Back to Journals » Eye and Brain » Volume 18
AstroOphthalmology: Basic and Pathophysiological Concepts of Space-Induced Ocular Changes
Authors Cheraqpour K ![]() , Shahriari M, Ghazi M, Heydari N, Moshfeghi S, Mousavi Ganji SM, Asgari S, Cheraqpour S
, Shahriari M, Ghazi M, Heydari N, Moshfeghi S, Mousavi Ganji SM, Asgari S, Cheraqpour S
Received 22 March 2026
Accepted for publication 19 May 2026
Published 22 May 2026 Volume 2026:18 611235
DOI https://doi.org/10.2147/EB.S611235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sotiria Palioura
Kasra Cheraqpour,1 Mansoor Shahriari,2 Mahya Ghazi,3,4 Navid Heydari,5 Saeedreza Moshfeghi,3 Seyed Mohammad Mousavi Ganji,6 Sina Asgari,7 Shaqayeq Cheraqpour7
1Eye Research Center, Farabi Eye Hospital, Tehran University of Medical Sciences, Tehran, Iran; 2Imam Hossein Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 3Eye Research Center, Department of Ophthalmology, Isfahan University of Medical Sciences, Isfahan, Iran; 4Ophthalmic Research Center, Research Institute for Ophthalmology and Vision Science, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 5School of Medicine, Ahvaz Jondishapur University of Medical Sciences, Ahvaz, Khuzestan, Iran; 6Department of Cardiology, Faculty of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran; 7School of Medicine, TeMS.C., Islamic Azad University, Tehran, Iran
Correspondence: Kasra Cheraqpour, Eye Research Center, Farabi Eye Hospital, Tehran University of Medical Sciences, Tehran, Iran, Tel +982155421080, Email [email protected]
Abstract: Long-duration space missions pose a considerable risk to eye health, and visual dysfunction is recognized as a primary health concern for astronauts. Hence, we have developed a series of review reports to study the effects of space on the eye, called AstroOphthalmology (including Basics, Ocular Anterior Segment, Ocular Posterior Segment). This report serves as the first report of our series, and integrates the current insights into the pathophysiological consequences of the space environment on the eye. The two key space-specific stressors include microgravity and cosmic radiation. Both stressors are the interconnected pathways of oxidative stress and mitochondrial dysfunction, which inflict damage on cellular components and disrupt the function of essential ocular tissues. Microgravity triggers a cephalad fluid shift, which leads to vascular congestion, changes in hemodynamics, and increased intracranial pressure. The aforementioned changes are considered to be culprits in the onset of spaceflight-associated neuro-ocular syndrome (SANS). Exposure to galactic cosmic radiation and solar particle events presents a substantial risk for the formation of cataracts, retinal cotton-wool spots, and optic neuropathy. This review indicates that ocular damage during spaceflight is influenced by multiple factors, resulting from the synergistic interaction of fluid shifts and radiation. In addition to pathophysiology, we summarize the current in-flight evaluations such as optical coherence tomography and fundoscopy. Future research should focus on assessing combined countermeasures and establishing predictive biomarkers to mitigate these risks, which is imperative for the success of future lunar and Martian missions.
Keywords: space, spaceflight, microgravity, radiation, eye, ophthalmology
Introduction
Long-duration spaceflight (LDSF) has a profound effect on the human body due to extraordinary conditions, including microgravity, radiation, and hypercapnia. It is acknowledged that LDSF induces multi-systemic effects, including bone demineralization, muscle atrophy, cardiovascular deconditioning, vestibular and sensory imbalance, alterations in metabolic and nutritional status, and dysregulation of the immune system. LDSF also has the potential to induce structural and functional changes in the eyes, posing risks to both the safety and success of space missions.1 Wernher von Braun, a German-American space engineer, once remarked, “Man is not made for space. But with the help of biologists and medical doctors, he can be prepared and accommodated.” This viewpoint underscores the importance of medical proficiency to establish a microcosm of human existence in a challenging environment.2
The influence of microgravity and cosmic radiation exposure ultimately leads to a decline in the health of the ocular system, which may pose significant acute and chronic risks to astronauts. National Aeronautics and Space Administration (NASA) has considered visual impairment as a high-priority risk for future exploration class missions, acknowledging its potential to affect crew performance during critical operations such as landing, docking, and extravehicular activities.3,4 Visual changes were reported by 23% and 48% of astronauts on short-duration and long-duration missions, respectively.5 The space environment can impact both anterior and posterior segments of the eye. A collection of findings, initially termed spaceflight-associated neuro-ocular syndrome (SANS), revealed structural and functional changes in astronauts. These ocular manifestations include optic disc edema, globe flattening, chorioretinal folds, and hyperopic refractive shifts.6 Chorioretinal folds are a prominent structural characteristic of SANS, consisting of undulations in the choriocapillaris, Bruch’s membrane, and the retinal pigment epithelium above.7,8 While SANS is the most recognized and unique effect of spaceflight on eyes, the other conditions and concerns during or after spaceflights such as dry eye disease, cataract, glaucoma, and trauma present specific challenges and require distinct attention.
Given the scarcity of in-flight experimental opportunities, much of the mechanistic insight into ocular changes caused by space has been obtained through ground-based analogues. The head-down tilt bed rest, dry immersion, and animal irradiation models have been essential in isolating the roles of cephalad fluid shift and radiation in ocular pathophysiology.9 However, considerable knowledge gaps still persist; the relative contributions of cephalad fluid shift, altered cerebrospinal fluid dynamics, radiation-induced damage, and their synergistic effects are not fully elucidated. Furthermore, early and reliable biomarkers for SANS are lacking, and the long-term effects of partial-gravity exposure on the lunar and Martian surfaces remain uncertain. Hence, we have decided to develop a series of AstroOphthalmology—studying the effects of space on the eye—which will contain several review reports (including Basics, Ocular Anterior Segment, Ocular Posterior Segment) to cover different aspects of space travel on ocular health.
Although numerous narrative reviews have described the clinical features of SANS or summarized potential countermeasures, few have tried to comprehensively integrate the molecular and cellular pathways that connect the two dominant stressors—microgravity and radiation—to specific ocular tissue responses. This review article, as the first report of our series, offers a meticulous overview of the environmental factors that impact the eyes in space, as well as the basic biological mechanisms that are hypothesized to underlie these events. Herein, we aim to provide a comprehensive synthesis of the current understanding of how microgravity and space radiation impact the eye. Specifically, we examine the fundamental biological mechanisms—particularly fluid redistribution, oxidative stress, and mitochondrial dysfunction—that underlie ocular pathology induced by space conditions. We also summarize the current in-flight screening protocols and highlight the emergence of new diagnostic tools. By integrating these diverse lines of evidence, this review serves as a roadmap for researchers and clinicians dedicated to protecting astronaut vision in the forthcoming era of deep-space exploration.
Space-Specific Stressors
Microgravity
The role of gravity in ocular health is critical, as it regulates intraocular pressure (IOP), aqueous humor dynamics, and aids in the alignment of the eyes. It also supports the structural integrity of the eye. Exposure to microgravity can lead to disturbances in these well-adjusted mechanisms.10 Microgravity is defined as a reduced gravitational force (compared to normal 1 g), resulting in a sensation of weightlessness for the body. Spaceflight conditions do not represent the total absence of gravity; rather, the gravitational force is significantly decreased to values that fall between 0.0001 and 0.000001 g.11 This can have a substantial impact on blood circulation, the lymphatic system, intracranial pressure (ICP), and cerebrospinal fluid (CSF) hemodynamics.10
Blood Circulation
The absence of gravitational forces from Earth results in numerous adaptations and maladaptations in blood circulation.12 Studies have underscored the physiological responses to microgravity, which include diminished venous pressures, a reduction in plasma volume, and orthostatic intolerance. In space, the absence of blood pressure gradients that are usually present under Earth’s gravity leads to a redistribution of mean arterial pressure, ultimately causing facial swelling and a decrease in volume in the lower limbs.13 At 1g, the arterial pressure in the head is lower (approximately 70 mmHg), while the blood pressure in the feet is considerably higher (around 200 mmHg). Within a few minutes of being in a microgravity environment, roughly 2 liters of blood are redistributed from the lower body to the cephalic area (Figure 1). Consequently, blood pressure in the upper body rises, heart rate diminishes due to the activation of neck baroreceptors, vasodilation is observed, and mean arterial pressure decreases.14 A further impact of microgravity on venous adaptations is the heightened coagulation in the cephalad venous system.15 The lack of Earth’s gravitational force results in increased venous pressure and decreased cranial venous drainage. This situation can lead to venous distension, endothelial damage, and a risk of hypercoagulability.15 Moreover, microgravity affects the migration of endothelial cells, which are vital for maintaining the structure and stability of vascular cell walls. Microgravity conditions effectively decrease the compression of blood vessels from the surrounding tissues throughout the body, which in turn lowers central venous pressure (CVP).16
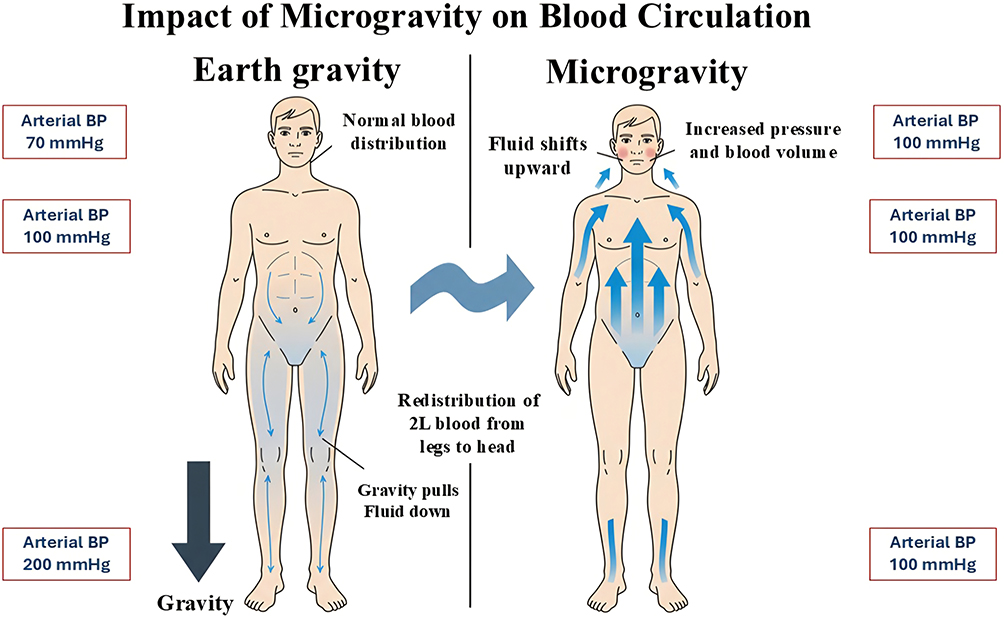 |
Figure 1 Impact of microgravity on blood circulation. |
In microgravity, the stasis of cerebral venous blood due to cephalad fluid shifts may lead to interruptions in nutrient delivery and metabolic activity.17 This can result in impaired adenosine triphosphate (ATP) generation, which may subsequently decrease Na+/K+ ATPase activity. The inability to maintain the physiologic low levels of intracellular Na+ can lead to the occurrence of edema. Areas with a higher demand for ATP, such as the optic nerve head that contains unmyelinated nerve fibers, may be more severely affected by this stasis, resulting in optic disc edema in SANS.18
Lymphatic System
The lymphatic system is essential for the prevention and resolution of edema, the maintenance of normal tissue fluid volume, and the facilitation of immunologic responses. Furthermore, it plays a significant role in the clearance of CSF from the cranial region.19 Disruption of CSF drainage into the lymphatics during spaceflight could be correlated with several pathological issues, such as SANS.19,20 Microgravity conditions hinder lymphatic function due to various deconditioning mechanisms, including the loss of hydrostatic pressure, decreased sensory information, reduced mechanical stimulation, and changes in Starling-Landis pressure.16 However, the significance of the ocular glymphatic pathway is an emerging and largely unverified concept. There is a deficiency of direct evidence regarding impaired glymphatic clearance in astronauts, with the majority of data originating from rodent models or indirect measurements. As a result, this hypothesis should be interpreted as provisional and in need of further validation.
Intracranial and Intraocular Pressures
The reduction in CVP impacts the ocular transmural pressure. An equilibrium is present between ICP, which pushes against the eye, and the IOP, which counters this force. The decrease in CVP due to microgravity leads to an increase in ICP. It has been hypothesized that a disproportionate elevation in ICP in comparison to IOP results in a decrease in the translaminar pressure gradient (TLPG) across the posterior part of the eye, leading to compression at the back of the eye.21,22 Nonetheless, this hypothesis is still a subject of ongoing debate. A number of studies have found no reliable correlation between ICP estimates and the severity of SANS, and some have reported optic disc edema even in cases where significant ICP elevation is not present. Moreover, alternative (and potentially complementary) hypotheses have been suggested, such as impaired drainage of cerebral veins and venous stasis within the vortex veins, modifications in ocular glymphatic clearance, and variations in scleral compliance.23 Therefore, SANS is probably a multifactorial condition where increased ICP is a contributing factor, though it may not be the sole causative element.
In terrestrial settings, choroid plexus is the primary site for the production of CSF, which drains into the lower pressure cervical venous system.24 The drainage of CSF, lymphatics, and vasculature is enhanced by the influence of gravity. In microgravity conditions, the increase in venous cross-sectional area and alterations in blood flow velocity indicate potential for venous congestion.25,26 The internal jugular veins (IJV) are the main outflow pathway. Such venous congestion may compromise the outflow from cerebral and ocular veins, including the vortex veins, which facilitate the majority of ocular blood drainage. A decrease in venous outflow may lead to reduced CSF outflow, resulting in increased ICP and transmission along the optic nerve sheath (ONS). The choroid is the primary blood supply to the ocular tissues.27 The significance for ocular function is that a localized increase in choroidal thickness at the posterior globe may lead to foveal displacement, resulting in a hyperopic shift and an increase in IOP.28,29 Various studies have demonstrated that acute exposure to both simulated and actual microgravity environments result in an increase in IOP. In the initial 15 minutes of exposure to microgravity, IOP shows a 92% increase relative to baseline measurements.30 The reasons for this increase after acute exposure to microgravity may include increased choroidal thickness, elevated episcleral venous pressure, and a narrowing of the anterior chamber angle.31–33 It was later noted during the flight that IOP returns to levels that were similar to pre-flight baselines. The decrease in IOP with chronic exposure may be linked to an increase in the drainage of aqueous humor and a reduction in its synthesis, which may be a consequence of dehydration.3
Radiation
While the magnetic field in low Earth orbit (LEO) offers a degree of protection against radiation, astronauts venturing beyond LEO are no longer shielded by the magnetosphere, thus facing exposure to solar particle events (SPEs) and galactic cosmic radiation (GCR) that originate from outside the solar system (MM). SPEs are largely constituted of low linear energy transfer (LET) protons, with levels surpassing 106 protons/cm2.34 These protons are relatively easy to shield against using spacecraft hulls, but they can pose risks during extravehicular activities (EVA).35 On the other hand, GCR is composed of high LET protons (87%), alpha particles (12%), and a small fraction of high charge and energy ions (1–2%).36
Studies have established that radiation exposure can result in injury to eye structures, contributing to conditions like dry eye, cataract, retinal detachment, glaucoma, madarosis, abnormal vascularity, and optic neuropathy.37 Astronauts on International Space Station (ISS) are exposed to radiation doses that are nearly 200 times higher than those on Earth. When on the surfaces of the Moon and Mars, they will experience even greater radiation exposure, estimated at around 2.6 and 3.5 times the radiation levels on the ISS, respectively.38 Research has shown a correlation between the radiation dose a subject receives and the development of ocular complications.39–42 The latest NASA standards impose a limit of 600mSv for radiation exposure over the career of American astronauts, whereas other international space agencies allow for exposure levels up to 1000mSv.43 Although the majority of ISS missions operate well below this limit, a Mars mission spanning 1 to 2 years may exceed it.44
Cataract
Research has shown that radiation can lead to the destruction of aromatic and sulfur-containing amino acids, as well as aggregation, crosslinking, dissociation, fragmentation, and partial folding. Specifically, crystallins, which are the primary protein components of the lens, are significantly influenced by the aggregation of proteins and the degradation of aromatic amino acid residues. This results in a dose-dependent reduction in fluorescence intensity, which alters the structure of aromatic compounds. Consequently, these changes impact lens transparency and heighten the likelihood of cataract formation.45 In light of the elevated radiation doses encountered during deep space missions, investigations are being carried out to assess the effects of low- and high-dose radiation exposure on the crystalline lens. Results from Phase 2 of the 5-year NASA Study of Cataract in Astronauts (NASCA) revealed that the progression rate of cortical cataracts was related to the amount of space radiation exposure. However, no association was identified between space radiation and nuclear or posterior subcapsular cataracts.46
Cotton Wool Spots
Retinal cotton wool spots (CWSs) have been extensively recorded following LDSF and are thought to be indicative of radiation exposure. After LDSF, CWSs were documented in four astronauts, three of whom had engaged in EVA during their missions. Since EVA suits provide less radiation shielding than the ISS, these astronauts may have been exposed to higher radiation levels. In another case, one astronaut exhibited a single CWS surrounded by a superficial retinal hemorrhage after an ISS mission, suggesting concurrent localized vascular damage. CWSs are a well-known side effect of radiation therapy, which typically involves short bursts of high-dose radiation that far exceed the prolonged low doses encountered by astronauts, and their appearance may be delayed for months to years following radiation exposure. It is hypothesized that the CWSs observed in astronauts may represent the cumulative outcome of a relatively low but prolonged radiation dose.3 However, the small number of cases limits the ability to draw definitive conclusions. It remains uncertain whether CWSs are a result of cumulative radiation exposure, an interaction with microgravity-induced vascular changes, or an individual susceptibility. Furthermore, the occurrence of CWSs is not universal among astronauts with similar mission profiles, which underscores the necessity for larger, controlled studies.
Optic Neuropathy
Radiation exposure has been shown to significantly affect the optic nerve, with a substantial body of literature highlighting an increased risk of optic neuropathy following external beam radiation therapy. Through these investigations, it has been determined that the maximum radiation dose to the anterior visual pathway is a key factor influencing the development of radiation-induced optic neuropathy, with evidence suggesting that this pathway can tolerate no more than 50Gy of cumulative radiation in fractions of less than 2 Gy.47–50 The inquiry into whether chronic, low-dose, mixed-field radiation from deep space can cause clinically significant optic neuropathy remains an open question. Currently, the risk is extrapolated from radiotherapy data and has not been verified in the context of space missions.
Phosphene
During deep space missions, astronauts participating in the Apollo program observed flashes of light, known as phosphenes, in their vision which are thought to be caused by high energy radiation particles impacting the retina. Astronauts aboard the ISS have similarly reported experiencing these flashes. Investigations indicated that these phosphenes result from GCR and SEPs interacting with the retina, optic nerve, and occipital cortex.51 Comparable phosphenes are also noted in ocular oncology and in radiotherapy treatments directed at the head and neck area. The most frequently observed phosphenes manifest as either moving or stationary white dots or lines. Nevertheless, only a small number of astronauts have reported seeing blue phosphenes.52–54
Hypercapnia
The atmospheric CO2 concentration on Earth is 0.04%, with PCO2 of 0.3 mmHg at an atmospheric pressure of 760 mmHg. In contrast, the PCO2 levels aboard the International Space Station vary significantly, ranging from 1 to 9 mmHg, and are usually found between 2.3 and 5.3 mmHg. Additionally, while air convection occurs on Earth, it is absent in space, which may lead to localized regions with particularly elevated PCO2 levels.55 While these levels are not high enough to result in CO2 toxicity, they can still impact vascular tone, as shown by a greater frequency of headaches.56 CO2 serves as a powerful vasodilator for systemic arteries, which leads to an increase in cerebral blood flow. This rise in flow is likely a contributing factor to the increase in ICP, worsening issues related to cranial venous congestion and facilitating the emergence of SANS.57,58 It has been concluded that the elevated PCO2 experienced during spaceflight, potentially exacerbated by stagnant PCO2 around the mouth in microgravity, may be linked to optic disc edema, particularly when the air circulator is ineffective or when an individual remains in a static position for extended periods. Nevertheless, the observed increases in peripapillary retinal nerve fiber layer thickness are believed to be primarily driven by hypoxia rather than hypercapnia.59
Pathophysiological Pathways
Oxidative Stress
Oxidative stress induced by spaceflight may result in certain visual abnormalities in astronauts.60 The body’s antioxidant defense mechanisms may become overwhelmed in microgravity, leading to oxidative damage in tissues, including the eyes. Oxidative stress occurs when there is an imbalance between the production of reactive oxygen species (ROS) and the body’s antioxidant defenses.61 ROS are molecules that can damage cellular components like DNA, proteins, and lipids. Antioxidants are molecules that help protect the body from oxidative damage by neutralizing ROS. The eye is particularly susceptible to oxidative stress due to its high metabolic rate and exposure to environmental stressors, including light and oxygen.62 The levels of various biomarkers in the blood and urine of astronauts were evaluated in a study conducted before, during, and after space missions. The results demonstrated that the levels of 8-hydroxy-2′-deoxyguanosine (8-OHdG), a known marker of DNA damage, were significantly elevated during spaceflight when compared to pre-flight levels and were closely correlated with telomere length.63 This indicates that the increased oxidative stress experienced during spaceflight may play a role in the development of SANS.63
The retinal layer is highly sensitive to oxidative injury due to its elevated oxygen consumption, the presence of oxidizable unsaturated lipids, and its limited antioxidant defenses.64 The oxidative damage may result in cell death, at least partially through apoptosis, causing morphological changes in the inner nuclear and ganglion cell layers, which may eventually result in a decline in retinal function.65 A mouse experiment has shown various impacts on the retina as a result of spaceflight.66 These impacts include a decrease in retinal thickness, a reduction in cone photoreceptor count, and an increase in oxidative stress. Additionally, there was a noted rise in 4-hydroxynonenal (4-HNE), a marker of oxidative damage to the retina, which was found to be elevated in cone photoreceptors, the retinal inner nuclear layer (INL), and the ganglion cell layer (GCL) after spaceflight relative to terrestrial control mice.66 In another study, ten-week-old male C57BL/6 mice were transported to the ISS aboard Space-X 24 for 35 days and returned to Earth alive.67 Immunofluorescence evaluations showed an increase in retinal oxidative stress and apoptotic cell death after the spaceflight. The electroretinography (ERG) data indicated that the average amplitudes of the a- and b-waves were significantly reduced (by 39% and 32%, respectively) compared to habitat ground controls. These findings imply that the conditions of spaceflight induce oxidative stress in the retina, which may lead to damage in photoreceptor cells and impair retinal function.67
Mitochondrial Dysfunction
Mitochondria are fundamental cellular organelles that are responsible for energy generation through oxidative phosphorylation.68 They are crucial in regulating apoptosis and ensuring cellular homeostasis, neuronal excitability, and synaptic transmission.68 In the eye, mitochondria play a vital role in the transmission of visual information from the retina to the brain, and they are densely packed in the axons of retinal ganglion cells. The inner segments of retinal photoreceptors are rich in mitochondria, which are essential for the renewal of outer segments and the process of phagocytosis.69 The phenomenon of microgravity and the augmented exposure to galactic cosmic radiation during spaceflight are well-documented to exert considerable effects on mitochondrial function.68 Recent investigations utilizing multi-omics and systems biology, which analyzed data from 59 astronauts and mice, along with findings from NASA’s GeneLab, have shown that mitochondrial stress is a common phenotype observed in spaceflight. This notable study illustrates the significant repercussions of spaceflight on mitochondrial function, leading to altered gene expression, weakened antioxidant defenses, and increased oxidative stress.70 While this finding is noteworthy, it is derived from a single multi-omics analysis and has not yet been independently validated through dedicated ocular tissue studies. Mao et al explored the consequences of spaceflight on mitochondrial function and oxidative stress in mice, indicating that the spaceflight environment resulted in mitochondrial dysfunction and an increase in oxidative stress.71 The research highlighted changes in the expression of genes related to mitochondrial function, as well as shifts in antioxidant levels and markers of oxidative damage observed in the study mice. This included significant rises in the levels of 4-hydroxynonenal (4-HNE) protein, a marker for lipid peroxidation, in the retina following spaceflight, along with notable modifications in the genes associated with a mitochondria-related apoptotic pathway in the ocular tissue of mice after spaceflight compared to ground-control mice.71 The correlation between systemic mitochondrial changes and specific ocular pathologies, such as SANS or cataracts, remains to be established; functional validation in retinal and choroidal cells under real or simulated space conditions is still required.
Immunologic and Inflammatory Responses
Crucian et al studied the dynamics of plasma cytokine levels in astronauts during prolonged space missions aboard the International Space Station (ISS).72 The research involved collecting plasma samples from 28 crewmembers at multiple time points: pre-flight, in-flight, and post-flight, with a focus on understanding the changes in the immune system and the potential health risks related to space travel.72 Samples were collected at various intervals, including before, during, and after the flight, to capture the fluctuations in cytokine levels. It was found that while baseline cytokine levels were generally low, spaceflight caused significant increases in certain cytokines, especially IL-8 and TNFα, indicating a mild inflammatory response.72 Elevated levels of chemokines such as CCL2, CCL4, and CXCL5 further supported the notion of chronic inflammation during spaceflight.73 Notably, plasma levels of IL-1ra, an inhibitor of the proinflammatory effects of IL-1, were consistently elevated during spaceflight. This increase may represent an adaptive physiological response to inflammatory stress. The research highlights the importance of monitoring cytokine levels as biomarkers for assessing immune system health and the potential health risks associated with extended space missions.72
The alterations caused by microgravity can lead to a reduction in lymphocyte and monocyte counts, thus impairing immune function.74 Studies have indicated that spaceflight results in decreased cytokine production, which makes astronauts more prone to infections.75 This was brought to light in research by Rooney et al, which identified a potential relationship between stress induced by spaceflight and immune dysregulation, contributing to the reactivation of latent herpes viruses in astronauts.76 The study observed increased shedding of these viruses in bodily fluids during and after missions, highlighting the potential health risks associated with viral reactivation upon returning to Earth.76
Tissue-Based Cellular and Molecular Interactions
Extended exposure to microgravity and space radiation causes significant physiological and pathological changes within human biology. At the cellular level, the predominant pathological effects of microgravity and cosmic radiation involve structural modifications resulting from free radical-mediated molecular damage.71,77,78
Cornea
Long-term exposure to microgravity has been associated with corneal edema, thickening, and tear film instability.79–81 Also, GCR and SEPs are capable of inducing DNA damage, oxidative stress, and apoptosis in the cornea.82 As the outermost layer of the eye, the cornea may face a specific challenge: lunar dust. The cornea may be detrimentally influenced by molecular changes associated with long-term exposure to low levels of dust.37 Recent findings have revealed that even chronic exposure to low concentrations of lunar dust can elicit a molecular response in corneal tissue. As a result, lunar dust exposure may impact a variety of pathways in ocular tissues, such as oxidative stress response, mitochondrial dysfunction, fibrosis, epithelial healing, TGF-beta signaling, extracellular matrix remodeling, and cellular proliferation.83
Retina
In a research study, C57BL/6 mice were launched into the ISS. After completing a 35-day mission, the mice were brought back to Earth alive.84 They were subsequently euthanized, and ocular tissues were gathered for analysis. The immunohistochemical analysis of the retina revealed that the flight mice had an increased expression of aquaporin-4 (AQP-4) compared to the control group, which strongly indicated a disturbance in the integrity of the blood-retinal barrier (BRB). Additionally, there was a significant increase in the expression of platelet endothelial cell adhesion molecule-1 (PECAM-1) and a decrease in the expression of the BRB-related tight junction protein, Zonula occludens-1 (ZO-1). Proteomic analysis indicated that numerous key proteins and pathways involved in cell death, cell cycle, immune response, mitochondrial function, and metabolic stress were significantly altered in the flight mice when compared to ground control animals. These results suggest a complex cellular response that may affect retinal structure and BRB integrity after prolonged spaceflight.84
The role of retinal pigment epithelium (RPE) is fundamental in maintaining the BRB, as it is involved in the metabolic activities of the visual cycle. Evidence from studies suggests that simulated microgravity can cause detrimental effects on human RPE cells in vitro, including alterations in the cytoskeleton and gene expression.85,86 In a study, human RPE cells were exposed to simulated microgravity (0.01 g) for 24 hours using a rotating bioreactor designed by NASA. The analysis of these cells was performed 48 hours after the rotation to detect the levels of prostaglandin E2 (PGE2) production, which serves as a marker for inflammatory responses and is a known risk factor for RPE cells. The findings demonstrated DNA breaks in RPE cells and an increase in PGE2 synthesis. Additionally, it was found that the negative impact of simulated microgravity on RPE cells could be reduced or eliminated by pretreatment with cysteine, an agent recognized for its anti-inflammatory effects.85 One study reported that simulated microgravity enhances the epithelial–mesenchymal transition (EMT) of a human RPE cell line known as ARPE19 and promotes the expression of vascular endothelial growth factor (VEGF). Additionally, they demonstrated that the antioxidant Ishophloroglucin A could effectively inhibit EMT triggered by microgravity or VEGF by lowering VEGF–VEGFR2 signaling.87
The ARPE19 cell line was employed in experiments using the Random Positioning Machine system to simulate microgravity conditions. The outcomes indicated adverse effects on the cells, such as diminished cell viability, increased rates of apoptosis, disruption of the S-phase of the cell cycle, and oxidative stress.88 In another study, the clinorotation technique within a bioreactor that mimics microgravity was applied to cultivate the human ARPE19 cell line. A comparison of the outcomes with the 1 g control in a static 2D culture indicated the formation of multicellular spheroids, a decline in cell migration, an increase in intracellular ROS levels, mitochondrial dysfunction, activation of autophagic pathways, and stimulation of ciliogenesis.89 In contrast, in one investigation, ARPE-19 cells were relocated and grown for 3 days on the ISS.90 It was found that a 3-day incubation of ARPE-19 cells on the ISS did not affect their proliferation rate nor induce apoptosis.90
The endothelial vascular cells of the human retina and choroid are another population of retinal cells that show significant sensitivity to microgravity effects. Zhao et al cultured these cells for a period of 3 days under simulated microgravity. At the cellular level, the cells displayed a reduced cell body size, chromatin condensation and vacuolization, mitochondrial cavitation, and apoptosis. It was also noted that the simulated microgravity effect on choroidal vascular cells results in changes to the cellular ensemble, a reduction in the number of F-actin microfilaments, and the activation of the Bcl-2 apoptosis pathway along with the PI3K/AKT pathway.91
Some evidence suggests that cosmic rays induce cell death in the outer nuclear layer of rats that have been flown in space.92 In addition, research indicates that microgravity enhances apoptosis in astrocytes.93 A significant rise in apoptosis in the photoreceptors of spaceflight mice compared to ground-control mice was observed in another study.94 In a controlled in vitro experiment on primary Müller glia cells from adult rats, the natural antioxidants aloin and ginkgolide A flavonoids were assessed to clarify their protective role in the cultivation of Müller glia cells that were exposed to cosmic radiation. This radiation was simulated using cosmic galactic rays at the Brookhaven NASA Space Radiation Laboratory. The results revealed a favorable effect of antioxidants on the viability of Müller glia cells, as indicated by a decrease in ROS production within these cells.95
Although rodent models are invaluable for dissecting molecular pathways—including oxidative stress, blood retinal barrier disruption, and mitochondrial dysfunction—they are inherently limited for studying the pressure-induced structural hallmarks of SANS, such as choroidal folds and globe flattening. Rodents lack a robust, collagenous lamina cribrosa comparable to that of humans and non-human primates; consequently, their optic nerve head (ONH) does not experience the same translaminar pressure gradient mechanics that are thought to drive posterior globe deformation and folding of the chorioretinal layers in astronauts. Larger animal models that possess a true lamina cribrosa and human-like ONH architecture are therefore essential.96–98 Integrating data from these anatomically appropriate models with the molecular insights gained from rodent studies will be critical for a comprehensive understanding of space-induced ocular pathology.
Screening
The astronaut selection program is extremely specialized. This intensive process is aimed at identifying candidates with strong physical and mental well-being. Ophthalmic examinations are a significant part of this selection, with the purpose of preventing eye-related incidents in space. Those with existing ocular conditions face a heightened risk of both physical and mental health issues, which could be more challenging to manage during long-duration missions.2
NASA performs comprehensive evaluations of candidates’ visual capabilities (eg., uncorrected visual acuity, refractive error, near point of accommodation, near point convergence, IOP) employing specialized devices. NASA mandates a visual acuity of 20/20 in each eye, which can be accomplished through corrective interventions such as eyeglasses or refractive surgical methods. A majority of crewmembers experience presbyopia, with about 80% utilizing some form of vision correction.2 All crewmembers undergo yearly eye examinations in addition to pre-flight, in-flight, and post-flight assessments to explore the physiological effects of spaceflight.2 It is advisable that a minimum follow-up period of 2 years for brain and eye evaluations become standard protocol. Higher sampling during the initial mission return phase (2–3 months) could be extended to 6- or even 12-month intervals after one year.22
Clinical Manifestations
Table 1 lists the different ophthalmic clinical manifestations and concerns related to space environment. These items are separately discussed in other reports of AstroOphthalmology elsewhere.
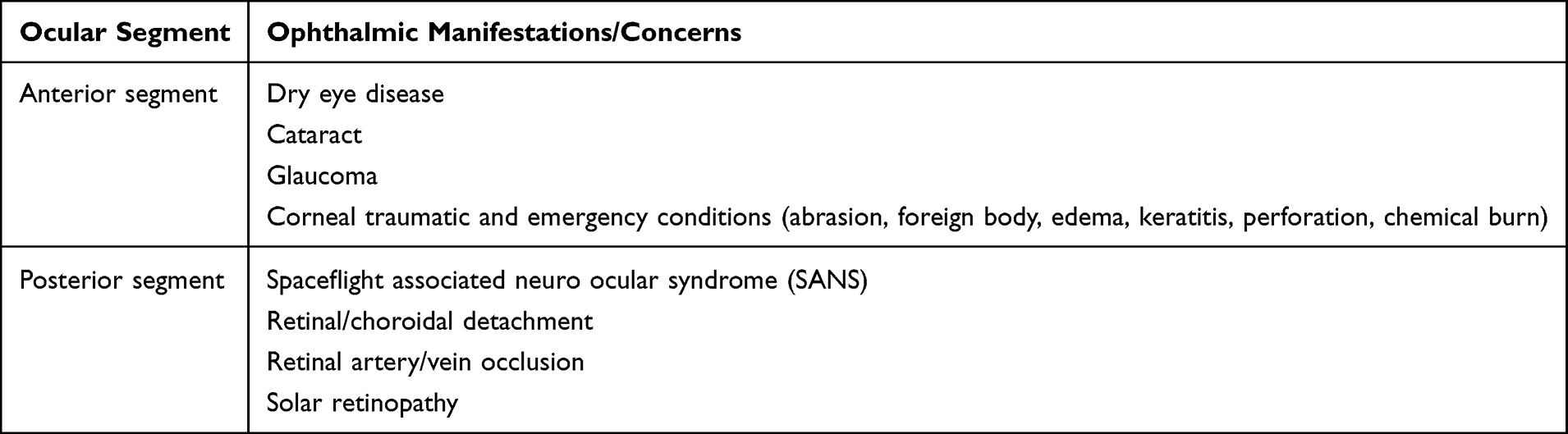 |
Table 1 Pathological Manifestations and Concerns Related to Space Environment |
In-Flight Evaluations
During missions, data gathering capabilities include vision questionnaires, visual acuity testing, Amsler grid testing, fundus photography, orbital ultrasound, and optical coherence tomography (OCT) (Table 2).99
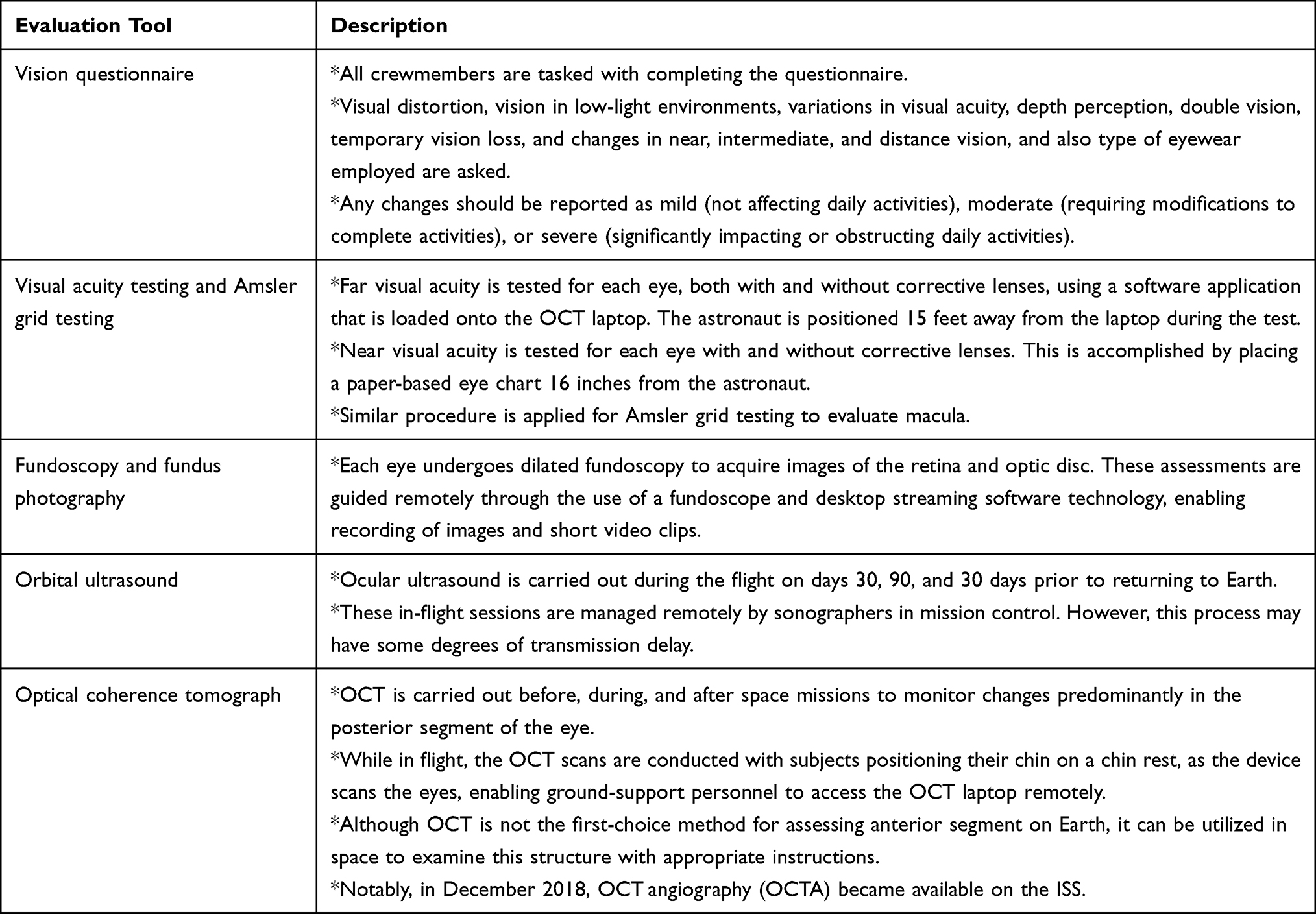 |
Table 2 In-Flight Evaluation Tools |
Teleophthalmology and Artificial Intelligence
Teleophthalmology can connect spacecraft crews with specialists on Earth, facilitating assistance for ocular emergencies through high-resolution imaging instruments, including anterior segment cameras and fundus photography devices. These systems support detailed assessments that can be transmitted for expert analysis.100,101 However, as missions extend into deep space, communication delays of up to 20 minutes will occur, necessitating onboard diagnostic autonomy and advanced remote healthcare approaches.102 Regarding ocular health, the integration of diagnostic systems with artificial intelligence (AI) and teleophthalmology frameworks allows astronauts to execute initial evaluations and interventions on their own when Earth-based consultations are not immediately available. AI-driven decision support enhances the capabilities of astronauts by offering customized treatment options, minimizing reliance on terrestrial expertise, and facilitating prompt handling of ocular emergencies.102,103
Discussion and Future Perspective
Various pathophysiological concepts in this area are supported by strong evidence, while others remain unproven. Well-documented findings include the presence of optic disc edema, globe flattening, and chorioretinal folds in astronauts after extended missions; the dose-dependent increased risk of cortical cataract due to space radiation; the acute rise in intraocular pressure (IOP) upon entering microgravity; and the cephalad fluid shift confirmed by various imaging modalities. Emerging yet less validated theories consist of the glymphatic hypothesis associated with SANS, mitochondrial dysfunction as a primary cause of retinal damage, the impact of hypercapnia on optic disc edema, and the gradient-wise mechanical stress model of chorioretinal folds.
Given the limited opportunities for actual spaceflight, ground-based analogues are pivotal in exploring the pathophysiology of SANS and in evaluating countermeasures. The head-down tilt bed rest, which ranges from −6° to −15°, is the most widely used terrestrial model, consistently reproducing cephalad fluid shifts, choroidal thickening, and optic disc edema.104,105 Dry immersion, which simulates the absence of support and the fluid redistribution typical of weightlessness, further mimics the cardiovascular and ocular responses observed in orbit.106 Additional techniques include lower body negative pressure to counteract fluid shifts, parabolic flights for brief periods of microgravity, and short radius centrifugation to generate artificial gravity as a potential countermeasure.107,108 These analogue environments, each with unique advantages and limitations, form the backbone of experimental SANS research and are crucial for developing both diagnostic protocols and preventive strategies for future lunar and Martian missions.
Studies show that shifts in fluid due to microgravity result in vascular congestion and a decrease in CSF outflow, potentially leading to a state of low-grade, chronic hypoxia in the optic nerve head and retina.13,16 A novel trend that has recently emerged in the fields of astrobiology and space physiology research is gravitational dose-response modeling.7,109 This quantitative framework is designed to map the relationship between progressive alterations in the gravitational vector (referred to as the “dose” of gravity) and the resulting physiological changes (known as the “response”). Rather than considering microgravity as a simple binary state, this methodology employs graded tilt paradigms (for instance, from +45° head-up to −45° head-down) to create continuous response curves for hemodynamic, autonomic, and ocular variables. The fundamental concept is that various tissues and functions display unique thresholds and slopes regarding their sensitivity to gravity. Whittle et al109 were the pioneers in applying this methodology to cardiovascular hemodynamics, revealing a significant gravitational dependence across a spectrum of variables—including heart rate, stroke volume, cardiac output, and autonomic indices—across a tilt range from 45° head-up to 45° head-down. Following this approach, Iftime et al7 investigated the differences in visual performance during acute exposure to a microgravity analogue. They utilized simple reaction time tasks in the central and perimacular visual fields during vertical, bed rest, −6°, and −15° head-down tilt, constructing dose-response models that associate the gravitational component with visual function parameters. Their research uncovered that the perimacular (peripheral) retina is the first region to be functionally impacted by changes in gravity, while the central retina is the last to be affected. This gradient of topographical vulnerability has direct consequences for SANS, indicating that functional testing of the extra-macular retina—especially towards the optic disc—may allow for earlier identification of SANS-related pathologies compared to standard central visual assessments alone. The application of dose-response modeling in spaceflight ocular research provides various advantages: to begin with, it identifies the gravitational thresholds at which certain ocular tissues begin to demonstrate dysfunction; next, it facilitates a quantitative evaluation of countermeasure efficacy; and ultimately, it offers a predictive framework for estimating ocular risk during partial-gravity exposures on the lunar (0.16 g) and Martian (0.38 g) surfaces—settings for which empirical ocular data is notably lacking.
Tissues that are hypoxic are more prone to damage from radiation, as the efficiency of repairing DNA strand breaks caused by radiation is diminished in low-oxygen conditions.62,82,85 Thus, the radiation exposure experienced during a mission may exert a more severe influence on ocular tissues that have already been compromised by the fluid dynamics associated with microgravity.
Both microgravity and radiation independently cause significant oxidative stress. Microgravity disrupts the function of mitochondria and compromises antioxidant defenses, while radiation directly creates ROS. Hence, it is crucial for future research to extend beyond the study of isolated risks. Future investigations should explicitly test the combined effects of radiation and microgravity in animal models.
Numerous countermeasures are presently under investigation to alleviate SANS. Lower body negative pressure (LBNP) has been demonstrated to decrease the diameter of the optic nerve sheath during head down tilt and to partially normalize choroidal thickness, thereby addressing the fluid shift aspect of SANS. Another promising strategy involves artificial gravity produced by short radius centrifugation, with or without exercise, which may help restore hydrostatic gradients and cardiovascular tone. Pharmacological agents, including antioxidants (such as cysteine and Ishophloroglucin A), have shown protective effects on retinal pigment epithelial cells in simulated microgravity, while radioprotectors are currently undergoing preliminary testing for the prevention of cataracts and retinal damage. Venoconstrictive thigh cuffs are designed to retain blood in the lower extremities and mitigate cephalad fluid shift, although their effectiveness on ocular health necessitates further investigation. Future countermeasures should be multi-targeted, including the development of pharmacological agents that can protect against oxidative damage from radiation and vascular stress due to microgravity. Additionally, it is essential to identify early predictive biomarkers in biofluids (for example, oxidative stress markers) that can signal ocular damage before it is clinically observable. The challenges posed by communication delays that prevent real-time telemedicine in deep-space missions have rendered the establishment of fully autonomous AI-driven diagnostic systems an essential requirement. These systems must be proficient in integrating OCT-A, fundus imagery, and biomarker data to provide astronauts with diagnostic and treatment advice without the involvement of Earth-based support.
The evidence presented in this review is constrained by notable limitations. To begin with, most human data is derived from a small group of astronauts, the vast majority of whom are male; the sex-specific differences in fluid regulation and radiation sensitivity are largely unexamined. Additionally, ground-based microgravity analogues only approximate the genuine spaceflight environment and do not replicate all features of weightlessness, particularly the absence of tissue compression and the complete range of fluid dynamics. Moreover, many mechanistic studies rely on animal models (mainly mice), whose retinal anatomy is different from that of humans, and on in vitro cell cultures subjected to simulated microgravity or simplified radiation protocols that may not capture the complex, mixed field radiation of deep space. Furthermore, longitudinal in-flight studies are limited; the timeline of SANS development is still poorly understood, and post-flight follow-up is often too brief to assess long-term reversibility. Finally, the small sample sizes and limited statistical power of many studies complicate the detection of small but clinically relevant effects. Future research should focus on larger, more diverse cohorts, direct in-flight measurements, and rigorous validation of analog models against actual spaceflight data.
Conclusion
The human eye is highly sensitive to the environment of space. This review has gathered evidence that illustrates how extended spaceflight poses a multifaceted threat to eye health, mainly through two interconnected pathways: the mechanical and hemodynamic effects resulting from cephalad fluid shift, and the direct and indirect damage to tissues caused by cosmic radiation. At the core of both pathways is the prevalent mechanism of oxidative stress and mitochondrial dysfunction, which injures cellular components and hinders the operation of vital tissues. With aspirations directed towards lunar and Martian missions, the risk of irreversible damage that could compromise vision is considerable. The clinical significance of these changes extends beyond individual astronaut health: even mild visual impairment can degrade task performance, reduce mission safety, and limit operational capabilities during extravehicular activities or planetary surface operations. As space agencies plan lunar habitats and crewed Mars missions, unrecognized or unmanaged ocular pathology could threaten the success of these endeavors. Therefore, future research must move beyond descriptive characterization and focus on actionable solutions, including development of integrated countermeasures that simultaneously address the mechanical effects of fluid shift and the molecular damage caused by radiation, identification and validation of early predictive biomarkers to enable pre-clinical detection of SANS and other space-related eye diseases, and establishment of autonomous, AI driven diagnostic platforms capable of operating without real time Earth support, which is essential for deep space missions.
Data Sharing Statement
All data reported in this study are publicly available.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Krittanawong C, Singh NK, Scheuring RA, et al. Human health during space travel: state-of-the-art review. Cells. 2023;12(1):40. doi:10.3390/cells12010040
2. Suh A, Ditelberg S, Szeto JJ, et al. Safety protocols, precautions, and countermeasures aboard the International Space Station to prevent ocular injury. Surv Ophthalmol. 2024;70:1003–16. doi:10.1016/j.survophthal.2024.08.005
3. Özelbaykal B, Öğretmenoğlu G, Gedik Ş. The effects of space radiation and microgravity on ocular structures. Turk J Ophthalmol. 2022;52(1):57. doi:10.4274/tjo.galenos.2021.29566
4. Antonsen EL, Connell E, Anton W, Reynolds RJ, Buckland DM, Van Baalen M. Updates to the NASA human system risk management process for space exploration. Npj Microgravity. 2023;9(1):72. doi:10.1038/s41526-023-00305-z
5. Mader TH, Gibson CR, Pass AF, et al. Optic disc edema, globe flattening, choroidal folds, and hyperopic shifts observed in astronauts after long-duration space flight. Ophthalmology. 2011;118(10):2058–2069. doi:10.1016/j.ophtha.2011.06.021
6. Rodrigues GA, Russomano T, Santos Oliveira E. Understanding the relationship between intracranial pressure and spaceflight associated neuro-ocular syndrome (SANS): a systematic review. Npj Microgravity. 2025;11(1):22. doi:10.1038/s41526-025-00464-1
7. Iftime A, Tofolean IT, Pintilie V, Călinescu O, Busnatu S, Papacocea IR. Differential functional changes in visual performance during acute exposure to microgravity analogue and their potential links with spaceflight-associated neuro-ocular syndrome. Diagnostics. 2024;14(17):1918. doi:10.3390/diagnostics14171918
8. Ferguson CR, Pardon LP, Laurie SS, et al. Incidence and progression of chorioretinal folds during long-duration spaceflight. JAMA Ophthalmol. 2023;141(2):168–175. doi:10.1001/jamaophthalmol.2022.5681
9. Kermorgant M, Chedmail T, Varenne F, et al. Neuro-ophthalmological changes in healthy females exposed to a 5-day dry immersion: a pilot study. Npj Microgravity. 2024;10(1):4. doi:10.1038/s41526-024-00344-0
10. Adamopoulos K, Koutsouris D, Zaravinos A, Lambrou GI. Gravitational influence on human living systems and the evolution of species on earth. Molecules. 2021;26(9):2784. doi:10.3390/molecules26092784
11. Unsworth BR, Lelkes PI. Growing tissues in microgravity. Nature Med. 1998;4(8):901–907. doi:10.1038/nm0898-901
12. Hargens AR, Watenpaugh DE. Cardiovascular adaptation to spaceflight. Med Sci Sports Exercise. 1996;28(8):977–982. doi:10.1097/00005768-199608000-00007
13. Michel EL, Johnston RS, Dietlein LF. Biomedical results of the Skylab Program. Life Sci Space Res. 1976;14:3–18.
14. Gharib C, Hughson RL. Fluid and electrolyte regulation in space. Adv Space Biol Med. 1992;2:113–130.
15. Kim DS, Vaquer S, Mazzolai L, et al. The effect of microgravity on the human venous system and blood coagulation: a systematic review. Exp Physiol. 2021;106(5):1149–1158. doi:10.1113/EP089409
16. Ly V, Velichala SR, Hargens AR. Cardiovascular, lymphatic, and ocular health in space. Life. 2022;12(2):268. doi:10.3390/life12020268
17. Galdamez L. Pathophysiology of cerebral edema and its connection to spaceflight associated neuro-ocular syndrome. In: Lee AG, Ong J, editors. Spaceflight Associated Neuro-Ocular Syndrome. Cambridge, MA: Academic Press; 2022:107–133.
18. Galdamez LA, Brunstetter TJ, Lee AG, Tarver WJ. Origins of cerebral edema: implications for spaceflight-associated neuro-ocular syndrome. J Neuroophthalmol. 2020;40:84–91. doi:10.1097/WNO.0000000000000852
19. Rasmussen JC, Kwon S, Pinal A, et al. Assessing lymphatic route of CSF outflow and peripheral lymphatic contractile activity during head‐down tilt using near‐infrared fluorescence imaging. Physiological Reports. 2020;8(4):e14375. doi:10.14814/phy2.14375
20. Jacob L, Boisserand LS, Geraldo LH, et al. Anatomy and function of the vertebral column lymphatic network in mice. Nat Commun. 2019;10(1):4594. doi:10.1038/s41467-019-12568-w
21. Buckey JC, Lan M, Phillips SD, Archambault-Leger V, Fellows AM. A theory for why the spaceflight-associated neuro-ocular syndrome develops. J Appl Physiol. 2022;132(5):1201–1203. doi:10.1152/japplphysiol.00854.2021
22. Seidler RD, Stern C, Basner M, Stahn AC, Wuyts FL, Zu Eulenburg P. Future research directions to identify risks and mitigation strategies for neurostructural, ocular, and behavioral changes induced by human spaceflight: a NASA-ESA expert group consensus report. Front Neural Circuits. 2022;16:876789. doi:10.3389/fncir.2022.876789
23. Wostyn P, De Winne F, Stern C, Mader TH, Gibson CR, De Deyn PP. Potential involvement of the ocular glymphatic system in optic disc edema in astronauts. Aerosp Med Hum Perform. 2020;91(12):975–977. doi:10.3357/AMHP.5670.2020
24. Jessen NA, Munk AS, Lundgaard I, Nedergaard M. The glymphatic system: a beginner’s guide. Neurochem Res. 2015;40(12):2583–2599. doi:10.1007/s11064-015-1581-6
25. Iwasaki KI, Levine BD, Zhang R, et al. Human cerebral autoregulation before, during and after spaceflight. J Physiol. 2007;579(3):799–810. doi:10.1113/jphysiol.2006.119636
26. Arbeille P, Provost R, Zuj K, Vincent N. Measurements of jugular, portal, femoral, and calf vein cross-sectional area for the assessment of venous blood redistribution with long duration spaceflight (Vessel Imaging Experiment). Eur J Appl Physiol. 2015;115(10):2099–2106. doi:10.1007/s00421-015-3189-6
27. Nickla DL, Wallman J. The multifunctional choroid. Prog Retinal Eye Res. 2010;29(2):144–168. doi:10.1016/j.preteyeres.2009.12.002
28. Ansari RR, Suh KI, Moret F, Messer RK, Manuel FK. Measurement of choroidal blood flow in zero gravity. In: Ophthalmic Technologies XIII. Vol. 4951. SPIE; Jul 2003:177–184.
29. Kiel JW. Choroidal myogenic autoregulation and intraocular pressure. Exp. Eye Res. 1994;58(5):529–543. doi:10.1006/exer.1994.1047
30. Draeger J, Schwartz R, Groenhoff S, Stern C. Self-tonometry under microgravity conditions. The Clinical Investigator. 1993;71(9):700–703. doi:10.1007/BF00209723
31. Mader CT, Gibson CR, Caputo M, et al. Intraocular pressure and retinal vascular changes during transient exposure to microgravity. Am J Ophthalmol. 1993;115(3):347–350. doi:10.1016/S0002-9394(14)73586-X
32. Friberg TR, Sanborn G, Weinreb RN. Intraocular and episcleral venous pressure increase during inverted posture. Am J Ophthalmol. 1987;103(4):523–526. doi:10.1016/S0002-9394(14)74275-8
33. Shinojima A, Iwasaki K, Aoki K, Ogawa Y, Yanagida R, Yuzawa M. Subfoveal choroidal thickness and foveal retinal thickness during head-down tilt. Aviat Space Environ Med. 2012;83:388–393. doi:10.3357/ASEM.3191.2012
34. Cucinotta FA, Kim MH, Chappell LJ, Huff JL. How safe is safe enough? Radiation risk for a human mission to Mars. PLoS One. 2013;8:e74988. doi:10.1371/journal.pone.0074988
35. National Council of Radiation Protection and Measure ments (NCRP). Guidance on Radiation Received in Space Activity. Bethesda: NCRP; 1989.
36. Simpson JA. Elemental and isotopic composition of the galactic cosmic rays. Ann Rev Nucl Part Sci. 1983;33:323–382. doi:10.1146/annurev.ns.33.120183.001543
37. Meer E, Grob S, Antonsen EL, Sawyer A. Ocular conditions and injuries, detection and management in spaceflight. Npj Microgravity. 2023;9(1):37. doi:10.1038/s41526-023-00279-y
38. Zhang S, Wimmer-Schweingruber RF, Yu J, et al. First measurements of the radiation dose on the lunar surface. Sci Adv. 2020;6(39):eaaz1334. doi:10.1126/sciadv.aaz1334
39. Chancellor JC, Scott GB, Sutton JP. Space radiation: the number one risk to astronaut health beyond low earth orbit. Life. 2014;4(3):491–510. doi:10.3390/life4030491
40. Danesh-Meyer HV. Radiation-induced optic neuropathy. J Clin Neurosci. 2008;15(2):95–100. doi:10.1016/j.jocn.2007.09.004
41. Hamada N, Azizova TV, Little MP. An update on effects of ionizing radiation exposure on the eye. British J Radiol. 2020;93(1115):20190829. doi:10.1259/bjr.20190829
42. Jeganathan VS, Wirth A, MacManus MP. Ocular risks from orbital and periorbital radiation therapy: a critical review. Int J Radiat Oncol Biol Phys. 2011;79(3):650–659. doi:10.1016/j.ijrobp.2010.09.056
43. NASA-STD-3001. Space Flight Human-System Standard and the Human Integration Design Handbook; 2012. https://ntrs.nasa.gov/search.jsp?R=20130000738.
44. Valinia A, Allen JR, Francisco DR, Minow JI, Pellish JA, Vera AH. Safe human expeditions beyond low Earth orbit (LEO). Acta Astronaut. 2022;194:1–15.
45. Durchschlag H, Fochler C, Abraham K, Kulawik B. Radiation effects on eye components. Radiat Phys Chem. 1999;55(5–6):691–697. doi:10.1016/S0969-806X(99)00213-3
46. Chylack LT, Feiveson AH, Peterson LE, et al. NASCA report 2: longitudinal study of relationship of exposure to space radiation and risk of lens opacity. Radiat Res. 2012;178(1):25–32. doi:10.1667/RR2876.1
47. Kumre D, Jeswani V, Benurwar S, Tumram NK. Role of total dose and hyperfractionation in reducing risk of radiation-induced optic neuropathy. Oman J Ophthalmol. 2015;8(1):75–76. doi:10.4103/0974-620X.149901
48. Ballian N, Androulakis II, Chatzistefanou K, et al. Optic neuropathy following radiotherapy for Cushing’s disease: case report and literature review. Hormones. 2010;9(3):269–273. doi:10.1007/BF03401278
49. Pollock BE, Link MJ, Leavitt JA, Stafford SL. Dose-volume analysis of radiation-induced optic neuropathy after single-fraction stereotactic radiosurgery. Neurosurgery. 2014;75(4):456–460. doi:10.1227/NEU.0000000000000457
50. Narici L, Bidoli V, Casolino M, et al. ALTEA: anomalous long term effects in astronauts. A probe on the influence of cosmic radiation and microgravity on the central nervous system during long flights. Adv Space Res. 2003;31(1):141–146. doi:10.1016/S0273-1177(02)00881-5
51. Mathis T, Vignot S, Leal C, et al. Mechanisms of phosphenes in irradiated patients. Oncotarget. 2017;8(38):64579. doi:10.18632/oncotarget.18719
52. Narici L. Heavy ions light flashes and brain functions: recent observations at accelerators and in spaceflight. New J Phys. 2008;10(7):075010. doi:10.1088/1367-2630/10/7/075010
53. Newman F, Asadi‐Zeydabadi M, Durairaj VD, Ding M, Stuhr K, Kavanagh B. Visual sensations during megavoltage radiotherapy to the orbit attributable to Cherenkov radiation. Med Phys. 2008;35(1):77–80. doi:10.1118/1.2815358
54. Fuglesang C, Narici L, Picozza P, Sannita WG. Phosphenes in low earth orbit: survey responses from 59 astronauts. Aviat Space Environ Med. 2006;77(4):449–452.
55. Law J, Van Baalen M, Foy M, et al. Relationship between carbon dioxide levels and reported headaches on the international space station. J Occup Environ Med. 2014;56(5):477–483. doi:10.1097/JOM.0000000000000158
56. Laurie SS, Vizzeri G, Taibbi G, et al. Effects of short‐term mild hypercapnia during head‐down tilt on intracranial pressure and ocular structures in healthy human subjects. Physiol Rep. 2017;5(11):e13302. doi:10.14814/phy2.13302
57. Banker LA, Salazar AP, Lee JK, et al. The effects of a spaceflight analog with elevated CO2 on sensorimotor adaptation. J Neurophysiol. 2021;125(2):426–436. doi:10.1152/jn.00306.2020
58. Basner M, Stahn AC, Nasrini J, et al. Effects of head-down tilt bed rest plus elevated CO2 on cognitive performance. J Appl Physiol. 2021;130(4):1235–1246. doi:10.1152/japplphysiol.00865.2020
59. Jaki Mekjavic P, Lenassi E, Eiken O, Mekjavic IB. Effect of acute hypercapnia during 10-day hypoxic bed rest on posterior eye structures. J Appl Physiol. 2016;120(10):1241–1248. doi:10.1152/japplphysiol.00930.2015
60. Masalkhi M, Ong J, Waisberg E, Lee AG. Ocular oxidative changes and antioxidant therapy during spaceflight. Eye. 2024;38(6):1034–1035. doi:10.1038/s41433-023-02841-0
61. Beatty S, Koh HH, Phil M, Henson D, Boulton M. The role of oxidative stress in the pathogenesis of age-related macular degeneration. Surv Ophthalmol. 2000;45(2):115–134. doi:10.1016/S0039-6257(00)00140-5
62. Waisberg E, Ong J, Lee AG. Space radiation and the potential for early cataract development. Eye. 2024;38(3):416–417. doi:10.1038/s41433-023-02742-2
63. Luxton JJ, McKenna MJ, Lewis A, et al. Telomere length dynamics and DNA damage responses associated with long-duration spaceflight. Cell Rep. 2020;33(10):108457. doi:10.1016/j.celrep.2020.108457
64. Cingolani C, Rogers B, Lu L, Kachi S, Shen J, Campochiaro PA. Retinal degeneration from oxidative damage. Free Radic Biol Med. 2006;40(4):660–669. doi:10.1016/j.freeradbiomed.2005.09.032
65. Kim JH, Kang SW, Kong MG, Ha HS. Assessment of retinal layers and visual rehabilitation after epiretinal membrane removal. Graefes Arch Clin Exp Ophthalmol. 2013;251(4):1055–1064. doi:10.1007/s00417-012-2120-7
66. Overbey EG, da Silveira WA, Stanbouly S, et al. Spaceflight influences gene expression, photoreceptor integrity, and oxidative stress-related damage in the murine retina. Sci Rep. 2019;9(1):13304. doi:10.1038/s41598-019-49453-x
67. Mao X, Stanbouly S, Holley J, Pecaut M, Crapo J. Evidence of spaceflight-induced adverse effects on photoreceptors and retinal function in the mouse eye. Int J Mol Sci. 2023;24(8):7362. doi:10.3390/ijms24087362
68. Hüttemann M, Lee I, Samavati L, Yu H, Doan JW. Regulation of mitochondrial oxidative phosphorylation through cell signaling. BBA. 2007;1773(12):1701–1720. doi:10.1016/j.bbamcr.2007.10.001
69. Wang J, Deretic D. Molecular complexes that direct rhodopsin transport to primary cilia. Prog Retinal Eye Res. 2014;38:1–9. doi:10.1016/j.preteyeres.2013.08.004
70. da Silveira WA, Fazelinia H, Rosenthal SB, et al. Comprehensive multi-omics analysis reveals mitochondrial stress as a central biological hub for spaceflight impact. Cell. 2020;183(5):1185–1201. doi:10.1016/j.cell.2020.11.002
71. Mao XW, Pecaut MJ, Stodieck LS, et al. Spaceflight environment induces mitochondrial oxidative damage in ocular tissue. Radiat Res. 2013;180(4):340–350. doi:10.1667/RR3309.1
72. Crucian BE, Zwart SR, Mehta S, et al. Plasma cytokine concentrations indicate that in vivo hormonal regulation of immunity is altered during long-duration spaceflight. J Interferon Cytokine Res. 2014;34(10):778–786. doi:10.1089/jir.2013.0129
73. Masalkhi M, Ong J, Waisberg E, Lee AG. Ocular immunology and inflammation under microgravity conditions and the pathogenesis of spaceflight associated neuro-ocular syndrome (SANS). Eye. 2024;38(10):1799–1801. doi:10.1038/s41433-024-03005-4
74. Streilein JW. Ocular immune privilege: the eye takes a dim but practical view of immunity and inflammation. J Leucocyte Biol. 2003;74(2):179–185. doi:10.1189/jlb.1102574
75. Crabbé A, Nielsen-Preiss SM, Woolley CM, et al. Spaceflight enhances cell aggregation and random budding in Candida albicans. PLoS One. 2013;8(12):e80677. doi:10.1371/journal.pone.0080677
76. Rooney BV, Crucian BE, Pierson DL, Laudenslager ML, Mehta SK. Herpes virus reactivation in astronauts during spaceflight and its application on earth. Front Microbiol. 2019;10:16. doi:10.3389/fmicb.2019.00016
77. Bradbury P, Wu H, Choi JU, et al. Modeling the impact of microgravity at the cellular level: implications for human disease. Front Cell Develop Biol. 2020;8:96. doi:10.3389/fcell.2020.00096
78. Beck M, Moreels M, Quintens R, et al. Chronic exposure to simulated space conditions predominantly affects cytoskeleton remodeling and oxidative stress response in mouse fetal fibroblasts. IntJ Mol Med. 2014;34(2):606–615. doi:10.3892/ijmm.2014.1785
79. Hughson RL, Irving EL. Spaceflight not an eye‐popping experience for astronauts. Journal of Physiology. 2021;599(4):1011–1012. doi:10.1113/JP281009
80. Ax T, Ganse B, Fries FN, et al. Dry eye disease in astronauts: a narrative review. Front Physiol. 2023;14:1281327. doi:10.3389/fphys.2023.1281327
81. Zanello SB, Theriot CA, Prospero Ponce CM, Chevez-Barrios P. Spaceflight effects and molecular responses in the mouse eye: preliminary observations after shuttle mission STS-133. Gravitat Space Res. 2013;1(1):29–46. doi:10.2478/gsr-2013-0003
82. Delic NC, Lyons JG, Di Girolamo N, Halliday GM. Damaging effects of ultraviolet radiation on the cornea. Photochem Photobiol. 2017;93(4):920–929. doi:10.1111/php.12686
83. Theriot CA, Glass A, Lam CW, James J, Zanello SB. Chronic lunar dust exposure on rat cornea: evaluation by gene expression profiling. In:
84. Mao XW, Nishiyama NC, Byrum SD, et al. Characterization of mouse ocular response to a 35-day spaceflight mission: evidence of blood-retinal barrier disruption and ocular adaptations. Sci Rep. 2019;9(1):8215. doi:10.1038/s41598-019-44696-0
85. Roberts JE, Kukielczak BM, Chignell CF, Sik BH, Hu DN, Principato MA. Simulated microgravity induced damage in human retinal pigment epithelial cells. Mol Vis. 2006;12(12):633–638.
86. Corydon TJ, Mann V, Slumstrup L, et al. Reduced expression of cytoskeletal and extracellular matrix genes in human adult retinal pigment epithelium cells exposed to simulated microgravity. Cell Physiol Biochem. 2016;40(1–2):1–7. doi:10.1159/000452520
87. Son M, Ryu B, Je JG, Jeon YJ, Kim DY. Ishophloroglucin A ameliorates VEGF-induced epithelial-mesenchymal transition via VEGFR2 pathway inhibition in microgravity-stimulated human retinal pigment epithelial cells. Antioxidants. 2022;11(11):2212. doi:10.3390/antiox11112212
88. Huyan T, Li M, Chen W, et al. Simulated microgravity promotes oxidative stress-induced apoptosis in ARPE-19 cells associated with Nrf2 signaling pathway. Acta Astronaut. 2022;198:161–169. doi:10.1016/j.actaastro.2022.05.012
89. Nguyen HP, Shin S, Shin KJ, et al. Protective effect of TPP-Niacin on microgravity-induced oxidative stress and mitochondrial dysfunction of retinal epithelial cells. Biochimica et Biophysica Acta. 2023;1870(1):119384. doi:10.1016/j.bbamcr.2022.119384
90. Cialdai F, Bolognini D, Vignali L, et al. Effect of space flight on the behavior of human retinal pigment epithelial ARPE-19 cells and evaluation of coenzyme Q10 treatment. Cell Mol Life Sci. 2021;78(23):7795–7812. doi:10.1007/s00018-021-03989-2
91. Zhao H, Shi Y, Qiu C, et al. Effects of simulated microgravity on ultrastructure and apoptosis of choroidal vascular endothelial cells. Front Physiol. 2021;11:577325. doi:10.3389/fphys.2020.577325
92. Philpott DE, Corbett R, Turnbill C, et al. Cosmic ray effects on the eyes of rats flown on Cosmos No. 782, experimental K-007. Aviat Space Environ Med. 1978;49(1 Pt 1):19–28.
93. Uva BM, Masini MA, Sturla M, Tagliafierro G, Strollo F. Microgravity-induced programmed cell death in astrocytes. J Gravitat Physiol. 2002;9(1):P275–6.
94. Mao XW, Green LM, Mekonnen T, Lindsey N, Gridley DS. Gene expression analysis of oxidative stress and apoptosis in proton-irradiated rat retina. in vivo. 2010;24(4):425–430.
95. Cliver RN, Castro N, Russomano T, et al. Antioxidants derived from natural products reduce radiative damage in cultured retinal glia to prevent oxidative stress. Neuroglia. 2022;3(3):84–98. doi:10.3390/neuroglia3030006
96. Oikawa K, Teixeira LB, Keikhosravi A, Eliceiri KW, McLellan GJ. Microstructure and resident cell-types of the feline optic nerve head resemble that of humans. Exp Eye Res. 2021;202:108315. doi:10.1016/j.exer.2020.108315
97. Zhu Z, Waxman S, Wang B, et al. Interplay between intraocular and intracranial pressure effects on the optic nerve head in vivo. Exp Eye Res. 2021;213:108809. doi:10.1016/j.exer.2021.108809
98. Fleischman D, Kaskar O, Shams R, et al. A novel porcine model for the study of cerebrospinal fluid dynamics: development and preliminary results. Front Neurol. 2019;10:1137. doi:10.3389/fneur.2019.01137
99. Stenger MB, Tarver WJ, Brunstetter TJ. Risk of spaceflight associated neuro-ocular syndrome (SANS). Npj Microgravity. 2017;3:2. doi:10.1038/s41526-016-0001-9
100. Williams DR, Bashshur RL, Pool SL, Doarn CR, Merrell RC, Logan JS. A strategic vision for telemedicine and medical informatics in space flight. Telemed J E Health. 2000;6(4):441–448. doi:10.1089/15305620050503924
101. Meshkin RS, Armstrong GW, Hall NE, Rossin EJ, Hymowitz MB, Lorch AC. Effectiveness of a telemedicine program for triage and diagnosis of emergent ophthalmic conditions. Eye. 2023;37(2):325–331. doi:10.1038/s41433-022-01940-8
102. Thirsk RB. Health care for deep space explorers. Ann ICRP. 2020;49(1_suppl):182–184. doi:10.1177/0146645320935288
103. Krishnan Ganapathy MN. Space medicine: the ultimate in remote healthcare. Telehealth Med Today. 2020;5(2).
104. Watenpaugh DE. Analogs of microgravity: head-down tilt and water immersion. J Appl Physiol. 2016;120(8):904–914. doi:10.1152/japplphysiol.00986.2015
105. Marshall-Goebel K, Mulder E, Bershad E, et al. Intracranial and intraocular pressure during various degrees of head-down tilt. Aerosp Med Hum Perform. 2017;88(1):10–16. doi:10.3357/AMHP.4653.2017
106. Pandiarajan M, Hargens AR. Ground-based analogs for human spaceflight. Front Physiol. 2020;11:716. doi:10.3389/fphys.2020.00716
107. Diaz-Artiles A, Heldt T, Young LR. Short-term cardiovascular response to short-radius centrifugation with and without ergometer exercise. Front Physiol. 2018;9:1492. doi:10.3389/fphys.2018.01492
108. Laurie SS, Greenwald SH, Marshall‐Goebel K, et al. Optic disc edema and chorioretinal folds develop during strict 6 head‐down tilt bed rest with or without artificial gravity. Physiological Reports. 2021;9(15):e14977. doi:10.14814/phy2.14977
109. Whittle RS, Keller N, Hall EA, et al. Gravitational dose‐response curves for acute cardiovascular hemodynamics and autonomic responses in a tilt paradigm. J Am Heart Assoc. 2022;11(14):e024175. doi:10.1161/JAHA.121.024175
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pain Experience and Sensory Changes in Astronauts During and After Short-Lasting Commercial Spaceflight: A Proof-of-Concept Study
Sauer AK, Vigouroux M, Dougherty PM, Cata JP, Ingelmo PM
Journal of Pain Research 2023, 16:4253-4266
Published Date: 11 December 2023