")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Association of Serum Total Bilirubin and Uric Acid with Low Glomerular Filtration Rate Diabetic Kidney Disease in Type 2 Diabetic Patients
Authors Tafese R, Genet S , Addisu S
Received 5 October 2022
Accepted for publication 15 December 2022
Published 21 December 2022 Volume 2022:15 Pages 3993—3999
DOI https://doi.org/10.2147/DMSO.S391777
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Rihobot Tafese,1 Solomon Genet,2 Sisay Addisu2
1Biomedical Sciences Department, Arba Minch University, Arba Minch, Ethiopia; 2Department of Biochemistry, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Solomon Genet, Department of Biochemistry, Addis Ababa University, PO Box 9086, Addis Ababa, Ethiopia, Tel +251933944457, Fax +25115513099, Email [email protected]
Background: Diabetic kidney disease (DKD) is one of the major complications of Type 2 diabetes, clinically characterized by a progressive increase in albuminuria and/or a subsequent decline in glomerular filtration rate. Identification of novel risk factors contributes to reduction in the risk of diabetic kidney disease. Bilirubin, as an antioxidant and anti-inflammatory molecule, is believed to have a protective role in kidney disease. On the other hand, uric acid is implicated in the pathogenesis of DKD due to its pro-oxidant and pro-inflammatory property in vascular tissues.
Methods: A hospital based comparative cross-sectional study was conducted from October 2020 to March 2021 on 200 eligible Type 2 diabetic patients (58 with DKD and 142 without DKD) to assess the association of serum total bilirubin and serum uric acid levels with low GFR diabetic kidney disease using consecutive sampling technique.
Results: The serum total bilirubin level was significantly decreased (0.15± 2.29, mean±SD) in the DKD group compared to the non-DKD group (0.19± 2.26), whereas the mean±SD serum uric acid was significantly increased in the DKD group (7.13± 2.21) compared to the non-DKD group (5.24± 1.92). A low serum total bilirubin level was significantly associated with increased risk of DKD in multivariate analysis (AOR=2.23, 95% CI=1.55– 4.13) also to high serum uric acid levels (AOR=2.09, 95% CI=1.06– 4.12). Moreover, a low serum total bilirubin level was significantly associated with increased risk of DKD among patients with high serum uric acid (AOR=2.55, 95% CI=1.05– 6.19). Similarly, high serum uric acid was significantly associated with increased risk of DKD among patients with low serum total bilirubin (AOR=3.49, 95% CI=1.29– 9.42).
Conclusion: Co-presence of low serum total bilirubin and high serum uric acid may be useful for stratification of DKD risk among patients with Type 2 diabetes mellitus.
Keywords: diabetic kidney disease, Type 2 diabetes, serum total bilirubin, serum uric acid
Introduction
Diabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia.1 Diabetic nephropathy (DN) is one of the most frequent microvascular complications of Type 2 DM, characterized by glomerular, tubular, and tubule-interstitial injury.2
Bilirubin, one of the most highly conserved groups of non-polar molecules, is a metabolic end product of heme degradation by heme oxygenase.3 It has been shown to have antioxidant and anti-inflammatory effects.4
Uric acid is a heterocyclic organic compound endogenously produced by animals as a purine catabolite.5 It is formed by the liver and mainly excreted by the kidneys and intestine.6 Humans, due to the absence of uricase activity, have a higher uric acid level than other mammals.7
According to the 2017 estimate by International Diabetes Federation (IDF), Ethiopia has 1.92 million (3.3%) adult people aged 20–79 years with diabetes, making it the largest diabetes population in sub-Saharan Africa.8 With the increasing incidence of Type 2 DM worldwide, diabetic nephropathy has become a global health concern.9 Information about diabetic kidney disease (DKD) is scarce in Ethiopia, but the estimated prevalence of diabetic nephropathy is 6–16% in Sub-Saharan Africa and 6.1% in Ethiopia.10 Thus, understanding the association between serum total bilirubin and serum uric acid levels among Type 2 DM patients with diabetic kidney disease has a paramount importance. However, to our knowledge, no study has been documented yet in Ethiopia regarding the association between the two parameters among patients with diabetic kidney disease. Therefore, this study will supply baseline data for the country, from which further studies could be planned.
The health service organizations may also use the output of this research to plan, monitor, evaluate, and predict management outcomes and possible complications, which helps to improve health care services for Type 2 DM patients with nephropathy.
Methods
Study Design and Period
An institution-based comparative cross-sectional study was carried out from October 2020 to March 2021 at Ottena teaching and referral hospital, Southern Ethiopia, to assess the association of serum total bilirubin and serum uric acid levels with low GFR diabetic kidney disease. Chronic kidney disease caused by DM is defined as a persistent estimated glomerular filtration rate (eGFR) of <60 mL per min per 1.73 m2. Hyperuricemia is a condition in which serum uric acid level is highly raised. Serum uric acid is more than 8.0 mg/dL (for adult males) and more than 6.2 mg/dL (for adult females).
Study Population and Variables
All Type 2 DM patients attending Ottena referral hospital during the study period were taken as the source population. Renal functional tests such as serum creatinine and eGFR were taken as dependent variables of the study. HIV positive patients, patients with a history of hepatic disorders, chronic pulmonary obstructive disease, patients taking uric acid lowering drugs and those with cardio-vascular disease were excluded from the study.
Sample Size Determination
The total sample size was calculated using StatCalc-Epi-info for a comparative cross-sectional study by double proportion formula taking into account the following assumptions: 2-sided confidence level at 95% confidence interval, power of 80% and 1:3 ratios. Hypothetical mean values of serum bilirubin among diabetic patients with diabetic kidney disease and without diabetic kidney disease were taken as 9.96±4.71 and 12.46±5.35, respectively.11 Taking 10% as the non-respondent rate, a total of 200 study participants, 58 with diabetic kidney disease and 142 without diabetic kidney disease, were included in the study.
Sampling Technique and Procedure
A consecutive sampling technique was used. A structured questionnaire was used for data collection. Every client who visited the Diabetic clinic during the study period was evaluated by the data collectors for eligibility criteria. Finally, 5 mL of venous blood was drawn by venipuncture by a trained lab-technologist aseptically and immediately sent to the clinical laboratory for analysis.
Data Management and Statistical Analysis
Data analysis was carried out using SPSS version 16 statistical software package. Categorical and discrete variables were described as frequency and percentage, and comparisons of the categorical variables were made using Chi-Square tests. A Q-Q plot was used to assess the normality of distribution of both serum total bilirubin (STBIL) and uric acid. Bilirubin level was not normally distributed and it was log transformed. Pearson’s correlation, multiple linear regression models and Binary logistic regression analyses were performed. P-value<0.05 was accepted as statistically significant.
Assay Method and Instrument
Serum total bilirubin, uric acid, and creatinine were measured spectrophotometrically using assay standard kits. Absorbance was measured spectrophotometrically at 500 nm using COBAS INTEGRA 400 PLUS instrument (Roche, Germany). The manufacturers protocols and procedures were followed during the assay.
Ethics Statement
The research was conducted after obtaining ethical clearance from the Institutional Review Board of Addis Ababa University, college of health sciences and Department of Medical Biochemistry. All the principles of ethics like confidentiality were strictly observed and consent was obtained from study participants. Standard clinical and laboratory procedures were also followed during sample collection and analyses. This study complies with the Declaration of Helsinki.
Results
A total of 200 study participants diagnosed with Type 2 DM (58 with DKD and 142 without DKD) were recruited in this study. The mean±SD ages of patients with DKD and without DKD were 45.71±11.60 and 41.23±13.47, respectively, with a significant mean value difference (p=0.028).
Serum Total Bilirubin Level of Study Participants
The mean±SD serum total bilirubin of patients with DKD and without DKD were 0.15±2.29 and 0.19±2.26, respectively, with significant difference (p=0.035). Out of 200 study participants, 98, ie, 37 with DKD and 61 without DKD, had low serum total bilirubin level, whereas the remaining 102, ie, 21 with DKD and 81 without DKD, had a high serum total bilirubin level.
Serum Uric Acid Level of Study Participants
The mean±SD serum uric acid of patients with DKD and without DKD were 7.13±2.21 and 5.24±1.92, respectively, with significant mean value difference. Out of 200 study participants, 99, ie, 20 with DKD and 79 without DKD, had low serum uric acid level, whereas the remaining 101, ie, 38 with DKD and 63 without DKD, had high serum uric acid level.
Estimated Glomerular Filtration Rates (GFR) of Participants
According to eGFR calculated using serum creatinine level, out of 200 study participants, 128 (64.0%) had normal or elevated GFR (≥90 mL/min/1.73 m2), 14 (7.0%) had mild GFR reduction (GFR=60–89 mL/min/1.73 m2), 28 (14.0%) moderately decreased GFR (GFR=30–59 mL/min/1.73 m2), 25 (12.5%) had severe GFR reduction (GFR=15–29 mL/min/1.73 m2), and the remaining five (2.5%) study participants had stage five kidney disease (GFR<15 mL/min/1.73 m2).
No correlation was observed between serum total bilirubin level and socio-demographic and clinical characteristics like: residence duration of diabetes, BMI, SBP, DBP, and serum creatinine (Table 1).
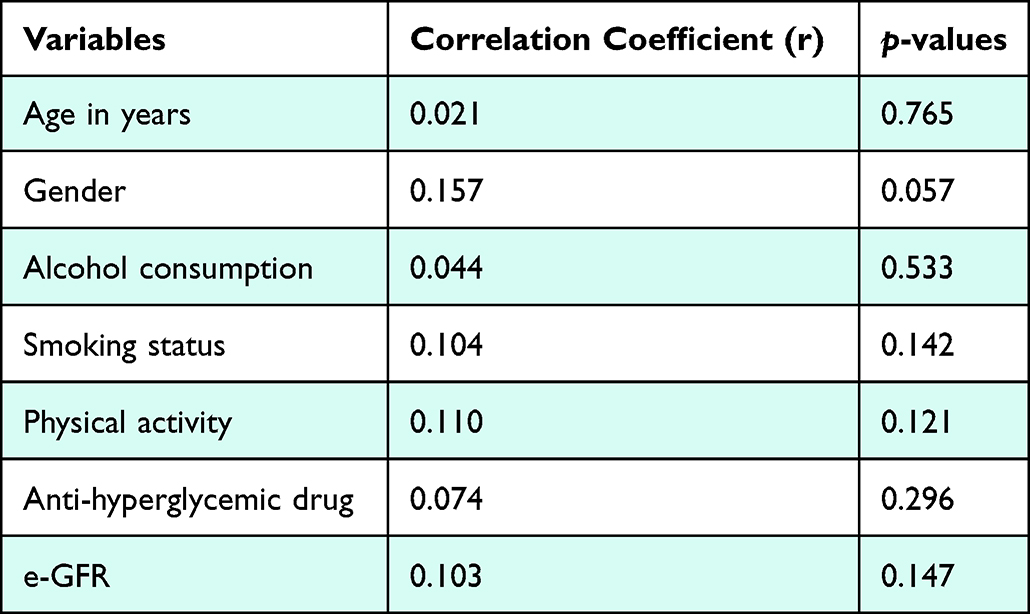 |
Table 1 Correlation Between Serum Total Bilirubin Level (Mg/dL) and Independent Variables |
A significant positive correlation was observed between serum uric acid level and independent variables like: age (r=0.234, p=0.001), smoking (r=0.214, p=0.002), duration of diabetes (r=0.142, p=0.045), BMI (r=0.289, p=0.001), and serum creatinine (r=0.147, p=0.001) (Table 2).
 |
Table 2 Correlation Between Serum Uric Acid Level (Mg/Dl) and Independent Variables |
Smoking, duration of diabetes ≥10, BMI≥25 kg/m2, systolic BP (SBP)≥140 mmHg, and diastolic BP (DBP)≥90 mmHg are significantly associated with DKD (Table 3).
 |
Table 3 Association of Socio-Demographic and Clinical Characteristics with DKD in T2DM |
Low serum total bilirubin was significantly associated with increased risk of diabetic kidney disease in both unadjusted and adjusted models. On the other hand, high serum uric acid was also significantly associated with increased risk of diabetic kidney disease in both unadjusted (p=0.007) and adjusted models (p=0.034). The crude odds ratio (COR) and adjusted odds ratio (AOR) of high versus low serum uric acid (SUA≥5.15 mg/dL vs SUA<5.15 mg/dL) for diabetic kidney disease are 2.38 (95% CI=1.26–4.49) and 2.09 (95% CI=1.06–4.12), respectively.
Subgroup effects of serum total bilirubin and serum uric acid on diabetic kidney disease were also investigated. High serum uric acid was significantly associated with increased risk of diabetic kidney disease among patients with low serum total bilirubin. The crude odds ratio (COR) and adjusted odds ratio (AOR) of high versus low serum uric acid (SUA≥5.15 mg/dL vs SUA<5.15 mg/dL) for diabetic kidney disease are 1.17 (95% CI=0.63–4.39) and 1.31 (95% CI=0.45–3.80), respectively, among patients with high serum total bilirubin and COR=2.98 (95% CI=1.25–7.08) and AOR=3.49 (95% CI=1.29–9.42), respectively, among patients with low serum total bilirubin.
On the other hand low serum total bilirubin level was significantly associated with increased risk of diabetic kidney disease among patients with high serum uric acid. The crude odds ratio (COR) and adjusted odds ratio (AOR) of low versus high serum total bilirubin (STBIL<0.16 mg/dL vs STBIL≥0.16 mg/dL) for diabetic kidney disease is COR=2.89 (95% CI=1.24–6.73) and AOR=2.55 (95% CI=1.05–6.19), respectively, among patients with high serum uric acid and COR=1.62 (95% CI=0.60–4.34) and AOR=1.48 (95% CI=0.49–4.42), respectively, among patients with low serum uric acid.
Discussion
Diabetes Mellitus is one of the most common endocrine diseases and a big health challenge in the world, especially in developing countries.12 Diabetic kidney disease is one of the major complications of Type 2 diabetes, it occurs in 20–40% of patients with diabetes and is the most common cause of end-stage renal disease.13 In this study, mean serum total bilirubin level was observed to be significantly different (p=0.035) between the DN and non-DN group. The mean±SD serum total bilirubin of patients with DKD and without DKD were 0.15±2.29 and 0.19±2.26, respectively. Our result is supported by a study done by Hamamoto et al,14 who reported that total bilirubin levels in patients with diabetic nephropathy were significantly lower than in those without diabetic kidney disease.
The results of the present study indicated that the serum total bilirubin negatively correlated with serum creatinine (r=−0.132, p=0.062) and positively correlated with e-GFR (r=0.103, p=0.147), but the correlation was non-significant. Contrary to our findings, many studies have reported a statistically significant and positive correlation between serum total bilirubin level and e-GFR.15–17 In addition, Riphagen et al18 found a negative correlation between baseline serum bilirubin levels and the doubling of serum creatinine levels. The possible reason for these differences may be due to differences in study design, which is cross-sectional, and the sample size of the study participant.
In the present study it was observed that patients with low serum total bilirubin were significantly associated with risk of diabetic kidney disease. Patients having lower serum total bilirubin were found to be 2.23-times more likely to develop diabetic kidney disease than patients with a high serum total bilirubin level. This is supported by the findings of Takeaki et al.19
Uric acid (UA) is the end product of purine metabolism in humans, and its high serum levels (hyperuricemia) are classically related to the precipitation of crystals in the joints, leading to arthritis.20 In our study it was observed that there is a significant mean value difference (p<0.001) and the serum uric acid level was observed to be higher in patients with diabetic nephropathy. The mean±SD serum uric acid of patients with DKD and without DKD were 7.13±2.21 and 5.24±1.92, respectively. Our finding is supported by a study done by Razi et al,21 who reported that serum uric acid levels in patients with diabetic kidney disease were significantly higher than those without diabetic kidney disease (p<0.005).
It was also observed that a significant positive correlation existed between serum uric acid and serum creatinine (r=0.497, p=0.001) with a significant negative correlation between serum uric acid and e-GFR (r=−0.501, p=0.001). Our result is in line with other studies. In a prospective observational study on Japanese patients with type 2 DM, high serum uric acid concentration was associated with reduced GFR in 12 months.22 In this study it was also observed that patients with high serum uric acid were significantly associated with risk of diabetic kidney disease.
In our study it was observed that high serum uric acid was significantly associated (p=0.014) with increased risk of diabetic kidney disease among patients with low serum total bilirubin level. On the other hand low serum total bilirubin level was significantly associated (p=0.038) with increased risk of diabetic kidney disease among patients with high serum uric acid level. Our results also indicated that the co-presence of low serum total bilirubin and high serum uric acid is more associated with risk of diabetic kidney disease than that of low serum total bilirubin and high serum uric acid alone; which is supported by the findings of Ren et al,2 who revealed the co-presence of high serum uric acid and low serum total bilirubin level with two-fold micro vascular risk for those with co-presence of low serum uric acid and high serum total bilirubin compared to low serum total bilirubin or high serum uric acid alone.
It is fundamental to acknowledge that uric acid is associated with an increase in insulin resistance,23 which in turn is responsible for worsening diabetes and increased complication onset.
Based on our findings, the following recommendations can be suggested. First, further prospective studies need to be conducted to clearly show the association of serum total bilirubin and serum uric acid with diabetic kidney disease. Second, given the increasing risk of diabetic kidney disease in a high proportion of Type 2 DM patients, we recommend clinicians give prior attention for patients with both low serum total bilirubin level and high serum uric acid level that might increase the risk for DKD and we also recommend regular screening among Type 2 diabetics. This study used only serum creatinine based eGFR to define diabetic kidney disease; other renal function tests such as urinary albumin were not analyzed due to limited resources, which is the major limitation of the study. We did not assess the dietary habit of patients and drugs taken by patients, which can affect the levels of serum uric acid, and this can be a limitation of the study.
Conclusion
The co-presence of low serum total bilirubin and high serum uric acid may be useful for stratification of diabetic kidney disease risk among patients with Type 2 DM.
Data Sharing Statement
Extra data is available on the data repository of Addis Ababa University library.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Institutional Research Review Board of the College of Health Sciences and also from the Research Review Committee of the Department of Biochemistry, Addis Ababa University. Written informed consent was obtained from all participants after a clear briefing of the purpose of the research.
Acknowledgment
Special thanks are extended to Addis Ababa University College of Health Sciences, Department of Biochemistry, Arba Minch University, Ottena teaching and referral hospital, Dr Lukas Dingato, Mr Temesgen Meja, Mr Feyissa Challa, Mr Bedilu, and the study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was supported by the graduate school of Addis Ababa University, Ethiopia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Oktayoglu GS, Basaraner H, Yanardag R, Bolkent S. The effects of combined treatment of antioxidants on the liver injury in STZ diabetic rats. Diges Dis Sci. 2009;54:538–546. doi:10.1007/s10620-008-0381-0
2. Ren Y, Gao L, Guo X, et al. Interactive effect of serum uric acid and total bilirubin for microvascular disease of type 2 diabetes in China. J Diabetes Complications. 2018;32(11):1000–1005. doi:10.1016/j.jdiacomp.2018.09.002
3. Donovan A, Brownlie A, Zhou Y, et al. Positional cloning of zebrafish ferroportin1 identifies a conserved vertebrate iron exporter. Nature. 2000;403:776–781. doi:10.1038/35001596
4. Basiglio CL, Arriaga SM, Pelusa F, et al. Complement activation and disease: protective effects of hyperbilirubinemia. Clin Sci. 2010;118(2):99–113. doi:10.1042/CS20080540
5. Remedios C, Shah M, Bhasker AG, Lakdawala M. Hyperuricemia: a reality in the Indian obese. Obes Surg. 2012;22:945–948. doi:10.1007/s11695-012-0655-7
6. Franҫois RR, Guisan B. Renal transport of urate in humans. News Physiol Sci. 1999;14:80–84. doi:10.1152/physiologyonline.1999.14.2.80
7. Alvarez-Lario B, Macarron-Vicente J. Uric acid and evolution. Rheumatology. 2010;49:2010–2015. doi:10.1093/rheumatology/keq204
8. International Diabetes Federation. International Diabetes Federation Atlas.
9. Wan Q, Xu Y, Dong E. Diabetic nephropathy research in China: data analysis and review from the National Natural Science Foundation of China. J Diabetes. 2015;7(3):307–314. doi:10.1111/1753-0407.12265
10. Yirsaw B. Chronic kidney disease in sub-Saharan Africa: hypothesis for research demand. Ann Afr Med. 2012;11(2):119. doi:10.4103/1596-3519.93537
11. Shen Y, Zhang H, Li G, et al. The analysis on serum bilirubin levels in different stages diabetic nephropathy patients. Clin Focus. 2010;2010:329–331.
12. Bandarian F, Omidvar M, Farideh R, Nasli-Esfahani E, Saeedi S, Larijani B. Iran diabetes research roadmap (IDRR) study; knowledge gap in Genetic research on diabetes mellitus in Iran: a review article. Iran J Public Health. 2017;46:53–59.
13. Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease: a report from an ADA consensus conference. Diabetes Care. 2014;37:2864–2883. doi:10.2337/dc14-1296
14. Hamamoto S, Kaneto H, Kamei S, et al. Low bilirubin levels are an independent risk factor for diabetic retinopathy and nephropathy in Japanese patients with type 2 diabetes. Diabetes Metab. 2015;41(5):429–431.
15. Fukui M, Tanaka M, Shiraishi E, et al. Relationship between serum bilirubin and albuminuria in patients with type 2 diabetes. Kidney Int. 2008;74(9):1197–1201. doi:10.1038/ki.2008.398
16. Hwang HJ, Kim SH. Inverse relationship between fasting direct bilirubin and metabolic syndrome in Korean adults. Clin Chim Acta. 2010;411:1496–1501. doi:10.1016/j.cca.2010.06.003
17. Mashitani T, Hayashino Y, Okamura S, Tsujii S, Ishii H. Correlations between serum bilirubin levels and diabetic nephropathy progression among Japanese type 2 diabetic patients: a prospective cohort study. Diabetes Care. 2014;37:252–258. doi:10.2337/dc13-0407
18. Riphagen IJ, Deetman PE, Bakker SJ, et al. Bilirubin and progression of nephropathy in type 2 diabetes: a post hoc analysis of RENAAL with independent replication in IDNT. Diabetes. 2014;63:2845–2853. doi:10.2337/db13-1652
19. Katoh T, Kawamoto R, Kohara K, Miki T. Association between serum bilirubin and estimated glomerular filtration rate among diabetic patients. Int Scholar Res Not. 2015. doi:10.1155/2015/480418
20. Rymal E, Rizzolo D. Gout: a comprehensive review. JAAPA. 2014;27:26–31. doi:10.1097/01.JAA.0000453233.24754.ec
21. Salman R, Avais J, Allesandro P, et al. Thyroid hormones and cardiovascular function and diseases. JACC. 2018;71(16):1781–1796. doi:10.1016/j.jacc.2018.02.045
22. Ito H, Abe M, Mifune M, et al. Hyperuricemia is independently associated with coronary heart disease and renal dysfunction in patients with type 2 diabetes mellitus. PLoS One. 2011;6:27817. doi:10.1371/journal.pone.0027817
23. Xingyong W, Chengfu X, Yiming L, et al. Uric acid regulates hepatic steatosis and insulin resistance through the NLRP3 inflammasome-dependent mechanism. J Hepatol. 2016;64(4):925–932. doi:10.1016/j.jhep.2015.11.022
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.