Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Association of Serum Cholinesterase with Contrast-Associated Acute Kidney Injury and Adverse Outcomes in Percutaneous Coronary Intervention Patients
Authors Zhang LW, Zeng JL, Wang CX, Luo MQ, Lin KY, Guo Y
Received 20 January 2025
Accepted for publication 12 May 2025
Published 24 October 2025 Volume 2025:21 Pages 1499—1508
DOI https://doi.org/10.2147/TCRM.S514823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Li-Wei Zhang,1– 3,* Ji-Lang Zeng,4,* Chang-Xi Wang,1– 3,* Man-Qing Luo,5 Kai-Yang Lin,1– 3 Yansong Guo1– 3
1Department of Cardiology, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou University Affiliated Provincial Hospital, Fuzhou, People’s Republic of China; 2Fujian Provincial Key Laboratory of Cardiovascular Disease, Fujian Provincial Center for Geriatrics, Fujian Provincial Clinical Research Center for Severe Acute Cardiovascular Diseases, Fuzhou, People’s Republic of China; 3Fujian Heart Failure Center Alliance, Fuzhou, People’s Republic of China; 4Department of Cardiology, Fujian Medical University Union Hospital, Fuzhou, People’s Republic of China; 5Department of Cardiology, Fuwai Hospital, National Clinical Research Center for Cardiovascular Diseases, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yansong Guo, Department of Cardiology, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou University Affiliated Provincial Hospital, 134 East Street, Gulou District, Fuzhou, Fujian, 350001, People’s Republic of China, Fax +86-591-87557768, Email [email protected] Kai-Yang Lin, Department of Cardiology, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou University Affiliated Provincial Hospital, 134 East Street, Gulou District, Fuzhou, Fujian, 350001, People’s Republic of China, Fax +86-591-87557768, Email [email protected]
Purpose: Serum cholinesterase (SChE) is a pleiotropic biomarker that is closely related to malnutrition, systemic inflammation, and hepatocyte injury. However, the utility of SChE in patients undergoing percutaneous coronary intervention (PCI) remains unclear. This study sought to investigate the associations between SChE and contrast-associated acute kidney injury (CA-AKI) as well as mortality in patients undergoing PCI.
Patients and Methods: We retrospectively observed 1,696 patients at a tertiary hospital from January 2016 to December 2018. CA-AKI was defined as an increase in serum creatinine ≥ 50% or 0.3 mg/dL within 48 h after contrast medium exposure.
Results: During hospitalization, 198 patients (11.7%) developed CA-AKI. Restricted cubic spline (RCS) and receiver operating characteristic (ROC) analysis demonstrated that SChE levels were negatively correlated with CA-AKI and had predictive value (AUC, 0.655; 95% CI, 0.613– 0.697). Multivariable regression analysis showed that patients in low-SChE group (≤ 7.5 kU/L) had a higher risk of developing CA-AKI (OR, 1.80; 95% CI, 1.21– 2.67) compared to those in the high-SChE group (> 7.5 kU/L). Regarding prognosis, SChE levels were also negatively associated with long-term mortality and were capable of predicting 90-day mortality (AUC, 0.826; 95% CI, 0.760– 0.892). Patients in the low-SChE group had significantly higher long-term mortality risks (HR, 2.56; 95% CI, 1.55– 4.32). Mediation analyses further indicated that CA-AKI partially mediated the relationship between SChE and short-term mortality, with a mediation proportion of 12.79%.
Conclusion: Low SChE is an independent risk factor for CA-AKI and a poor prognosis after PCI. Short-term mortality associated with SChE levels is partially mediated through the occurrence of CA-AKI. It is recommended that clinicians evaluate SChE levels prior to PCI and adjust hydration therapy according to SChE levels.
Keywords: serum cholinesterase, percutaneous coronary intervention, contrast-associated acute kidney injury, prognosis, mediation analyses
Introduction
Despite advances in medical technology, cardiovascular disease (CVD) remains the leading cause of mortality worldwide. According to the data for 2019, the age-adjusted mortality from CVD in the United States was 214.6 cases per 100, 000 people.1 Over the past few decades, significant progress has been achieved in the prevention and treatment of CVD, particularly through the application of percutaneous coronary intervention (PCI), resulting in a substantial reduction in CVD mortality.2 However, PCI procedures may also give rise to complications, including contrast-associated acute kidney injury (CA-AKI), which is the third major pathogenic factor of acute kidney injury.3 The occurrence of CA-AKI is associated with renal function deterioration and both short- and long-term mortality.3,4 At present, the main prevention and treatment strategy for CA-AKI is to identify risk factors and provide hydration for high-risk populations.5
Serum cholinesterase (SChE), synthesized in the liver, serves as a pleiotropic biomarker linked to malnutrition, systemic inflammation, and hepatocyte injury.6,7 Previously, SChE was included in the Vienna and Ludwigshafen Coronary Artery Disease (VILCAD) risk score8 to predict the risk of mortality in stable coronary heart disease patients. In subsequent study,9 the predictive role of SChE on prognosis was extended to the population of acute coronary syndrome. The relationship between SChE and cardiovascular diseases has recently received increasing attention, particularly its potential prognostic predictive value for patients with heart failure.10,11 Recently, evidence has demonstrated that SChE levels can effectively forecast adverse outcomes in patients with decompensated heart failure.12
However, there are few studies investigating the correlation between SChE levels with CA-AKI and poor prognosis in patients undergoing PCI. Our research was intended to evaluate whether the decrease in SChE serves as an independent risk factor for CA-AKI and adverse prognoses in PCI patients and its predictive value.
Materials and Methods
Study Population
This observational, retrospective, single-center study was conducted at a tertiary hospital in Fujian Province, China. It included a consecutive cohort of patients who underwent elective or emergency PCI between January 2016 and December 2018. We excluded the following patients from the analysis: (1) loss of SChE or serum creatinine (Scr) data; (2) with concomitant diseases (malignant tumors with a life expectancy of less than 1-year, severe liver dysfunction, eGFR less than 15 mL/min/1.73m2 or dialysis); (3) patients who were taking an oral SChE inhibitor at admission; (4) died within 72 hours after admission (Supplementary Figure 1). Finally, 1,696 patients were enrolled in this analysis. Baseline characteristics between patients excluded and included in this study were shown in Supplementary Table 1.
Study Protocol
Blood samples were collected after an overnight fast on the next morning after hospital admission, including routine blood examination, blood biochemical analysis, and other laboratory tests, including SChE and SCr. Furthermore, we continuously monitored SCr levels for two days after the PCI procedure. All laboratory tests were conducted in the central laboratory of Fujian Provincial Hospital and evaluated based on established reference ranges. The reference range for SChE is 5.0–12.0 kU/L. Additional patient data, such as demographic information including BMI, medical history, comorbidities, medication records, and PCI procedure information, were obtained from the electronic medical record system.
Percutaneous Coronary Intervention
All PCI procedures followed the AHA/ACC guidelines and were performed by experienced interventional cardiologists through radial or femoral artery access. Each patient provided informed consent before the procedure. All patients received nonionic and low-osmolar contrast, either ultravist or iopamiron, both with a concentration of 370 mgI/mL. In addition, hydration therapy entailed intravenous infusion of 0.9% normal saline at a rate of 1 mL/kg/h for 12 hours. If patients were unable to tolerate the standard rate, the hydration rate was reduced to 0.5 mL/kg/h.
Outcomes and Follow-Up
According to the Acute Kidney Injury Network (AKIN) criteria,13 CA-AKI was defined as an absolute increase in SCr of 0.3 mg/dL or a ≥50% increase in SCr within 48 hours after contrast exposure. Follow-up assessments were conducted at multiple time points, including one month, three months, and every six months post-discharge, facilitated by trained medical personnel through telephone interviews or outpatient visits. Follow-up data were accessible up to December 2021. The study encountered attrition, with 40 patients (2.4%) lost to follow-up at one month, 83 patients (4.9%) at 90 days, and 173 patients (10.2%) at one year.
Statistical Analysis
All patients were categorized into two groups: the low SChE group (≤7.5 kU/L) and the high SChE group (>7.5 kU/L), based on the optimal cut-off value determined by receiver operating characteristic (ROC) analysis. Data was described as mean ± standard deviations (SD) for normally distributed continuous variables, median and interquartile range (IQR) for abnormally distributed continuous variables, and numbers and percentages (%) for categorical variables. Differences between the two groups were identified using the ANOVA test (normally distributed continuous variables), Mann–Whitney U-test (abnormally distributed continuous variables), and chi-squared test or Fisher’s exact test (categorical variables).
Restricted cubic spline (RCS) functions with three knots were performed to detect the non-linear associations between SChE and CA-AKI as well as long-term mortality. Univariate logistic regressions were further performed to identify the risk factors associated with CA-AKI, and factors with P < 0.05 or significant clinical significance were retained in the multivariable regressions. Specifically, the multivariable logistic models were adjusted as follows: Model 1 was adjusted for age >75 years and sex. Model 2 included adjustments for Model 1 variables as well as hypertension, diabetes, congestive heart failure, atrial fibrillation, chronic kidney disease, AMI and anemia. Model 3 further accounted for hypotension and contrast medium (CM) volume >150 mL based on the variables in Model 2. Meanwhile, multicollinearity among all covariates was assessed using the variance inflation factor (VIF), and a VIF value of ≥5 indicated the presence of multicollinearity.
Regarding long-term mortality, the multivariable Cox regressions exhibited slight differences compared to logistic regressions. Specifically, Model 3 in the Cox regression involved adjustments for the variables included in Model 2, with additional considerations for factors such as multivessel disease, left ventricular ejection fraction (LVEF) < 40%, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker (ACEI/ARB), beta-blockers. The time-dependent ROC (tROC) curves and the corresponding AUCs at 90 days, 1 year, and 3 years were constructed to compare the predictive accuracy. Multivariable Cox proportional hazard models were then used to assess the predictive value of SChE for prognosis. Lastly, survival curves were analyzed by the Kaplan–Meier method, and Log rank tests were used to assess significance.
The mediation analysis was conducted using the R “mets” package version 1.3.2. To determine the proportion of the mediated effect, we calculated it by dividing the indirect effect by the total effect. E-values were calculated to evaluate unmeasured confounding effects.14 A larger E-value indicates that a substantial degree of unmeasured confounding would be required to explain away an effect estimate.
All statistical analyses were done using R software (version 4.3.0). Post-hoc power analysis indicated >90% power to detect clinically meaningful differences (α = 0.05) for all primary outcomes. Statistical significance was defined as a two-sided P value < 0.05.
Results
Baseline Characteristics
The average age of the overall study population was 64.4 ± 11.3 years, and 340 (20%) were female. SChE levels in the study population followed a normal distribution, with an average value of 8.5 ± 2.1 kU/L. Table 1 described the baseline characteristics of the low- and high-SChE groups. Compared to the high SChE group, participants in the low SChE group were older, more often men, and had a higher prevalence of congestive heart failure, chronic kidney disease, hypotension, and AMI. However, other comorbidities such as hypertension, diabetes, and prior myocardial infarction were similarly distributed between the two groups. In terms of laboratory findings, the low SChE group exhibited lower levels of hemoglobin, albumin, and LVEF, while having higher white blood cell count, D-dimer, and NT-proBNP levels. Additionally, they were more likely to receive emergency PCI treatment and diuretics therapy. Supplementary Table 2 displayed the baseline characteristics of patients with and without CA-AKI.
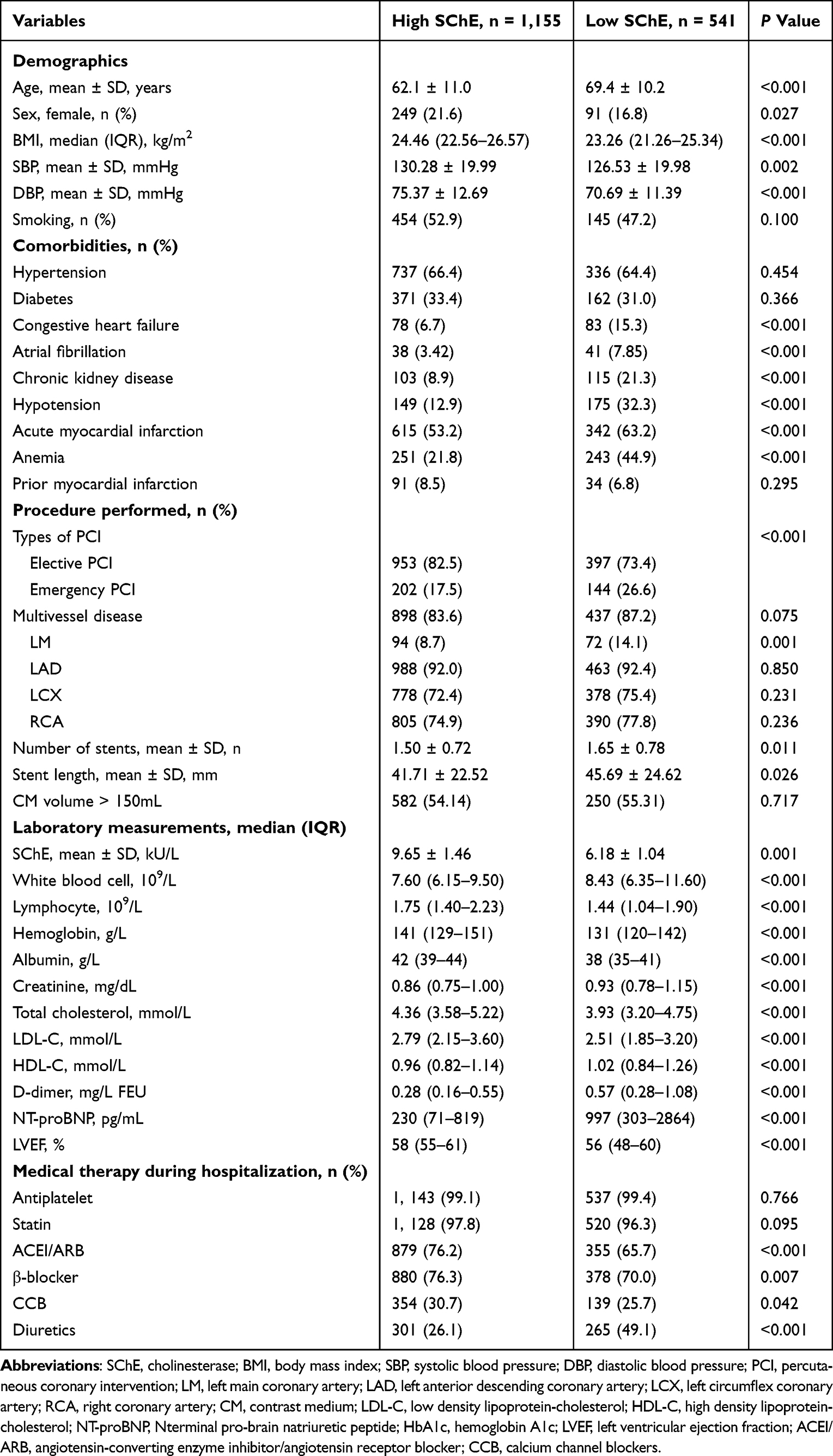 |
Table 1 Baseline Characteristics Between High- and Low-SChE Groups |
Predictive Value of SChE for CA-AKI
A total of 198 (11.7%) patients developed CA-AKI during hospitalization, and the incidence of CA-AKI was significantly higher in the low SChE group compared to the high SChE group (20.0% vs 7.8%, P < 0.001). The results of the ROC analysis indicated that SChE demonstrated predictive performance for CA-AKI, with an area under the curve (AUC) of 0.655 [95% Confidence Interval (CI): 0.613–0.697, Figure 1A] The RCS model further revealed a linear and negative correlation between SChE and CA-AKI (P for nonlinearity = 0.0853, Figure 1C).
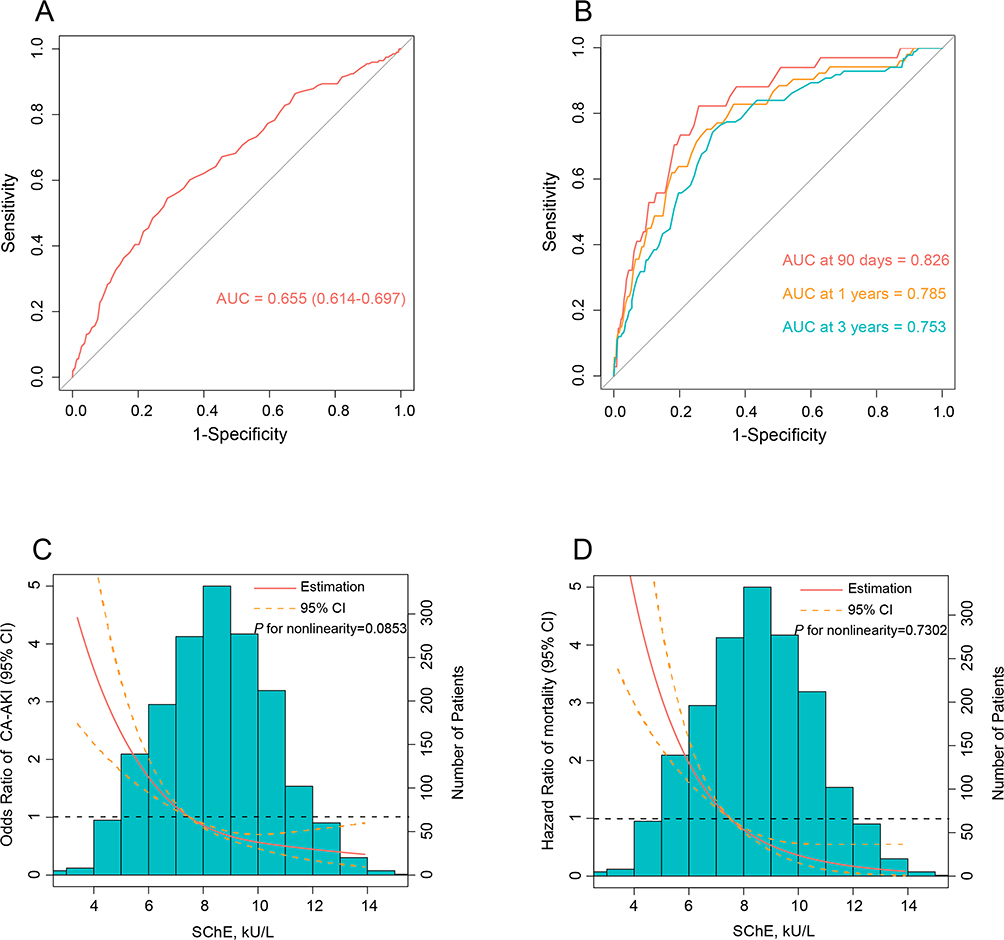 |
Figure 1 Predictive value of serum cholinesterase (SChE) for contrast-associated acute kidney injury (CA-AKI) and prognosis. Abbreviations: ROC, receiver operating characteristic; SChE, serum cholinesterase; CA-AKI, contrast-associated acute kidney injury; RCS, restricted cubic spline. Notes: (A) The ROC curve of SChE for CA-AKI. (B) The ROC curve of SChE for 90 days mortality, 1 year mortality and 3 years mortality. (C) RCS of the association between the SChE and CA-AKI. (D) RCS of the association between the SChE and prognosis. |
To further elucidate the predictive value of SChE for CA-AKI, three multivariable logistic regression models were constructed. Compared to higher SChE levels, lower SChE levels were consistently linked to a higher risk of CA-AKI across all three models (Table 2). In Model 3, after fully adjusting for covariates, patients with lower SChE levels exhibited an odds ratio (OR) of 1.80 for the risk of CA-AKI (95% CI: 1.21–2.67, P < 0.001, vs high SChE group). The multicollinearity analysis suggested that there was no collinearity among covariates (all VIF < 5).
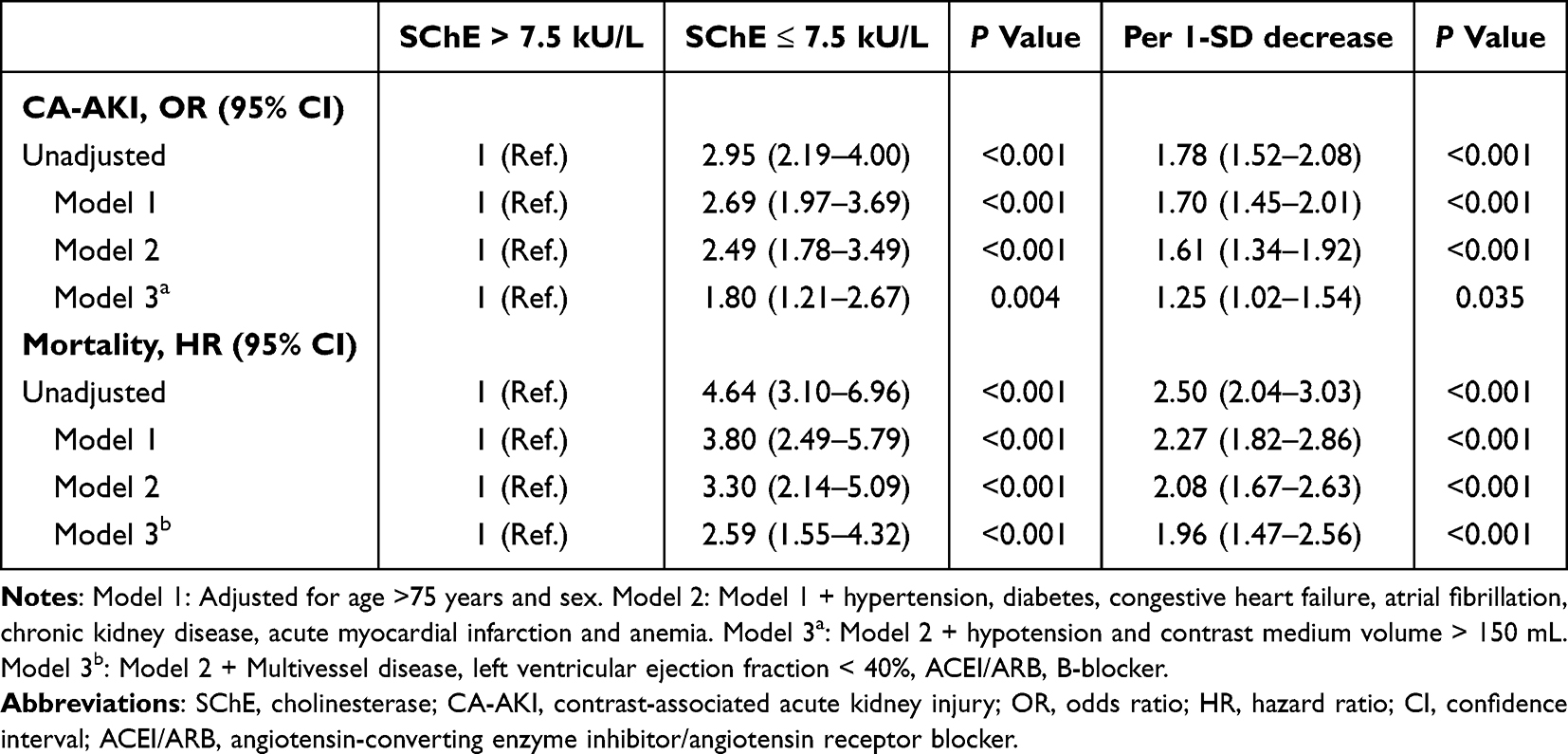 |
Table 2 The Relationship of SChE with CA-AKI and Prognosis |
Predictive Value of SChE for Mortality
After a median follow-up of 29.6 months, 113 (6.8%) patients died. The time-dependent ROC analysis demonstrated that SChE had a prognostic value for all-cause mortality, with an AUC of 0.826 at 90 days (95% CI, 0.760–0.892), 0.785 at 1 year (95% CI, 0.721–0.850), and 0.753 at 3 years (95% CI, 0.691–0.813) (Figure 1B). RCS in COX regression analysis indicated a linear association between SChE and mortality (P for nonlinearity = 0.7302, Figure 1D).
Univariate Cox regression analysis revealed that the low SChE group had a 4.64-fold higher risk of all-cause mortality compared to the high SChE group [(hazard ratio (HR), 4.64, 95% CI: 3.10–6.96, P < 0.001, Table 2] This difference was attenuated after further adjustment but remained significant in the fully adjusted model (Model 3, fully adjusted HR, 2.59; 95% CI, 1.55–4.32; P < 0.001). The Kaplan–Meier curves likewise showed that patients with lower SChE levels had significantly higher rates of all-cause mortality than those in the high SChE group (Log rank test, P < 0.001, Figure 2A). Besides, we observed a significant difference in the risk of all-cause mortality between patients with and without CA-AKI during hospitalization (Log rank test, P < 0.001, Figure 2B).
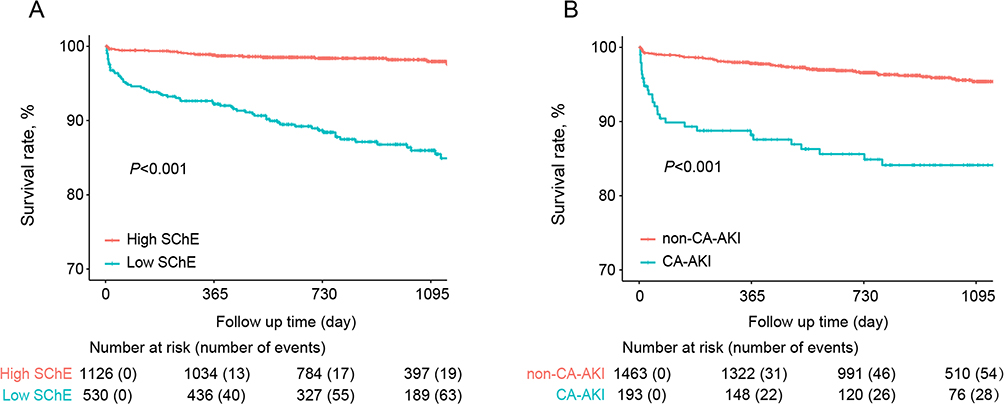 |
Figure 2 Kaplan–Meier curves for all-cause mortality. Abbreviations: SChE, serum cholinesterase; CA-AKI, contrast-associated acute kidney injury. Notes: (A) Survival difference between the low- and the high-SChE group. (B) Survival difference between the CA-AKI group and the non-CA-AKI group. |
Mediation Analysis
In accordance with Model 3, we conducted a comprehensive mediation analysis. The outcomes illuminated that CA-AKI served as a partial mediator in the connection between SChE and 90-day mortality, with a mediation proportion for 12.76%, as shown in Figure 3. Nevertheless, when extending the follow-up period from 90 days to 1 year, none of the mediation effects retained statistical significance.
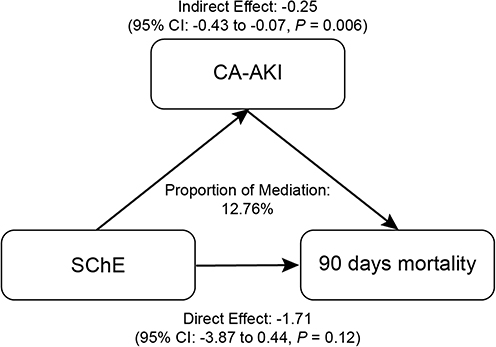 |
Figure 3 The mediating effects of CA-AKI between SChE and 90 days mortality. Abbreviations: SChE, serum cholinesterase; CA-AKI, contrast-associated acute kidney injury. |
Sensitivity Analysis
After excluding individuals with missing BMI data, we conducted a sensitivity analysis. The results aligned consistently with our primary findings. Specifically, Further adjusting for BMI, low SChE remained intensely associated with CA-AKI and prognosis (Supplementary Table 3).
The calculated E-values for CA-AKI were 3.0 (CI = 1.71) and for mortality were 4.62 (CI = 2.47), indicating that the observed correlation would be unlikely to disappear in the presence of unmeasured confounders.
Discussion
As far as we know, this is the first study to reveal the association between SChE and the incidence of CA-AKI and poor prognosis in PCI patients. Our study showcased the utility of SChE levels as a valuable predictor for both CA-AKI and prognosis in patients undergoing PCI. Furthermore, our findings revealed a significant association between SChE and short-term prognosis in PCI patients, with the development of CA-AKI partially mediating this relationship.
First, our research represented the first instance of uncovering a relationship between SChE levels and CA-AKI, a common post-PCI complication. The research findings showed that low SChE levels were an independent risk factor for CA-AKI. This discovery broadened the scope of SChE’s utility within the CVD population, and also provides new insights into the risk stratification of CA-AKI. In addition, identifying high-risk populations for CA-AKI and strengthening management is an important step in the prevention and treatment of CA-AKI.15 The currently identified risk factors for CA-AKI include old age, coronary artery disease type, eGFR, left ventricular ejection fraction, diabetes, hemoglobin, congestive heart failure, etc.16 In our study, the AUC for predicting CA-AKI using SChE was 0.655, indicating moderate predictive value. The predictive performance of SChE supports its consideration as a complementary parameter in future iterations of CA-AKI risk models. In terms of mechanism, low SChE reflects a state of systemic inflammation characterized by elevated pro-inflammatory cytokines such as IL-6 and TNF-α, which contribute to endothelial dysfunction, oxidative stress, and microvascular injury—key mechanisms in the development of CA-AKI.17 Additionally, SChE serves as a marker of malnutrition-inflammation syndrome, wherein hypoalbuminemia and metabolic derangements further predispose patients to hemodynamic instability, impaired contrast clearance, and reduced renal perfusion, thereby increasing susceptibility to AKI and adverse outcomes.18 Previously, it was believed that there was no specific treatment for CA-AKI, and the main preventive measures included reducing contrast agent dosage, hydration therapy, and opting for radial approach.19–22 Recently, the NITRATE-CIN23 study showed that in patients at risk of renal injury undergoing coronary angiography for acute coronary syndrome (ACS), a brief (5-day) regimen of once-daily inorganic nitrate administration significantly reduced the incidence of CA-AKI when compared to placebo. Consequently, treatment with inorganic nitrate may benefit high-risk patients, including those with low SChE level.
Furthermore, our study underscored the practicality and value of SChE in prognosticating patient outcomes following PCI. SChE exhibited predictive capabilities for mortality at various intervals: 90 days (AUC: 0.826), 1 year (AUC: 0.785), and 3 years (AUC: 0.753). The robust predictive capability of SChE for prognosis, though unexpected, was inherently reasonable. Prior studies, exemplified by the VILCAD score8 (comprising variables like age, LVEF, SChE, SCr, heart rate, and HbA1c), conducted on patients diagnosed with stable coronary artery disease, have consistently underscored SChE as the preeminent inverse risk factor. Besides, a cross-sectional study24 showed that SChE was associated with established cardiovascular risk factors, with SChE activity negatively correlated with age and positively correlated with serum albumin concentration. It was also associated with cholesterol, triglycerides, obesity, overweight, and body fat distribution. Additionally, several studies25,26 have observed an association between SChE activity and metabolic risk factors such as obesity, hyperlipidemia, and diabetes. The association between SChE and various cardiovascular risk factors may partially explain the relationship between SChE and cardiovascular mortality. These cumulative findings offered compelling support for both the clinical adoption of SChE. Additionally, the association between low SChE and adverse outcomes likely reflects the convergence of multiple pathological pathways. In coronary heart disease, especially in patients with ACS, there is oxidative stress, neurohormonal activation, and a systemic inflammatory state, which can lead to insulin resistance, protein and lipid metabolic dysfunction, reduced synthetic metabolism, and an imbalance between synthetic and catabolic metabolism.2,27 In this case, SChE levels are a better multifaceted biomarker because they reflect various factors such as malnutrition, systemic inflammation, and liver cell damage.28,29 Furthermore, cholinesterase is extensively utilized in clinical settings, featuring low cost and high accessibility, and thus presenting a favorable application outlook.30
Our study demonstrated a significant relationship between SChE levels, CA-AKI, and prognosis in PCI patients. Through mediation analysis, we further explored the role of CA-AKI in this process, designating 90-day mortality as the endpoint. The results revealed that CA-AKI partially mediated the effect of SChE on short-term prognosis, with a mediation proportion of 12.79%. This indicates that while CA-AKI contributes to the impact of SChE on prognosis, its role is relatively minor. While this suggests that preventing CA-AKI could modestly reduce mortality risk in patients with low SChE, the majority of the association appears to be driven by other factors, such as systemic inflammation, malnutrition, or underlying liver dysfunction. This underscores the importance of a comprehensive management approach that not only targets CA-AKI prevention—through strategies like optimized hydration and contrast minimization—but also addresses the broader systemic conditions associated with low SChE, such as nutritional support and management of comorbidities like heart failure. Interestingly, when the follow-up period was extended to one year, the mediation effect of CA-AKI disappeared. This phenomenon may be explained by the transient and partially reversible nature of CA-AKI’s effects, which are primarily linked to short-term outcomes.31 These findings suggest that while CA-AKI is an important factor in the acute phase, its long-term impact may be limited. Future research should investigate other mechanisms through which SChE influences prognosis, as well as explore potential interventions to mitigate CA-AKI’s short-term effects.
These findings have important clinical implications. First, SChE measurement could be incorporated into pre-PCI risk assessment to identify patients who may benefit from enhanced renal protection strategies. Second, the persistent association between low SChE and long-term mortality highlights the need for comprehensive management of these patients, including nutritional support, anti-inflammatory therapies, and close follow-up for comorbidities like heart failure and liver disease. Future studies should evaluate whether SChE-guided management protocols can improve clinical outcomes in PCI patients.
This study exhibits several limitations. Firstly, its observational design within a single-center cohort implies the potential introduction of bias. Secondly, despite meticulous adjustments for potential confounding factors, there might still exist unknown confounding factors. Nevertheless, in the sensitivity analysis, we employed the E-value to assess the possible influence of potential confounding factors on the results of this study. The relatively large E-value indicates that it is improbable for unknown factors to alter the conclusions of this study. Thirdly, SChE was only measured upon admission, lacking follow-up data. Evidently, this does not affect the relationship between SChE and CA-AKI, but it precludes further analysis of the relationship between the dynamic changes of SChE and prognosis. In future research, the dynamic changes of cholinesterase and its comparison with other biomarkers should be further considered to provide more evidence for the clinical application of SChE.
Conclusion
Low SChE is an independent risk factor for CA-AKI and a poor prognosis after PCI. Short-term mortality associated with SChE levels is partially mediated through the occurrence of CA-AKI.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study conformed to the Declaration of Helsinki and was approved by the Ethics Committee of the Fujian Provincial Hospital, China (ethics approval number: K2019-07-011). Due to the retrospective design of this study, the ethical committee waived the requirement for informed consent. To ensure the protection of patients’ privacy, all data that could potentially identify individual patients, such as names and addresses, were removed before analysis.
Funding
This study was funded by grants from National Natural Science Foundation of China General Program (Grant number: 82171569, 82470335), Natural Science Foundation of Fujian Province (Grant number: 2023J01176), Heart Failure Center Research Foundation of Fujian Provincial Hospital (supported by Fujian Provincial Department of Finance), National Key Clinical Specialty Construction Project of China (Cardiovascular Medicine 2021), Cardiovascular Disease Clinical and Research Platform (National Regional Medical Center). The grants had no role in the design of the study, collection of data, interpretation of data.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics-2021 update: a report from the American heart association. Circulation. 2021;143(8):e254–e743. doi:10.1161/CIR.0000000000000950
2. Bhatt DL, Lopes RD, Harrington RA. Diagnosis and treatment of acute coronary syndromes: a review. JAMA. 2022;327(7):662–675. doi:10.1001/jama.2022.0358
3. Weisbord SD, Palevsky PM, Kaufman JS, et al. Contrast-associated acute kidney injury and serious adverse outcomes following angiography. J Am Coll Cardiol. 2020;75(11):1311–1320. doi:10.1016/j.jacc.2020.01.023
4. Giacoppo D, Madhavan MV, Baber U, et al. Impact of contrast-induced acute kidney injury after percutaneous coronary intervention on short- and long-term outcomes: pooled analysis from the HORIZONS-AMI and ACUITY trials. Circ Cardiovasc Interv. 2015;8(8):e002475. doi:10.1161/CIRCINTERVENTIONS.114.002475
5. Liu Y, Tan N, Huo Y, et al. Simplified rapid hydration prevents contrast-associated acute kidney injury among CKD patients undergoing coronary angiography. JACC. 2023;16(12):1503–1513. doi:10.1016/j.jcin.2023.03.025
6. Davis L, Britten JJ, Morgan M. Its significance in anaesthetic practice. Anaesthesia. 1997;52(3):244–260. doi:10.1111/j.1365-2044.1997.084-az0080.x
7. Santarpia L, Grandone I, Contaldo F, Pasanisi F. Butyrylcholinesterase as a prognostic marker: a review of the literature. J Cachexia Sarcopenia Muscle. 2013;4(1):31–39. doi:10.1007/s13539-012-0083-5
8. Goliasch G, Kleber ME, Richter B, et al. Routinely available biomarkers improve prediction of long-term mortality in stable coronary artery disease: the vienna and ludwigshafen coronary artery disease (VILCAD) risk score. Eur Heart J. 2012;33(18):2282–2289. doi:10.1093/eurheartj/ehs164
9. Goliasch G, Haschemi A, Marculescu R, et al. Butyrylcholinesterase activity predicts long-term survival in patients with coronary artery disease. Clin Chem. 2012;58(6):1055–1058. doi:10.1373/clinchem.2011.175984
10. Seo M, Yamada T, Tamaki S, et al. Prognostic significance of serum cholinesterase in patients with acute decompensated heart failure: a prospective comparative study with other nutritional indices. Am J Clin Nutr. 2019;110(2):330–339. doi:10.1093/ajcn/nqz103
11. Shiba M, Kato T, Morimoto T, et al. Serum cholinesterase as a prognostic biomarker for acute heart failure. Eur Heart J Acute Cardiovasc Care. 2021;10(3):335–342. doi:10.1093/ehjacc/zuaa043
12. Seo M, Yamada T, Tamaki S, et al. Prognostic significance of serum cholinesterase level in patients with acute decompensated heart failure with preserved ejection fraction: insights from the PURSUIT-HFpEF registry. J Am Heart Assoc. 2020;9(1):e014100. doi:10.1161/JAHA.119.014100
13. Mehran R, Owen R, Chiarito M, et al. A contemporary simple risk score for prediction of contrast-associated acute kidney injury after percutaneous coronary intervention: derivation and validation from an observational registry. Lancet. 2021;398(10315):1974–1983. doi:10.1016/S0140-6736(21)02326-6
14. VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167(4):268–274. doi:10.7326/M16-2607
15. Landi A, Chiarito M, Branca M, et al. Validation of a contemporary acute kidney injury risk score in patients with acute coronary syndrome. JACC. 2023;16(15):1873–1886. doi:10.1016/j.jcin.2023.06.015
16. Ma B, Allen DW, Graham MM, et al. Comparative performance of prediction models for contrast-associated acute kidney injury after percutaneous coronary intervention. Circ Cardiovasc Qual Outcomes. 2019;12(11):e005854. doi:10.1161/CIRCOUTCOMES.119.005854
17. Seeliger E, Sendeski M, Rihal CS, et al. Contrast-induced kidney injury: mechanisms, risk factors, and prevention. Eur Heart J. 2012;33(16):2007–2015. doi:10.1093/eurheartj/ehr494
18. Zhang F, Lu Z, Wang F. Advances in the pathogenesis and prevention of contrast-induced nephropathy. Life Sci. 2020;259:118379. doi:10.1016/j.lfs.2020.118379
19. Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA guideline for the management of patients with chronic coronary disease: a report of the American heart association/American college of cardiology joint committee on clinical practice guidelines. Circulation. 2023;148(9):e9–e119. doi:10.1161/CIR.0000000000001168
20. Briguori C, D’Amore C, De Micco F, et al. Left ventricular end-diastolic pressure versus urine flow rate-guided hydration in preventing contrast-associated acute kidney injury. JACC. 2020;13(17):2065–2074. doi:10.1016/j.jcin.2020.04.051
21. Andò G, Gragnano F, Calabrò P, et al. Radial vs femoral access for the prevention of acute kidney injury (AKI) after coronary angiography or intervention: a systematic review and meta-analysis. Catheter Cardiovasc Interv. 2018;92(7):E518–E526. doi:10.1002/ccd.27903
22. Cesaro A, Moscarella E, Gragnano F, et al. Transradial access versus transfemoral access: a comparison of outcomes and efficacy in reducing hemorrhagic events. Expert Rev Cardiovasc Ther. 2019;17(6):435–447. doi:10.1080/14779072.2019.1627873
23. Jones DA, Beirne AM, Kelham M, et al. Inorganic nitrate benefits contrast-induced nephropathy after coronary angiography for acute coronary syndromes: the NITRATE-CIN trial. Eur Heart J. 2024;45(18):1647–1658. doi:10.1093/eurheartj/ehae100
24. Calderon-Margalit R, Adler B, Abramson JH, Gofin J, Kark JD. Butyrylcholinesterase activity, cardiovascular risk factors, and mortality in middle-aged and elderly men and women in Jerusalem. Clin Chem. 2006;52(5):845–852. doi:10.1373/clinchem.2005.059857
25. Alcântara VM, Chautard-Freire-Maia EA, Scartezini M, Cerci MS, Braun-Prado K, Picheth G. Butyrylcholinesterase activity and risk factors for coronary artery disease. Scand J Clin Lab Invest. 2002;62(5):399–404. doi:10.1080/00365510260296564
26. Vallianou NG, Evangelopoulos AA, Bountziouka V, et al. Association of butyrylcholinesterase with cardiometabolic risk factors among apparently healthy adults. J Cardiovasc Med. 2014;15(5):377–383. doi:10.2459/JCM.0b013e3283627700
27. Libby P. Pathogenesis of atherothrombotic events: from lumen to lesion and beyond. Circulation. 2024;150(16):1217–1219. doi:10.1161/CIRCULATIONAHA.124.070087
28. Xing S, Li Q, Xiong B, et al. Structure and therapeutic uses of butyrylcholinesterase: application in detoxification, Alzheimer’s disease, and fat metabolism. Med Res Rev. 2021;41(2):858–901. doi:10.1002/med.21745
29. Furtado-Alle L, Tureck LV, de Oliveira CS, Hortega J, Souza R. Butyrylcholinesterase and lipid metabolism: possible dual role in metabolic disorders. Chem Biol Interact. 2023;383:110680. doi:10.1016/j.cbi.2023.110680
30. Miao Y, He N, Zhu JJ. History and new developments of assays for cholinesterase activity and inhibition. Chem Rev. 2010;110(9):5216–5234. doi:10.1021/cr900214c
31. Kurogi K, Ishii M, Sakamoto K, et al. Persistent renal dysfunction in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. J Am Heart Assoc. 2019;8(23):e014096. doi:10.1161/JAHA.119.014096
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Value of Systemic Inflammation Score for Contrast-Associated Acute Kidney Injury and Adverse Outcomes Among Patients Undergoing Elective Percutaneous Coronary Intervention
Zeng JL, Xiang YF, Zhang LW, Chen LC, Chen JH, Liang WJ, You Z, Wang CX, Lin ZJ, Lin KY, Guo Y
Journal of Inflammation Research 2023, 16:2845-2854
Published Date: 8 July 2023
Association of Systemic Inflammatory Response Index and Pan-Immune-Inflammation-Value with Long-Term Adverse Cardiovascular Events in ST-Segment Elevation Myocardial Infarction Patients After Primary Percutaneous Coronary Intervention
Liu Y, Liu J, Liu L, Cao S, Jin T, Chen L, Wu G, Zong G
Journal of Inflammation Research 2023, 16:3437-3454
Published Date: 14 August 2023
Advanced Lung Cancer Inflammation Index for Predicting Prognostic Risk for Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention
Wang X, Wei C, Fan W, Sun L, Zhang Y, Sun Q, Liu Y, Liu J
Journal of Inflammation Research 2023, 16:3631-3641
Published Date: 23 August 2023
The Association of Intraindividual Difference Between Cystatin- and Creatinine-Based Estimated GFR and Contrast-Associated Acute Kidney Injury
Zhang LW, Luo MQ, Zeng JL, You ZB, Chen LC, Chen JH, Lin KY, Guo YS
Clinical Interventions in Aging 2024, 19:411-420
Published Date: 8 March 2024
Clinical Application of PINK1 and ACSL4 Protein Levels in the Acute Myocardial Infarction Patients and Prognosis Evaluation After PCI
Ao W, Duan P, Luo P, Xiang D, Wang Q, Ren Y, He Q
Research Reports in Clinical Cardiology 2024, 15:45-53
Published Date: 4 June 2024