Back to Journals » Psychology Research and Behavior Management » Volume 17
Attention-Dominated Cognitive Dysfunction May Be a Biological Marker for Distinguishing SA from SI in Adolescents: A Network Analysis Study Based on Adolescent Depression
Authors Wang Q, Wen M ![]() , Fan S, Liu J, Wang X, Guo W, Hu J, Zhang J, Li B, Zhang L, Zhang Y, Li K
, Fan S, Liu J, Wang X, Guo W, Hu J, Zhang J, Li B, Zhang L, Zhang Y, Li K
Received 8 November 2023
Accepted for publication 27 February 2024
Published 6 March 2024 Volume 2024:17 Pages 945—956
DOI https://doi.org/10.2147/PRBM.S448904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Qi Wang,1,2,* Min Wen,2,3,* Shaohang Fan,2,4 Jinning Liu,2 Xiaowen Wang,5 Wentao Guo,2 Jinyun Hu,6 Jialan Zhang,2 Bing Li,2,7 Lili Zhang,2,7 Yunshu Zhang,1,2,7 Keqing Li2,7
1Clinical Medicine College, Hebei University, Hebei, People’s Republic of China; 2Hebei Provincial Mental Health Center, Hebei, People’s Republic of China; 3Department of Psychiatry, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China; 4School of Psychology and Mental Health, North China University of Science and Technology, Tangshan, People’s Republic of China; 5Psychosomatic Medicine Department, Jiangxi Provincial People’s Hospital, Nanchang, People’s Republic of China; 6Psychiatric Department, The Second People’s Hospital of Yuxi, Yunnan, People’s Republic of China; 7Hebei Provincial Key Laboratory of Major Mental and Behavioral Disorders, Hebei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Keqing Li, Hebei Provincial Mental Health Center, Hebei, People’s Republic of China, Email [email protected] Yunshu Zhang, Hebei Provincial Mental Health Center, Hebei, People’s Republic of China, Email [email protected]
Objective: Suicidal behavior is strongly correlated with depressive symptoms and the degree of suicidal ideation. Cognitive impairment may have varying degrees of influence on suicidal ideation (SI) and suicidal attempts (SA). The aim of this study was to identify the cognitive biomarkers that distinguish suicidal ideation from suicidal attempts in adolescents.
Methods: The cross-sectional sample comprised 54 adolescents with major depressive disorder (MDD) and 32 healthy controls (HC). The THINC-it was utilized to assess cognitive function of all the samples. Suicidal ideation was examined by the Positive and Negative Suicide Ideation Scale (PANSI). Based on the type of data, one-way ANOVA or Kruskal–Wallis was performed to investigate group differences. Bonferroni post-hoc analysis was employed for regulating type I error for pairwise comparisons. Network analysis was used to compare the networks associated with suicidal ideation, depression symptoms, and cognitive function between SA and SI.
Results: The depression symptoms (HAMD-17) (F=72.515, P< 0.001) and suicidal ideation (PANSI) (F=267.952, P< 0.001) in the SA were higher than those in the SI. Analysis of between-group differences showed SA performed worse in THINC-it, especially in “Spotter (SP)” (P=0.033), “Objective cognition score (OS)” (P=0.027) and “Composite score (CS)” (P=0.017). Compared with SI, network analysis revealed that SA had a unique network of cognitive function, depressive symptoms, and suicidal ideation. Nevertheless, both networks exhibit comparable performance concerning the node strength of cognitive function. Within their separate networks, the aspects of CS, OS, and SP have emerged as the three most crucial elements.
Conclusion: Adolescents with SI or SA exhibit a broad spectrum of cognitive impairments. Attention impairment can be beneficial in discerning between SI and SA. Future interventions for adolescent suicide can center on attention and the comprehensive cognitive ability that it represents.
Keywords: attention impairment, suicide ideation, suicide attempts, adolescent, THINC-it tool, network analysis
Introduction
On a global scale, suicide represents a substantial public health concern. It is among the leading causes of mortality for adolescents between 15 and 19.1–3 In Europe, suicide is the second most prevalent cause of mortality among individuals aged 13 to 19 following vehicle accidents.4 Each year, more than 10,000 young individuals in China commit suicide, which contributes to approximately 20% of total mortality rates.5 To date, the issue of youth suicide presents a significant impediment to global public health. Consequently, there is an urgent need to enhance suicide prevention interventions specifically aimed at the adolescent population in China.
With increasing research, suicide is no longer defined as a singular symptom but as a cluster of symptoms characterized as suicidal thinking and behaviors (SITBs), which include SI, suicidal plans (SP), suicidal threats (ST), non-suicidal self-injury (NSSI) and SA. SI refers to the thought or contemplation of ending one’s own life; SP means the intention to terminate one’s life via self-harm; ST applies to a definition for conveying to the outside world that suicidal behavior may occur in the immediate future; NSSI describes it as the intentional infliction of physical harm without the intent to kill, which is unacceptable in a social context. SA is the term for an act of self-harm or self-destruction intended to be fatal but not be realized.6–9 Accumulating evidence suggests that SI and SA are considered separate factors that can independently predict suicide behavior.10–12 Contrary to the conventional definition of suicide, the “ideation-to-action” framework theory contends that SI and SA have distinct etiological pathways. Furthermore, there is evidence of a reciprocal transition between symptoms. About one-third of SI will convert to SA.13 Simultaneously, Baker’s investigation on adolescent suicide produced comparable findings.14 In the sample of 4772 adolescents, the lifetime prevalence of suicidal ideation and suicide attempts was 9.6% and 6.8%, respectively. A study by Nock et al13 on 6483 teenagers between the ages of 13 and 18 revealed that 12.1% had SI and 4.1% had SA in the past. Following a comprehensive survey conducted on a sample size of over 60,000 adolescents from China, the research findings indicated that the 12-month prevalence rates for SI and SA were recorded at 13% and 4.8%, respectively.15 However, some investigations into adolescent depression discovered that SI and SA exhibit a substantial relationship in stability and duration, providing additional evidence for a psychopathological continuum between these phenomena.16 Given that SA is a strong predicator of suicidal behavior, it is crucial to search for biomarker that can differentiate between SA and SI status in adolescents. This will postpone the shift from SI to SA during the initial phase, thereby intervening in patients’ suicidal behavior at an early stage of the illness. Hence, we conducted a targeted assessment on depressed adolescents who exhibited SA and/or SI in order to find distinct biomarker that differentiate SI from SA. Furthermore, we compared these characteristics with those of mentally healthy adolescents.
Notably, in the context of therapeutic practice, mental illnesses associated with depression frequently coexist with SI or SA, which can eventually lead to suicidal behaviors. According to existing research, depression has been identified as the most influential risk factor for SI and SA. However, it is unfortunate that most symptom descriptions in clinical case data are based on retrospective clinical interviews, which are obviously subjective.17–20 Consequently, it is still challenging to distinguish the objective distinctions between the two components using psychological and behavioral representations. Thus, some readily implemented testing methods can help provide more and faster clinical information for future targeted interventions. The THINC-it was released at the 2016 annual meeting of the European College of Neuropsychopharmacology (ECNP) (website: https://thinc.progress.im/en). THINC-it has the advantages of simplicity, flexibility, and speed, as it can be administered at any time on a mobile device or computer and has been extensively used to assess cognitive function (attention, executive function, working memory, etc.) in depression. The complete testing method often spans around 10 to 15 minutes and can be promptly followed by feedback on the results.21,22 Compared with routine cognitive function testing, there’s a legitimate reason to think it can successfully prevent the tiredness reaction. Simultaneously, the Chinese simplified version of THINC-it has been applied to the clinical research of adolescent depression and yielded similar results in specific terms of executive function and Integrated visual and aural continuous performance test (IVA-CPT).23,24
Research demonstrated that depression with SI and SA accompanied extensive cognitive impairment, particularly cognitive control impairment that was crucial in suicidal behavior.25 According to the cognitive neural model of suicide, cognitive impairment reduces individuals’ capacity to coordinate attention and thought behavior. SA was distinguished from SI by overt symptoms, which might impede the individual’s ability to shift their attention away from negative emotional states such as despair and pain, resulting in a slower reaction time and relating to high levels of violence and fatal suicide behaviors.26–30 Recent investigations indicated that individuals with SA exhibited more pronounced cognitive control impairments than those without this disposition. Consequently, it was plausible to hypothesize that SA exacerbates the extent of cognitive control impairments.25 Similar results were found in a study involving adolescents with depression, in which attention responses were delayed in medication-naive patients compared to healthy controls. The above results were more pronounced in those with suicidal tendencies.31 It has been revealed that executive dysfunction is also positively correlated with the severity of suicide in the neurocognitive characteristics of individuals who commit suicide; even though controlling for depressive symptoms, such a relationship still exists.32 In the study of adolescent depression, which is characterized by attention impairment of executive functions, similar findings have been reported.33 A review of 63 studies on SA reveals a high degree of result consistency. Working memory, executive function, attention, and cognitive control were all impaired; however, results in the SI population were inconsistent.34 The study of SA and SI in adults and adolescents is receiving growing attention. Due to the lack of consistent findings, it is plausible to consider that SI and SA may represent distinct clinical states despite sharing comparable clinical manifestations.16
While a limited number of studies have yielded consistent findings in the adolescent population,20 most research has focused on investigating specific dimensions of cognition, such as executive function and attention. The potential correlation could be attributed to the protracted and laborious procedures involved in conventional cognitive assessments, along with the limited capacity of adolescents to endure such processes.22 Few studies have conducted comprehensive reviews of adolescents’ cognitive function in a brief time. To differentiate between SI and SA in adolescent depression, the study aimed to use THINC-it as a cognitive assessment tool to execute comprehensive cognitive function tests quickly. This assessment tool entails attention, working memory, and the subjective evaluation of cognitive ability, allowing for a more apparent distinction between SA and SI regarding symptom dimensions and cognitive performance. Conventional investigations on psychopathology mostly rely on scale scores to measure the intensity of symptoms and employ basic linear correlation to establish connections within the disorder. This might undermine significant associations within or among mental disorders.35,36 The study employed network analysis as a novel visual statistical technique to effectively illustrate the association between symptoms and symptoms/illnesses, hence facilitating the identification of intervention targets.37 Given that SA and SI are different disease states, we hypothesized that adolescents with SA would have more severe attention impairment. In addition, the comprehensive manifestations of cognitive impairment can also help distinguish between SI and SA.
Methods
Participants
This research is characterized as a cross-sectional observational study. It consisted of a sample of 86 adolescents aged 12 to 18 years old. There was a total of 54 teenage depression patients, including both outpatients (n = 14) and inpatients(n = 40); 32 teenagers who participated as healthy controls were from the community. According to self-reported suicide status and Hamilton Depression Scale score-17 (HAMD-17),38 the score for suicide (ie, item-3 on the HAMD-17 scale) in the two groups is greater than zero. Adolescents with depression were divided into (a) SI group (n=22), there was suicide ideation in the last two weeks but no reported history of attempted suicide; (b) SA group (n=32), A lifetime history of suicidal ideation and self-reported suicide attempt.39
The patients included in this study were diagnosed by experienced attending physicians and physicians holding the position of deputy director or above. These patients were picked based on meeting the predetermined selection criteria. The following are the inclusion and exclusion criteria. The following are the inclusion requirements for patients with SI and SA: 1) The patients were diagnosed with major depressive disorder (MDD) based on the diagnostic criteria outlined in the International Classification of Diseases Tenth Revision (ICD-10); 2) 12 to 18 years of age, Han Chinese; 3) Patients with HAMD-17 total score>17 and item-3 score>0; 4) Parents or individuals are aware of the content of the study and provide informed consent in writing; 5) Both inpatients and outpatients had examinations in the absence of medication. The exclusion criteria pertaining to patients with SI and SA are as follows: 1) Individuals presenting with comorbid mental or physical conditions that have the potential to impact cognitive function; 2) Patients were diagnosed with mental retardation, substance dependence or abuse (excluding nicotine and caffeine), bipolar disorder, obsessive-compulsive disorder, post-traumatic stress disorder, and eating disorders; 3) Taking any medication that may influence cognitive function (such as glucocorticoids, β-receptor blockers, opioid analgesics, and central stimulants); 4) Patients who had consumed benzodiazepines within 12 hours prior to the THINC-it test; 5) Antipsychotic medication has been utilized for the past three months; 6) Patients who had ingested alcohol within eight hours prior to the THINC-it clinical trial; 7) Patients who received electroconvulsive therapy (ECT) in the previous six months; 8) Patients identified as attention deficit hyperactivity disorder (ADHD); Or 9) Patients incapable of reading or comprehending the informed consent form. Inclusion criteria for HC: 1) No mental disorder and no history of mental disorder in the family; 2) 12 to 18 years of age, Han Chinese; 3) Junior high school or higher level of education; 4) HAMD-17 total score≤7, item-3 score= 0; 5) Parents or individuals were aware of the content of the investigation and provided written consent.
Procedure
The study was approved by the Clinical Research Ethics Committee of Hebei Mental Health Center. It was compliant with the Code of Ethics of the World Medical Association (Declaration of Helsinki). Informed written consent was obtained from all participants or their legal guardians after a complete and extensive description.
Instruments
Assess Depressive Symptoms (HAMD-17)
The HAMD-1738 is a validated measurement tool consisting of 17 items that are utilized to evaluate the severity of depressive symptoms in individuals during clinical interviews. This scale employs a 5-point scale ranging from 0 to 4, and as the total score increases, it indicates that the patient’s depressive symptoms are becoming increasingly severe. The severe depression total score is≥24; The mild or moderate depression total score is≥17; the No depression symptoms total score is≤7. There is good consistency in Chinese research (α=0.714).40
Assess Suicidal Ideation (PANSI)
PANSI41 is a 14-item self-evaluation scale for evaluating suicidal ideation. It includes two dimensions: positive suicidal ideation (6 items) and negative suicidal ideation (8 items). This measure, which uses the Likert 5-level scoring technique, rates the frequency of suicidal ideation from “never” to “always” on a range of 1 to 5. The scoring methodology is the summation of two aspects of scores related to suicide ideation. Higher scores indicate more significant suicidal ideation. It is crucial to recognize that the assessment of positive suicidal thoughts utilizes the reverse scoring system. The Chinese version of PANSI, including negative suicidal ideation (α= 0.94) and positive suicidal ideation (α= 0.86), has excellent internal consistency in studies of adolescents in China.42
Evaluate Cognitive Function (The Simplified Chinese Version of THINC-It)
The digital cognitive evaluation instrument comprises five sub-tests: The Perceived Deficits Questionnaire for Depression,5-item (PDQ-5-D) is a self-report instrument designed to evaluate the cognitive components of an individual’s subjective experience of depression; There are four cognitive tests that serve as objective measures: 1) Spotter (SP): The Choice Reaction Time(CRT) paradigm and the Identification Task (IDN) are used to measure the mean latency for correct responses, expressed in milliseconds, and can evaluate the subjects’ attention reflexes and flexibility; 2) Symbol Check (SC): The One-Back Test measures the number of correct responses, and subjects’ working memory, executive function, and attention can be evaluated using the item; 3) Codebreaker (CB): The Digit Symbol Substitution Test (DSST) is employed to assess participants’ capacity for observation, reaction, and execution by quantifying the number of accurate responses; 4) Trails (TRA): The Trail Making Test Part B is a cognitive assessment tool that utilized the duration of completion as a metric to evaluate executive function.21,24 The objective score(OS) calculation involved summing the Z-scores for each objective test measure, with equal weights assigned to each measure for every participant; the composite score (CS) calculation involved summing the OS and the PDQ-5-D score.43 Recent studies in China have demonstrated that the PDQ-5-D in depressed populations has a Cronbach’s alpha of = 0.704% and that all four sub-tests have excellent simultaneous validity (r range from 0.343 to 0.835, all P<0.01).44
Demographic Data
We used a self-administered general information questionnaire, and the following variables were collected: Age, BMI, Years of education, Gender, Disease course, Type of depressive episode, and Family history.
Cognition Research Process
The sequence of cognitive function assessment was: PDQ-5-D→ Spotter→ Symbol Check→ Code Breaker→ Trails, and on the first day of admission, each group was assessed in the same order.44 The classification of subjects was unknown to both the assessor and the subjects. The specific experimental steps are detailed in the English version of the THINC-it study conducted by McIntyre et al.22
Sample Size Calculation
Regarding sample size, we used the G * Power (3.1)45 software to analyze the required sample size, which was presented at the effect level f=0.4,46 significance level α=0.05 (bilateral), statistical test capability 1-β= 0.8, and the total sample size was 66. It can be considered that our sample size is sufficient under the above requirements.
Statistical Analysis
We followed the method that McIntyre et al22 described for calculating cognitive function scores from raw scores to Z-scores in detail. This study was analyzed with SPSS 26.0. The Kolmogorov–Smirnov test was employed to assess the conformity of the measurement data to a normal distribution. Continuous variables were utilized as means (standard deviations), and categorical variables were used as frequencies (percentages) in descriptive analysis. The median (upper - lower quartile) was applied to non-normal metrics. In the research, the chi-square test was utilized for the study of count data. In contrast, the one-way ANOVA was utilized to analyze the difference among groups of normality data. The Kruskal–Wallis test was applied to compare the non-normal data among groups. To reduce the likelihood of Type I errors that may arise from doing multiple tests, Bonferroni post-hoc analyses were employed to compare variables in a two-way method. A p-value less than 0.05 in a two-tailed test was deemed statistically significant.
The study utilized the R package qgraph47 and applied a Gaussian graphical model(GGM)48 to compare networks related to cognitive function, depressive symptoms, and suicide in patients with SI and SA. In the GGM, the edges describe conditional dependence relationships between components. In the resultant graph, even though all other variables are controlled, a connection between two items also indicates their dependence. Conversely, the two items are considered conditionally independent if there is no connection. GGM is commonly performed using the graphical lasso method, which has the advantage of employing regularization to minimize the estimation of spurious edges.49 Consequently, this approach can effectively balance network sparsity and the goodness-of-fit. The method seeks to maximize the penalized log-likelihood by combining a log-likelihood function with a penalty term dependent on the network density. The tuning parameter (λ1) corresponds to the sparse and dense features of the network. The extended Bayesian information criterion (EBIC) can be utilized as a method for calculating an optimal score of λ1 to obtain a network estimate that closely approximates the most realistic outcome.50 The graph lasso method was ultimately employed to optimize the estimation of the network and provide sparse and succinct networks that effectively describe the data. The network estimation graphic can illustrate the strength of correlations between variables. Thicker edges represent stronger correlations, whereas red dashed lines indicate negative correlations, and solid blue lines indicate positive correlations. Various colored nodes correspond to different psychology measurement dimensions. To provide a quantitative assessment of the significance of network structure, three indices of node centrality, notably strength, closeness, and betweenness, were calculated.51 Strength refers to the cumulative weight of all edges directly related to the nodes. If the node has more robust direct connections to other nodes, it will have greater strength. Closeness corresponds to a given node to all the other connected ones, equal to the inverse weight sum of the shortest path. If a node exhibits more closeness, it will have a more rapid impact on other nodes. Betweenness is a measure of a node’s connective value in the network and is defined as the frequency with which a node links to two other nodes on the shortest path possible.52 According to research findings, closeness and betweenness cannot be reliably estimated, so we only considered node strength when comparing centrality differences. In addition, the research also included expected influence (EI), one of the most reliable centrality measures, which was utilized to get the total of the absolute values of each node’s connection weights.53
Results
The sociodemographic, clinical, and laboratory characteristics are shown in Table 1. The depression symptoms (HAMD-17) (F=72.515, P<0.001) and suicidal ideation (PANSI) (F=267.952, P<0.001) in the SA were higher than those in the SI. Moreover, no statistically significant differences were observed in terms of Age, Gender, BMI, Years of education, Disease course, Type of depressive episode, and Family history between the SA and SI.
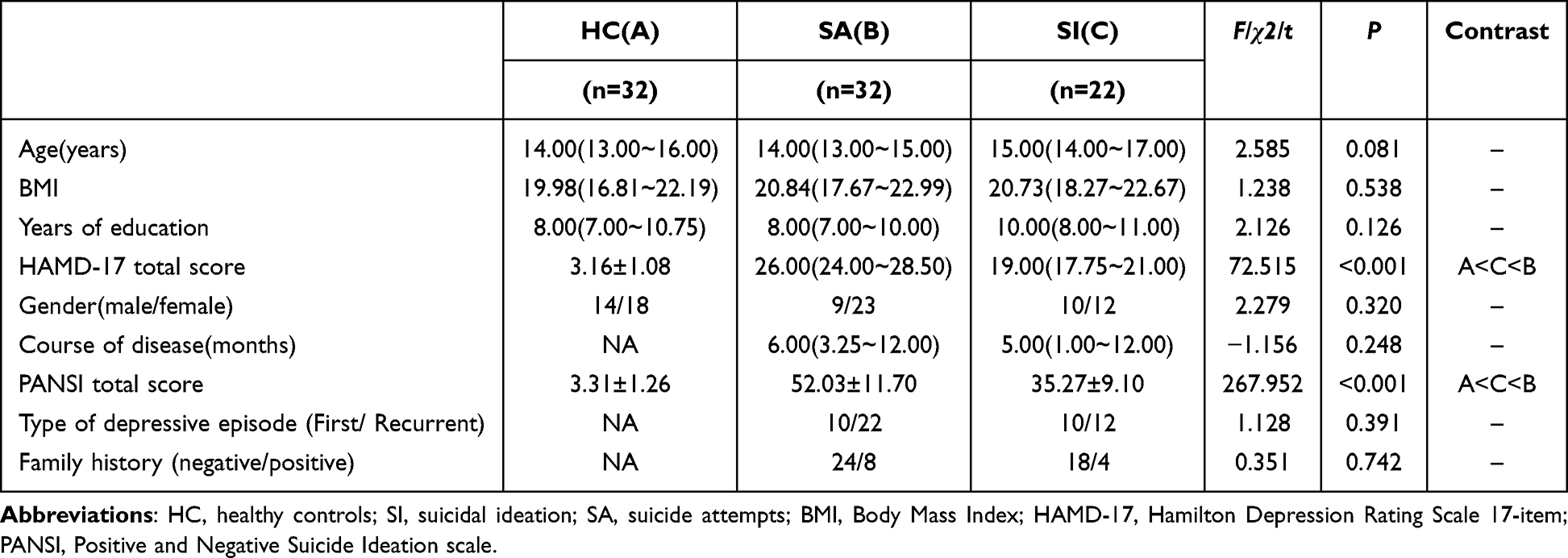 |
Table 1 General Demographic Information |
The analysis of intergroup differences in THINC-it cognitive scores was illustrated in Table 2 and Figure 1. Based on the available data, the one-way ANOVA analysis of variance was used to compare the cognitive differences in SP, CB, PDQ-5-D, OS, and CS among the three groups. The statistical analysis revealed a significant difference among the three groups in SP; Subsequent Bonferroni post hoc analysis indicated that the SA group had a significantly lower value than the SI group (P=0.033). On the PDQ-5-D, there were statistically significant differences between groups; Bonferroni post hoc analysis revealed SA<HC (P=0.001) and SI<HC (P=0.001), but no statistical difference between SA and SI. Differences in OS were statistically significant among groups; Bonferroni post hoc tests revealed SA<SI (P=0.027). CS demonstrated statistically significant differences among groups. Further post-hoc analyses using the Bonferroni method revealed that SA significantly differed from both SI (P=0.017) and HC (P=0.001); However, there was no statistically significant difference between SI and HC. The Kruskal–Wallis test examined the cognitive disparities among the three groups in the SC and TRA contexts. Nevertheless, no significant statistical distinction was observed among the various groups.
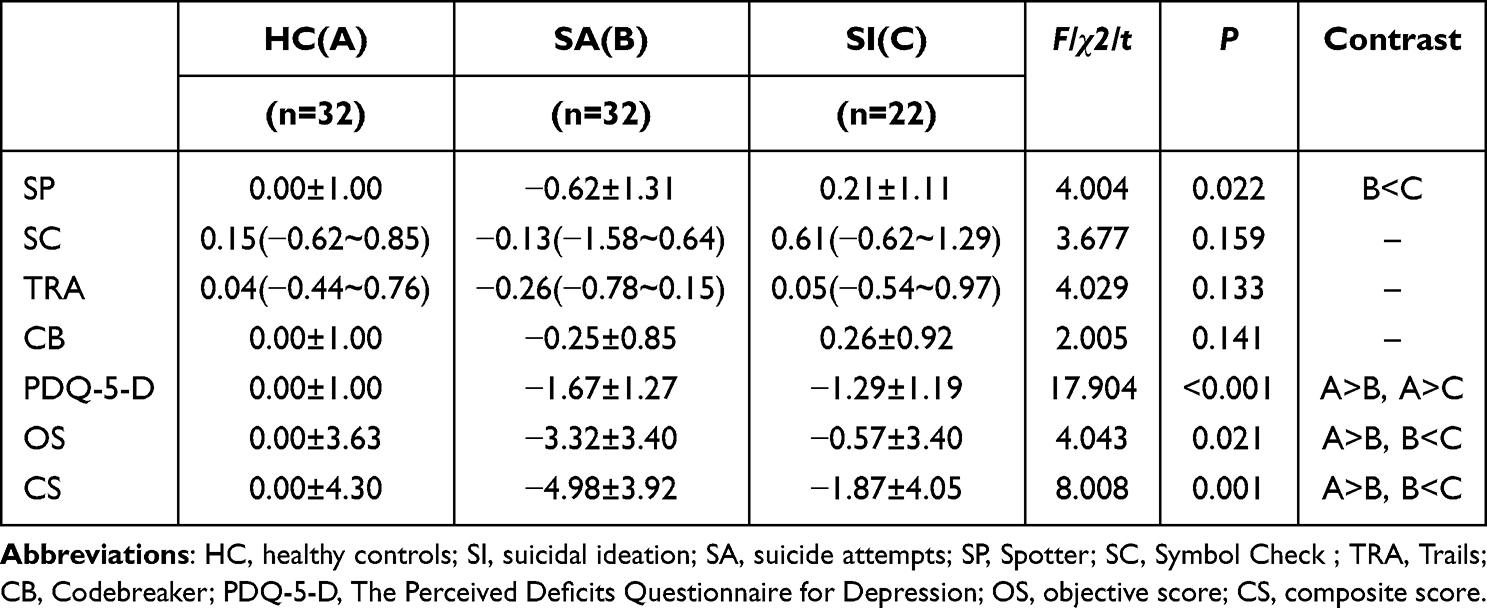 |
Table 2 Comparison of THINC-It Z Scores Between SA, SI, and HC Groups |
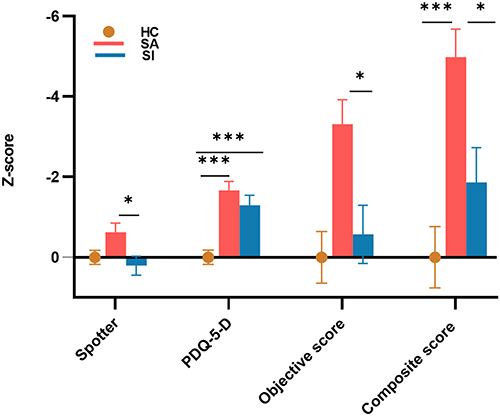 |
Figure 1 Intergroup differences in THINC-it cognition scores. Notes: HC, healthy controls; SA, suicidal attempts; SI, suicidal ideation; PDQ-5-D, five-item Perceived Deficits Questionnaire for Depression; Objective Score, Composite score of THINC-it objective test; Composite score, Composite score of THINC-it; The vertical axis in the graph indicates the Z-score of cognitive function, while the horizontal axis represents the various grouping strategies; *P value is significant at the 0.05 level; ***P value is significant at the 0.001 level. |
Regarding model estimation, network analysis revealed that the SA had a unique network of cognitive function, depressive symptoms, and suicide compared to the SI (Figure 2). Meanwhile, the network of SI was sparser than that of SA, as well as depressed symptoms and suicidal ideation were conditionally independent of the other variables. The study showed a direct and negative correlation between suicidal ideation (ie, PS: PANSI Score) and objective cognitive function (ie, OS: Objective Score) in the SA group. However, in the SI group, suicidal ideation did not exhibit any directly or indirectly associated characteristics. Despite this, it is worth noting that both groups had similar results regarding the centrality index of cognitive performance. In the centrality difference of strength, CS, OS, and SP were key central symptoms in their respective networks. The results are presented in Figure 3. Moreover, the results of bootstrapped 95% confidence intervals (CIs), case-dropping bootstrapping, and bootstrapped difference tests of node weights and edge weights are presented in Figure S1–S4.
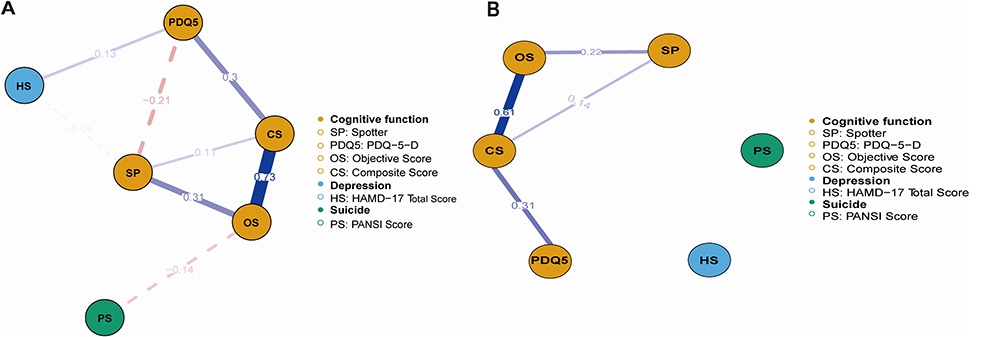 |
Figure 2 Networks estimation of cognitive function, Depression symptoms and suicide in SA and SI. Notes: The presence of red dashed lines in the graph signifies negative correlations, while solid blue lines show positive correlations. The greater thickness of edges indicates an elevated level of correlations. Specific relevance is denoted by numbers on the edge. (A) illustrates the network estimation diagram for group SA, while (B) depicts the network estimation diagram for the SI group. |
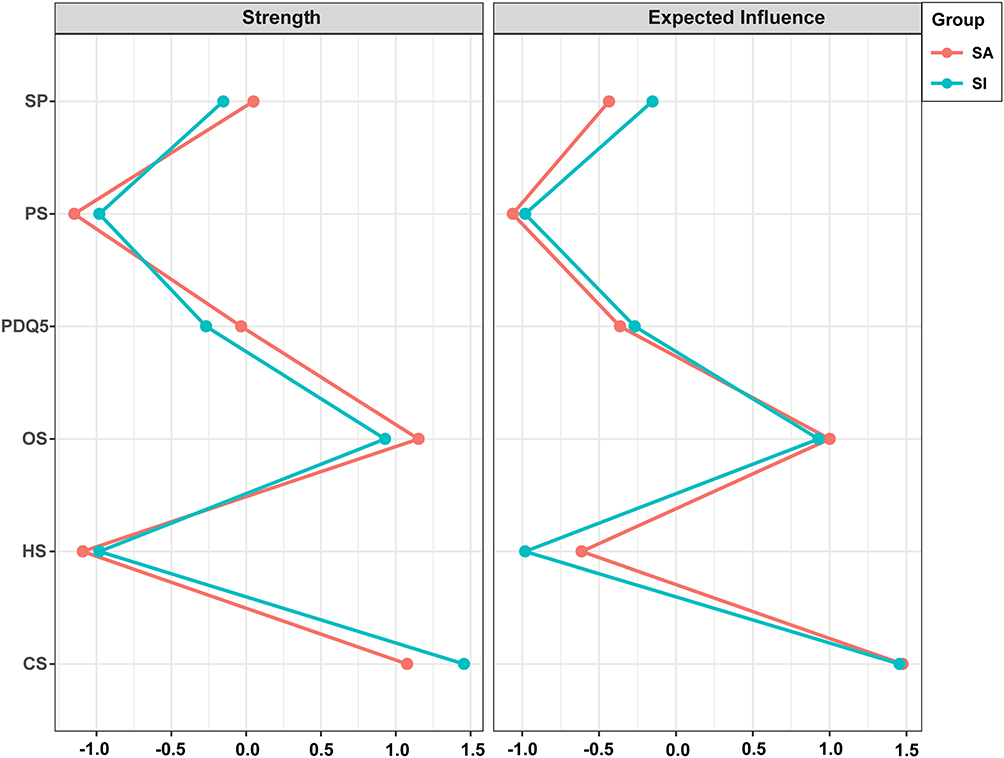 |
Figure 3 Comparison of the centrality difference of strength and expected influence (EI) in the networks across two samples. Notes: Nodes are plotted on the y-axis. Centrality indices represented as z-scores are plotted on the x-axis. EI measures the influence of a given node on its directly connected neighbors by summing the values of all the edges connected to it. Higher values of EI and strength indicate stronger interconnections between nodes. SA, suicidal attempts; SI, suicidal ideation; SP, spotter; PS, PANSI score; PDQ5, five-item Perceived Deficits Questionnaire for Depression; OS, Composite score of THINC-it objective test; HS, HAMD-17 total score; CS, Composite score of THINC-it. |
Discussion
It is essential to clarify the relationship between SA and SI to comprehend and prevent suicide among depressed adolescents. The present study illustrated the difference between SA and SI by describing the changes in cognitive function among depressed adolescents with different suicide dimensions and giving a more positive interpretation with healthy adolescents as the control group. The findings revealed that adolescents with SA had more severe attention impairment and depressive symptoms than those with SI. Furthermore, it could be observed that SA exhibited a more compact network structure in relation to cognitive function, depression, and suicide.
Existing research indicates a link between frequent attention impairment and fatal SA.31 In this study, the analysis of cognitive function differences revealed that SA was associated with a more severe attention impairment, particularly concerning attention flexibility and reaction time. Based on the scoring principle of THINC-it, it is posited that the disparity between the CS and the OS primarily arises from the SP component. The observed distinction between groups attributed to the SP factor remained statistically significant even after including other items that exhibited no discernible variation between the groups. The study on adolescent depression yielded comparable findings, indicating that SA had a greater propensity for delayed attention responses on the Attention Network Task (ANT) test.31 In addition, the Continuous Performance Test, Identical Pairs (CPT) instrument used to evaluate depression in adolescents’ attention also revealed comparable group differences.54 Therefore, attention impairment may be indicative of SA, and more severe attention impairments tend to reflect cognitive control deficiencies, consistent with most prior research.28,55,56 Cognitive control is related to an individual’s capacity to effectively regulate their attention, cognitive processes, and behaviors to attain desired objectives. The absence of this capacity significantly contributes to the occurrence of suicide.26 Recent results indicate a correlation between cognitive control impairment and impaired cognitive regulation in adolescents. This correlation suggests that individuals may have challenges while attempting to assess the potential costs and rewards associated with conflict events. This behavior can exacerbate challenges in maintaining positive social relationships, impede the ability to redirect focus away from negative emotions such as despair and suffering and contribute to a more entrenched inclination to avoid and resolve difficulties by choosing suicide as a solution. In addition, the presence of persistent negative thoughts and feelings can often trigger contemplation of suicide, therefore suggesting that cognitive control dysfunction may serve as a significant risk factor for suicidal tendencies.13,29,57,58
The brain regions implicated in cognitive control and attention impairments exhibit strong connections with the anterior cingulate cortex (ACC) and consistently demonstrate links to depression and cognitive impairment.59,60 SI and SA figures indicate that the risk of depression is approximately six times higher than in healthy people.61 Furthermore, Chinese teenagers who experienced SA were significantly more prone to developing depression (adjusted odds ratio for depression: 3.63; P<0.05).14 In accordance with our findings, SA is frequently associated with more severe depression. This phenomenon can be linked to the theoretical framework highlighting “suicide capability”. The framework posits that the transition from ideation to actual behavior is influenced by increasing negative emotional experiences and tolerance for the misery connected with death.12
For the first time, network analysis is a potent empirical method for visualizing interactions among depressive symptoms, cognitive function, and suicidal ideation in SA and SI. Firstly, while comparing SI with SA, it could be observed that SA possesses a distinct and highly interconnected network structure. A possible explanation was that SA has a broader cognitive and depressive symptom distress profile, so external performance for closer relationships in the network.25 Secondly, compared with SA, the network of SI associated with depression and suicidal ideation does not appear to be robust, and this further explains the different causes of SI and SA, as well as their belonging to distinct disease states.16 Meanwhile, the prior study confirmed that individuals with SA demonstrated heightened levels of depressive symptoms and cognitive impairment. These findings may also be utilized to verify the accuracy of the network model’s estimations.25,32,34 However, it is essential to note that attention and comprehensive cognitive ability, considered critical nodes in network analysis, may significantly trigger activation and lead to various suicidal behaviors. Thus, targeting these key nodes can potentially provide widespread symptomatic improvements.62 To sum up, it may be advantageous to incorporate attention as the focal point of cognitive rehabilitation exercises to enhance the pathological condition, attain the objective of addressing depression, and mitigate suicide among teenagers.
The findings of the study are subject to some limitations. This study is classified as a cross-sectional study, and it should be noted that the sample size is relatively small. The lack of longitudinal data has problems establishing causation and generalizing the findings to the adolescent population. Nevertheless, given the importance of this research for the targeted demographic, it remains justifiable to extend its applicability to a broader group in further studies. Furthermore, the present study operationalized SA as a state that manifests across an individual’s entire lifespan without imposing any precise temporal constraints. This limitation can potentially impact the association between SA and suicide. Subsequent investigations may benefit from more precisely delineating the timing of SA occurrences to investigate potential variations in temporal effects. As there is increasing evidence that substance abuse and adolescent suicide share risk factors,63 such as impulse control, pressure events, mood disorders, etc., future research can incorporate the above evidence to investigate adolescent suicide risk and protection mechanisms.
In general, adolescents who have SA and SI exhibit significant cognitive dysfunction as compared to their healthy counterparts. However, it seems that adolescents with SA exhibit more pronounced symptoms of depression and cognitive dysfunction. Impaired attention can serve as biological marker to differentiate between SA and SI in teenagers within the realm of cognitive function. Early intervention in adolescent attention has the potential to improve future adolescent suicidal behavior.
Data Sharing Statement
The original contributions presented in the study are included in the article material. Further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by the Research Committee of the Hebei Provincial Mental Health Center. The patients/participants provided their written informed consent to participate in this study.
Acknowledgments
We are grateful to the subjects and scholars who contributed to this study. At last, thanks to the support of the Hebei Provincial Mental Health Center.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Program of Medical Science Research of Hebei Province (20220700).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Suicide. 2021. Available from https://www.who.int/news-room/fact-sheets/detail/suicide.2021.
2. Franklin JC, Ribeiro JD, Fox KR, et al. Risk factors for suicidal thoughts and behaviors: a meta-analysis of 50 years of research. Psychol Bull. 2017;143(2):187–232. doi:10.1037/bul0000084
3. O’Connor RC, Portzky G. The relationship between entrapment and suicidal behavior through the lens of the integrated motivational-volitional model of suicidal behav ior. Curr Opinion Psyc. 2018;22:12–17. doi:10.1016/j.copsyc.2017.07.021
4. Zygo M, Pawłowska B, Potembska E, Dreher P, Kapka-Skrzypczak L. Prevalence and selected risk factors of suicidal ideation, suicidal te ndencies and suicide attempts in young people aged 13-19 years. Ann agri envir med. 2019;26(2):329–336. doi:10.26444/aaem/93817
5. Parry J. Falling suicide rates in China mask emerging upward trends. BMJ. 2014;348:g4486. doi:10.1136/bmj.g4486
6. Silverman MM, Berman AL, Sanddal ND, O’Carroll PW, Joiner TE. Rebuilding the tower of babel: a revised nomenclature for the study of suicide and suicidal behaviors. part 1: background, rationale, and methodology. Suicide Life-Threatening Behav. 2007;37(3):248–263. doi:10.1521/suli.2007.37.3.248
7. Ose SO, Tveit T, Mehlum L. Non-suicidal self-injury (NSSI) in adult psychiatric outpatients - A nationwide study. J Psychiatr Res. 2021;133:1–9. doi:10.1016/j.jpsychires.2020.11.031
8. Asarnow JR, Porta G, Spirito A, et al. Suicide attempts and nonsuicidal self-injury in the treatment of resistant depression in adolescents: findings from the TORDIA study. J Am Acad Child Adolesc Psychiatry. 2011;50(8):772–781. doi:10.1016/j.jaac.2011.04.003
9. Fox KR, Millner AJ, Franklin JC. Classifying nonsuicidal overdoses: nonsuicidal self-injury, suicide attempts, or neither? Psychiatry Res. 2016;244:235–242. doi:10.1016/j.psychres.2016.07.052
10. Klonsky ED, May AM. Differentiating suicide attempters from suicide ideators: a critical frontier for suicidology research. Suicide Life Threat Behav. 2014;44(1):1–5. doi:10.1111/sltb.12068
11. Klonsky ED, Qiu T, Saffer BY. Recent advances in differentiating suicide attempters from suicide ideators. Curr Opin Psychiatry. 2017;30(1):15–20. doi:10.1097/yco.0000000000000294
12. Klonsky ED, May AM. The three-step theory (3ST): a new theory of suicide rooted in the ”ideation-to-action. Framework. 2015;8(2):114–129. doi:10.1521/ijct.2015.8.2.114
13. Nock MK, Green JG, Hwang I, et al. Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: results from the national comorbidity survey replication adolescent supplement. JAMA Psychiatry. 2013;70(3):300–310. doi:10.1001/2013.jamapsychiatry.55
14. Mars B, Heron J, Klonsky ED, et al. What distinguishes adolescents with suicidal thoughts from those who have attempted suicide? A population-based birth cohort study. J Child Psychol Psyc Allied Dis. 2019;60(1):91–99. doi:10.1111/jcpp.12878
15. Yan Y, Gai X. Prevalence and correlational factors of suicidal ideation and suicide attempts among Chinese adolescents. Frontiers in Psychology. 2022;13:911502. doi:10.3389/fpsyg.2022.911502
16. Masi G, Lenzi F, Fabiani D, Sudano SD, D’Acunto G, Mucci M. Suicidal ideation, suicidal attempts and non-suicidal self-injuries in referred adolescents. Riv Psichiatr. 2020;55(3):168–174. doi:10.1708/3382.33573
17. Tang J, Yu Y, Wu Y, et al. Association between non-suicidal self-injuries and suicide attempts in Chinese adolescents and college students: a cross-section study. PLoS One. 2011;6(4):e17977. doi:10.1371/journal.pone.0017977
18. Goldston DB, Daniel SS, Erkanli A, et al. Psychiatric diagnoses as contemporaneous risk factors for suicide attempts among adolescents and young adults: developmental changes. J Consult Clin Psychol. 2009;77(2):281–290. doi:10.1037/a0014732
19. Gould MS, Greenberg T, Velting DM, Shaffer D. Youth suicide risk and preventive interventions: a review of the past 10 years. J Am Acad Child Adolesc Psychiatry Apr. 2003;42(4):386–405. doi:10.1097/01.Chi.0000046821.95464.Cf
20. Stewart JG, Glenn CR, Esposito EC, Cha CB, Nock MK, Auerbach RP. Cognitive control deficits differentiate adolescent suicide ideators from attempters. J Clin Psychiatry. 2017;78(6):e614–e621. doi:10.4088/JCP.16m10647
21. Harrison JE, Barry H, Baune BT, et al. Stability, reliability, and validity of the THINC-it screening tool for cognitive impairment in depression: a psychometric exploration in healthy volunteers. Int J Methods Psychiatr Res. 2018;27(3):e1736. doi:10.1002/mpr.1736
22. McIntyre RS, Best MW, Bowie CR, et al. The THINC-integrated tool (THINC-it) screening assessment for cognitive dysfunction: validation in patients with major depressive disorder. J Clin Psychiatry. 2017;78(7):873–881. doi:10.4088/JCP.16m11329
23. Chen H, Hu X, Gao J, Han H, Wang X, Xue C. Early effects of repetitive transcranial magnetic stimulation combined with sertraline in adolescents with first-episode major depressive disorder. Front Psychiatry. 2022;13:853961. doi:10.3389/fpsyt.2022.853961
24. Diao X, Luo D, Wang D, et al. Lurasidone versus quetiapine for cognitive impairments in young patients with bipolar depression: a randomized, controlled study. Pharmaceuticals. 2022;1511:1403. doi:10.3390/ph15111403
25. Richard-Devantoy S, Szanto K, Butters MA, Kalkus J, Dombrovski AY. Cognitive inhibition in older high-lethality suicide attempters. Int J Geriatr Psychiatry. 2015;30(3):274–283. doi:10.1002/gps.4138
26. Richard-Devantoy S, Berlim MT, Jollant F. A meta-analysis of neuropsychological markers of vulnerability to suicidal behavior in mood disorders. Psychol Med. 2014;44(8):1663–1673. doi:10.1017/s0033291713002304
27. Wenzel A, Beck AT.A cognitive model of suicidal behavior: theory and treatment. Am J Appl Psychol. 2008;12(4):189–201. doi:10.1016/j.appsy.2008.05.001
28. Keilp JG, Gorlyn M, Oquendo MA, Burke AK, Mann JJ. Attention deficit in depressed suicide attempters. Psychiatry Res. 2008;159(1–2):7–17. doi:10.1016/j.psychres.2007.08.020
29. Keilp JG, Gorlyn M, Russell M, et al. Neuropsychological function and suicidal behavior: attention control, memory and executive dysfunction in suicide attempt. Psychol Med. 2013;43(3):539–551. doi:10.1017/s0033291712001419
30. Cha CB, Najmi S, Park JM, Finn CT, Nock MK. Attentional bias toward suicide-related stimuli predicts suicidal behavior. J Abnorm Psychol. 2010;119(3):616–622. doi:10.1037/a0019710
31. Sommerfeldt SL, Cullen KR, Han G, Fryza BJ, Houri AK, Klimes-Dougan B. Executive attention impairment in adolescents with major depressive disorder. J Clin Child Adolesc Psychol. 2016;45(1):69–83. doi:10.1080/15374416.2015.1072823
32. Keilp JG, Sackeim HA, Brodsky BS, Oquendo MA, Malone KM, Mann JJ. Neuropsychological dysfunction in depressed suicide attempters. Am J Psychiatry. 2001;158(5):735–741. doi:10.1176/appi.ajp.158.5.735
33. Han G, Klimes-Dougan B, Jepsen S, et al. Selective neurocognitive impairments in adolescents with major depressive disorder. J Adolesc. 2012;35(1):11–20. doi:10.1016/j.adolescence.2011.06.009
34. Lalovic A, Wang S, Keilp JG, Bowie CR, Kennedy SH, Rizvi SJ. A qualitative systematic review of neurocognition in suicide ideators and attempters: implications for cognitive-based psychotherapeutic interventions. Neurosci Biobehav Rev. 2022;132:92–109. doi:10.1016/j.neubiorev.2021.11.007
35. Fried EI, Nesse RM. The impact of individual depressive symptoms on impairment of psychosocial functioning. PLoS One. 2014;9(2):e90311. doi:10.1371/journal.pone.0090311
36. Jones PJ, Ma R, McNally RJ. Bridge centrality: a network approach to understanding comorbidity. Multi Behav Res Mar-Apr. 2021;56(2):353–367. doi:10.1080/00273171.2019.1614898
37. Schmittmann VD, Cramer AOJ, Waldorp LJ, Epskamp S, Kievit RA, Borsboom D. Deconstructing the construct: a network perspective on psychological phenomena. New Ideas Psyc. 2013;31(1):43–53. doi:10.1016/j.newideapsych.2011.02.007
38. Hamilton M. Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol. 1967;6(4):278–296. doi:10.1111/j.2044-8260.1967.tb00530.x
39. Auerbach RP, Millner AJ, Stewart JG, Esposito EC. Identifying differences between depressed adolescent suicide ideators and attempters. J Affect Disord. 2015;186:127–133. doi:10.1016/j.jad.2015.06.031
40. Zheng YP, Zhao JP, Phillips M, et al. Validity and reliability of the Chinese hamilton depression rating scale. Br J Psychiatry. 1988;152(5):660–664. doi:10.1192/bjp.152.5.660
41. Osman A, Gutierrez PM, Kopper BA, Barrios FX, Chiros CE. The positive and negative suicide ideation inventory: development and validation. Psychol Rep. 1998;82(3 Pt 1):783–793. doi:10.2466/pr0.1998.82.3.783
42. Chang HJ, Lin CC, Chou KR, Ma WF, Yang CY. Chinese version of the positive and negative suicide ideation: instrument development. J Adv Nurs. 2009;65(7):1485–1496. doi:10.1111/j.1365-2648.2009.05005.x
43. Han H, Hou Y, Yao S, et al. The relationship between cognitive dysfunction through thinc-integrated Tool (THINC-it) and psychosocial function in Chinese patients with major depressive disorder. Frontiers in Psychiatry. 2021;12:763603. doi:10.3389/fpsyt.2021.763603
44. Hou Y, Yao S, Hu S, et al. PSYCHOMETRIC properties of the Chinese version of the THINC-it tool for cognitive symptoms in patients with major depressive disorder. J Affect Disord. 2020;273:586–591. doi:10.1016/j.jad.2020.03.146
45. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/bf03193146
46. Cohen J, Cohen J, Cohen JW, et al. Statistical power analysis for the behavioral science. Braz J Phys Ther. 1988;31(4):499–500. Doi:10.1016/0198-9715(90)90050-4
47. Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, Borsboom D. qgraph: network visualizations of relationships in psychometric Data. J Stat Software. 2012;48(4):1–18. doi:10.18637/jss.v048.i04
48. Lauritzen SL. Graphical Models. Clarendon Press; 1996.
49. Friedman J, Hastie T, Tibshirani R. Sparse inverse covariance estimation with the graphical lasso. Biostatistics. 2008;9(3):432–441. doi:10.1093/biostatistics/kxm045
50. Epskamp S, Fried EI. A tutorial on regularized partial correlation networks. Psychol Methods. 2018;23(4):617–634. doi:10.1037/met0000167
51. Opsahl T, Agneessens F, Skvoretz J. Node centrality in weighted networks: generalizing degree and shortest paths. Social Networks. 2010;32(3):245–251. doi:10.1016/j.socnet.2010.03.006
52. Deng J, Wang MC, Shou Y, Gao Y. Core features of callous-unemotional traits: network analysis of the inventory of callous-unemotional traits in offender and community samples. J Clin Psychol. 2021;77(6):1487–1498. doi:10.1002/jclp.23090
53. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50(1):195–212. doi:10.3758/s13428-017-0862-1
54. Horesh N. Self-report vs. computerized measures of impulsivity as a correlate of suicidal behavior. Crisis. 2001;22(1):27–31. doi:10.1027//0227-5910.22.1.27
55. Legris J, Links PS, van Reekum R, Tannock R, Toplak M. Executive function and suicidal risk in women with borderline personality disorder. Psychiatry Res. 2012;196(1):101–108. doi:10.1016/j.psychres.2011.10.008
56. Malloy-Diniz LF, Neves FS, Abrantes SS, Fuentes D, Corrêa H. Suicide behavior and neuropsychological assessment of type I bipolar patients. J Affect Disord. 2009;112(1–3):231–236. doi:10.1016/j.jad.2008.03.019
57. Joormann J, Quinn ME. Cognitive processes and emotion regulation in depression. Depress Anxiety. 2014;31(4):308–315. doi:10.1002/da.22264
58. Rahdar A, Galván A. The cognitive and neurobiological effects of daily stress in adolescents. Neuroimage. 2014;92:267–273. doi:10.1016/j.neuroimage.2014.02.007
59. Carter CS, van Veen V. Anterior cingulate cortex and conflict detection: an update of theory and data. Cogn Affect Behav Neurosci. 2007;7(4):367–379. doi:10.3758/cabn.7.4.367
60. Fan J, McCandliss BD, Fossella J, Flombaum JI, Posner MI. The activation of attentional networks. Neuroimage. 2005;26(2):471–479. doi:10.1016/j.neuroimage.2005.02.004
61. Gawęda Ł, Pionke R, Krężołek M, Frydecka D, Nelson B, Cechnicki A. The interplay between childhood trauma, cognitive biases, psychotic-like experiences and depression and their additive impact on predicting lifetime suicidal behavior in young adults. Psychol Med. 2020;50(1):116–124. doi:10.1017/s0033291718004026
62. Borsboom D. A network theory of mental disorders. World Psychiatry. 2017;16(1):5–13. doi:10.1002/wps.20375
63. Resko SM, Kruman Mountain S, Browne S, Kondrat DC, Kral M. Suicidal ideation and suicide attempts among women seeking treatment for substance use and trauma symptoms. Health Soc Work. 2018;43(2):76–83. doi:10.1093/hsw/hly004
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Network Analysis of Anxiety, Insomnia, Depression, and Suicide Attempts in Chinese Outpatients with Somatic Symptom Disorder
Fang J, Tang H, Liao H, Zhong Y, Li Y, Liao Y, Li Y
Neuropsychiatric Disease and Treatment 2025, 21:1091-1105
Published Date: 22 May 2025
A Network Analysis of the Interrelationships Between Depression, Anxiety, Insomnia and Non-Suicidal Self-Injury in Middle School Students
Qian H, Zhang J, Duan X, Wu TM, Xie YF, Yang BX, Luo D, Liu LZ, Yu P
Psychology Research and Behavior Management 2026, 19:570928
Published Date: 12 January 2026