Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Awareness and Sociodemographic Factors as Predictors of Knowledge About Health Economics and Pharmacoeconomics Among Registered Nurses: A Cross-Sectional Study
Authors Alanazi HI ![]() , Tumala RB
, Tumala RB ![]() , Asiri MY, Alharbi HA
, Asiri MY, Alharbi HA ![]() , Alenazy BA
, Alenazy BA ![]() , Al-Ghareeb SA
, Al-Ghareeb SA ![]() , Alsmari AA, Alsbaie MA
, Alsmari AA, Alsbaie MA
Received 18 September 2025
Accepted for publication 5 December 2025
Published 12 December 2025 Volume 2025:17 Pages 897—913
DOI https://doi.org/10.2147/CEOR.S568493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Homoud Ibrahim Alanazi,1,* Regie Buenafe Tumala,1,* Mousa Yahya Asiri,1,* Homood Awadh Alharbi,1,* Badr Ayed Alenazy,2,* Sahar Abdulkarim Al-Ghareeb,3,* Abdurahman Abdullah Alsmari,4,* Mohammed Abdulaziz Alsbaie5,*
1College of Nursing, King Saud University, Riyadh, 12372, Kingdom of Saudi Arabia; 2Nursing Department, Northern Borders Health Cluster, Arar, 73311, Kingdom of Saudi Arabia; 3College of Nursing, Imam Abdulrahman bin Faisal University, Dammam, 34211, Kingdom of Saudi Arabia; 4Nursing Department, King Khalid University Hospital, King Saud University Medical City, Riyadh, 12372, Kingdom of Saudi Arabia; 5Nursing Department, Dental University Hospital, King Saud University Medical City, Riyadh, 12372, Kingdom of Saudi Arabia
*These authors contributed equally to this work
Correspondence: Homoud Ibrahim Alanazi, College of Nursing, King Saud University, Riyadh, 12372, Kingdom of Saudi Arabia, Tel +966507177727, Email [email protected] Regie Buenafe Tumala, College of Nursing, King Saud University, Riyadh, 12372, Kingdom of Saudi Arabia, Tel +966554773976, Email [email protected]
Background and Objectives: Global demand for health economics/pharmacoeconomics (HE/PE) has significantly increased, leading to a greater need for competent and skilled healthcare professionals in this field. However, the current literature indicates a lack of research regarding HE/PE among healthcare professionals, including those in the Kingdom of Saudi Arabia (KSA), particularly among registered nurses. Hence, this study assessed registered nurses’ levels of awareness and knowledge of HE/PE and their sociodemographic and HE/PE-related predictors.
Methods: A descriptive–correlational, cross-sectional design was used. The study was conducted on a convenience sample of 324 registered nurses working at the three hospitals within King Saud University Medical City, Riyadh, KSA. Data were collected from May 2025 to June 2025, and analyzed using SPSS v.30. Binary logistic regression analyses were conducted for HE/PE awareness, and multiple linear regression analyses were performed for knowledge about HE/PE. The significance level was established at p < 0.05.
Results: Registered nurses demonstrated an overall low level of knowledge (2.39/5), while showing a good level awareness about HE/PE across four awareness items (52.8% to 84.6%) but suboptimal for the remaining two items (38.6% and 38.9%). Several sociodemographic and HE/PE-related factors were identified as significant predictors of the registered nurses’ awareness and knowledge regarding HE/PE. Notably, four out of the six awareness items: “have heard about HE/PE” (p =0.040), “read articles related to HE/PE regularly” (p < 0.001), “participate in HE/PE decisions at work” (p < 0.042), and “implement HE/PE techniques to make decisions” (p < 0.001) were revealed as significant predictors of registered nurses’ knowledge about HE/PE.
Conclusion: The findings indicate that the knowledge level regarding HE/PE among registered nurses was low; nevertheless, their awareness was acceptable. It is crucial to develop and implement targeted educational strategies and interventions aimed at enhancing both awareness and knowledge about HE/PE among registered nurses in the KSA, while meticulously considering pertinent sociodemographic and HE/PE-related factors.
Keywords: awareness, health economics, knowledge, registered nurse, pharmacoeconomics, Saudi Arabia
Introduction
The global demand for health economics (HE) has significantly increased, leading to a greater need for professionals skilled in this field.1 Pharmacoeconomics (PE) can be classified as a branch of HE that identifies, quantifies, and compares the costs and consequences associated with pharmaceutical products and services.2 Possessing thorough awareness and knowledge of HE/PE is crucial for healthcare professionals,3–5 especially for registered nurses in the following aspects of clinical decision-making, responsible resource allocation, and provision of cost-effective care.6–9 A key aspect of these competencies is that by examining the economic consequences of various treatment alternatives, having a solid understanding of HE/PE assists nurses in making well-informed decisions about the distribution of healthcare resources, thereby optimizing the utilization of available financial resources.6–9 Additionally, a robust grasp of HE/PE empowers nurses to prioritize interventions that enhance health outcomes while reducing waste, ultimately improving the overall efficiency of healthcare.6–9 Furthermore, they enable nurses to assess the cost-effectiveness of medications and healthcare interventions, ensuring that treatment choices are based on their value in relation to health outcomes and the associated costs.6–9 In essence, nurses who are well-versed in HE/PE are better prepared to make decisions that enhance patient care and support the sustainability of healthcare systems. These competencies are crucial for nurses to adeptly navigate the complexities of healthcare decision-making and to deliver cost-effective care that addresses patient needs while managing the financial resources of healthcare systems.
From a historical standpoint, the Health Economics and Outcomes Research (HEOR) originated in the 1960s, driven by the necessity to enhance healthcare quality through an understanding of the value of health-improving interventions.1 In the subsequent decades, heightened global focus on the cost-effective application of medical treatments has augmented the field’s importance of assessing clinical effectiveness, economic outcomes, and health-related quality of life.1 During the COVID-19 pandemic, healthcare expenses have risen.10 In 2020, the Intercontinental Medical Statistics – Institute for Healthcare Informatics reported that around 500 billion standard units of pharmaceuticals (medicines/drugs) were utilized by the populations in the Middle East and North Africa region.11 As a country, the Kingdom of Saudi Arabia (KSA) is part of the Middle East, particularly as one of the six countries that comprise the Arab Gulf or Gulf Cooperation Council (GCC).12 Nonetheless, there exists a significant correlation between inefficient public pharmaceutical spending and an urgent requirement for medications.11 In this context, families with extremely low monthly incomes rely entirely on public health institutions, which are severely lacking in resources, including products, personnel, and expertise. This underscores the critical necessity for cost-analysis studies, particularly in the KSA. In alignment to Vision 2030 of the KSA, the Health Sector Transformation Program seeks to enhance both the accessibility and quality of healthcare services.13 This initiative includes essential skills in HE/PE, including the economic evaluation of healthcare interventions, the formulation of health policies, and cost-effectiveness analysis.13 This set of skills is essential for the successful implementation of this program, necessitating that healthcare professionals, including nurses, possess the required HE/PE competencies.
Existing literature clearly depicts that research in HE/PE has primarily involved pharmacists and pharmacy students, with only a single study involving solely nurses in the United States of America (USA).9 This topic has remained unexplored among registered nurses in the KSA. Hence, the main contribution of this study is the identification of HE/PE that is currently perceived by registered nurses, which should be brought to the attention of the nursing profession to improve their overall awareness and knowledge of HE/PE. In addition, the exploration should include the demographic and HE/PE-related characteristics that are linked to perceptions of specific HE/PE of registered nurses in the KSA. The results have important policy implications regarding the development of appropriate educational strategies to strengthen registered nurses’ awareness and knowledge of HE/PE as well as the value of HE/PE competencies in their profession in the KSA.
Aim and Specific Objectives
The aim of this study was to assess registered nurses’ levels of awareness and knowledge of HE/PE, and their sociodemographic and HE/PE-related predictors. The study’s aim was achieved through the following specific objectives, which are to:
- Identify sociodemographic and HE/PE-related characteristics of registered nurses.
- Assess the awareness of registered nurses regarding the application of HE/PE into practice.
- Determine the level of knowledge of registered nurses in HE/PE.
- Examine how registered nurses’ sociodemographic and HE/PE-related factors influence their awareness of HE/PE.
- Explore the influence of awareness factors as well as registered nurses’ sociodemographic and HE/PE-related factors on their overall knowledge of HE/PE.
Materials and Methods
Research Design
This is a quantitative study that employed a cross-sectional and correlational design involving the administration of an online survey directed at registered nurses. The cross-sectional online survey aimed to assess registered nurses’ levels of awareness and knowledge of HE/PE. In addition, correlational design was employed to explore the associations between the study variables as well as specific socio-demographic and HE/PE-related characteristics of registered nurses. It also allowed the examination of the predictors of awareness and knowledge of HE/PE among registered nurses.
In the current study, the meanings of awareness and knowledge in HE/PE have been distinctly defined based on prior study, particularly when used in public health research.14 According to the recommendations from Trevethan’s study,14 awareness pertains to information that holds personal relevance, whereas knowledge pertains to information that is, to varying degrees, detailed and factual in nature. Particularly, specific knowledge resides at the upper end of a continuum characterized by information specificity and accuracy, while general awareness is positioned at the lower end of the same continuum, indicating a lack of, or minimal, knowledge regarding a given topic.14 Awareness and knowledge essentially occupy opposing ends of a single continuum—a knowledge continuum.14 As applied in the context of the present study, awareness of HE/PE is situated at the lower end of the same continuum, while knowledge of HE/PE is located at the upper end of the continuum. Consequently, this guided the direction of the relationship of study variables, wherein a total of 17 predictor variables were identified. These predictors included awareness of HE/PE (comprising six items) along with 11 sociodemographic and HE/PE-related characteristics of registered nurses, which were set as predictor variables for their overall knowledge of HE/PE.
Setting and Population
This study was conducted in the three hospitals of King Saud University Medical City (KSUMC) in Riyadh, KSA, namely: King Khalid University Hospital (KKUH), King Abdulaziz University Hospital (KAUH), and Dental University Hospital (DUH). Registered nurses employed in the three hospitals of KSUMC were invited to participate in the online survey of this study.
Sampling Technique and Sample Size
This study used a convenience sampling technique. This sampling technique, which is commonly used in survey research, was utilized to recruit registered nurses by selecting a sample of research respondents who were readily accessible to the researchers and conveniently located within the research settings of the study.15 To qualify for inclusion in this study, registered nurses must be employed at one of the three hospitals of KSUMC, assigned to any nursing unit, and have completed over one year of employment. Nurses who underwent the general orientation program and had less than one year of employment were excluded from participating in this study.
To determine the required sample size, the G*Power version 3.1.9.7 software was utilized for the A-priori sample size calculation, aimed at conducting a statistical test of multiple linear regression with Fixed Model and R-squared increase having 17 predictor variables for knowledge of HE/PE. A minimum sample size of 208 was calculated as adequate for achieving a medium effect size of 0.15, with a margin of error set at 5% and a confidence interval of 95%. In addition, for regression analyses that involve six or more predictor variables, it is recommended to have a minimum of 10 respondents for each predictor.16 Moreover, the total number of respondents should exceed the number of predictors by a minimum of 50.16 In this study, we have 17 predictors, leading to a calculation of 17×10 = 170 respondents. When summing 170 and 50, the resulting minimum sample size was 220, which closely aligns with the calculated value of 208 derived from the abovementioned A-priori sample size calculation. Instead of merely adding the recommended minimum of 50 respondents,16 we opted to double the number of respondents (170 X 2) to enhance participation from the registered nurses. Consequently, we invited 340 registered nurses to participate in the online survey.
Instruments
The questionnaire of the online survey for this study consists of three parts. The first part contains 11 inquiries pertaining to the sociodemographic and HE/PE-related characteristics of registered nurses. It encompassed the following aspects of registered nurses: (1) age, (2) gender, (3) education, (4) work experience, (5) position, (6) unit, (7) course and (8) training in HE/PE, (9) interest in employing bachelor’s degree graduates who have more knowledge in HE/PE, (10) agreement for bachelor’s degree graduates needing more HE/PE skills, and (11) perspective on hiring new employees possessing HE/PE skills.
The second part employed the HE/PE awareness tool utilized in the research conducted by Hammad et al.8 The use of this tool has written permission from the copyright holder (as confirmed by an Email from Professor Eman A. Hammad, dated March 1, 2025). It comprises six items: two pertaining to having heard and familiarity with the concept of HE/PE, and four concerning the perceived application of HE/PE. Respondents answered these questions with either Yes or No. The content and face validity of this tool were previously evaluated; however, its reliability has not been established.8
The third part used the self-reported knowledge tool on HE/PE that was utilized in the research conducted by Hammad et al.8 The use of this tool has been granted written permission from the copyright holder, as verified by an Email from Professor Eman A. Hammad, dated March 1, 2025. This tool comprises 18 items pertaining to a specific set of terminologies associated with HE/PE. Registered nurses were required to answer these items using a five-point Likert scale, ranging from 1 (no knowledge) to 5 (very knowledgeable). The content and face validity of this tool have been assessed, with its reliability has yet to be established.8 In the current study, the evaluation and interpretation of each item, as well as the overall scale concerning knowledge of HE/PE, were specified within the following ranges: 1.00–1.80 indicates a very low level, 1.81–2.60 signifies a low level, 2.61–3.40 reflects an average level, 3.41–4.20 denotes a high level, and 4.21–5.00 represents a very high level of knowledge. The total score for a respondent on the scale was determined by calculating the average of the ratings given to each individual item.
Pilot Testing
A pilot study was conducted before the main study involving a sample of 25 registered nurses working at a different hospital. This assessment concentrated on the visual aspects of the instruments, encompassing elements such as formatting, readability, stylistic uniformity, and the clarity of terminology for the respondents. The pilot respondents were presented with the question, “Are the questions and terminology clear? If your answer is ‘No,’ please indicate which questions or terms were unclear.” This question was placed at the end of each page in the online survey, enabling respondents to offer feedback prior to proceeding to the next page of the questionnaire. After completing the survey, respondents were asked three additional questions: (1) “Is the online survey user-friendly and easy to navigate?”; (2) “How long did it take you to complete the survey?” to determine the average completion time; and (3) “Do you have any further comments?”. The pilot respondents reported that the online survey was user-friendly and simple to complete, allowing them to finish it within 5 to 7 minutes. Additionally, the reliability of the tools was also established from this pilot study. Reliability results revealed that the six items of awareness of HE/PE demonstrated acceptable Cronbach’s alpha coefficients: “heard about HE/PE” (0.77), “familiar with the term of HE/PE” (0.75), “consider knowledge of HE/PE to be important in job practice” (0.80), “read articles related to HE/PE regularly” (0.76), “participate in HE decisions at work” (0.77), and “implement HE techniques to decisions” (0.75). The overall scale measuring knowledge in HE/PE achieved a highly acceptable Cronbach’s alpha coefficient of.98.
Ethical Considerations
For this study, ethical approval was obtained from the Institutional Review Board of KSUMC. To secure the consent of registered nurses, respondents were required to provide informed consent prior to participating in the online survey. They were instructed to click the “Yes” button in the survey, indicating that they read and comprehended the study information presented in the consent form from the Ethics Committee of KSUMC, and that they voluntarily agreed to participate. Those respondents who accessed the online survey but chose not to continue were asked to click the “No” button and were directed to exit the survey. The completion of the survey was then regarded as implied consent, information that was explicitly stated within the consent form. Microsoft Excel tally sheets containing the implied consent of the registered nurses were securely stored on a password-protected hard drive of the researchers, particularly the corresponding author of this study.
Data Collection Procedure
After obtaining ethical approval and conducting the pilot test, data collection for the main survey was opened online for a total of four weeks. To collect the data, the online survey link and invitation emails were sent by the primary researcher to nurse managers of the three hospitals at KSUMC. Nurse managers were instructed to forward the research invitation and survey link to their nurses by email. In addition, the survey link distributed on the flyers were posted to notice (bulletin) boards of the nursing units. After respondents completed the online survey, their responses were automatically recorded to the Google Form of the online survey. Data were collected from May 2025 to June 2025.
Data Analysis
The collected data were extracted from the online survey (Google Form) and were transferred to Microsoft Excel; data cleaning was undertaken by the researchers. The clean data as well as the log code book were checked by the research team before performing data analysis in IBM SPSS version 30. For descriptive statistics, frequency counts, percentages, means, and standard deviations were calculated to analyse sociodemographic and HE/PE-related characteristics of registered nurses, and their levels of awareness and knowledge HE/PE.
Inferential statistics were also computed. In this study, nonparametric statistics was used because the data gathered were not normally distributed. In particular, the evaluation of data distribution normality utilized both the Kolmogorov–Smirnov test (p <0.001) and the Shapiro–Wilk test (p <0.001). The results of these normality tests suggested that the data did not adhere to a normal distribution, thereby validating the use of non-parametric inferential tests. Hence, the test of correlations used to determine relationships between variables was the Spearman rank correlations test. Binary logistic regression analyses were conducted for the six items of awareness of HE/HE where the 11 demographic profile and HE/PE-related variables were set in the six models as predictors. Lastly, multiple linear regression analyses were calculated where the 11 demographic profile and HE/PE-related variables, as well as the six items of the awareness of HE/PE were set in the model as predictor variables of registered nurses’ overall knowledge of HE/PE.
Results
Sociodemographic and HE/PE-Related Characteristics
Out of the 340 registered nurses invited to participate in the cross-sectional online survey, 324 responded with no missing data, resulting in a response rate of 95.3%. In this study, Table 1 presents the descriptive statistics regarding the sociodemographic and HE/PE-related characteristics of registered nurses. The average age of the nurse participants was 35.76 years (SD = 7.12), with ages ranging from 23 to 60 years, and the majority were female (n = 237, 72.1%). Most of them held a bachelor’s degree (n = 272, 84.0%) and with the highest proportion who worked in medical/surgical care units (n = 99, 30.6%) and had nursing experience for 6 to 10 years (n = 98, 30.2%). Most respondents were staff nurses (n = 216, 66.7%) who did not attend HE/PE course (n = 253, 78.1%) and did not have HE/PE training or workshop (n = 266, 82.1%) yet most of them preferred to hire new registered nurses with knowledge and skills in HE/PE (n = 258, 79.6%). Lastly, the highest proportion of the respondents agreed that “having knowledge of HE/PE is valued within the organization” (n = 157, 48.5%) and that “graduates with a bachelor’s degree need more HE/PE skills than most of them currently have” (n = 156, 48.1%).
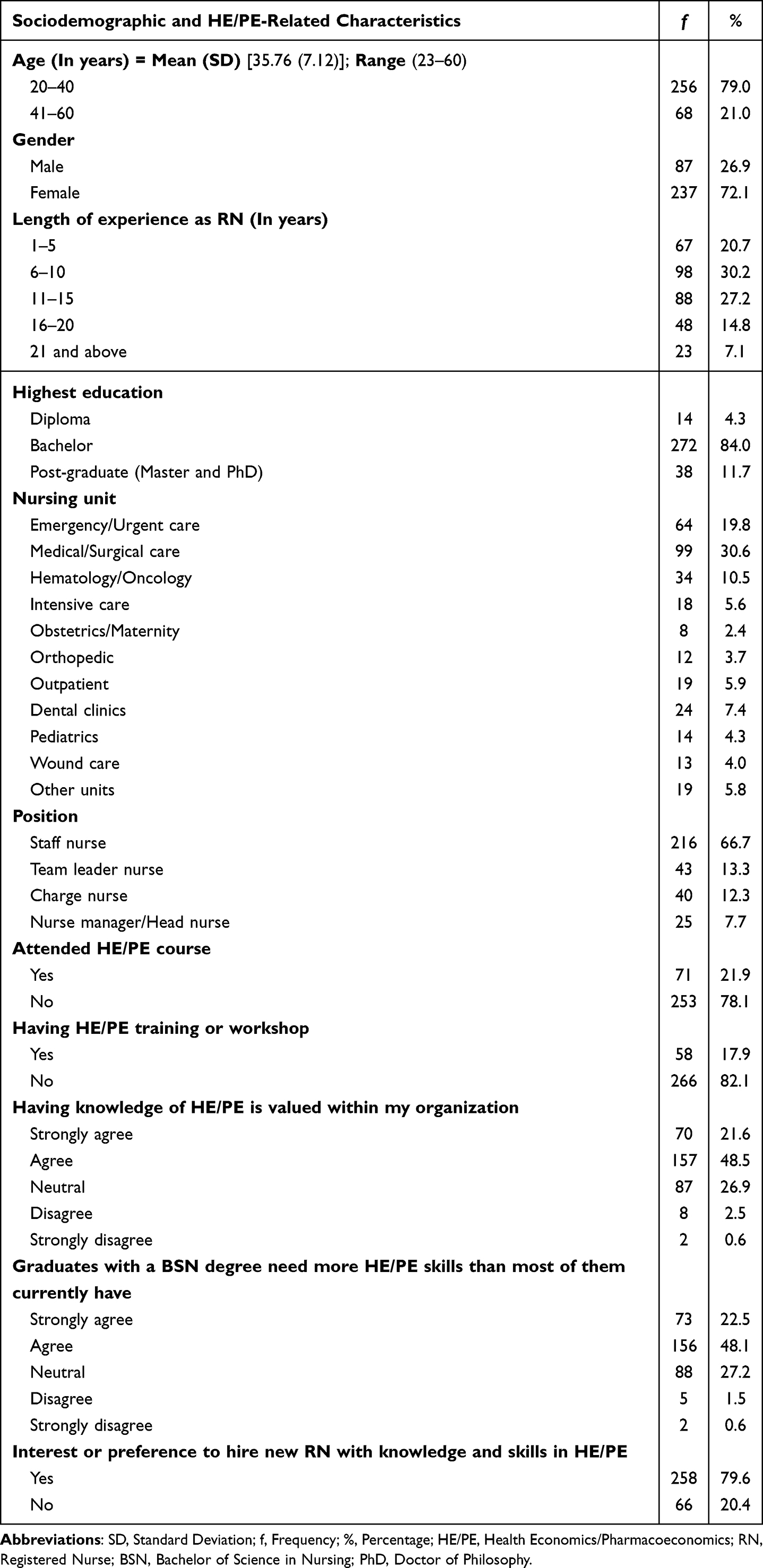 |
Table 1 Sociodemographic and HE/PE-Related Characteristics (n = 324) |
Awareness of Health Economics and Pharmacoeconomics
In the current study, there were six questions answerable by a yes or no, that evaluated the awareness of HE/PE of registered nurses as shown in Table 2. Majority of the respondents claimed that they were aware when asked if they heard about (n = 215, 66.4%) and familiar with (n = 186, 57.4%) HE/PE. In addition, they also considered the knowledge of HE/PE to be important in their job practice (n = 274, 84.6%) and implemented HE techniques to make decisions (n = 171, 52.8%). However, majority respondents reported that they did not participate in HE decisions at work (n = 198, 61.1%) and did not regularly read articles related to HE/PE (n = 199, 61.4%).
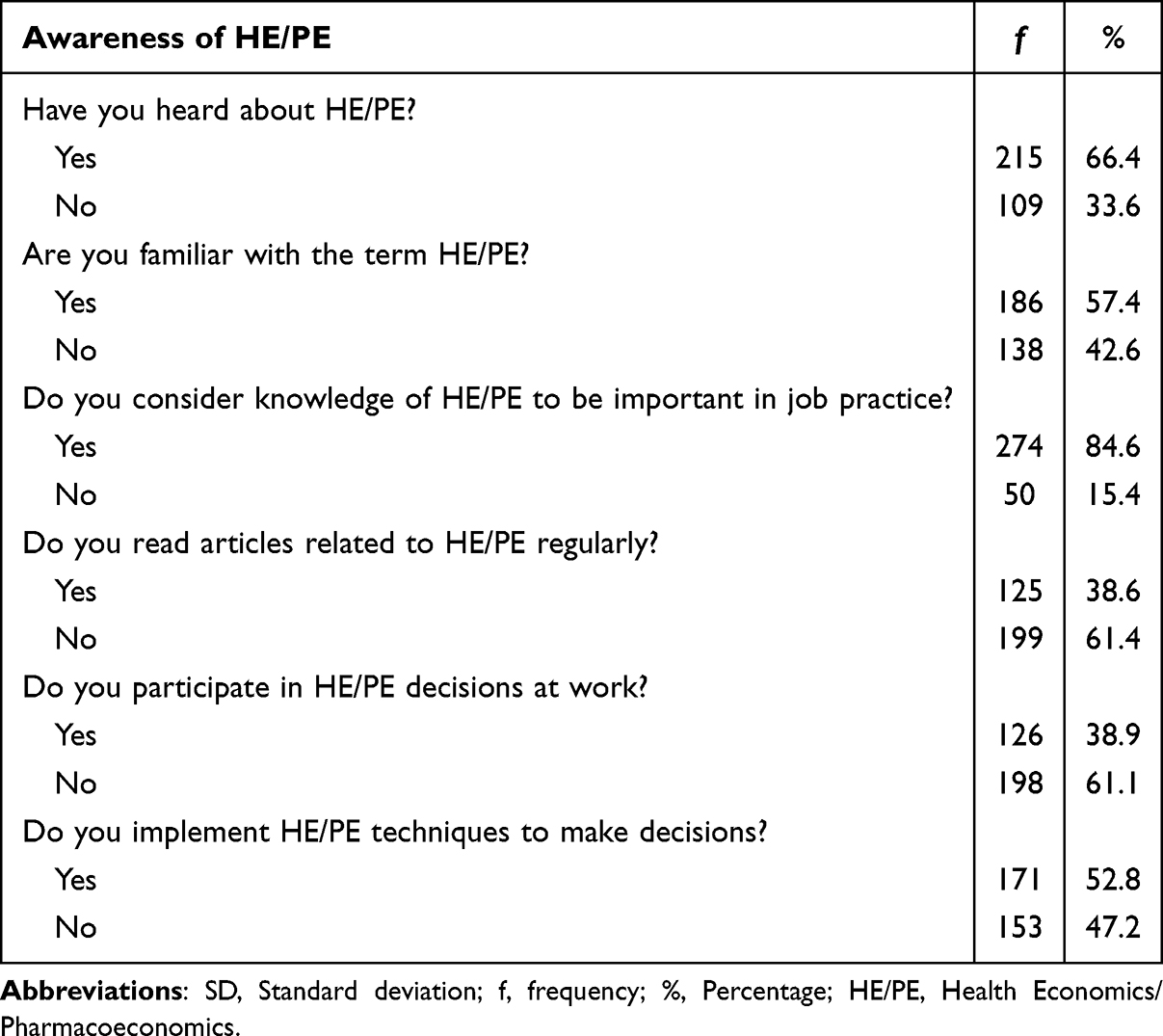 |
Table 2 Awareness of Health Economics/Pharmacoeconomics (n = 324) |
Knowledge of Health Economics and Pharmacoeconomics Terms
Overall, the registered nurses demonstrated a low level of knowledge of 18 HE/PE terms (see Table 3), with a mean score of 2.39 out of 5. Based on the findings, it is important to highlight that the respondents had average level of knowledge only in the term of “economic evaluation” (Mean = 2.64, standard deviation [SD] = 1.03). Notably, the respondents displayed low level of knowledge regarding the other 17 HE/PE terms, with the following terms with the lowest ratings: “sensitivity analysis” (Mean = 2.29, SD = 1.15), followed by incremental cost effectiveness analysis (Mean = 2.27, SD = 1.16) and lastly, “gross national product (GNP) spent by Saudi Arabia on health” (Mean = 2.20, 1.13).
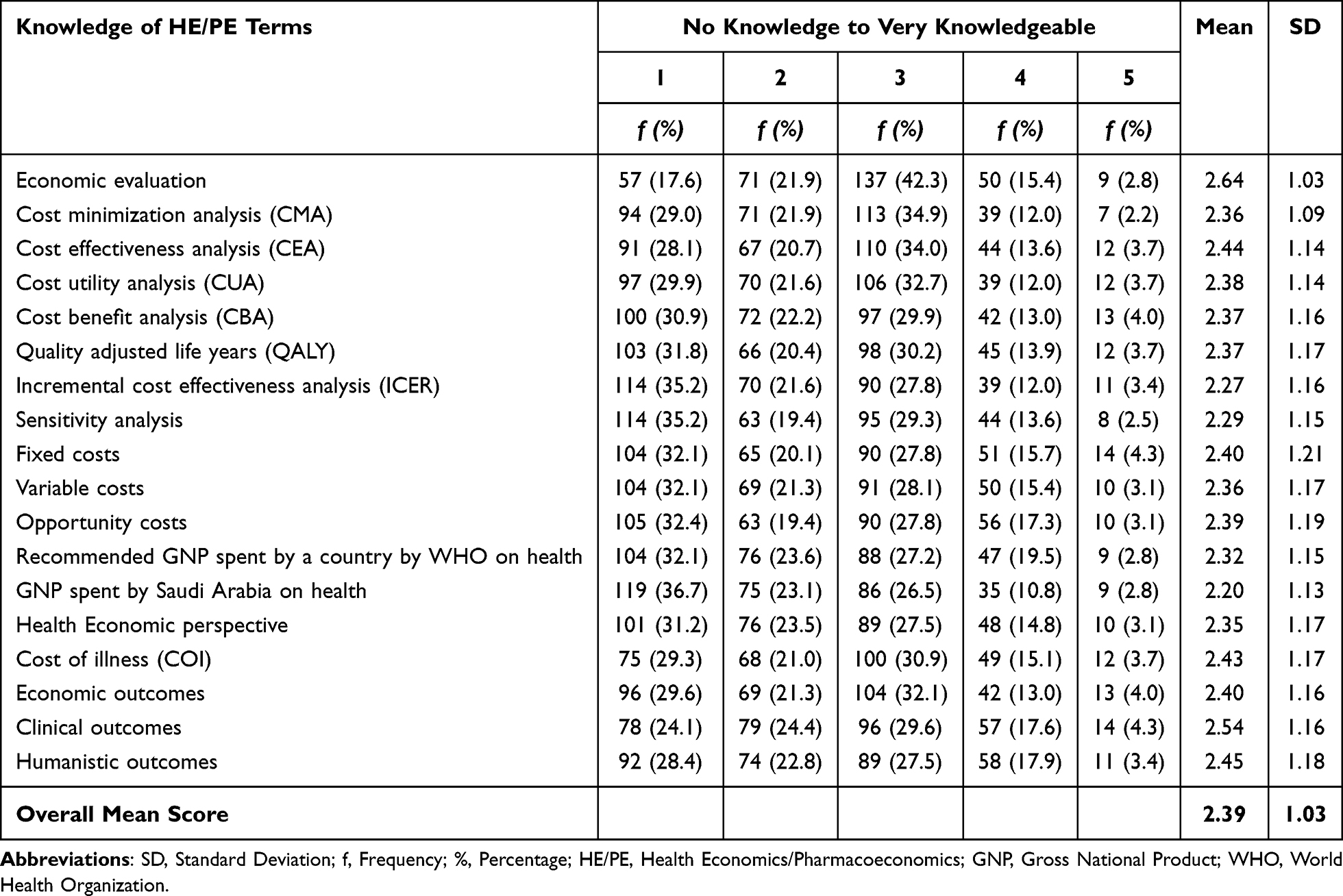 |
Table 3 Knowledge of Health Economics/Pharmacoeconomics Terms (n = 324) |
Correlation and Binary Logistic Regression Analyses
In this study, six sets of correlation analyses were performed utilizing the Spearman rho correlation test. Moreover, six models were employed for binary logistic regression analyses, corresponding to the six items related to the awareness of HE/PE among registered nurses (Table 4). This means that a test of relationship and a binary regression analysis were conducted for each of the six items of awareness in HE/PE.
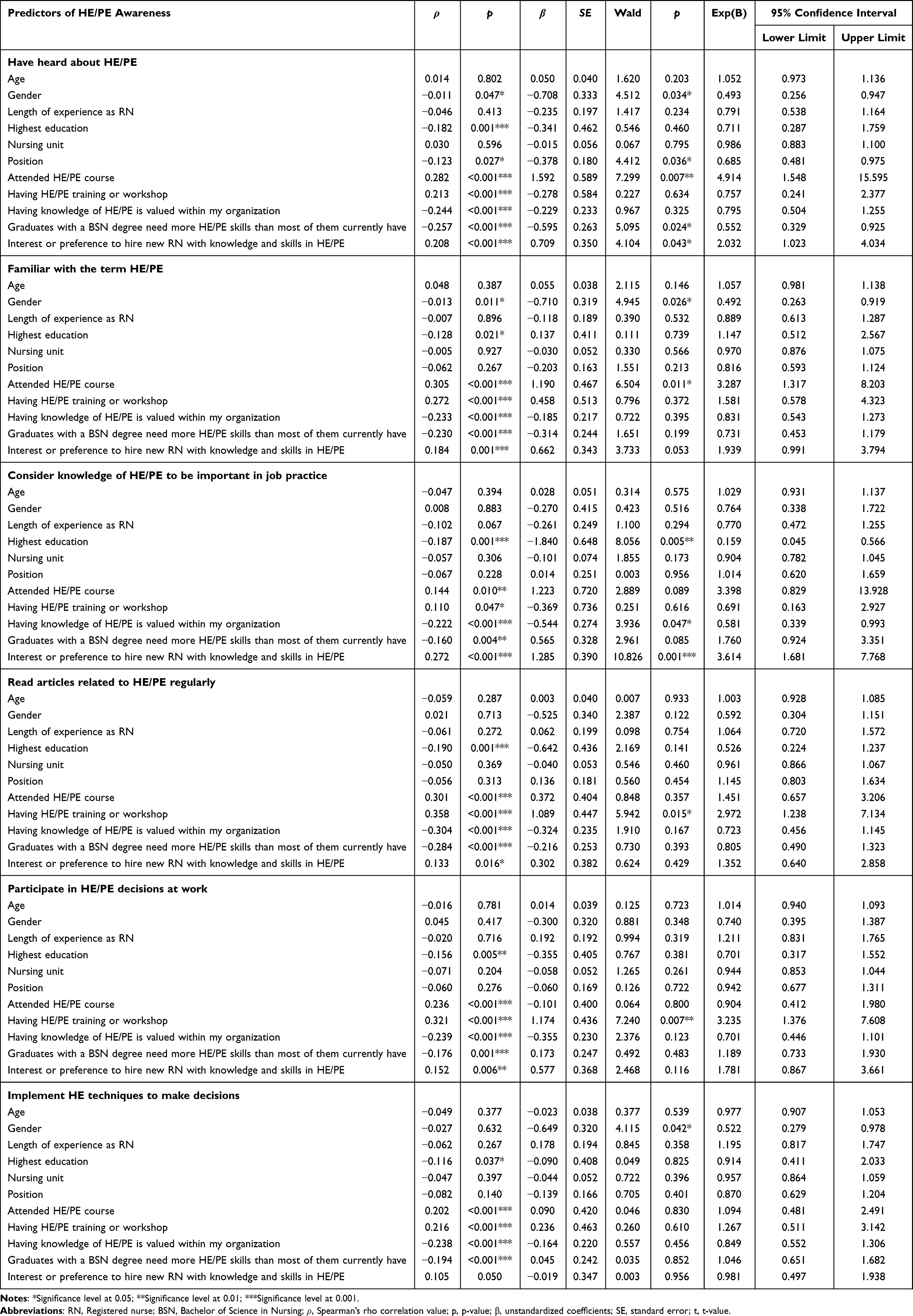 |
Table 4 Correlation and Binary Logistic Regression Analyses |
For Item 1, which pertains to “having heard about HE/PE,” the findings showed significant relationships with the following eight sociodemographic and HE/PE-related characteristics, including: gender (ρ = −0.011, p =0.047), highest education (ρ = −0.182, p =0.001), position (ρ = −0.123, p =0.027); having attended HE/PE course (ρ =0.282, p <0.001), having HE/PE training or workshop (ρ =0.213, p <0.001), “having knowledge of HE/PE is valued within my organization” (ρ = −0.244, p <0.001), “graduates with a bachelor’s degree need more HE/PE skills than most of them currently have” (ρ = −0.257, p <0.001), and having “interest or preference to hire new registered nurse with knowledge and skills in HE/PE” (ρ =0.208, p <0.001). Of these eight sociodemographic and HE/PE-related characteristics, five were identified as significant predictors. First, the regression coefficient (B) for gender was −0.708, with an odds ratio (OR) of .493. Furthermore, the calculated Wald statistics value was 4.512 (p =0.034; 95% CI =0.256,0.947), suggesting that gender served as a statistically significant predictor for having heard about HE/PE. Second, the position of registered nurses was also identified as a significant predictor for awareness of HE/PE (B = −0.378; OR =0.685), with a Wald statistics value of 4.412 (p =0.036; 95% CI =0.481,0.975). Third, attendance in HE/PE course also emerged as a significant predictor for awareness of HE/PE (B = 1.592; OR = 4.914), with a Wald statistics value of 7.299 (p =0.007; 95% CI = 1.548, 15.595). Fourth, the agreement with the assertion that graduates with a Bachelor of Science in Nursing (BSN) degree need more HE/PE skills than most of them currently have was also a significant predictor for having heard of HE/PE (B = −0.595; OR =0.552), with a Wald statistics value of 5.095 (p =0.024; 95% CI =0.329,0.925). Fifth, the interest or preference to hire new registered nurses with knowledge and skills in HE/PE emerged as a significant predictor for having heard of HE/PE (B =0.709; OR = 2.032), with a Wald statistics value of 4.104 (p =0.043; 95% CI = 1.023, 4.034).
With regard to Item 2, which pertains to “being familiar with the term HE/PE,” the results revealed significant correlations with seven sociodemographic and HE/PE-related characteristics, including: gender (ρ = −0.013, p =0.011), highest education (ρ = −0.128, p =0.021), having attended HE/PE course (ρ =0.305, p <0.001), having HE/PE training or workshop (ρ =0.272, p <0.001), “having knowledge of HE/PE is valued within my organization” (ρ = −0.233, p <0.001), “graduates with a bachelor’s degree need more HE/PE skills than most of them currently have” (ρ = −230, p <0.001) and having “interest or preference to hire new registered nurse with knowledge and skills in HE/PE” (ρ =0.184, p <0.001). Among the seven sociodemographic and HE/PE-related characteristics, two revealed significant predictions. First, gender emerged as a significant predictor (B = −0.710; OR =0.492), with a Wald statistics value of 4.945 (p =0.026; 95% CI =0.263,0.919). In addition, attendance in HE/PE course also emerged as a significant predictor for being familiar with the term HE/PE (B = 1.190; OR = 3.287), with a Wald statistics value of 6.504 (p =0.011; 95% CI = 1.317, 8.203).
In relation to Item 3, which pertains to “considering knowledge of HE/PE to be important in job practice,” the test of correlations indicated significant findings with six sociodemographic and HE/PE-related characteristics, including: highest education (ρ = −0.187, p =0.001), having attended HE/PE course (ρ =0.144, p =0.010), having HE/PE training or workshop (ρ =0.110, p =0.047), “having knowledge of HE/PE is valued within my organization” (ρ = −0.222, p <0.001), “graduates with a bachelor’s degree need more HE/PE skills than most of them currently have” (ρ = −0.160, p =0.004) and having “interest or preference to hire new registered nurse with knowledge and skills in HE/PE” (ρ =0.272, p <0.001). For the binary regression results, three significant predictions were identified, with the highest education being a significant predictor (B = −1.840; OR =0.159), with a Wald statistics value of 8.056 (p =0.005; 95% CI =0.045,0.566). Furthermore, “having knowledge of HE/PE is valued within the organization” also surfaced as a significant predictor for considering knowledge of HE/PE to be important in job practice (B = −0.544; OR =0.581), with a Wald statistics value of 3.936 (p =0.047; 95% CI =0.339,0.993). Moreover, the “interest or preference to hire new registered nurses with knowledge and skills in HE/PE” served as a significant predictor for considering HE/PE knowledge to be important in job practice (B = 1.285; OR = 3.614), with a Wald statistics value of 10.826 (p <0.001; 95% CI = 1.681, 7.768).
With respect to Item 4, having read articles related to HE/PE regularly, the test of relationships revealed that six sociodemographic and HE/PE-related characteristics showed significant correlations, including: highest education (ρ = −0.190, p =0.001), having attended HE/PE course (ρ =0.301, p <0.001), having HE/PE training or workshop (ρ =0.358, p <0.001), “having knowledge of HE/PE is valued within my organization” (ρ = −0.304, p <0.001), “graduates with a bachelor’s degree need more HE/PE skills than most of them currently have” (ρ = −0.284, p <0.001) and having “interest or preference to hire new registered nurse with knowledge and skills in HE/PE” (ρ =0.133, p =0.016). Meanwhile, the regression analysis indicated that only having HE/PE training or workshop was a significant predictor (B = 1.089; OR = 2.972), with a Wald statistics value of 5.942 (p =0.015; 95% CI = 1.238, 7.134).
In the context of Item 5, which pertains to “participating in HE/PE decisions at work,” the test of relationships uncovered that six showed significant correlations with sociodemographic and HE/PE-related characteristics, including the highest education (ρ = −0.156, p =0.005), having attended HE/PE course (ρ =0.236, p <0.001), having HE/PE training or workshop (ρ =0.321, p <0.001), “having knowledge of HE/PE is valued within my organization” (ρ = −0.239, p <0.001), “graduates with a bachelor’s degree need more HE/PE skills than most of them currently have” (ρ = −0.176, p <0.001) and having “interest or preference to hire new registered nurse with knowledge and skills in HE/PE” (ρ =0.152, p =0.006). On the other hand, the regression analysis showed that having HE/PE training or workshop was again identified as a significant predictor (B = 1.174; OR = 3.235), with a Wald statistics value of 7.240 (p =0.007; 95% CI = 1.376, 7.608).
Lastly, concerning Item 6, which pertains to “implementing HE/PE techniques to make decisions,” the test of correlations indicated that six sociodemographic and HE/PE-related characteristics displayed significant relationships, such as the highest education (ρ = −0.116, p =0.037), having attended HE/PE course (ρ =0.202, p <0.001), having HE/PE training or workshop (ρ =0.216, p <0.001), “having knowledge of HE/PE is valued within my organization” (ρ = −0.238, p <0.001), “graduates with a bachelor’s degree need more HE/PE skills than most of them currently have” (ρ = −0.194, p <0.001) and having “interest or preference to hire new registered nurse with knowledge and skills in HE/PE” (ρ =0.105, p =0.050). According to the regression analysis, the results revealed that gender was revealed as a significant predictor (B = −0.649; OR =0.522), with a Wald statistics value of 4.115 (p =0.042; 95% CI =0.279,0.978).
Correlation and Multiple Linear Regression Analyses
In this study, two correlation analyses were performed utilizing the Spearman rho correlation test, in conjunction with two multiple linear regression analyses for the overall knowledge of HE/PE, as the dependent variable (Table 5).
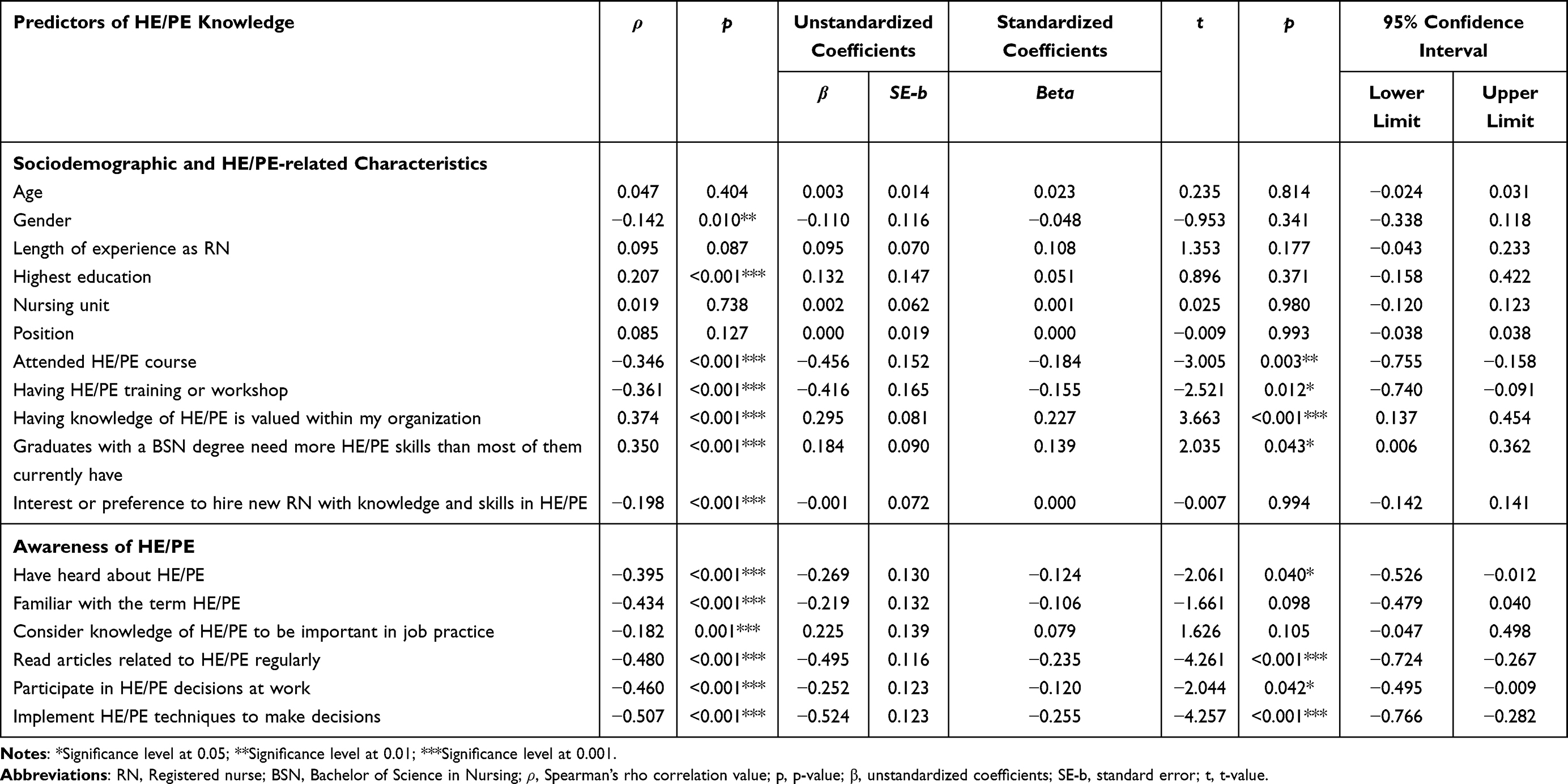 |
Table 5 Correlation and Multiple Linear Regression Analyses |
Regarding registered nurses’ knowledge of HE/PE, the correlation test indicated the presence of seven sociodemographic variables showed significant correlations, including: gender (ρ = −0.142, p =0.010), highest education (ρ =0.207, p <0.001), having attended HE/PE course (ρ = −0.346, p <0.001), having HE/PE training or workshop (ρ = −0.361, p <0.001), “having knowledge of HE/PE is valued within my organization” (ρ =0.374, p <0.001), “graduates with a bachelor’s degree need more HE/PE skills than most of them currently have” (ρ =0.350, p <0.001) and having “interest or preference to hire new registered nurse with knowledge and skills in HE/PE” (ρ = −0.198, p <0.001). In addition, all six awareness items: “heard about HE/PE” (ρ = −0.395, p <0.001), “familiar with the term of HE/PE” (ρ = −0.434, p <0.001), “consider knowledge of HE/PE to be important in job practice” (ρ = −0.182, p =0.001), “read articles related to HE/PE regularly” (ρ = −0.480, p <0.001), “participate in HE decisions at work” (ρ = −0.460, p <0.001), and “implement HE techniques to decisions” (ρ = −0.507, p <0.001) had significant relationships with registered nurses’ overall knowledge of HE/PE.
Meanwhile, the regression model 1 for knowledge of HE/PE was statistically significant (F [11, 308] = 9.622, p <0.001), explaining approximately 55.2% of the variance (R2 =0.304, Adjusted R2 =0.273). Model 1 identified four sociodemographic variables as significant predictors of knowledge of HE/PE, including having attended HE/PE course (β = −0.456, p =0.003, 95% CI = −0.755, −0.158), having HE/PE training or workshop (β = −0.416, p =0.012, 95% CI = −0.740, −0.091), “having knowledge of HE/PE is valued within my organization” (β =0.295, p = <0.001, 95% CI =0.137,0.454), and “graduates with a bachelor’s degree need more HE/PE skills than most of them currently have” (β =0.184, p =0.043, 95% CI =0.006,0.362). Additionally, the regression model 2 for knowledge of HE/PE was also statistically significant (F [6, 317] = 30.930, p <0.001), explaining approximately 60.8% of the variance (R2 =0.369, Adjusted R2 =0.357). Model 2 identified four awareness items as significant predictors of registered nurses’ knowledge of HE/PE, including: “heard about HE/PE” (β = −0.269, p =0.040, 95% CI = −0.526, −0.012), “read articles related to HE/PE regularly” (β = −0.495, p <0.001, 95% CI = −0.724, −0.267), “participate in HE decisions at work” (β = −0.252, p =0.042, 95% CI = −0.495, −0.009), and “implement HE techniques to decisions” (β = −0.524, p <0.001, 95% CI = −0.766, −0.282).
Discussion
This study explored levels of awareness and knowledge of HE/PE and their sociodemographic and HE/PE-related predictors based on the self-reports of registered nurses in the KSA. Overall, the awareness in HE/PE among registered nurses in the current study varied from low to good levels. In particular, majority of the registered nurses showed good awareness when asked if they considered the knowledge of HE/PE to be important in their job practice (84.6%), heard about (66.4%) and familiar with (57.4%) HE/PE, and in implementing HE/PE techniques to make decisions (52.8%). These results align with a previous study that indicated approximately 65% among health professions students in Jordan reported they had heard of HE/PE.8 However, respondents of the present study reported suboptimal awareness in participating in HE/PE decisions at work (38.9%), and not regularly reading articles related to HE/PE (38.6%). These findings are comparable to prior Iranian studies among clinical and managerial nurses,17 and critical care nurses,18 who reported low level of awareness related to HE. Likewise, similar findings from previous study in India indicated insufficient awareness of HE among nurses.19
The above findings discussed regarding registered nurses’ awareness in HE/PE could be explained by presenting the influencing factors. Based on the binary regression analyses, several predictor variables of awareness in HE/PE were identified. For instance, gender served as the first statistically significant predictor for having heard about HE/PE. This indicates that being a female nurse increases the likelihood of having heard about HE/PE in comparison to being a male nurse. Second, the position of registered nurses was also identified as a significant predictor which implies that nurse managers or head nurses have a greater likelihood of being aware of HE/PE in comparison to other nursing positions. Third, attendance in HE/PE course also emerged as a significant predictor suggesting that registered nurses who attended the HE/PE course had nearly five times higher probability of being aware of HE/PE compared to those who did not attend. Fourth, the agreement with the assertion that graduates with a BSN degree need more HE/PE skills than most of them currently have, was also identified as a significant predictor. This finding implies that registered nurses who strongly agreed with the notion that “graduates with a BSN degree need more HE/PE skills than most of them currently have” had a greater probability of being aware of HE/PE than those who strongly disagreed. Fifth, the interest or preference to hire new registered nurses with knowledge and skills in HE/PE emerged as a significant predictor indicating that respondents who expressed interest or preference in hiring new registered nurses with competencies in HE/PE had a twofold increase in the likelihood of being aware of HE/PE in comparison to those who did not show such interest. Furthermore, the binary regression analyses also revealed significant predictors of “being familiar with the term HE/PE.” Gender emerged again as a significant predictor indicating that being a female nurse increases the likelihood of familiar with the term HE/PE in comparison to being a male nurse. In addition, attendance in HE/PE course also emerged as a significant predictor suggesting that registered nurses who attended the HE/PE course had more than three times higher probability of being familiar with the term HE/PE compared to those who did not attend. For considering knowledge of HE/PE to be important in job practice, the highest education was identified as a significant predictor indicating that possessing a diploma in nursing increases the likelihood of considering knowledge of HE/PE to be important in job practice when compared to holding BSN and post-graduate degrees. Also, “having knowledge of HE/PE is valued within the organization” also surfaced as a significant predictor implying that registered nurses who strongly agreed that HE/PE knowledge is valued within the organization had a greater probability of considering HE/PE knowledge to be important in job practice than those who strongly disagreed. Moreover, the “interest or preference to hire new registered nurses with knowledge and skills in HE/PE” also served as a significant predictor. This indicates that respondents who expressed interest or preference in hiring new registered nurses with competencies in HE/PE had more than three times increase in the likelihood of considering HE/PE knowledge to be important in job practice in comparison to those who did not show such interest. Moreover, participation in HE/PE training or workshop was a significant predictor for having read articles related to HE/PE regularly. The result suggests that registered nurses who had HE/PE training or workshop had a threefold higher probability of reading articles related to HE/PE regularly compared to those who did not have such training or workshop. Likewise, participation in HE/PE training or workshop was a significant predictor for registered nurses to participate in HE/PE decisions at work. This finding suggests that registered nurses who had no HE/PE training or workshop had a likelihood of three times higher to participate in HE/PE decisions at work compared to those who had undergone such training or workshop. Lastly, the binary regression results revealed that gender was revealed as a significant predictor for implementing HE/PE techniques to make decisions. This finding indicates that female nurses are more likely to implement HE/PE techniques in decision-making than male nurses. The results could not be compared with prior studies as there has been no previous investigation into these specific aspects of awareness regarding HE/PE, except for gender. A prior study conducted in the United Arab Emirates revealed that male health professionals possess better awareness of HE/PE compared to their female counterparts.20
The study’s findings also revealed that the registered nurses demonstrated an overall low level of knowledge regarding HE/PE (2.39/5). This finding contradicts the HEOR competencies framework established by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR), as registered nurses exhibited suboptimal knowledge regarding HE/PE. The ISPOR emphasizes the necessity for healthcare providers to recognize and define terminology, outline the different categories of economic evaluations, comprehend the circumstances under which an economic evaluation is warranted, and acknowledge the basic principles of quality of life and patient-reported outcome measures.21 These HEOR competencies are also in alignment with the six HE competencies developed by Platt et al22 for BSN programs. The study’s finding implies that registered nurses might be unable to participate in clinical decision-making, manage resources effectively, and deliver cost-efficient care to their patients. Such limitations could lead to poor patient outcomes, increased healthcare expenses for the organization, and lack compliance with healthcare regulations. Furthermore, it may hinder registered nurses’ opportunities for health policy involvement and professional development as well as their capacity to make positive contributions to the healthcare system in the aspects of HE/PE. The finding also suggests that there is a dire necessity to enhance the knowledge of registered nurses regarding HE/PE. This has been echoed in the findings of prior study among health professions students in Jordan, including nursing students.8 This is also consistent with a previous study conducted among nurses in the USA, indicating the importance to improve nurses’ understanding and awareness about the value of HE/PE skills at work.9 However, it indicates a lower level of knowledge regarding HE/PE compared to a prior study conducted in Southwest China which revealed that health professions students possess a moderate level of knowledge about health economics.23
Our position of this finding is that the overall suboptimal knowledge in HE/PE terminologies was influenced by the insufficient awareness among registered nurses, as all six awareness factors exhibited a significant and negative correlation with their level of HE/PE knowledge. Additionally, four out of the six awareness factors were significant predictors of the overall low level of HE/PE knowledge among registered nurses. There are also other influencing factors that should be considered affecting or contributing to the overall low level of HE/PE knowledge among registered nurses. The study’s findings showed that four sociodemographic and HE/PE-related variables were found as significant predictors of knowledge of HE/PE, including having attended HE/PE course, having HE/PE training or workshop, “having knowledge of HE/PE is valued within my organization”, and “graduates with a bachelor’s degree need more HE/PE skills than most of them currently have”. These findings have several practical implications for registered nurses as well as nursing administrators. For instance, encouraging registered nurses to participate in a training course or workshop on HE/PE can enhance their awareness, foster their understanding of HE/PE terminologies, and develop their ability to apply the skills associated with HE/PE. A prior study supports these implications indicating that health professions students who had taken a HE/PE course were more inclined to agree about the role and usefulness of HE/PE as well as report higher level of knowledge regarding HE/PE.8 Likewise, previous research, particularly in the area of HEOR, has substantiated these implications, highlighting the necessity for health professionals to exhibit competence in HE/PE.1
Limitations of the Study
The following limitations must be considered in interpreting the findings of this study. The self-reported nature of registered nurses’ knowledge and awareness regarding HE/PE, combined with the use of a convenience sampling approach, could potentially lead to bias in their responses during the completion of the online survey. Particularly, the possibility of response bias existed as registered nurses with greater or lesser knowledge of HE/PE might have been more inclined to participate in the online survey, which could have potential influence on the results. Therefore, the findings must be treated with caution, as the ratings provided by registered nurses may not accurately reflect the overall knowledge and awareness of HE/PE among registered nurses in different healthcare settings throughout the KSA, including privately managed healthcare institutions. As a result, these limitations restrict the generalizability of the findings from the current study.
Conclusions
The findings of the study revealed that the level of knowledge regarding HE/PE among registered nurses was low. Nevertheless, their awareness was claimed to be acceptable, demonstrating good awareness in four items but suboptimal for the other two items. These findings suggest a need to enhance awareness as well as knowledge of HE/PE among registered nurses. Targeted educational strategies and interventions must be designed and implemented taking into careful consideration the relevant sociodemographic and HE/PE-related predictor variables in enhancing the awareness and knowledge of HE/PE among registered nurses. By fostering awareness and knowledge of HE/PE, the value and competence associated with HE/PE among registered nurses can expand. This, in turn, may contribute to a more cost-effective healthcare delivery system in the KSA.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of King Saud University Medical City with Reference No.: E-25-10157.
Data Sharing Statement
The data presented in this study are all included in the paper.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
Homoud Ibrahim Alanazi would like to thank the Deanship of Scientific Research (DSR) in King Saud University, Riyadh, Saudi Arabia for funding and supporting this research through the initiative of the DSR Graduate Students Research Support (GSRS).
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest.
References
1. Pizzi LT, Onukwugha E, Corey R, Albarmawi H, Murray J. Competencies for professionals in health economics and outcomes research: the ISPOR health economics and outcomes research competencies framework. J Int Society Pharmacoecon Outcomes Res. 2020;23(9):1120–1127. doi:10.1016/j.jval.2020.04.1834
2. Rai M, Goyal R. Chapter 33 - pharmacoeconomics in healthcare. Pharmaceutical Medicine and Translational Clinical Research. Academic Press. 2018;465–472. doi:10.1016/B978-0-12-802103-3.00034-1
3. Makiya N. The crucial role of pharmacoeconomics in healthcare decision-making. Clin Pharmacol Biopharm. 2023;12(9):380. doi:10.4172/2167-065X.1000380
4. Sienko M. The role of pharmacoeconomics in health policy decision-making. Pharmacoeconomics. 2024;9:240. doi:10.37421/2472-1042.2024.9.240
5. Weng C. The significance of pharmacoeconomics: a brief commentary. J Pharm Care Health Syst. 2024;11:312. doi:10.35248/2376-0419.24.11.312
6. Algharibi EDA, Fadel BA, Al-Hanawi MK. Assessment of knowledge of health economics among healthcare professionals in the Kingdom of Saudi Arabia: a cross-sectional study. Healthcare. 2024;12(2):185. doi:10.3390/healthcare12020185
7. Alqahtani MA, Tafyan MM, Aqeeli AI, et al. Awareness, knowledge, and attitude of health professionals towards health economics and pharmacoeconomics education. Indo Am J Pharm Sci. 2021;08(12):129–137. doi:10.5281/zenodo.5783966
8. Hammad EA, Mousa R, Hammad AA, Al-Qudah M. Awareness, knowledge, and attitudes of health professions students toward health economics and pharmacoeconomics education in Jordan. Curr Pharm Teach Learn. 2020;12(9):1072–1080. doi:10.1016/j.cptl.2020.04.027
9. Platt M, Kwasky A, MacDonald DA, Spetz J. Exploring health economics course competencies’ value for nurse administrators. Nurs Outlook. 2019;67(3):270–279. doi:10.1016/j.outlook.2018.11.007
10. Haakenstad A, Bintz C, Knight M, et al. Catastrophic health expenditure during the COVID-19 pandemic in five countries: a time-series analysis. Lancet Glob Health. 2023;11(10):e1629–e1639. doi:10.1016/S2214-109X(23)00330-3
11. Intercontinental medical statistics HEALTH® market research and reports repository. 2020. Available from: https://www.iqvia.com/insights/the-iqvia-institute/available-iqvia-data/ims-health-market-research-and-reports-repository.
12. Shahbaz AA, Hassaniyan A. The growing autonomy for GCC states’ foreign policy and structural changes in the balance of power in the region. Asian J Middle East Islamic Stud. 2024;18(4):321–339. doi:10.1080/25765949.2025.2480007
13. Health Sector Transformation Report. Health sector transformation program. 2024. Available from: https://www.vision2030.gov.sa/en/explore/programs/health-sector-transformation-program.
14. Trevethan R. Deconstructing and assessing knowledge and awareness in public health research. Front Public Health. 2017;5:194. doi:10.3389/fpubh.2017.00194
15. Clark R. Convenience Sample. In: Ritzer G, editor. The Blackwell Encyclopedia of Sociology. 2017. doi:10.1002/9781405165518.wbeosc131.pub2
16. Wilson VanVoorhis CR, Morgan BL. Understanding power and rules of thumb for determining sample sizes. Tutor Quant Methods Psychol. 2007;3(2):43–50. doi:10.20982/tqmp.03.2.p043
17. Heydari A, Mazloom R, Najar AV, Bakhshi M. Awareness and performance of iranian nurses with regard to health economics: a cross-sectional study. North Am J Med Sci. 2015;7:384–389. doi:10.4103/1947-2714.166214
18. Heydari A, Hosseini M. Knowledge, attitude, and practice of ICU nurses in relation to health economics. 2022. Available from: https://www.researchgate.net/publication/364329255_Knowledge_attitude_and_practice_of_ICU_nurses_in_relation_to_health_economics.
19. Dash M, Chitra AF. Knowledge and knowledge on practice of nurses on health economics. J Nurs Sci Pract Res Adv. 2019;1(1):19–23. doi:10.5281/zenodo.2564429
20. Al-Hemyari SS, Noor DAM, El-Dahiyat F. Knowledge, attitude and perception of pharmacists and healthcare professionals about principles and methodology evaluation of pharmacoeconomic in the United Arab Emirates. J Pharm Health Serv Res. 2023;14(2):141–150. doi:10.1093/jphsr/rmad019
21. International Society for Pharmacoeconomics and Outcomes Research. Health Economics and Outcomes Research (HEOR) Competencies Framework. 2025. https://www.ispor.org/strategic-initiatives/more/heor-competencies-framework.
22. Platt M, Kwasky A, Spetz J. Filling the gap: developing health economics competencies for baccalaureate nursing programs. Nurs Outlook. 2016;64(1):49–60. doi:10.1016/j.outlook.2015.10.004
23. Yang J, Wei Q, Yang X, Jiao J, Yang Z, Li F. Assessment and predictive analysis of health professions students’ proficiency in health economics and pharmacoeconomics in Southwest China: a cross-sectional study. BMC Med Educ. 2024;24(1):1239. doi:10.1186/s12909-024-06214-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Caregiver Perspectives on Physiotherapy Treatment for Paediatric Burns in the United Arab Emirates
Mohamed Muftah Alzaabi FS, Bairapareddy KC, Alaparthi GK, Hegazy F
Patient Preference and Adherence 2022, 16:1477-1486
Published Date: 17 June 2022
Knowledge and Awareness of Non-Technical Skills Over the Course of an Educational Program in Nursing - A Repeated Cross-Sectional Study
Wevling A, Olsen BF, Nygaard AM, Heiberg T
Advances in Medical Education and Practice 2023, 14:31-41
Published Date: 10 January 2023
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024
Knowledge, Attitude and Practice Toward Artificial Intelligence Among Healthcare Workers in Private Polyclinics in Jeddah, Saudi Arabia
Serbaya SH, Khan AA, Surbaya SH, Alzahrani SM
Advances in Medical Education and Practice 2024, 15:269-280
Published Date: 5 April 2024
Radiologic Technology Students’ Perceptions on Adoption of Artificial Intelligence Technology in Radiology
Arif WM
International Journal of General Medicine 2024, 17:3129-3136
Published Date: 16 July 2024