Back to Journals » International Journal of General Medicine » Volume 18
Associations Between Sleep Quality, Anxiety, Depression, and Gastroesophageal Reflux Disease in a Tertiary Hospital Sleep Center: A Retrospective Study
Authors Hsieh MT, Kuo HY, Lin SH, Chang WL, Lin CY
Received 16 July 2025
Accepted for publication 11 October 2025
Published 28 October 2025 Volume 2025:18 Pages 6533—6542
DOI https://doi.org/10.2147/IJGM.S554279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Ming-Tsung Hsieh,1 Hsin-Yu Kuo,1,2 Sheng-Hsiang Lin,3 Wei-Lun Chang,1 Cheng-Yu Lin4,5
1Department of Internal Medicine, National Cheng Kung University Hospital, Tainan, Taiwan; 2Institute of Clinical Medicine, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 3Biostatistics Consulting Center, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 4Department of Otolaryngology, National Cheng Kung University Hospital, Tainan, Taiwan; 5Sleep Medicine Center, National Cheng Kung University Hospital, Tainan, Taiwan
Correspondence: Cheng-Yu Lin, Department of Otolaryngology, National Cheng Kung University Hospital, No. 138, Sheng Li Road, Tainan, Taiwan, Tel + 886 6 2353535 ext 5311, Email [email protected]
Background: Gastroesophageal reflux disease (GERD) often coexists with anxiety, depression, and poor sleep quality, which worsen symptom perception and reduce quality of life. While each factor has been linked to GERD, their combined effects have rarely been examined, especially in sleep clinic populations. This study aimed to assess the individual and combined associations of anxiety, depression, and sleep quality with probable GERD in patients at a tertiary hospital sleep center.
Methods: This retrospective cross-sectional study examined patient data from the Sleep Center of National Cheng Kung University Hospital collected between July 2020 and July 2021. All included patients completed the Gastroesophageal Reflux Disease Questionnaire (GERDQ), Pittsburgh Sleep Quality Index (PSQI), and Hospital Anxiety and Depression Scale (HADS). Multivariable logistic regression was used to determine associations between elevated HADS-A (anxiety), HADS-D (depression), PSQI scores, and probable GERD (GERDQ score ≥ 9), adjusting for relevant confounders.
Results: Among 877 patients, 93 (10.6%) had probable GERD. Elevated HADS-A (adjusted odds ratio [aOR]: 2.18, 95% confidence interval [CI]: 1.40– 3.39, p < 0.001), HADS-D (aOR: 2.10, 95% CI: 1.34– 3.29, p = 0.001), and PSQI (aOR: 3.32, 95% CI: 2.10– 5.27, p < 0.001) scores were significantly associated with probable GERD. Patients with both high HADS-A and PSQI scores had a stronger association (aOR: 4.74, 95% CI: 2.62– 8.60), and those with both high HADS-D and PSQI scores had the greatest odds (aOR: 5.09, 95% CI: 2.72– 9.41).
Conclusion: Results reaffirm that anxiety, depression, and poor sleep quality are significantly associated with probable GERD. However, given the cross-sectional design, causal relationships cannot be established. The combined use of HADS and PSQI may enhance GERD risk identification, suggesting that individuals with psychological and/or sleep disturbances should consider gastroenterological evaluation.
Keywords: anxiety, depression, gastroesophageal reflux disease, sleep
Introduction
Gastroesophageal reflux disease (GERD) is a prevalent chronic condition among adults, occurring when stomach contents reflux into the esophagus, and produce symptoms such as heartburn, regurgitation, and dyspepsia.1,2 GERD affects 13.3% of the population globally, including 15.4% in North America. Besides its clinical implications, GERD significantly affects patients’ quality of life and also places a significant economic burden on healthcare systems, costing an estimated $10 billion annually in the United States alone.3,4
GERD is often comorbid with psychological distress, including anxiety and depression, which may increase symptom sensitivity.5,6 Sleep disturbances are also common, forming a bidirectional relationship that can perpetuate both reflux symptoms and mental health issues.7,8 Potential pathophysiological mechanisms linking these conditions include heightened visceral hypersensitivity, altered central pain processing, and autonomic nervous system dysregulation, which may impair lower esophageal sphincter function and amplify symptom perception.9,10
The Pittsburgh Sleep Quality Index (PSQI), which is widely used to assess sleep quality, has consistently shown that patients with GERD often experience poorer sleep, which aggravates their reflux symptoms.11,12 This bidirectional relationship complicates clinical management of GERD and/or anxiety/depression and sleep disturbances because treating one condition without addressing the others may not improve the targeted condition.
Despite increasing recognition of the links between GERD, anxiety, depression, and sleep disturbances, most previous studies have examined these associations in isolation and in general population samples, with very limited research focusing on patients presenting to sleep clinics. Furthermore, few studies have investigated the potential joint effects of psychological distress and poor sleep quality on GERD, particularly using validated tools such as HADS and PSQI.13
Addressing this gap is important because identifying high-risk patients through combined psychological and sleep assessments may facilitate earlier intervention, improve GERD management, and guide integrated care in both sleep and gastroenterology settings. For example, one study demonstrated that elevated HADS and PSQI scores worsened tinnitus symptoms, suggesting that their interplay may influence other conditions as well.14 We therefore hypothesized that combined elevated HADS and PSQI scores would be more strongly associated with probable GERD than either score alone. Building on these findings, this study aimed to explore whether the combined use of HADS and PSQI scores is more strongly associated with the presence of probable GERD than either measure alone, using data from a tertiary hospital sleep center.
Methods
Study Design and Population
This retrospective cross-sectional study was conducted at the Sleep Center of National Cheng Kung University Hospital (NCKUH) in Taiwan using patient data collected from July 2020 to July 2021. Adult patients aged 18 years and older who were referred from outpatient clinics in the otolaryngology, psychiatry, pulmonology, and other departments of NCKUH who presented with sleep difficulties were eligible. Specifically, patients who had completed the Gastroesophageal Reflux Disease Questionnaire (GERDQ), PSQI, and HADS questionnaires were included. A total of 910 patients were initially identified. After excluding 33 patients with incomplete questionnaire data, 877 participants were included in the final analysis. All questionnaires were self-administered using a tablet-based electronic system at the outpatient clinic.
Ethics Statement
The study protocol was reviewed and approved by the Institutional Review Board of NCKUH (IRB number: B-ER-111-328). The study was conducted in accordance with the Declaration of Helsinki. Since patient data were analyzed retrospectively and were deidentified to protect identity, the IRB waived the need for included patients’ signed informed consent.
Characteristics of Included Patients
The following demographic and clinical variables were collected from the medical records of all included patients: age, sex, body mass index (BMI; kg/m²), sleeping systolic blood pressure (SBP; mmHg), heart rate (HR; bpm), neck circumference (cm) and waist-to-hip ratio (WHR). These variables provided a comprehensive profile of the physical characteristics and health status of all participants (Table 1).
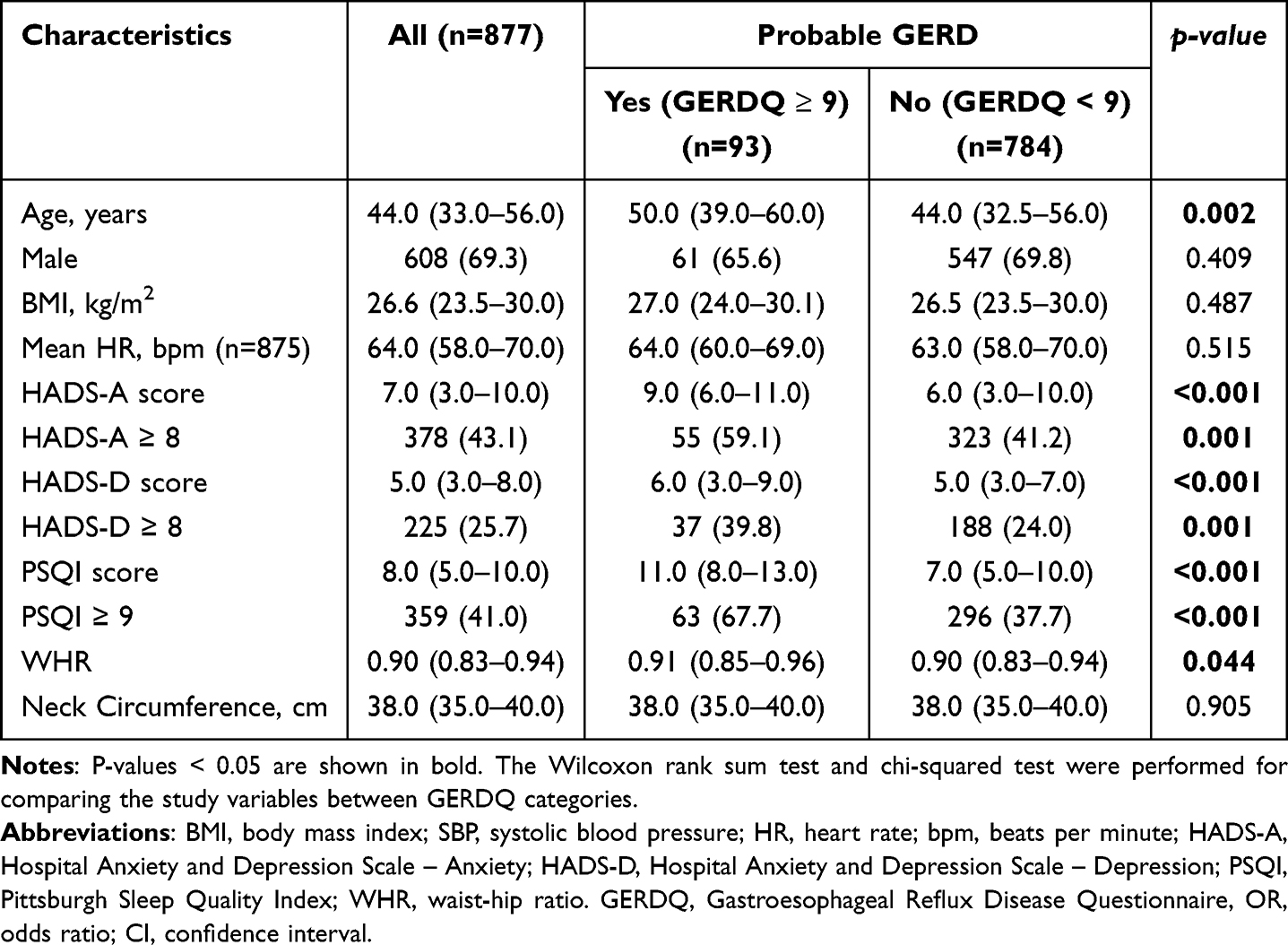 |
Table 1 Characteristics of the Study Population Stratified by Indicators of Probable GERD |
Gastroesophageal Reflux Disease Questionnaire (GERDQ)
The GERDQ is a previously validated complementary tool for diagnosing GERD in primary care settings, helping to reduce the need for upper endoscopy and improving resource utilization.14 A validated 6-item GERDQ questionnaire, as used in this study, scores each item on a scale from 0 to 3, where 0 indicates no symptoms, 1 indicates 1 day per week, 2 indicates 2–3 days per week, and 3 indicates 4–7 days per week. A total score of ≥9 was used as the cut-off for diagnosing probable GERD, as previously demonstrated.15 Previous research has shown that the GERDQ instrument has a high positive predictive value of 92% (95% confidence interval [CI]: 86–97), although its negative predictive value is relatively low (22%).15 In addition, a recent large-scale meta-analysis of 11,166 participants demonstrated that GERDQ has moderate sensitivity and specificity for GERD diagnosis.16 Given the absence of endoscopic data for patients visiting the Sleep Center, a GERDQ score of ≥9 was used in this study as a surrogate marker for GERD, referring to it as “probable GERD”, as this score does not indicate a definitive diagnosis.
Pittsburgh Sleep Quality Index (PSQI)
Sleep quality was assessed using the PSQI, which is a self-reported questionnaire used to assess sleep quality and disturbances over a single month.17 The PSQI instrument evaluates various aspects of sleep, including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleep medications, and daytime dysfunction. Nineteen items grouped into seven components are scored on a 0–3 interval scale, with global scores ranging from 0 to 21. A global score of ≥9 was used as the cut-off point to indicate poor sleep quality, as described previously.18 The PSQI has demonstrated good internal consistency (Cronbach’s α = 0.83) and validity for assessing sleep quality in both clinical and research settings.19
Hospital Anxiety and Depression Scale (HADS)
Patients’ anxiety and depression statuses were evaluated using the HADS, a 14-item questionnaire used to evaluate individual patients’ anxiety and depressive symptoms.20 Each of the 14 items is scored from 0 to 3, resulting in two global scores: one for anxiety (HADS-A) and one for depression (HADS-D). Scores of ≥8 on either scale were considered indicative of anxiety or depression symptoms, as determined previously.21 The HADS has shown high reliability (Cronbach’s α ranging from 0.80 to 0.93) and construct validity across diverse patient populations.20,22
Statistical Analysis
Continuous data are presented as medians with interquartile ranges (IQR), and categorical data as counts and percentages. To assess differences between patients with and without probable GERD (GERDQ score ≥ 9 vs < 9), categorical variables were compared using the chi-squared test, while continuous variables without normal distribution were analyzed using the Wilcoxon rank sum test. Univariate regression analysis was performed to assess associations between the study variables and the presence of probable GERD. Variables that reached statistical significance in univariate analysis were added into the multivariable models. Multivariable logistic regression analysis was performed to determine the associations between the HADS-A, HADS-D, and PSQI scores and the presence of probable GERD, presented as adjusted odds ratios (aORs) and corresponding 95% CI.
A two-tailed p-value of <0.05 was established as statistical significance, and all statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
In total, 877 patients were included in the present study (mean age 44.6 years, 69.3% males) (Table 1). A total of 93 individuals (10.6%) had probable GERD based on GERDQ scores. Those with probable GERD exhibited significantly higher proportions of HADS-A ≥ 8 (59.1% vs 41.2%, p = 0.001, OR = 2.07, 95% CI: 1.33–3.20), HADS-D ≥ 8 (39.8% vs 24.0%, p = 0.001, OR = 2.10, 95% CI: 1.34–3.27), and PSQI ≥ 9 (67.7% vs 37.7%, p < 0.001, OR = 3.46, 95% CI: 2.19–5.47). They were also older (median age: 50.0 vs 44.0 years, p = 0.002, OR = 1.02, 95% CI: 1.01–1.04) and had a slightly higher WHR (median: 0.91 vs 0.90, p = 0.044, OR = 27.70, 95% CI: 1.84–417.27) compared to those without probable GERD. No significant differences were observed between probable GERD and non-GERD groups in gender (p = 0.409, OR = 0.80, 95% CI: 0.51–1.26), BMI (p = 0.843, OR = 1.01, 95% CI: 0.97–1.05), or neck circumference (p = 0.905, OR = 1.00, 95% CI: 0.96–1.06) (Table 2).
 |
Table 2 Crude Associations Between the Study Variables and Probable GERD |
Multivariable logistic regression confirmed the independent associations between these variables and probable GERD after adjusting for relevant confounders, including age, WHR, and sleeping SBP. Anxiety (HADS-A ≥ 8) was associated with higher odds of probable GERD (adjusted OR (aOR) = 2.18, 95% CI: 1.40–3.39, p = 0.001), as was depression (HADS-D ≥ 8, aOR = 2.10, 95% CI: 1.34–3.29, p = 0.001). Poor sleep quality (PSQI ≥ 9) demonstrated the strongest independent association with probable GERD (aOR = 3.32, 95% CI: 2.10–5.27, p < 0.001). Additionally, each year of increased age was linked to a higher likelihood of probable GERD (aOR = 1.02, 95% CI: 1.00–1.03, p = 0.016 to p = 0.035, across models). No significant associations were observed between BMI, neck circumference, or gender and GERD in either univariate or multivariable analyses (Table 3).
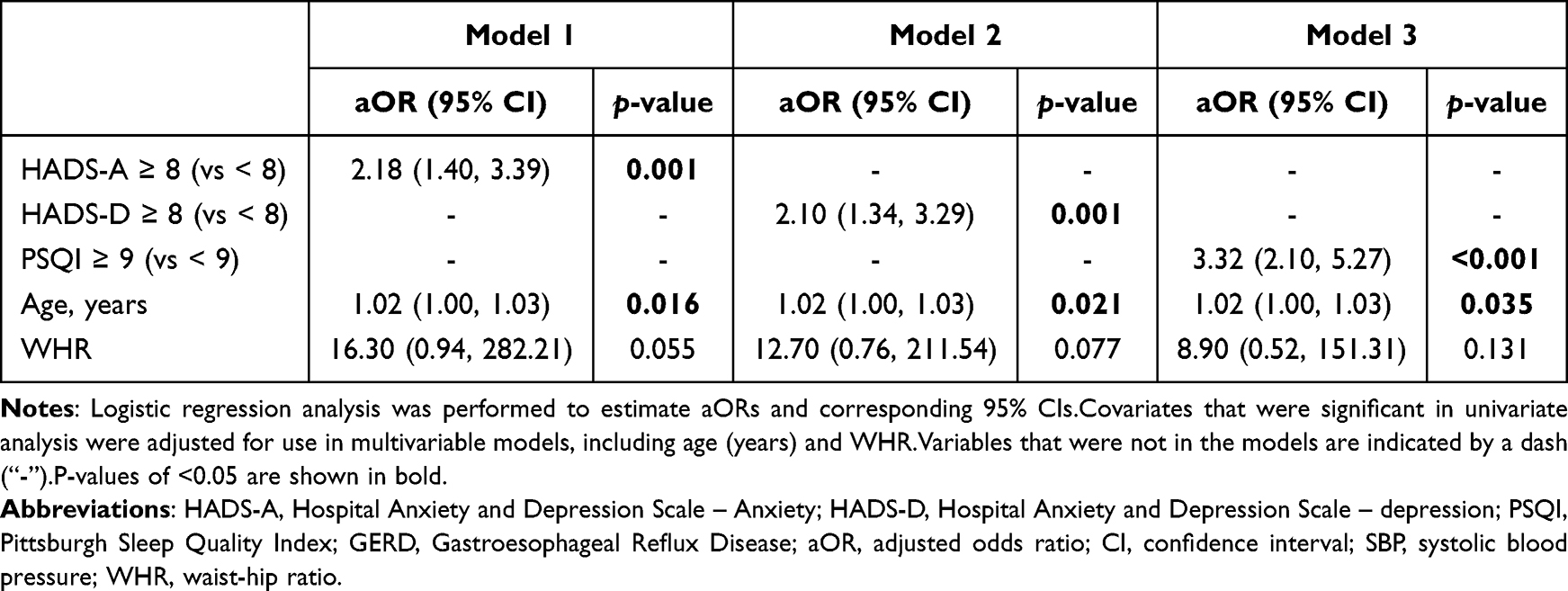 |
Table 3 Multivariable Analysis of Associations Between HADS-A, HADS-D, PSQI, and Probable GERD |
Joint Associations Between HADS-A with PSQI, HADS-S with PSQI, and Probable GERD
Analyses of the joint effects of HADS-A and PSQI scores associated with GERD are shown in Figure 1. Compared to individuals with both low HADS-A and PSQI scores, those with high HADS-A but low PSQI scores showed a non-significant trend toward an increased likelihood of probable GERD (aOR = 1.95, 95% CI: 0.92–4.15). Individuals with low HADS-A but high PSQI scores had significantly higher odds of probable GERD (aOR = 3.43, 95% CI: 1.73–6.76) compared to those with both low scores. Furthermore, individuals with both elevated HADS-A and PSQI scores exhibited the highest odds of probable GERD (aOR = 4.74, 95% CI: 2.62–8.60). This progressive increase highlights the joint impact of anxiety and poor sleep quality on GERD risk.
 |
Figure 1 Associations between the joint effects of Hads-A, HADS-S, and PSQI scores and probable GERD. Abbreviations: HADS-A, Hospital Anxiety and Depression Scale – Anxiety; HADS-D, Hospital Anxiety and Depression Scale – Depression; PSQI, Pittsburgh Sleep Quality Index; SBP, systolic blood pressure; WHR, waist-hip ratio. Notes: Logistic regression was performed to estimate adjusted odds ratios and the corresponding 95% confidence interval. Covariates that were significant in univariate analysis were adjusted for use in multivariable models, including age (years) and WHR. |
Regarding the potential joint effects of HADS-D with PSQI scores, individuals with elevated HADS-D and low PSQI scores had significantly higher odds of developing probable GERD than those with low HADS-D and low PSQI scores (aOR = 2.41, 95% CI 1.09–5.37). Similarly, individuals with low HADS-D and elevated PSQI scores had significantly higher odds of probable GERD than those with low HADS-D and low PSQI scores (aOR = 3.62, 95% CI 2.03–6.46). In addition, individuals with both high HADS-D and PSQI scores had the greatest odds of probable GERD (aOR = 5.09, 95% CI 2.72–9.41) (Figure 1).
Discussion
The large-scale design of this study revealed that individuals with anxiety (HADS-A ≥ 8), depression (HADS-D ≥ 8), and poor sleep quality (PSQI ≥ 9) had 2–3 times higher likelihood of the presence of probable GERD (GERDQ ≥ 9) after adjusting for relevant demographic and clinical parameters, including age, SBP, and WHR. Importantly, the present study is one of the few to examine the joint associations of anxiety, depression, and poor sleep quality on probable GERD. The findings have demonstrated that the combined use of HADS-A and PSQI or HADS-D and PSQI revealed stronger associations with probable GERD.
Associations between GERD and sleep disturbances are common in clinical settings, often coexisting and mutually influencing each other. Although causality cannot be established due to the cross-sectional design, the combined associations observed in this study may be explained by overlapping pathophysiological pathways. Both anxiety and sleep disturbances have been linked to heightened visceral hypersensitivity, altered central pain processing, and autonomic dysregulation—all of which can amplify esophageal discomfort and impair lower esophageal sphincter function. These mechanisms may collectively contribute to the exacerbation of GERD symptoms. Conversely, GERD—particularly nocturnal reflux—may disrupt sleep and contribute to stress and mood disturbances, creating a potential vicious cycle.
Previous research has consistently demonstrated that approximately half of patients with GERD may experience nighttime awakenings because of the sensation of heartburn.23,24 Sleep deficiency has also demonstrated individuals’ enhanced perception of visceral stimuli leading to esophageal hypervigilance. Findings of the present study align with and are supported by previous study results that highlight the associations between sleep disturbances and heightened esophageal sensitivity in patients with GERD.25,26 An earlier study by Schey et al25 demonstrated that sleep deprivation leads to hyperalgesia in patients with GERD, evidenced by a decreased lag time to symptom onset and increased symptom intensity in response to esophageal acid perfusion. This suggests that lack of sleep exacerbates GERD symptoms, likely through increased sensitivity to esophageal stimuli. However, that study did not evaluate associations between GERD and anxiety and depression. To further support these findings, a recent systematic review by El Hage Chehade et al27 highlighted a significant association between obstructive sleep apnea and GERD, suggesting that sleep-related physiological changes, such as increased intra-abdominal pressure, may exacerbate reflux symptoms. Additionally, a study by Li et al28 used ordered logistic regression to confirm a correlation between GERD and anxiety/depression, reinforcing the psychological component of GERD symptom perception.
Similar to results mentioned above, Yi et al26 further confirmed that sleep disturbances significantly enhanced esophageal sensitivity to capsaicin by showing that patients with poor sleep exhibited shorter lag times and a greater intensity of heartburn perception in response to capsaicin infusion. Collectively, these studies support the present findings that disrupted sleep may play a key role in amplifying symptom severity in patients with GERD, likely via mechanisms involving heightened sensory responses to typical reflux stimuli.
The PSQI cut-off value may vary depending on the population and clinical context. For instance, a cut-off score of 9.5 has been used in patients with obstructive sleep apnea (OSA) to differentiate good and poor sleep quality, supported by its correlation with objective measures such as sleep efficiency and total sleep time from polysomnography findings.29 Similarly, a cut-off score of 7 has been shown to effectively evaluate sleep disturbances in patients with brain injury or cancer, reflecting the specific characteristics of these populations.30,31 In the general population, the PSQI cut-off value is commonly set at 5 to distinguish good from poor sleep quality. However, this threshold may not adequately capture the severity of sleep disturbances in specialized cohorts. In the present study, the PSQI cut-off threshold was adjusted to 9 to better align with the characteristics of the study population—patients with pronounced sleep difficulties seeking care at a tertiary hospital sleep center. This adjustment enhances specificity and ensures the identification of clinically significant sleep disturbances, enabling a more accurate assessment of their associations with GERD.
Associations between GERD and stress in life was also investigated. In a prospective study involving 105 patients with GERD, GERDQ scores correlated with results from psychological assessments, including the Beck Anxiety Inventory, Beck Depression Inventory-II, and Somatic Symptom Scale 8.32 Results of another retrospective literature review demonstrated an association between GERD symptoms and scores of the Esophageal Hypervigilance and Anxiety Scale, a questionnaire designed for the cognitive-affective evaluation of visceral sensitivity.33 Therefore, correlations between GERD and anxiety/depression have been clearly demonstrated, but evidence is lacking to show whether sleep has a common effect on anxiety and depression.
The bidirectional relationship between GERD and psychological conditions requires attention.34 Not only do anxiety and poor sleep quality aggravate GERD, but persistent discomfort and disruption caused by GERD symptoms, particularly nocturnal reflux, may also perpetuate or worsen anxiety, depression, and sleep disturbances, creating a vicious cycle.35 This underscores the need for integrated treatment approaches that address both psychological and physiological aspects of GERD in patients with comorbid conditions. By interrupting this cycle, either by improving sleep quality, managing psychological distress, or optimizing GERD treatment, clinicians may achieve better symptom control and improve the overall quality of life of these patients.36–38 Results of the present study indicate that individuals with anxiety/depression combined with sleep disorders need to be more vigilant about the possibility of GERD, allowing for earlier intervention to disrupt this cycle. To facilitate this, clinicians in sleep or psychiatric outpatient clinics could integrate brief screening tools, such as the HADS and PSQI, to identify patients at higher risk of GERD, prompting earlier gastroenterological evaluation and multidisciplinary care. For example, routine use of these questionnaires in sleep clinics could help detect probable GERD in patients presenting with sleep disturbances and psychological distress, enabling timely referrals and interventions.
The diagnosis of GERD is often challenging owing to its diverse and non-specific symptoms, including heartburn, acid reflux, and difficulty swallowing. These symptoms can easily be mistaken for other conditions such as angina or indigestion. Some patients may even have “silent GERD” with no typical symptoms, or present with atypical signs, such as chronic cough or sore throat, leading to underdiagnosis or delayed diagnosis.39 Although diagnostic tools such as upper endoscopy or 24-hour esophageal pH monitoring are accurate, their high cost, invasiveness, and limited accessibility make widespread use difficult, complicating early detection.40 These challenges emphasize the importance of effective screening tools. Questionnaires, such as the GERDQ, have shown good sensitivity and specificity; however, standardized screening processes are still lacking.16 This is particularly problematic in patients with comorbid anxiety, depression, or sleep disturbances as these conditions may mask or confuse GERD symptoms, making the diagnosis even more complex.35 In summary, clinicians should be aware in daily practice that patients with both elevated anxiety and poor sleep quality, as indicated by high HADS-A or HADS-D and PSQI scores, may be at a significantly higher risk of developing GERD. Screening for sleep quality using tools, such as the PSQI in combination with the HADS may be beneficial for the early identification of at-risk individuals.
From a clinical standpoint, our findings suggest that elevated HADS or PSQI scores may serve as supportive indicators prompting further GERD evaluation. Routine GERD screening in patients with high levels of psychological distress or poor sleep may aid in earlier identification of comorbid GERD, although its implementation must be balanced against resource limitations and the potential for overdiagnosis. Integrating brief symptom questionnaires in mental health or sleep clinics could be a practical first step in multidisciplinary care. Once again, it should be clarified that we do not consider the HADS and PSQI to be diagnostic tools for GERD. Instead, based on the findings of this study, their potential utility lies in enhancing clinical awareness and raising suspicion of GERD, particularly in cases presenting with overlapping symptoms.
Strength and Limitations
This study was strengthened by the use of widely accepted, previously validated and reliable questionnaires to evaluate sleep disturbances and psychological distress, thereby enhancing the clinical applicability of results. The inclusion of a substantial sample size was adequate to validate the cumulative positive effects of anxiety and sleep quality on the risk of GERD.
However, interpretation of results is limited by several factors. First, no a priori power analysis was performed due to the retrospective design; however, post-hoc analyses based on the main regression models indicated adequate statistical power (95.8%, 90.7%, and 99.0% for Models 1–3, respectively), supporting the robustness of the findings. Second, GERDQ was used to define probable GERD rather than confirm diagnosis through objective tools like endoscopy or 24-hour pH monitoring, which may lead to potential misclassification bias. Third, self-reported questionnaires such as HADS, PSQI, and GERDQ are subject to recall bias and may not fully reflect clinical severity, potentially exacerbated by their self-administration via tablet in this study. Fourth, the generalizability of these findings may be limited due to the study’s single-center design at a tertiary hospital in Taiwan and its focus on a predominantly Taiwanese population, which may not fully reflect diverse clinical or cultural contexts. Additionally, the study did not control for lifestyle factors such as diet, caffeine intake, smoking, or medication use, which could influence GERD symptoms and represent a limitation in interpreting the observed associations. Fifth, while patients were referred from various outpatient departments, the exact distribution across specialties and the presence of underlying gastrointestinal or psychiatric conditions were not recorded, limiting interpretation of background influences. Furthermore, the somatic symptoms of depression—such as appetite changes or gastrointestinal discomfort—may overlap with GERDQ-assessed symptoms, potentially inflating associations between HADS-D scores and probable GERD. Since both questionnaires rely on subjective symptom reporting, it is difficult to distinguish whether certain gastrointestinal symptoms are due to true reflux or depression-related effects. Additionally, data on antidepressant use, which can independently cause gastrointestinal side effects, were not available, introducing potential residual confounding.
Future research should utilize objective diagnostic measures of GERD to validate whether the psychological and sleep-related indicators assessed in the present study can reliably support GERD risk assessment. Additionally, longitudinal studies and interventional designs are needed to better assess causality and determine whether treating anxiety, depression, or sleep disturbances influences GERD outcomes.
Conclusions
This large-scale study demonstrates that poor sleep quality, anxiety, and depression are associated with the presence of probable GERD among patients with sleep problems. While these psychological and sleep-related factors may help raise clinical awareness, they should not be interpreted as predictive tools. The combined use of validated tools such as HADS and PSQI may facilitate early identification of patients at higher risk for GERD and support integrated management strategies in sleep and gastroenterology clinics. Clinicians should consider GERD as a possible comorbidity in patients presenting with both sleep disturbances and psychological symptoms. Future longitudinal studies are warranted to clarify causal relationships, and interventional trials may help determine whether improving sleep quality or treating psychological distress can reduce GERD symptoms.
Data Sharing Statement
All of the data supporting underlying findings are included in the manuscript. Further enquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
The study protocol was reviewed and approved by the Institutional Review Board of NCKUH (IRB number: B-ER-111-328). Since patient data were analyzed retrospectively and were deidentified to protect identity, the IRB waived the need for included patients’ signed informed consent. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors wish to thank Ms. Wen-Kuei Lin, Ms. Li-Chen Lin, Ms. Yi-Jung Chen, Ms. Yen-Su Lin, Ms. E-Ping Lo, Mr. Jiun-Yu Hsu, and the staff of the Sleep Medicine Centers at National Cheng Kung University Hospital and Tainan Hospital, who participated in the study. We are grateful to Dr. Sheng-Hsiang Lin and Ms. Chih-Hui Hsu from the Biostatistics Consulting Center, Clinical Medicine Research Center, and National Cheng Kung University Hospital, who provided statistical consulting services.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by National Cheng Kung University Hospital, Tainan, Taiwan (NCKUH-11404083).
Disclosure
The authors have no conflicts of interest relevant to this article.
References
1. Fass R. Gastroesophageal reflux disease. N Engl J Med. 2022;387(13):1207–1216. doi:10.1056/NEJMcp2114026
2. Dunbar KB. Gastroesophageal reflux disease. Ann Intern Med. 2024;177(8):Itc113–itc128. doi:10.7326/AITC202408200
3. N EHC, Fu Y, Ghoneim S, et al. Association between obstructive sleep apnea and gastroesophageal reflux disease: a systematic review and meta-analysis. J Gastroenterol Hepatol. 2023;38(8):1244–1251. doi:10.1111/jgh.16245
4. Gerson LB, Fass R. A systematic review of the definitions, prevalence, and response to treatment of nocturnal gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2009;7(4):372–378. doi:10.1016/j.cgh.2008.11.021
5. Li Q, Duan H, Wang Q, et al. Analyzing the correlation between gastroesophageal reflux disease and anxiety and depression based on ordered logistic regression. Sci Rep. 2024;14(1):6594. doi:10.1038/s41598-024-57101-2
6. He M, Wang Q, Yao D, Li J, Bai G. Association between psychosocial disorders and gastroesophageal reflux disease: a systematic review and meta-analysis. J Neurogastroenterol Motil. 2022;28(2):212–221. doi:10.5056/jnm21044
7. Baranwal N, Yu PK, Siegel NS. Sleep physiology, pathophysiology, and sleep hygiene. Prog Cardiovasc Dis. 2023;77:59–69. doi:10.1016/j.pcad.2023.02.005
8. Kanki M, Nath AP, Xiang R, et al. Poor sleep and shift work associate with increased blood pressure and inflammation in UK Biobank participants. Nat Commun. 2023;14(1):7096. doi:10.1038/s41467-023-42758-6
9. Tougas G. The autonomic nervous system in functional bowel disorders. Gut. 2000;4:iv78–80.
10. Sarkar S, Aziz Q, Woolf CJ, Hobson AR, Thompson DG. Contribution of central sensitisation to the development of non-cardiac chest pain. Lancet. 2000;356(9236):1154–1159. doi:10.1016/S0140-6736(00)02758-6
11. Sahin E, Hawro M, Weller K, et al. Prevalence and factors associated with sleep disturbance in adult patients with psoriasis. J Eur Acad Dermatol Venereol. 2022;36(5):688–697. doi:10.1111/jdv.17917
12. Johnson DA, Orr WC, Crawley JA, et al. Effect of esomeprazole on nighttime heartburn and sleep quality in patients with GERD: a randomized, placebo-controlled trial. Am J Gastroenterol. 2005;100(9):1914–1922. doi:10.1111/j.1572-0241.2005.00285.x
13. On ZX, Grant J, Shi Z, et al. The association between gastroesophageal reflux disease with sleep quality, depression, and anxiety in a cohort study of Australian men. J Gastroenterol Hepatol. 2017;32(6):1170–1177. doi:10.1111/jgh.13650
14. Ponce J, Garrigues V, Agréus L, et al. Structured management strategy based on the Gastro-oesophageal Reflux Disease (GERD) Questionnaire (GerdQ) vs. usual primary care for GERD: pooled analysis of five cluster-randomised European studies. Int J Clin Pract. 2012;66(9):897–905. doi:10.1111/j.1742-1241.2012.02992.x
15. Jonasson C, Wernersson B, Hoff DA, Hatlebakk JG. Validation of the GerdQ questionnaire for the diagnosis of gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2013;37(5):564–572. doi:10.1111/apt.12204
16. Simadibrata DM, Ngadiono E, Sinuraya FAG, et al. Diagnostic accuracy of gastroesophageal reflux disease questionnaire for gastroesophageal reflux disease: a systematic review and meta-analysis. Neurogastroenterol Motil. 2023;35(12):e14619. doi:10.1111/nmo.14619
17. Zitser J, Allen IE, Falgàs N, et al. Pittsburgh Sleep Quality Index (PSQI) responses are modulated by total sleep time and wake after sleep onset in healthy older adults. PLoS One. 2022;17(6):e0270095. doi:10.1371/journal.pone.0270095
18. Kawaratani H, Miyaaki H, Hiraoka A, et al. The usefulness of the athens insomnia scale for evaluating sleep disturbance in patients with chronic liver disease comparing with pittsburgh sleep quality index and epworth sleepiness scale. Medicina. 2022;58(6):741. doi:10.3390/medicina58060741
19. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
20. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
21. Brehaut E, Neupane D, Levis B, et al. Depression prevalence using the Hads-D compared to SCID major depression classification: an individual participant data meta-analysis. J Psychosom Res. 2020;139(110256):110256. doi:10.1016/j.jpsychores.2020.110256
22. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. an updated literature review. J Psychosom Res. 2002;52(2):69–77. doi:10.1016/S0022-3999(01)00296-3
23. Farup C, Kleinman L, Sloan S, et al. The impact of nocturnal symptoms associated with gastroesophageal reflux disease on health-related quality of life. Arch Internal Med. 2001;161(1):45–52. doi:10.1001/archinte.161.1.45
24. Shaker R, Castell DO, Schoenfeld PS, Spechler SJ. Nighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function: the results of a Gallup survey conducted on behalf of the American Gastroenterological Association. Am J Gastroenterol. 2003;98(7):1487–1493. doi:10.1111/j.1572-0241.2003.07531.x
25. Schey R, Dickman R, Parthasarathy S, et al. Sleep deprivation is hyperalgesic in patients with gastroesophageal reflux disease. Gastroenterology. 2007;133(6):1787–1795. doi:10.1053/j.gastro.2007.09.039
26. Yi CH, Lei WY, Hung JS, et al. Sleep disturbance and enhanced esophageal capsaicin sensitivity in patients with gastroesophageal reflux disease. J Gastroenterol Hepatol. 2016;31(12):1940–1945. doi:10.1111/jgh.13428
27. Chehade NEH, Fu Y, Lor D, et al. 0879 The association between obstructive sleep apnea and gastroesophageal reflux disease: a meta-analysis and systematic review. Sleep. 2023;46(Supplement_1):A387–A387. doi:10.1093/sleep/zsad077.0879
28. Li E, Ai F, Liang C, et al. Latent profile analysis of depression in US adults with obstructive sleep apnea hypopnea syndrome. Front Psychiatry. 2024;15(1398669).
29. Lusic Kalcina L, Valic M, Pecotic R, Pavlinac Dodig I, Dogas Z. Good and poor sleepers among OSA patients: sleep quality and overnight polysomnography findings. Neurol Sci. 2017;38(7):1299–1306. doi:10.1007/s10072-017-2978-6
30. Fichtenberg NL, Zafonte RD, Putnam S, Mann NR, Millard AE. Insomnia in a post-acute brain injury sample. Brain Inj. 2002;16(3):197–206. doi:10.1080/02699050110103940
31. Beck SL, Schwartz AL, Towsley G, Dudley W, Barsevick A. Psychometric evaluation of the pittsburgh sleep quality index in cancer patients. J Pain Symptom Manage. 2004;27(2):140–148. doi:10.1016/j.jpainsymman.2003.12.002
32. Wang HM, Huang PY, Yang SC, et al. Correlation between psychosomatic assessment, heart rate variability, and refractory GERD: a prospective study in patients with acid reflux esophagitis. Life. 2023;13(9):1862. doi:10.3390/life13091862
33. Wong MW, Liu TT, Yi CH, et al. Oesophageal hypervigilance and visceral anxiety relate to reflux symptom severity and psychological distress but not to acid reflux parameters. Aliment Pharmacol Ther. 2021;54(7):923–930. doi:10.1111/apt.16561
34. Miao Y, Yuan S, Li Y, et al. Bidirectional association between major depressive disorder and gastroesophageal reflux disease: mendelian randomization study. Genes. 2022;13(11):2010. doi:10.3390/genes13112010
35. Zamani M, Alizadeh-Tabari S, Chan WW, Talley NJ. Association between anxiety/depression and gastroesophageal reflux: a systematic review and meta-analysis. Am J Gastroenterol. 2023;118(12):2133–2143. doi:10.14309/ajg.0000000000002411
36. Scott AJ, Webb TL, Martyn-St James M, Rowse G, Weich S. Improving sleep quality leads to better mental health: a meta-analysis of randomised controlled trials. Sleep Med Rev. 2021;60(101556):101556. doi:10.1016/j.smrv.2021.101556
37. Schuitenmaker JM, Kuipers T, Smout A, Fockens P, Bredenoord AJ. Systematic review: clinical effectiveness of interventions for the treatment of nocturnal gastroesophageal reflux. Neurogastroenterol Motil. 2022;34(12):e14385. doi:10.1111/nmo.14385
38. Nakamura F, Kuribayashi S, Tanaka F, et al. Impact of improvement of sleep disturbance on symptoms and quality of life in patients with functional dyspepsia. BMC Gastroenterol. 2021;21(1):78. doi:10.1186/s12876-021-01659-y
39. Gyawali CP, Yadlapati R, Fass R, et al. Updates to the modern diagnosis of GERD: lyon consensus 2.0. Gut. 2024;73(2):361–371. doi:10.1136/gutjnl-2023-330616
40. Katz PO, Dunbar KB, Schnoll-Sussman FH, et al. ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2022;117(1):27–56. doi:10.14309/ajg.0000000000001538
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relation Among Anxiety, Depression, Sleep Quality and Health-Related Quality of Life Among Patients with Systemic Lupus Erythematosus: Path Analysis
Chen HJ, Wang H, Qiu LJ, Ling HY, Wu LL, Wang TR, Zhou Y, Xue Y, Ye DQ, Wang B
Patient Preference and Adherence 2022, 16:1351-1358
Published Date: 25 May 2022
Mind, Body and Machine: Preliminary Study to Explore Predictors of Treatment Response After a Sleep Robot Intervention for Adults with Insomnia
Støre SJ, Tillfors M, Wästlund E, Angelhoff C, Andersson G, Norell A
Nature and Science of Sleep 2023, 15:567-577
Published Date: 13 July 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Functional Brain Activity Alterations in Type 1 Narcolepsy Patients with Anxiety and Depression: A 7-Tesla Resting State-Functional Magnetic Resonance Imaging Study
Chen Y, Ye J, Chen J, Zhen Z, Tang C, Ren S, Han Q, Gao D
Nature and Science of Sleep 2025, 17:1303-1317
Published Date: 13 June 2025
Prevalence and Predictors of Poor Sleep Quality Among Adolescents in Central Sudan: The Role of Depression, Anxiety, and Gender
Omar SM, Al-Nafeesah A, Alwabili AA, AlEed A, Adam I
International Journal of General Medicine 2026, 19:600482
Published Date: 21 April 2026