Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Awareness of Usher Syndrome and the Need for Multidisciplinary Care: A Cross-Occupational Survey of Allied Health Clinicians
Authors Ayton LN ![]() , Galvin KL, Johansen L, O'Hare F, Shepard ER
, Galvin KL, Johansen L, O'Hare F, Shepard ER ![]()
Received 21 March 2023
Accepted for publication 29 June 2023
Published 13 July 2023 Volume 2023:16 Pages 1927—1936
DOI https://doi.org/10.2147/JMDH.S411306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Lauren N Ayton,1– 3,* Karyn L Galvin,4,* Lauren Johansen,5 Fleur O’Hare,1,3 Emily R Shepard5
1Department of Optometry and Vision Sciences, University of Melbourne, Parkville, VIC, Australia; 2Department of Surgery (Ophthalmology), University of Melbourne, Parkville, VIC, Australia; 3Centre for Eye Research Australia, Royal Victorian Eye and Ear Hospital, East Melbourne, VIC, Australia; 4Department of Audiology and Speech Pathology, University of Melbourne, Parkville, VIC, Australia; 5UsherKids Australia, Mordialloc, VIC, Australia
*These authors contributed equally to this work
Correspondence: Lauren N Ayton, Department of Optometry and Vision Sciences, The University of Melbourne, 202 Berkeley Street, Carlton, VIC, 3053, Australia, Email [email protected]
Background: Usher syndrome is the most common cause of deaf-blindness, affecting up to 1 in 6000 people. Multidisciplinary care is required to maximize outcomes for individuals and families. This study assessed awareness of Usher Syndrome amongst allied health clinicians who provide care related to the primarily affected senses of hearing and vision, ie, optometry, orthoptics and audiology.
Methods: A prospective cross-sectional online survey of clinicians working in Australian university-affiliated clinics (7 optometry, 1 orthoptics and 4 audiology) was completed between September 2021 and January 2022. Questions were asked about the cause, common symptoms, and awareness of health professions who manage Usher syndrome.
Results: The 27 audiologists, 40 optometrists, and 7 orthoptists who completed the survey included 53 females (71.6%), had an average age of 37 years (range 24– 70), and had an average duration of clinical experience of 13 years (range 1– 45 years). The majority of respondents correctly identified Usher syndrome as a genetic condition (86%), identified at least two of the affected senses (97%), and identified the progressive nature of the vision and hearing losses (> 90%). Awareness of vestibular dysfunction and its characteristics was low, as was knowledge of the key treatment roles that speech pathologists, genetic counsellors and geneticists play in the management of Usher Syndrome. The majority of respondents also did not identify important aspects of care within their own discipline.
Conclusion: This study has shown that there is a need for targeted education to be delivered to hearing and vision care allied health clinicians to raise awareness of the vestibular impacts and aspects of vision loss experienced by people with Usher syndrome. This education needs to target the broad range of clinicians who have a key role in providing multidisciplinary care (including speech pathologists, geneticists, and genetic counsellors) and to identify the key aspects of good-quality multidisciplinary care.
Keywords: deaf-blindness, optometry, audiology, orthoptics, genetics, physiotherapy
Usher syndrome is an autosomal recessive genetic condition.1 It is characterized by abnormal development of hair cells resulting in hearing impairment (Figure 1A), loss of retinal photoreceptor cells resulting in progressive vision loss (retinitis pigmentosa; Figure 1B), and possible vestibular dysfunction which is also due to hair cell abnormalities. Usher syndrome is thought to affect approximately 1 in 6000 individuals globally2 and is the leading cause of deaf-blindness worldwide.3
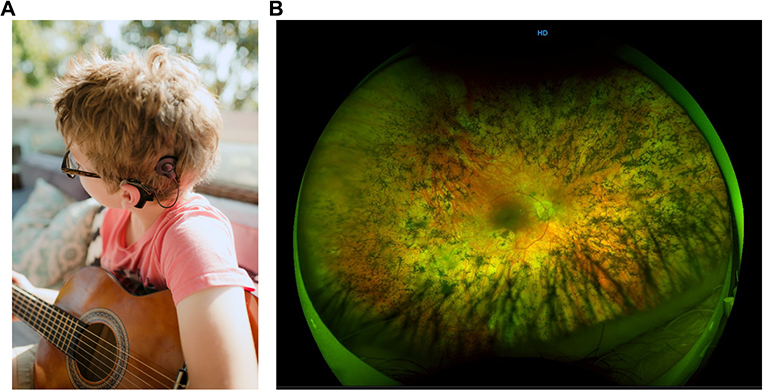 |
Figure 1 Child with profound sensorineural hearing impairment due to Usher syndrome using a cochlear implant to access sound (A) and image of another adult Usher patient’s retina, showing degeneration from retinitis pigmentosa (B). Image A courtesy of K. Disher-Quill, Image B courtesy of the VENTURE IRD registry, Centre for Eye Research Australia and the University of Melbourne.4 |
There are four recognized categories of Usher syndrome, each varying in severity, rate of progression and presence of vestibular dysfunction.5 Type I is defined by a profound congenital sensorineural hearing loss, onset of retinitis pigmentosa within the first decade of life, and vestibular dysfunction. Individuals with Type II commonly experience mild-to-moderate congenital sensorineural hearing impairment and the onset of retinitis pigmentosa from late adolescence to late twenties. The vestibular system is typically unaffected in individuals with Type II. Individuals with Type III usually experience the onset of progressive sensorineural hearing impairment in late childhood, with vision deterioration commencing any time between late adolescence and middle adulthood. Vestibular dysfunction is experienced by approximately half of individuals diagnosed with Type III. Recently, an atypical form of Usher syndrome (Type IV) has been identified, which is characterized by the late onset of retinitis pigmentosa and the usually late-onset progressive hearing impairment, without vestibular involvement.6 Each syndrome type has various subtypes, based on the causal gene mutation or genetic diagnosis. A recent review of the clinical characteristics of the condition has been published by Nisenbaum (2022).7
The dual sensory vision and hearing loss (deaf-blindness), potential vestibular involvement, and progressive nature of Usher syndrome results in multiplicative impacts for individuals. Adults with Usher syndrome have been found to have poor educational attainment and to be underemployed compared to those without the syndrome.8 They have reported higher rates of loneliness, increased prevalence of psychological disorders (such as depression and anxiety) and poorer physical health in comparison to the general population.9,10 Parents and carers may also be impacted due to the significant burden of coordination of care required for their child while managing their own grief about the uncertainty of their child’s future. Unaddressed vestibular dysfunction can lead to delayed motor development, poor school performance, and challenges in independent living due to the risk of accident and injury.11–13 In order to maximize outcomes, it is imperative that individuals with this complex and highly impactful condition receive timely multidisciplinary care from clinicians who are knowledgeable about the various types of Usher syndrome.
Individuals with rare conditions (with comparable prevalence rates to Usher syndrome) report significant challenges in accessing condition-informed care and treatment. In a survey of 1218 adults in the USA with a diverse range of rare diseases, respondents reported that the majority of clinicians were unaware of the existence and clinical characteristics of their specific condition.14 Furthermore, patients reported that their clinicians were often uninformed regarding the best- practice treatment or therapy for the condition and were unaware of suitable support available.14 A lack of clinician awareness and knowledge is associated with a delayed or absent diagnosis and with poorer outcomes for individuals in various health and wellbeing domains.14
In Australia, parents/guardians of children with rare conditions report not being connected to appropriate support services, increased burden on the child (and/or their families) to educate their healthcare team, and reduced confidence in clinicians’ abilities to provide effective therapy and treatment.15 As a result, individuals and their families may experience significant psychosocial distress, a lack of support, poor quality of life and reduced capacity to self-advocate.16 The lack of knowledge of rare diseases also often leads to delayed diagnosis. A study of 810 Australian adults with rare diseases found that 30% waited five or more years for a diagnosis, 66% had seen three or more doctors when seeking a diagnosis, and 46% had received at least one incorrect diagnosis.17 This study also reported that almost three-quarters (72%) of those surveyed felt that they did not receive enough information about their condition at the time of diagnosis.17
As Usher syndrome involves significant impairments in vision, hearing and, in some cases, vestibular function, best-practice treatment and therapy require not only condition-informed care from individual practitioners but also appropriate referral to clinicians of other disciplines. Anecdotally, families impacted by Usher syndrome report a lack of awareness of the condition and its impact on multiple senses, even amongst allied health clinicians who have a role in treating the major sensory impacts of Usher syndrome, ie, hearing and vision (personal communication, E. Shepard, June 2021). This limits timely access to appropriate multidisciplinary care, which is essential for Usher syndrome, as many of the symptoms are best managed with early intervention (for example, vestibular therapy, mobility training, and cochlear implantation). In addition, poor knowledge of the condition within the healthcare system is a barrier to the recommended best practices of patient or family-centered care for early intervention of conditions such as Usher syndrome.
To determine how best to improve the quality and accessibility of multidisciplinary care by improving knowledge of Usher syndrome and its management, it is first necessary to identify gaps in awareness that can be targeted in future educational efforts. The aim of the current study was to determine the level of awareness that allied health clinicians had of Usher syndrome, its cause and impacts, and the disciplines which have a role in caring for affected individuals. The allied health disciplines targeted in this study are those likely to be involved in the diagnosis of impairment in the primarily affected senses of hearing and vision, ie, audiology, optometry and orthoptics.
Methods and Materials
Ethical approval was received from the University of Melbourne (ID 2021–22187). Purposive sampling was used, with participants grouped by allied health discipline. The only inclusion criteria were that participants were audiologists, optometrists or orthoptists working in a clinical role in an Australian University teaching clinic. These clinics were approached with the view that clinicians employed in a university setting would be more likely to participate in research; the intention was to minimize, as far as possible, the self-selection bias of clinicians being more likely to participate if they had an interest in Usher syndrome, and therefore knew more about it. There was no pre-determined sample size; the aim was to recruit as close as possible to 100% of clinicians in each clinic. As participation was anonymous, no incentive was provided to participants nor was feedback given. Participants who wished to receive information about study outcomes provided an email address.
Data were collected using an online mixed-methods survey accessed via the Qualtrics platform (Qualtrics, Provo, UT). This was hosted by the University of Melbourne (license holder), with authors affiliated with the University of Melbourne (KG and LA) managing data collection. The survey was constructed by authors KG (audiologist with cochlear implant expertise), LA (optometrist with inherited retinal disease expertise), ES (community advocacy and support group director, mother with lived experience of a child with Usher syndrome Type I), LJ (community advocacy and support group staff member), and FOH (orthoptist with inherited retinal disease and hearing loss expertise) to examine basic awareness of Usher syndrome. To maximize the response rate within each clinic, a balance was achieved between the breadth and depth of data collected and the expected survey response time.
The initial survey questions were drafted by the authors based on previous literature, clinician experience, and lived family/carer experience. External, independent clinicians (two audiologists, two speech pathologists, one optometrist and one orthoptist) provided feedback on the draft survey; they also indicated their answers to the healthcare clinicians who had a key or secondary role in supporting people with Usher syndrome. In response to the feedback, some questions were removed or added, and modifications were made to the wording and the response format of other questions. The survey was then trialed via the survey link to the Qualtrics platform by three optometrists, two orthoptists, two speech pathologists and two audiologists. These clinicians did not work in university teaching clinics, and their data were not included in the final data set.
The final survey included nine closed-set demographic questions, including age, gender, years of clinical experience, patient groups treated, and type of clinical specialty. There were also five open-set and four closed-set questions related to the cause of Usher syndrome, the senses impacted, common sequelae, and the involvement of healthcare clinicians in management. The full list of survey questions is provided as Supplemental Digital Content. Survey branching ensured that participants were only presented with questions relevant to the level of knowledge demonstrated in their earlier responses, so the expected time to complete the survey was two minutes for participants with minimal knowledge and five to eight minutes for participants who completed all questions.
The managers of all Australian university teaching clinics in optometry, orthoptics and audiology (n = 16) were emailed an invitation for their clinic to participate, and twelve managers agreed. To ensure the anonymity of respondents, each clinic’s manager circulated the advertising material containing the survey link to their own clinical staff and re-circulated the material one week later as a reminder to participate. The link accessed the plain-language participant information form. Ticking the consent box at the end of this form enabled access to the survey questions. Data were collected from September 2021 to February 2022.
Survey data was downloaded from the Qualtrics platform and imported into SPSS software for statistical analysis. Eight incomplete responses were removed during data cleaning prior to analysis. Descriptive statistics (percentage answering correctly) were calculated for each item as a function of the clinical discipline. Fisher’s exact test of association was used to make comparisons between the “eye” professions (optometry and orthoptics) and the “ear” profession (audiology). We collapsed the eye professions into one group, given similar percentages of respondents and results in these related professions and the small sample size of orthoptists. Content analysis was applied to the open-set data related to the key aspects of hearing-related care (for audiologists) and vision-related care (for optometrists and orthoptists) to identify the most commonly reported management strategies. Content categories were generated through discussion between authors FO, ES and LA. The percentage of respondents who provided a response within each category was then calculated as a function of the clinical discipline independently by authors LA and FO and checked for discrepancies by author ES. Any disagreements in categorisations were discussed by this group of authors, and a consensus reached.
Results
Table 1 presents response rates and demographic information for each discipline. Fifty-three respondents (71%) were female. Only one respondent, an optometrist, reported particular expertise in Usher syndrome.
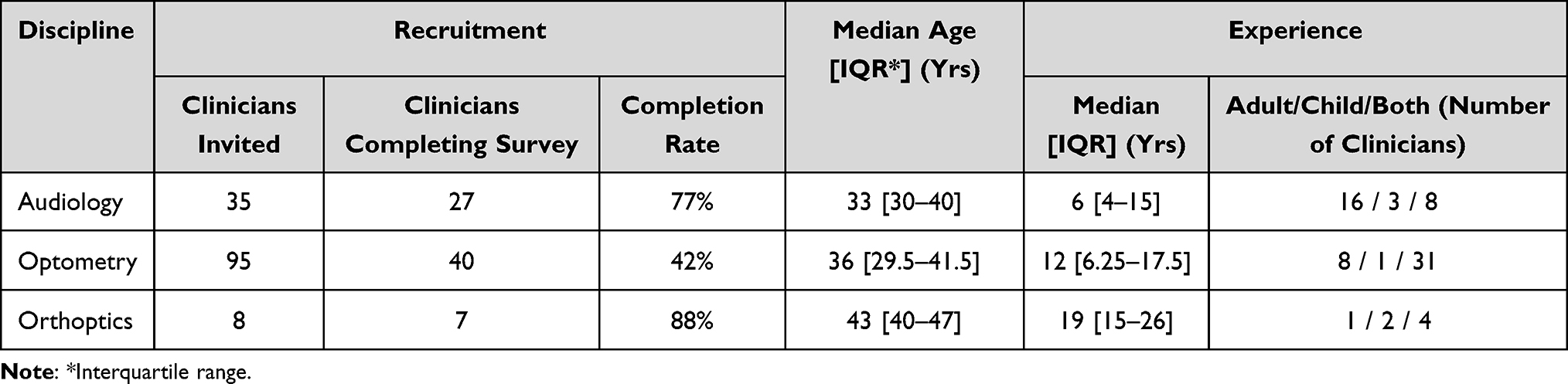 |
Table 1 Recruitment and Demographic Information for Each Discipline |
Awareness of Usher Syndrome and Affected Senses
Seventy-one (96%) of the 74 respondents had heard of Usher syndrome, with the other three “unsure”. Forty-nine (66%) respondents were confident that they knew the cause of Usher syndrome, with 15 unsure; all 64 of these respondents (86% of the total) subsequently correctly identified the cause as genetic. Half of all respondents identified all three senses affected by Usher syndrome, and an additional 47% identified hearing and vision but not vestibular. Overall, vestibular aspects were only identified by 50% of respondents.
Characteristics of Usher Syndrome
Table 2 presents the number of clinicians in each discipline correctly identifying the characteristics of Usher syndrome. In general, the key characteristics were well identified by all respondents and in each discipline group; these included vision loss (100%), which was progressive with onset in adolescence (>93%), and hearing loss (>95%), which was sensorineural, progressive and could be congenital in onset (>90%). Other characteristics of vision loss, such as retinitis pigmentosa, the presence of night blindness, and the possible congenital onset, were less well identified by both discipline groups but still recognized by at least 75% of respondents. Vestibular-related characteristics were least well identified, particularly gross motor delay (≤43%) and postural instability (≤51%) by both discipline groups. Audiologists were less likely to identify vestibular dysfunction as a feature of Usher syndrome, compared to the discipline group of optometrists and orthoptists (59% versus 87%, respectively, p = 0.009).
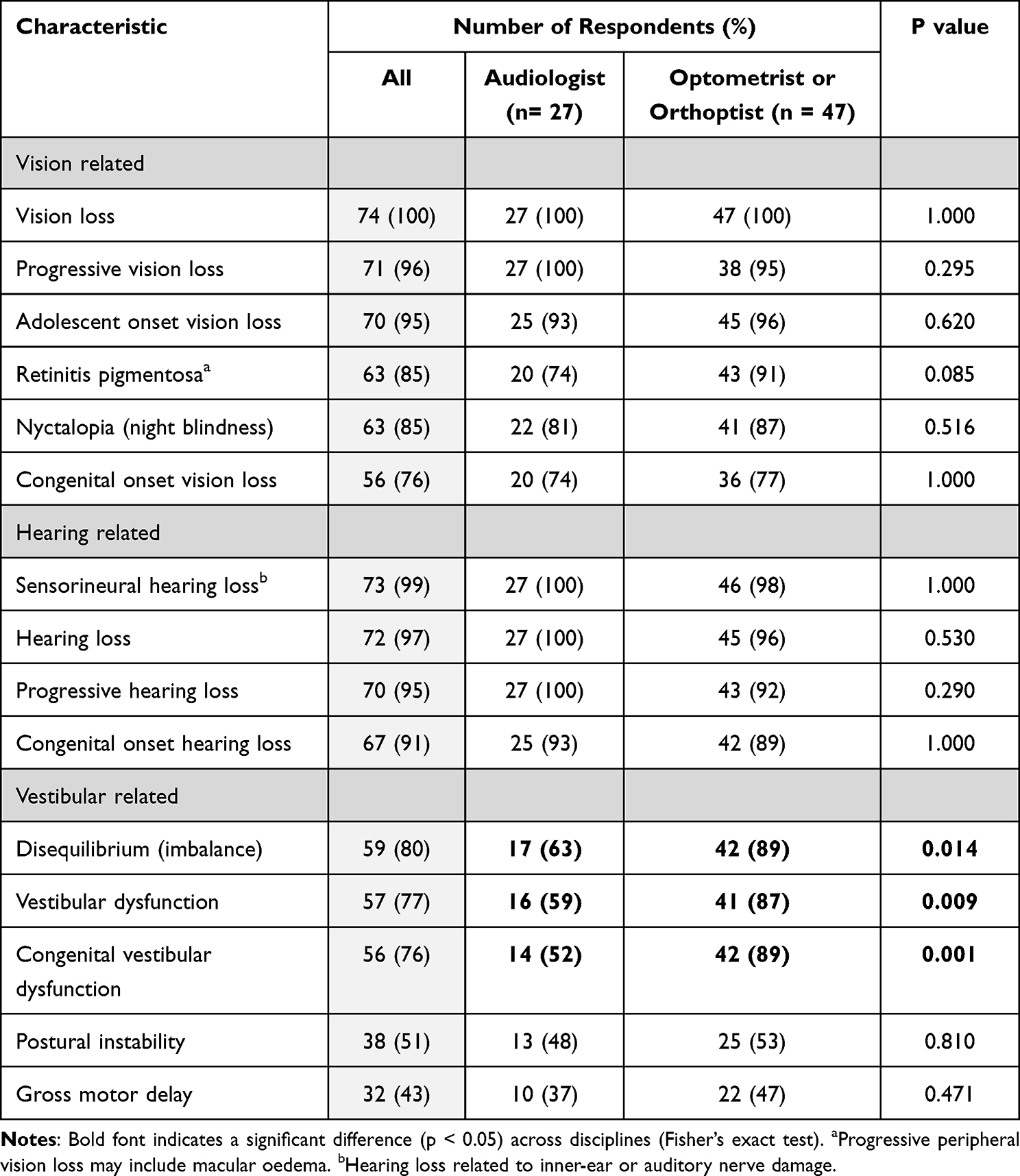 |
Table 2 Number (and Percentage) of Respondents Across and Within Each Discipline Group Correctly Identifying the Characteristics of Usher Syndrome |
Differing Roles of Various Disciplines in Usher Syndrome Support
Respondents were asked to select whether each of the 22 healthcare professions listed had a key role, a secondary (or possible) role, or no particular role in the management of Usher syndrome (refer to Supplemental Digital Content, Q15).
Table 3 presents the number of respondents in each discipline correctly identifying healthcare clinicians with a key role in managing Usher syndrome. On average across all discipline groups, the percentage of respondents recognizing the key role of audiologists, ophthalmologists, general practitioners, pediatricians and otolaryngologists was moderately high and varied between 70% and 93%. There was relatively poor recognition of the key role of speech pathologists across respondents, with no significant difference between discipline groups (audiologists (43%) and orthoptist/optometrist group (37%), p > 0.05). The discipline group of audiologists, was less likely to identify a both a geneticist and genetic counsellor as having a key or secondary role in the management of Usher syndrome, compared to the discipline group of optometrists and orthoptists (geneticist p = 0.006, and genetic counsellor p = 0.004, respectively).
 |
Table 3 Number (and Percentage) of Respondents, Across and Within Each Discipline Group, Correctly Identifying Healthcare Clinicians Which Play a Key Role, Secondary Role or No Role in the Management of Usher Syndrome. All Other Clinician Roles from the Survey Were Correctly Identified as Not Playing a Role by All Respondents |
Knowledge of Discipline-Specific Care for Usher Syndrome
The percentage of respondents identifying particular aspects of care within their own discipline for individuals with Usher syndrome are shown in Figure 2. The 11 categories in Figure 2 were identified through our content analysis process: regular monitoring, assistive technology, collaborative care, rehabilitation, referral to other healthcare disciplines, early diagnosis, counselling/patient education, skills-based training, environmental modifications, genetic testing and school-based supports. Audiologists frequently identified the need for regular monitoring (78%) and for assistive technology (67%), and orthoptists identified the need for assistive technology (57%) and counselling/patient education (57%), however these findings were the exception, and relatively few respondents within any discipline identified other important aspects of care such as referral to other healthcare disciplines, collaborative care or early diagnosis.
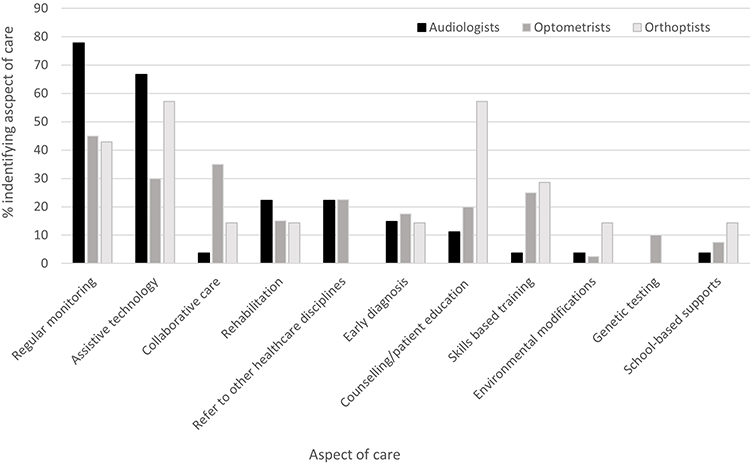 |
Figure 2 Percentage of audiologists (n = 27), optometrists (n = 40), and orthoptists (n = 7) who identified a particular aspect of care when describing care within their own discipline for individuals with Usher syndrome. |
Discussion
As Usher syndrome is a complex and highly impactful condition, it is important that allied health clinicians who provide vision and hearing-related care are aware of the cause, the symptoms, and how to care for this condition. This survey of audiologists, representing a hearing-related discipline, and optometrists and orthoptists, representing a vision-related discipline, showed high levels of awareness of Usher syndrome and its genetic cause. Additionally, there were moderately high levels of awareness across respondents and discipline groups of the key characteristics of the vision and hearing loss experienced by people with Usher syndrome. Vestibular characteristics of the condition were the least well identified, with audiologists less likely than eyecare practitioners to identify key vestibular characteristics. All surveyed disciplines were particularly poor at identifying the outcomes of postural instability and gross motor delay. Educational activities for audiologists, optometrists and orthoptists should focus on the variability and details of vision and hearing loss, along with the possibility of vestibular dysfunction, experienced by individuals with Usher syndrome. These educational activities will be relevant to all three disciplines.
In terms of the role of different disciplines in Usher syndrome care, only audiologists were correctly identified as having a key role by more than 90% of all respondents. Educational activities should emphasize the critical importance of referring to clinicians in key disciplines, and of the need for the engagement of a multidisciplinary team in the care of individuals with Usher syndrome. Priority should be given to educating audiologists, optometrists and orthoptists regarding the role of speech pathologists in the development of clear speech, expressive and receptive language, and pragmatic communication skills.
Recent initiatives, such as university cross-disciplinary allied health education,18 will likely improve understanding of the role of different disciplines in healthcare in general. Nevertheless, specialized educational programs will likely be required to maximize multidisciplinary co-operation in caring for people with Usher syndrome. Such co-operation is particularly important in rare and complex conditions, as a lack of coordinated care and consistent information across both medical and non-medical domains can lead to poorer outcomes.19 The contribution of various medical practitioners (ophthalmologist, pediatrician, GP, and ENT) needs to be made clearer to audiologists, optometrists, and orthoptists, given that, for each type of medical practitioner, their key role was not well recognized by the respondents. In reality, each of these medical practitioners has an important contribution to make; this includes the GP who, in Australia, has a critical liaison role in managing treatment across multidisciplinary teams.
Of note, this study found that only around half of audiologists identified geneticists and genetic counsellors as having a key role in Usher syndrome management. Audiologists will benefit from targeted education regarding the role of genetic counsellors in helping people with Usher syndrome to navigate challenges such as family planning, and the important role of geneticists in diagnosing Usher syndrome variants, given the variation in symptom pattern and severity across Types I, II, and III described above. As audiologists are involved in providing care to very young children with hearing loss and more than half of all children with bilateral sensorineural hearing loss have a genetic cause,19 audiologists are uniquely positioned to provide families with information and referral for genetic testing. Information and referral are particularly important for families with concerns about visual symptoms and/or poor coordination and clumsiness, as this combination of symptoms may be due to Usher syndrome. As 95% of children with hearing loss are born to parents with normal hearing,20 an audiologist is often the first point-of-contact with relevant sections of the healthcare system, and the main source of early information. As such, it is critical that audiologists have the knowledge required to provide accurate and supportive information to families and to refer them to appropriate services.18
Regarding respondents’ knowledge of key aspects of care for individuals with Usher syndrome within their own discipline, the results indicate relatively low levels of awareness. These findings could be due to the clinician not considering a particular aspect of care, such as genetic testing, as being relevant to their own discipline. Although such testing would not be conducted by the respondents in this study, referral for genetic testing should be part of the care they provide. The low level of awareness is perhaps not surprising, given that 73 of the 74 respondents had no particular experience caring for people with Usher syndrome.
There are no specialized Usher syndrome clinics in Australia, so families will be attending general clinics, especially prior to and around the time of diagnosis. This is at a time when families are most vulnerable and can be easily traumatized by poorly informed comments or advice from treating clinicians. The important point here is not whether respondents have all of the required knowledge to provide ongoing quality care for people with Usher syndrome, but rather that they are sufficiently aware to take appropriate initial steps in response to the needs of an individual and their family.
Potential limitations of this study included the low response rate for invited optometrists (42%) and the small number of orthoptists (n = 7). Only one of the three university-affiliated orthoptic clinics in Australia agreed to participate in the study, and the small number of participants may have resulted in skewed data. The low response rate of optometrists is, if anything, likely to have over-estimated levels of awareness amongst this group. This is because individuals are more likely to respond to a survey if the topic is salient, ie, noticeable or important to them.21 The topic of Usher syndrome is most likely to be salient for individuals who already know something about the syndrome and less salient for those with no knowledge. The targeted recruitment of clinicians in university-affiliated clinics in an effort to maximize response rates is a limitation in terms of the generalizability of the results across the broader clinician population. Again, if anything, data collected from this highly educated population, which is exposed to the conduct and outcomes of research in their workplace, are likely to have overestimated the level of awareness of Usher syndrome.
Conclusion
This survey of audiologists, optometrists and orthoptists in Australian university-affiliated clinics found high levels of awareness of the genetic cause of Usher syndrome, and of the presence and most key characteristics of hearing loss and vision loss. The allied-health clinician respondents were less aware of the possibility of vestibular dysfunction and its consequences. Awareness of the key role of various healthcare disciplines in multi-disciplinary care varied, with no respondent group demonstrating high levels of awareness across different professionals. Awareness was particularly low for all respondent groups regarding the role of speech pathologists and low for audiologists regarding the role of geneticists and genetic counsellors. Levels of awareness of important aspects of care within the respondent’s own discipline were generally low, although this may have been influenced by the open-set nature of the questions.
Evidence suggests that early and appropriate referral to the key professionals involved in the care of patients with Usher syndrome is imperative in ensuring that they, and their families, receive a timely diagnosis, appropriate psychosocial support and specific management for all three sensory aspects. Not only does this optimize the potential benefits of early intervention but also improves the psychosocial impact of the diagnosis. Whilst there is no cure for Usher syndrome, the importance of proactive referral from the start and enabling patients and families to ask questions and be provided with accurate information can improve long-term outcomes. The findings from this study suggest that audiology, optometry and orthoptic professionals could benefit from education regarding the key aspects of Usher syndrome care. Future research should examine optimal tools and methods for delivering this education.
Ethics Approval and Consent to Participate
Ethical approval was received from the University of Melbourne (ID 2021-22187). All participants provided informed consent through the online participant information and consent form, before the survey opened. Informed parental consent was provided for publication of the image of the child in Figure 1.
Acknowledgments
We thank the Melbourne Disability Institute at The University of Melbourne for its role in connecting researchers with the UsherKids Australia community group. We thank the Australian clinics that distributed the survey to their staff: Melbourne Audiology and Speech Pathology Clinic and Melbourne Eyecare Clinic (University of Melbourne); Deakin University School of Medicine, Optometry Clinic; University of New South Wales Optometry Clinic; Centre for Eye Health (University of New South Wales); Flinders Health 2GO (Flinders University); QUT Health Clinics – Optometry (Queensland University of Technology); University of Western Australia Audiology and Optometry clinics; Latrobe Communication Clinic (Latrobe University); and University of Queensland Audiology Clinic. Statistical assistance was provided by Dr Myra McGuiness. Feedback on the survey prior to data collection was provided by two audiologists, two speech pathologists, two orthoptists and three optometrists, otherwise not involved in the study. We also acknowledge the contribution of a University of Melbourne Master of Audiology student who contributed to the data collection.
Funding
LA is funded by a National Health and Medical Research Council Investigator Grant (GNT#1195713) and a University of Melbourne Driving Research Momentum Fellowship. The funding bodies had no role in the study design, execution or writeup of this manuscript.
Disclosure
Dr Karyn L Galvin is a Principal Investigator on several clinical studies sponsored by Cochlear Limited. These studies are entirely separate to the work included in the submitted paper. The authors declare that they have no other competing interests in this work.
References
1. Vernon M. Usher’s syndrome—deafness and progressive blindness: clinical cases, prevention, theory and literature survey. J Chronic Dis. 1969;22:133–151. doi:10.1016/0021-9681(69)90055-1
2. Hope CI, Bundey S, Proops D, Fielder AR. Usher syndrome in the city of Birmingham--prevalence and clinical classification. Br J Ophthalmol. 1997;81(1):46–53. doi:10.1136/bjo.81.1.46
3. Fortnum HM, Summerfield AQ, Marshall DH, Davis AC, Bamford JM. Prevalence of permanent childhood hearing impairment in the United Kingdom and implications for universal neonatal hearing screening: questionnaire based ascertainment study. Br Med J. 2001;323(7312):536–540. doi:10.1136/bmj.323.7312.536
4. Britten-Jones AC, O’Hare F, Edwards TL, Ayton LN, Consortium VS. Victorian evolution of inherited retinal diseases natural history registry (VENTURE study): rationale, methodology and initial participant characteristics. Clin Experiment Ophthalmol. 2022;50(7):768–770. doi:10.1111/ceo.14110
5. Friedman TB, Schultz JM, Ahmed ZM, Tsilou ET, Brewer CC. Usher syndrome: hearing loss with vision loss. Adv Otolaryngol. 2011;70:56–65.
6. Khateb S, Kowalewski B, Bedoni N, et al. A homozygous founder missense variant in arylsulfatase G abolishes its enzymatic activity causing atypical Usher syndrome in humans. Genet Med. 2018;20(9):1004–1012. doi:10.1038/gim.2017.227
7. Nisenbaum E, Thielhelm TP, Nourbakhsh A, et al. Review of genotype-phenotype correlations in Usher syndrome. Ear Hear. 2022;43(1):1–8. doi:10.1097/AUD.0000000000001066
8. Ellis L, Hodges L. Life and change with usher: the experiences of diagnosis for people with usher syndrome. University of Birmingham School of Education Thesis; 2013. Available from: http://www.birmingham.ac.uk/Documents/collegesocial-sciences/education/projects/final-report-on-life-and-change-with-usher.
9. Arcous M, Putois O, Dalle-Nazebi S, et al. Psychosocial determinants associated with quality of life in people with usher syndrome. A scoping review. Disabil Rehabil. 2020;42(19):2809–2820. doi:10.1080/09638288.2019.1571637
10. Ehn M, Wahlqvist M, Danermark B, Dahlstrom O, Moller C. Health, work, social trust, and financial situation in persons with Usher syndrome type 1. Work. 2018;60(2):209–220. doi:10.3233/WOR-182731
11. Christy J. Use of vestibular rehabilitation in the pediatric population. Perspect ASHA Spec Interest Groups. 2019;4(6):1399–1405. doi:10.1044/2019_PERS-SIG7-2019-0002
12. Gioacchini FM, Alicandri-Ciufelli M, Kaleci S, Magliulo G, Re M. Prevalence and diagnosis of vestibular disorders in children: a review. Int J Pediatr Otorhinolaryngol. 2014;78(5):718–724. doi:10.1016/j.ijporl.2014.02.009
13. Rine RM, Cornwall G, Gan K, et al. Evidence of progressive delay of motor development in children with sensorineural hearing loss and concurrent vestibular dysfunction. Perceptual Motor Skills. 2000;90(3):1101–1112. doi:10.2466/pms.2000.90.3c.1101
14. Bogart KR, Irvin VL. Health-related quality of life among adults with diverse rare disorders. Orphanet J Rare Dis. 2017;12(1):177. doi:10.1186/s13023-017-0730-1
15. Zurynski Y, Deverell M, Dalkeith T, et al. Australian children living with rare diseases: experiences of diagnosis and perceived consequences of diagnostic delays. Orphanet J Rare Dis. 2017;12(1):68. doi:10.1186/s13023-017-0622-4
16. Lopez-Bastida J, Oliva-Moreno J, Linertova R, Serrano-Aguilar P. Social/economic costs and health-related quality of life in patients with rare diseases in Europe. Eur J Health Econ. 2016;17 Suppl 1:1–5. doi:10.1007/s10198-016-0780-7
17. Molster C, Urwin D, Di Pietro L, et al. Survey of healthcare experiences of Australian adults living with rare diseases. Orphanet J Rare Dis. 2016;11:30. doi:10.1186/s13023-016-0409-z
18. Cham KM, Gaunt H, Delany C. Pilot study: thinking outside the square in cultivating “soft skills”-going beyond the standard optometric curriculum. Optom Vis Sci. 2020;97(11):962–969. doi:10.1097/OPX.0000000000001594
19. Valerie S, Downie L, Paxton GA, et al. Childhood Hearing Australasian Medical Professionals (CHAMP) network: consensus guidelines on investigation and clinical management of childhood hearing loss. J Paediatr Child Health. 2019;55(9):1013–1022. doi:10.1111/jpc.14508
20. Koleilat A, Schimmenti LA, Poling GL. Current approaches to the management of Usher Syndrome for the clinician. Perspect ASHA Special Interest Groups. 2020;5(4):907–916. doi:10.1044/2020_PERSP-20-00013
21. Fan W, Yan Z. Factors affecting response rates of the web survey: a systematic review. Comput Human Behav. 2010;26(2):132–139. doi:10.1016/j.chb.2009.10.015
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.