Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Associations of Glycemic Control with Cognitive Flexibility and Mental Health-Related Quality of Life in Type 2 Diabetes
Authors Bulguroglu M, Bulguroglu HI ![]() , Hepsen S, Dincer S, Gevrek Aslan C
, Hepsen S, Dincer S, Gevrek Aslan C ![]() , Zorlu Develik S, Suicmez S
, Zorlu Develik S, Suicmez S ![]() , Adiguzel E
, Adiguzel E
Received 8 September 2025
Accepted for publication 10 February 2026
Published 19 February 2026 Volume 2026:19 565976
DOI https://doi.org/10.2147/DMSO.S565976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Merve Bulguroglu,1 Halil Ibrahim Bulguroglu,1 Sema Hepsen,2 Sezen Dincer,1 Cansu Gevrek Aslan,1 Serenay Zorlu Develik,1 Selcan Suicmez,1 Emre Adiguzel3
1Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Ankara Medipol University, Ankara, Turkey; 2Department of Endocrinology and Metabolism, Ankara Etlik City Hospital, Ankara, Turkey; 3Ankara Bilkent City Hospital, Physical Medicine and Rehabilitation Hospital, Ankara, Turkey
Correspondence: Halil Ibrahim Bulguroglu, Faculty of Health Science, Department of Physiotherapy and Rehabilitation, Ankara Medipol University, Ankara, 06050, Turkey, Tel +90 507 305 46 56, Email [email protected]
Purpose: Cognitive flexibility, a core executive function, enables individuals to adapt to the behavioral demands of chronic disease management. Poor glycemic control, indicated by elevated glycated hemoglobin (HbA1c), may impair cognition, adherence, and quality of life in type 2 diabetes mellitus (T2DM). This study examined associations between glycemic control, cognitive flexibility, and HRQoL.
Methods: This cross-sectional study included 268 adults with T2DM recruited from a tertiary endocrinology clinic between March and September 2024. Eligible participants had been diagnosed within the past 10 years and maintained a stable regimen across their two most recent HbA1c assessments. Exclusion criteria included major comorbidities, psychiatric or neurological treatment, and pregnancy. HbA1c values were obtained from medical records. Cognitive flexibility was assessed using the Cognitive Flexibility Inventory (CFI), and health-related quality of life with the 12-Item Short Form Survey (SF-12). Group comparisons (adequate vs poor glycemic control), Pearson’s correlations and multiple linear regression analyses adjusting for potential confounders were conducted using IBM SPSS Statistics. An a priori power analysis was performed using G*Power, confirming a sufficient sample size (power = 0.91).
Results: Of the 268 participants, 55.9% had poor glycemic control (HbA1c ≥ 7%). Compared with adequate control, those with poor control scored lower on CFI-Alternatives (p = 0.017, d = 0.51) and SF-12 mental component summary (p = 0.023, d = 0.56). Smaller but significant differences were found for CFI-Total (p = 0.037, d = 0.33) and SF-12 physical component summary (p = 0.042, d = 0.21). HbA1c correlated inversely with CFI-Alternatives (r = – 0.228, p = 0.035), CFI-Total (r = – 0.208, p = 0.038), and MCS-12 (r = – 0.247, p = 0.022). These associations were clinically meaningful and remained significant in multiple linear regression analyses.
Conclusion: Poor glycemic control is associated with reduced cognitive flexibility and impaired HRQoL, particularly in the mental domain, among individuals with T2DM. The role of cognitive flexibility in treatment adherence warrants further investigation.
Keywords: type 2 diabetes, HbA1c, cognitive flexibility, executive function, health-related quality of life
Introduction
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder characterized by impaired insulin secretion and/or insulin resistance, leading to disturbances in carbohydrate, lipid, and protein metabolism.1 Glycated hemoglobin (HbA1c) is widely used as a biomarker for diagnosing diabetes, monitoring long-term glycemic control, and predicting complications.2 According to current clinical guidelines, HbA1c values below 5.7% indicate normoglycemia, values between 5.7–6.4% define prediabetes, and levels ≥6.5% confirm diabetes.3
Type 2 diabetes mellitus represents a major global public health challenge, with a steadily increasing global prevalence, according to the American Diabetes Association Standards of Care.3 The association between T2DM and cognitive dysfunction is well established. Recent systematic reviews show that diabetes increases the risk of cognitive decline not only in older adults but also across the lifespan.4,5 Cognitive impairments in domains such as memory, attention, and particularly cognitive flexibility may significantly hinder self-management and treatment adherence in individuals with T2DM,6,7 thereby posing challenges for patient-centered care.
Cognitive flexibility, an executive function regulated by the prefrontal cortex, refers to the ability to shift strategies, adapt to novel situations, and generate alternative solutions.8 Neuroimaging studies have identified structural and functional alterations in the prefrontal cortex of patients with T2DM, providing a neurological basis for these deficits.9 Hyperglycemia has also been linked to neuroinflammation, microvascular dysfunction, and impaired prefrontal activity—mechanisms that may compromise executive functioning and reduce patients’ capacity for adaptive disease management.10 Because diabetes care requires continuous behavioral adjustment—including medication adherence, dietary regulation, glucose monitoring, and physical activity—deficits in cognitive flexibility may impair patients’ ability to process disease-related information, adapt to fluctuating glycemic conditions, and adhere to complex treatment regimens, ultimately worsening outcomes and health-related quality of life (HRQoL).11,12
HRQoL encompasses physical, psychological, and social well-being. Poor glycemic control has consistently been associated with reduced HRQoL, particularly in the mental domain.13 However, studies on the relationship between HbA1c and HRQoL have yielded inconsistent findings,14–16 underscoring the need to explore psychosocial moderators—such as executive function—that may influence this association.
Despite extensive research on glycemic regulation, cognitive function, and HRQoL, to our knowledge, few studies have directly investigated cognitive flexibility, a specific executive function, in relation to patient-reported outcomes. This gap limits our understanding of how modifiable cognitive processes may mediate the link between glycemic control and HRQoL in T2DM.
Given the central role of cognitive flexibility in behavioral and psychosocial adaptation, and the lack of consensus in prior findings on HbA1c and HRQoL, the present study aimed to examine these associations in adults with T2DM. Previous studies have reported associations between poor glycemic control and reduced health-related quality of life in individuals with type 2 diabetes.13–15 Accordingly, we hypothesized that higher HbA1c levels would be associated with lower cognitive flexibility and poorer HRQoL, highlighting the importance of integrative care approaches that address both cognitive and metabolic factors in diabetes management.
Materials and Methods
Study Population and Design
This cross-sectional study included 268 adults with T2DM who received outpatient care at the Endocrinology Clinic of Ankara Etlik City Hospital between March and September 2024. The study was guided by a self-regulation and executive function framework, which posits that cognitive flexibility facilitates adaptive behavior and treatment adherence in chronic disease management. Eligible participants had a diagnosis of T2DM within the past 10 years and had maintained a stable treatment regimen during their two most recent HbA1c measurements. To ensure sample homogeneity, we excluded individuals with major comorbidities (eg, renal or vascular disease), those receiving psychiatric or neurological treatment, individuals with severe sensory impairments, and pregnant women, as these conditions may independently affect cognitive performance and health-related quality of life. Participants were identified through electronic health records and approached consecutively during routine visits. The study protocol was approved by the Ankara Medipol University Ethics Committee (Decision No: 020, Date: 28/02/2024). Written informed consent was obtained from all participants in accordance with the Declaration of Helsinki.
Sample Size Determination
A priori power analysis was conducted using G*Power version 3.1. Assuming a medium effect size for correlations (r = 0.30), α = 0.05, and power = 0.80, the required sample size was 228. With 268 participants, the achieved power was 0.91, indicating sufficient sensitivity to detect meaningful associations.
Clinical and Demographic Data Collection
Medication use and HbA1c values were extracted from medical records. Glycemic control was classified as adequate (HbA1c < 7.0%) or poor (HbA1c ≥ 7.0%) in line with international guidelines.3 The thresholds of 5.7% for normoglycemia, 5.7–6.4% for prediabetes, and ≥6.5% for diabetes represent diagnostic criteria, whereas the 7% cut-off reflects a clinically relevant management target.3 Demographic and lifestyle data—including age, sex, body mass index (BMI), diabetes duration, education, diet, and physical activity—were obtained using a structured self-report questionnaire administered by trained researchers. Diet and physical activity were assessed using standardized yes/no questions regarding adherence to a healthy diet and regular exercise.
Assessment of Cognitive Flexibility
Cognitive flexibility was assessed using the Cognitive Flexibility Inventory (CFI), a validated 20-item self-report measure by Dennis and Vander Wal.17 It comprises two subscales: Alternatives (13 items), assessing the ability to generate multiple strategies, and Control (7 items), reflecting perceived control over difficult situations. Items were rated on a 5-point Likert scale (1 = “strongly disagree” to 5 = “strongly agree”), with higher scores indicating greater flexibility. The validated Turkish version (Gülüm & Dağ)18 was employed, which shows excellent psychometric properties. Internal consistency in this study was high (α = 0.86 for Alternatives, 0.88 for Control, 0.92 total).
Assessment of Health-Related Quality of Life (HRQoL)
Health-related quality of life was measured with the 12-Item Short Form Health Survey (SF-12),19 which yields two composite scores: Physical Component Summary (PCS-12) and Mental Component Summary (MCS-12). The Turkish version (Soylu & Kütük)20 has demonstrated reliability. In this study, Cronbach’s alpha was 0.81 for PCS-12 and 0.79 for MCS-12. Higher scores reflected better HRQoL.
Survey Administration
The survey battery (CFI, SF-12, demographics) was self-administered on paper in a quiet room adjacent to the clinic and required 15–20 minutes. A trained research assistant was present to provide clarification if needed.
Statistical Analysis
Analyses were performed using IBM SPSS version 22.0. Normality was assessed by visual inspection and Kolmogorov–Smirnov/Shapiro–Wilk tests. Descriptive statistics were presented as means ± SD for continuous variables and frequencies (%) for categorical variables. Group comparisons (adequate vs poor glycemic control) were conducted with independent-samples t-tests. Pearson’s correlations examined associations between HbA1c, cognitive flexibility, and HRQoL. Effect sizes followed Cohen’s criteria: small (r ≥ 0.10, d ≥ 0.20), medium (r ≥ 0.30, d ≥ 0.50), and large (r ≥ 0.50, d ≥ 0.80).21 A two-tailed p < 0.05 was considered significant. Missing data was minimal (<5%) and did not materially affect results. Additionally, multiple linear regression analyses controlled for age, sex, BMI, diabetes duration, and education. Multicollinearity diagnostics confirmed all variance inflation factors and tolerance values were within acceptable limits.
Results
Of the 310 patients approached, 268 agreed to participate, yielding a response rate of 86.5%. The descriptive characteristics of the study sample are presented in Table 1. The mean HbA1c level was 8.91 ± 2.19%. The average total score on the CFI was 63.26 ± 19.59, with subscale scores of 40.23 ± 12.20 for Alternatives and 23.03 ± 8.25 for Control. The mean scores for the SF-12 composite measures were 37.26 ± 10.10 for PCS-12 and 37.30 ± 10.58 for MCS-12 (Table 2).
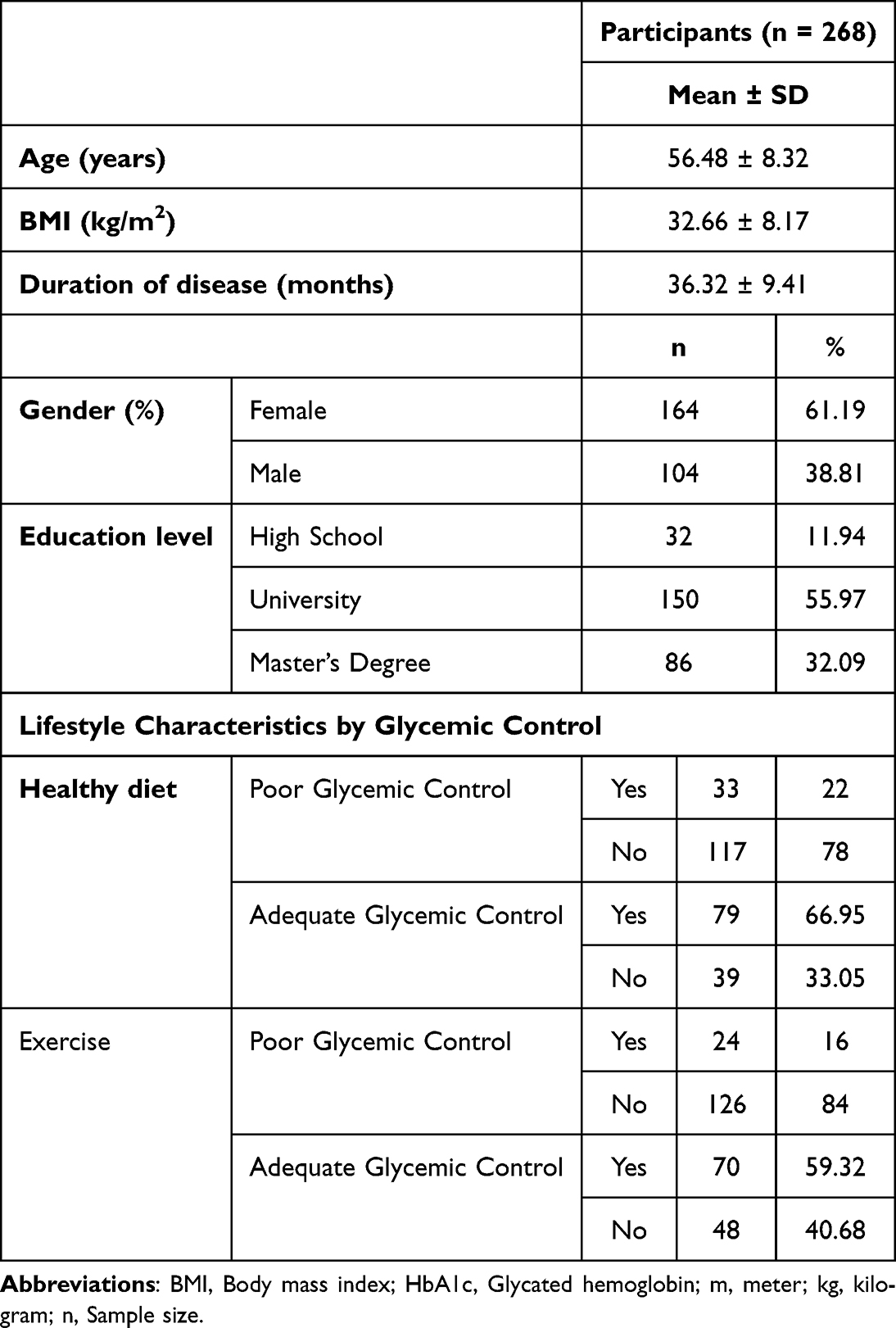 |
Table 1 Demographic, Clinical, and Lifestyle Characteristics of Participants by Glycemic Control |
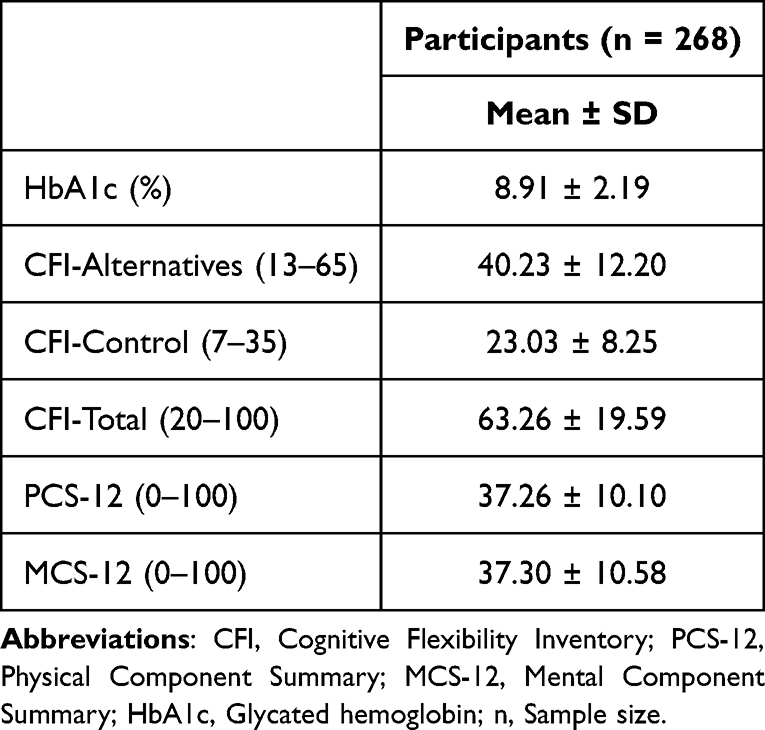 |
Table 2 Cognitive Flexibility, Quality of Life, and HbA1c Scores |
Based on HbA1c thresholds, 150 participants (55.95%) were classified as having poor glycemic control (HbA1c ≥ 7%), while 118 (44.05%) demonstrated adequate control (HbA1c < 7%) (Table 3). Higher HbA1c (%) levels were associated with lower cognitive flexibility scores and poorer health-related quality of life. Pearson’s correlation analysis revealed statistically significant negative correlations between HbA1c (%) levels and CFI-Alternatives (r = –0.228, p = 0.035), CFI-Total (r = –0.208, p = 0.038), and MCS-12 (r = –0.247, p = 0.022). No significant correlations were observed between HbA1c and either CFI-Control or PCS-12 (Table 4).
 |
Table 3 Glycemic Control Status of Participants |
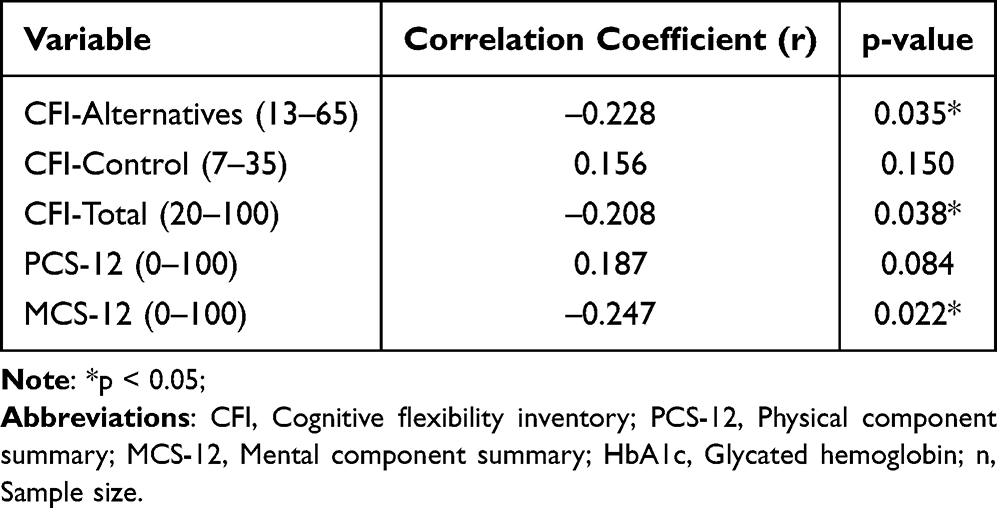 |
Table 4 Correlation Between HbA1c and Cognitive Flexibility and Quality of Life (n = 268) |
Group comparisons revealed significant differences. Participants with adequate control scored higher on CFI-Alternatives (p = 0.017, d = 0.51) and MCS-12 (p = 0.023, d = 0.56), both reflecting moderate effect sizes. These findings indicate that adequate glycemic control is associated with better cognitive flexibility and mental health-related quality of life. Additional significant differences, with small effect sizes, were observed in CFI-Total (p = 0.037, d = 0.33) and PCS-12 (p = 0.042, d = 0.21) (Table 5). In multiple linear regression analyses adjusting for age, sex, BMI, diabetes duration, and education, higher HbA1c (%) remained independently associated with lower cognitive flexibility (CFI-Alternatives) and poorer mental health-related quality of life (MCS-12). (Table 6).
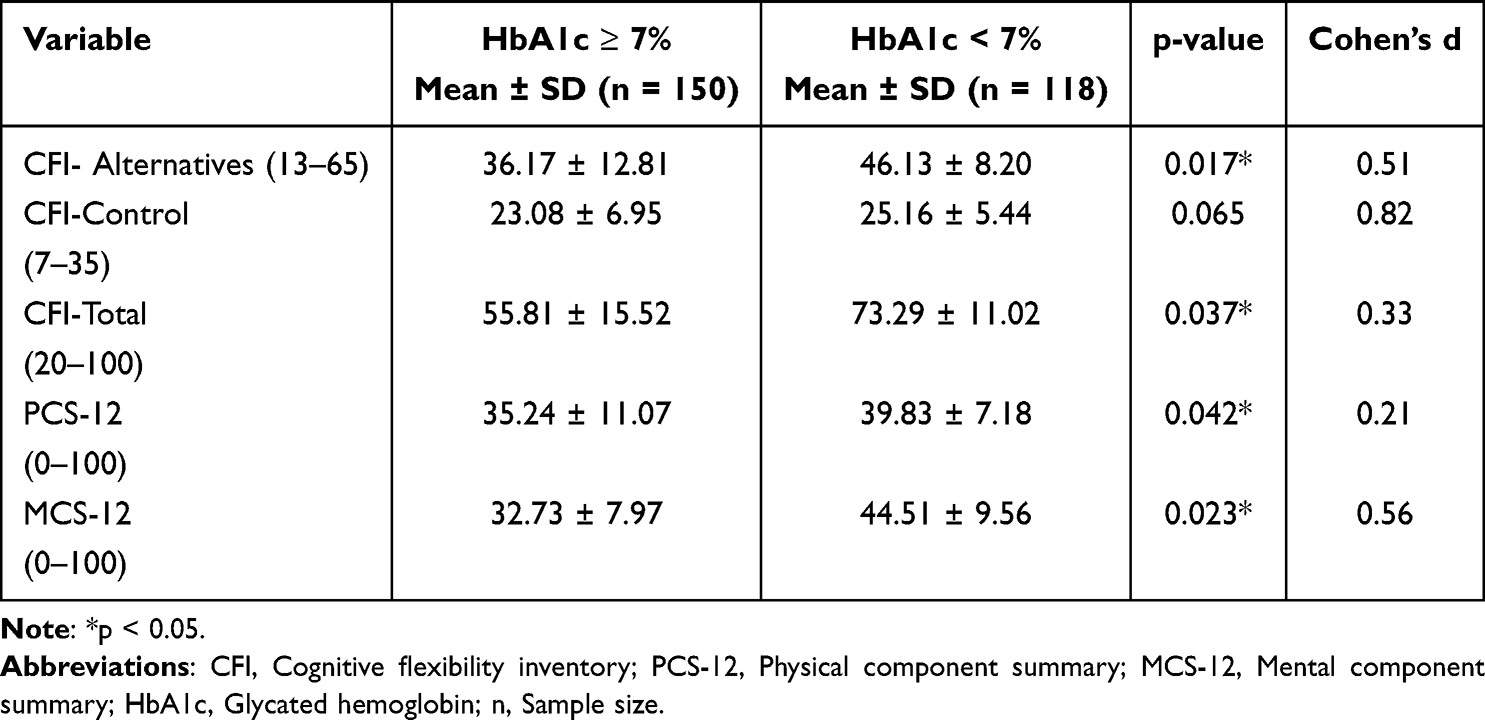 |
Table 5 Comparison of Cognitive Flexibility and Quality of Life Scores by Glycemic Control |
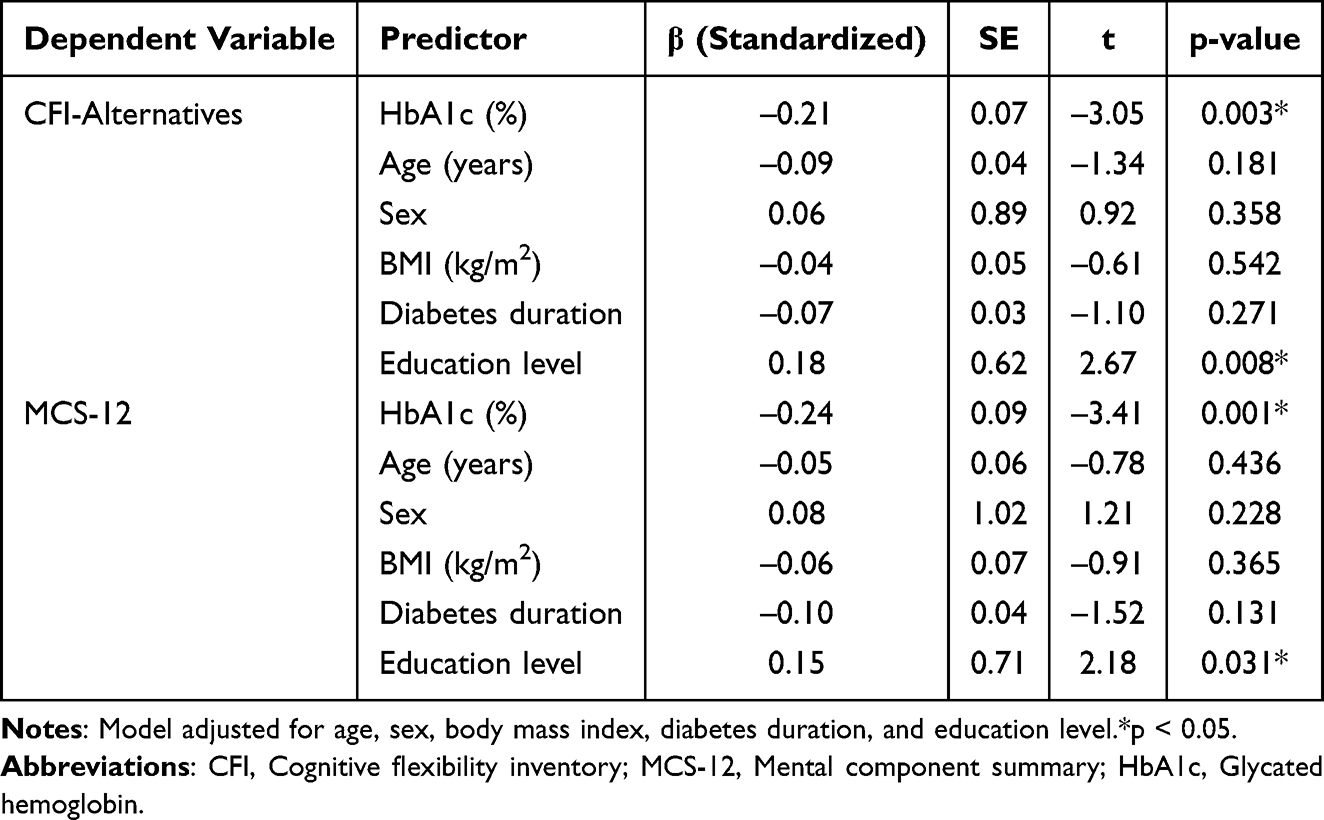 |
Table 6 Multiple Linear Regression Analyses Examining Associations of HbA1c (%) with Cognitive Flexibility and Mental Health-Related Quality of Life |
Discussion
This study shows that higher HbA1c levels in adults with T2DM are associated with lower cognitive flexibility and poorer HRQoL, with the most consistent signal in the mental domain (MCS-12). Although the CFI does not have a validated clinical cut-off, participants’ average scores were below those reported in healthy samples,17,18,22 supporting the presence of meaningful executive-function vulnerabilities in this population.
Existing work on cognitive flexibility in T2DM is limited;23–25 however, our findings are consistent with evidence linking chronic hyperglycemia to executive dysfunction, particularly in domains related to cognitive control and adaptive functioning.26 In line with reports that glycemic variability contributes to cognitive decline,27 HbA1c correlated inversely with CFI indices, most notably the Alternatives subscale—an index of generating multiple problem-solving strategies. Participants with adequate glycemic control performed better on these indices, suggesting that more favorable metabolic regulation may help preserve executive resources relevant to daily self-management.
Beyond lifestyle measures, emerging pharmacological options such as GLP-1 receptor agonists may improve glycemic control and could plausibly yield downstream cognitive benefits,28 while structured exercise programs have been shown to enhance executive function and modestly reduce HbA1c.29,30 Taken together, these data underscore the value of multidisciplinary strategies that target both metabolic and cognitive outcomes.
Importantly, associations between HbA1c, cognitive flexibility, and HRQoL remained materially unchanged after adjustment for age, sex, BMI, diabetes duration, and education, indicating that the observed relationships were not explained by these covariates. The lack of association between HbA1c and the CFI-Control subscale may reflect its broader appraisal of coping, which is likely influenced by mood and stress; the absence of mood measures in the present study limits inferences on this pathway. Higher Alternatives scores in the adequately controlled group may partly mirror healthier behaviors (diet, physical activity) and educational advantages that support cognitive resilience.
With respect to HRQoL, HbA1c related inversely to MCS-12 but not PCS-12. This pattern could reflect low habitual physical activity and higher BMI in our cohort, factors known to weigh more heavily on physical functioning.31 While between-group differences in PCS-12 achieved statistical significance, the effect size was small; these findings should be interpreted cautiously and confirmed in larger, more physically active samples.
Clinically, our results suggest that brief screening for executive dysfunction may help identify patients at risk of suboptimal engagement, enabling tailored education and adherence-support interventions.32 Integrating cognitive-behavioral strategies with diabetes education and exercise programming may improve both self-management behaviors and psychosocial well-being.
Finally, given the complex, lifelong demands of T2DM, care models that integrate metabolic management with cognitive and psychosocial support are likely to be most effective. Dietary strategies (eg, Mediterranean or ketogenic approaches) and modern pharmacotherapies, including glucagon-like peptide-1 receptor agonists (eg, semaglutide, liraglutide) and sodium–glucose cotransporter-2 inhibitors (eg, empagliflozin), have been shown to improve glycemic control and confer cardiometabolic benefits,33,34 reinforcing the rationale for comprehensive, patient-centered care.
Strengths and Limitations
Key strengths include the use of validated instruments, stratified analyses by glycemic control, preregistered power considerations with adequate sample size, and multivariable adjustment for relevant covariates. Nonetheless, several limitations merit consideration. First, the cross-sectional design precludes causal inference; temporal sequencing should be tested prospectively. Second, the single-center setting may limit generalizability; replication across multiple sites with broader cultural and socioeconomic diversity is warranted. Third, cognitive flexibility was assessed via self-report rather than performance-based neuropsychological tasks, introducing potential response bias; future work should combine both modalities. Fourth, mood and diabetes-distress measures were not collected, constraining insight into affective pathways that likely influence both cognition and adherence. Finally, despite adjusting for major covariates, residual confounding cannot be excluded.
Future Directions
Prospective and interventional studies should test whether enhancing cognitive flexibility—through targeted cognitive training, structured education, cognitive-behavioral therapy, and exercise—produces sustained improvements in HbA1c, adherence behaviors, and HRQoL. Incorporating performance-based executive-function tests alongside self-report measures, assessing mood/diabetes distress, and sampling diverse, multi-center cohorts will clarify mechanisms and improve external validity. Trials that integrate lifestyle and pharmacologic optimization with cognitive-focused behavioral components may be especially informative for real-world diabetes care.
Conclusion
Poor glycemic control in adults with T2DM was associated with reduced cognitive flexibility and impaired mental health-related quality of life. These findings identify cognitive flexibility as a potentially modifiable factor that may play a role in diabetes self-management and patient engagement. Incorporating cognitive and psychosocial assessments into routine diabetes care may help clinicians personalize education and optimize outcomes. Further studies are needed to clarify the role of cognitive flexibility in treatment adherence and long-term disease management.
Abbreviations
HbA1c, Glycated hemoglobin; T2DM, Type 2 diabetes mellitus; HRQoL, Health-related quality of life; CFI, Cognitive flexibility inventory; SF-12, 12-item short-form health survey; MCS-12, SF-12 mental component summary; PCS-12, SF-12 physical component summary; BMI, Body mass index.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available to preserve participant confidentiality but are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Ethical approval for this study was obtained from the Non-Interventional Clinical Research Ethics Committee of Ankara Medipol University approval (Date: 28/02/2024—Decision No: 020). The principles of the Declaration of Helsinki performed this study. Written informed consent was obtained from all participants before the study.
Author Contributions
Conceptualization: MB, HIB, SH, EA, SZD, SS; Methodology: MB, HIB, SZD, SS; Formal analysis: CGA; Investigation: SD, SZD, SS; Resources: SH, EA; Supervision: MB, HIB, EA; Writing-original draft preparation: MB, HIB; Writing-review and editing: MB, HIB, SH, EA, SZD, SS, CGA, SD; All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gieroba B, Kryska A, Sroka-Bartnicka A. Type 2 diabetes mellitus - conventional therapies and future perspectives in innovative treatment. Biochem Biophys Rep. 2025;42:102037. doi:10.1016/j.bbrep.2025.102037
2. Sherwani SI, Khan HA, Ekhzaimy A, Masood A, Sakharkar MK. Significance of HbA1c test in diagnosis and prognosis of diabetic patients. Biomark Insights. 2016;11:95–9. doi:10.4137/BMI.S38440
3. American Diabetes Association Professional Practice Committee. 2. Diagnosis and classification of diabetes: standards of care in diabetes-2025. Diabetes Care. 2025;48(1 Suppl 1)S27–S49. doi:10.2337/dc25-S002
4. Kan W, Qu M, Wang Y, Zhang X, Xu L. A review of type 2 diabetes mellitus and cognitive impairment. Front Endocrinol. 2025;16:1624472. doi:10.3389/fendo.2025.1624472
5. Xie K, Perna L, Schöttker B, Kliegel M, Brenner H, Mons U. Type 2 diabetes mellitus and cognitive decline in older adults in Germany - results from a population-based cohort. BMC Geriatr. 2022;22(1):455. doi:10.1186/s12877-022-03151-y
6. Vlachou E, Ntikoudi A, Owens DA, Nikolakopoulou M, Chalimourdas T, Cauli O. Effectiveness of cognitive behavioral therapy-based interventions on psychological symptoms in adults with type 2 diabetes mellitus: an update review of randomized controlled trials. J Diabetes Complications. 2022;36(5):108185. doi:10.1016/j.jdiacomp.2022.108185
7. Świątoniowska-lonc N, Polański J, Tański W, Jankowska-Polańska B. Impact of cognitive impairment on adherence to treatment and self-care in patients with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2021;14:193–203. doi:10.2147/DMSO.S284468
8. Friedman NP, Robbins TW. The role of prefrontal cortex in cognitive control and executive function. Neuropsychopharmacology. 2022;47(1):72–89. doi:10.1038/s41386-021-01132-0
9. Lei H, Hu R, Luo G, et al. Altered structural and functional MRI connectivity in type 2 diabetes mellitus related cognitive impairment: a review. Front Hum Neurosci. 2022;15:755017. doi:10.3389/fnhum.2021.755017
10. Rom S, Zuluaga-Ramirez V, Gajghate S, et al. Hyperglycemia-Driven neuroinflammation compromises BBB leading to memory loss in both Diabetes Mellitus (DM) type 1 and type 2 mouse models. Mol Neurobiol. 2019;56(3):1883–1896. doi:10.1007/s12035-018-1195-5
11. American Diabetes Association Professional Practice Committee. 5. Facilitating positive health behaviors and well-being to improve health outcomes: standards of care in diabetes-2024. Diabetes Care. 2024;47(Suppl 1)S77–S110. doi:10.2337/dc24-S005
12. Schwartz SS, Herman ME, Tun MTH, et al. The double life of glucose metabolism: brain health, glycemic homeostasis, and your patients with type 2 diabetes. BMC Med. 2024;22(1):582. doi:10.1186/s12916-024-03763-8
13. Teli M, Thato R, Rias YA. Predicting factors of health-related quality of life among adults with type 2 diabetes: a systematic review. SAGE Open Nurs. 2023;9:23779608231185921. doi:10.1177/23779608231185921
14. Svedbo Engström M, Leksell J, Johansson UB, et al. Health-related quality of life and glycaemic control among adults with type 1 and type 2 diabetes - a nationwide cross-sectional study. Health Qual Life Outcomes. 2019;17(1):141. DOI:10.1186/s12955-019-1212-z
15. Imai D, Ushigome E, Sakai R, et al. Association between variation in hemoglobin A1c levels and diabetes therapy-related quality of life in patients with diabetes. J Diabetes Investig. 2024;15(8):1042–1046. DOI:10.1111/jdi.14218
16. Alshayban D, Joseph R. Health-related quality of life among patients with type 2 diabetes mellitus in Eastern Province, Saudi Arabia: a cross-sectional study. PLoS One. 2020;15(1):e0227573. doi:10.1371/journal.pone.0227573
17. Dennis JP, Vander Wal JS. The cognitive flexibility inventory: instrument development and estimates of reliability and validity. Cogn Ther Res. 2010;34:241–253. doi:10.1007/s10608-009-9276-4
18. Gülüm IV, Dağ I. The Turkish adaptation of the cognitive flexibility inventory: the study of validity and reliability. Clin Psychiatry. 2012;15(2):123–131.
19. Ware JJ, Kosinski M, Keller SD. A 12-Item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
20. Soylu C, Kütük B. Reliability and validity of the Turkish version of SF-12 health survey. Turk Psikiyatri Derg. 2022;33(2):108–117. doi:10.5080/u25700
21. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
22. Sapmaz F, Doğan T. Assessment of cognitive flexibility: reliability and validity studies of Turkish version of the Cognitive Flexibility Inventory. Ankara Univ J Fac Educ Sci. 2013;46(1):143–162. doi:10.1501/Egifak_0000001278
23. Aderinto N, Olatunji G, Abdulbasit M, et al. The impact of diabetes in cognitive impairment: a review of current evidence and prospects for future investigations. Medicine. 2023;102(43):e35557. DOI:10.1097/MD.0000000000035557
24. van den Berg E, Reijmer YD, de Bresser J, et al. A 4 year follow-up study of cognitive functioning in patients with type 2 diabetes mellitus. Diabetologia. 2010;53(1):58–65. DOI:10.1007/s00125-009-1571-9
25. Amin SN, El-Akabawy G, Abuqasem MA, et al. Assessment of cognitive flexibility in jordanian diabetic patients by wisconsin card sorting and trail making tests: implications with demographic, anthropometric and therapeutic variables. Diabetes Metab Syndr Obes. 2024;17:2655–2670. doi:10.2147/DMSO.S457799
26. Choe A, Fredericks EM, Albright D, et al. Executive functioning, diabetes distress, and diabetes management among adolescents with type 1 diabetes: youth and parent perspectives. Pediatr Diabetes. 2025;2025:7036544. doi:10.1155/pedi/7036544
27. Ding J, Shi Q, Tao Q, et al. Correlation between long-term glycemic variability and cognitive function in middle-aged and elderly patients with type 2 diabetes mellitus: a retrospective study. Peer J. 2023;11:e16698. doi:10.7717/peerj.16698
28. Chuansangeam M, Phadungsaksawasdi P, Park HJ, Yang YH. Exploring the link between GLP-1 receptor agonists and dementia: a comprehensive review. J Alzheimers Dis Rep. 2025;9:25424823251342182. doi:10.1177/25424823251342182
29. Cai YH, Wang Z, Feng LY, Ni GX. Effect of exercise on the cognitive function of older patients with type 2 diabetes mellitus: a systematic review and meta-analysis. Front Hum Neurosci. 2022;16:876935. doi:10.3389/fnhum.2022.876935
30. Zhao RR, O’Sullivan AJ, Fiatarone Singh MA. Exercise or physical activity and cognitive function in adults with type 2 diabetes, insulin resistance or impaired glucose tolerance: a systematic review. Eur Rev Aging Phys Act. 2018;15:1. doi:10.1186/s11556-018-0190-1
31. Sabag A, Chang CR, Francois ME, et al. The effect of exercise on quality of life in type 2 diabetes: a systematic review and meta-analysis. Med Sci Sports Exerc. 2023;55(8):1353–1365. doi:10.1249/MSS.0000000000003172
32. Zullig LL, Gellad WF, Moaddeb J, et al. Improving diabetes medication adherence: successful, scalable interventions. Patient Prefer Adherence. 2015;9:139–149. doi:10.2147/PPA.S69651
33. Alzahrani M, Rammal L, Felemban R, et al. Effects of semaglutide on glycemic control and body weight in patients with type 2 diabetes: a retrospective cohort study in a primary care setting. Cureus. 2025;17(4):e82123. DOI:10.7759/cureus.82123
34. Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–2786. doi:10.2337/dci22-0034
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment-Related Attributes of Diabetes Therapies and How People with Type 2 Diabetes Report Their Impact on Indicators of Medication-Taking Behaviors
Sims TJ, Boye KS, Robinson S, Kennedy-Martin T
Patient Preference and Adherence 2022, 16:1919-1939
Published Date: 4 August 2022
Data-Driven Identification of Long-Term Glycemia Clusters and Their Individualized Predictors in Finnish Patients with Type 2 Diabetes
Lavikainen P, Chandra G, Siirtola P, Tamminen S, Ihalapathirana AT, Röning J, Laatikainen T, Martikainen J
Clinical Epidemiology 2023, 15:13-29
Published Date: 5 January 2023
A Patient-Centered Self-Management Intervention to Improve Glycemic Control, Self-Efficacy and Self-Care Behaviors in Adults with Type 2 Diabetes Mellitus: A SPIRIT Compliant Study Protocol for Randomized Controlled Trial
Asmat K, Dhamani K, Froelicher ES, Gul R
Diabetes, Metabolic Syndrome and Obesity 2023, 16:225-236
Published Date: 26 January 2023
Comparison of Efficacy and Adherence of Patient-Preferred (1 Unit Daily) and ADA/EASD Guideline-Recommended (2 Units Every 3 Days) Basal Insulin Titration Algorithms: Multicenter, Randomized, Clinical Study
Li L, Zhang X, Zhang T, Zeng L, Lin M, Li Y, Li W
Patient Preference and Adherence 2024, 18:687-694
Published Date: 18 March 2024
Normoglycemia and Weight Reduction: Perspectives of People with Type 2 Diabetes in Australia
Newson RS, Barraclough H, Lapthorn J, Stewart M, Colman S, D’Emden M
Patient Preference and Adherence 2025, 19:897-905
Published Date: 4 April 2025