention based on the health action process approach for increasing fruit and vegetable consumption in Iranian adolescents. Psychol Health. 2017;32(12):1449–1468.
11. Lin C-Y, Strong C, Scott AJ, Broström A, Pakpour AH, Webb TL. A cluster randomized controlled trial of a theory-based sleep hygiene intervention for adolescents. Sleep. 2018;41(11):zsy170. doi:10.1093/sleep/zsy061.448
12. Murphy G, Medin DL. The role of theories in conceptual coherence. Psychol Rev. 1985;92(3):289–316. doi:10.1037/0033-295X.92.3.289
13. Suh KH. Verification of a theory of planned behavior model of medication adherence in Korean adults: focused on moderating effects of optimistic or present bias. BMC Public Health. 2021;21(1):1–12. doi:10.1186/s12889-021-11460-x
14. Q-H H, Zheng J, Liu J-L, Wang J, You L-M. Predictors of medication adherence of patients with coronary heart disease after percutaneous coronary intervention: a structural equation modeling based on the extended theory of planned behavior. J Cardiovasc Nurs. 2022;37(4):350–358. doi:10.1097/JCN.0000000000000755
15. Kopelowicz A, Zarate R, Wallace CJ, Liberman RP, Lopez SR, Mintz J. Using the theory of planned behavior to improve treatment adherence in Mexican Americans with schizophrenia. J Consult Clin Psychol. 2015;83(5):985. doi:10.1037/a0039346
16. Lin C-Y, Updegraff JA, Pakpour AH. The relationship between the theory of planned behavior and medication adherence in patients with epilepsy. Epilepsy Behavi. 2016;61:231–236. doi:10.1016/j.yebeh.2016.05.030
17. Rich A, Brandes K, Mullan B, Hagger MS. Theory of planned behavior and adherence in chronic illness: a meta-analysis. J Behav Med. 2015;38:673–688.
18. Şanlıtürk D, Ayaz-Alkaya S. The effect of a theory of planned behavior education program on asthma control and medication adherence: a randomized controlled trial. J Allergy Clin Immunol Pract. 2021;9(9):3371–3379. doi:10.1016/j.jaip.2021.03.060
19. Godin G, Kok G. The theory of planned behavior: a review of its applications to health-related behaviors. Am J Health Promot. 1996;11(2):87–98. doi:10.4278/0890-1171-11.2.87
20. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
21. Fishbein M, Ajzen I. Belief, attitude, intention, and behavior: an introduction to theory and research. Contemp Sociol. 1977;5:6–244.
22. Madden TJ, Ellen PS, Ajzen I. A comparison of the theory of planned behavior and the theory of reasoned action. Pers Soc Psychol Bull. 1992;18(1):3–9. doi:10.1177/0146167292181001
23. Ajzen I. Constructing a theory of planned behavior questionnaire: conceptual and methodological considerations. Amherst, MA; 2006: 1–12.
24. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–497. doi:10.1002/nur.20147
25. Marsh HW, Balla JR, McDonald RP. Goodness-of-fit indexes in confirmatory factor analysis: the effect of sample size. Psychol Bull. 1988;103(3):391. doi:10.1037/0033-2909.103.3.391
26. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238. doi:10.1037/0033-2909.107.2.238
27. Fabrigar LR, Wegener DT, MacCallum RC, Strahan EJ. Evaluating the use of exploratory factor analysis in psychological research. Psychol Methods. 1999;4(3):272. doi:10.1037/1082-989X.4.3.272
28. Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis. Pearson Education Limited; 2013.
29. Bland JM, Altman DG. Statistics notes: cronbach’s Alpha. Br Med J. 1997;314(7080):572. doi:10.1136/bmj.314.7080.572
30. Hair JF, Hult GTM, Ringle CM, Sarstedt M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM). Sage Publications; 2021.
31. Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Market Res. 1981;18(1):39–50. doi:10.1177/002224378101800104
32. Ab Hamid M, Sami W, Sidek MM. Discriminant Validity Assessment: Use of Fornell & Larcker Criterion versus HTMT Criterion. IOP Publishing; 2017.
33. Rosseel Y. lavaan: an R package for structural equation modeling. J Stat Softw. 2012;48(2):1–36. doi:10.18637/jss.v048.i02
34. Revelle W, Revelle MW. Package ‘psych’. Comprehens R Arch Net. 2015;337:338.
35. Schriesheim CA, Eisenbach RJ. An exploratory and confirmatory factor-analytic investigation of item wording effects on the obtained factor structures of survey questionnaire measures. J Manage. 1995;21(6):1177–1193. doi:10.1177/014920639502100609
36. Dillon WR, Kumar A, Mulani N. Offending estimates in covariance structure analysis: comments on the causes of and solutions to Heywood cases. Psychol Bull. 1987;101(1):126. doi:10.1037/0033-2909.101.1.126
37. Grimm P. Social desirability bias. In: Wiley International Encyclopedia of Marketing. John Wiley & Sons Ltd; 2010. doi10.1002/9781444316568.wiem02057
38. Streiner DL, Norman GR, Cairney J. Health Measurement Scales: A Practical Guide to Their Development and Use. Oxford University Press; 2015.
39. Naumann A, Hochweber J, Klieme E. A psychometric framework for the evaluation of instructional sensitivity. Educ Asses. 2016;21(2):89–101. doi:10.1080/10627197.2016.1167591
40. Reise SP, Waller NG. Item response theory and clinical measurement. Annu Rev Clin Psychol. 2009;5(1):27–48. doi:10.1146/annurev.clinpsy.032408.153553
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Medication Adherence on Emergency Department Visits in Patients with COPD in a Single Tertiary Hospital in Saudi Arabia
Alshehri S, Alshibani M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:593-598
Published Date: 17 April 2023
Effects of Adherence to an mHealth Tool for Self-Management of COPD Exacerbations
Bischoff EW, Ariens N, Boer L, Vercoulen J, Akkermans RP, van den Bemt L, Schermer TR
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2381-2389
Published Date: 1 November 2023
Adherence to Self - Care Practice Among Type 2 Diabetes Mellitus Patients Using the Theory of Planned Behavior and Health Belief Model at Comprehensive Specialized Hospitals of Amhara Region, Ethiopia: Mixed Method
Simegn W, Mohammed SA, Moges G
Patient Preference and Adherence 2023, 17:3367-3389
Published Date: 13 December 2023
Mucolytic Therapy in COPD: Patient Usage and Preferences in Real-World Italian Settings
D’Antonio S, Pennisi A, Cazzola M
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:479-486
Published Date: 1 March 2025
Validation of the Traditional Chinese Version of the Belief About Medicines Questionnaire-Specific Among Adults with Type 2 Diabetes in Taiwan
Huang YM, Yang YM, Wang T, Ho YF, Chan HY
Patient Preference and Adherence 2025, 19:2039-2053
Published Date: 16 July 2025