Back to Journals » Journal of Pain Research » Volume 16
Neurocognitive Functioning in Patients with Painful Temporomandibular Disorders
Authors Staniszewski K, Ronold EH ![]() , Hammar Å, Rosén A
, Hammar Å, Rosén A ![]()
Received 21 April 2023
Accepted for publication 8 June 2023
Published 14 June 2023 Volume 2023:16 Pages 2015—2025
DOI https://doi.org/10.2147/JPR.S414922
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Keith
Kordian Staniszewski,1 Eivind Haga Ronold,2 Åsa Hammar,2,3 Annika Rosén1,4
1Department of Clinical Dentistry, University of Bergen, Bergen, Norway; 2Department of Biological and Medical Psychology, University of Bergen, Bergen, Norway; 3Department of Clinical Sciences Lund, Psychiatry, Faculty of Medicine, Lund University, Lund, Sweden; 4Department of Oral and Maxillofacial Surgery, Haukeland University Hospital, Bergen, Norway
Correspondence: Kordian Staniszewski, Department of Clinical Dentistry, University of Bergen, Årstadveien 19, Bergen, 5009, Norway, Tel +47 47602632, Email [email protected]
Aim: To investigate psychosocial factors in painful TMD (pTMD) which could have consequences for mastering chronic pain.
Methods: Our study included 22 patients (20 women, 2 men) with pTMD, refractory to conservative treatment, and 19 healthy controls. The control group was matched for gender, age, and educational level, and IQ tested on the Wechsler Abbreviated Scale of Intelligence. Neurocognitive function was tested with the Color-Word Interference Test (CWIT). Pain intensity was reported according to the General Pain Intensity Questionnaire (GPI), using the Numeric Rating Scale (NRS). Self-perceived cognitive difficulties were reported by the Perceived Deficits Questionnaire-Depression 5-item (PDQ-5). Two measures of rumination were included: the Rumination-Reflection Questionnaire (RRQ) and the Ruminative Response Scale (RRS). The Montgomery Åsberg Depression Rating Scale Self-report (MADRS-S) was used to measure depressive symptoms, and the Oral Health Impact Profile-TMD (OHIP-TMD) to measure QoL related to oral health.
Results: There were no statistical differences in age (median pTMD: 55 years, median control: 53 years), educational level, and IQ between pTMD and controls. Median pain intensity in pTMD was NRS 8 at maximum and the median pain duration was 18 years. There were no significant differences in CWIT between pTMD and controls. Self-perceived cognitive function (PDQ) was significantly poorer in pTMD. Rumination scores from both measures, and the depression score from MADRS, were significantly higher in pTMD. The OHIP-TMD score revealed a significantly poorer QoL in pTMD.
Conclusion: The group of pTMD patients have self-perceived cognitive difficulties that may make it more difficult to master chronic pain and common everyday tasks. They reported significantly more self-perceived cognitive difficulties, higher rumination, more depressive symptoms, and lower QoL compared to healthy controls, suggesting that these psychosocial factors could be targeted in treatment and interventions. However, the tested neurocognitive performance was equivalent to the control group.
Keywords: cognitive function, chronic pain, self-perceived deficits, depressive symptoms, rumination, quality of life
Introduction
Temporomandibular disorders (TMD) are conditions that can cause pain, discomfort, and functional difficulties in the temporomandibular joint and the muscles involved in chewing.1 TMD have been found to be associated with several other comorbidities, including fibromyalgia, irritable bowel syndrome, and depression, and additionally to trauma and stress symptoms2 In the OPPERA study, it was found that individuals with TMD symptoms were more likely to have higher prevalence of psychosocial factors such as somatic awareness, distress, catastrophizing, pain amplification, and psychosocial stress, when compared to healthy individuals.3–5 Several studies have strongly associated catastrophizing, anxiety, and depression with TMD,6,7 and one study observed a significant correlation between catastrophizing and higher pain intensity in a group of patients with temporomandibular joint disorders and chronic pain.8 Previous research has demonstrated a higher likelihood of TMD in patients with a history of specific mental health and behavioral disorder diagnoses.9 Increased anxiety in the general population due to the COVID-19 pandemic has also been associated with increased incidence of TMD.10
TMD patients make high demands of the healthcare system in terms of resources and finances, due to experienced non-resolving pain, sick leave, and disability.11 Based on the outcome from a review of chronic pain, it has been suggested that the patient’s emotional state may have a significant effect on how pain is experienced, through modulation of neuroendocrine and peripheral factors.12 Despite this link between chronic pain and cognitive processes and their impact, few studies have investigated the relationship between pain and neurocognitive function.
Neurocognitive function is a complex theoretical concept which can be divided into three main domains comprising memory, executive function, and attention. There are several aspects within each domain.13 Executive function (EF) is defined as the neurocognitive processes that regulate behavior, affects, and thoughts.14 One aspect of EF is cognitive inhibition, which can be measured by the Stroop effect,15 and is defined as “The stopping or overriding of a mental process, in whole or in part, with or without intention”.16–18 The Stroop test assesses this effect as the ability to inhibit/stop an automated skill (specifically reading) and is a measure of prepotent response inhibition, which is the ability to deliberately suppress dominant responses. Cognitive functioning, including EF, can also be assessed by self-reported measures, but most studies find small correlations between standardized tests and self-reported measures.19 Both these aspects of cognition contribute to everyday functioning, and therefore both the Stroop task and self-reported cognition EF might be useful when conducting studies of neurocognitive functioning in patients with TMD.
As far as we know, few studies have investigated associations between EF and chronic pain outside more general conditions such as fibromyalgia,20 and only one of these focused on TMD patients.21 This study of 17 female TMD patients and matched controls reported a slower cognitive rate and longer response times for a cognitive inhibition task in the TMD group.21 A meta-analysis suggested that there were small to medium differences between chronic pain patients and neurocognitive inhibition.20 In populations of patients with fibromyalgia, neurocognitive testing has given contraindicatory results, however. More research of cognitive functioning in chronic pain patients is thus needed to investigate the extent to which neurocognitive deficits contribute to functioning, symptoms, and quality of life.
Self-reported complaints have also previously been reported to be associated with the increased severity of chronic pain, including self-perceived cognitive deficits,22 quality of life (QoL) related to oral health,23,24 and rumination.25,26 Rumination is an emotional regulation strategy consisting of repetitive negative thoughts about past events and aspects of oneself, and is associated with anxiety, depression, and neurocognitive deficits.27 Ruminative processes could potentially exacerbate pain,25 and can be separated into reflective depressive and brooding rumination, of which the former is the least pathological.28 Depressive rumination28 is associated with low mood and could mediate the association between pain and depression. Pain could induce a lowered mood, causing depressive rumination. Neurotic rumination is the tendency to ruminate more independently of sad mood,29 which could be important with regard to chronic pain, as it represents a general tendency for maladaptive emotional regulation processes.26 However, little is known about the presence of these emotional regulation strategies in groups with chronic pain. Rumination would be expected to be higher in connection with chronic pain and associated with depressive states, lowered mood, and lower QoL.
The overall aim of the present study was to investigate psychosocial factors in painful TMD (pTMD) that could have consequences for the mastering of chronic pain. The psychosocial factors, including neurocognitive function, self-perceived cognitive difficulties, rumination, depression and QoL, were compared to healthy controls. We hypothesized that: 1) Cognitive inhibition measured by the Stroop test is significantly poorer in patients with pTMD compared to controls; and 2) Self-reported cognitive function and QoL is poorer, and rumination and depression is higher, in pTMD patients compared to controls.
Methods
Study Design
The present study utilized a controlled cross-sectional design to compare patients with pTMD to a healthy control group. The patients in the present study were previously assessed as part of a national interdisciplinary evaluation program for program for pTMD at Haukeland University Hospital (HUH) in Bergen, Norway.30
Study Population
The pTMD patients were referred by their GMP to the National TMD project from all health regions in Norway during the years 2013–2018, for assessment by the interdisciplinary team, and were consecutively included in the study. The patients with pTMD were referred to the National TMD project by GMP from various health regions in Norway between 2013 and 2018. These patients underwent assessment by the interdisciplinary team and were consecutively included in the study. The inclusion criteria were adults older than 18 years with TMD-related pain at least during the last year. The patients included were diagnosed by the interdisciplinary team in accordance with a beta version of the TMD guidelines from the Norwegian National Health Directorate that were later published in 2016,31 which are comparable with the diagnosis included in the Diagnostic Criteria for TMD (DC/TMD).32 Exclusion criteria were non-TMD-related orofacial pain, substance abuse, obvious psychiatric diagnoses, and unresolved economic disability claims. In total, 129 pTMD patients were clinically examined.
During 2021, the pTMD patients were invited by email to participate in the present study. Exclusion criteria for the TMD patients in the present study were the same as for the interdisciplinary investigation, in addition to (color) blindness, poor Norwegian language skills, and IQ< 70. A control group was randomly selected using the Norwegian National Population Register (Folkeregisteret) and invited by email to join the project, and also by recruiting acquaintances of the research group. In total, 150 control subjects were invited via the Norwegian National Population Register. The control group was matched with the pTMD patients in terms of age, gender, and educational level. The control group were adults matched by age and gender with the pTMD patient group. Exclusion criteria for controls were TMD symptoms or other musculoskeletal pain, and symptoms in the head and neck area, (color) blindness, poor Norwegian language skills, and IQ< 70.
Ethics
Ethical approval was granted by the Regional Ethical Review Board Southeast (2015/930) for the first 60 TMD patients, and (2018/647) for an extension to 129 patients, in accordance with the Helsinki Declaration (1964). The present study was a continuation of previous research from the interdisciplinary evaluation program at HUH. Written informed consent was received from all subjects prior to testing, and participating in the study.
Educational Level
The educational level of each subject was registered and categorized in 6 levels: 1) primary school, 2) vocational diploma, 3) high school, 4) bachelor’s degree, 5) master’s degree, 6) PhD or higher.
Assessment of General Cognitive Functioning
To assess whether the subjects’ general intelligence differed, the 2-subtest form of the Wechsler Abbreviated Scale of Intelligence (WASI) was performed for both the TMD patients and the healthy controls. The test consisted of a vocabulary and a matrix reasoning task.33 This was performed in order to evaluate whether differences between the groups in the Color-Word Interference Test (CWIT), and other outcomes, were due to specific deficits in inhibition or differences in general cognitive functioning (IQ).
Neurocognitive Inhibition Test/Stroop Test
The neurocognitive testing of the TMD patients and control subjects was performed at the Neuropsychological Clinic at the Faculty of Psychology, University of Bergen. The test applied was the CWIT from the Delis-Kaplan Executive Functioning Scale, consisting of four subtests to evaluate processing speed, inhibition, and mental flexibility.34 The subtests include S1) naming colors, S2) reading colors, S3) inhibition, and S4) switching. Subtest 3 consists of naming colored words, where there is a mismatch between the name of a color (eg “blue”, “green”, or “red”) and the color it is printed in (eg the word “red” printed in blue ink, instead of red ink). The test subject is asked to name the color of the print, and not the incongruently written word, resulting in an inhibition of the automatic tendency to read (Stroop effect). In subtest 4, the subject alternates between reading color words and naming the color printed in a mismatching ink (S2 and S3 switching). A test score was registered for each subject, based on the time in seconds the subject needed to perform each subtest, and the number of errors for each subtest. Two additional CWIT measurements were calculated; 1) Contrast inhibition = S3-((S1+S2)/2) and 2) Contrast switching = S4-((S1+S2)/2).
Questionnaires
Subjects in the pTMD and control groups were asked to fill in personal information, including age, gender, and educational level. Several validated questionnaires were included in the study for self-administration by the subjects.
A four-item General Pain Intensity Questionnaire (GPI) was used to indicate the subjects’ subjective experience of pain and degree of suffering from pain, according to the Numeric Rating Scale (NRS). The subjects reported their: 1) pain intensity when it is at a minimum, 2) pain intensity when it is at a maximum, 3) how much they suffered from pain, and 4) the highest pain intensity they could accept to live with. A 0–10 NRS was used, where 0 represents no pain at all, and 10 represents the worst imaginable pain.35
Both the Rumination-Reflection Questionnaire (RRQ)29 and the Rumination Response Scale (RRS)28 were included. The RRQ is a 24-item questionnaire based on a 1–5 scale, where 1 represents “strongly disagree” and 5 represents “strongly agree” to statements on the tendency to ruminate or reflect on various aspects of self-related thought. The first 12-point rumination scale (RRQ questions 1–12) consists of questions concerning negative self-referential thought associated with neuroticism (Trapnell & Campbell, 1999). The second 12-point rumination scale (RRQ questions 13–24) measures reflection. The RRS is a 22-item 4-point scale measuring depressive rumination from 1-“almost never” to 4-“almost always” (range 22–88).
The Montgomery Åsberg Depression Rating Scale Self-report (MADRS-S)36 is a 9-item questionnaire measuring depressive symptoms during the past three days. MADRS-S is based on a 7-point scale (0–6) to evaluate the state of depression, where a higher score refers to a higher level of depression symptoms.
For brief assessment of self-perceived cognitive difficulties, the Perceived Deficits Questionnaire-Depression 5-item (PDQ-5)37 was used. The PDQ-5 is a five-item, 5-scale (0–4) questionnaire, where a higher score refers to greater difficulties.
The Oral Health Impact Profile (OHIP) is a reliable and validated measure of QoL related to oral health.38 OHIP is based on a numeric 0–4 scale, where 0 represents “never” and 4 represents “very often”. OHIP-TMD was the version administrated by the subjects in the present study. OHIP-TMD is a 22-item questionnaire that has previously been reported to be an appropriate psychosocial measure of QoL in patients with TMD.39
Statistical Analyses
All statistical analyses were performed in STATA (StataCorp, College Station, TX, USA v.17). Mean, median, range, and standard deviation (SD) were calculated for each variable in both study groups. A p-value of no difference between the pTMD group and the control group was calculated with a Wilcoxon rank-sum test (Mann–Whitney U-test) for all variables, except pain duration due to non-applicable data in the control group.
Results
Study Population
In total, 126 of the 129 pTMD patients from the National pTMD project at HUH received an invitation to participate in the study. 39 out of the 126 pTMD patients signed up to participate in the study. 22 out of 39 pTMD patients completed the tests in the present study. In the control group, 11 out of 19 subjects were tested and included by random selection from the Norwegian National Population Register. The remainder of the control subjects were recruited from among acquaintances and co-workers at the university who were not part of the research group in the present study. The final study group consisted of 20 women and 2 men in the pTMD group, and 17 women and 2 men in the control group. Further details of the study population included are presented in Figure 1.
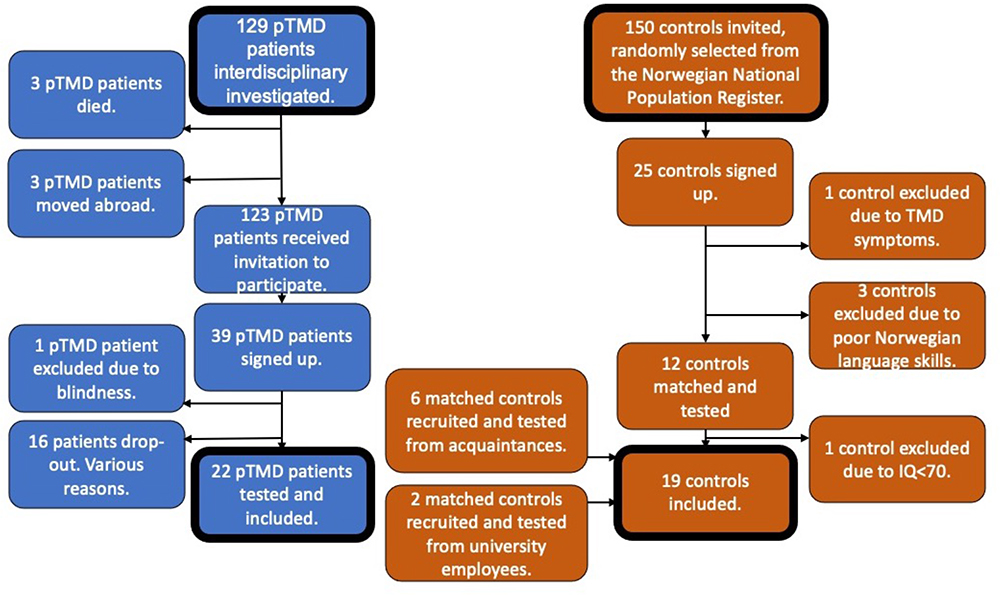 |
Figure 1 Flow chart of pTMD patients and healthy individuals included. Abbreviations: TMD, temporomandibular disorder; pTMD, painful temporomandibular disorder. Note: In total, 22 pTMD patients and 19 controls were tested and included in the study. |
Demographic Data
There were no statistical differences in age, educational level, and IQ between the pTMD group and the control group. Demographic data is presented in Table 1.
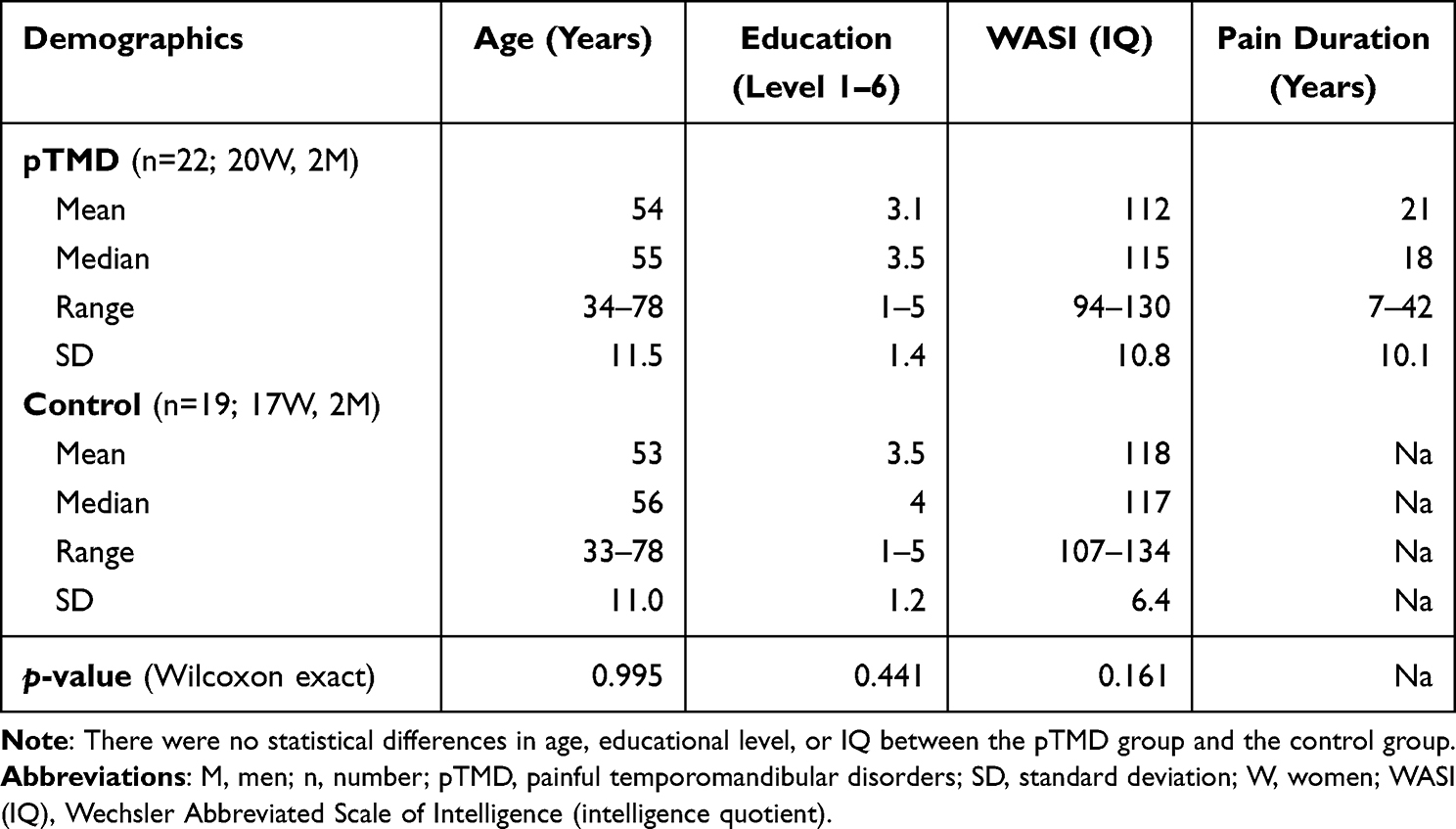 |
Table 1 Demographic Data of pTMD Patients and Controls |
TMD Diagnoses and Pain Intensity
The TMD diagnoses for the full study group of 22 pTMD patients were myalgia (n = 10), arthralgia (n = 2), disc derangement (n = 3), and combinations (n = 7). The median pain duration in the pTMD group was 18 years, range 7–42. The median pain intensity for the pTMD group was NRS 8 at maximum and NRS 3 at minimum. The median suffering from pain was reported to be NRS 5 out of 10. Only one control subject reported pain (not in the head and neck area). The median highest intensity of pain with which the subjects could accept to live was significantly higher for the pTMD group than for the control group. Details of pain intensity are presented in Table 2.
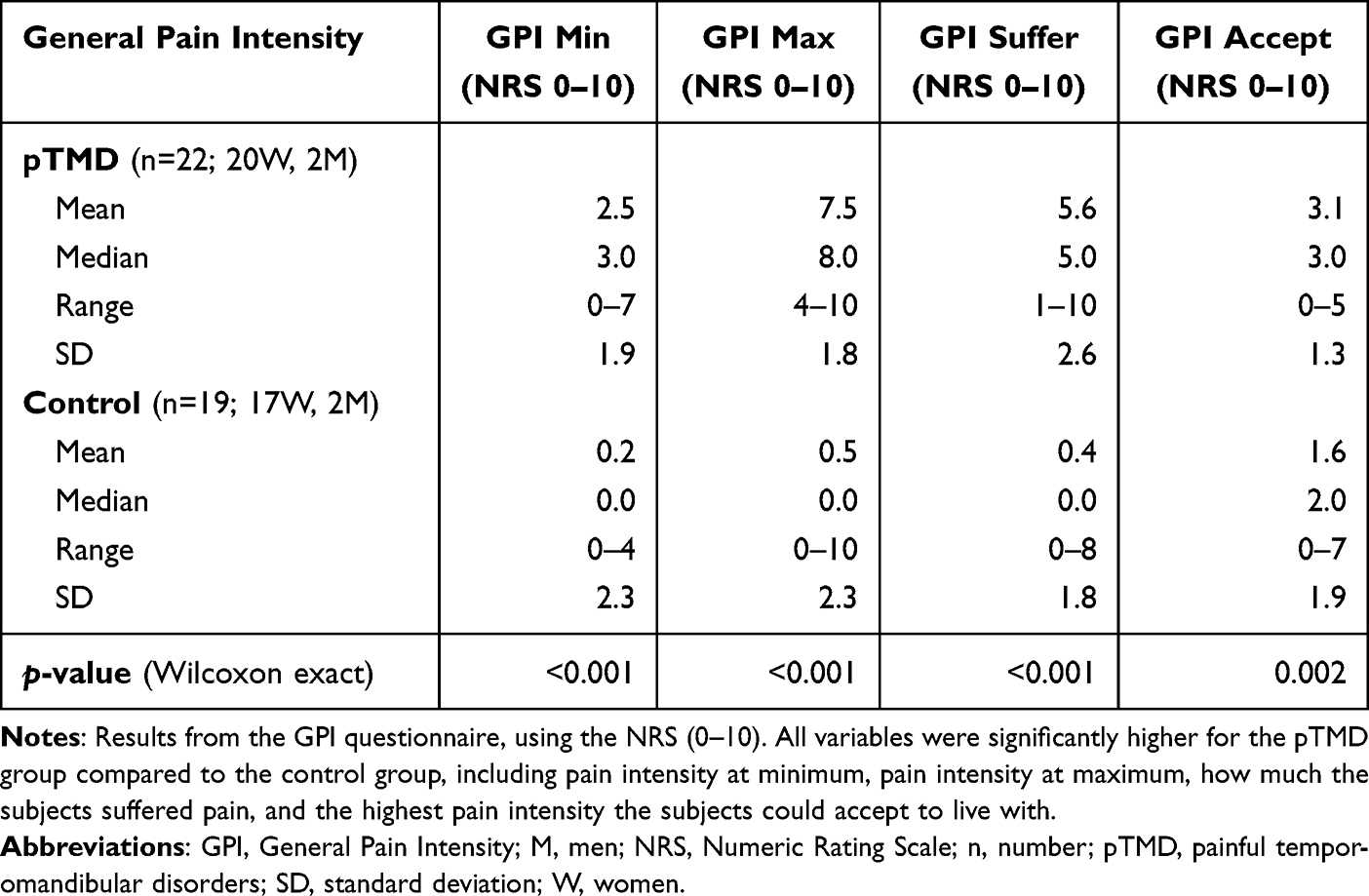 |
Table 2 General Pain Intensity Questionnaire Using the Numeric Rating Scale |
Neurocognitive Inhibition
There were no statistical differences in CWIT performance between the pTMD group and the control group (Table 3).
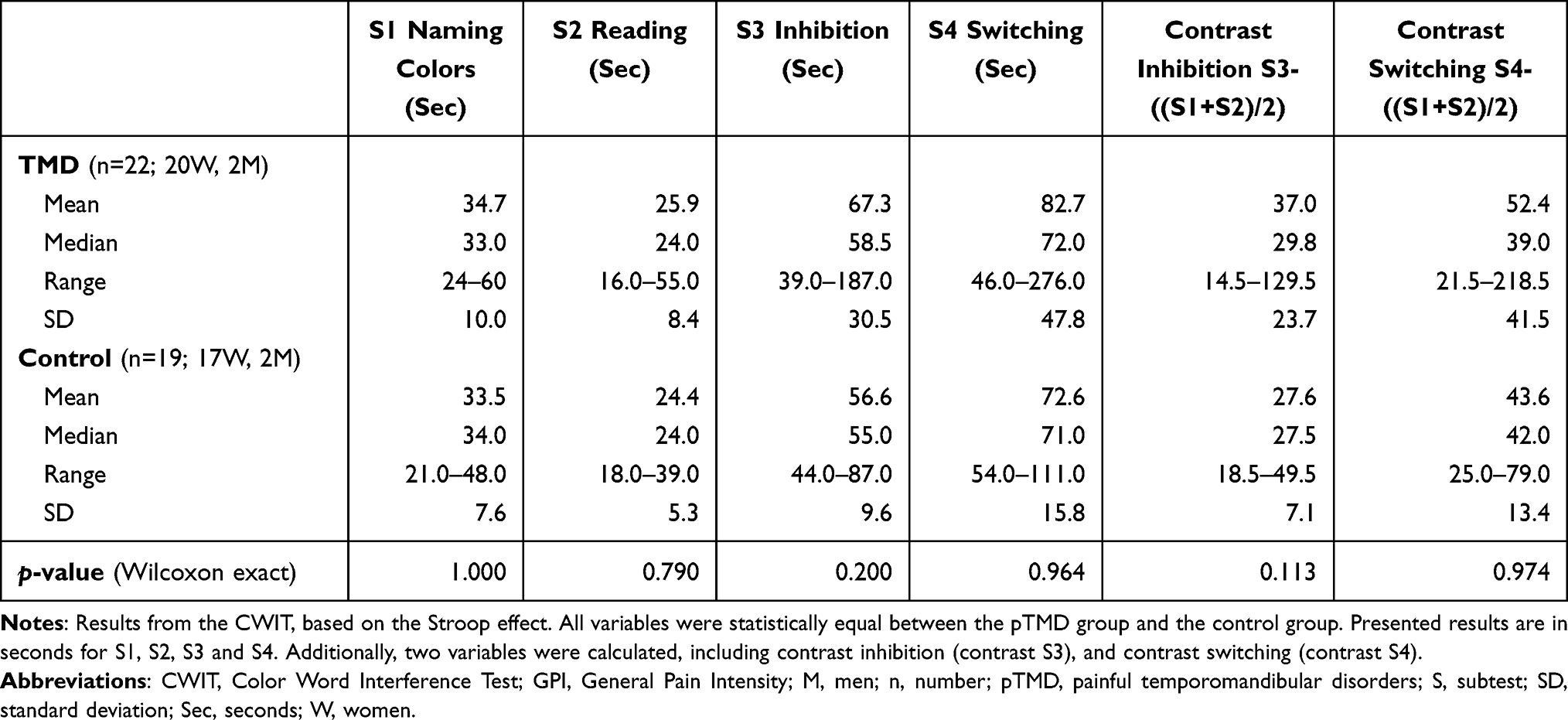 |
Table 3 Neurocognitive Performance Tested with the Color Word Interference Test (CWIT) |
Questionnaires
Rumination scores from RRQ questions 1–12, and the RRS, were significantly higher for the pTMD group. The depression score from MADRS was also significantly higher for the pTMD group. Self-perceived cognitive function, shown by tPDQ, was significantly poorer for the pTMD group. The score from the OHIP-TMD revealed a significantly poorer QoL related to oral health in the pTMD group. There were no differences in reflection scores from the RRQ. Details of results from the questionnaires are presented in Table 4.
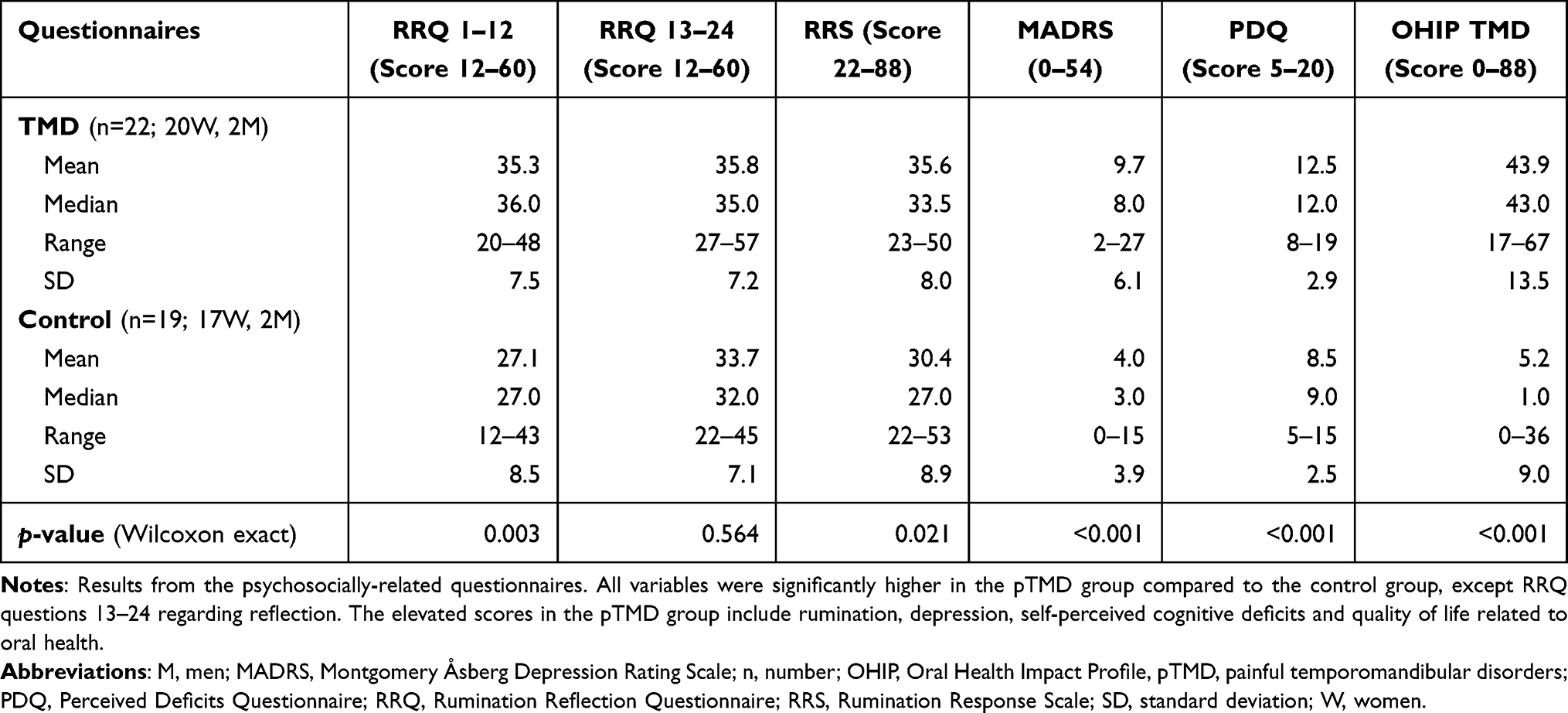 |
Table 4 Results from Psychosocially-Related Questionnaires |
Discussion
In the present study, we observed that pTMD patients reported higher pain intensity, more self-reported cognitive difficulties, depression, low oral-health related quality of life (QoL), and more rumination (not reflection) compared to the control group. However, neurocognitive inhibition measured by a Stroop test did not differ significantly between the pTMD group and the control group.
Hypothesis 1) regarding group differences in neurocognitive inhibition measured by the Stroop test was not supported. The authors of a small, previous study of TMD patients, using similar measures of inhibition, observed a slower response to all Stroop tasks compared to a control group.21 This could suggest a more general deficit in processing speed, rather than a specific deficit in inhibition in TMD patients. However, none of the CWIT conditions measuring processing speed differed in the present study, contrary to this notion. There are few studies of TMD in relation to cognitive inhibition. However, several studies of patients with fibromyalgia and general chronic pain have investigated the relationship between chronic pain and impaired cognitive function. Similar to our results, one study of fibromyalgia patients reported subjective patient complaints, while cognitive inhibition examined by errors on a Stroop task did not differ from a healthy control group.40 In another study, patients with fibromyalgia showed poorer attention, but not inhibition, compared to a control group.41 On the other hand, results from a Stroop test have shown slower cognitive processing in patients with fibromyalgia compared to healthy subjects.42 Better cognitive inhibition shown by Stroop interference score has also been associated with lower pain intensity in healthy subjects.43 Similarly, poorer cognitive inhibition was observed in patients with high-intensity chronic pain, compared to healthy individuals.44 The conclusion from a meta-analytic review was that there were significant deficits in cognitive inhibition in populations with chronic pain, although the risk of bias is high.20 In the present study, the results of no significant difference in cognitive inhibition in pTMD compared to the control group might be due to a small sample size and selection bias, as the recruitment rate to participate in our study was low. Future studies of neurocognitive deficits in EF and inhibition in pTMD should therefore use sensitive measures and be adequately powered to detect small to medium effects.
Hypothesis 2) regarding group differences in self-reported cognitive functioning, depression, QoL, and rumination was supported. The pTMD patients reported significantly poorer cognitive function, higher depression, rumination, and reduced quality of life (QoL) related to oral health, compared to the healthy controls. The fact that neurocognitive inhibition measured by the Stroop task did not differ from the control group indicates that mastering of chronic pain and everyday tasks is more related to self- perceived cognitive deficits, rather than neurocognitive function measured by behavioral/neuropsychological tests. Patients experience more cognitive impairments than they show in task performance. The results are similar to a study of patients with chronic idiopathic pain, where self-perceived cognitive deficits, pain-related disability, and reduced QoL were observed, compared to a healthy control group.22 It thus seems that patients with chronic pain and pain-related disabilities suffer from self-perceived cognitive deficits and depression, even when executive function measured by neurocognitive tests is similar to healthy individuals. There could be several reasons for this, as previously discussed by Friedman and Gustavson.19 Self-reported cognitive functioning is more sensitive to certain deficits than neurocognitive tests, the latter often being administered in highly controlled, stationary environments. Subjectively reported cognitive functioning could thus be more ecologically valid, since it measures how patients actually function in their everyday life.19 This could be particularly relevant for chronic pain patients who might not be disrupted by pain in stationary tasks, such as neuropsychological testing, but might experience increasing difficulties and distress when out and about in their everyday lives. This was supported by a previous study that found an interaction between gait movement and Stroop performance in a population with chronic back pain.45 In conclusion, self-reported cognitive deficits are more apparent in pTMD than objective deficits, they could influence everyday functioning, and interventions reducing such deficits should be developed. In addition, future studies of pTMD should utilize more extensive cognitive self-reported measures to assess which areas of cognitive functioning (eg memory/EF) are most affected.
The group of pTMD patients in the present study reported significantly higher depressive (RRS) and neurotic (RRQ questions 13–24) rumination. Notably, reflection (RRQ questions 13–24) as an adaptive form of rumination did not differ from the control group. Rumination could potentially exacerbate pain,25 disrupt cognitive functioning and predispose individuals for depression, anxiety, and insomnia,27 and contribute to relapse and recurrence of depression.46 Neurotic rumination could influence sensitivity to negative emotion, and has been associated with a more severe course of illness in depression,47 and as likely to contribute to the relatively high levels of depression in the pTMD group. Importantly, the groups did not differ in reflection, supporting the presence of pathological emotional regulation in this group. In sum, the current findings support significantly pronounced dysfunctional emotional regulation strategies in pTMD patients compared to controls, which represents a risk factor for psychiatric disorders. Interventions targeting pathological rumination, such as cognitive behavioral therapy and mindfulness interventions, could be useful to prevent exacerbation of pain and the development of psychiatric disorders, and should be considered for pTMD patients.
Results from the OHIP-TMD questionnaire in the present study revealed that oral health-related QoL was significantly poorer in the pTMD group compared to the control group. Poorer oral health-related QoL has also been related to more severe TMD in a previous study.23 In another study, oral health-related QoL was also significantly lower in TMD patients compared to a control group, and significantly correlated with higher pain intensity in the TMD group.24 Findings indicate that the severity and pain intensity in TMD are correlated with poorer QoL.
The study had several considerable strengths. A well-selected pTMD sample underwent comprehensive cognitive assessment, including neurocognitive tests, emotional regulation, depression and pain, controlled by an IQ measure. To the authors’ knowledge this is one of the most comprehensive assessments of cognitive functioning in chronic pain patients in general and pTMD patients in particular. The groups were matched according to age and gender and did not differ in terms of important demographical variables. In addition, random sampling through recruitment under the Norwegian National Population Register was implemented. The internal validity and comprehensive assessments came at the cost of external validity and statistical power.
The limitation of the present study is, as mentioned, the small sample size, and possibly selection bias. The recruitment rate was low for both the pTMD group and the control group, and it is reasonable to assume that individuals with poor cognitive skills would seek to avoid participating in the study, as they might feel that they did not perform well enough in such tasks. A lack of significant results from neurocognitive tests could be due to a type-II error due to the small sample size.
Altogether, it seems that patients with pTMD might suffer from self-perceived cognitive deficits, rumination, and depressive symptoms, which would probably make it even harder for them to handle their pain and could put them at risk of exacerbation and developing psychiatric disorder It is possible that patients with pTMD could increase their cognitive functioning by completing a cognitive training program to increase QoL. Such interventions have previously shown significant results for the cognitive functioning of patients with a history of depression of depression and residual symptoms,48,49 and significant long-term improvements in self-reported EF.50 In patients with chronic myofascial pain, self-care interventions have been shown to reduce pain intensity, and increase QoL.51 Nowadays, such interventions can be developed through digital platforms, with professional treatment feedback for patients.
Conclusion
Our results show that pTMD patients have self-perceived cognitive difficulties which may make it more difficult to master chronic pain and common everyday tasks. However, the neurocognitive inhibition tested by CWIT did not significantly differ from the control group. Based on our results, the hypothesis of “Neurocognitive inhibition is poorer in pTMD” was rejected, and the hypothesis “Self-perceived cognitive function and QoL is poorer, and rumination and depression are higher in pTMD” was approved, and the latter might put patients at risk of functional and psychological exacerbation. To improve pTMD treatment outcomes, a learning and mastering course in orofacial pain and digital treatment feedback was recently launched at HUH. To further increase the quality of care and the opportunity for patients to take responsibility for their own recovery, cognitive training and psychoeducation via digital platforms are being developed, and future studies should assess how those influence cognitive function and QoL.
Acknowledgments
The authors of the present study want to thank all patients for participating.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Scrivani SJ, Keith DA, Kaban LB. Temporomandibular disorders. N Engl J Med. 2008;359(25):2693–2705. doi:10.1056/NEJMra0802472
2. Hoffmann RG, Kotchen JM, Kotchen TA, Cowley T, Dasgupta M, Cowley AW. Temporomandibular disorders and associated clinical comorbidities. Clin J Pain. 2011;27(3):268–274. doi:10.1097/AJP.0b013e31820215f5
3. Slade GD, Ohrbach R, Greenspan JD, et al. Painful temporomandibular disorder: decade of discovery from OPPERA studies. J Dent Res. 2016;95(10):1084–1092. doi:10.1177/0022034516653743
4. Fillingim RB, Slade GD, Diatchenko L, et al. Summary of findings from the OPPERA baseline case-control study: implications and future directions. J Pain. 2011;12(11 Suppl):T102–7. doi:10.1016/j.jpain.2011.08.009
5. Fillingim RB, Slade GD, Greenspan JD, et al. Long-term changes in biopsychosocial characteristics related to temporomandibular disorder: findings from the OPPERA study. Pain. 2018;159(11):2403–2413. doi:10.1097/j.pain.0000000000001348
6. Staniszewski K, Lygre H, Bifulco E, et al. Temporomandibular disorders related to stress and HPA-axis regulation. Pain Res Manage. 2018;2018:7020751. doi:10.1155/2018/7020751
7. Willassen L, Johansson AA, Kvinnsland S, Staniszewski K, Berge T, Rosén A. Catastrophizing has a better prediction for TMD than other psychometric and experimental pain variables. Pain Res Manage. 2020;2020:1–8. doi:10.1155/2020/7893023
8. Velly AM, Look JO, Carlson C, et al. The effect of catastrophizing and depression on chronic pain--a prospective cohort study of temporomandibular muscle and joint pain disorders. Pain. 2011;152(10):2377–2383. doi:10.1016/j.pain.2011.07.004
9. Salinas Fredricson A, Krüger Weiner C, Adami J, et al. The role of mental health and behavioral disorders in the development of temporomandibular disorder: a SWEREG-TMD nationwide case-control study. J Pain Res. 2022;15:2641–2655. doi:10.2147/JPR.S381333
10. Minervini G, Franco R, Marrapodi MM, et al. The association between COVID-19 related anxiety, stress, depression, temporomandibular disorders, and headaches from childhood to adulthood: a systematic review. Brain Sci. 2023;13(3):481. doi:10.3390/brainsci13030481
11. Salinas Fredricson A, Krüger Weiner C, Adami J, et al. Sick leave and disability pension in a cohort of TMD-patients - The Swedish National Registry Studies for Surgically Treated TMD (SWEREG-TMD). BMC Public Health. 2022;22(1):916. doi:10.1186/s12889-022-13329-z
12. Heir GM. Chronic orofacial pain, cognitive‐emotional‐motivational considerations: a narrative review. J Oral Rehabil. 2019;46(11):1065–1070. doi:10.1111/joor.12848
13. Hammar Å, Ronold EH, Rekkedal GÅ. Cognitive impairment and neurocognitive profiles in major depression-a clinical perspective. Front Psychiatry. 2022;13:764374. doi:10.3389/fpsyt.2022.764374
14. Anderson PJ. Towards a developmental model of executive function. In: Executive Functions and the Frontal Lobes: A Lifespan Perspective. Psychology Press; 2008:21.
15. Stroop JR. Studies of interference in serial verbal reactions. J Exp Psychol. 1935;18(6):643–662. doi:10.1037/h0054651
16. Macleod C. The Concept of Inhibition in Cognition. American Psychological Association; 2007.
17. Friedman NP, Miyake A. The relations among inhibition and interference control functions: a latent-variable analysis. J Exp Psychol Gen. 2004;133(1):101–135. doi:10.1037/0096-3445.133.1.101
18. Friedman NP, Robbins TW. The role of prefrontal cortex in cognitive control and executive function. Neuropsychopharmacology. 2022;47(1):72–89. doi:10.1038/s41386-021-01132-0
19. Friedman NP, Gustavson DE. Do rating and task measures of control abilities assess the same thing? Curr Dir Psychol Sci. 2022;31(3):262–271. doi:10.1177/09637214221091824
20. Berryman C, Stanton TR, Bowering KJ, Tabor A, McFarlane A, Moseley GL. Do people with chronic pain have impaired executive function? A meta-analytical review. Clin Psychol Rev. 2014;34(7):563–579. doi:10.1016/j.cpr.2014.08.003
21. Weissman-Fogel I, Moayedi M, Tenenbaum HC, Goldberg MB, Freeman BV, Davis KD. Abnormal cortical activity in patients with temporomandibular disorder evoked by cognitive and emotional tasks. Pain. 2011;152(2):384–396. doi:10.1016/j.pain.2010.10.046
22. Coppieters I, De Pauw R, Kregel J, et al. Differences between women with traumatic and idiopathic chronic neck pain and women without neck pain: interrelationships among disability, cognitive deficits, and central sensitization. Phys Ther. 2017;97(3):338–353. doi:10.2522/ptj.20160259
23. Yap AU, Zhang MJ, Cao Y, Lei J, Fu KY. Comparison of psychological states and oral health–related quality of life of patients with differing severity of temporomandibular disorders. J Oral Rehabil. 2022;49(2):177–185. doi:10.1111/joor.13216
24. Onoda N, Mikami T, Saito N, Kobayashi T. Evaluation of oral health-related quality of life in patients with temporomandibular disorders. CRANIO®. 2021;1–8. doi:10.1080/08869634.2021.1883378
25. Meints SM, Stout M, Abplanalp S, Hirsh AT. Pain-related rumination, but not magnification or helplessness, mediates race and sex differences in experimental pain. J Pain. 2017;18(3):332–339. doi:10.1016/j.jpain.2016.11.005
26. Miller MM, Meints SM, Hirsh AT. Catastrophizing, pain, and functional outcomes for children with chronic pain: a meta-analytic review. Pain. 2018;159(12):2442–2460. doi:10.1097/j.pain.0000000000001342
27. Watkins ER, Roberts H. Reflecting on rumination: consequences, causes, mechanisms and treatment of rumination. Behav Res Ther. 2020;127:103573. doi:10.1016/j.brat.2020.103573
28. Treynor W, Gonzalez R, Nolen-Hoeksema S. Rumination reconsidered: a psychometric analysis. Cognit Ther Res. 2003;27(3):247–259. doi:10.1023/A:1023910315561
29. Trapnell PD, Campbell JD. Private self-consciousness and the five-factor model of personality: distinguishing rumination from reflection. J Pers Soc Psychol. 1999;76(2):284–304. doi:10.1037/0022-3514.76.2.284
30. Berge T, Schjødt B, Bell RF, et al. Assessment of patients with severe temporomandibular disorder in Norway – a multidisciplinary approach. Den NorskeTannlegeforeningens Tidene. 2016;126:114–121.
31. Helsedirektoratet TNDo H. Nasjonal faglig retningslinje for utredning og behandling av TMD. (National guidelines in diagnostics and treatment of TMD; 2016. Available from: https://www.helsedirektoratet.no/retningslinjer/temporomandibulaer-dysfunksjon-tmd.
32. Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J Oral Facial Pain Headache. 2014;28(1):6–27. doi:10.11607/jop.1151
33. Wechsler D. Wechsler Abbreviated Scale of Intelligence. San Antonio, TX: The Psychological Corporation; 1999.
34. Delis DC, Kramer JH, Kaplan E, Holdnack J. Reliability and validity of the Delis-Kaplan executive function system: an update. J Int Neuropsychol Soc. 2004;10(2):301–303. doi:10.1017/S1355617704102191
35. Lundeberg T, Lund I, Dahlin L, et al. Reliability and responsiveness of three different pain assessments. J Rehabil Med. 2001;33(6):279–283. doi:10.1080/165019701753236473
36. Svanborg P, Åsberg M. A comparison between the Beck Depression Inventory (BDI) and the self-rating version of the Montgomery Åsberg Depression Rating Scale (MADRS). J Affect Disord. 2001;64(2–3):203–216. doi:10.1016/S0165-0327(00)00242-1
37. Sullivan MJ, Edgley K, Dehoux E. A survey of multiple sclerosis: i. Perceived cognitive problems and compensatory strategy use. Can J Rehabil. 1990;4(2):99–105.
38. Sierwald I, John MT, Durham J, Mirzakhanian C, Reissmann DR. Validation of the response format of the Oral Health Impact Profile. Eur J Oral Sci. 2011;119(6):489–496. doi:10.1111/j.1600-0722.2011.00884.x
39. Yule PL, Durham J, Playford H, et al. OHIP-TMDs: a patient-reported outcome measure for temporomandibular disorders. Community Dent Oral Epidemiol. 2015;43(5):461–470. doi:10.1111/cdoe.12171
40. Veldhuijzen DS, Sondaal SFV, Oosterman JM. Intact cognitive inhibition in patients with fibromyalgia but evidence of declined processing speed. J Pain. 2012;13(5):507–515. doi:10.1016/j.jpain.2012.02.011
41. Oosterman JM, Derksen LC, van Wijck AJM, Kessels RPC, Veldhuijzen DS. Executive and attentional functions in chronic pain: does performance decrease with increasing task load? Pain Res Manage. 2012;17:962786. doi:10.1155/2012/962786
42. Martinsen S, Flodin P, Berrebi J, et al. Fibromyalgia patients had normal distraction related pain inhibition but cognitive impairment reflected in caudate nucleus and hippocampus during the Stroop Color Word Test. PLoS One. 2014;9(9):e108637. doi:10.1371/journal.pone.0108637
43. Oosterman JM, Dijkerman HC, Kessels RPC, Scherder EJA. A unique association between cognitive inhibition and pain sensitivity in healthy participants. Eur J Pain. 2010;14(10):1046–1050. doi:10.1016/j.ejpain.2010.04.004
44. Grisart JM, Plaghki LH. Impaired selective attention in chronic pain patients. Eur J Pain. 1999;3(4):325–333. doi:10.1016/S1090-3801(99)90014-9
45. Lamoth CJ, Stins JF, Pont M, Kerckhoff F, Beek PJ. Effects of attention on the control of locomotion in individuals with chronic low back pain. J Neuroeng Rehabil. 2008;5:13. doi:10.1186/1743-0003-5-13
46. Ronold EH, Joormann J, Hammar Å. Facing recovery: emotional bias in working memory, rumination, relapse, and recurrence of major depression; an experimental paradigm conducted five years after first episode of major depression. Appl Neuropsychol Adult. 2020;27(4):299–310. doi:10.1080/23279095.2018.1550406
47. Ronold EH, Schmid MT, Oedegaard KJ, Hammar Å. A longitudinal 5-year follow-up study of cognitive function after first episode major depressive disorder: exploring state, scar and trait effects. Front Psychiatry. 2020;11:575867. doi:10.3389/fpsyt.2020.575867
48. Hammar Å, Semkovska M, Borgen IMH, et al. A pilot study of cognitive remediation in remitted major depressive disorder patients. Appl Neuropsychol Adult. 2022;29(2):172–182. doi:10.1080/23279095.2020.1726919
49. Ronold EH, Joormann J, Hammar Å. Computerized working memory training in remission from major depressive disorder: effects on emotional working memory, processing speed, executive functions, and associations with symptoms. Front Behav Neurosci. 2022;16:887596. doi:10.3389/fnbeh.2022.887596
50. Ronold EH, Myklebost BS, Hammar ÅH. Improvement in self-reported cognitive functioning but not in rumination following online working memory training in a two-year follow-up study of remitted major depressive disorder. Front I Psych. 2023;14:1163073. doi:10.3389/fpsyt.2023.1163073
51. Liu J-Q, Wan Y-D, Xie T, Miao T, Wang J, Xiong X. Associations among orthodontic history, psychological status, and temporomandibular-related quality of life: a cross-sectional study. Int J Clin Pract. 2022;2022:1–7. doi:10.1155/2022/3840882
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hemophilic Arthropathy: Barriers to Early Diagnosis and Management
Cuesta-Barriuso R, Donoso-Úbeda E, Meroño-Gallut J, Ucero-Lozano R, Pérez-Llanes R
Journal of Blood Medicine 2022, 13:589-601
Published Date: 17 October 2022
Depression and Associated Factors Among Diabetic Patients Undergoing Diabetic Retinopathy Assessments at a Tertiary Care Center: A Cross-Sectional Study
Upaphong P, Choovuthayakorn J, Choovuthayakorn J, Phinyo P, Patikulsila D, Nanegrungsunk O, Chaikitmongkol V, Kunavisarut P, Apivatthakakul A, Wongpakaran N, Wongpakaran T
Clinical Ophthalmology 2025, 19:1793-1803
Published Date: 5 June 2025
Threshold Effect of Anxiety in the Comorbidity of Depression and Chronic Pain: A Cross-Sectional Study Based on Pain Sensitivity
Liu Y, Cheng J, Gao H, Chen Y, Chen H, Xia Q, Yan J, Li C, Ju P, Zhu C
Neuropsychiatric Disease and Treatment 2026, 22:580711
Published Date: 17 March 2026
Associations of Sleep Quality with Cognitive Function in Chinese Older Adults: The Roles of Self-Efficacy and Depressive Symptoms
Wang L, Wang Y, Huo J, Luo Y, Ding Y, Wang Z
Clinical Interventions in Aging 2026, 21:594997
Published Date: 20 May 2026
Cognitive Mediation of Biopsychosocial Determinants of Quality of Life in Epilepsy
Chen X, Zhou B, Liu Y, Sun L, Lu Z, Liu L, An S, Xie C, Jiang Y, Zhu C
Psychology Research and Behavior Management 2026, 19:602750
Published Date: 29 June 2026