Back to Journals » Psychology Research and Behavior Management » Volume 17
The Impact of Problematic Smartphone Use on Sleep Quality Among Chinese Young Adults: Investigating Anxiety and Depression as Mediators in a Three-Wave Longitudinal Study
Authors Wu R, Niu Q, Wang Y, Dawa Y, Guang Z, Song D, Xue B, Lu C, Wang S ![]()
Received 22 January 2024
Accepted for publication 18 April 2024
Published 29 April 2024 Volume 2024:17 Pages 1775—1786
DOI https://doi.org/10.2147/PRBM.S455955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gabriela Topa
Ruipeng Wu,1– 3,* Qiong Niu,1,2,* Yingting Wang,1,2 Yundan Dawa,4 Zixuan Guang,1,2 Dongji Song,1 Bei Xue,1 Ciyong Lu,5 Shaokang Wang1,3
1Key Laboratory for Molecular Genetic Mechanisms and Intervention Research on High Altitude Disease of Tibet Autonomous Region, School of Medicine, Xizang Minzu University, Xianyang, 712082, People’s Republic of China; 2Key Laboratory of High Altitude Hypoxia Environment and Life Health, School of Medicine, Xizang Minzu University, Xianyang, 712082, People’s Republic of China; 3Key Laboratory of Environmental Medicine and Engineering of Ministry of Education, Department of Nutrition and Food Hygiene, School of Public Health, Southeast University, Nanjing, 210009, People’s Republic of China; 4Department of Tibetan Medicine, University of Tibetan Medicine(UTC), Lhasa, 850000, People’s Republic of China; 5Department of Medical Statistics and Epidemiology, School of Public Health, Sun Yat-Sen University 510080, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence : Ciyong Lu; Shaokang Wang, Email [email protected]; [email protected]
Background: Sleep disorders are a significant health issue that urgently needs to be addressed among undergraduate students, and one of the potential underlying problems could be problematic smartphone use (PSU). This study aimed to clarify the relationship between PSU and poor sleep quality by investigating the independent and serial mediating roles of anxiety and depressive symptoms in a population of university students in Tibet, China.
Methods: A total of 2993 Tibetan college students completed three waves of data surveys, with all participants completing questionnaires on PSU, anxiety, depressive symptoms, and sleep quality (Time 1 (T1) -Time 3 (T3)). Bootstrapped mediation analysis was used to explore the mediating role of anxiety and depressive symptoms in the longitudinal relationship between PSU and sleep quality.
Results: Both direct and indirect effects of PSU on poor sleep quality were found. PSU (T1) can had not only a direct negative influence on poor sleep quality (T3) among young adults (direct effect = 0.021, 95% CI = 0.010– 0.033) but also an indirect negative impact via three pathways: the independent mediating effect of anxiety symptoms (T2) (indirect effect 1 = 0.003, 95% CI = 0.001– 0.006), the independent mediating effect of depressive symptoms (T2) (indirect effect 2 = 0.004, 95% CI = 0.002– 0.006), and the serial mediating effects of anxiety (T2) and depressive symptoms (T2) (indirect effect 3 = 0.008, 95% CI=0.005– 0.011).
Conclusion: These findings highlight the role of anxiety and depression symptoms as joint mediating factors in the relationship between PSU and sleep disturbances. Interventions focused on improving sleep that incorporate behavioural measures could benefit from treatment approaches targeting mental disorders.
Keywords: sleep quality, problematic smartphone use, anxiety, depressive symptoms, longitudinal study
Introduction
Sleep disorders have become a significant public health issue in society. According to a report by the World Health Organization, one-third of the global population is affected by sleep disturbances. 1–3 Sleep disorders can have short-term effects such as mood disturbances, decreased attention, and somatic symptoms. Long-term sleep issues may be associated with physiological and psychological problems, including cardiovascular diseases, metabolic disorders, and an increased risk of suicide.3,4 University students are in a transitional stage from adolescence to adulthood, a phase known as “emerging adulthood”, which is crucial for the development of various health behaviours that are important for their future adulthood and throughout their lifespan.5 University students face numerous challenges such as interpersonal adaptation, academic pressure and financial stress, and may be at high risk for a variety of psychological issues and unhealthy behaviours.5 Similarly, sleep problems are widespread among this group. A meta-analysis incorporating 57 studies showed that the average sleep duration for Chinese university students is 7.08 hours. The proportions of students sleeping less than 6 hours and 7 hours were 8.4% and 43.9%, respectively. The percentage of students who took more than 30 minutes to fall asleep is 25.5%. The average bedtime was at 00:51 AM, with approximately 23.8% of students going to bed after midnight.6 Although sleep problems among university students are serious, effective measures for addressing these problems are lacking.
In recent years, while attention has been given to the effects of sleep on “downstream” health or disease outcomes, an increasing number of studies have focused on the determinants or “upstream” factors of sleep disorders.4 Interventions targeting these modifiable behavioral lifestyle factors are highly important for maintaining sleep health. Among the factors influencing sleep disorders, the impact of excessive smartphone use on sleep has increasingly received scholarly attention.
As a notable type of technology, smartphones have become ubiquitous, providing convenience for people while also bringing about negative consequences that cannot be ignored. The excessive use of smartphones, inability to control the dependence on smartphones, and resulting impairment of daily functions can be termed problematic smartphone use (PSU).7,8 Although PSU has not been classified as a clinical disorder, its manifestations are similar to the symptoms of internet gaming addiction and substance abuse as described in the Diagnostic and Statistical Manual of Mental Disorders (DSM-V).9 The relationship between PSU and sleep disturbances has been extensively studied. The excessive use of smartphones, especially before bedtime, can delay sleep onset, disrupt sleep rhythms, and reduce total sleep duration. Studies have shown that the excessive use of smartphones increases exposure to blue light, which suppresses the secretion of melatonin, leading to disruptions in circadian rhythms and sleep problems, and may also be closely related to mental issues such as depression.10 Multiple studies, including cross-sectional and longitudinal studies focusing on college students, have shown that PSU can significantly predict the risk of developing sleep disorders.11–14 For instance, in a study involving 1181 college students, baseline smartphone addiction significantly predicted bedtime procrastination and poor sleep quality one year later.12 This singular prediction of sleep quality by smartphone addition differs from the bidirectional predictive relationship found between the two variables in another study.15 Given the current lack of consensus on the longitudinal predictive relationship between PSU and sleep quality, it is necessary to further explore the relationship between the two. Additionally, in addition to directly affecting sleep, PSU might serve as an aversive emotional avoidance strategy, indirectly impacting sleep health through negative psychological states such as anxiety and depressive symptoms.
Anxiety and depression disorders are very common mental health issues among college students, and both may independently mediate the relationship between PSU and sleep quality. Anxiety disorders refer to feelings of fear, distress, and panic caused by external objective factors or the subjective thoughts of an individual;16 depression disorders are characterized by low spirits, loss of interest, self-deprecation, and despair.17 A large number of cross-sectional studies have reported a positive correlation between PSU and anxiety/depression, and cohort studies have further shown that PSU can increase the risk of anxiety and depression.18,19 Moreover, existing research evidence suggests that individuals with anxiety and depression are more prone to experiencing poor sleep quality, indicating that mental illnesses may serve as characteristic markers of a high-risk population for sleep issues.20 Furthermore, since sleep problems are core symptoms of specific anxiety and depression disorders according to the fourth edition of the Diagnostic and Statistical Manual for Mental Disorders (DSM-IV), chronic sleep disorders accompanied by mental illness are commonly observed in both clinical and nonclinical populations.21
Previous cross-sectional studies have independently explored the mediating roles of anxiety or depression in the relationship between PSU and sleep quality.22,23 A cross-lagged study based on two waves of panel data suggested that the individual mediating roles of anxiety or depression is only one aspect explaining the relationship between smartphone addiction and sleep quality.12 Considering the common genetic susceptibility and comorbidity rates, anxiety and depression have a high rate of co-occurrence.24,25 Anxiety can be considered a significant cause of depression.26 Both cohort studies and meta-analyses have shown that anxiety can effectively predict future depressive symptoms, and vice versa.26,27 Furthermore, compared to individual symptoms, the combination of these two emotional disorders leads to poorer social and psychological functioning, lower perceived quality of life, and a greater burden of illness.28 The individual and combined effects of both anxiety and depression play a significant role in explaining the relationships between other independent variables and outcomes.29–31 The impact of excessive smartphone dependence on sleep quality may be influenced by symptoms of anxiety and/or depression. To some extent, sleep quality depends on people’s lifestyles and the extent to which diseases affect various aspects of life. Whether the effect of PSU on sleep quality operates through symptoms of anxiety and/or depression deserves in-depth exploration.
In general, numerous studies have investigated the pathways through which PSU impacts sleep, including the independent mediating roles of depressive or anxiety symptoms.12,14,32–34 However, to our knowledge, the majority of earlier investigations into the mechanisms by which smartphone use impacts sleep have employed cross-sectional designs or, at most, two-wave longitudinal studies. These studies have primarily focused on the individual mediating roles of anxiety or depression in this relationship. However, such approaches may not fully capture the dynamic and potentially cumulative effects these factors exert over time. In contrast, utilizing data from a three-wave survey is very necessary for a more nuanced and comprehensive understanding of how these variables interact across multiple points in time. Furthermore, our unique demographic and highland environmental background adds a degree of novelty. In highland areas characterized by high altitude, low oxygen, extreme cold, and low atmospheric pressure, the occurrence of anxiety and depression is significantly higher than in plains areas,35 and it is only recently that this topic has begun to attract attention. This study used data from a three-wave survey of university students at two universities in Tibet, China, to explore the independent and joint mediating effects of anxiety and depressive symptoms. We hypothesize that anxiety symptoms at Time 2 (T2) would mediate the relationship between PSU at Time 1 (T1) and sleep quality at Time 3 (T3) (Hypothesis 1); depressive symptoms at Time 2 (T2) would mediate the relationship between PSU at Time 1 (T1) and sleep quality at Time 3 (T3) (Hypothesis 2); and anxiety and depressive symptoms at T2 would play a serial mediating role in the relationship between PSU at T1 and sleep quality at T3 (Hypothesis 3).
Methods
Participants and Procedure
This study was conducted in June, September, and December 2021 first-year and second-year students were selected from two universities in the Tibet Autonomous Region to complete questionnaire surveys and follow-up research. The students participated on a voluntary basis and provided informed consent, and they could withdraw from the study at any time during the follow-up. Before the survey, the research team members communicated with the relevant leaders of each participating college and the instructors responsible for student affairs. The instructors then preformed the student representatives and their respective classes about the purpose and significance of the survey, emphasizing the principle of voluntariness. Members of the research team and graduate students who had undergone on-site questionnaire training coordinated the survey timing with the instructors and student representatives. The students were then gathered in classrooms, where a paperless questionnaire (wenjuanxing) was administered. QR codes for the questionnaire were distributed to the students, who completed the questionnaire anonymously. During the implementation of the survey, if students had any questions, they were addressed on the spot by the survey team members or trained surveyors. The questionnaire took approximately 18 minutes to complete. For students who did not come to the classroom, trained student representatives from their respective colleges introduced the survey method and content, guiding the students through the questionnaire completion and submission process. A total of 2993 students participated in the three surveys.
Measures
Sleep Quality
The widely-used Chinese version of the Pittsburgh Sleep Quality Index (PSQI) self-rating scale was adopted to measure students’ sleep quality and disturbances over the past month. The PSQI comprises 19 items, divided into seven component scores: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. The score for each component ranges from 0 to 3 points. The total PSQI score ranges from 0 to 21, with a higher score indicating poorer sleep quality.36,37 The PSQI has been extensively used in the Chinese population and has good validity and reliability, with an overall reliability coefficient of 0.82–0.83. In the Chinese population, a PSQI total score exceeding 7 points indicates poor sleep quality or sleep disturbances.37 This self-rating scale was utilized at T1-T3.
Problematic Smartphone Use
Smartphone use behaviours comprises smartphone dependence and usage duration. This was assessed using the short version of the Smartphone Addiction Scale38 (Smartphone Addiction Scale-short Version, SAS-SV). The scale was originally constructed by Kwon and others, mainly to evaluate smartphone use problems.39 Researchers created a simplified version of the scale with 10 items based on the original 33 items. The SAS-SV has been widely applied in different cultural contexts and includes aspects such as daily life impact, withdrawal, and tolerance.40 Examples items include “I constantly check my smartphone so as not to miss new messages from social apps such as WeChat, Weibo, and QQ” and “I feel impatient and restless when my smartphone is not within reach”. A six-point Likert scale is used for each item, with scores ranging from 1 to 6: “strongly disagree”, “disagree”, “somewhat disagree”, “somewhat agree” “agree”, and “strongly agree”. The total score for the scale ranges from 10 to 60 points, with a higher score indicating a greater degree of smartphone dependence. According to previous literature, cut-off scores of ≥31 (for males) and ≥33 (for females) are used to determine smartphone use dependence, reflecting the smartphone dependence situation among university students.39,40 The Chinese short version of the Smartphone Addiction Scale has good reliability and validity.38 The Cronbach’s alpha in this scale was 0.912 at T1.31
Anxiety Symptoms
Anxiety symptoms were assessed using the Generalized Anxiety Disorder-7 (GAD-7) scale. In this scale, Cronbach’s alpha coefficient of the GAD-7 at T1-T3 was 0.935–0.937. This scale was originally developed by Spitzer et al and is widely used due to its simplicity, ease of administration, and scoring ability.41 The frequency of seven core symptoms over the past two weeks is assessed through seven items scored on a 4-point Likert scale, ranging from “not at all = 0” to “nearly every day = 3”. The total score for the GAD-7 ranges from 0 to 21. A score exceeding 10 points is considered indicative of anxiety symptoms.41 The higher the score, the greater the severity of anxiety.
Depressive Symptoms
The assessment of depressive symptoms was conducted using the Patient Health Questionnaire-9 (PHQ-9), a scale composed of 9 items, reflecting the occurrence of symptoms over the past 14 days. The response options for each item include “Not at all (scored 0)”, “Several days (1 point)”, “More than half the days (2 points)”, and “Nearly every day (3 points)”. The total score of the scale ranges from 0 to 27, with higher scores indicating more severe depressive symptoms. A score exceeding 10 points is considered indicative of depressive symptoms.42 The scale has good reliability and validity.42 In T1-T3, the Cronbach’s alpha coefficient in our scale was 0.920–0.921.31
Covariates
This study collected data on multiple baseline demographic characteristics, interpersonal relationships, academic stress, and behavioral factors. Sex (male/female), age (years), place of origin (urban/rural), family economic status (better/average/poor), ethnicity (Han/Tibetan and others), and parents’ marital status (harmonious/sometimes, frequent quarrels/separated, divorced/other) were all considered. The respondents’ relationships with their families, classmates, and teachers (all rated as better/average/poor) were evaluated. Previous studies have shown that sleep quality is strongly associated with students’ academic performance.43 Considering the relationship between academic stress and sleep quality, drawing on previous methods of measuring academic stress,44,45 we collected students’ academic stress levels by their self-assessed levels (1 = Minor, 2 = Moderate, and 3 = Major). A respondent who smoked at least once in the past month was considered a current smoker; a respondent who drank alcohol at least once in the past month was considered a current drinker.
Statistical Analyses
Data analysis was conducted using SPSS V23.0. The basic demographic characteristics of the study participants at baseline are described. Qualitative data are presented as rates or percentages, while quantitative data are expressed as the mean ± standard deviation. In the mediation analysis study, a sub dataset was established based on the original dataset. This sub dataset was created by excluding individuals with poor sleep quality at baseline (T1) and follow-up (T2) (PSQI score ≥7) and individuals with anxiety (GAD-7 score≥10) and depressive symptoms at baseline T1 (PHQ-9 score≥10). Pearson correlation analysis was used for pairwise correlation analysis of the variables. SPSS PROCESS V3.3 Model 6 was used for the chain mediation analysis to explore the mediating role of anxiety and depressive symptoms in the relationship between PSU at T1 and sleep quality at T3. The significance of the mediation effect was tested using the bias-corrected bootstrap method, with 5000 bootstrap samples. A 95% bootstrap confidence interval that did not include 0, it was considered to indicate statistical significance.46
Results
Descriptive Analyses
Among the 2993 subjects included in the study, the average age at T1 was 19.7±1.25 years. There were 1007 (34.3%) male participants and 1926 (65.7%) female participants. Among the participants, 1267 (43.2%) were of Han ethnicity, 1583 (54.0%) were of Tibetan ethnicity, and 83 (2.8%) belonged to other minority ethnic groups. Regarding academic status, 1610 (54.9%) participants were first-year students, and 1383 (45.1%) were second-year students. In terms of self-assessed family economic status, 478 (16.3%) considered it good, 1540 (52.5%) considered it average, and 915 (31.2%) considered it poor. Among the participants, 304 (10.2%) were smokers, and 391 (13.1%) consumed alcohol. The basic demographic characteristics of the study subjects are summarized in Table 1.
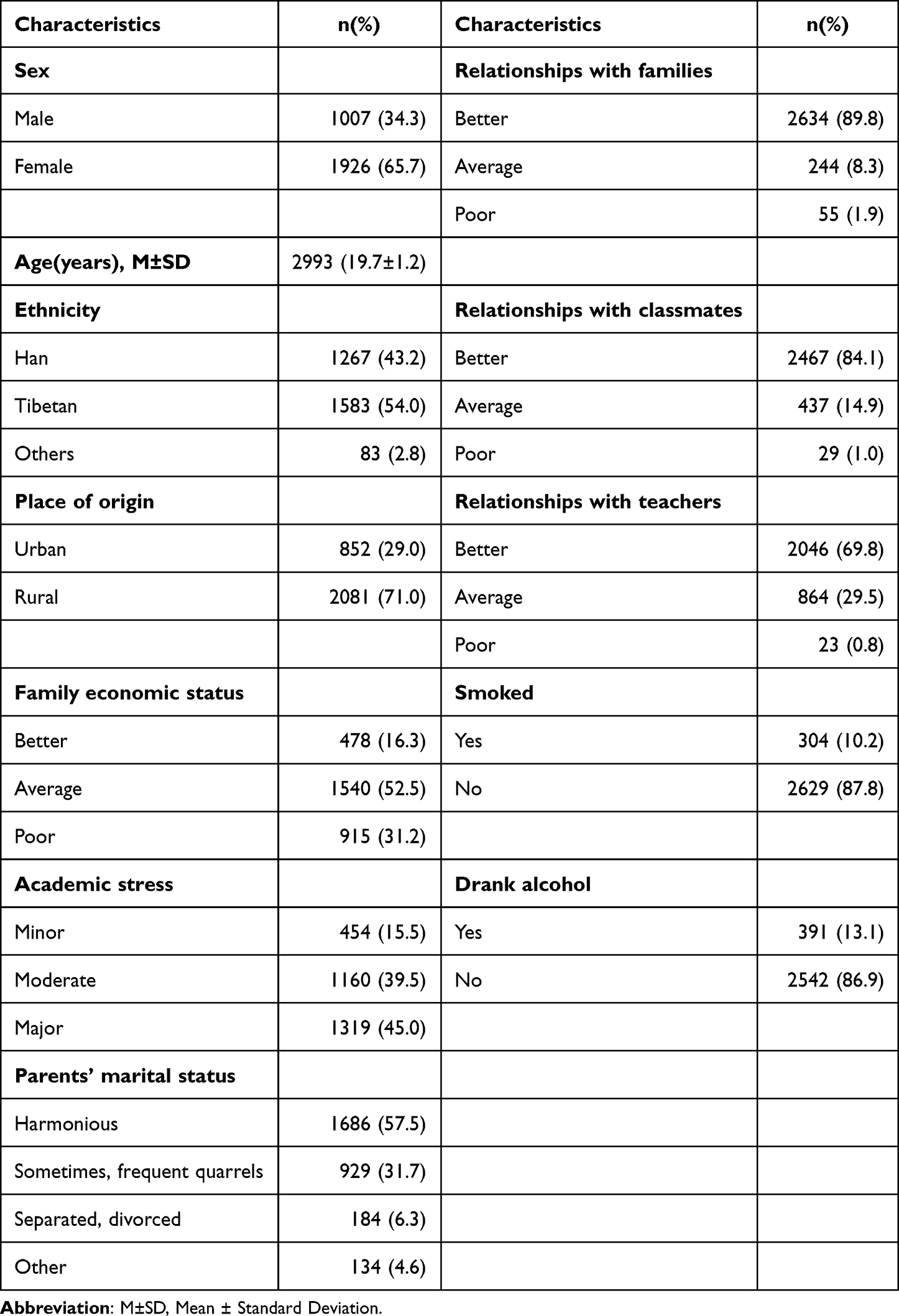 |
Table 1 The Basic Demographic Characteristics of the Study Subjects (n=2993) |
Bivariate correlation analysis revealed that at T1, PSU was positively correlated with anxiety symptoms at T2 (r=0.20, P<0.001), depressive symptoms at T2 (r=0.23, P<0.001), and poor sleep quality at T3 (r=0.16, P<0.001). Furthermore, anxiety at T2 and depressive symptoms at T2 were positively correlated (r=0.76, P<0.001), as was poor sleep quality at T3 (r=0.34, P<0.001). Depressive symptoms at T2 and sleep quality at T3 were also positively correlated (r=0.39, P<0.001). Please refer to Table 2 for the detailed results.
 |
Table 2 Variable Correlation Analysis |
Serial Mediation Model
From the original dataset, students with poor sleep quality at T1 and T2, as well as those with symptoms of anxiety and depression at T1, were excluded from the new dataset. This new dataset was used to investigate the serial mediating roles of anxiety and depressive symptoms in the relationship between PSU and sleep quality. The details are shown in Figure 1.
 |
Figure 1 The chain mediating pathway of T2 anxiety and depressive symptoms on T1 PSU and T3 sleep quality; The model corrected for baseline factors like sex, age, place of origin, family economic status, ethnicity, academic pressure, parents’ marital status, the respondents’ relationships with their families, classmates, and teachers, smoked and drank alcohol consumption; ***P<0.001, **P<0.01, *P<0.05. Abbreviation: PSU, problematic smartphone use. |
Table 3 presents the results of the serial mediation analysis, taking anxiety and depressive symptoms at T2 as the mediator variables, PSU at T1 as the independent variable, and sleep quality at T3 as the dependent variable. This analysis controlled for baseline factors such as age, sex, ethnicity, family economic status, family relationships, parental marital status, academic pressure, peer relationships, and teacher relationships. The relationship between baseline PSU and sleep quality at T3 was significant (total effect=0.036, 95% CI=0.024–0.048). The direct effect between the two variables was also significant (direct effect=0.021, 95% CI=0.010–0.033), with a significant total indirect effect (total indirect effect=0.015, 95% CI=0.011–0.019), accounting for 41.7% of the total effect. Specifically, the mediating effect of anxiety at T2 on the relationship between PSU at T1 and poor sleep quality at T3 was significant (indirect effect 1=0.003, 95% CI=0.001–0.006), accounting for 20.0% of the total indirect effect. The mediating effect of depressive symptoms at T2 was significant (indirect effect 2=0.004, 95% CI=0.002–0.006), accounting for 26.7% of the total indirect effect. Moreover, the chain mediating effect of anxiety and depressive symptoms at T2 was significant (indirect effect 3=0.008, 95% CI=0.005–0.011), representing 53.3% of the total indirect effect. Upon further comparison of the mediating effects, a significant difference between the chain mediating effect (indirect effect 3) and indirect effect 2 was found, suggesting that the impact of PSU on poor sleep quality is considerably enhanced when mediated by both anxiety and depressive symptoms.
 |
Table 3 The Effect of T1 PSU on T3 Sleep Quality: Serial Mediating Effects of T2 Anxiety and Depressive Symptoms (n=1807)a |
Discussion
Based on the findings of previous studies, this research further explored the possible mechanisms linking PSU and poor sleep quality. Using a sample of 2993 Tibetan college students, the study employed a longitudinal multiple mediation model to investigate the independent and combined mediating roles of anxiety and depression symptoms in the relationship between poor and poor sleep quality.
This study’s findings reveal that anxiety symptoms significantly mediate the link between problematic smartphone use (PSU) and diminished sleep quality. In essence, higher PSU levels correlate with intensified anxiety symptoms and deteriorating sleep quality, aligning with past research.34,47,48 Yet, Yingnan Zhang’s work introduces a nuanced perspective, identifying anxiety symptoms as a complete mediator in the PSU-sleep quality association, highlighting anxiety’s detrimental role on sleep.49 This distinction underscores the seductive lure of smartphones for college students, offering a virtual escape that, while momentarily soothing, potentially exacerbates stress-handling incapacity, heightening anxiety and subsequently impairing sleep quality.48 Moreover, excessive smartphone engagement may erode the fabric of real-life social interactions, fueling interpersonal strains and anxiety,50 which directly precipitate sleep disturbances like insomnia, superficial sleep, and sensitivity to disruptions.51
Biologically, anxiety magnifies the emotional fragility wrought by sleep loss. Experiments show that sleep-deprived individuals exhibit amplified amygdala and anterior insula responses to stressors, with heightened anxiety amplifying these reactions. This suggests that even minor anxiety levels can worsen emotional susceptibility under sleep deprivation.52 Comparative studies on anxious versus non-anxious adolescents reveal that sleep deprivation in anxious individuals dampens activity in emotion-regulation centers (dorsal anterior cingulate cortex and hippocampus) while enhancing specific neural connections, indicating a unique vulnerability to sleep loss.53 These insights pivot us toward reevaluating the multifaceted impacts of PSU, especially as it pertains to mental health and sleep hygiene. Understanding the intricate dynamics between PSU, anxiety, and sleep quality not only sheds light on the underlying mechanisms but also urges the development of nuanced intervention strategies.
This study illuminates the critical mediating role of depression symptoms in the nexus between problematic smartphone use (PSU) and sleep quality deterioration. It prompts us to question: How does the escalation of PSU exacerbate depression symptoms and concurrently impair sleep quality, paralleling earlier discoveries?54,55 The journey into excessive smartphone engagement leads to a solitary lifestyle shift, from tangible to digital social exchanges, potentially deepening the chasm of loneliness. This introspection raises another inquiry: Could the loneliness and diminished self-esteem faced by college students, amplified by life’s pressures and academic demands, heighten their vulnerability to depression and sleep disturbances?56
Joel et al’s “Inappropriate Use of Mobile Phones Path Model” posits PSU as a quest for solace, marred by impulse control failure and extraversion.57 This model challenges us to consider: Is emotional dysregulation the root, fueling the inability to curb unnecessary impulses, thereby diminishing emotional self-efficacy and exacerbating depression symptoms?58,59
Furthermore, the discourse on biological mechanisms offers a provocative angle—could PSU-induced depressive symptoms be intricately linked to the brain’s reward system? This exploration unveils the reward circuitry, including the ventral striatum and medial prefrontal cortex, as potential culprits in the reduced sensation of pleasure, a hallmark of depression. Intriguingly, does severe PSU correlate with structural brain changes, such as reduced grey matter volume in the anterior cingulate cortex, implicating the reward circuit in this maladaptive pattern?60 Research has shown that the more severe the PSU is, the smaller the volume of grey matter in the anterior cingulate cortex, and the poorer the integrity of white matter in the brain. PSU is associated with the function of the reward circuit. Moreover, in the PSU group, the functional connectivity (FC) between the left inferior frontal gyrus and the left parahippocampal gyrus and specific brain regions was enhanced. This suggests that brain structure and the reward circuit are related to PSU.61
In this investigation, we find that PSU impairs sleep quality via a sequential mediation of anxiety and depressive symptoms, accumulating negative emotional burdens. This pattern aligns with prior research, revealing the intricate dance between PSU, social anxiety, and depression among university students. A curious question emerges: How does PSU, through its intricate web of social anxiety and depressive symptoms, erode the foundation of good sleep? Research underscores social anxiety’s full mediation role between PSU and depression,62 spotlighting its pivotal position in the depression narrative. Could this highlight a deeper, more complex interaction at play, where social anxiety not only bridges but amplifies the relationship between PSU and depressive symptoms?
As students’ reliance on smartphones grows, so does the time and energy devoted to these devices, inversely affecting physical activity. A striking finding from Su et al’s study29 among adults in Guangdong points to a noteworthy conclusion: the more physically inactive one becomes, the poorer the sleep quality, mediated by anxiety and depression. This cascading effect—physical activity reduction leading to anxiety, which in turn leads to depression and subsequently poor sleep—accounts for a significant portion of the impact on sleep quality. Could this suggest a deeper, systemic issue where lifestyle choices intertwined with digital habits are fundamentally altering our well-being?
The Social Replacement Hypothesis offers another layer of insight, proposing that excessive smartphone use diminishes the quality and frequency of real-world social interactions, a crucial component of mental health.63 Meanwhile, Harvey’s cognitive model of insomnia64 introduces a psychological perspective, suggesting that negative emotions, primarily anxiety, and depressive symptoms, catalyze cognitive biases towards stressful life scenarios, such as the interpersonal issues stemming from smartphone dependency. This cognitive spiraling, fixating on stressors, incrementally degrades sleep quality, potentially leading to insomnia. Could these models collectively offer a framework to understand the nuanced ways in which our digital habits are reshaping our psychological landscape, sleep patterns, and overall health? This prompts a broader contemplation on the mechanisms through which PSU influences our lives and the potential pathways for mitigating its effects, inviting further exploration into the complex interplay between digital engagement, emotional health, and sleep hygiene.
Limitations and Future Directions
This study has the following limitations. First, although self reports are easily accepted by respondents, recall bias is inevitable In the future, a variety of methods, such as face-to-face interviews, sleep diaries and more objective measurements (such as polysomnography), should be used. Second, our study only included university students as subjects; future studies should be conducted in a broader population. Third, given that we did not investigate the usage tendencies for different apps or other issues, we were unable to explore the specific relationships between the collected data on usage content and anxiety, depressive symptoms, and sleep quality;65 moreover, we did not consider information on the usage of other electronic devices such as tablets, computers, or televisions.66,67 Fourth, this study did not have an experimental design, so causal relationships among the four variables cannot be determined. Interventional study designs are needed in the future. Fifth, the relationship between PSU and sleep quality may be mediated by complex psychological and behavioral mechanisms. Previous studies have shown that factors such as bedtime procrastination, self-regulation, and psychological inflexibility can mediate the relationship between PSU and sleep quality.12,33,68 These factors were not included in this study, which may limit the interpretability of the results. Future studies should comprehensively explore the mediating role of the above factors in this relationship.
Despite the aforementioned limitations, this study still has several advantages, including the three-wave longitudinal design, the relatively large sample size, and better control for covariates. This research will have theoretical and practical significance for reducing PSU, sleep issues, and psychological distress among college students. Theoretically, this study preliminarily clarifies the longitudinal mediating role of anxiety and depressive symptoms in the relationship between college students’ PSU and sleep quality, filling the gap in previous studies that used only cross-sectional or two-wave data. Moreover, as this study is based on the comprehensive relationships of multiple variables, it can provide a foundation for further research into related mechanisms. Practically speaking, when addressing sleep disorders, more attention should be given to students’ behavioural issues. Student counsellors should adopt appropriate methods to strengthen interventions for excessive smartphone use among students. Mental health professionals can mitigate the impact of PSU on sleep quality by reducing students’ psychological distress, including symptoms of anxiety and depression.
Conclusion
This study explored the potential pathways connecting PSU and sleep quality among university students in Tibet, China, thereby expanding upon the findings of previous research. Anxiety and depressive symptoms were found to play independent and serial mediating roles in the longitudinal relationship between PSU and sleep quality. Specifically, the mediating role of depressive symptoms was more significant than that of anxiety. Consequently, effective interventions aimed at addressing university students’ PSU and psychological distress, including anxiety and depression, could be beneficial for improving their sleep quality.
Ethics Statement
This study received approval from the Ethics Committee of Xizang Minzu University [No. 202329] and complied with the Declaration of Helsinki. The subjects were fully informed of the content and purpose of the survey before participation. All participants provided informed consent before the participation in the present study.
Acknowledgment
The authors would like to express their special thanks for the support and assistance of the participating schools and student administrators, as well as the study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Scientific Research Plan Projects of Shaanxi Province Education Department (Grant No. 22JK0205), National Natural Science Foundation of China (International Cooperation and Exchange Programme) (Grant No. 81761128030), Natural Science Foundation of Tibet Autonomous Region (Grant No. XZ202201ZR0055G), Tibet Autonomous Region Higher Education Teaching Reform Project (Grant No. JG2023-53), Research Projects of Xizang Minzu University (Grant No. 23MDY08), the Scientific Research Project of Xizang Minzu University (No. 23MDQ03).
Disclosure
The authors declare that they have no competing interests.
References
1. Institute of Medicine (US) Committee on Sleep Medicine and Research. Sleep disorders and sleep deprivation: an unmet public health problem. National Academies Press (US); 2006. Avilable from: http://www.ncbi.nlm.nih.gov/books/NBK19960/.
2. Stranges S, Tigbe W, Gómez-Olivé FX, Thorogood M, Kandala NB. Sleep problems: an emerging global epidemic? Findings from the INDEPTH WHO-SAGE study among more than 40,000 older adults from 8 countries across Africa and Asia. Sleep. 2012;35(8):1173–1181. doi:10.5665/sleep.2012
3. Irwin MR, Olmstead R, Carroll JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiatry. 2016;80(1):40–52. doi:10.1016/j.biopsych.2015.05.014
4. Grandner MA. Sleep and Health. Academic Press; 2019.
5. Arnett JJ. Emerging Adulthood: The Winding Road from the Late Teens Through the Twenties. Oxford University Press; 2023.
6. Li L, Wang YY, Wang SB, et al. Sleep duration and sleep patterns in Chinese university students: a comprehensive meta-analysis. J Clin Sleep Med. 2017;13(10):1153–1162. doi:10.5664/jcsm.6760
7. Elhai JD, Dvorak RD, Levine JC, Hall BJ. Problematic smartphone use: a conceptual overview and systematic review of relations with anxiety and depression psychopathology. J Affective Disorders. 2017;207:251–259. doi:10.1016/j.jad.2016.08.030
8. Busch PA, McCarthy S. Antecedents and consequences of problematic smartphone use: a systematic literature review of an emerging research area. Comput Human Behav. 2021;114:106414. doi:10.1016/j.chb.2020.106414
9. Diagnostic and Statistical Manual of Mental Disorders. Available from: https://www.sciencedirect.com/topics/medicine-and-dentistry/diagnostic-and-statistical-manual-of-mental-disorders.
10. Touitou Y, Touitou D, Reinberg A. Disruption of adolescents’ circadian clock: the vicious circle of media use, exposure to light at night, sleep loss and risk behaviors. J Physiol Paris. 2016;110(4 Pt B):467–479. doi:10.1016/j.jphysparis.2017.05.001
11. Huang Q, Li Y, Huang S, et al. Smartphone use and sleep quality in Chinese college students: a preliminary study. Front Psychiatry. 2020;11:352. doi:10.3389/fpsyt.2020.00352
12. Cui G, Yin Y, Li S, et al. Longitudinal relationships among problematic mobile phone use, bedtime procrastination, sleep quality and depressive symptoms in Chinese college students: a cross-lagged panel analysis. BMC Psychiatry. 2021;21(1):449. doi:10.1186/s12888-021-03451-4
13. Liu S, Wing YK, Hao Y, Li W, Zhang J, Zhang B. The associations of long-time mobile phone use with sleep disturbances and mental distress in technical college students: a prospective cohort study. Sleep. 2019;42(2). doi:10.1093/sleep/zsy213
14. Sohn SY, Krasnoff L, Rees P, Kalk NJ, Carter B. The association between smartphone addiction and sleep: a UK cross-sectional study of young adults. Frontiers in Psychiatry. 2021;2021:12.
15. Kang Y, Liu S, Yang L, et al. Testing the bidirectional associations of mobile phone addiction behaviors with mental distress, sleep disturbances, and sleep patterns: a one-year prospective study among Chinese college students. Frontiers in Psychiatry. 2020;11:11. doi:10.3389/fpsyt.2020.00011
16. Julian LJ. Measures of Anxiety. Arthritis Care Res. 2011;63(0 11):
17. Miller K, Massie MJ. Depression and Anxiety. Cancer J. 2006;12(5):388. doi:10.1097/00130404-200609000-00008
18. Sohn SY, Rees P, Wildridge B, Kalk NJ, Carter B. Prevalence of problematic smartphone usage and associated mental health outcomes amongst children and young people: a systematic review, meta-analysis and GRADE of the evidence. BMC Psychiatry. 2019;19(1):356. doi:10.1186/s12888-019-2350-x
19. Augner C, Vlasak T, Aichhorn W, Barth A. The association between problematic smartphone use and symptoms of anxiety and depression-A meta-analysis. J Public Health (Oxf). 2021;fdab350. doi:10.1093/pubmed/fdab350
20. Manber R, Chambers AS. Insomnia and depression: a multifaceted interplay. Curr Psychiatry Rep. 2009;11(6):437–442. doi:10.1007/s11920-009-0066-1
21. Nutt D, Wilson S, Paterson L. Sleep disorders as core symptoms of depression. Dialogues Clin Neurosci. 2008;10(3):329–336. doi:10.31887/DCNS.2008.10.3/dnutt
22. Liu J, Liu CX, Wu T, Liu BP, Jia CX, Liu X. Prolonged mobile phone use is associated with depressive symptoms in Chinese adolescents. J Affect Disord. 2019;259:128–134. doi:10.1016/j.jad.2019.08.017
23. Zou L, Wu X, Tao S, et al. Mediating effect of sleep quality on the relationship between problematic mobile phone use and depressive symptoms in college students. Front Psychiatry. 2019;10:822. doi:10.3389/fpsyt.2019.00822
24. Middeldorp CM, Cath DC, Dyck RV, Boomsma DI. The co-morbidity of anxiety and depression in the perspective of genetic epidemiology. A review of twin and family studies. Psychological Medicine. 2005;35(5):611–624. doi:10.1017/S003329170400412X
25. Brown TA, Campbell LA, Lehman CL, Grisham JR, Mancill RB. Current and lifetime comorbidity of the DSM-IV anxiety and mood disorders in a large clinical sample. J Abnormal Psychol. 2001;110(4):585–599. doi:10.1037/0021-843X.110.4.585
26. Jacobson NC, Newman MG. Anxiety and depression as bidirectional risk factors for one another: a meta-analysis of longitudinal studies. Psychol Bull. 2017;143:1155–1200. doi:10.1037/bul0000111
27. Jacobson NC, Newman MG. Avoidance mediates the relationship between anxiety and depression over a decade later. J Anx Disord. 2014;28(5):437–445. doi:10.1016/j.janxdis.2014.03.007
28. Kang HJ, Bae KY, Kim SW, et al. Impact of anxiety and depression on physical health condition and disability in an Elderly Korean population. Psychiatry Invest. 2017;14(3):240–248. doi:10.4306/pi.2017.14.3.240
29. Su Y, Wang SB, Zheng H, et al. The role of anxiety and depression in the relationship between physical activity and sleep quality: a serial multiple mediation model. J Affect Disord. 2021;290:219–226. doi:10.1016/j.jad.2021.04.047
30. Liu Y, Xu Y, Yang X, Miao G, Wu Y, Yang S. Sensory impairment and cognitive function among older adults in China: the mediating roles of anxiety and depressive symptoms. Int J Geriatr Psychiatry. 2023;38(1):e5866. doi:10.1002/gps.5866
31. Wu R, Guo L, Rong H, et al. The role of problematic smartphone uses and psychological distress in the relationship between sleep quality and disordered eating behaviors among Chinese college students. Front Psychiatry. 2021;12:793506. doi:10.3389/fpsyt.2021.793506
32. Chen JK, Wu WC. Reciprocal relationships between sleep problems and problematic smartphone use in Taiwan: cross-lagged panel study. Int J Environ Res Public Health. 2021;18(14):7438. doi:10.3390/ijerph18147438
33. Peltz JS, Bodenlos JS, Kingery JN, Abar C. Psychological processes linking problematic smartphone use to sleep disturbance in young adults. Sleep Health. 2023;9(4):524–531. doi:10.1016/j.sleh.2023.05.005
34. Demirci K, Akgönül M, Akpinar A. Relationship of smartphone use severity with sleep quality, depression, and anxiety in university students. J Behav Addict. 2015;4(2):85–92. doi:10.1556/2006.4.2015.010
35. Wu R, Guang Z, Wang Y, et al. Eating disorders symptoms and depressive symptoms in Chinese Tibetan University students: a network analysis. BMC Psychiatry. 2023;23(1):957. doi:10.1186/s12888-023-05452-x
36. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
37. Tsai PS, Wang SY, Wang MY, et al. Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Qual Life Res. 2005;14(8):1943–1952. doi:10.1007/s11136-005-4346-x
38. Luk TT, Wang MP, Shen C, et al. Short version of the smartphone addiction scale in Chinese adults: psychometric properties, sociodemographic, and health behavioral correlates. J Behav Addict. 2018;7(4):1157–1165. doi:10.1556/2006.7.2018.105
39. Kwon M, Kim DJ, Cho H, Yang S. The smartphone addiction scale: development and validation of a short version for adolescents. PLoS One. 2013;8(12):e83558. doi:10.1371/journal.pone.0083558
40. Elhai JD, Tiamiyu MF, Weeks JW, Levine JC, Picard KJ, Hall BJ. Depression and emotion regulation predict objective smartphone use measured over one week. Pers Individ Dif. 2018;133:21–28. doi:10.1016/j.paid.2017.04.051
41. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
42. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
43. Curcio G, Ferrara M, De Gennaro L. Sleep loss, learning capacity and academic performance. Sleep Med Rev. 2006;10(5):323–337. doi:10.1016/j.smrv.2005.11.001
44. Wang Y, Guang Z, Zhang J, et al. Effect of sleep quality on anxiety and depression symptoms among college students in China’s Xizang region: the mediating effect of cognitive emotion regulation. Behav Sci. 2023;13(10):861. doi:10.3390/bs13100861
45. Guo L, Wang W, Wang T, et al. Association of emotional and behavioral problems with single and multiple suicide attempts among Chinese adolescents: modulated by academic performance. J Affective Disorders. 2019;258:25–32. doi:10.1016/j.jad.2019.07.085
46. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis, Second Edition: A Regression-Based Approach. Guilford Publications; 2017.
47. Jiang X, He B, Wang J. Analysis of the Relationship Between Smartphone Addiction and Sleep Quality Among Undergraduate Students at a Medical University in Nanjing City and the Mediating Role of Generalized Anxiety. Occupation and Health. 2019;35(13):1851–1853.
48. Wang J, Liu W, Li Q. Mobile phone addiction and college students’ sleep quality: the role of anxiety and rumination. Chin J Clin Psychol. 2021;29:1060–1063.
49. Zhang Y, Di X, Sun W. The impact of mobile phone dependence on sleep quality: the mediating role of anxiety. Cont Med Educ Chin. 2020;12(26):94–97.
50. Kuss DJ, Griffiths MD. Online social networking and addiction--A review of the psychological literature. Int J Environ Res Public Health. 2011;8(9):3528–3552. doi:10.3390/ijerph8093528
51. Sullivan EC, Halstead EJ, Ellis JG, Anxiety DD. Insomnia, and napping predict poorer sleep quality in an autistic adult population. Int J Environ Res Public Health. 2021;18(18):9883. doi:10.3390/ijerph18189883
52. Goldstein AN, Greer SM, Saletin JM, Harvey AG, Nitschke JB, Walker MP. Tired and apprehensive: anxiety amplifies the impact of sleep loss on aversive brain anticipation. J Neurosci. 2013;33(26):10607–10615. doi:10.1523/JNEUROSCI.5578-12.2013
53. Carlisi CO, Hilbert K, Guyer AE, Ernst M. Sleep-amount differentially affects fear-processing neural circuitry in pediatric anxiety: a preliminary fMRI investigation. Cogn Affect Behav Neurosci. 2017;17(6):1098–1113. doi:10.3758/s13415-017-0535-7
54. Islam M. Link between excessive smartphone use and sleeping disorders and depression among South Korean University students. Healthcare. 2021;9(9):1213. doi:10.3390/healthcare9091213
55. Li Q. A study on the relationship between depression, sleep quality, and smartphone use among college students. J Zunyi Normal Coll. 2021;23(06):158–161.
56. Shi X, Wang A, Zhu Y. Longitudinal associations among smartphone addiction, loneliness, and depressive symptoms in college students: disentangling between– and within–person associations. Addict Behav. 2023;142:107676. doi:10.1016/j.addbeh.2023.107676
57. Billieux J, Maurage P, Lopez-Fernandez O, Kuss DJ, Griffiths MD. Can disordered mobile phone use be considered a behavioral addiction? An update on current evidence and a comprehensive model for future research. Curr Addict Rep. 2015;2(2):156–162. doi:10.1007/s40429-015-0054-y
58. Berte DZ, Mahamid FA, Affouneh S. Internet Addiction and Perceived Self-Efficacy Among University Students. Int J Ment Health Addict. 2021;19(1):162–176. doi:10.1007/s11469-019-00160-8
59. Hu G, Cheng X, Yan C, Hong S, Li N, Xu Z. Impacts of college students’mobile phone addiction on depression: the mediating of regulatory emotional self-efficacy. J Ningbo Univer. 2019;41(01):13–19.
60. Keren H, O’Callaghan G, Vidal-Ribas P, et al. Reward processing in depression: a conceptual and meta-analytic review across fMRI and EEG studies. AJP. 2018;175(11):1111–1120. doi:10.1176/appi.ajp.2018.17101124
61. Zou L, Wu X, Tao S, et al. Functional connectivity between the parahippocampal gyrus and the middle temporal gyrus moderates the relationship between problematic mobile phone use and depressive symptoms: evidence from a longitudinal study. J Behav Addict. 2022;11(1):40–48. doi:10.1556/2006.2021.00090
62. Hou J, Zhu Y, Fang X. Smartphone addiction and depression: the multiple mediating roles of social anxiety and negative emotional information attention bias. J Psychol. 2021;53(4):362.
63. Choi HS, Lee HK, Ha JC. The influence of smartphone addiction on mental health, campus life and personal relations-Focusing on K university students. J Korean Data Inform Sci Soc. 2012;23(5):1005–1015. doi:10.7465/jkdi.2012.23.5.1005
64. Harvey AG. A cognitive model of insomnia. Behav Res Ther. 2002;40(8):869–893. doi:10.1016/S0005-7967(01)00061-4
65. Kaya F, Bostanci Daştan N, Durar E. Smart phone usage, sleep quality and depression in university students. Int J Soc Psychiatry. 2021;67(5):407–414. doi:10.1177/0020764020960207
66. Carter B, Rees P, Hale L, Bhattacharjee D, Paradkar MS. Association between portable screen-based media device access or use and sleep outcomes: a systematic review and meta-analysis. JAMA Pediat. 2016;170(12):1202–1208. doi:10.1001/jamapediatrics.2016.2341
67. Brautsch LA, Lund L, Andersen MM, Jennum PJ, Folker AP, Andersen S. Digital media use and sleep in late adolescence and young adulthood: a systematic review. Sleep Med Rev. 2023;68:101742. doi:10.1016/j.smrv.2022.101742
68. Zhang MX, Wu AMS. Effects of smartphone addiction on sleep quality among Chinese university students: the mediating role of self-regulation and bedtime procrastination. Addict Behav. 2020;111:106552. doi:10.1016/j.addbeh.2020.106552
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Evidence-Based Nursing Intervention Decreases Anxiety, Depression, Sleep Quality and Somatic Symptoms of Patients with Acute Ischemic Stroke
Gao WJ, Bao WJ, Sun SJ
Neuropsychiatric Disease and Treatment 2022, 18:2443-2451
Published Date: 25 October 2022
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W
Nature and Science of Sleep 2023, 15:407-421
Published Date: 26 May 2023
Modulatory Effects of XIAOPI Formula on CXCL1 and Selected Outcomes in Triple-Negative Breast Cancer: A Randomized Controlled Clinical Trial
Guo L, Hong SC, Wang X, Wang SQ, Wang N, Wei XQ, Situ HL, Wang ZY
Breast Cancer: Targets and Therapy 2024, 16:289-303
Published Date: 31 May 2024
Innovative Analysis of the Interconnected Network Structure Between Anxiety and Sleep Quality Among College Students
He Y, Yang T, Guo Q, Wu S, Liu W, Xu T
Psychology Research and Behavior Management 2025, 18:607-618
Published Date: 13 March 2025
Sleep Quality and Its Predictors Among Pregnant Women in Jordan: A Cross-Sectional Study
Alasmer Z, Nazzal MS, Mohamed Z, Al-Jaber A, Ali R, Alshar F, Ababneh EM, Alshdaifat E, Kanaan SF
International Journal of Women's Health 2025, 17:1285-1296
Published Date: 7 May 2025