Back to Journals » Journal of Pain Research » Volume 16
Pain Experience and Sensory Changes in Astronauts During and After Short-Lasting Commercial Spaceflight: A Proof-of-Concept Study
Authors Sauer AK, Vigouroux M ![]() , Dougherty PM, Cata JP
, Dougherty PM, Cata JP ![]() , Ingelmo PM
, Ingelmo PM
Received 17 October 2023
Accepted for publication 2 December 2023
Published 11 December 2023 Volume 2023:16 Pages 4253—4266
DOI https://doi.org/10.2147/JPR.S440630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Andrea K Sauer,1,* Marie Vigouroux,2,3,* Patrick M Dougherty,4 Juan Pablo Cata,5,6,* Pablo M Ingelmo2,3,7,8,*
1Department of Anesthesia, University of Bonn, Bonn, Germany; 2Department of Anesthesia, McGill University, Montreal, QC, Canada; 3Edwards Family Interdisciplinary Center for Complex Pain, Montreal Children’s Hospital, Montreal, QC, Canada; 4Department of Pain Medicine, The University of Texas – MD Anderson Cancer Center, Houston, TX, USA; 5Department of Anesthesia and Perioperative Medicine, The University of Texas – MD Anderson Cancer Center, Houston, TX, USA; 6Anesthesiology and Surgical Oncology Research Group, Houston, TX, USA; 7Alan Edwards Centre for Research on Pain, McGill University, Montreal, QC, Canada; 8Research Institute, McGill University Health Center, Montreal, QC, Canada
*These authors contributed equally to this work
Correspondence: Pablo M Ingelmo, Edwards Family Interdisciplinary Center for Complex Pain, Montreal Children’s Hospital, Room A02.3525, Glen Site, 1001 Boul, Décarie, Montreal, QC, H4A 3J1, Canada, Tel +1 514 412-4448, Fax +1 514 412-4341, Email [email protected]
Abstract: Space travel has been associated with musculoskeletal pain, yet little is known about the nociceptive changes and pain experience during spaceflight. This preliminary study aims to investigate the pain experience and sensory alterations in astronauts following a 17-day mission to the International Space Station (ISS) on Axiom Space’s AX-1 commercial space flight. Two participants were enrolled, and data were collected pre-flight, in-flight, post-flight, and three-month post-flight. Validated pain questionnaires assessed anxiety, catastrophizing, impact on physical and mental health, disability, and overall pain experience. Qualitative interviews were conducted post-landing and conditioned pain modulation (CPM) and quantitative sensory testing (QST) were performed. Both astronauts reported musculoskeletal pain during and after the flight, which was managed with anti-inflammatories and stretching techniques. Pain levels returned to baseline after three months. Pain questionnaires revealed heightened pain experiences in-flight and immediately post-flight, although their adequacy in assessing pain in space is uncertain. Qualitative interviews allowed astronauts to describe their pain experiences during the flight. Sensory changes included increased mechanical touch detection thresholds, temporal pain summation, heat pain thresholds, and differences in conditioned pain modulation post-flight. This preliminary study suggested that spaceflight may affect various aspects of sensory perception and regulation in astronauts, albeit in a variable manner. More data are needed to gain insight of on gain and loss of sensory functions during space missions. Further investigation into the multifactorial stressors affecting the somatosensory system during space travel could contribute to advancements in space and pain medicine.
Keywords: chronic pain, quantitative sensory testing, microgravity, radiation, back pain
Introduction
Adaptation to microgravity during space flights imposes significant challenges on the physiological, physical, and psychological well-being of astronauts.1–3 Pain has been frequently reported by astronauts during space missions, immediately after returning to Earth, and even in the years following their flights. Notably, a substantial proportion of astronauts (86%) have reported back and neck pain during the initial days of microgravity exposure, and a similar rate reported using anti-inflammatory drugs to relieve pain post-flight. Furthermore, more than half continue to experience back pain after their return, with 40% undergoing spinal magnetic resonance imaging for evaluation of their back pain.4–6
The exact causes of pain syndromes associated with space flights are not yet fully understood. However, several potential mechanisms have been proposed, including a decrease in muscle mass, increased bone resorption, alterations in intervertebral discs and articular cartilage, and changes in immune response.1–13 Moreover, the effects of space radiation are an additional concern, as they may pose a significant risk for central and peripheral nervous system changes that can impact pain perception.1–11 Other factors affecting the sensory process such as emotional dysregulation, inadequate sleep, sensory deprivation, previous pain experience, or altered cognition/mood may also play a role in postflight pain syndromes.3,12–16
Surprisingly, despite the high prevalence of pain reported by astronauts and the potential mechanisms underlying its occurrence, there is a notable dearth of research specifically examining the pain experience and changes in pain sensation during short trips to the International Space Station (ISS).
This proof of concept study aimed to evaluate the pain experience and potential sensory changes in astronauts during a short travel to the ISS on Axiom Space’s AX-1 commercial space flight.
Materials and Methods
Experimental Design
The participants were Axiom Space’s AX-1 commercial space flight crew to ISS and remained in orbit for seventeen days, completing 240 orbits. A standard day of the study participants included eight hours of sleep following a 16-hour mission day. The participants engage in a bustling daily routine that includes experiments, planning sessions, meals, and exercise. Astronauts must dedicate two hours daily to exercise, utilizing either the treadmill or stationary bicycle. Additionally, crew members actively participate in self-conducted experiments. The private crew successfully executed over 25 diverse research experiments throughout their tenure aboard the ISS.
Ethics and Informed Consent
The study was approved by the National Aeronautics and Space Administration (NASA) Institutional Review Board (#STUDY00000403), the University of Texas - M.D. Anderson Institutional Review Board (#2021-1179), and the McGill University Health Centre for Applied Ethics (#2022-7768). All study procedures were conducted in accordance with the guidelines of the Declaration of Helsinki. Written informed consent was obtained from each participant before the study. After an informed consent briefing in October 2021, two crew members agreed to participate in the study and signed the informed consent forms in December 2021 before the baseline evaluations. Both participants signed a revised consent form in March 2022 following a change in the original protocol. Both subjects have signed informed consent to publish the study.
Data Collection Time Points
Data were collected at four time points: T0, within two weeks before the flight (Pre-Flight); T1, during the flight (In-Flight) except for quantitative sensory testing (QST); T2, within two weeks after the flight (Post-Landing); and T3, three months after the flight (3-month follow-up).
Pain Experience Questionnaires
The following validated pain questionnaires were used to assess various aspects of pain and related factors:
State-Trait Anxiety Inventory (STAI)
This scale measures anxiety in adults and assesses apprehension, tension, nervousness, and worry in response to perceived physical and psychological stress. It has 20 items for assessing trait anxiety and 20 for state anxiety. State anxiety items include: “I am tense; I am worried” and “I feel calm; I feel secure.” Trait anxiety items include: “I worry too much over something that really does not matter” and “I am content; I am a steady person.” All items are rated on a 4-point scale (eg, from “Almost Never” to “Almost Always”). Higher scores indicate more significant anxiety.17
Pain Catastrophizing Scale (PCS)
This scale measures through 13 items the tendency of individuals to catastrophize when experiencing acute or chronic pain. It comprises three components: rumination (PCS-R), magnification (PCS-M), and helplessness (PCS-H). The PCS instructions ask participants to reflect on past painful experiences and to indicate the degree to which they experienced each of 13 thoughts or feelings when experiencing pain on a 5-point scale with the endpoints (0) not at all and (4) all the time. The PCS total score is computed by summing responses to all 13 items. PCS total scores range from 0 to 52.18
Medical Outcomes Short Form 12 Health Survey (SF-12)
Derived from a 36-question version, this 12-question scale measures eight areas of health, including limitations in physical and social activities due to physical or mental health issues, pain, vitality, and general health perceptions. The SF12 data calculate two summary component scores, Physical Component Summary Score (PCS) and Mental Health Component Summary Score (MCS), with eight sub-domains. Scores range from 0 to 100, where a zero score indicates the lowest level of health, and 100 indicates the highest level of health.19
Quebec Back Pain Disability Scale (QBPDS)
The Quebec Back Pain Disability Scale measures functional disability for patients with back pain. Functional disability is operationalized regarding perceived difficulty associated with simple physical activities. The scale has 20 items, representing six empirically derived categories of activities affected by back pain. The items are scored 0 to 5, and the scale provides an overall disability score ranging from 0 to 100 by simple summation of the scores of each item.20
Short-Form McGill Pain Questionnaire (SF-MPQ)
The SF-MPQ is a shorter version of the original MPQ used for standard registration and evaluation of patient pain complaints. The SF-MPQ has two subscales: The sensory subscale with 11 words and the affective subscale with four words. These words or items are rated on an intensity scale as 0 = none, 1 = mild, 2 = moderate and 3 = severe. There is one item for present pain intensity and one for a 10 cm visual analogue scale (VAS) for average pain.21
Qualitative Interview
Each participant completed a 20- to 30-minute semi-structured qualitative interview, conducted remotely and recorded using video-conferencing software. The interviews were transcribed verbatim and analyzed using qualitative description. The semi-structured interview guide consisted of open-ended questions that explored the participants’ experience with pain before, during, and after spaceflight. The conversational nature of the interviews allowed for complementary data collection alongside the pain questionnaires.22 The interview guide followed a funnel format, progressing from general to specific questions, to ensure relevance and meaningfulness to each participant’s experience, ensuring methodological rigor and data integrity.23 Analysis involved repeated reading of each interview transcript to identify overlapping or differing passages between the participants’ narratives. This process provided insights to inform and guide future research on the topic.24
Quantitative Sensory Testing (QST)
Quantitative sensory testing (QST) and the conditioned pain modulation paradigm (CPM) use cutaneous evaluations of somatosensory information using calibrated stimuli and self-report to create a sensory profile for an individual. Several phenotypes, including peripheral sensitization, central sensitization, and inefficient endogenous pain modulation, have been proposed based on the somatosensory profile and the individual facilitatory and inhibitory pain modulation response.25–27 A single tester performed QSTs at time points T0 and T2. A different tester performed the sensory determinations at T3. Patients were given clear and identical instructions before each test.
Mechanical Detection Threshold (MDT)
The MDTs were determined using von Frey filaments in an up/down method. Bending forces between 0.008 and 300 g were sequentially applied to a spot of hairless skin less than 2 mm in diameter for approximately one second. Thresholds were obtained from two test sites: left or right anterior forearm (1–2 inches below the elbow crease) and lower back. The mean of the three last-detected and three first-detected filaments was used to calculate the thresholds.25–27 Mechanical pain may be assessed through pinprick stimulations using needle-like stimulators. It evaluates the function of Aδ-fibers and C-fibers.28,29 Allodynia, described as pain in response to non-nociceptive stimuli, is a phenomenon modulated by A-fibers that can be assessed using Von Frey filaments.28,29
Mechanical Pain Summation (MPS)
Repeated cutaneous pinprick stimulations are used to determine features of central sensitization, which manifests as a sharp increase in pain sensation after repeated pinprick stimulations.30 MPS was determined using a calibrated 40-gram pinprick. A single stimulation was first applied, and participants were asked to rate the pain intensity using a 0–10 numeric rating scale (NRS); 0 = no pain, 10 = worst pain imaginable. After that, ten stimulations at a rate of one contact per second were applied. Then, the astronauts were asked to provide a rating immediately and every 15 seconds post-stimuli for 60 seconds.31 The presence of painful after sensations at the end of the 60 seconds after one and after 10 stimuli were also recorded. The whole sequence was conducted three times. Measurements were obtained from the same test sites as MDT. The wind-up ratio (WUR), a measure for the frequency-dependent increase in excitability of spinal cord neurons, was measured as the ratio of the average pain intensity immediately reported after the train of ten stimuli over the average pain intensity immediately after one stimulus.25,30
Thermal Detection Thresholds
All tests were conducted at room temperature (22°C). Thermal ramps were applied using a calibrated 9 cm2 thermode connected to a Q-sense apparatus (Medoc Advanced Medical Systems, Israel) with a baseline temperature set at 32°C. Skin heating was carried out at a rate of 0.3°C/second to reach the maximum value of 50°C as a security cut-off, while skin cooling used a downslope of 0.3°C/second to reach a limit of 5°C. Thermal thresholds were obtained from three test sites on the left anterior forearm: wrist (trial 1), mid-forearm (trial 2), and upper forearm 1–2 inches below the elbow crease (trial 3). Participants were instructed to rate the pain intensity of each thermal stimulus on the NRS from 0 = no pain to 100 = worst pain imaginable. During each trial, temperatures were recorded when the stimulus was first perceived as painful and unbearable (NRS=100/P100). In addition, moderate pain intensity (NRS=50/P50) was documented when calibrating the heat pain threshold. If a participant failed to register cold pain before the maximum value of 5 °C or heat pain before the maximum value of 50 °C was reached, this was recorded as the default value. The final heat and cold pain thresholds were determined by calculating the mean of three heating and three cooling trials.25 Peripheral sensitization is suggested by QST when a patient reports thermal hyperalgesia. This technique assesses the function of Aδ-fibers and C-fibers. Values obtained experimentally can be compared to reference values available in a healthy population corrected for sex and age and with consideration to the test site.32
Conditioned Pain Modulation
The CPM paradigm is a procedure that investigates to what extent a pain response to a test stimulus can be inhibited through applying a conditioning stimulus.33–35 CPM was evaluated using tonic heat on the right forearm as the test stimulus and immersion of the left forearm in cold water (12 °C) as the conditioning stimulus. The temperature recorded at a pain intensity rating of 50/100 (P50) was designated as the CPM test stimulus. It was determined by averaging the results of three heating trials. To prevent burn injuries, a maximum temperature of 46.9 °C was used. During the first trial, the test stimulus was applied for 120s once the target temperature was reached, while the participants were instructed to rate the pain intensity at 15 seconds intervals. This was immediately followed by the participants submerging their left forearm in cold water for 120s and providing a pain intensity rating every 15 seconds. Once the participants had removed their forearms from the cold water bath, the third trial consisted of a second test stimulus. Average pain intensities were calculated after each trial.25–27
The CPM efficiency was calculated using the percentage difference in average pain intensity of the test stimuli changes:
(100% × (CPMafter – CPMbefore)/CPMbefore)
CPM efficiency was categorized as optimal, suboptimal, and inefficient. CPM efficiency between −100% and −30% was defined as optimal, between −30% and −10% as suboptimal, and between ‑10% and +100% as inefficient. A 30% reduction in pain intensity was considered a clinically relevant difference and approximately the mean value of inhibitory CPM. An inadequate CPM result reflects an incapacity to trigger a proper endogenous pain inhibition.25–27
Results
Participant 1
Pain Questionnaires
Anxiety levels exhibited a decrease over the duration of the study. Catastrophizing tendencies followed a similar pattern, showing a decrease from pre-flight to in-flight, followed by an increase upon return to Earth, and subsequent decline at the three-month post-flight assessment. The impact of physical health on quality of life showed a reduction from T0 to T3, while mental health scores demonstrated an improvement over the same period. Functional disability attributable to back pain was not reported at T0, T1, and T3. However, Participant 1 reported experiencing functional limitations upon returning to Earth. The pain experience exhibited a gradual decline throughout the study, as evidenced by the decrease from T0 to T3 (Figure 1).
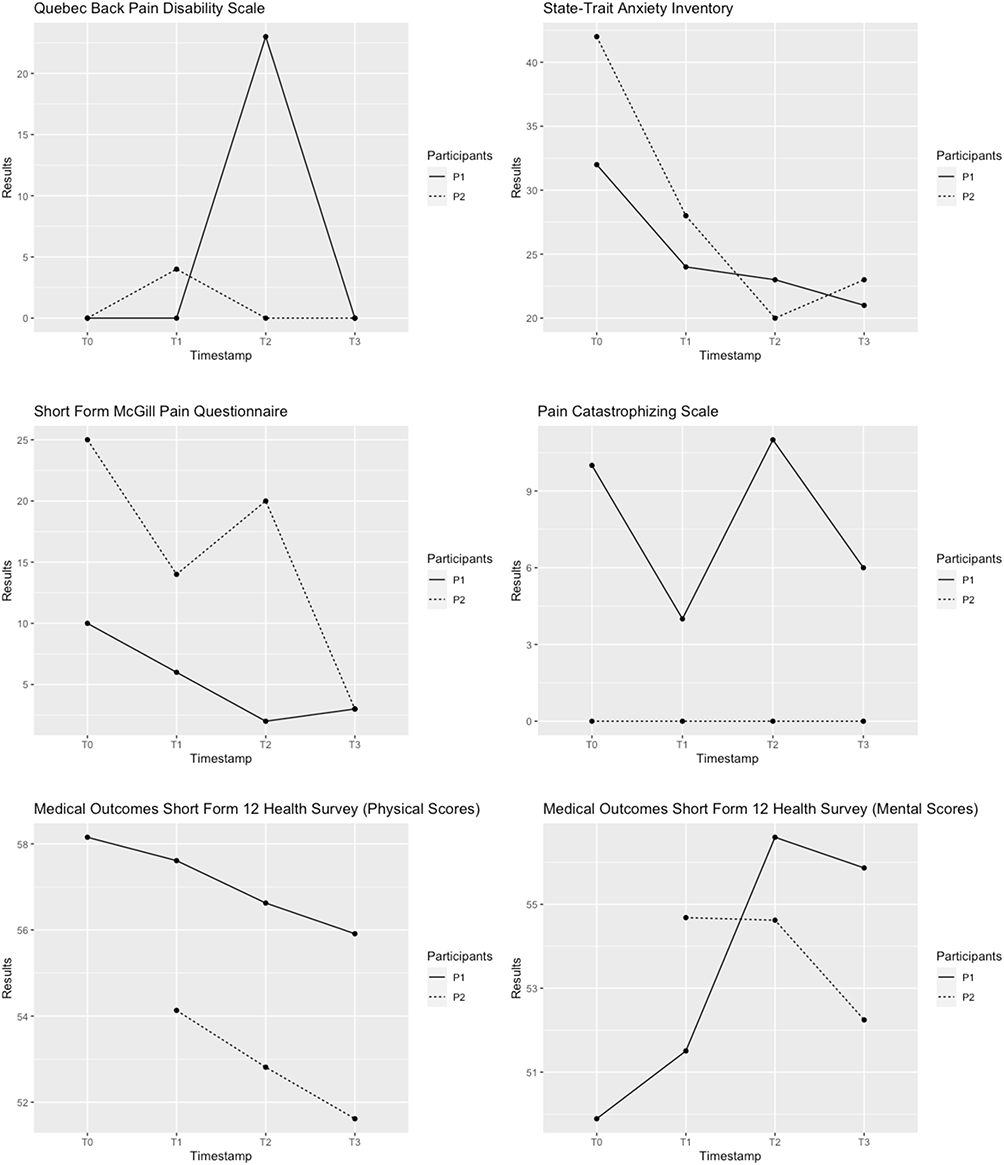 |
Figure 1 Questionnaires to evaluate pain experience. The Quebec Back Pain Disability Scale (QBPDS) assesses functional limitations due to back pain and their fluctuation. The State-Trait Anxiety Inventory (STAI) measures anxiety and considers apprehension, tension, nervousness, and worry in response to perceived physical and psychological stress. The Short Form McGill Pain Questionnaire (SF-MPQ) combines two subscales, sensory and affective, and participants rate their pain experience by selecting words from a list that accurately describe their pain. Pain intensity is rated with a visual analog scale. The Pain Catastrophizing Scale (PCS) measures the tendency of individuals to catastrophize when experiencing acute or chronic pain. It comprises three components: rumination, magnification, and helplessness. The Medical Outcomes Short Form 12 Health Survey (SF-12) measures eight areas of health, including limitations in physical and social activities due to physical or mental health issues, pain, vitality, and general health perceptions. |
Qualitative Interview
Participant 1 recounted his history of playing contact sports, resulting in frequent pain, particularly in his shoulder. He disclosed having undergone four surgical interventions on his shoulder, referring to it as “a lifetime sentence” of pain. Despite this, he clarified that he did not consider himself to have chronic pain, explaining, “I’ve put myself in situations where I feel temporary pain, but I have no chronic pain.” During his space training program, he sustained a knee injury unrelated to the training but endured “intense pain” during several SpaceX simulations.
Upon exposure to microgravity, Participant 1 described experiencing lower back pain and headaches. Although the low-back pain subsided after two to three days on the International Space Station (ISS), he continued to experience a “higher than normal number of headaches.” He also noted feelings of “nausea, disorientation, and general discomfort”, which gradually improved over two to three days. Remarkably, he expressed relief at the absence of shoulder pain throughout the seventeen days in space, stating, “I did not notice any shoulder pain at all for the seventeen days that I was in space. That was great!”
However, upon his return to Earth, he reported that the pain in his shoulder had returned “back to where it was before.” Additionally, he mentioned experiencing muscle soreness and stiffness, particularly in his calves, immediately upon return, likening it to having had an intense calf workout. He further described low back pain, which he characterized as “spasming”, although seven days after his return to Earth (R+7), he reported that the muscle soreness and low back pain had mostly subsided, remarking, “my muscles are getting used to carrying my body around in 1G.”
Participant 1 also shared his pain management strategies during spaceflight. He explained how he had to develop his own technique for donning the space suit due to his shoulder pain. To manage low back pain and headaches during his initial days on-orbit, he self-administered ibuprofen (400mg every four to six hours). Upon returning to Earth, he used Robaxacet to treat his low back pain, and all three of these strategies proved successful in managing his pain.
QST/CPM
Mechanical Detection Threshold: The mechanical detection threshold, reflecting Aβ fiber function,35 showed a gradual increase from pre-flight to post-landing, reaching its highest level at the 3-month follow-up in forearm skin. Notably, alterations in the mechanical detection threshold were also observed in the skin of the lower back. While there was only a minimal change immediately post-landing (T0: 0.017 g vs T2: 0.019 g), the most significant change in threshold occurred at the 3-month follow-up, with an increase to 0.192 g (Figure 2). These findings highlight the dynamic somatosensory changes experienced by astronauts during and after spaceflight.
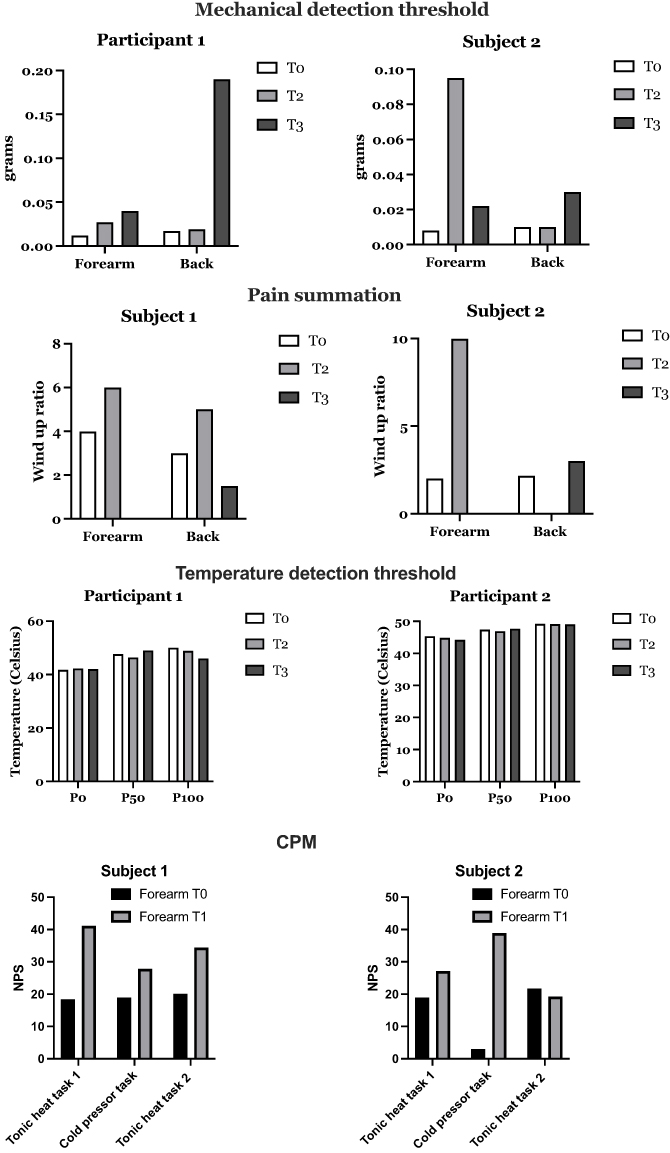 |
Figure 2 Individual sensory profile of astronauts. The somatosensory phenotype of the participants was evaluated with the Quantitative sensory testing (QST) and the conditioned pain modulation paradigm (CPM). Astronauts were tested before landing (T0), after returning from space (T1) and three months after the mission (T3). The mechanical detection threshold, assessed through pinprick stimulations using needle-like stimulators, evaluates the function of Aδ-fibers and C-fibers. Pain summation was considered using repeated cutaneous pinprick stimulations to determine features of central sensitization, which manifests as a sharp increase in pain sensation after repeated pinprick stimulations. The temperature detection threshold was evaluated using a calibrated 9 cm2 thermode connected to a Q-sense apparatus (Medoc Advanced Medical Systems, Israel) with a baseline temperature set at 32°C. During each trial, temperatures were recorded when the stimulus was first perceived as painful and unbearable (NRS=100/P100). In addition, moderate pain intensity (NRS=50/P50) was documented when calibrating the heat pain threshold. Conditioned Pain Modulation (CPM) evaluates the endogenous descending pain inhibitory function by applying tonic heat on the right forearm as the test stimulus and immersion of the left forearm in cold water (12 °C) as the conditioning stimulus. The CPM efficiency was categorized as optimal, suboptimal, and inefficient. CPM efficiency between −100% and −30% was defined as optimal, between −30% and −10% as suboptimal, and between −10% and +100% as inefficient. A 30% reduction in pain intensity was considered a clinically relevant difference. |
Mechanical Pain Summation: The wind-up ratios, indicative of temporal pain summation,30 exhibited similar values in the forearm and lower back pre-flight (forearm: 3.98 vs back: 3.0). However, post-landing, the ratios increased in both test sites (forearm: 6.0 vs back: 5.0). Interestingly, at the 3-month follow-up, the wind-up ratio for the lower back was lower than at baseline (T0). Nevertheless, at time point T3, the wind-up ratio for the forearm could not be calculated due to a denominator of zero (Figure 2).
Thermal Detection Thresholds: As depicted in Figure 2, the initial heat-pain perception threshold increased post-landing and then returned to baseline at the 3-month follow-up (T0: 41.7°C vs T2: 42.3°C vs T3: 41.9°C). Interestingly, the threshold for unbearable heat-pain (NRS = 100) continuously decreased over time, with the lowest value recorded three months post-landing (T0: 50°C vs T2: 48.9°C vs T3: 46°C). The moderate heat-pain threshold (NRS = 50), utilized as the test stimulus for CPM, was reduced post-landing (T0: 47.6°C vs T2: 46.4°C) and increased by 2.5°C at the 3-month follow-up (T2: 46.4°C vs T3: 49.1°C). During pre-flight and post-landing test trials, skin cooling was not perceived as painful. However, at the 3-month follow-up, out of 3 trials, pain was reported once at 5.2°C. Notably, no cold-pain thresholds could be determined at any time point.
Conditioned Pain Modulation: CPM efficiency (Figure 2), reflecting the endogenous descending pain inhibitory pathway,25–27,35 was inefficient pre-flight and suboptimal immediately post-landing (T0: +5.46 vs T1: −16.3). Surprisingly, at the 3-month follow-up, the CPM efficiency decreased once again (T3: +1.5). These findings suggest the complex interplay of pain regulatory mechanisms during and after spaceflight.
Participant 2
Pain Questionnaires
Participant two’s pain-related anxiety exhibited a general decrease throughout the study, but there was a notable spike during orbit. However, no catastrophizing was reported at any point in the study. The impact of physical health on quality of life showed a slight improvement over time, while mental health remained stable from in-flight to the 3-month follow-up. It should be noted that during the pre-flight assessment, Participant 2 omitted to answer several questions on the SF-12 questionnaire, making it challenging to compile a comprehensive score for this specific time point. Despite a slight increase in test scores in-flight, no functional disability was observed throughout the study. The pain experience, as measured by the pain questionnaires, demonstrated an overall decrease from pre-flight to the 3-month follow-up (Figure 1). These findings offer insights into the dynamic nature of pain and psychological well-being experienced by astronauts during and after spaceflight missions.
Qualitative Interview
Participant 2 shared his perspective on previous experiences with pain, describing them as “pretty average”, often related to injuries, with his most recent being a tibia fracture four years ago. During his space training program, he encountered pain and soreness in his tibia, depending on his level of exercise, standing, and walking. This discomfort became “predictable” over time.
Once exposed to microgravity, Participant 2 recounted experiencing “fairly significant lower back pain early on” and also mentioned pain in his left iliotibial band. Upon return to Earth, he described pain in his distal tibia, especially when getting up from a chair or after being off his right leg for a while.
When I said pre-flight that the pain became predictable, it is fairly painful when I get up in the morning or when I get up out of a chair or something that I’m off my right leg for a while, the first few steps are quite painful. And effectively, I was off my right leg for seventeen days, so coming back from that was really pretty uncomfortable for I would say, 24 to 36 hours.
To manage his pain, Participant 2 self-administered anti-inflammatory medication for his iliotibial band pain during the initial days aboard the ISS. He found stretching helpful in alleviating low back pain: “it’s very helpful to stretch and to actually wrap something around your lower back and your knees, kind of pull your knees to your chest.” Sleeping in this position also provided relief. At the time of the interview, eight days after splashdown, he was still using anti-inflammatories to manage his pain.
Furthermore, when asked if he wanted to add anything, Participant 2 expressed that the questionnaires provided during the study were not very helpful in identifying or characterizing his experience accurately. While he answered truthfully, the questionnaires “didn’t capture [his] experience very well” and he was not sure they were “very reflective of the experience [he] was having.” He questioned their suitability for space travelers, citing an example of a questionnaire asking about pain interfering with housework. Despite this, he acknowledged the value of the interview in providing additional context to the questionnaire responses. This insight highlights the challenges in assessing and characterizing pain experiences in the unique environment of spaceflight.
QST/CPM
Mechanical Detection Threshold: In the skin of the lower back, the mechanical detection thresholds tripled at the 3-month follow-up compared to the pre-flight and post-landing values (Figure 2, T0 and T2: 0.01 vs T3: 0.030). On the other hand, in forearm skin, the mechanical detection threshold was highest immediately post-landing (T0: 0.008 vs T2: 0.095) and decreased at the 3-month follow-up (T3: 0.023).
Mechanical Pain Summation: The WUR primarily increased immediately post-landing in the skin of the forearm (T0: 2, T2: 10). At T3, the ratio could not be determined because the denominator was zero. Ratios in the lower back pre-flight and at the 3-month follow-up were similar (T0: 2.17, T3: 3.03), while the ratio for timepoint T2 could not be calculated (Figure 2).
Thermal Detection Thresholds: This participant’s perception of pain was slightly altered (Figure 2). Pre-flight, heat pain was initially perceived at 45.3°C, with thresholds further lowered at T2 (44.8°C) and T3 (44.4°C). Consistent with this, unbearable heat-pain thresholds minimally decreased from 49.2°C (T0) to 48.9°C (T3) at the 3-month follow-up. Moderate heat-pain threshold also slightly reduced post-flight (T0: 47.4°C vs T2: 46.9°C); however, at the 3-month follow-up, we observed almost identical thresholds as before exposure to microgravity (T3: 47.6°C vs T0: 47.4°C). Similar to participant 1, no pain from skin cooling was reported at timepoints T1 and T3, while post-landing skin cooling was perceived as painful in only one out of 3 trials at 5.2°C. Hence, no thresholds could be calculated.
Conditioned Pain Modulation: In line with participant 1, CPM was highly inefficient pre-flight and at the 3-month follow-up (T0: 14.70, T3: 323.1, Figures 2 and 3) while efficiency was markedly improved immediately after microgravity exposure (T2: −29.1).
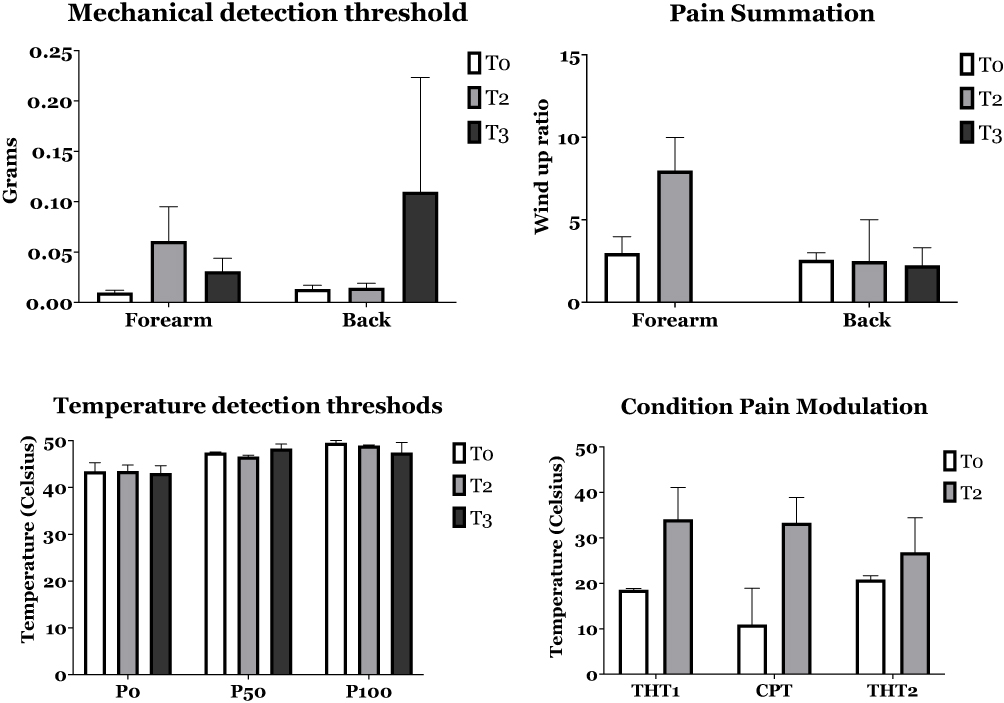 |
Figure 3 Aggregated QST data from both astronauts. The figure illustrates aggregated data from sensory thresholds from participants 1 and 2. Data are expressed in the mean and standard error of the mean. Abbreviations: CPT, Cold pressor task; THT, Tonic heat task. |
Discussion
The present proof of concept investigation examined two astronauts’ pain experience and changes in pain perception during their seventeen-day stay in orbit at the International Space Station (ISS). Both astronauts reported experiencing musculoskeletal pain during the flight and after landing, but they were able to effectively manage their symptoms using anti-inflammatories and stretching techniques. The pain levels returned to preflight levels after three months. However, the questionnaires used to assess the pain experience were found to be inconsistent and inappropriate by one of the participants. A qualitative interview post-landing allowed the astronauts to provide a more comprehensive description of their pain experience during the flight. Post-flight, both astronauts exhibited alterations in pain perception, including increased mechanical touch detection thresholds, temporal pain summation, heat pain thresholds, and differences in conditioned pain modulation.
The pain experience reported by both astronauts aligns with previous findings in astronauts exposed to microgravity.36 The term “space adaptation pain” is used to describe the acute onset of low back pain occurring within the first 24–48 hours of exposure to microgravity, lasting for 9–15 days. In-flight surveys conducted over 15 days revealed that pain incidence and intensity were highest during the first two days, followed by a gradual decrease in incidence. Notably, previous studies have reported significantly lower post-flight low back pain incidence (10%) after a 15-day flight compared to longer duration flights (40–50%).37,38 Astronauts with previous low back pain referred an increase on their previous pain. In contrast, astronauts reporting low back pain for first-time experienced pain with a distribution between L1 and L3.38 In this study, both participants had preexisting asymptomatic spinal pathology, which is acknowledged as a risk factor for in-flight back pain.6,38 Further investigations are required to compare astronauts with and without symptomatic pre-existing spine pathology, as well as those with and without low back pain, both prior to and during space flights.
The overall decrease in anxiety and pain, coupled with the increase in mental health, suggests that external factors, such as the extraordinary opportunity and experience of space flight, could influence the overall emotional experience of pain in space, different from that on Earth. While previous studies have emphasized the risks to psychological well-being during space flight, the majority of these studies have focused on long-duration flights and professional astronauts.3 The results of the pain questionnaires highlight the need to contextualize participants’ pain experience within the unique context of space travel, particularly for short-term flights involving non-professional astronauts.
Interestingly, Participant 2 exhibited a complete lack of catastrophizing, which is unusual considering the increased pain perception. Previous literature has linked increased stress with higher levels of pain catastrophizing.39 The absence of pain catastrophizing in Participant 2 may indicate specific psychological traits, such as stoicism, not commonly prevalent in the general population. On the other hand, Participant 1 showed signs of low-grade disability, with a significant increase in his QBPDS score and an increase in catastrophizing, consistent with existing literature on the relationship between catastrophizing and disability.40
It is essential to consider the limitations of the questionnaires used in this study, which were designed and validated for the general population or patients with chronic pain conditions in clinical settings on Earth. As such, they may only partially reflect new onset pains associated with space flight. Moreover, these questionnaires may not adequately capture the magnitude of new pain experiences or account for the participants’ training or previous space flight experience, all variables that may influence pain perception and reporting. The timing of questionnaire administration may also have influenced the responses, and administering questionnaires at multiple timepoints during the flight could provide a more comprehensive understanding of the changes in pain experience during the journey.
These challenges underscore the need to develop pain experience measurement tools tailored to professional or commercial astronauts, with greater sensitivity to lower pain levels, more relevant questions regarding the reality of space travel, and capturing the previous spaceflight experience of participants. Additionally, evaluating the impact of in-flight pain on daily function under microgravity conditions can shed light on the effect of pain experienced during space travel.
The qualitative interview provided valuable insights complementing the validated questionnaires by capturing essential aspects of the astronauts’ pain experience, including changes in previous pain and coping strategies during and after the space flight. Moreover, the interview allowed participants to contextualize the magnitude of their pain, distinguishing between pain experience and nociceptive changes. Furthermore, the qualitative discussion highlighted the need for a different approach to evaluating experienced, trained personnel in space flights versus non-professional astronauts. Therefore, future research should include qualitative interviews to provide context to the collected data on pain in space.
The present proof of concept study suggested that alterations in nociception and changes in pain sensation may exist after a short trip to the ISS. The mechanical touch detection thresholds increased in both participants post-flight but remained within reported normative thresholds, suggesting that if an impaired Aβ-fiber function was present, it was not clinically relevant.41,42 Both participants also did not report impairment in tasks related to Aβ-fiber function (ie, buttoning). The increase in WUR in both test sites post-landing suggests transient central sensitization due to the rapid facilitation of synaptic transmission between nociceptive afferents and spinal projection neurons.31
Regarding heat pain, mediated by unmyelinated fibers, it was minimally affected after the flight, and both participants reported normal heat pain thresholds according to age and race.42–45 However, cold pain was rarely perceived, possibly due to the chosen cut-off of 5°C being too high, preventing the determination of thresholds. It is plausible that factors like previous pain experience, intense training, stoicism, and lack of pain reporting may have contributed to perception aberrations and pseudo-reduction in sensory responses, similar to findings observed in athletes, who displayed higher pain tolerance and alterations in pain thresholds. Moreover, evidence indicates that pain perception is reduced after strenuous exercise.
CPM was suboptimal post-landing, suggesting an inefficient descending endogenous pain inhibitory control mediated by serotonin and norepinephrine, a dysfunctional inhibition phenotype.4,36,45,46 A similar phenomenon was recently identified in an observational cohort with chronic musculoskeletal pain.25 These findings call for attention on the complexity of pain modulation and sensory changes experienced by astronauts during space travel. However, more data is needed to understand the extent and magnitude of the sensory changes related to space travel.
We applied a QST and CPM protocol mainly used for research purposes to identify alterations in sensory function, particularly young adults with musculoskeletal conditions, and patients with cancer. We used the normalized our results using the German Research Network on Neuropathic Pain and previous other groups to assure repeatability.25,27,34,42,43,45,46 We used the forearm and lower back for the von Frey filament and pinprick assessment (temporal summation). It is challenging to detect mechanical pressure accurately in the trunk because its region does not have a high concentration of A-Beta fibres. However, the attenuation of the paraspinal muscle morphology may contribute to back pain in astronauts.4 The forearm was chosen as a musculoskeletal control area for intra-individual differences in mechanical sensory assessment because it has similar spatial acuity to the lower back.47
We evaluated the thermal thresholds stimulating on three different areas of the forearm to prevent subsequent reporting of lower thresholds potentially caused by heat-induced hyperalgesia from the previous trial.48
Finally, we only conducted a thermal CPM assessment and paradigm because it is an experimental model to measure excitatory and inhibitory pain mechanisms in one testing session.36 However, this methodology is not the common protocol used for clinical use by other groups.46 Future studies should include more mechanical sensory assessment like pressure pain threshold to align the results to a clinical standardized QST protocols.
Potential Explanations of Findings
Terminal endings of sensory neurons in the dermis and epidermis may be particularly vulnerable to space radiation-induced damage, as skin-level radiation doses are 5–10 times higher than those experienced by internal organs.12 Consequently, astronauts frequently report skin-related issues such as itching, rashes, and dryness during space flights. While high doses of medical radiation can damage nerves by affecting their vascular supply, low dosages experienced during space flights can also lead to neuronal damage.13 Additionally, microgravity can induce adaptive changes in skin cell function and shape.15,16 Studies have shown that fibroblasts and keratinocytes exhibit altered gene expression after exposure to simulated microgravity, and when combined with low-dose ionic radiation, this could potentially trigger changes in neuronal terminals and sensory processing.16,39 It is yet to be ascertained if multiple exposures to microgravity result in a recurring impact on an already altered nociceptive system.
Prolonged spinal unloading, as experienced during spaceflight or bed rest, can lead to intervertebral disc swelling.49 The unloading of the spine in microgravity may cause the discs to become over-saturated with water, leading to swelling. This increased disc volume can result in tensile stress within the nucleus pulposus, causing stretching of the annulus fibrosis and abnormal innervation, particularly in the outer annulus fibrosus. Increased disc innervation is more prevalent in individuals with existing spinal pathologies.9,38,50
The stretching of the disc annulus fibrosus can activate the Cox-2 pathways, resulting in increased production of prostaglandin E2 (PGE2), which can cause hyperalgesia and mechanical allodynia, contributing to pain.51,52 Spaceflight also impacts bone health by stimulating bone resorption.53 Bone turnover, which is generally a slow process, increases significantly within 10 to 14 days of spaceflight and remains stable thereafter.53 Bone resorption is associated with pain sensitization to thermal stimuli.54 Additionally, spinal elongation is a well-known effect of exposure to microgravity, which may impact major neural pathways.55 Moreover, returning from space has been associated with persistent modulation of the sensory and motor systems.56,57 Thus, the nociceptive system’s alteration after multiple exposures to microgravity cannot be ruled out and might partly explain the presence of low back pain and the quantitative sensory testing (QST) results.
Conclusion
This proof of concept study suggested that, at least in part, space flight exerts diverse effects on the pain experience and on various sensory perception and regulation aspects of nociception with variability among individuals. Due to the small sample size (n = 2), these preliminary results need a cautious interpretation and no causal or definitive implications could be drawn. More data is required to understand and confirm the observed changes in sensory functions and pain experience.
Acknowledgments
The authors would like to thank the Axiom team for their support and expertise. We would also want to thank Dr. Don Daniel Okay for his constant support and expertise.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by a grant from the Montreal Children’s Hospital Foundation to Dr. Ingelmo.
Disclosure
All authors declare no competing interests in this work.
References
1. Fritsch-Yelle JM, Charles JB, Jones MM, Wood ML. Microgravity decreases heart rate and arterial pressure in humans. J Appl Physiol. 1996;80:910–914. doi:10.1152/jappl.1996.80.3.910
2. Roberge E. The gravity of it all: from osteoporosis to immunosuppression, exploring disease in a microgravity environment holds promise for better treatments on earth. IEEE Pulse. 2014;5:35–41. doi:10.1109/MPUL.2014.2321933
3. Arone A, Ivaldi T, Loganovsky K, et al. The burden of space exploration on the mental health of astronauts: a narrative review. Clin Neuropsychiatry. 2021;18:237–246. doi:10.36131/cnfioritieditore20210502
4. Burkhart K, Allaire B, Bouxsein ML. Negative effects of long-duration spaceflight on paraspinal muscle morphology. Spine. 2019;44:879–886. doi:10.1097/BRS.0000000000002959
5. Chang DG, Healey RM, Snyder AJ, et al. Lumbar spine paraspinal muscle and intervertebral disc height changes in astronauts after long-duration spaceflight on the international space station. Spine. 2016;41:1917–1924. doi:10.1097/BRS.0000000000001873
6. Shackelford LC Musculoskeletal response to space flight. Principles of Clinical Medicine for Space Flight; 2019:581–607.
7. Bailey JF, Miller SL, Khieu K, et al. From the international space station to the clinic: how prolonged unloading may disrupt lumbar spine stability. Spine J. 2018;18:7–14. doi:10.1016/j.spinee.2017.08.261
8. Treffel L, Navasiolava N, Mkhitaryan K, et al. DI-5-cuffs: lumbar intervertebral disc proteoglycan and water content changes in humans after five days of dry immersion to simulate microgravity. Int J Mol Sci. 2020;21. doi:10.3390/ijms21113748
9. Harrison MF, Garcia KM, Sargsyan AE, Ebert D, Riascos-Castaneda RF, Dulchavsky SA. Preflight, in-flight, and postflight imaging of the cervical and lumbar spine in astronauts. Aerosp Med Hum Perform. 2018;89:32–40. doi:10.3357/AMHP.4878.2018
10. Hides JA, Lambrecht G, Sexton CT, et al. The effects of exposure to microgravity and reconditioning of the lumbar multifidus and anterolateral abdominal muscles: implications for people with LBP. Spine J. 2021;21:477–491. doi:10.1016/j.spinee.2020.09.006
11. Hides JA, Lambrecht G, Stanton WR, Damann V. Changes in multifidus and abdominal muscle size in response to microgravity: possible implications for low back pain research. Eur Spine J. 2015;25:175–182. doi:10.1007/s00586-015-4311-5
12. Kim M-HY, George KA, Cucinotta FA. Evaluation of skin cancer risk for lunar and Mars missions. Adv Space Res. 2006;37:1798–1803. doi:10.1016/j.asr.2006.03.032
13. Delanian S, Lefaix J-L, Pradat P-F. Radiation-induced neuropathy in cancer survivors. Radiother Oncol. 2012;105:273–282. doi:10.1016/j.radonc.2012.10.012
14. Cialdai F, Vignali L, Morbidelli L, et al. Modeled microgravity affects fibroblast functions related to wound healing. Microgravity Sci Technol. 2017;29:121–132. doi:10.1007/s12217-016-9532-7
15. Loesberg WA, Walboomers XF, Bronkhorst EM, van Loon JJWA, Jansen JA. The effect of combined simulated microgravity and microgrooved surface topography on fibroblasts. Cell Motil Cytoskelet. 2007;64:174–185. doi:10.1002/cm.20174
16. Clement JQ, Lacy SM, Wilson BL. Gene expression profiling of human epidermal keratinocytes in simulated microgravity and recovery cultures. Genom Proteom Bioinform. 2008;6:8–28. doi:10.1016/S1672-0229(08)60017-0
17. Gaudry E, Vagg P, Spielberger CD. Validation of the state-trait distinction in anxiety research. Multivariate Behav Res. 1975;10:331–341. doi:10.1207/s15327906mbr1003_6
18. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7:524–532. doi:10.1037/1040-3590.7.4.524
19. Ware JE, Kosinski M, Keller SD. A 12-item short-form health survey. Med Care. 1996;34:220–233. doi:10.1097/00005650-199603000-00003
20. Kopec JA, Esdaile JM, Abrahamowicz M, et al. The Quebec back pain disability scale: conceptualization and development. J Clin Epidemiol. 1996;49:151–161. doi:10.1016/0895-4356(96)00526-4
21. Melzack R, Raja Srinivasa N. The McGill pain questionnaire. Anesthesiology. 2005;103:199–202. doi:10.1097/00000542-200507000-00028
22. Neergaard MA, Olesen F, Andersen RS, Sondergaard J. Qualitative description – the poor cousin of health research? BMC Med Res Methodol. 2009;9. doi:10.1186/1471-2288-9-52
23. Milne J, Oberle K. Enhancing rigor in qualitative description. J Wound Ostomy Cont Nurs. 2005;32:413–420. doi:10.1097/00152192-200511000-00014
24. Patton MQ. Qualitative Research & Evaluation Methods: Integrating Theory and Practice.
25. Ocay DD, Larche CL, Betinjane N, et al. Phenotyping chronic musculoskeletal pain in male and female adolescents: psychosocial profiles, somatosensory profiles and pain modulatory profiles. J Pain Res. 2022;15:591–612. doi:10.2147/JPR.S352607
26. Ocay DD, Ross BD, Moscaritolo L, et al. The psychosocial characteristics and somatosensory function of children and adolescents who meet the criteria for chronic nociplastic pain. J Pain Res. 2023;16:487–500. doi:10.2147/JPR.S397829
27. Teles AR, Ocay DD, Bin Shebreen A, et al. Evidence of impaired pain modulation in adolescents with idiopathic scoliosis and chronic back pain. Spine J. 2019;19:677–686. doi:10.1016/j.spinee.2018.10.009
28. Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by central neural plasticity. J Pain. 2009;10:895–926. doi:10.1016/j.jpain.2009.06.012
29. La JH, Chung JM. Peripheral afferents and spinal inhibitory system in dynamic and static mechanical allodynia. Pain. 2017;158:2285–2289. doi:10.1097/j.pain.0000000000001055
30. Herrero JF, Laird JM, Lopez-Garcia JA. Wind-up of spinal cord neurones and pain sensation: much ado about something? Prog Neurobiol. 2000;61:169–203. doi:10.1016/S0301-0082(99)00051-9
31. Clarke RW, Eves S, Harris J, Peachey JE, Stuart E. Interactions between cutaneous afferent inputs to a withdrawal reflex in the decerebrated rabbit and their control by descending and segmental systems. Neuroscience. 2002;112:555–571. doi:10.1016/S0306-4522(02)00093-3
32. Mücke M, Cuhls H, Radbruch L, et al. Quantitative sensory testing (QST). English version. Schmerz. 2016;35:153–160. doi:10.1007/s00482-015-0093-2
33. Kunz M, Bunk SF, Karmann AJ, Bar KJ, Lautenbacher S. Conditioned Pain Modulation (CPM) effects captured in facial expressions. J Pain Res. 2021;14:793–803. doi:10.2147/JPR.S300313
34. Cata JP, Weng HR, Burton AW, Villareal H, Giralt S, Dougherty PM. Quantitative sensory findings in patients with bortezomib-induced pain. J Pain. 2007;8:296–306. doi:10.1016/j.jpain.2006.09.014
35. Tousignant-Laflamme Y, Pagé S, Goffaux P, Marchand S. An experimental model to measure excitatory and inhibitory pain mechanisms in humans. Brain Res. 2008;1230:73–79. doi:10.1016/j.brainres.2008.06.120
36. Laughlin MS, Murray JD, Wear ML, Van Baalen M Post-flight back pain following international space station missions: evaluation of spaceflight risk factors;
37. Johnston SL, Campbell MR, Scheuring R, Feiveson AH. Risk of herniated nucleus pulposus among U.S. astronauts. Aviat Space Environ Med. 2010;81:566–574. doi:10.3357/ASEM.2427.2010
38. Pool-Goudzwaard AL, Belavý DL, Hides JA, Richardson CA, Snijders CJ. Low back pain in microgravity and bed rest studies. Aerosp Med Hum Perform. 2015;86:541–547. doi:10.3357/AMHP.4169.2015
39. McHugh RK, Kneeland ET, Edwards RR, Jamison R, Weiss RD. Pain catastrophizing and distress intolerance: prediction of pain and emotional stress reactivity. J Behav Med. 2020;43:623–629. doi:10.1007/s10865-019-00086-5
40. Michaelides C, Nguyen TN, Chiappa KH, Kwolek CJ, Simon MV. Cerebral embolism during elective carotid endarterectomy treated with tissue plasminogen activator: utility of intraoperative EEG monitoring. Clin Neurol Neurosurg. 2010;112:446–449. doi:10.1016/j.clineuro.2010.01.009
41. Dougherty PM, Cata JP, Cordella JV, Burton A, Weng HR. Taxol-induced sensory disturbance is characterized by preferential impairment of myelinated fiber function in cancer patients. Pain. 2004;109:132–142. doi:10.1016/j.pain.2004.01.021
42. González‐Duarte A, Lem‐Carrillo M, Guerrero‐Torres L. Normative values of quantitative sensory testing in Hispanic Latino population. Brain Behav. 2016;6:e00466. doi:10.1002/brb3.466
43. Yarnitsky D, Sprecher E, Zaslansky R, Hemli JA. Heat pain thresholds: normative data and repeatability. Pain. 1995;60:329–332. doi:10.1016/0304-3959(94)00132-X
44. Rolke R, Baron R, Maier C, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): standardized protocol and reference values. Pain. 2006;123:231–243. doi:10.1016/j.pain.2006.01.041
45. Yarnitsky D, Bouhassira D, Drewes AM, et al. Recommendations on practice of conditioned pain modulation (CPM) testing. Eur J Pain. 2015;19:805–806. doi:10.1002/ejp.605
46. Suzuki H, Tahara S, Mitsuda M, et al. Current concept of quantitative sensory testing and pressure pain threshold in neck/shoulder and low back pain. Healthcare (Basel). 2022;10(8):1485. doi:10.3390/healthcare10081485
47. Mancini F, Bauleo A, Cole J, et al. Whole-body mapping of spatial acuity for pain and touch. Ann Neurol. 2014;75:917–924. doi:10.1002/ana.24179
48. Jürgens TP, Sawatzki A, Henrich F, Magerl W, May A. An improved model of heat-induced hyperalgesia--repetitive phasic heat pain causing primary hyperalgesia to heat and secondary hyperalgesia to pinprick and light touch. PLoS One. 2014;9:e99507. doi:10.1371/journal.pone.0099507
49. Urban JPG, Holm S, Maroudas A, Nachemson A. Nutrition of the intervertebral disc. Clin Orthop Relat Res. 1982;170. doi:10.1097/00003086-198210000-00039
50. Groh AMR, Fournier DE, Battié MC, Séguin CA. Innervation of the human intervertebral disc: a scoping review. Pain Med. 2021;22:1281–1304. doi:10.1093/pm/pnab070
51. Zhang F, Huan L, Xu T, et al. Inflammatory macrophages facilitate mechanical stress-induced osteogenesis. Aging. 2020;12:3617–3625. doi:10.18632/aging.102833
52. Chen J, Liu Z, Zhong G, et al. Cyclic stretch enhances apoptosis in human lumbar ligamentum flavum cells via the induction of reactive oxygen species generation. J Spinal Cord Med. 2016;39:450–454. doi:10.1080/10790268.2016.1141470
53. Stavnichuk M, Mikolajewicz N, Corlett T, Morris M, Komarova SV. A systematic review and meta-analysis of bone loss in space travelers. Microgravity. 2020;6. doi:10.1038/s41526-020-0103-2
54. Abdelaziz DM, Stone LS, Komarova SV. Osteolysis and pain due to experimental bone metastases are improved by treatment with rapamycin. Breast Cancer Res Treat. 2014;143:227–237. doi:10.1007/s10549-013-2799-0
55. Thornton W, Hoffler G, Rummel J Anthropometric changes and fluid shifts. Biomedical results from Skylab. Scientific and Technical Information Office. National Aeronautics and Space Administration:[for sale by the Supt of Docs, US Govt Print Off]; 1976:330–339.
56. Clement G, Wood SJ. Rocking or rolling--perception of ambiguous motion after returning from space. PLoS One. 2014;9:e111107. doi:10.1371/journal.pone.0111107
57. Green DA, Scott JPR. Spinal health during unloading and reloading associated with spaceflight. Front Physiol. 2017;8:1126. doi:10.3389/fphys.2017.01126
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychosocial Characteristics and Somatosensory Function of Children and Adolescents Who Meet the Criteria for Chronic Nociplastic Pain
Ocay DD, Ross BD, Moscaritolo L, Ahmed N, Ouellet JA, Ferland CE, Ingelmo PM
Journal of Pain Research 2023, 16:487-500
Published Date: 15 February 2023
Thermal Grill Illusion in Chronic Lower Back Pain: A Case-Control Study
Kim HC, Chang MC, Oh SH, Lee SB, Yang SY, Shin DA
Journal of Pain Research 2023, 16:1573-1579
Published Date: 17 May 2023
Navigating Pregnancy Testing in Chronic Pain Management for Women of Reproductive Age
Tamura S, Vardhan S, Breidenbach K, Shaparin N, Vydyanathan A, Gritsenko K
Journal of Pain Research 2025, 18:2605-2612
Published Date: 21 May 2025
AstroOphthalmology: Basic and Pathophysiological Concepts of Space-Induced Ocular Changes
Cheraqpour K, Shahriari M, Ghazi M, Heydari N, Moshfeghi S, Mousavi Ganji SM, Asgari S, Cheraqpour S
Eye and Brain 2026, 18:611235
Published Date: 22 May 2026