Back to Journals » Journal of Pain Research » Volume 16
Associations Between Opioid Prescriptions and Use of Hospital-Based Services Among US Adults with Longstanding Physical Disability or Inflammatory Conditions Compared to Other Adults in the Medical Expenditure Panel Survey, 2010–2015
Authors Turk MA, McDermott S, Zhang W, Cai B, Love BL ![]() , Hollis N
, Hollis N
Received 5 December 2022
Accepted for publication 24 April 2023
Published 8 June 2023 Volume 2023:16 Pages 1949—1960
DOI https://doi.org/10.2147/JPR.S400264
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Margaret A Turk,1 Suzanne McDermott,2 Wanfang Zhang,3 Bo Cai,3 Bryan L Love,4 NaTasha Hollis5,6
1Department of Physical Medicine and Rehabilitation, State University of New York (SUNY) Upstate Medical University, Syracuse, NY, USA; 2Department of Environmental, Occupational, and Geospatial Health Sciences, CUNY Graduate School of Public Health & Health Policy, New York, NY, USA; 3Department of Epidemiology and Biostatistics, Arnold School of Public Health, University of South Carolina, Columbia, SC, USA; 4Department of Clinical Pharmacy and Outcome Science, University of South Carolina College of Pharmacy, Columbia, SC, USA; 5Disability and Health Promotion Branch, Division of Human Development and Disability, National Center on Birth Defects and Developmental Disabilities, Centers for Disease Control and Prevention, Atlanta, GA, USA; 6U.S Public Health Service, Atlanta, GA, USA
Correspondence: Suzanne McDermott, Department of Environmental, Occupational, and Geospatial Health Sciences, CUNY Graduate School of Public Health & Health Policy, 55 West 125th Street, New York, NY, 10027, USA, Tel +1 646 364 9649, Email [email protected]
Purpose: To investigate the association of filling opioid prescriptions with healthcare service utilization among a nationally representative sample of adults with disability.
Materials and Methods: The Medical Expenditure Panel Survey (MEPS) for 2010– 2015, Panels 15– 19, was used to identify adults who were prescribed opioids during each two-year period. We examined the data for associations between opioid prescription filling and the number of emergency department (ED) visits and hospitalizations. The participants were grouped as those with inflammatory conditions or with longstanding physical disability, and a comparison group of those without these conditions.
Results and conclusions: Opioid prescription filling differed among adults with inflammatory conditions and longstanding physical disability compared to the comparison group (44.93% and 40.70% vs 18.10%, respectively). For both groups of people with disability, the relative rates for an ED visit or hospitalization were significantly higher for those who filled an opioid prescription, compared to adults with the same conditions who did not fill an opioid prescription. People with a longstanding physical disability who filled an opioid prescription had the highest rate ratio of ED use and hospitalization. Results from this investigation demonstrate that opioid prescription filling among persons with inflammatory conditions and longstanding physical disabilities is associated with higher rates of ED visits and hospitalizations.
Keywords: opioids, rheumatoid arthritis, disabled person, chronic pain, health care utilization
Plain Language Summary
A US national survey “The Medical Expenditure Panel Survey (MEPS)” for 2010–2015 was used to identify adults who were prescribed opioids during two-year periods in order to look for associations between filling opioid prescriptions and use of health care, specifically use of the emergency department (ED) and hospitalizations. We compared people with an inflammatory condition (eg, rheumatoid or psoriatic arthritis, lupus), longstanding physical disability (eg, spinal cord injury, cerebral palsy, stroke), and a comparison group of people without these conditions. We found opioid prescription filling differed among adults with inflammatory conditions and longstanding physical disabilities compared to the comparison group (44.93% and 40.70% vs 18.10%, respectively). For both groups of people with disabling conditions, rates for an ED visit or hospitalization were significantly higher for those who filled an opioid prescription, compared to adults with the same conditions who did not fill an opioid prescription. People with a longstanding physical disability who filled an opioid prescription had the highest rate of ED use and hospitalization.
Introduction
Pain is a common medical complaint of the general United States (US) adult population; an estimated 56% of adults report having some pain in the last 3 months, while 11% report having chronic pain, which is defined as pain every day for the past 3 months.1 People with a variety of disability conditions, representing one in four American adults,2 report higher levels of chronic pain and pain interference for daily tasks than people without disability.3–7 Pain is a common secondary health condition for people with longstanding physical disabilities (eg, spinal cord injury, cerebral palsy),6 with reports of pain interference not decreasing with aging, unlike reports of those without disability.7 People with adult onset inflammatory conditions (eg, ankylosing spondylitis, inflammatory bowel disease) report acute and chronic pain8 that might result in early withdrawal from the workforce.9
Pain management can be complex, especially for chronic pain or pain confounded by the disability and multiple health conditions. Treatment for progressive symptoms of many inflammatory conditions focuses on treating the underlying condition, and that approach is not always successful for alleviating pain.8 There is no clear consensus for managing pain complaints in adults with longstanding physical disabilities.10–12 Opioids are commonly prescribed for pain among people with disability, despite risks for harm. A 2013–2015 Swedish study reported that about one in four people with knee or hip osteoarthritis were dispensed opioids.13 People with longstanding physical disabilities and inflammatory conditions are reported to have higher dosing of opioids compared to people without those conditions.14
Health-care utilization is known to be increased in people using prescription opioids, along with higher health-care costs for those demonstrating nonadherence to opioid prescriptions.15,16 Prescription opioid use has been associated with misuse and addiction, especially in the face of certain mental health conditions.17 People with disability are known to have high use of health-care services;18 however, it is unknown how prescription opioid use contributes to health service use among people with disability.
In a previous study, we reported higher opioid prescription dosing in people with inflammatory conditions and longstanding physical disabilities compared to people without those disabilities.14 These two conditions were chosen for comparison in that study since management strategies for underlying pathologies, pain, and other comorbid conditions differ between the two types of disabling conditions. Using the previously defined disability condition groupings defined by International Classification of Disease Version 9 (ICD-9) codes and a comparison group, the study being presented examined the association between opioid prescriptions filled and hospital services utilization. Our study objectives were to examine: (1) the proportion of adults with inflammatory conditions and longstanding physical disability conditions who filled opioid prescriptions during a two-year period and (2) the rate ratio of emergency department (ED) visits and hospitalizations for people with inflammatory conditions and longstanding physical disabilities with and without filled opioid prescriptions. The comparison group was adults without inflammatory conditions or longstanding physical disability diagnoses. People with cancer were excluded from the case and comparison groups to capture opioid prescription filling practices likely related to the underlying conditions of interest. We hypothesized that (1) people with inflammatory conditions and longstanding physical disabilities were more likely to utilize the ED and be hospitalized, compared to the comparison group, and, (2) people with inflammatory conditions and longstanding physical disabilities who were prescribed opioids would be more likely to frequent the ED and hospital, compared to people with the same conditions who did not have opioid prescriptions filled during the two-year study period.
Materials and Methods
Data Source
Data for this study were obtained from 2010 to 2015 (Panels 15–19) of the Medical Expenditure Panel Survey (MEPS) which are weighted to be nationally representative of the US civilian noninstitutionalized population. The survey was conducted by the Agency for Healthcare Research and Quality. Data for MEPS was obtained from a subset of the National Health Interview Study (NHIS) households (also referred to as Dwelling Units: DU) and people or group of people in the DU who are related (referred to as Reporting Units.) The RU is interviewed as a single unit for MEPS and each MEPS panel was selected from the prior year’s NHIS. Each MEPS panel included data for two sequential years. During the interviews, respondents were asked information about demographic characteristics, insurance coverage, income, employment, health conditions, access to care, and charges and source of payments for all household members. After interview completion, a sample of medical providers participated in the Medical Provider Component. Providers were contacted by telephone to obtain, verify, and/or replace the health-care information that was not fully provided by participants. Recorded information was collected from hospitals, physician offices, home health-care providers, and pharmacies. More information can be found at: https://meps.ahrq.gov/mepsweb/about_meps/survey_back.jsp.
IRB Approval
This study was not subject to approval by an Institutional Review Board, because the deidentified data used here was obtained from a free and publicly available dataset (URL is shown above). The authors of this manuscript did not enroll any subjects nor collect any data.
Study Sample
The study sample is based on previous MEPS analysis related to disability conditions associated with pain complaints and opioid use.14 Five panels of MEPS data for 48,681 US adults aged 18 through 64 years were included: those with inflammatory conditions (n = 1055), those with longstanding physical disabilities (n = 543), and the comparison group (n = 47,083). Three-digit ICD-9 codes were used to identify the three groups (Table 1). Adults with inflammatory conditions were those with rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, systemic lupus erythematosus, or inflammatory bowel disease. Adults with longstanding physical disabilities reported stroke, spina bifida, spinal cord injury, multiple sclerosis, or cerebral palsy. Clinical reports have documented that both of these groups report a high prevalence of pain and require different complex medical management, making it problematic to combine them into one group.3–9 The comparison group of people was all other MEPS participants in the sample who did not meet the case definitions for inflammatory conditions or longstanding physical disabilities (n = 47,083). Adults with reported cancer were eliminated from the entire sample since opioid use for palliative care would complicate our interpretation of the results.
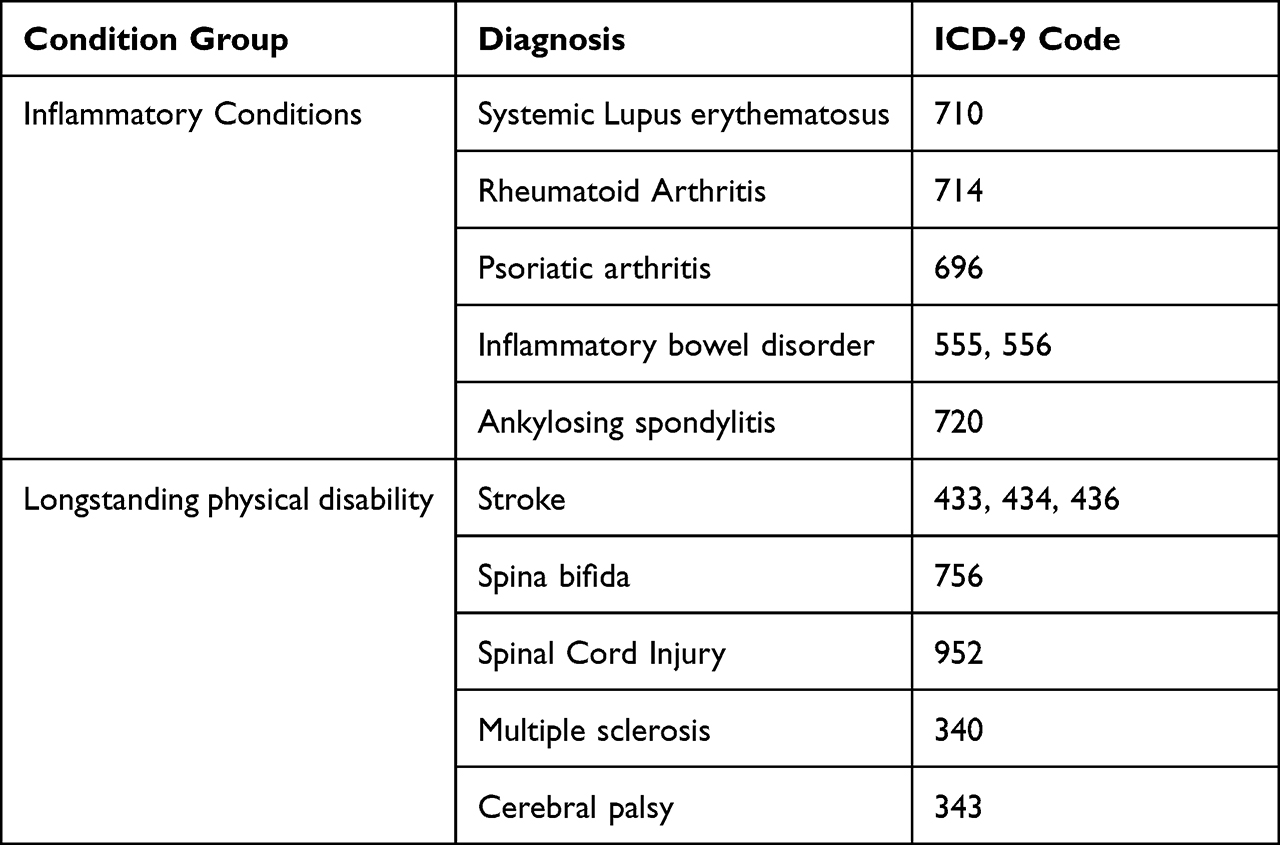 |
Table 1 ICD-9CM Codes for Inflammatory Conditions and Longstanding Physical Disability |
Participants were further defined by filling patterns of opioid prescriptions. Participants who filled a prescription for opioids are referred to as adults with filled an opioid prescription; those who did not fill any opioid prescriptions are referred to as adults without filled opioid prescription.
Outcomes
The outcomes of interest in this investigation were the numbers of ED visits and hospitalizations. Some participants had no ED visits or hospitalizations, while others had multiple ED visits and/or hospitalizations.
Variables
The primary independent variable was prescription opioid use. Those with an opioid prescription during the two-year panel period were self-reported and confirmed by pharmacy records. Opioid prescriptions were identified using a list of opioid analgesics compiled by the Centers for Disease Control and Prevention in 2017 (Appendix 1). Opioid prescriptions filled within the panel period were dichotomized as ≥1 opioid prescription filled (adults with opioid prescription filled) or no opioid prescription filled (adults without opioid prescription filled).
Demographic and medical variables were used as covariates in the modeling. The demographic variables included age (continuous), sex (male, female), race/ethnicity (non-Hispanic white, non-Hispanic black, non-Hispanic other, Hispanic), marital status (married, widowed, divorced/separated, never married), health insurance coverage (private, public, uninsured), census region (northeast, Midwest, south, west), poverty level (poor, near poor, low income, middle income, high income), and education level (less than high school, high school, college or above). Other medical variables were an outpatient visit in the previous year (continuous), self-reported depression symptoms (ie, feeling down), smoking status (yes, no), body mass index (underweight, normal, overweight, obese), and physical activity status (active, inactive).
Statistical Methods
Baseline characteristics for the start of the two-year study period were summarized for the two case disability groups of people and the comparison group of people. Means (standard errors) were calculated for continuous variables and frequency (percent) was used for categorical variables.
Zero-inflated Poisson (ZIP)19 regression models were used for the analyses to identify the variables associated with higher numbers of ED visits and hospitalizations. ZIP regression considers the excessive zero number of visits for both ED visits and hospitalizations. ZIP models have two parts, a logit model to predict the group of people with zero ED visits and hospitalizations, and a Poisson count model for the group of people with one or more encounters. Over-dispersion of the Poisson model was tested using Pearson Chi-square dispersion statistic and Vuong test20 was used to test the Zero-inflation part of the model. Age and sex were used to calculate the probability of excessive zeros in the logistic model. Other covariates were included in the Poisson model initially and removed via step-wise elimination if the p-value was greater than 0.05; however, age and sex remained in the model since they are central to understanding of prescription opioid use. Parameter estimates were reported as coefficients and rate ratios (RR) with 95% confidence intervals (CI).
We comparatively analyzed the three groups of people identified for this study in three ways. First, the interactive effect between disability and comparison groups of people and prescription opioid use was examined to compare between those with inflammatory conditions or with longstanding physical disabilities with and without an opioid prescription filled. Second, we compared the two categories of people with disabling conditions with an opioid prescription filled with the comparison group (ie, those without those two disabling conditions) with opioid prescriptions filled. Lastly, because the longstanding physical disability group had the highest rates of emergency department and hospital utilization, we combined the inflammatory condition group with the comparison group and compared them to the longstanding physical disability group.
To account for having five MEPS panels for the analysis, we adjusted the analytic weights by dividing it by the five years being pooled. Data management and univariate tests were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). ZIP modeling was performed using STATA 12 (StataCorp, 2011). The statistical significance level was set at p = 0.05.
Results
In general, those who were prescribed opioids within each of the three cohorts were female, non-Hispanic white, married, with less than a high school education, and lived in the Southern US. Those with inflammatory conditions and those with longstanding physical disabilities differed from people without those two disabling conditions and who were prescribed opioids (now called the comparison group) in the proportion who had an opioid prescription filled during the two-year study window. Among the people in the comparison group, 81.9% had no opioid prescription filled, and 18.1% had one or more prescriptions filled. Those with inflammatory conditions and those with longstanding physical disabilities had 55.1% and 59.3%, respectively, no opioid prescription filled, and 44.9% and 40.7% having one or more opioid prescriptions filled (Table 2).
 |
Table 2 Characteristics of Adults Who Filled an Opioid Prescription in the 2010–2015 US Medical Expenditure Panel Study Data (Unadjusted for the Complex Survey Design) for Inflammatory Conditions, Longstanding Physical Disability, and a Comparison Group |
There was a higher rate of opioid prescription filling in those with inflammatory conditions among those who were female, obese (defined by body mass index ≥ 30 kg/cm2), and who had a higher education level compared to people with longstanding physical disabilities and the comparison group of people. There was a higher prevalence of non-Hispanic Black and poor adults with longstanding physical disabilities compared to the other cohorts. The number of ED visits were higher for those with inflammatory conditions or longstanding physical disabilities compared to the comparison group. There were relatively few hospitalizations for all three cohorts, although adults with longstanding physical disabilities had the highest number. For outpatient visits, those with longstanding physical disabilities have similar patterns to the comparison group, while those with inflammatory conditions had the lowest values. Further details can be found in Appendices 2 and 3, where we modeled the association between each patient characteristic with emergency department visits and hospitalizations. The only characteristics that were statistically significant risks were being physically inactive and having public insurance.
As shown in Table 3, those with inflammatory conditions who had an opioid prescription filled had 2.46 times the rate of ED use and 4.08 times the rate of hospitalization compared to those within that category without an opioid prescription filled. For people with longstanding physical disabilities, those with an opioid prescription filled had 1.81 higher utilization of the ED and 1.65 times the rate of hospitalization compared to those within that category who did not have an opioid prescription filled. The comparison group had the highest rate ratio of ED use (RR = 3.11) and 3.48 times the rate ratio for hospitalizations, for within group comparison.
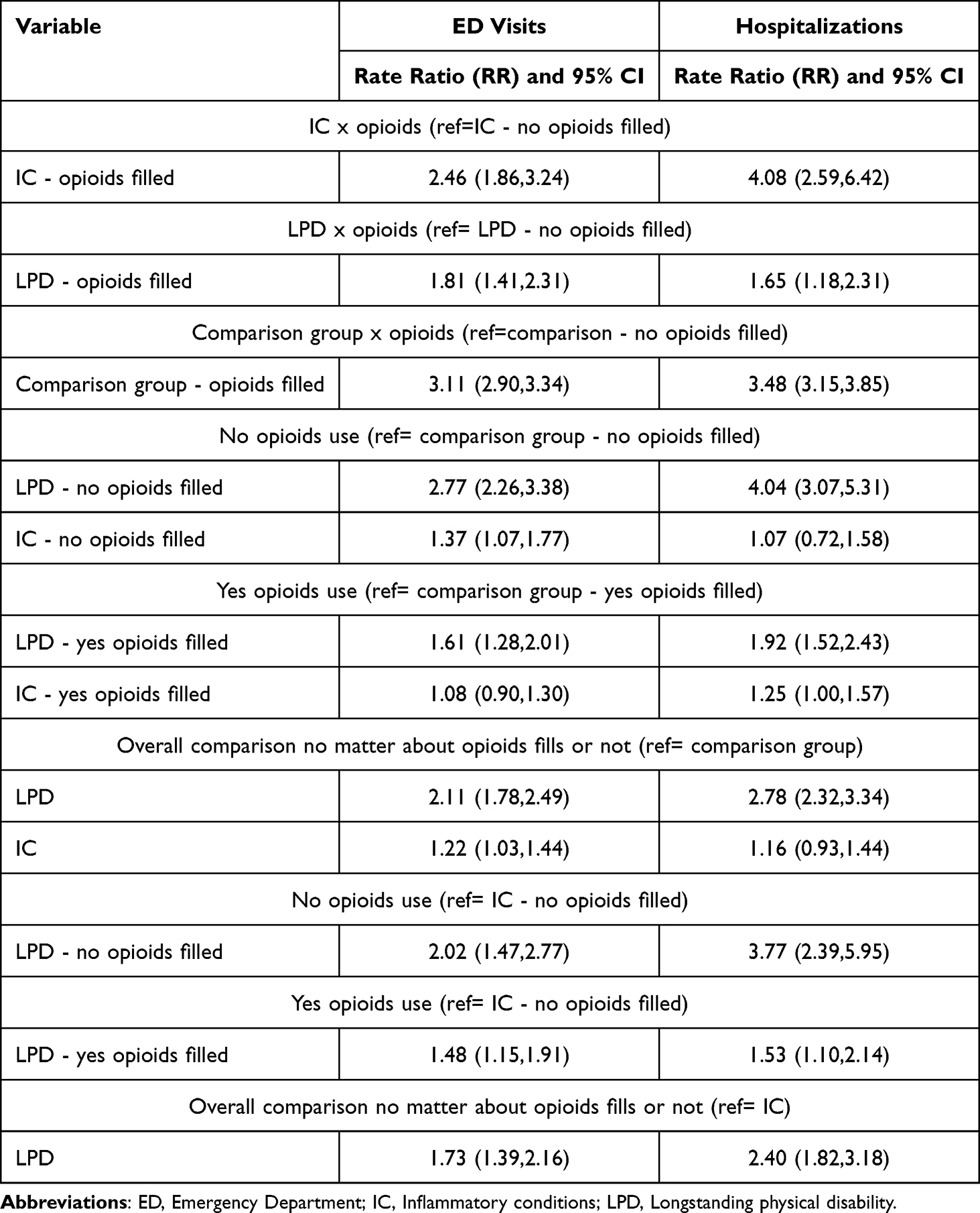 |
Table 3 The Interactive Effects Between Opioid Prescription Fills and Inflammatory Condition, Longstanding Physical Disability, and a Comparison Group, on Emergency Department Visits and Hospitalizations, from the US Medical Expenditure Panel Survey, 2010–2015 |
Also shown in Table 3, and Figure 1, the longstanding physical disability group had the highest relative risk for emergency department visits and hospitalizations when there was no opioid use (RR = 2.77, 95% CI: 2.26–3.38) and when there was opioid use (RR = 1.61, 95% CI: 1.28–2.01). And overall, people with longstanding physical disabilities, with and without opioid use, had highest ED utilization (RR = 2.11, 95% CI: 1.78–2.49) when compared to the comparison group.
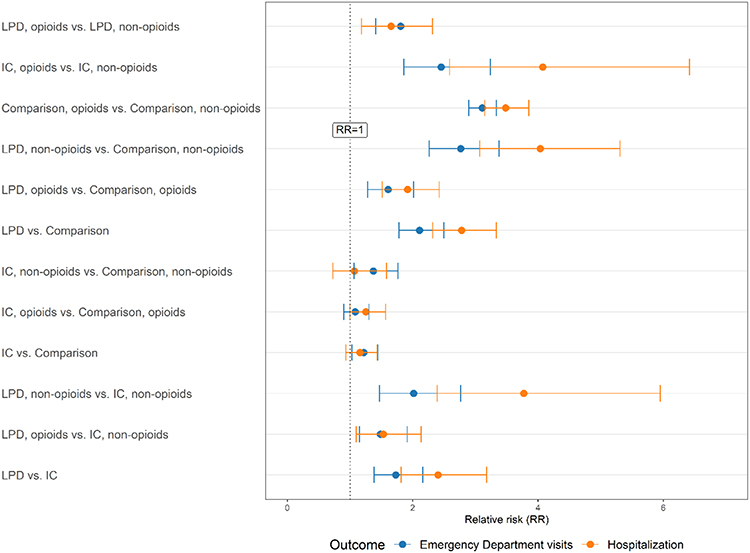 |
Figure 1 Interactive Effects Between Opioid Prescription Fills Among People with Inflammatory Conditions, Longstanding Physical Disabilities, and a Comparison Group, on Emergency Department Visits and Hospitalizations. |
Finally, because the longstanding physical disabilities group had substantially higher and statistically significant results for both ED and hospitalization, we compared them to a combined group of those with inflammatory conditions and the original comparison group of those without either disabling condition, shown in Table 4A and B. Those who had opioid prescriptions filled who were identified with longstanding physical disabilities were 5 times more likely to have an ED encounter compared to the combined group (ie, people with inflammatory conditions and people without either longstanding physical disabilities or inflammatory conditions) who did not have an opioid prescription filled, and 2.56 times more likely to have an ED visit compared to the combined group regardless of opioid prescription status. Those who used opioids and who had longstanding physical disabilities were 6.68 times more likely to have a hospitalization than those in the combined group who did not have an opioid prescription filled and 3.32 times more likely to be hospitalized compared to the combined group regardless of opioid prescription status.
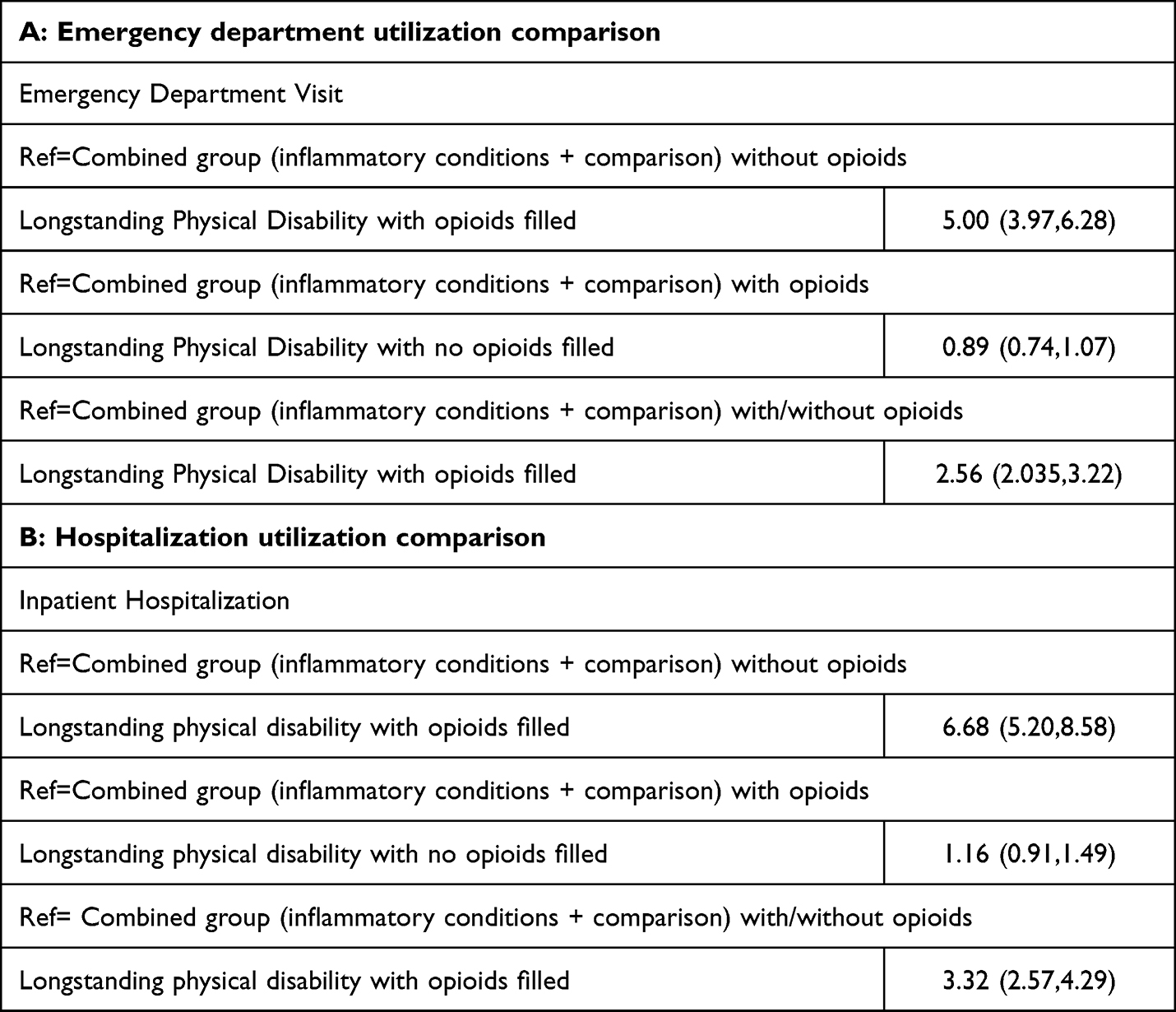 |
Table 4 Emergency Department and Hospital Inpatient Utilization for People with Longstanding Physical Disability, from the US Medical Expenditure Panel Survey, 2010–2015 |
Discussion
This study offers new insights about hospital-based utilization in the US for select groups of people with disabilities, with and without filled opioid prescriptions. Overall, adults with longstanding physical disabilities had the highest utilization for hospitalization and ED use (bottom row of Table 3). However, when we compared each group of people (with inflammatory condition, longstanding physical disabilities, and the comparison group without either) with and without opioid fills, the rate ratio was larger for the comparison group regarding ED visits, and the rate ratio was larger for the longstanding physical disability group for hospital stays. People with inflammatory conditions and longstanding physical disability are clinically and functionally different, and our results show they differ in the utilization of the ED and hospitalization; thus, we did not combine them in the analyses. Instead, we combined the inflammatory condition group with the comparison group and showed substantially higher utilization (RR from 2.56 to 6.68 depending on the comparison) for the longstanding physical disability group, with and without opioids, for emergency department use and hospitalizations.
Previous research notes that people with a variety of longstanding physical disabilities have higher use of health-care services,21–23 but prescription opioid filling within these conditions has not been previously investigated. We demonstrate the higher use of hospital-based health care by people with longstanding physical disabilities who fill an opioid prescription, but we are unable to explain the underlying reason for this finding with our data. It is likely that those with longstanding physical disabilities, all of whom had neurologic conditions, have more comorbidities and secondary health conditions which complicate their care and account for hospital utilization.24–27 To further support this possibility, there is ample evidence that clinicians, especially primary care clinicians or hospitalists, are not specifically trained in the care of people with disability8,28–30 or chronic pain management.31–33 People with longstanding physical disabilities who experience pain have reported their symptom was being treated with opioids without investigation for etiologies or consideration of other pain management strategies.34,35 During the time of this study, opioid use disorder was not yet described within clinical guidelines.36,37 There is a clear message that clinicians caring for people with longstanding physical disabilities require an understanding of their patients’ complexities of care and vulnerabilities, especially with the addition of opioid prescriptions. Further studies could be designed to identify how the underlying pathology and level of severity play into the choice of management and the effectiveness of non-opioid interventions. Additionally, assessing the utility of guidance about pain assessment and management38 and opioid prescribing within disability populations39 could be helpful.
We showed that people with inflammatory conditions filling an opioid prescription had increased health-care usage, although not at the higher levels seen in people with longstanding physical disabilities. Approximately 45% of those with inflammatory conditions filled prescriptions during the study period. Disease-modifying anti-rheumatic drugs and/or biologics, which focus on disease control or remission, are available and have been shown to decrease pain complaints.40 While we did not analyze the use of these medications, the increased health-care usage may reflect that the newer class of medications are not being used routinely because of insurance coverage restrictions, special drug handling requirements, limited drug distribution networks, or lack of clinician knowledge.41–43 Further analyses assessing utility of disease managing medications could help to better understand prescribing patterns.
Although the comparison group was not the focus of the study, the results do support previous studies that report people who fill an opioid prescription, regardless of their disability status, used hospital services more than those who do not fill opioid prescriptions.15,16
Limitations
There are some important limitations to note. Prescription filling of opioids was measured, not actual usage, and there are no objective measures for pain etiologies or severity, or determinations of dosing. Another limitation is that reasons for ED visits and hospitalizations were not analyzed. The information collected from respondents indicated they went to the hospital because of their disabling condition, and not the symptom that precipitated the ED or hospital visit (available from the authors on request). Additionally, the MEPS survey questions about pain varied in the panel years; so, a measure of pain frequency and severity during the study period was not possible. Therefore, future research that uses the clinical notes from electronic medical records could determine proximal reasons for hospital utilization. Nonetheless, the high rate of filling opioid prescriptions suggests that pain complaints are common among people with inflammatory conditions and longstanding physical disabilities and investigation to better understand pain and pain management among people with disability is important.
Conclusion
Our findings suggest that people with disabilities from inflammatory conditions and longstanding physical disabilities more frequently fill opioid prescriptions than the general population. Since this study used a nationally representative sample of the US population and complex analytic procedures, the results can be generalized. Overall, people with longstanding physical disabilities who filled an opioid prescription had the highest rate of ED visits and hospitalizations compared to those with inflammatory conditions or the comparison group, separately or combined. We suggest clinicians carefully consider prescribing opioids for management of pain for people with disabling conditions, especially in people with longstanding physical disabilities.
Data Sharing Statement
Data for this study were obtained from 2010 to 2015 (Panels 15–19) of the Medical Expenditure Panel Survey (MEPS). The survey was conducted by the Agency for Healthcare Research and Quality. https://meps.ahrq.gov/data_stats/download_data_files_results.jsp?cboDataYear=All&cboDataTypeY=1%2CHousehold+Full+Year+File&buttonYearandDataType=Search&cboPufNumber=All&SearchTitle=Longitudinal.
Acknowledgment
This work was supported by the University of South Carolina’s Disability Research and Dissemination Center (DRDC) through its Cooperative Agreement (Number 6U19DD001218) with the Centers for Disease Control and Prevention (CDC). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the DRDC or CDC.
Disclosure
The authors report that there are no competing interests to declare in this work.
References
1. Nahin RL. Estimates of pain prevalence and severity in adults: United States, 2012. J Pain. 2015;16(8):769–780. doi:10.1016/j.jpain.2015.05.002
2. Centers for disease control and prevention, disability and health promotion. Available from: https://www.cdc.gov/ncbddd/disabilityandhealth/infographic-disability-impacts-all.html.
3. Lo J, Chan L, Flynn S. A systematic review of the incidence, prevalence, costs, and activity and work limitations of amputation, osteoarthritis, rheumatoid arthritis, back pain, multiple sclerosis, spinal cord injury, stroke, and traumatic brain injury in the United States: a 2019 update. Arch Phys Med Rehabil. 2021;102(1):115–131. doi:10.1016/j.apmr.2020.04.001
4. Westerlind E, Singh R, Persson HC, Sunnerhagen KS. Experienced pain after stroke: a cross-sectional 5-year follow-up study. BMC Neurol. 2020;20(1):4. doi:10.1186/s12883-019-1584-z
5. Müller R, Brinkhof MW, Arnet U, et al. Prevalence and associated factors of pain in the Swiss spinal cord injury population. Spinal Cord. 2017;55(4):346–354. doi:10.1038/sc.2016.157
6. Ehde DM, Jensen MP, Engel JM, Turner JA, Hoffman AJ, Cardenas DD. Chronic pain secondary to disability: a review. Clin J Pain. 2003;19(1):3–17. doi:10.1097/00002508-200301000-00002
7. Molton I, Cook KF, Smith AE, Amtmann D, Chen WH, Jensen MP. Prevalence and impact of pain in adults aging with a physical disability: comparison to a US general population sample. Clin J Pain. 2014;30(4):307–315. doi:10.1097/AJP.0b013e31829e9bca
8. Borenstein DG, Hassett AL, Pisetsky D. Pain management in rheumatology research, training, and practice. Clin Exp Rheumatol. 2017;35(5):2–7.
9. Berkovic D, Briggs AM, Ayton D, Parker C, Ackerman I. Arthritis-related work outcomes experienced by younger to middle-aged adults: a systematic review [published online ahead of print, 2020 August 26. Occup Environ Med. 2020;106640. doi:10.1136/oemed-2020-106640
10. Norrbrink C, Löfgren M. Needs and requests--patients and physicians voices about improving the management of spinal cord injury neuropathic pain. Disabil Rehabil. 2016;38(2):151–158. doi:10.3109/09638288.2015.1035456
11. Vogtle LK. Pain in adults with cerebral palsy: impact and solutions. Dev Med Child Neurol. 2009;51(Suppl 4):113–121. doi:10.1111/j.1469-8749.2009.03423.x
12. Osborne TL, Jensen MP, Ehde DM, Hanley MA, Kraft G. Psychosocial factors associated with pain intensity, pain-related interference, and psychological functioning in persons with multiple sclerosis and pain. Pain. 2007;127:52–62. doi:10.1016/j.pain.2006.07.017
13. Thorlund JB, Turkiewicz A, Prieto-Alhambra D, Englund M. Opioid use in knee or Hip osteoarthritis: a region-wide population-based cohort study. Osteoarthritis Cartilage. 2019;27(6):871–877. doi:10.1016/j.joca.2019.01.005
14. Hong Y, Geraci M, Turk MA, Love BL, Mcdermott SW. Opioid prescription patterns for adults with longstanding disability and inflammatory conditions compared to other users, using a nationally representative sample. Arch Phys Med Rehabil. 2019;100(1):86–94. doi:10.1016/j.apmr.2018.06.034
15. Jensen MK, Thomsen AB, Højsted J. 10-year follow-up of chronic non-malignant pain patients: opioid use, health related quality of life and health care utilization. Eur J Pain. 2006;10(5):423–433. doi:10.1016/j.ejpain.2005.06.001
16. Leider HL, Dhaliwal J, Davis EJ, Kulakodlu M, Buikema AR. Healthcare costs and nonadherence among chronic opioid users. Am J Manag Care. 2011;17(1):32–40.
17. Wood E, Simel DL, Klimas J. Pain management with opioids in 2019–2020. JAMA. 2019;10:1–3. doi:10.1001/jama.2019.15802
18. National Center for Health Statistics (US). Health, United States, 2016: With Chartbook on Long-Term Trends in Health. Hyattsville (MD): National Center for Health Statistics (US); 2017.
19. Lambert D. Zero-inflated poisson regression, with an application to defects in manufacturing. Technometrics. 1992;34(1):1–14. doi:10.1080/00401706.1992.10485228
20. Vuong QH. Likelihood ratio tests for model selection and non-nested hypotheses. Econometrica. 1989;57:307–333. doi:10.2307/1912557
21. Xu H, Covinsky KE, Stallard E, Thomas J, Sands LP. Insufficient help for activity of daily living disabilities and risk of all-cause hospitalization. J Am Geriatr Soc. 2012;60(5):927–933. doi:10.1111/j.1532-5415.2012.03926.x
22. Jain NB, Ayers GD, Peterson EN, et al. Traumatic spinal cord injury in the United States, 1993–2012. JAMA. 2015;313(22):2236–2243. doi:10.1001/jama.2015.6250
23. Bennett KJ, Mann JR, Ouyang L. 30-Day all-cause readmission rates among a cohort of individuals with rare conditions. Disabil Health J. 2019;12(2):203–208. doi:10.1016/j.dhjo.2018.08.009
24. Alan KHT, Bayley MT. A narrative review of the impact of medical comorbidities on stroke rehabilitation outcomes. Disabil Rehabil. 2018;40(15):1842–1848. doi:10.1080/09638288.2017.1309465
25. Smith AE, Molton IR, Jensen MP. Self-reported incidence and age of onset of chronic comorbid medical conditions in adults aging with long-term physical disability. Disabil Health J. 2016;9(3):533–538. doi:10.1016/j.dhjo.2016.02.002
26. Zhang T, Tremlett H, Zhu F, et al. Effects of physical comorbidities on disability progression in multiple sclerosis. Neurology. 2018;90(5):e419–e427. doi:10.1212/WNL.0000000000004885
27. Hollung SJ, Bakken IJ, Vik T, et al. Comorbidities in cerebral palsy: a patient registry study. Dev Med Child Neurol. 2020;62(1):97–103. doi:10.1111/dmcn.14307
28. Symons AB, Morley CP, McGuigan D, Akl EA. A curriculum on care for people with disabilities: effects on medical student self-reported attitudes and comfort level. Disabil Health J. 2014;7(1):88–95. doi:10.1016/j.dhjo.2013.08.006
29. Ioerger M, Flanders RM, French-Lawyer JR, Turk MA. Interventions to teach medical students about disability: a systematic search and review. Am J Phys Med Rehabil. 2019;98(7):577–599. doi:10.1097/PHM.0000000000001154
30. Peiris-John R, Jain NR, Hogan A, Ameratunga S. Educating health science students about disability: teachers’ perspectives on curricular gaps. Disabil Health J. 2021;12(1):100985. doi:10.1016/j.dhjo.2020.100985
31. Loeser JD, Schatman ME. Chronic pain management in medical education: a disastrous omission. Postgrad Med. 2017;129(3):332–335. doi:10.1080/00325481.2017.1297668
32. Webster F, Bremner S, Oosenbrug E, Durant S, McCartney CJ, Katz J. From opiophobia to overprescribing: a critical scoping review of medical education training for chronic pain. Pain Med. 2017;18:1467–1475. doi:10.1093/pm/pnw352
33. Dueñas M, Salazar A, Sa´nchez M, De Sola H, Ojeda B, Failde I. Relationship between using clinical practice guidelines for pain treatment and physicians’ training and attitudes toward patients and the effects on patient care. Pain Pract. 2017;18:38–47. doi:10.1111/papr.12579
34. Löfgren M, Norrbrink C. “But I know what works” – patients’ experience of spinal cord injury neuropathic pain management. Disabil Rehabil. 2012;34(25):2139–2147. doi:10.3109/09638288.2012.676146
35. Hand BN, Krause JS, Simpson KN. Dose and duration of opioid use in propensity score–matched, privately insured opioid users with and without spinal cord injury. Arch Phys Med Rehabil. 2018;99:855–861. doi:10.1016/j.apmr.2017.12.004
36. Graupensperger S, Corey JJ, Turrisi RJ, Evans MB. Individuals with spinal cord injury have greater odds of substance use disorders than non-sci comparisons. Drug Alcohol Depend. 2019;205:107608. doi:10.1016/j.drugalcdep.2019.107608
37. Pergolizzi JV, Rosenblatt M, LeQuang JA. Three years down the road: the aftermath of the CDC guideline for prescribing opioids for chronic pain. Adv Ther. 2019;36:1235–1240. doi:10.1007/s12325-019-00954-1
38. Hooten M, Thorson D, Bianco J, et al; Institute for Clinical Systems Improvement. Pain: assessment, non-opioid treatment approaches and opioid management; 2017. Available from: https://www.icsi.org/guideline/pain/.
39. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain United States. MMWR Recomm Rep. 2022;71(3):1–95. doi:10.15585/mmwr.rr7103a1
40. Steiman AJ, Pope JE, Thiessen-Philbrook H, et al. Non-biologic disease-modifying antirheumatic drugs (DMARDs) improve pain in inflammatory arthritis (IA): a systematic literature review of randomized controlled trials. Rheumatol Int. 2013;33(5):1105–1120. doi:10.1007/s00296-012-2619-6
41. Hawkes JE, Mittal M, Davis M, Brixner D. Impact of online prescription management systems on biologic treatment initiation. Adv Ther. 2019;36(8):2021–2033. doi:10.1007/s12325-019-01000-w
42. Rohr MK, Mikuls TR, Cohen SB, Thorne JC, O’Dell JR. Underuse of methotrexate in the treatment of rheumatoid arthritis: a national analysis of prescribing practices in the US. Arthritis Care Res. 2017;69(6):794–800. doi:10.1002/acr.23152
43. Gleason PP, Alexander GC, Starner CI, et al. Health plan utilization and costs of specialty drugs within 4 chronic conditions. J Manag Care Pharm. 2013;19(7):542–548. doi:10.18553/jmcp.2013.19.7.542
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cohort Description: Preventing an Opioid Epidemic in Norway – Focusing on Treatment of Chronic Pain (POINT) – A National Registry-Based Study
Hamina A, Odsbu I, Borchgrevink PC, Chen LC, Clausen T, Espnes KA, Gjesdal K, Handal M, Hartikainen S, Hjellvik V, Holter MTS, Høibø T, Kurita GP, Langaas HC, Lid TG, Nøst TH, Sjøgren P, Skurtveit S
Clinical Epidemiology 2022, 14:1477-1486
Published Date: 8 December 2022
Tapentadol: A Review of Experimental Pharmacology Studies, Clinical Trials, and Recent Findings
Alshehri FS
Drug Design, Development and Therapy 2023, 17:851-861
Published Date: 21 March 2023
Engagement in Integrative and Nonpharmacologic Pain Management Modalities Among Adults with Chronic Pain: Analysis of the 2019 National Health Interview Survey
Rodgers-Melnick SN, Trager RJ, Love TE, Dusek JA
Journal of Pain Research 2024, 17:253-264
Published Date: 16 January 2024
Pharmacological Prescribing and Satisfaction with Pain Treatment Among Non-Hispanic Black Men with Chronic Pain
Oloruntoba O, Bergeron CD, Zhong L, Merianos AL, Sherman LD, Kew CL, Goidel RK, Smith ML
Patient Preference and Adherence 2024, 18:187-195
Published Date: 19 January 2024
Enhanced Recovery After Surgery (ERAS) Protocols in Orthopaedic Surgery: Opioids or Not Opioids?
Grossi P
Journal of Pain Research 2025, 18:1683-1695
Published Date: 28 March 2025