Back to Journals » Clinical Interventions in Aging » Volume 21
Associations of Sleep Quality with Cognitive Function in Chinese Older Adults: The Roles of Self-Efficacy and Depressive Symptoms
Authors Wang L, Wang Y, Huo J, Luo Y, Ding Y, Wang Z ![]()
Received 26 January 2026
Accepted for publication 7 May 2026
Published 20 May 2026 Volume 2026:21 594997
DOI https://doi.org/10.2147/CIA.S594997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Liqun Wang,1,2,* Yali Wang,1,* Junhao Huo,1 Yiling Luo,3 Yuyan Ding,1 Zhizhong Wang4
1Department of Epidemiology and Health Statistics, School of Public Health, Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China; 2Key Laboratory of Environmental Factors and Chronic Disease Control, Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China; 3Department of Health Management Center, People’s Hospital of Ningxia Hui Autonomous Region, Yinchuan, Ningxia, People’s Republic of China; 4Department of Epidemiology and Statistics, School of Public Health, Guangdong Medical University, Dongguan, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhizhong Wang, Department of Epidemiology and Statistics, School of Public Health, Guangdong Medical University, Dongguan, Guangdong, People’s Republic of China, Tel +8613469598129, Email [email protected]
Objective: To examine the associations among sleep quality, self-efficacy, depressive symptoms, and cognitive function in older adults, and to explore whether self-efficacy may be involved in the association between sleep quality and cognitive function and whether depressive symptoms may moderate this association.
Methods: A cross-sectional survey was conducted among 2,030 older adults in Ningxia, China. Sleep quality, cognitive function, self-efficacy, and depressive symptoms were assessed using validated instruments. After adjusting for age, gender, marital status, education level, residence, smoking and drinking status, living alone, exercise, hypertension, diabetes, and coronary heart disease, mediation and moderated mediation analyses were performed using the PROCESS macro.
Results: Significant correlations were observed among sleep quality, self-efficacy, depressive symptoms, and cognitive function. Self-efficacy showed a significant indirect effect in the association between sleep quality and cognitive function (B = − 0.034, 95% CI: − 0.048 to − 0.022). In addition, depressive symptoms significantly moderated the association between self-efficacy and cognitive function (B = 0.009, p < 0.01). The magnitude of the indirect association between sleep quality and cognitive function through self-efficacy was stronger at higher levels of depressive symptoms.
Conclusion: Poor sleep quality was associated with poorer cognitive function in older adults, and self-efficacy may be involved in this association. Depressive symptoms may further strengthen this indirect association. These findings suggest that sleep quality, self-efficacy, and depressive symptoms may all be relevant to cognitive health among older adults.
Plain Language Summary: Memory and thinking problems become more common with age. Poor sleep is also common in older adults and may be linked to worse brain health. However, less is known about the emotional and psychological factors that may be involved in this relationship. We carried out this study to better understand how sleep quality, confidence in handling daily challenges, and depressive symptoms are related to cognitive function in older adults.
We studied 2,030 older adults in Ningxia, China. We collected information on their sleep quality, depressive symptoms, and self-efficacy, which refers to a person’s confidence in managing problems and daily tasks. We also assessed cognitive function, including memory and other thinking abilities. We then examined how these factors were related to one another.
We found that older adults with poorer sleep quality tended to have lower cognitive function. Poorer sleep was also linked to lower self-efficacy, and lower self-efficacy was linked to poorer cognitive function. In addition, depressive symptoms were related to a stronger negative relationship between self-efficacy and cognitive function.
These findings suggest that sleep, mood, and confidence in daily self-management may all be important for cognitive health in older adults. This does not prove cause and effect, but it highlights several factors that may be useful for future prevention and support. Efforts to improve sleep and support emotional well-being may help promote healthy cognitive aging.
Keywords: sleep quality, cognitive function, self-efficacy, depressive symptoms, older adults, moderated mediation
Introduction
Cognitive impairment, including mild cognitive impairment (MCI) and dementia, is common among older adults. According to the World Health Organization (WHO), approximately 57 million people worldwide were living with dementia in 2021, with nearly 10 million new cases occurring each year. WHO further projects that the global number of people with dementia will reach around 78 million by 2030 and 139 million by 2050.1 As population aging accelerates worldwide, the burden of dementia continues to increase, placing growing pressure on healthcare systems, particularly in the provision of long-term care and dementia-related services.1 In China, the burden of Alzheimer’s disease and related dementias, as well as mild cognitive impairment, is especially high among adults aged 60 years and older,2 with the rates increasing significantly for those aged 65 and older.3 Previous studies have shown that, among Chinese adults aged 60 years and older, the prevalence of dementia is approximately 6.0%, affecting about 15.07 million people, while the prevalence of MCI is about 15.5%, affecting approximately 38.77 million people.4 Despite this growing burden, effective treatments and disease-specific medications for neurodegenerative disorders remain limited.5 Therefore, identifying modifiable factors associated with cognitive function is essential for delaying cognitive decline and promoting healthy aging.
In recent years, sleep quality has emerged as an important factor associated with cognitive function and has received increasing attention from researchers.6,7 Sleep disturbances are common among older adults, with reports suggesting that up to 41% of individuals aged 60 years and older experience sleep-related problems.8 A recent review of systematic reviews and meta-analyses indicated that sleep disturbances have a significant negative impact on cognitive function.9 Consistent with this evidence, epidemiological and clinical studies have shown that poor sleep quality is closely associated with cognitive impairment and may represent both an early indicator and a potential risk factor for cognitive decline in later life.10–13 Several biological mechanisms may underlie this association, including plasma Aβ accumulation, inflammation, abnormal function of the suprachiasmatic nucleus in the anterior hypothalamus, altered melatonin secretion, and dysregulation of neuronal cAMP and GABA signaling pathways.11 However, compared with the growing evidence on biological mechanisms, relatively limited research has examined the psychological pathways through which sleep quality may be associated with cognitive impairment.
Self-efficacy may represent one such psychological pathway. Self-efficacy refers to an individual’s belief in their ability to achieve specific goals or desired outcomes.14 As an important psychological resource, it has been linked to health-related behaviors and adaptation to challenges.15 Previous studies suggest that higher self-efficacy is associated with better sleep-related self-management and healthier sleep patterns.16,17 In addition, self-efficacy has been identified as an important predictor of cognitive abilities and behaviors.18,19 Taken together, these findings suggest that self-efficacy may be associated with both sleep quality and cognitive function, and may therefore represent a potential psychological pathway linking the two.
Depression may be another important factor within this pathway. Depression is common among older adults and is closely associated with self-efficacy. Blazer proposed that self-efficacy can be enhanced through successfully addressing and overcoming specific challenges, such as depression.20 Consistent with this view, self-efficacy has been found to be negatively associated with depressive symptoms.21,22 Moreover, numerous longitudinal studies and substantial experimental evidence have shown that depressive symptoms are closely linked to cognitive decline.23–25 A previous cross-sectional study also reported a significant interaction among self-efficacy, depressive symptoms, and cognitive function in older adults.26 However, few studies have examined whether depressive symptoms may moderate the association between self-efficacy and cognitive impairment.
Based on the existing literature, we constructed a moderated mediation model to examine the relationships among sleep quality, self-efficacy, depressive symptoms, and cognitive function (Figure 1). Specifically, we proposed the following hypotheses:
Hypothesis 1. Self-efficacy is expected to mediate the relationship between sleep quality and cognitive function. Hypothesis 2 posits that the association between self-efficacy and cognitive function is moderated by depressive symptoms. Hypothesis 3. Depressive symptoms moderate the mediating effect of self-efficacy in the relationship between sleep quality and cognitive function.
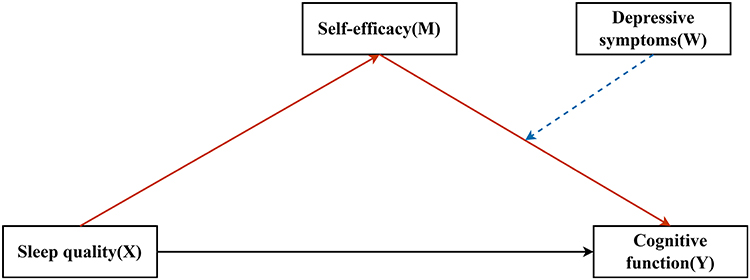 |
Figure 1 Proposed moderated mediation model. Self-efficacy M was hypothesized to mediate the association between sleep quality X and cognitive function Y, while depressive symptoms W were hypothesized to moderate the association between self-efficacy and cognitive function. The black solid line indicates the direct path, the red solid lines indicate the mediation paths, and the blue dashed line indicates the moderating effect. |
Methods
Study Participants
To ensure accessibility and feasibility,27 this study utilized convenience cluster sampling in three representative aging population regions of the Ningxia Hui Autonomous Region: Litong, Xingqing, and Dawukou. However, because the nonrandom sampling, the sample may not be fully representative of the general older adult population, and selection bias cannot be ruled out.28,29 The inclusion criteria were: 1) permanent residency in Ningxia, 2) age 60 years or older, and 3) consent to participate. The exclusion criteria were: 1) with visual or hearing impairment that prevented effective communication during the interview; and 2) with serious medical conditions that substantially limited participation in the survey or completion of the assessment. A total of 2,681 older adults were initially recruited. After excluding 148 participants without demographic information, 283 with missing data on sleep quality, 167 with missing data on cognitive function, and 53 with missing data on depressive symptoms, 2,030 participants were included in the final analysis (Figure 2).
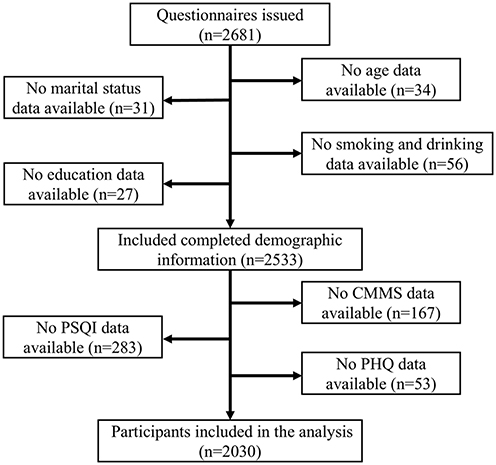 |
Figure 2 Sample selection flowchart. |
The study was approved by the Institutional Review Board of Ningxia Medical University (Approval No. 2018115). It was conducted in accordance with the 1964 Helsinki Declaration and its later amendments, or comparable ethical standards. All participants provided written informed consent before the survey.
Transparency and Openness
All relevant data are included in the paper. The SPSS code used for analysis can be provided upon request. The study design, hypotheses, and analysis plan were not pre-registered.
Cognitive Function
Cognitive function was assessed using the Chinese Mini-Mental Status (CMMS), which is widely used to identify cognitive deficits in Chinese populations.30 The assessment was conducted through face-to-face interviews, and all questions were answered directly by the participants. The CMMS includes 24 items covering orientation, registration, attention, memory, language, and visual construction skills. Total scores range from 0 to 30, with higher scores indicating better cognitive function. Cognitive impairment was identified using education-specific CMMS cut-off points: ≤17 for participants with no formal education, ≤20 for those with primary school education (≥6 years), and ≤24 for those with junior high school education or higher (≥9 years).31 Education-specific cut-off points were used because cognitive screening scores are influenced by educational attainment, especially among older Chinese adults with limited formal education. This approach has been supported in previous studies of Chinese older populations.30–32
Sleep Quality
The Pittsburgh Sleep Quality Index (PSQI) was used to assess sleep quality. It includes 19 items covering seven components: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction.33 Each component is scored from 0 to 3, with a total score ranging from 0 to 21; higher scores indicate poorer sleep quality.34 The PSQI has been widely used and validated in Chinese older adults.
Self-Efficacy
Self-efficacy was assessed using the General Self-Efficacy (GSE) Scale.35 The GSE consists of 10 items rated on a 4-point scale from 1 (“not at all true”) to 4 (“exactly true”), with total scores ranging from 10 to 40; higher scores indicate greater self-efficacy.36 The GSE has been widely used in Chinese populations and showed good reliability in the present study (Cronbach’s α = 0.94).
Depressive Symptoms
Depressive symptoms were assessed using the 9-item Patient Health Questionnaire (PHQ-9).37 Participants rated how often they had experienced depressive symptoms during the previous two weeks on a 4-point scale from 0 (“not at all”) to 3 (“every day”), yielding a total score ranging from 0 to 27; higher scores indicate greater depressive symptoms.38 The PHQ-9 has shown good reliability and validity in older Chinese adults, and the Cronbach’s α in the present study was 0.88.39
Covariates
In the analysis, participants’ sociodemographic characteristics, health-related behaviors, and chronic diseases that may be associated with sleep quality, depressive symptoms, self-efficacy, and cognitive function in older adults were included as covariates. Sociodemographic variables included age (calculated based on the participants’ reported date of birth and the date of data collection, and entered into the models as a continuous variable), gender (male or female), residence (urban or rural), education level (categorized as under primary school, primary school, junior high school, senior high school, and above), and marital status (married or unmarried, with the latter including divorced, widowed, or never married). Health-related behaviors included smoking, drinking, living alone (yes or no), and moderate-intensity exercise. Smoking status was determined by whether participants had ever smoked 100 cigarettes (yes or no). Drinking frequency was categorized as never, once a month, 2–4 times a month, 2–3 times a week, and more than 4 times a week. Moderate-intensity exercise was assessed by asking participants whether they engaged in such activities weekly. For chronic diseases, participants were asked whether they had ever been formally diagnosed with hypertension, diabetes, or coronary heart disease by a registered physician at a hospital above the county level, and were categorized according to their responses (yes or no).
Statistical Analysis
Data analysis was conducted using the Statistical Package for the Social Sciences (SPSS) version 26.0 (SPSS Inc., Chicago, Illinois) and R (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org/). Continuous variables are presented as means and standard deviations (SDs), whereas categorical variables are presented as percentages. The chi-square test and independent-samples t-test were used to examine differences across covariates. Correlation analyses were conducted to examine the relationships among cognitive function, sleep quality, self-efficacy, and depressive symptoms.
The mediation and moderated mediation models were analyzed using the PROCESS macro developed by Hayes.40 First, Model 4 was used to examine whether self-efficacy showed an indirect effect in the association between sleep quality and cognitive function. Next, Model 14 was used to test whether depressive symptoms moderated the second stage of this indirect pathway, namely the association between self-efficacy and cognitive function.41 Bias-corrected percentile bootstrap confidence intervals were estimated based on 5,000 resamples.
Simple slope analysis was conducted to further probe the interaction between self-efficacy and depressive symptoms in predicting cognitive function. Covariates included age, gender, marital status, education level, residence, smoking status, drinking status, living alone, exercise, hypertension, diabetes, and coronary heart disease. A two-sided p-value < 0.05 was considered statistically significant.
Results
Characteristics of the Participants
Among the 2,030 participants (922 men and 1,108 women), 310 (15.3%) individuals were found to have cognitive impairment; females have a higher prevalence (21.1%) than males (8.2%). As shown in Table 1, those with cognitive impairment were generally older, more likely to be female, had lower education levels, engaged in less physical activity, lived in rural areas, and had a higher prevalence of coronary heart disease.
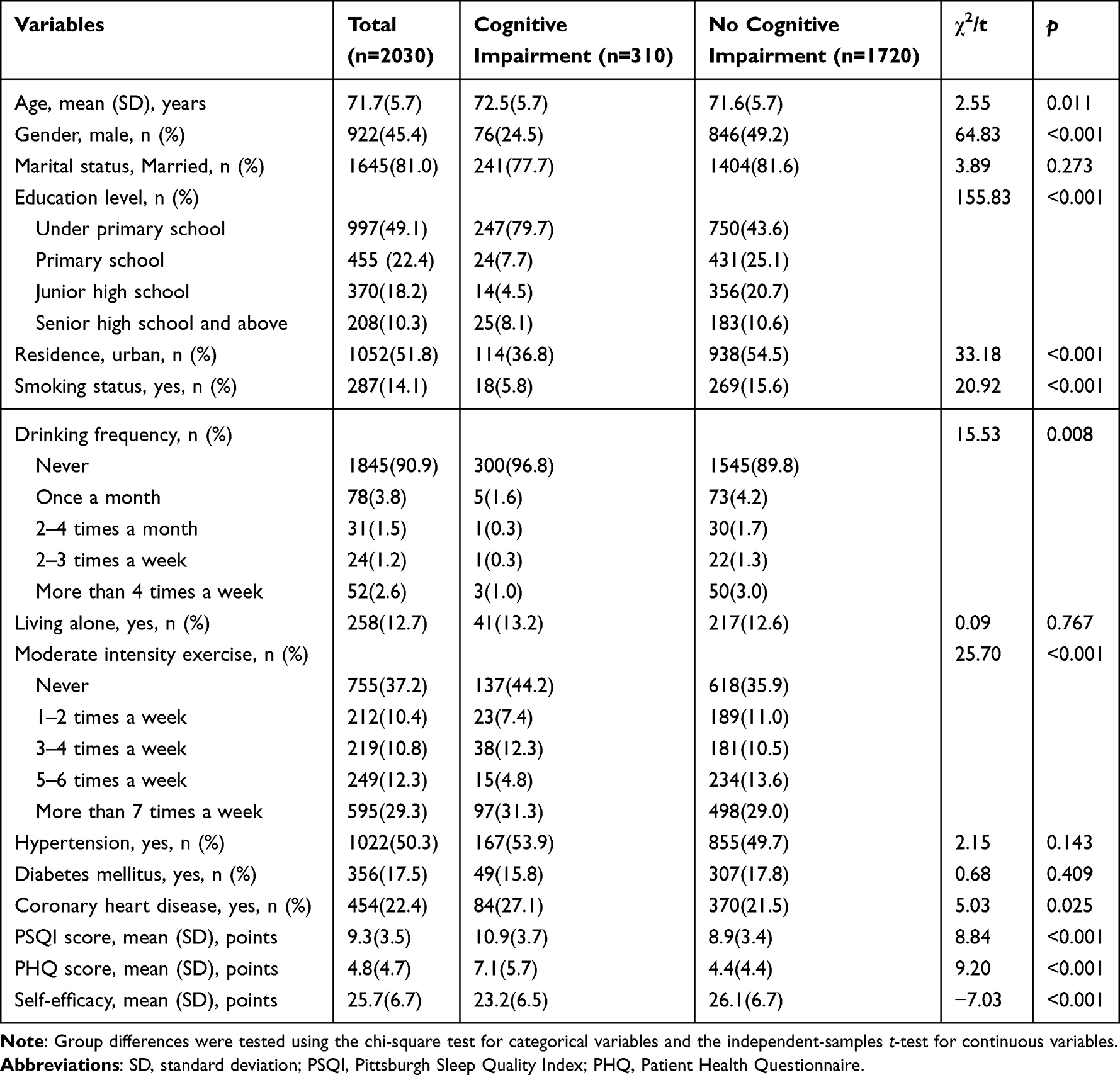 |
Table 1 Characteristics of Study Participants Stratified by Cognitive Status |
Correlations Among Sleep Quality, Self-Efficacy, Depressive Symptoms, and Cognitive Function
Bivariate Pearson correlations among the main variables are presented in Table 2. Higher PSQI scores were correlated with lower self-efficacy (r = −0.219, p < 0.001) and lower cognitive function (r = −0.299, p < 0.001), and with higher depressive symptoms (r = 0.497, p < 0.001). Self-efficacy was correlated with lower depressive symptoms (r = −0.296, p < 0.001) and higher cognitive function (r = 0.274, p < 0.001). Depressive symptoms were correlated with lower cognitive function (r = −0.267, p < 0.001). These findings supported examination of the proposed moderated mediation model.
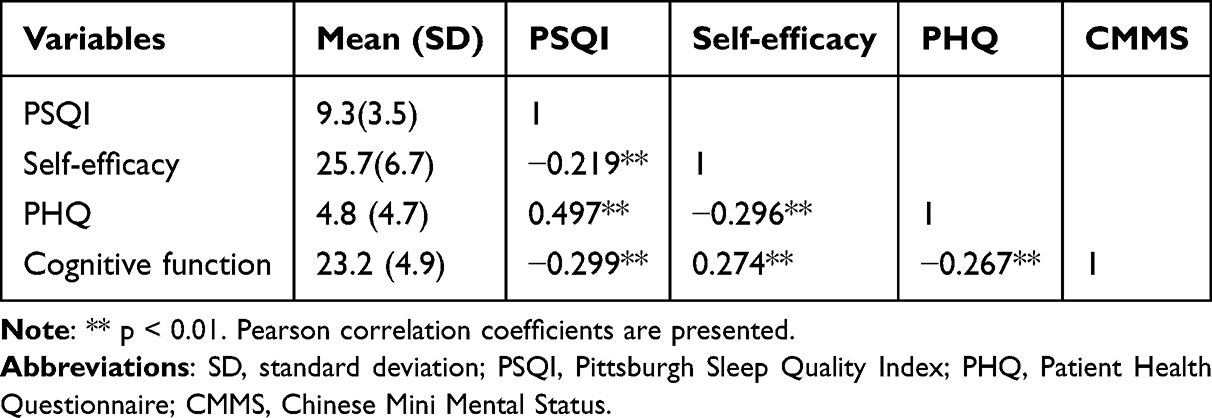 |
Table 2 Correlations for the Main Variables |
Indirect Effect of Self-Efficacy in the Association Between Sleep Quality and Cognitive Function
As shown in Table 3, poorer sleep quality was significantly associated with lower cognitive function (B = −0.230, 95% CI: −0.281 to −0.179), and a significant indirect effect through self-efficacy was observed (B = −0.034, 95% CI: −0.048 to −0.022), accounting for 12.88% of the total effect. These findings suggest that self-efficacy may be involved in the association between sleep quality and cognitive function.
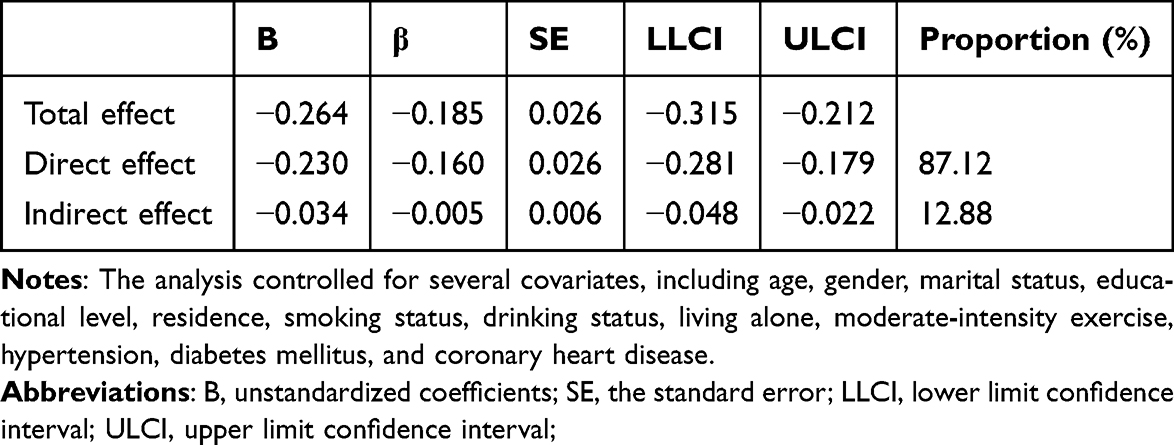 |
Table 3 Testing the Mediating Effect of Sleep Quality on Cognitive Function |
Moderated Mediation Effects of Sleep Quality on Cognitive Function
Model 14 of the PROCESS macro was used to examine the proposed moderated mediation model with relevant covariates controlled. In this model, depressive symptoms were specified as a moderator of the second stage of the indirect pathway, namely the association between self-efficacy and cognitive function. As shown in Table 4 and Figure 3, sleep quality was significantly associated with both self-efficacy (B = −0.328, p < 0.001) and cognitive function (B = −0.182, p < 0.001). Self-efficacy was also significantly associated with cognitive function (B = 0.048, p < 0.05), and this association was significantly moderated by depressive symptoms (B = 0.009, p < 0.01).
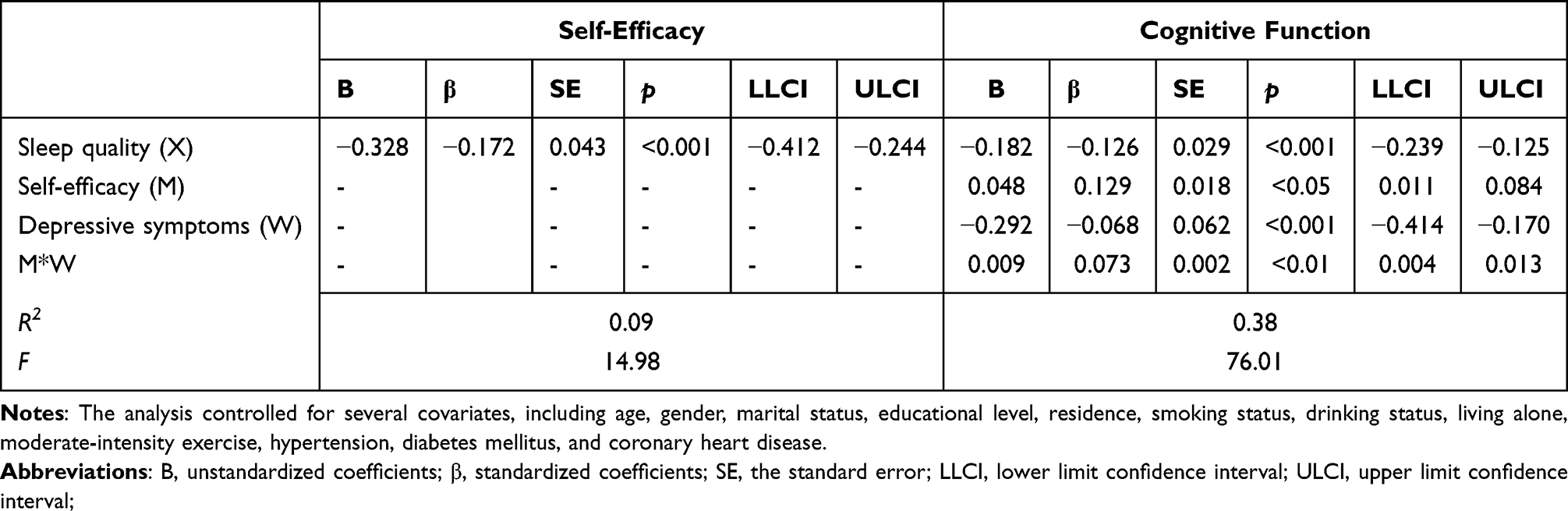 |
Table 4 Testing the Moderated Mediating Effect of Depressive Symptoms on Cognitive Function by Sleep Quality and Self-Efficacy |
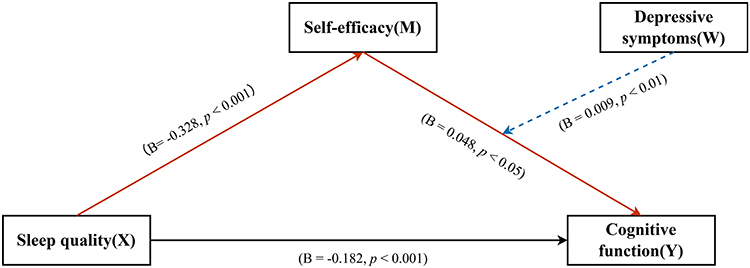 |
Figure 3 Moderated mediation model The values shown in the figure are unstandardized regression coefficients (B) derived from the moderated mediation model after adjustment for covariates. The black solid line indicates the direct path, the red solid lines indicate the mediation paths, and the blue dashed line indicates the moderating effect. |
As shown in Table 5, the conditional indirect association between sleep quality and cognitive function through self-efficacy varied across levels of depressive symptoms. Specifically, the conditional indirect effect was weaker at lower levels of depressive symptoms (B = −0.016, 95% CI: −0.028 to −0.004) and stronger at higher levels (B = −0.042, 95% CI: −0.064 to −0.025). Figure 4 presents the simple slopes for the interaction between self-efficacy and depressive symptoms in predicting cognitive function.
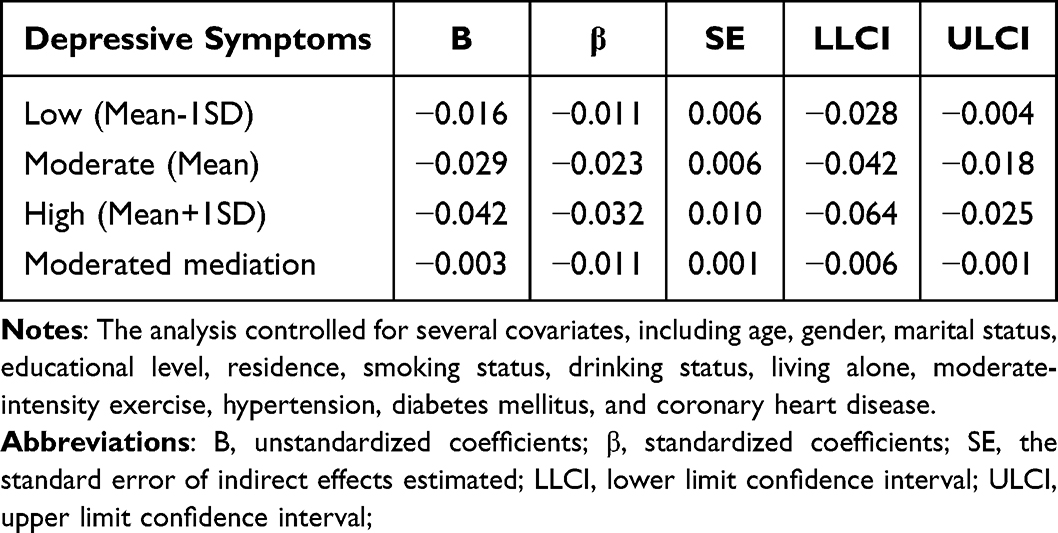 |
Table 5 Conditional Indirect Effects of Self-Efficacy on Cognitive Function by Depressive Symptoms and Moderated Mediation |
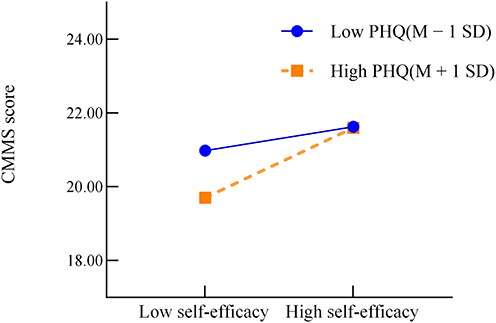 |
Figure 4 Simple Slopes of Depressive Symptoms.The blue solid line represents low depressive symptoms (Mean − 1 SD), and the Orange dashed line represents high depressive symptoms (Mean + 1 SD). |
Discussion
The present study suggests that self-efficacy may be involved in the association between sleep quality and cognitive function, and that depressive symptoms may be related to variation in this association. These findings highlight the potential relevance of psychological and sleep-related factors to cognitive health in older adults.
Previous studies have separately reported associations among sleep quality, self-efficacy, depressive symptoms, and cognitive function.42–45 However, relatively few studies, especially in Chinese older adults, have examined these factors simultaneously within a single analytical framework. Against this background, the present study provides a more integrated perspective by examining sleep quality, self-efficacy, depressive symptoms, and cognitive function within one moderated mediation framework. The findings were broadly consistent with our first hypothesis and suggest that self-efficacy may be a psychological factor contributing to the association between sleep quality and cognitive impairment. This interpretation is in line with previous research suggesting that self-efficacy may be relevant to cognitive health in older adults.46 Several mechanisms may help explain these observed associations. For example, poorer sleep quality may be associated with reduced physical performance and limited social support, which, in turn, may be related to lower self-efficacy.47,48 Self-efficacy may also be associated with cognitive function through differences in coping responses and behavioral choices.49 Common stressors may be related to sleep quality, self-efficacy, and cognitive function, and may partly contribute to the observed associations among these factors.
The findings were broadly consistent with our second and third hypotheses, suggesting that poorer sleep quality was associated with poorer cognitive function, with self-efficacy potentially involved in this association, and that the association between self-efficacy and cognitive function varied according to the level of depressive symptoms.50 However, the observed indirect and moderated effects were relatively modest, and their practical or clinical relevance should therefore be interpreted with caution. Previous research has also reported interactions involving self-efficacy and depressive symptoms.26 Our findings further suggest that social and psychological factors may be relevant considerations in future research on cognitive health in older adults. The conceptual contribution of the present study lies in linking these variables within a single conditional process model in a sample of Chinese older adults, thereby extending the current literature beyond conventional bivariate or simple mediation approaches.
Depressive symptoms may be related to variation in the indirect association between sleep quality and cognitive function through self-efficacy. Several mechanisms may help explain this observed pattern. Given the relatively small effect sizes, these findings may have limited immediate clinical applicability, although they still provide useful directions for future research. Previous studies suggest that depressive symptoms may be associated with dementia-related pathology, including vascular damage, activation of the stress hormone pathway, reductions in brain-derived neurotrophic factor and serotonin levels,51 and the decreased amygdala functional connectivity.52 Depressive symptoms in older adults have been associated with poorer cognitive outcomes, and social activities may be relevant to this relationship. Social interactions may be important for mental health and cognitive function in aging populations and may help buffer the association between depressive symptoms and poorer well-being.53 Better mental health may be associated with more favorable cognitive outcomes in older adults. These findings may have implications for future intervention development, suggesting that both psychological and physical factors could be considered when designing strategies to support cognitive health in older adults.
Limitations
This study contributes to understanding the associations among sleep quality, self-efficacy, depressive symptoms, and cognitive function through a moderated mediation framework, which may inform future research. However, several limitations should be acknowledged. First, because this study used a cross-sectional design, causal inferences cannot be made and the temporal direction of the observed associations cannot be determined. Bidirectional relationships among sleep quality, self-efficacy, depressive symptoms, and cognitive function are possible. Second, all key variables were assessed using self-reported measures, which may be subject to recall bias and common method variance. Third, although multiple covariates were controlled for, residual confounding from unmeasured factors cannot be ruled out. Finally, because the sample was drawn from a specific population in Ningxia using convenience cluster sampling, the generalizability of the findings to other older adult populations may be limited.
Conclusion
Poor sleep quality was associated with poorer cognitive function in older adults, and self-efficacy may be involved in this association. Depressive symptoms may strengthen the indirect association between sleep quality and cognitive function through self-efficacy. These findings suggest that sleep quality, self-efficacy, and depressive symptoms may be relevant factors to consider in future research and intervention development aimed at promoting cognitive health in older adults. However, because the present study was cross-sectional and observational, the causal relationships remain unclear.
Abbreviations
CMMS, Chinese Mini Mental Status; PSQI, Pittsburgh Sleep Quality Index; GSE, General Self-Efficacy; PHQ, Patient Health Questionnaire.
Data Sharing Statement
The data reported in this paper is available from the corresponding author upon reasonable request ([email protected]).
Ethics Approval and Consent to Participate
The research procedures of this study were approved by the Institutional Review Board of the Ningxia Medical University (Nos. 2018115) and accordance with the 1964 Helsinki Declaration and the later amendments or similar ethical standards. All participants signed a written informed consent form before the survey.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Scientific Research Funding Project of Ningxia Medical University (grant number XT2022014), and the Natural Science Foundation of Ningxia Province (grant number 2025AAC030727).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Organization WH. Risk reduction of cognitive decline and dementia: WHO guidelines. 2019. Report No.: 978-92-4-155054-3.
2. Lancet T. Ageing in China: a ticking bomb. Lancet. 2016;388(10056):2058. doi:10.1016/S0140-6736(16)32058-X
3. Jia L, Quan M, Fu Y, et al. Dementia in China: epidemiology, clinical management, and research advances. Lancet Neurol. 2020;19(1):81–12. doi:10.1016/S1474-4422(19)30290-X
4. Jia L, Du Y, Chu L, et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health. 2020;5(12):e661–e71. doi:10.1016/S2468-2667(20)30185-7
5. Arvanitakis Z, Shah RC, Bennett DA. Diagnosis and management of dementia: review. JAMA. 2019;322(16):1589–1599. doi:10.1001/jama.2019.4782
6. Ma XQ, Jiang CQ, Xu L, et al. Sleep quality and cognitive impairment in older Chinese: guangzhou Biobank Cohort Study. Age Ageing. 2019;49(1):119–124. doi:10.1093/ageing/afz120
7. Salinas-Rodríguez A, Manrique-Espinoza B, Moreno-Tamayo K, Guerrero-Zúñiga S. Trajectories of sleep duration and quality and their association with mild cognitive impairment, frailty, and all-cause mortality. Sleep Health. 2024;10(2):240–248. doi:10.1016/j.sleh.2023.12.002
8. Abdelbasset WK, Osailan A. Sleep quality and ventilatory efficiency in elderly heart failure patients: a pilot study on the short-term effect of 4-week low-intensity aerobic exercise. Kardiologiia. 2020;60(6):938. doi:10.18087/cardio.2020.6.n938
9. Kong J, Zhou L, Li X, Ren Q. Sleep disorders affect cognitive function in adults: an overview of systematic reviews and meta-analyses. Sleep Biol Rhythms. 2023;21(2):133–142. doi:10.1007/s41105-022-00439-9
10. Niu J, Han H, Wang Y, Wang L, Gao X, Liao S. Sleep quality and cognitive decline in a community of older adults in Daqing City, China. Sleep Med. 2016;17:69–74. doi:10.1016/j.sleep.2015.07.033
11. Liao H, Liao S, Gao YJ, Mu JP, Wang X, Chen DS. Correlation between sleep time, sleep quality, and emotional and cognitive function in the elderly. Biomed Res Int. 2022;2022:9709536.
12. Hu Q, Song Y, Wang S, Lin L, Ke Y, Zhang P. Association of subjective cognitive complaints with poor sleep quality: a cross-sectional study among Chinese elderly. Int J Geriatr Psychiatry. 2023;38(6):e5956.
13. Yu J, Mahendran R, Rawtaer I, Kua EH, Feng L. Poor sleep quality is observed in mild cognitive impairment and is largely unrelated to depression and anxiety. Aging Mental Health. 2017;21(8):823–828. doi:10.1080/13607863.2016.1161007
14. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
15. Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. 2001;52:1–26. doi:10.1146/annurev.psych.52.1.1
16. Ghose SM, Dzierzewski JM, Dautovich ND. Sleep and self-efficacy: the role of domain specificity in predicting sleep health. Sleep Health. 2023;9(2):190–195. doi:10.1016/j.sleh.2022.09.008
17. Przepiórka A, Błachnio A, Siu NY. The relationships between self-efficacy, self-control, chronotype, procrastination and sleep problems in young adults. Chronobiol Int. 2019;36(8):1025–1035. doi:10.1080/07420528.2019.1607370
18. Paunonen SV, Hong RY. Self-efficacy and the prediction of domain-specific cognitive abilities. J Pers. 2010;78(1):339–360. doi:10.1111/j.1467-6494.2009.00618.x
19. Su H, Zhou Y, Sun Y, Cai Y. The relationship between depression and subjective cognitive decline in older adults of China: the mediating role of general self-efficacy. Psychol Health Med. 2023;28(4):1057–1067. doi:10.1080/13548506.2022.2125165
20. Blazer DG. Self-efficacy and depression in late life: a primary prevention proposal. Aging Mental Health. 2002;6(4):315–324. doi:10.1080/1360786021000006938
21. Cheng ST, Leung CMC, Chan KL, et al. The relationship of self-efficacy to catastrophizing and depressive symptoms in community-dwelling older adults with chronic pain: a moderated mediation model. PLoS One. 2018;13(9):e0203964. doi:10.1371/journal.pone.0203964
22. Robinson-Smith G, Johnston MV, Allen J. Self-care self-efficacy, quality of life, and depression after stroke. Arch Phys Med Rehabil. 2000;81(4):460–464. doi:10.1053/mr.2000.3863
23. Brenowitz WD, Zeki Al Hazzouri A, Vittinghoff E, Golden SH, Fitzpatrick AL, Yaffe K. Depressive symptoms imputed across the life course are associated with cognitive impairment and cognitive decline. J Alzheimers Dis. 2021;83(3):1379–1389. doi:10.3233/JAD-210588
24. Chan CK, Soldan A, Pettigrew C, et al. Depressive symptoms in relation to clinical symptom onset of mild cognitive impairment. Int Psychogeriatr. 2019;31(4):561–569. doi:10.1017/S1041610218001138
25. Sumiyoshi T, Hoshino T, Mishiro I, et al. Prediction of residual cognitive disturbances by early response of depressive symptoms to antidepressant treatments in patients with major depressive disorder. J Affect Disord. 2022;296:95–102. doi:10.1016/j.jad.2021.09.025
26. O’Shea DM, Dotson VM, Fieo RA, Tsapanou A, Zahodne L, Stern Y. Older adults with poor self-rated memory have less depressive symptoms and better memory performance when perceived self-efficacy is high. Int J Geriatr Psychiatry. 2016;31(7):783–790. doi:10.1002/gps.4392
27. Martínez-Mesa J, González-Chica DA, Duquia RP, Bonamigo RR, Bastos JL. Sampling: how to select participants in my research study? An Bras Dermatol. 2016;91(3):326–330. doi:10.1590/abd1806-4841.20165254
28. Tyrer S, Heyman B. Sampling in epidemiological research: issues, hazards and pitfalls. BJPsych Bull. 2016;40(2):57–60. doi:10.1192/pb.bp.114.050203
29. Andrade C. The inconvenient truth about convenience and purposive samples. Indian J Psychol Med. 2021;43(1):86–88. doi:10.1177/0253717620977000
30. Katzman R, Zhang MY, Ouang Ya Q, et al. A Chinese version of the mini-mental state examination; impact of illiteracy in a shanghai dementia survey. J Clin Epidemiol. 1988;41(10):971–978. doi:10.1016/0895-4356(88)90034-0
31. Cui GH, Yao YH, Xu RF, et al. Cognitive impairment using education-based cutoff points for CMMSE scores in elderly Chinese people of agricultural and rural Shanghai China. Acta Neurol Scand. 2011;124(6):361–367. doi:10.1111/j.1600-0404.2010.01484.x
32. Li H, Jia J, Yang Z. Mini-mental state examination in elderly chinese: a population-based normative study. J Alzheimers Dis. 2016;53(2):487–496. doi:10.3233/JAD-160119
33. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
34. Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, Colantonio A. The pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. 2016;25:52–73. doi:10.1016/j.smrv.2015.01.009
35. Schwarzer R, Jerusalem M. Measures in health psychology: a user’s portfolio. causal and control beliefs. Causal and Control Beliefs. 1995;1:35–37.
36. Schwarzer R, Bäßler J, Kwiatek P, Schroder K, Zhang J. The assessment of optimistic self-beliefs: comparison of the german, spanish, and chinese versions of the general self-efficacy scale. Appl. Psychol. 1997;46:69–88.
37. Levis B, Benedetti A, Thombs BD. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:l1476. doi:10.1136/bmj.l1476
38. Bergmans RS, Malecki KM. The association of dietary inflammatory potential with depression and mental well-being among U.S. adults. Prev Med. 2017;99:313–319. doi:10.1016/j.ypmed.2017.03.016
39. Chen S, Chiu H, Xu B, et al. Reliability and validity of the PHQ-9 for screening late-life depression in Chinese primary care. Int J Geriatr Psychiatry. 2010;25(11):1127–1133. doi:10.1002/gps.2442
40. Hayes AF, Preacher KJ. Statistical mediation analysis with a multicategorical independent variable. Br J Math Stat Psychol. 2014;67(3):451–470. doi:10.1111/bmsp.12028
41. Igartua JJ, Hayes AF. Mediation, moderation, and conditional process analysis: concepts, computations, and some common confusions. Span J Psychol. 2021;24:e49. doi:10.1017/SJP.2021.46
42. Byun E, McCurry SM, Opp M, Liu D, Becker KJ, Thompson HJ. Self-efficacy is associated with better sleep quality and sleep efficiency in adults with subarachnoid hemorrhage. J Clin Neurosci. 2020;73:173–178. doi:10.1016/j.jocn.2019.12.010
43. Nielson SA, Kay DB, Dzierzewski JM. Sleep and depression in older adults: a narrative review. Curr Psychiatry Rep. 2023;25(11):643–658. doi:10.1007/s11920-023-01455-3
44. Irwin MR, Vitiello MV. Implications of sleep disturbance and inflammation for Alzheimer’s disease dementia. Lancet Neurol. 2019;18(3):296–306. doi:10.1016/S1474-4422(18)30450-2
45. Rubin-Norowitz M, Lipton RB, Petersen K, Ezzati A. Association of depressive symptoms and cognition in older adults without dementia across different biomarker profiles. J Alzheimers Dis. 2022;88(4):1385–1395. doi:10.3233/JAD-215665
46. Liu S. Study on the Correlation Between Health Promotion Behavior and Self-Efficacy in Elderly People with Mild Cognitive Impairment in the Community. Hubei University of Chinese Medicine.
47. Denison HJ, Jameson KA, Sayer AA, et al. Poor sleep quality and physical performance in older adults. Sleep Health. 2021;7(2):205–211. doi:10.1016/j.sleh.2020.10.002
48. Shen BJ, Tan JJL, Xu Y, Tay HY. Poor sleep quality predicts decline in physical health functioning in patients with coronary heart disease and moderating role of social support. Behav Med. 2022;48(4):294–304. doi:10.1080/08964289.2021.1895050
49. Jongen PJ, Wesnes K, van Geel B, et al. Does self-efficacy affect cognitive performance in persons with clinically isolated syndrome and early relapsing remitting multiple sclerosis? Mult Scler Int. 2015;2015:960282. doi:10.1155/2015/960282
50. Yin J, John A, Cadar D. Bidirectional associations of depressive symptoms and cognitive function over time. JAMA Netw Open. 2024;7(6):e2416305. doi:10.1001/jamanetworkopen.2024.16305
51. Castrén E, Monteggia LM. Brain-derived neurotrophic factor signaling in depression and antidepressant action. Biol Psychiatry. 2021;90(2):128–136. doi:10.1016/j.biopsych.2021.05.008
52. Du Y, Yu J, Liu M, et al. The relationship between depressive symptoms and cognitive function in Alzheimer’s disease: the mediating effect of amygdala functional connectivity and radiomic features. J Affect Disord. 2023;330:101–109. doi:10.1016/j.jad.2023.02.129
53. Zhao S, Wang X, Chen Z, et al. Sex differences in the association between symptom profiles and cognitive functioning in patients with depressive disorder. J Affect Disord. 2021;287:1–7. doi:10.1016/j.jad.2021.03.020
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relationship Between Physical Exercise and Cognitive Impairment Among Older Adults with Type 2 Diabetes: Chain Mediating Roles of Sleep Quality and Depression
Zhang H, Zhang Y, Sheng S, Xing Y, Mou Z, Zhang Y, Shi Z, Yu Z, Gao Q, Cai W, Jing Q
Psychology Research and Behavior Management 2023, 16:817-828
Published Date: 17 March 2023
Neurocognitive Functioning in Patients with Painful Temporomandibular Disorders
Staniszewski K, Ronold EH, Hammar Å, Rosén A
Journal of Pain Research 2023, 16:2015-2025
Published Date: 14 June 2023
The Impact of Problematic Smartphone Use on Sleep Quality Among Chinese Young Adults: Investigating Anxiety and Depression as Mediators in a Three-Wave Longitudinal Study
Wu R, Niu Q, Wang Y, Dawa Y, Guang Z, Song D, Xue B, Lu C, Wang S
Psychology Research and Behavior Management 2024, 17:1775-1786
Published Date: 29 April 2024
The Impact of Anesthetic Management Under Bispectral Index Monitoring on the Early Recovery Quality of Elderly Patients Undergoing Laparoscopic Surgery: A Blinded Randomized Controlled Trial
Shi M, Long Y, Zhou Z, Huang L, Wu D, Zhang X
Clinical Interventions in Aging 2025, 20:597-612
Published Date: 14 May 2025
The Effects of Social Media Addiction, Academic Stress, and Sleep Quality on Anxiety Symptoms: A Cross-Sectional Study of Chinese Vocational Students
Zheng G, Peng H
Psychology Research and Behavior Management 2025, 18:1571-1584
Published Date: 14 July 2025