Back to Journals » Journal of Pain Research » Volume 18
Auricular Plaster Therapy for Preoperative Anxiety in Major Surgery: A Prospective Matched-Cohort Study of Total Knee Arthroplasty and Pancreaticoduodenectomy Patients
Authors Mi Q, Shao Q, Bao F, Zhao X, Zan D, Liu Y ![]() , Wang W
, Wang W ![]()
Received 9 October 2025
Accepted for publication 12 December 2025
Published 23 December 2025 Volume 2025:18 Pages 6977—6991
DOI https://doi.org/10.2147/JPR.S562267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Qindong Mi,1,* Qianqian Shao,2,* Fei Bao,1 Xiaolong Zhao,3,* Defang Zan,3 Yuhao Liu,4 Weibin Wang2,5
1Department of TCM, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 2Department of General Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 3Department of Orthopedics, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 4School of Population Medicine and Public Health, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, 100730, People’s Republic of China; 5State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fei Bao, Department of TCM, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, No. 1, Shuaifuyuan, Dongcheng District, Beijing, 100730, People’s Republic of China, Email [email protected] Weibin Wang, Department of General Surgery, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 1, Shuaifuyuan, Dongcheng District, Beijing, 100730, People’s Republic of China, Email [email protected]
Objective: To investigate the association of auricular plaster therapy (AP) with preoperative anxiety in patients undergoing total knee arthroplasty (TKA) and pancreaticoduodenectomy (Whipple).
Methods: A prospective matched-cohort observational study was conducted at Peking Union Medical College Hospital from March 2024 to May 2025. The primary outcome was Perioperative Anxiety Scale-7 (PAS-7) scores at different preoperative timepoints. Secondary outcomes included modified Pittsburgh Sleep Quality Index (M-PSQI), satisfaction visual analog scale (VAS-satisfaction), intraoperative blood loss, postoperative VAS-pain scores, Self-Rating Anxiety Scale (SAS) scores, and incidence of delirium.
Results: A total of 168 patients completed the study, and 98 patients (49 matched pairs) were included in the final analysis. The results revealed that auricular plaster (AP) therapy was significantly associated with reduced preoperative anxiety scores. Specifically, the AP exposed group demonstrated substantially lower median PAS-7 scores at both 12± 2 hours before surgery (T2) and 2 hours before surgery (T3), with median differences of − 4.00 points and − 5.00 points, respectively (both p < 0.001). Generalized Estimating Equations further confirmed a significant group × time interaction effect (Wald χ2 = 44.73, p < 0.001), indicating a favorable association between AP therapy and attenuated anxiety progression. Similarly, AP therapy was significantly associated with improved perioperative sleep quality. The AP exposed group showed superior M-PSQI scores at T2 and at 72± 2 hours postoperatively (T4), with a median difference of − 4.00 points at T2 and a mean difference of − 3.27 points at T4 (both p < 0.001). This was supported by a significant cumulative trend (Wald χ2 = 30.44, p < 0.001). Furthermore, the AP exposed group was associated with more favorable postoperative outcomes, including significantly lower VAS pain scores (mean difference: − 1.00, p < 0.001) and SAS scores (mean difference: − 4.02, p = 0.012). Multivariable regression identified treatment allocation as a key predictor of PAS-7 scores, with the model demonstrating moderate goodness-of-fit (adjusted R2 = 0.50). No significant associations were observed between AP therapy and intraoperative blood loss, postoperative length of stay, or incidence of delirium. The AP exposed group exhibited a lower incidence of adverse events (10.2% vs 16.4%), with only three cases of mild local reactions reported, suggesting an acceptable safety profile.
Conclusion: In this observational study, AP was associated with reduced preoperative anxiety and improved sleep quality and may contribute to optimized postoperative recovery through its cumulative effects. Larger randomized controlled trials are needed to establish causality.
Keywords: preoperative anxiety, auriculotherapy, total knee arthroplasty, whipple, ERAS
Introduction
Preoperative anxiety (PA) is a common psychological stress response among surgical patients during the perioperative period. A multicenter study conducted in China reported a prevalence of 15.8% (95% CI: 14.8–16.9%),1 whereas the global prevalence is significantly higher at 48% (95% CI: 39–47%).2 It typically presents as multifaceted concerns regarding disease prognosis, anesthesia, surgical risks, pain, and perceived loss of control.3,4 Clinical evidence links PA to increased anesthetic and analgesic requirements, hemodynamic instability, prolonged recovery, heightened postoperative pain, extended hospital stays, and reduced patient satisfaction.5–8 In high-risk populations, severe PA may further elevate the risks of delirium and postoperative mortality, contributing to additional healthcare burdens.9–11 Total knee arthroplasty (TKA) and pancreaticoduodenectomy (Whipple) are both classified as major surgeries (Grade IV in the Chinese surgical classification) and are associated with significant technical complexity, procedural risk, and resource utilization.12 Patients undergoing these interventions often experience considerable PA, which may in turn worsen clinical outcomes. Current management of PA primarily involves pharmacologic sedatives and preoperative education. However, the safety and efficacy profile of sedatives remains uncertain,13 underscoring the importance of developing non-pharmacological alternatives.
Auricular plaster therapy (AP), a non-invasive modality derived from auricular acupuncture, involves the application of stimulants such as Vaccaria seeds, magnetic beads, or medicated patches to specific auricular points. Periodic manual stimulation of these points is thought to modulate physiological functions.14 Unlike needle-based acupuncture, AP is needle-free, enhancing its safety and feasibility in clinical settings. It also allows for more precise and sustained acupoint stimulation compared to acupressure, while enabling self-administration—features that may improve patient accessibility and adherence. These advantages support its applicability across various clinical scenarios.15–17 Although TKA and Whipple procedure belong to different surgical specialties (orthopedics and general surgery, respectively), both are major operations that can induce significant perioperative psychological stress.18,19 Including these two cohorts allows a preliminary assessment of the potential generalizability of AP across different surgical contexts. While previous studies have suggested a potential benefit of AP in reducing PA,20–22 most of the available evidence comes from retrospective studies with methodological limitations, highlighting the need for more rigorous prospective evaluations. To fill this gap examine the association between AP and PA, we conducted a prospective observational cohort study employing a matched-comparison design in patients undergoing TKA or Whipple.
Materials and Methods
Study Design
This prospective observational cohort study with matched comparison was conducted in accordance with the Declaration of Helsinki among participants from the Departments of Orthopedics and General Surgery. It received ethical approval from the Institutional Review Board of Peking Union Medical College Hospital in March 2024 and July 2024 (approval nos. I-24PJ0652/I-24PJ1454) and was prospectively registered at ClinicalTrials.gov (registration nos. NCT06273488/NCT06580197). This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement,23 and the reporting of the AP intervention adheres to the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA).24
Study Setting
This study was conducted between March 2024 and May 2025 in the Departments of Orthopedics and General Surgery at Peking Union Medical College Hospital and enrolled patients scheduled for TKA or Whipple procedure. Exposure factors were ascertained via clinical visits, electronic medical records, and telephone follow-up, with the final follow-up of all participants completed in June 2025.
Participants
The inclusion and exclusion criteria were defined separately for each surgical specialty-orthopedics and general surgery-as follows.
Orthopedics Inclusion criteria: (1) Aged 40–80 years, either sex. (2) Scheduled to undergo primary total knee arthroplasty (TKA) for knee osteoarthritis after standard preoperative evaluation. (3) American Society of Anesthesiologists (ASA) physical status class I or II. (4) Participant able to comprehend the study objectives (independently or, in cases of limited literacy or comprehension due to linguistic or educational barriers, with the assistance of a legal guardian/representative), exhibits adequate protocol adherence, and signs the Informed Consent Form (ICF) (or, upon the participant’s explicit request and for the reasons stated above, has the ICF signed by their legal guardian/representative). Orthopedics Exclusion criteria: (1) Emergency surgery without preoperative assessment. (2) TKA contraindications, documented psychiatric disorders, alcohol abuse, substance-use disorder, or history of vestibular dysfunction, Parkinson’s disease, multiple sclerosis, or muscular dystrophy. (3) Bilateral auricular lesions (eg, breakage, erythema, bleeding, infection) precluding auricular plaster therapy. (4) Cognitive impairment preventing comprehension of study requirements or adequate cooperation. (5) Any other condition deemed by the investigator to render the patient unsuitable for participation.
General Surgery Inclusion criteria: (1) Aged 40–80 years, either sex. (2) Scheduled to undergo pancreaticoduodenectomy (Whipple procedure) for malignant neoplasms of the pancreatic head, periampullary region, or distal bile duct after standard preoperative evaluation. (3) American Society of Anesthesiologists (ASA) physical status class I or II. (4) Participant able to comprehend the study objectives (independently or, in cases of limited literacy or comprehension due to linguistic or educational barriers, with the assistance of a legal guardian/representative), exhibits adequate protocol adherence, and signs the ICF (or, upon the participant’s explicit request and for the reasons stated above, has the ICF signed by their legal guardian/representative). General Surgery Exclusion criteria: (1) Emergency surgery without preoperative assessment. (2) Contraindications to pancreaticoduodenectomy, documented psychiatric disorders, alcohol abuse, substance-use disorder, or history of vestibular dysfunction, Parkinson’s disease, multiple sclerosis, or muscular dystrophy. (3) Bilateral auricular lesions (eg, breakage, erythema, bleeding, infection) precluding auricular plaster therapy. (4) Cognitive impairment preventing adequate understanding of study requirements or cooperation. (5) Any other condition that, in the opinion of the investigator, renders the patient unsuitable for participation.
Cohort Determination and Auricular Plaster Therapy Protocol
Upon admission, researchers approached eligible patients, provided detailed explanations of the study protocol, and obtained written informed consent from all participants or their legal guardians. All auricular plaster therapy was administered strictly on a voluntary basis and only after securing clinical approval. Based on the naturally formed exposure status to auricular plaster therapy within the actual clinical setting, participants from the orthopedic and general surgery departments were categorized into two groups: (1) the exposed group: patients scheduled for surgery who actually received auricular plaster therapy; and (2) the non-exposed group: patients scheduled for surgery who did not receive auricular plaster therapy. All auricular plaster interventions in this study were provided free of charge, with costs funded by the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences and the Peking Union Medical College Hospital Scientific Research Endowment.
All participants received routine preoperative education; the exposed group additionally underwent standardized auricular plaster therapy (AP) commencing four days before surgery (first visit) according to the operative schedule. The selected auricular acupoints were Shenmen (TF4), Sympathetic (AH6a), Brainstem (AT3, 4i), Occiput (AT3), Heart (CO15), Liver (CO12), Kidney (CO10), Sanjiao (CO17), and Subcortex (AT4). Procedures strictly adhered to the Chinese national standards “Nomenclature and Location of Auricular Points” (GB/T 13734–2008) and “Standardized Manipulations of Acupuncture and Moxibustion-Part 3: Auricular Acupuncture” (GB/T 21709.3–2021). Bilateral auricular plastering was performed using Vaccaria-seed adhesive patches (Beijing Zhongyan Taihe Medical Device Co., Ltd.) and maintained for 4 consecutive days, with all patches removed at a uniform time on the day before surgery. During the intervention period, nurses instructed participants to perform self-pressing three times daily for one minute each session (additional pressing was permitted when surgery-related worry arose) and monitored patch adherence; any loosened patches were promptly re-secured by clinical staff to ensure protocol compliance. Figure 1 illustrates the anatomical locations of the auricular acupoints.
 |
Figure 1 Primary auricular acupoint locations for Plaster Patches. Notes: The acupoint is located on the inner wall of the auricle; The acupoint is located on the surface of the auricle. |
Outcome Measures
Before conducting the outcome measurements, all participants had been informed of the “Participant Instructions for Self-Report Scale Assessment”. (Supplementary Material- Box S1).
Primary outcome: Preoperative anxiety was assessed with the Perioperative Anxiety Scale-7 (PAS-7), which recent evidence indicates outperforms the Amsterdam Preoperative Anxiety and Information Scale (APAIS) in Chinese surgical populations (ROC: 0.808 vs 0.674)25 PAS-7 scores were collected at three prespecified time points: 24±2h after the start of AP or first visit (T1), 12±2h before surgery (T2), and 2 h before surgery (T3). The PAS-7 scores at these consecutive time points served as the primary outcome measure to evaluate the efficacy of AP. The content of the PAS-7 scale can be found in Supplementary Material-Table S1.
Secondary outcomes were as follows: (1) Sleep quality was assessed using the modified Pittsburgh Sleep Quality Index (M-PSQI), a structured instrument adapted for profiling sleep quality in the inpatient surgical context. Assessments were conducted at T1, T2, and T4 (72±2 hours postoperatively). The adaptation process and its consideration of the instrument’s multidimensional structure are detailed in the Supplementary Material- Tables S2 and S3. (2) Patient satisfaction with pre-operative preparation assessed with the visual analogue scale (VAS-Satisfaction) at T3, (Supplementary Material- Box S2 and Figure S1); (3) Intra-operative blood loss (mL); (4) Incidence of AP-related adverse events, including auricular skin lesions, infection, pain, or dizziness; (5) Pain intensity and anxiety measured at T4 using the visual analogue scale for pain (VAS-Pain) and the Self-Rating Anxiety Scale (SAS), (Supplementary Material- Box S3, Figure S2 and Table S4); (6) Post-operative length of stay (days); (7) Delirium within T4, determined with the Confusion Assessment Method (CAM), (Supplementary Material- Box S4); (8) Anxiety- or depression-related adverse events (eg, falls, self-harm, non-adherence) occurring within one month after surgery. Figure 2 illustrates the temporal design for outcome measures assessment.
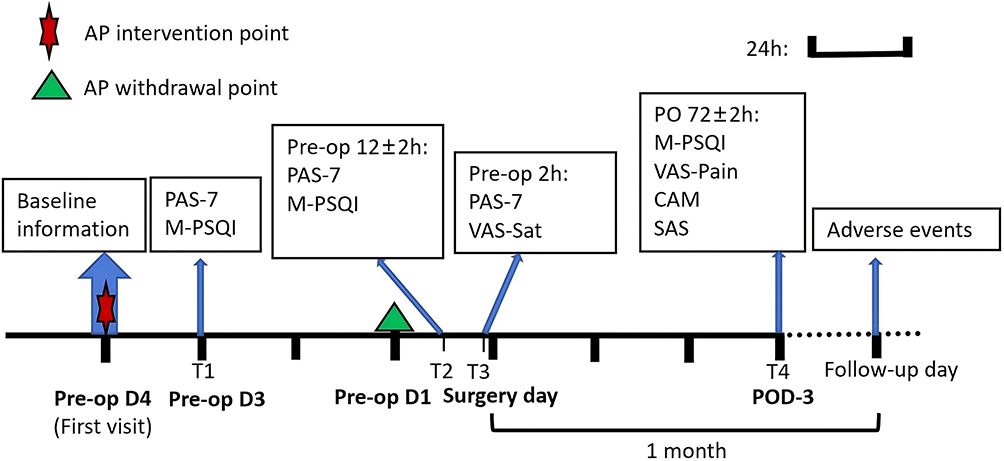 |
Figure 2 Temporal Design for Outcome Measures Assessment. |
Potential Biases
To minimize potential bias, the study employed a rigorous design in which both outcome assessors were blinded to group allocation. Patient screening and enrolment were conducted by six surgical teams (three orthopedic and three general surgery teams), each with more than 15 years of experience in the relevant fields. All participants or their legal guardians provided written ICF before surgery and pledged to maintain the confidentiality of their group assignment. An independent, blinded assessment team-comprising experienced perioperative professionals not involved in treatment decisions-was responsible for collecting and measuring all clinical data using standardized instruments and uniform procedures to ensure objectivity. However, due to the nature of the auricular intervention, complete blinding of patients and practitioners was not feasible. This limitation and its potential impact on subjective patient-reported outcomes are explicitly addressed in the Discussion section.
Integrity of blinding was monitored by a blinded assessor who conducted monthly unmasking evaluations; assessors’ accuracy in guessing group allocation was required not to exceed the 50% chance level. All study data were managed under hierarchical access controls, and statistical analyses were performed by an independent data team. Any unblinding had to be pre-approved by the principal investigator and was fully documented.
Sample Size Calculation
The sample size estimation was based on a preliminary analysis of 20 pilot cases (14 TKA, 6 Whipple) who received preoperative auricular plaster therapy (AP) between January and May 2024. These patients were propensity score-matched 1:1 with 20 concurrent control patients by surgical type, age, sex, education, occupation, residence, and prior surgical history. The AP group showed a mean PAS-7 score of 8.9 (±5.1), compared to 11.9 (±3.6) in the non-AP group. Using these parameters (α = 0.05, power = 0.90, allocation ratio 1:1), a minimum of 92 participants per group was required.
To ensure sufficient statistical power after accounting for potential matching failure, loss to follow-up, and attrition—common in observational matched-cohort designs—we planned to enroll at least 184 participants (92 per group) in the initial cohort.
Statistical Analysis
Throughout the trial, research staff documented the reasons for missing data at every stage to classify the missing-data mechanism. Appropriate remedial actions were then implemented as follows: listwise deletion for data assumed missing completely at random (MCAR) with <5% missingness; regression imputation for data missing at random (MAR) with <5% missingness; multiple imputation for variables with 5–30% missingness; and exclusion of variables with >30% missingness.
All analyses were conducted in SPSS 27.0. First, we ensured balanced case numbers between exposed and non-exposed participants within each surgical specialty. Propensity-score matching (PSM) was subsequently performed using 1:1 nearest-neighbour matching with a caliper width of 0.02 to control confounding; each participant was matched only once and pairs were fixed after matching. Post-matching, continuous primary outcomes were analysed with multivariable linear regression. Normality was assessed with the Kolmogorov–Smirnov test: normally distributed data were compared using independent-sample t-tests, non-normally distributed data with the Mann–Whitney U-test, categorical variables with χ2 tests, and repeated-measure outcomes with generalised estimating equations (GEE). A two-sided p-value <0.05 was considered statistically significant.
Additionally, To assess the consistency of AP effects across surgical disciplines, prespecified subgroup analyses were performed for the primary outcome (PAS-7 scores) by surgery type (TKA vs Whipple), with interaction terms tested in the regression models. To assess the robustness of our primary findings regarding the association between AP and perioperative outcomes, we performed a sensitivity analysis focused on the propensity score matching procedure. We tested the stability of our results by repeating the matching and primary analysis using alternative caliper widths of 0.01 and 0.05 (in addition to the primary caliper of 0.02). This approach evaluates whether our conclusions were sensitive to the specific stringency of the matching criteria.
Results
Baseline Characteristics
During the recruitment period, 227 patients (orthopedics n = 139; general surgery n = 88) scheduled for total knee arthroplasty, pancreaticoduodenectomy (Whipple procedure), distal pancreatectomy, or subtotal gastrectomy were screened. Of these, 212 individuals (orthopedics n = 136; general surgery n = 88) met the eligibility criteria, and all participants or their legal guardians provided written ICF; 12 were subsequently excluded after further application of the exclusion criteria, resulting in 200 participants enrolled (orthopedics n = 130; general surgery n = 70). Twenty-four participants were lost to follow-up or withdrew during the study, leaving 168 completers (orthopedics n = 111; general surgery n = 57). Propensity-score matching (PSM) was performed within each surgical cohort, yielding 49 well-matched pairs (general surgery 15 pairs; orthopedics 34 pairs; total n = 98) (Figure 3). Baseline comparison of the matched cohorts revealed no significant differences in age, sex, or body-mass index (BMI) (Table 1), confirming satisfactory balance.
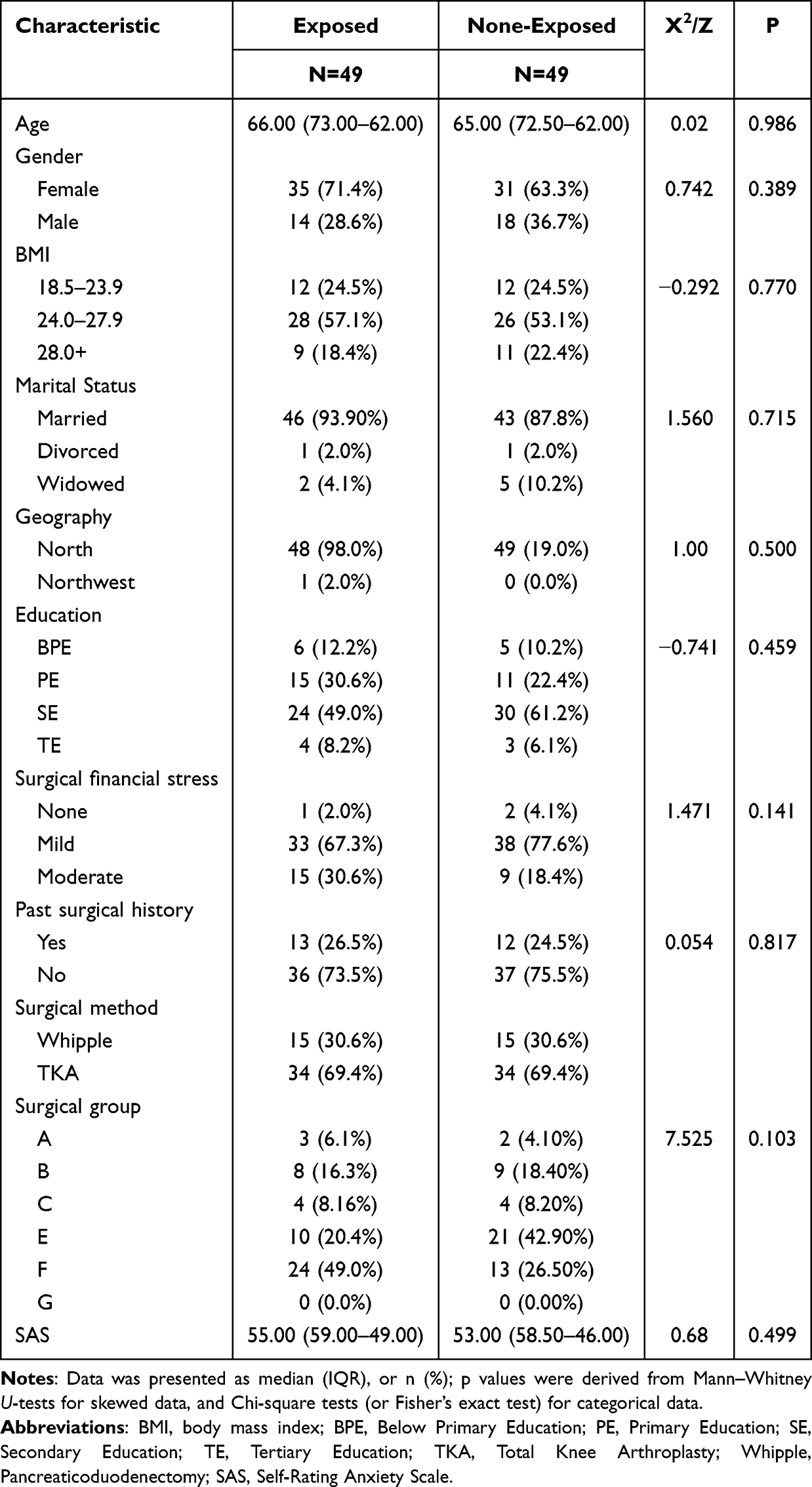 |
Table 1 Demographics and Baseline Characteristics |
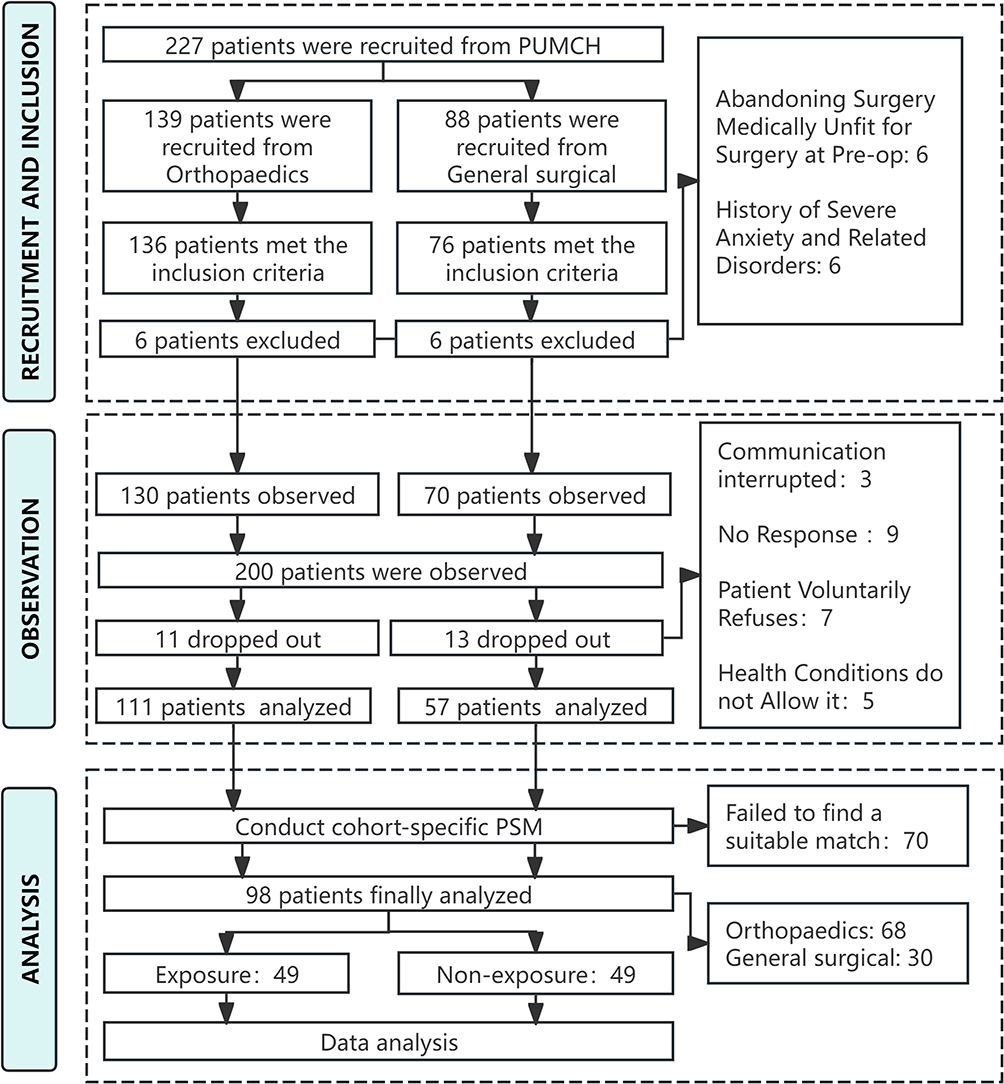 |
Figure 3 Flowchart of Data Screening Process. |
Multivariate Analysis
Multivariable regression analysis incorporating age, sex, and other relevant covariates identified the principal determinants of PAS-7 scores at T2. The results showed that treatment allocation (exposed vs non-exposed) and surgical method (TKA vs Whipple) were significant predictors of PAS-7 at T2 (P < 0.05), a relationship that is illustrated graphically in Figure 4. The model demonstrated moderate goodness of fit (adjusted R2 = 0.50), indicating that it partially explains the variance in PAS-7 scores (Table 2).
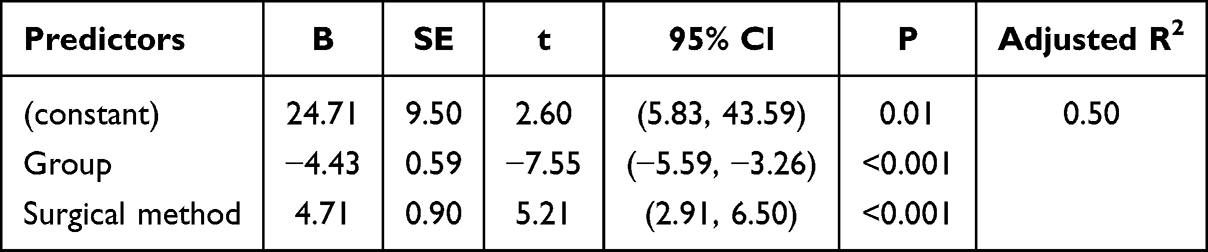 |
Table 2 Regression Analysis Results for Predictors of PAS-7(T2) |
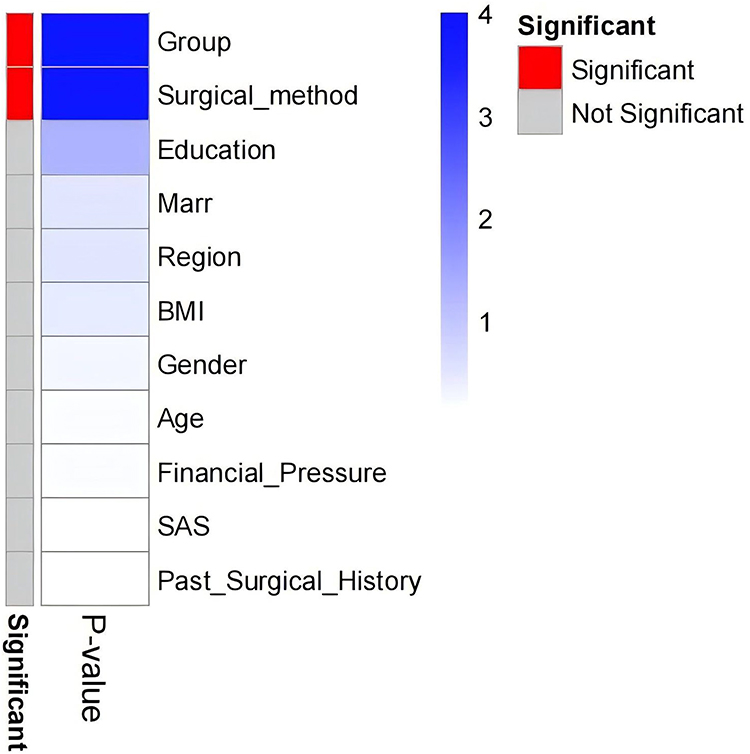 |
Figure 4 Significant predictor of PAS-7(T2). |
Comparison of Primary and Secondary Outcomes
In terms of PAS-7 scores, no significant between-group difference was observed at T1 (median both 4.00, P = 0.874); however, at T2 and immediately pre-operatively (T3), the exposed group exhibited markedly lower scores than the non-exposed group (T2: 7.00 vs 11.00, median difference –4.00, 95% CI [–5.00, –3.00], P < 0.001; T3: 8.00 vs 13.00, median difference –5.00, 95% CI [–6.00, –3.00], P < 0.001). Similarly, M-PSQI scores did not differ at T1 (9.00 vs 10.00, P = 0.113), whereas the exposed group showed significantly better sleep quality at both T2 (8.00 vs 13.00, median difference –4.00, 95% CI [–5.00, –3.00], P < 0.001) and T4 (11.51 ± 2.15 vs 14.78 ± 2.50, mean difference –3.27, 95% CI [–4.20, –2.33], P < 0.001). At T4, post-operative VAS-pain and SAS scores were more favorable in the exposed group (VAS-pain: 5.03 ± 1.05 vs 5.98 ± 1.20, mean difference –1.00, 95% CI [–1.50, –0.50], P < 0.001; SAS: 53.16 ± 6.56 vs 57.18 ± 8.79, mean difference –4.02, 95% CI [–7.13, –0.91], P = 0.012). No inter-group differences were detected for pre-operative VAS-satisfaction, intra-operative blood loss, or post-operative length of stay (all P > 0.05), and no participant in either group was adjudicated to have post-operative delirium between surgery and T4. Auricular-plaster-related adverse events in the exposed group consisted of mild local itching in one patient and mild local pain in two patients; all three individuals reported the symptoms but neither withdrew nor were lost to follow-up. The overall incidence of adverse events during follow-up was lower in the exposed group (10.2% vs 16.4%), although this difference did not reach statistical significance (P = 0.347) (Table 3). Psychometric evaluation of the M-PSQI at T2 revealed a Cronbach’s alpha of 0.460. Item analysis indicated a distinct “Daytime Dysfunction” component; its removal yielded a higher alpha of 0.550 for the core sleep items. Details are in Supplementary Material- Table S5.
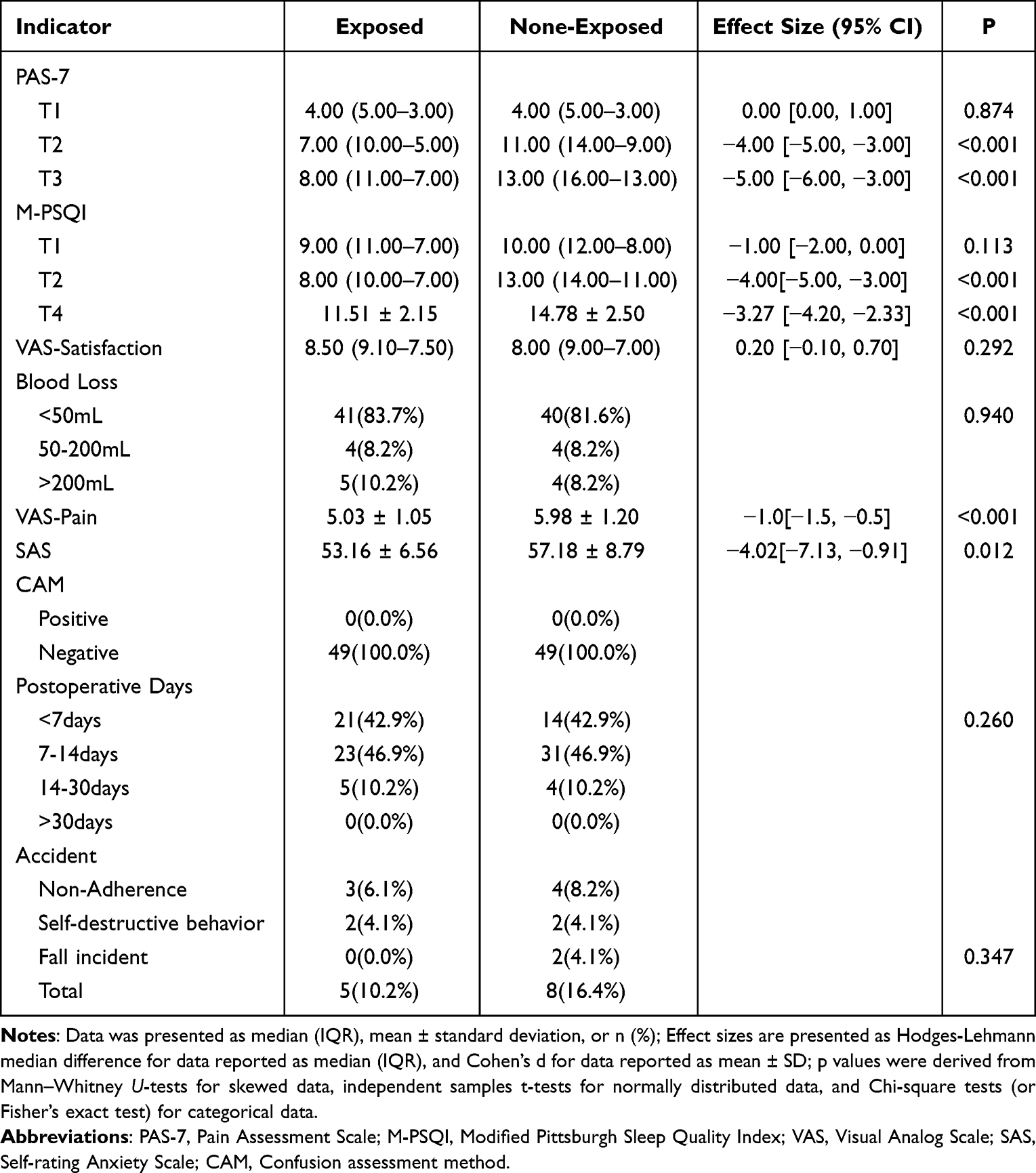 |
Table 3 Comparison of Outcomes Between Exposed and Non-Exposed Groups |
Generalized Estimating Equations (GEE) Analysis
To comprehensively evaluate the association between ear patch (AP) therapy and the dynamic changes in preoperative anxiety and sleep quality, we used the generalized estimating equation (GEE) method. The detailed parameter estimates are provided in Table 4. Analysis of anxiety scores revealed significant main effects of time (Wald χ2 = 452.28, P < 0.001) and group × time interaction (Wald χ2 = 44.73, P < 0.001). As shown in the upper part of Table 4, PAS-7 scores in the non-exposed group increased significantly as surgery approached. The exposed group, however, showed a significantly attenuated increase in anxiety, with between-group differences of −3.57 points at T2 and −4.49 points at T3 compared to the non-exposed group, indicating that the exposed group maintained relatively stable anxiety levels throughout the preoperative period (Figure 5A).
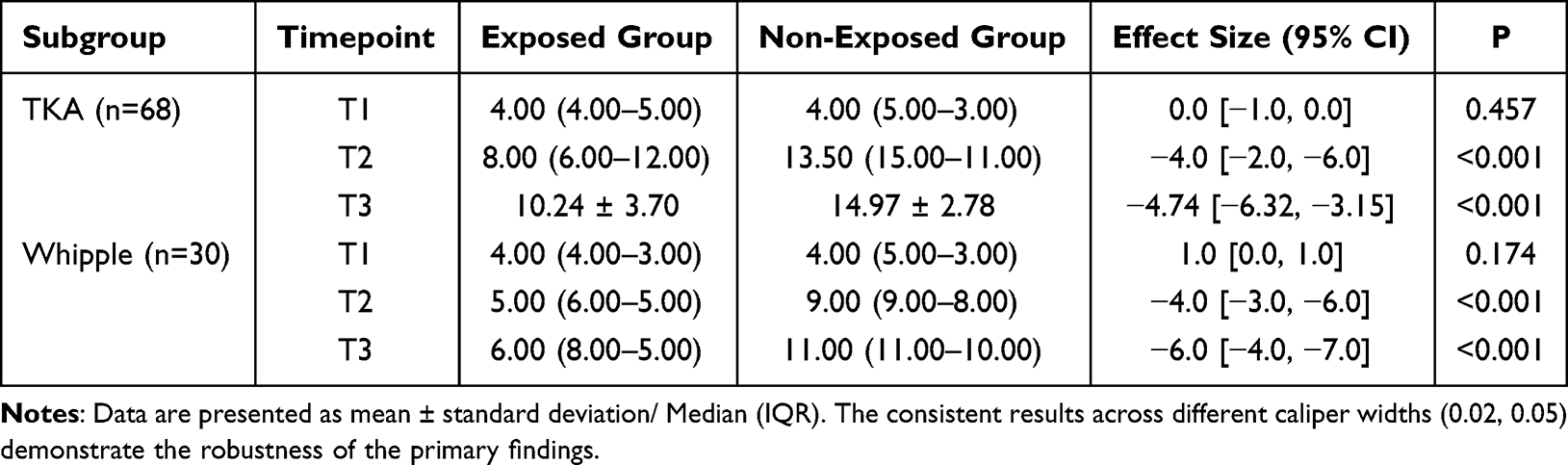 |
Table 4 Consistent Association Between Auricular Plaster Therapy and PAS-7 Score Reduction Across Surgical Subgroups |
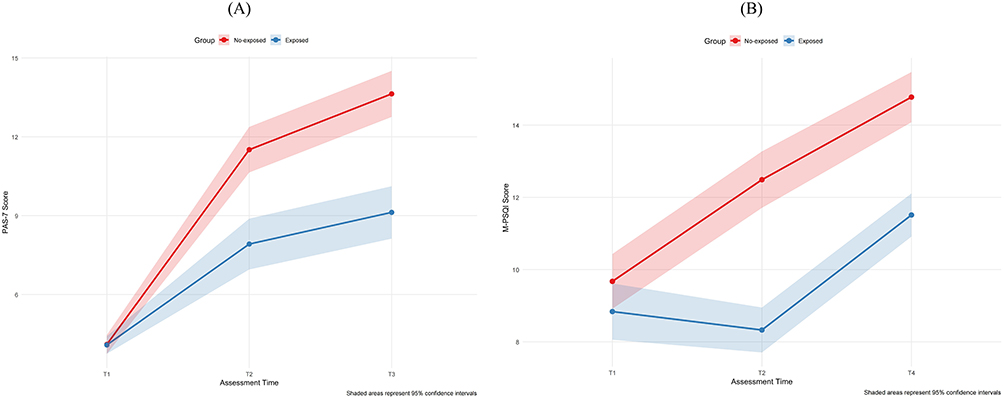 |
Figure 5 Trajectories of preoperative Anxiety and Sleep Quality Changes Across Study Time Points. Notes: (A) Trajectory of PAS-7. (B) Trajectory of M-PSQI; Higher scores indicate high preoperative anxiety or poorer sleep quality. |
Similarly, analysis of sleep quality showed significant main effects of time (Wald χ2 = 288.70, P <0.001) and a group × time interaction (Wald χ2 = 30.44, P <0.001). As detailed in the lower part of Table 4, M-PSQI scores (where higher scores indicate poorer sleep quality) worsened significantly over the perioperative period in the non-exposed group. The deterioration in sleep quality was significantly less pronounced in the exposed group, with between-group differences of −3.33 points at T2 and −2.43 points at T4, demonstrating that AP exposure was associated with improved perioperative sleep quality and may exerts a sustained, cumulative influence on post-operative sleep outcomes. (Figure 5B).
Subgroup and Sensitivity Analyses
A prespecified subgroup analysis was conducted to evaluate the consistency of auricular plaster therapy (AP) effects across the two surgical populations. As summarized in Table 4, the analysis revealed that while no significant between-group differences were observed at T1, AP demonstrated statistically significant associations with reduced PAS-7 scores in both the TKA and Whipple subgroups at T2 and T3 (all P <0.001). The results across all timepoints were consistent with the overall dataset. Furthermore, no significant subgroup-by-treatment interaction was found (χ2 = 0.0001, P for interaction = 0.993), indicating that the magnitude of the association between AP and anxiety improvement was comparable between the two surgical types.
Given the absence of missing data for the primary outcome measures in the matched cohort, no sensitivity analysis was conducted for this aspect. However, sensitivity analyses using different propensity score matching parameters confirmed the robustness of the main study findings. The association between auricular acupressure therapy and improved clinical outcomes remained substantially consistent when the propensity score matching parameters were altered. When a stricter caliper value of 0.01 was applied, the reduction in PAS-7 scores in the exposure group at T2 and T3 time points remained statistically significant (P < 0.001). Similarly, comparable results were obtained using a more lenient caliper value of 0.05 (P < 0.001). Neither strategy showed significant differences at the T1 time point (Table 5). These effect sizes were highly consistent with the results of the primary analysis using a caliper value of 0.02.
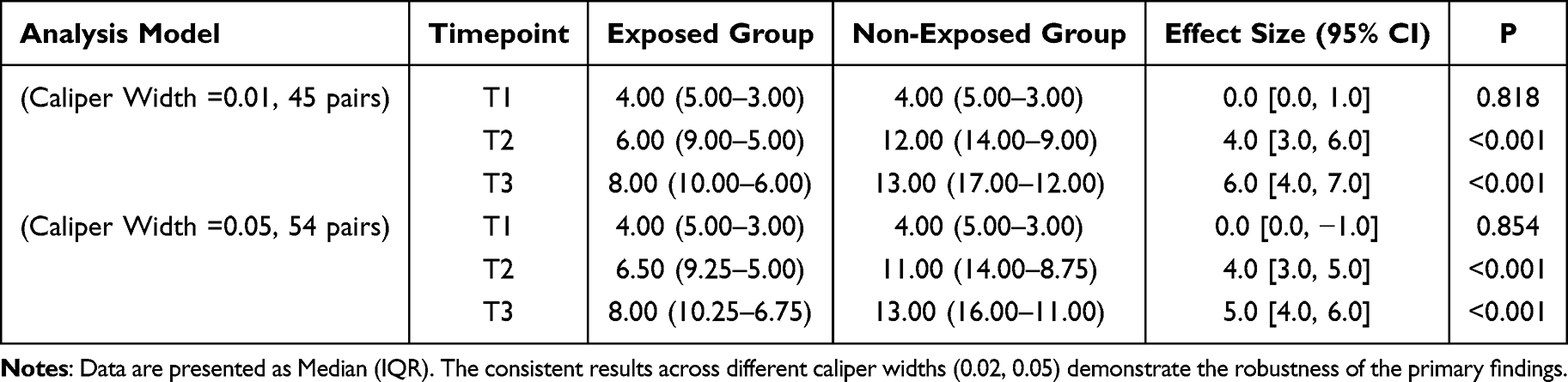 |
Table 5 Sensitivity Analysis of PAS-7 Using Different Propensity Score Matching Calipers |
Discussion
This prospective, observational cohort study with matched comparison in orthopedics and general surgery screened 227 patients and ultimately evaluated 98 matched pairs to examine the association between auricular plaster therapy (AP) on pre-operative anxiety. The findings demonstrate that AP was associated with significant improvements in both pre-operative anxiety and sleep quality, a result consistent with earlier meta-analyses and clinical reports on auricular interventions. It must be acknowledged, however, that prior trials were hampered by very low evidence quality.26 It should be noted that most previous studies were limited by retrospective designs and methodological constraints. In contrast, the present investigation provides a methodologically robust, prospective dataset that adopted a standardized design, reported the intervention in accordance with STRICTA guidelines, balanced baseline characteristics with propensity-score matching, and evaluated associations through multivariable modelling and trend analyses. This study thus contributes higher-quality observational evidence for the potential role of AP in managing pre-operative anxiety.
Total knee arthroplasty (TKA) and pancreaticoduodenectomy (Whipple) are complex, resource-intensive procedures commonly performed in orthopedic and general surgery departments; the substantial psychological and financial burden they impose frequently precipitates more severe pre-operative anxiety. Although pre-operative anxiety is recognized as an independent risk factor that adversely affects peri-operative outcomes and long-term prognosis,27 its systematic assessment and management regrettably remain absent from routine care pathways for these operations.28 In recent years, non-pharmacological interventions-primarily cognitive-behavioural strategies and pre-operative education-have been investigated,29–31 yet their efficacy has been modest32 and the interventions are difficult to integrate synergistically. This study suggests that AP therapy demonstrates significant associations with anxiety alleviation and sleep quality improvement. Although no statistically significant between-group differences in PAS-7 and M-PSQI scores were detected two hours post-intervention (T1) (Table 3), This therapy was significantly associated with reduced anxiety levels at the immediate preoperative time point (T3), and it closely related to improved sleep quality in the postoperative phase (T4) (Table 3), and may exerts a sustained, cumulative influence on post-operative sleep outcomes. (Table 6 and Figure 5B). These findings collectively support the potential clinical value of AP therapy. Therefore, AP therapy not only provides a safe and non-invasive alternative for preoperative anxiety management, but also demonstrates synergistic potential for developing multimodal intervention protocols with non-pharmacological approaches such as music therapy and virtual reality technology, thereby establishing a practical pathway toward enhancing comprehensive efficacy in preoperative anxiety management.
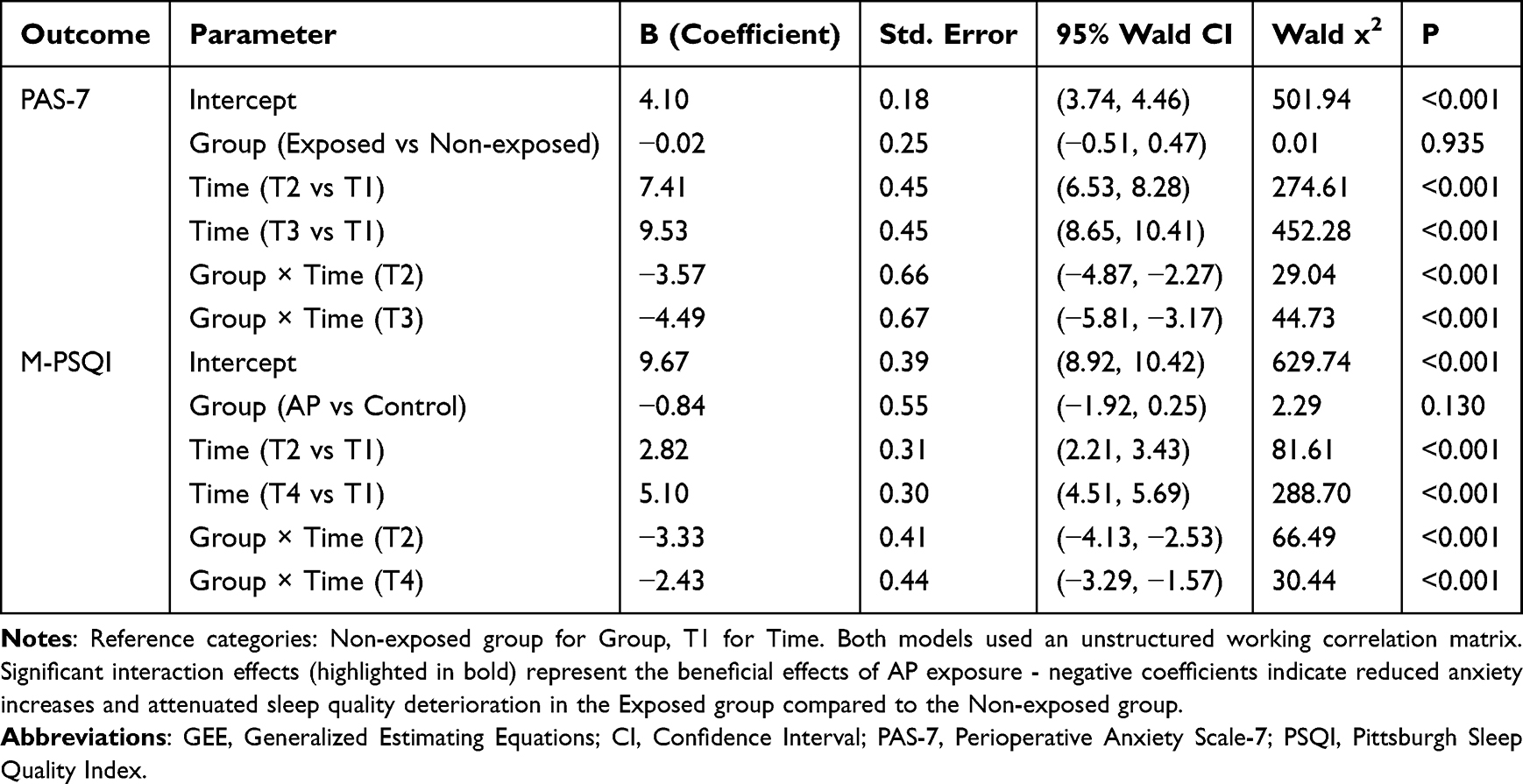 |
Table 6 Results of GEE Analysis for Time, Group, and Time-by-Group Interaction Effects |
The precise mechanisms by which AP therapy alleviates pre-operative anxiety remain to be fully elucidated; however, emerging evidence has begun to delineate its potential pathways. The acupoints selected in this study-Shenmen (TF4), Sympathetic (AH6a), Brainstem, Occiput (AT3), Heart (CO15), Liver (CO12), Kidney (CO10), Sanjiao (CO17), and Subcortex (AT4)-are situated within the overlapping territories of the auricular branches of the vagus (ABVN), trigeminal, and cervical plexus nerves.33 AP may therefore modulate activity in key stress-responsive brain regions through the synergistic action of the ABVN and other cranial nerves. Functional magnetic resonance imaging studies have identified functional connectivity of the putamen, globus pallidus, thalamus, angular gyrus, and inferior occipital gyrus as critical biomarkers predicting the therapeutic efficacy of transcutaneous auricular vagus nerve stimulation (taVNS).34,35 These cerebral areas participate in the regulation of anxiety, sleep, and mood via multiple neurotransmitters-including serotonin, dopamine, norepinephrine, GABA, and glutamate-that represent pharmacological targets of anxiolytic medications36–38 Notably, It is noteworthy that this study observed that the exposure effect of auricular acupressure showed a time-accumulated association, which is consistent with the hypothesis that acupoint stimulation can induce neural plasticity.39 We postulate that sustained AP may drive adaptive remodeling of relevant neural circuits, thereby persistently altering the functional activity and signaling patterns of key brain regions and ultimately producing enduring clinical benefits; this proposition, however, requires further clinical and mechanistic validation.
Limitations of the Study
Given the prospective observational design of this study, which aimed to evaluate the associations between AP therapy and preoperative anxiety along with multiple perioperative outcomes, several limitations should be acknowledged when interpreting the findings. First, as a single-center prospective cohort study conducted in a renowned tertiary academic hospital, our findings may be influenced by the specific medical infrastructure, surgical expertise, and patient demographics. The standardized protocols and high patient adherence, while strengthening internal validity, may limit the generalizability of our findings to primary-care settings or regions with different resources. Furthermore, the exclusion of patients with documented psychiatric histories, a decision made to control for confounding, may lead to an underestimation of the intervention’s effect in this high-risk population, which often experiences heightened preoperative anxiety. Second, the observational nature of this study introduces potential biases. The decision to receive AP was based on patient preference, introducing possible selection bias. Although propensity-score matching was used to balance known covariates, residual confounding from unmeasured factors cannot be entirely excluded. Third, the nature of auricular plaster therapy prevents blinding of patients and practitioners, potentially introducing bias in assessing subjective outcomes. More importantly, the required physical contact inherently generates placebo effects through therapeutic attention and tactile stimulation. While these nonspecific effects may enhance subjective symptom relief, they complicate the distinction between specific treatment effects and placebo responses. Fourth, this study lacked objective biomarker data (eg, heart rate variability, salivary cortisol) or neuroimaging to elucidate the biological mechanisms underlying the observed clinical benefits. While our discussion posits plausible pathways involving the auricular vagus nerve and neuroplasticity, based on extant literature, these hypotheses require direct validation in future trials designed with integrated mechanistic evaluations. Finally, while multiple comparisons were performed for a comprehensive outcome analysis, this increases the risk of Type I error; these findings should thus be interpreted as generating hypotheses. The four-day intervention period and 30-day follow-up, though informative for acute perioperative effects, preclude assessment of longer-term efficacy and sustainability.
Looking forward, the success of multi-modal prognostic models in fields like neuro-oncology provides a compelling roadmap.40 Future research on AP therapy could similarly integrate physiological biomarkers with clinical outcomes to elucidate mechanisms and personalize treatment strategies. Future directions should include rigorously designed multicenter RCTs that specifically incorporate sham AP or other control groups to disentangle the specific effects of AP from the potent contextual and placebo effects inherent to this intervention. Such studies, employing diverse patient populations, longer follow-up, and biomarker endpoints, are crucial to confirm efficacy, establish causality, and unravel the underlying mechanisms.
Conclusion
In summary, this prospective observational study suggests that auricular plaster therapy (AP) was associated with reduced preoperative anxiety and improved sleep quality in patients undergoing major surgery, with potential benefits extending to short-term postoperative outcomes. These preliminary findings indicate that AP could be considered as a potential non-pharmacological adjunct in perioperative care. This methodologically standardized investigation provides a foundation for future research, though larger, multicenter randomized controlled trials are needed to verify these observed associations and further evaluate the intervention’s efficacy.
Data Sharing Statement
The individual deidentified participant data underlying the results reported in this article will not be publicly shared due to restrictions imposed by the ethical review board/privacy laws. However, the data can be made available to qualified researchers upon reasonable request. Proposals for data access should be directed to the corresponding author. All requests will be reviewed and must be approved by the Ethics Committee of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences.
Ethical Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. This study received ethical approval from the Institutional Review Board of Peking Union Medical College Hospital, with approvals granted in March 2024 (No. I-24PJ0652) and July 2024 (No. I-24PJ1454).
Acknowledgments
We would like to thank the six surgical teams of the Department of Orthopedics and Basic Surgery of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences for their strong support to this study. We greatly appreciate your professional guidance and selfless assistance in study design, data collection, and clinical practice. In addition, we sincerely thank all the medical staff and patients in the Department of Orthopedics and Basic Surgery of Peking Union Medical College Hospital for their support and cooperation. Your hard work and active participation have provided a solid foundation for the successful implementation of this study.
Funding
This work was supported by 1. Application of Opioids in Combined Postoperative Anesthesia - Clinical Research of ERAS in Laparoscopic Pancreatic Surgery (No. O459800). 2. Peking Union Medical College Hospital Sedimentation Research Funding Integration Entrustment Project (No. ZC201903189).
Disclosure
The authors report no conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Yu J, Zhang Y, Yu T, et al. Preoperative anxiety in Chinese adult patients undergoing elective surgeries: a multicenter cross-sectional study. World J Surg. 2022;46(12):2927–2938. doi:10.1007/s00268-022-06720-9
2. Abate SM, Chekol YA, Basu B. Global prevalence and determinants of preoperative anxiety among surgical patients: a systematic review and meta-analysis. Int J Surg Open. 2020;25:6–16. doi:10.1016/j.ijso.2020.05.010
3. Mulugeta H, Ayana M, Sintayehu M, Dessie G, Zewdu T. Preoperative anxiety and associated factors among adult surgical patients in debre markos and felege hiwot referral hospitals, Northwest Ethiopia. BMC Anesthesiol. 2018;18(1):155. doi:10.1186/s12871-018-0619-0
4. Eberhart L, Aust H, Schuster M, et al. Preoperative anxiety in adults - a cross-sectional study on specific fears and risk factors. BMC Psychiatry. 2020;20(1):140. doi:10.1186/s12888-020-02552-w
5. Yilmaz Inal F, Yilmaz Camgoz Y, Daskaya H, Kocoglu H. The effect of preoperative anxiety and pain sensitivity on preoperative hemodynamics, propofol consumption, and postoperative recovery and pain in endoscopic ultrasonography. Pain Ther. 2021;10(2):1283–1293. doi:10.1007/s40122-021-00292-7
6. Kil HK, Kim WO, Chung WY, Kim GH, Seo H, Hong J-Y. Preoperative anxiety and pain sensitivity are independent predictors of propofol and sevoflurane requirements in general anaesthesia. Br J Anaesth. 2012;108(1):119–125. doi:10.1093/bja/aer305
7. Ali A, Lindstrand A, Sundberg M, Flivik G. Preoperative anxiety and depression correlate with dissatisfaction after total knee arthroplasty: a prospective longitudinal cohort study of 186 patients, with 4-year follow-up. J Arthroplasty. 2017;32(3):767–770. doi:10.1016/j.arth.2016.08.033
8. Ali A, Altun D, Oguz BH, Ilhan M, Demircan F, Koltka K. The effect of preoperative anxiety on postoperative analgesia and anesthesia recovery in patients undergoing laparascopic cholecystectomy. J Anesth. 2014;28(2):222–227. doi:10.1007/s00540-013-1712-7
9. Ma J, Li C, Zhang W, et al. Preoperative anxiety predicted the incidence of postoperative delirium in patients undergoing total Hip arthroplasty: a prospective cohort study. BMC Anesthesiol. 2021;21(1):48. doi:10.1186/s12871-021-01271-3
10. Aspalter M, Enzmann FK, Hölzenbein TJ, et al. Preoperative anxiety as predictor of perioperative clinical events following carotid surgery: a prospective observational study. Perioper Med. 2021;10(1):53. doi:10.1186/s13741-021-00223-2
11. Schaal NK, Hepp P, Heil M, et al. Perioperative anxiety and length of hospital stay after caesarean section - A cohort study. Eur J Obstet Gynecol Reprod Biol. 2020;248:252–256. doi:10.1016/j.ejogrb.2020.03.045
12. Notice of the general office of the national health commission on printing and distributing the measures for the classification of surgery in medical institutions 2022.
13. Bucx MJL, Krijtenburg P, Kox M. Preoperative use of anxiolytic-sedative agents; are we on the right track? J Clin Anesth. 2016;33:135–140. doi:10.1016/j.jclinane.2016.03.025
14. Cheng K, Zhou L. Diagnosis and Treatment of Auricular Acupuncture. Beijing: People’s Health Publishing House; 2020.
15. Aminizadeh M, Tirgari B, Rashtabadi OR, Jahani Y, Tajadini H. Effectiveness of auricular acupressure on constipation and related quality of life among the older people in the residential care home: a randomized clinical trial. BMC Geriatr. 2023;23(1):171. doi:10.1186/s12877-023-03881-7
16. Mi A, Hao M, Zhou Z, et al. Acupuncture for patients after percutaneous coronary intervention: a scoping review. Complement Ther Med. 2024;85:103081. doi:10.1016/j.ctim.2024.103081
17. Wang J, Zhang J, Sun D. Randomized crossover study of auricular plaster therapy to relieve dental anxiety in children. Front Psychiatry. 2022;13:862575. doi:10.3389/fpsyt.2022.862575
18. Wang Z, Chen Y, Ge X, et al. Preoperative anxiety state is an independent risk factor for delayed gastric emptying after pylorus-preserving pancreaticoduodenectomy: a single-center retrospective case-control study. Ann Med. 2025;57(1):2564278. doi:10.1080/07853890.2025.2564278
19. Alattas SA, Smith T, Bhatti M, Wilson-Nunn D, Donell S. Greater pre-operative anxiety, pain and poorer function predict a worse outcome of a total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2017;25(11):3403–3410. doi:10.1007/s00167-016-4314-8
20. Qiu P, Liu GZ, Liu JB, Cao LP. Effect of auricular point sticking therapy on preoperative anxiety in general surgery patients. J Qilu Nursing. 2009;15:30.
21. Lan XF, Shu JZ. Clinical observation on auricular point sticking therapy combined with herbal medicine oxygen inhalation for preoperative anxiety in 30 cases of cerebral angiography. Chin J Ethnomed Ethnopharm. 2020;29:105–108.
22. Gao L, Mu SF, Yan SZ, Song ZR. Therapeutic effect of auricular point sticking therapy combined with five-element music therapy on preoperative anxiety in patients undergoing total knee arthroplasty. J Hunan University Chin Med. 2019;39:117–120.
23. von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
24. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. J Evid Based Med. 2010;3(3):140–155. doi:10.1111/j.1756-5391.2010.01086.x
25. Wang L, Lu X, Wang L, et al. PAS-7 is superior to APAIS for assessing preoperative anxiety in the chinese population. J Perianesth Nurs. 2024;39(5):853–858. doi:10.1016/j.jopan.2023.12.022
26. Usichenko TI, Hua K, Cummings M, et al. Auricular stimulation for preoperative anxiety - A systematic review and meta-analysis of randomized controlled clinical trials. J Clin Anesth. 2022;76:110581. doi:10.1016/j.jclinane.2021.110581
27. Shebl MA, Toraih E, Shebl M, et al. Preoperative anxiety and its impact on surgical outcomes: a systematic review and meta-analysis. J Clin Transl Sci. 2025;9(1):e33. doi:10.1017/cts.2025.6
28. Lindner M, Nosseir O, Keller-Pliessnig A, Teigelack P, Teufel M, Tagay S. Psychosocial predictors for outcome after total joint arthroplasty: a prospective comparison of Hip and knee arthroplasty. BMC Musculoskelet Disord. 2018;19(1):159. doi:10.1186/s12891-018-2058-y
29. Chiu PL, Li H, Yap KY-L, Lam K-MC, Yip P-LR, Wong CL. Virtual reality-based intervention to reduce preoperative anxiety in adults undergoing elective surgery: a randomized clinical trial. JAMA Network Open. 2023;6(10):e2340588. doi:10.1001/jamanetworkopen.2023.40588
30. Suleiman-Martos N, García-Lara RA, Membrive-Jiménez MJ, et al. Effect of a game-based intervention on preoperative pain and anxiety in children: a systematic review and meta-analysis. J Clin Nurs. 2022;31(23–24):3350–3367. doi:10.1111/jocn.16227
31. Tola YO, Chow KM, Liang W. Effects of non-pharmacological interventions on preoperative anxiety and postoperative pain in patients undergoing breast cancer surgery: a systematic review. J Clin Nurs. 2021;30(23–24):3369–3384. doi:10.1111/jocn.15827
32. Hounsome J, Lee A, Greenhalgh J, et al. A systematic review of information format and timing before scheduled adult surgery for peri-operative anxiety. Anaesthesia. 2017;72(10):1265–1272. doi:10.1111/anae.14018
33. Peuker ET, Filler TJ. The nerve supply of the human auricle. Clin Anat. 2002;15(1):35–37. doi:10.1002/ca.1089
34. Sun J, Sun K, Chen L, et al. A predictive study of the efficacy of transcutaneous auricular vagus nerve stimulation in the treatment of major depressive disorder: an fMRI-based machine learning analysis. Asian J Psychiatr. 2024;98:104079. doi:10.1016/j.ajp.2024.104079
35. Zhao B, Bi Y, Chen Y, et al. Altered functional connectivity of the thalamus in patients with insomnia disorder after transcutaneous auricular vagus nerve stimulation therapy. Front Neurol. 2023;14:1164869. doi:10.3389/fneur.2023.1164869
36. Groves DA, Brown VJ. Vagal nerve stimulation: a review of its applications and potential mechanisms that mediate its clinical effects. Neurosci Biobehav Rev. 2005;29(3):493–500. doi:10.1016/j.neubiorev.2005.01.004
37. Mohr P, Rodriguez M, Slavíčková A, Hanka J. The application of vagus nerve stimulation and deep brain stimulation in depression. Neuropsychobiology. 2011;64(3):170–181. doi:10.1159/000325225
38. Manta S, Dong J, Debonnel G, Blier P. Enhancement of the function of rat serotonin and norepinephrine neurons by sustained vagus nerve stimulation. J Psychiatry Neurosci. 2009;34(4):272–280. doi:10.1139/jpn.0936
39. Liu C-Z, Kong J, Wang K. Acupuncture therapies and neuroplasticity. Neural Plast. 2017;2017:6178505. doi:10.1155/2017/6178505
40. Yuan Y, Zhang X, Wang Y, et al. Multimodal data integration using deep learning predicts overall survival of patients with glioma. View. 2024;5(5):20240001. doi:10.1002/VIW.20240001
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.