Back to Journals » International Journal of Women's Health » Volume 17
Association of Regular and Weekend Warrior Physical Activity Patterns with Gynecologic Cancer Risk: A Cross-Sectional Study of NHANES 2007-2018
Authors Ye J, Zhang B, Yang Q, Zeng Q, Jin Q, Guo H, Lin H
Received 18 June 2025
Accepted for publication 11 October 2025
Published 4 November 2025 Volume 2025:17 Pages 4165—4175
DOI https://doi.org/10.2147/IJWH.S547839
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Jiahui Ye,1– 3 Bixia Zhang,2 Qi Yang,2 Qianru Zeng,2 Qilin Jin,1,2 Hua Guo,2 Hanmei Lin2
1Guangxi University of Chinese Medicine, Nanning, Guangxi Zhuang Autonomous Region, People’s Republic of China; 2Department of Gynecology, The First Affiliated Hospital of Guangxi University of Chinese Medicine, Nanning, Guangxi Zhuang Autonomous Region, People’s Republic of China; 3The Faculty of International Education of Guangxi University of Chinese Medicine, Guangxi University of Chinese Medicine, Nanning, Guangxi Zhuang Autonomous Region, People’s Republic of China
Correspondence: Hanmei Lin, Email [email protected] Hua Guo, Email [email protected]
Objective: The impact of different physical activity (PA) patterns, including the less-studied “weekend warrior” pattern, on gynecologic cancer risk remains unclear. This study aimed to examine the associations of regular and “weekend warrior” PA patterns with the risk of cervical cancer (CC), ovarian cancer (OC), and uterine cancer (UC).
Methods: A total of 13,675 women from the 2007– 2018 National Health and Nutrition Examination Survey (NHANES) cycles were included in this cross-sectional analysis. Weighted multivariable logistic regression models were applied to assess associations between PA patterns and the prevalence of gynecologic cancers. Subgroup analyses stratified by PA patterns and cancer subtypes were performed to explore potential interactions. In addition, restricted cubic spline (RCS) regression was used to examine possible nonlinear relationships between PA patterns and gynecologic cancer risk.
Results: Among the 13,675 participants, 331 women self-reported a gynecologic cancer diagnosis, including 172 cases of CC, 58 cases of OC, and 101 cases of UC. In fully adjusted models, regular PA was significantly associated with a lower prevalence of gynecologic cancers (OR = 0.635, 95% CI: 0.448– 0.901; p = 0.012), whereas the weekend warrior pattern PA showed a non-significant association with cancer risk (OR = 0.544, 95% CI: 0.162– 1.824, p = 0.32). RCS analysis demonstrated a significant nonlinear association between PA patterns and gynecologic cancer risk (p for nonlinearity < 0.001). Subgroup analyses further identified a significant interaction with race/ethnicity (p for interaction = 0.038).
Conclusion: Our findings suggest that regular PA may be inversely associated with the risk of gynecologic cancers. Although the weekend warrior PA pattern did not show a statistically significant association, the wide confidence interval indicates limited statistical power, and the true effect cannot be reliably estimated. These results highlight the potential importance of consistent PA for cancer prevention, while emphasizing the need for larger studies to clarify the impact of weekend warrior PA patterns.
Keywords: weekend warrior, physical activity, gynecologic, cancers, cervical cancer, ovarian cancer, endometrial cancer
Introduction
Globally, gynecologic cancers (GC) are among the most prevalent malignancies affecting women. Approximately 3.6 million new GC cases are diagnosed each year, resulting in about 1.3 million deaths worldwide.1 In 2020, GCs accounted for 15% of all new cancer cases and nearly 48% of all cancer-related deaths among women globally.2 Cervical cancer (CC), ovarian cancer (OC), and uterine cancer (UC) constitute the three major subtypes of GCs and represent the primary contributors to the global gynecologic cancer burden.3 These subtypes exhibit striking disparities in five-year relative survival rates, with OC having the lowest survival (50.9%) compared to CC (67.0%) and endometrial cancer (80.8%).4 GCs often have an insidious onset, are difficult to diagnose early, and involve complex treatment regimens with high recurrence rates. Consequently, they have become a significant public health concern, posing substantial threats to women’s health and placing heavy burdens on healthcare systems worldwide.5
Among modifiable lifestyle factors, physical activity (PA) has emerged as a key focus in GC prevention due to its adaptability and wide-ranging health benefits.6 The American Cancer Society (ACS) recommends that adults engage in at least 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity PA per week.6 In recent years, growing attention has been paid to the role of different PA patterns in relation to various disease risks.7,8 Although a previous cross-sectional study suggested that high-intensity PA may reduce the risk of breast cancer in adult women,9 the specific relationship between PA and GC remains unclear. Studies exploring the influence of PA duration and activity patterns on GC risk remain limited.
Given that modern populations often face increasingly demanding schedules, consolidating PA into weekends or leisure time has become a more practical approach. As daily exercise routines become harder to maintain, the “weekend warrior” (WW) PA pattern—defined as engaging in the recommended amount of aerobic activity concentrated in one or two sessions per week—has gained popularity,10 with its prevalence steadily rising.11 Previous studies have shown that the WW PA pattern is associated with reduced all-cause mortality, as well as decreased risks of cardiovascular disease and metabolic syndrome.12,13 However, evidence regarding the association between the WW PA pattern and the risk of GC remains sparse, and comprehensive data are largely lacking.
Given the significance of PA as a modifiable risk factor for GC, promoting PA has the potential to directly improve public health and quality of life. The primary objective of this study was to evaluate the association between different PA patterns—including the WW PA pattern and other PA patterns—and the prevalence of GC using data from the National Health and Nutrition Examination Survey (NHANES) in the United States. Since the NHANES database includes information only on three common types of GCs—CC, OC, and UC—the present study focused specifically on these subtypes. Additionally, our findings aim to inform PA recommendations tailored to adults with limited time for exercise, offering evidence-based guidance for cancer prevention in real-world settings.
Methods
Study Design and Population
Data were obtained from the NHANES spanning the years 2007 to 2018. NHANES is a nationally representative, cross-sectional survey conducted in the United States to assess the health and nutritional status of individuals across all age groups and ethnic backgrounds. This high-quality survey integrates data from demographic interviews, dietary assessments, physical examinations, laboratory tests, and structured questionnaires. The NHANES study protocol was approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board, and all participants provided written informed consent. According to the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (China, February 18, 2023), this secondary analysis of de-identified, publicly available data is exempt from additional ethical approval, in line with Article 32, Items 1 and 2.14
Initially, 59,842 participants from the 2007-2018 NHANES cycles met the preliminary inclusion criteria. After excluding individuals under 18 years of age (n=23,262), 36,580 adult participants remained. The sample was then restricted to females, resulting in 18,797 individuals. Following the exclusion of participants with missing cancer diagnosis information and those with missing data on covariates, the final analytic sample consisted of 13,675 participants. The participant selection process is shown in Figure 1.
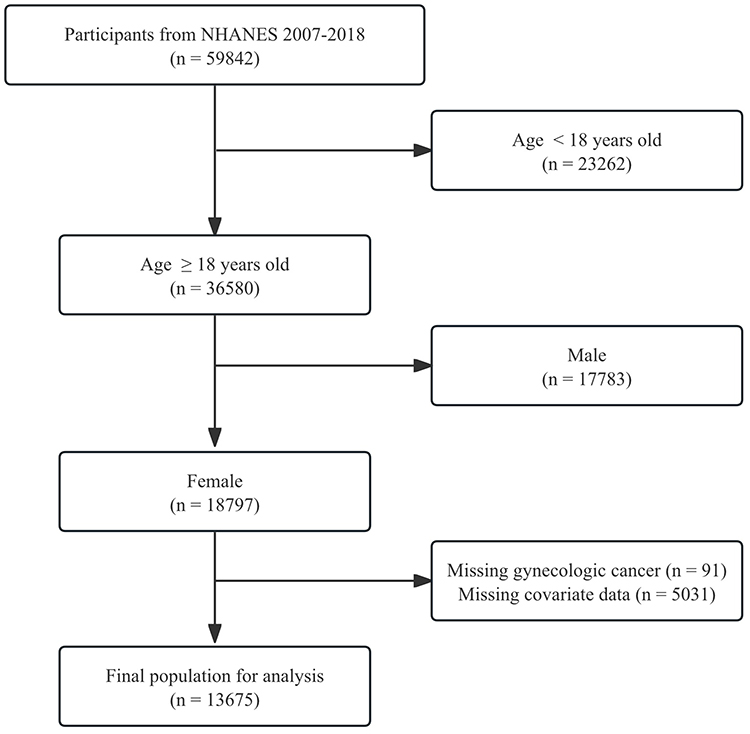 |
Figure 1 Flow chart of the study design. |
Definition of Gynecologic Cancer (GC)
Information on GC diagnoses was obtained through a structured questionnaire. Participants were asked whether they had ever been told by a health professional that they had cancer or a malignancy (MCQ-220). Those who responded affirmatively were further asked to specify the type of cancer (MCQ-230A). In this coding system, CC was coded as 15, OC as 28, and UC as 38. As cancer status was self-reported, it may be subject to recall bias, which should be acknowledged to enhance methodological transparency.
Assessment of Weekend Warrior PA Pattern
PA data were derived from the Global PA Questionnaire (GPAQ), which collects detailed information on participants’ activity intensity and duration. Activity intensity was classified based on MET values: moderate-intensity PA corresponds to 3–5.9 METs (eg, brisk walking, cycling), while vigorous-intensity PA corresponds to ≥6 METs (eg, running, swimming). According to established guidelines, one minute of vigorous-intensity PA is considered equivalent to two minutes of moderate-intensity PA. Therefore, total weekly moderate-to-vigorous PA (MVPA) was calculated using the following formula: MVPA total time (minutes/week) = (Vigorous-intensity activity time × 2) + Moderate-intensity activity time.15 Participants were classified into four PA patterns based on total weekly MVPA and frequency: those engaging in ≥150 minutes/week of MVPA across ≥3 days were considered regularly active; participants accumulating ≥150 minutes/week of MVPA in only 1–2 sessions per week were defined as weekend warriors (WW); those performing 1–149 minutes/week of MVPA were classified as insufficiently active; and individuals with 0 minutes/week of MVPA were considered inactive.
Covariates
Based on prior studies,16 a set of sociodemographic, behavioral, and clinical factors were included as covariates. These included age, race/ethnicity, marital status, education level, poverty-to-income ratio (PIR), smoking status, alcohol consumption, self-reported history of hypertension and diabetes, as well as history of hormone therapy and oral contraceptive use. Age and PIR were modeled as continuous variables, whereas the others were treated as categorical variables. To ensure model stability, multicollinearity was assessed using the variance inflation factor (VIF), with values < 5 indicating no concerning collinearity.
Statistical Analysis
All statistical analyses were conducted using R software (version 4.3.3, R Foundation for Statistical Computing), following the guidelines issued by the Centers for Disease Control and Prevention (CDC), with appropriate sampling weights applied to account for the complex, multistage probability design of NHANES.
The distribution of continuous variables was assessed using the Anderson-Darling test. Non-normally distributed variables were presented as medians with interquartile ranges (IQR) and compared between groups using the Mann–Whitney U-test. Categorical variables were expressed as frequencies and weighted percentages, with between-group differences assessed using the chi-square test.
To investigate the association between different PA patterns and the risk of GC, three weighted logistic regression models were constructed to estimate odds ratios (ORs) and corresponding 95% confidence intervals (CIs). Model 1 was unadjusted. Model 2 was adjusted for demographic variables, including age, race/ethnicity, education level, and marital status. Model 3 was further adjusted for lifestyle and health-related factors, including PIR, smoking status, alcohol consumption, history of hypertension and diabetes, hormone therapy, and oral contraceptive use. For trend tests, PA patterns were treated as an ordinal variable coded as: inactive = 0, insufficiently active = 1, weekend warrior = 2, and regularly active = 3, reflecting increasing levels of activity. This numeric variable was included as a continuous covariate in regression models to test for a linear trend in GC risk. The p-value for trend was derived from the regression coefficient of this ordinal variable.
Subgroup analyses and interaction term tests were conducted to evaluate the potential modifying effects of covariates on the observed associations. To assess potential non-linear relationships, restricted cubic spline (RCS) regression models were applied. A 1:1 Propensity Score Matching (PSM) Sensitivity Analysis was conducted to match participants across PA groups based on key baseline covariates (age, race/ethnicity, education, marital status, PIR, smoking, alcohol, hypertension, diabetes, oral contraceptive use, and hormone therapy). Balance was assessed using standardized differences (p > 0.05). Post-matching, multivariable logistic regression adjusted for the same covariates was used to evaluate associations between PA patterns and GC risk.
All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant.
Results
Characteristics of Study Participants and VIF Analysis
Baseline characteristics of the study participants are presented in Table 1. Among the 13,675 participants, 331 women self-reported a gynecologic cancer diagnosis, including 172 cases of CC, 58 cases of OC, and 101 cases of UC. Statistically significant differences were observed between the two groups in terms of age, race/ethnicity, education level, marital status, PIR, PA pattern, smoking status, history of hypertension, diabetes, and use of exogenous female hormones (all p < 0.05). In contrast, no significant differences were found in alcohol consumption or oral contraceptive use (p > 0.05).
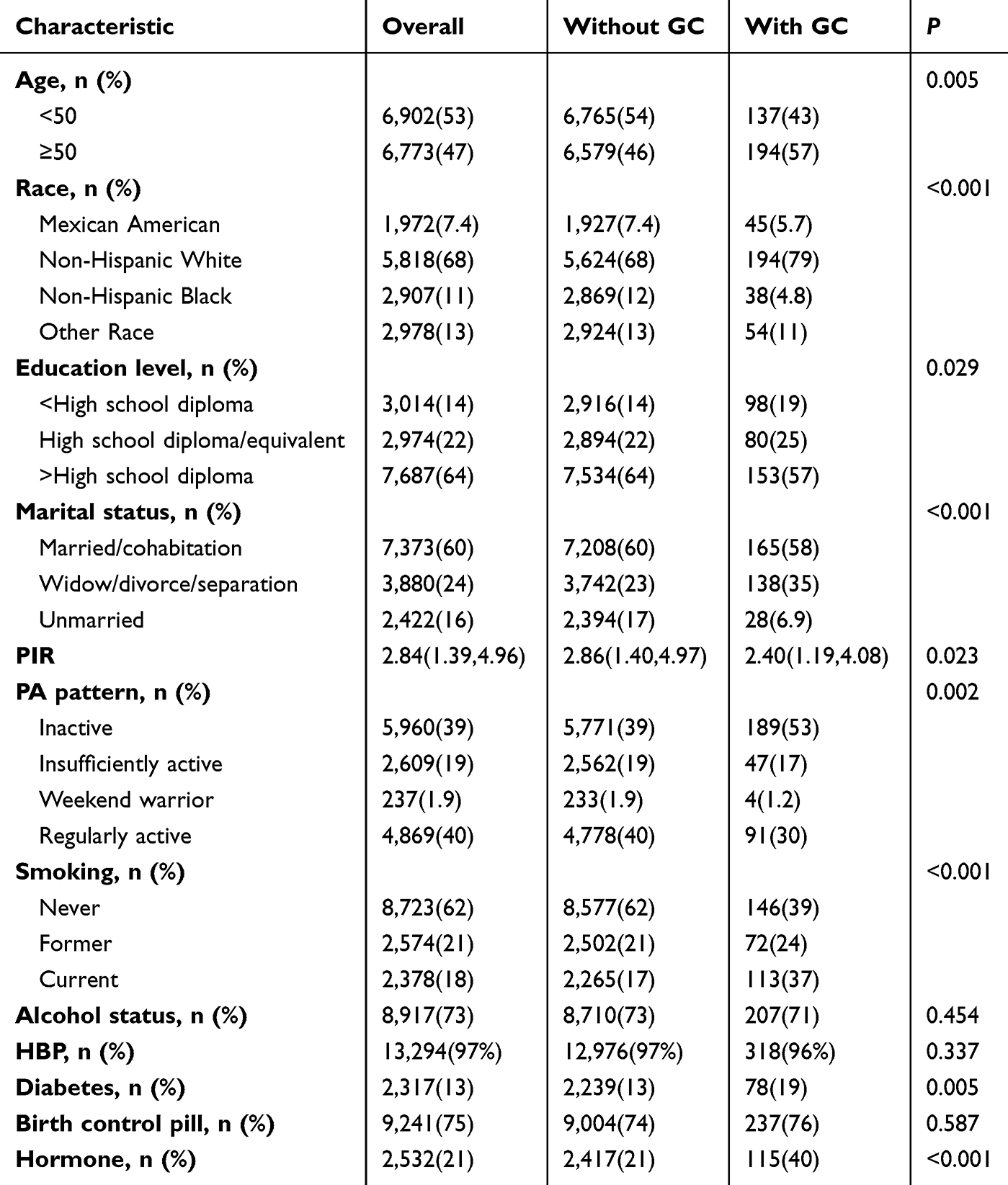 |
Table 1 Baseline Characteristics of the Study Population |
We selected several covariates from Table 1 for variance inflation factor (VIF) analysis to assess potential multicollinearity among the variables. These covariates included age, race, education level, marital status, PIR, smoking status, alcohol consumption, hypertension, diabetes, use of birth control pills, and hormone use. The VIF results (Supplementary Table S1) indicated that all covariates exhibited low VIF values, suggesting that there was no significant multicollinearity among the covariates.
Association Between WW and Other PA Patterns and Gynecological Cancers
Table 2 presents the logistic regression analyses examining the associations between PA patterns and GC risk. In the unadjusted model (Model 1), compared to the inactive group, the regularly active group was significantly inversely associated with GC risk (OR = 0.548, 95% CI: 0.388–0.774, p < 0.001), whereas the WW group showed no significant association with GC risk (OR = 0.484, 95% CI: 0.144–1.628, p = 0.2). Consistent trends were observed in the minimally adjusted model (Model 2) and the fully adjusted model (Model 3). Specifically, regularly active participants exhibited significantly lower GC risk in Model 2 (OR = 0.621, 95% CI: 0.435–0.888, p = 0.01) and Model 3 (OR = 0.635, 95% CI: 0.448–0.901, p = 0.012). Conversely, the WW pattern was not significantly associated with GC risk in Model 2 (OR = 0.550, 95% CI: 0.165–1.834, p = 0.30) or Model 3 (OR = 0.544, 95% CI: 0.162–1.824, p = 0.32). The consistency between univariate and multivariate logistic regression results suggests that a regularly active PA pattern is inversely associated with gynecologic cancer risk, whereas the WW pattern shows no significant relationship, even after adjusting for potential confounders.
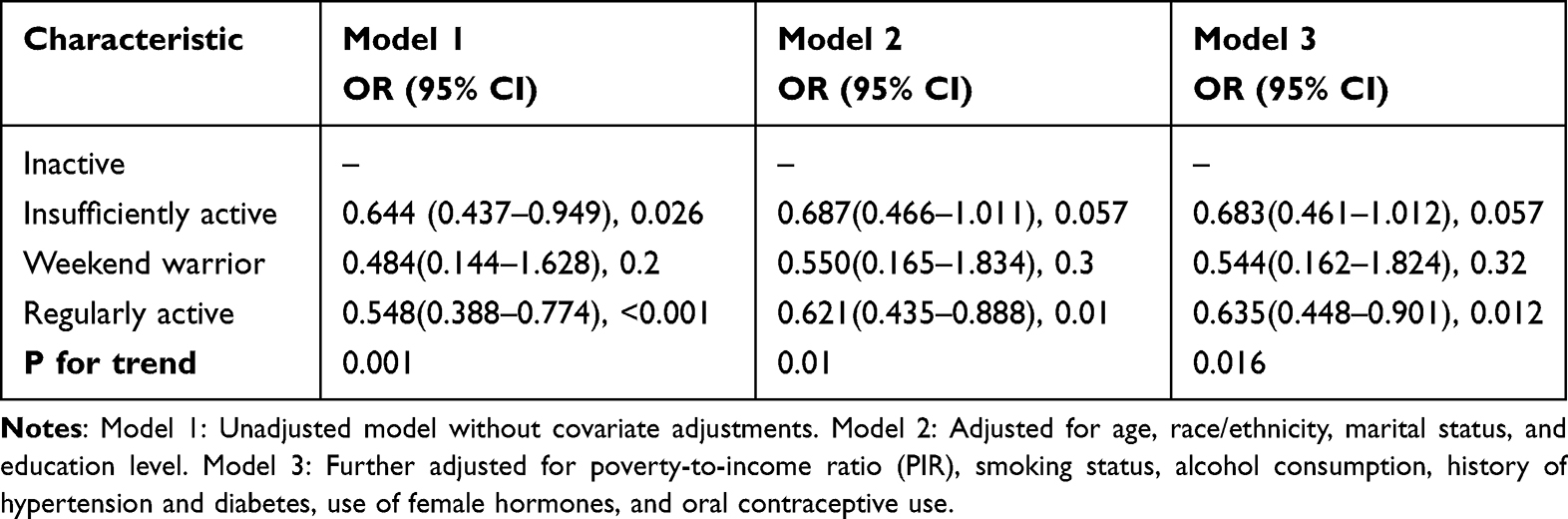 |
Table 2 Association Between WW and Other PA Patterns and Gynecological Cancers |
Nonlinear Association Between PA Patterns and the Risk of Gynecological Cancer
A multivariable-adjusted RCS regression model was employed to investigate the dose-response relationship between PA and GC risk (Figure 2). A significant nonlinear association was observed between PA and GC risk (nonlinearity p < 0.001). Specifically, weekly PA ranging from approximately 51 to 1130 minutes was inversely associated with GC risk.
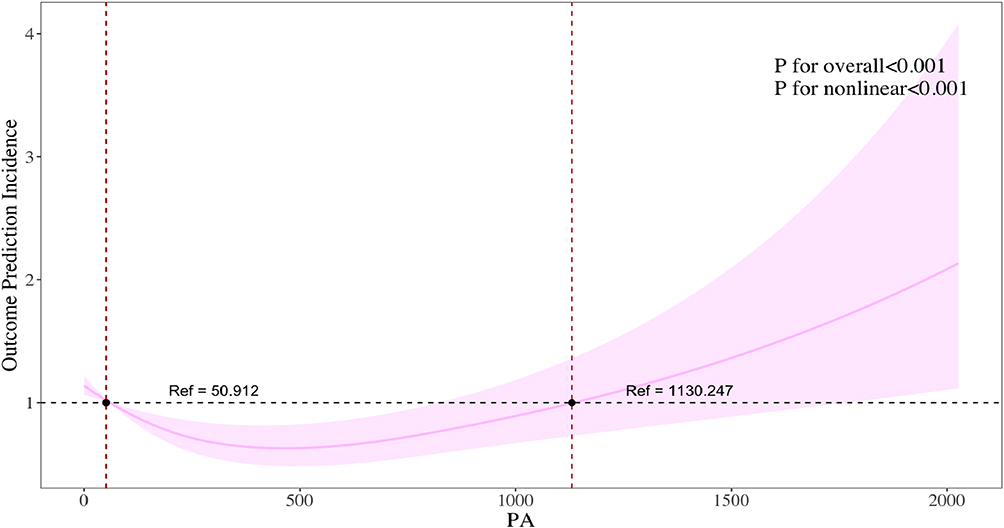 |
Figure 2 Dose-response relationship between PA and GC. |
Stratified Analysis and Sensitivity Analysis
Subgroup analyses revealed a significant interaction effect of race/ethnicity on the association between PA patterns and GC risk (interaction p = 0.038). No significant interactions were observed across other stratified variables (Figure 3). It should be noted that participants classified as WW PA pattern accounted for less than 2% of the cohort, which may limit the ability to detect significant associations and the generalizability of findings for this subgroup.
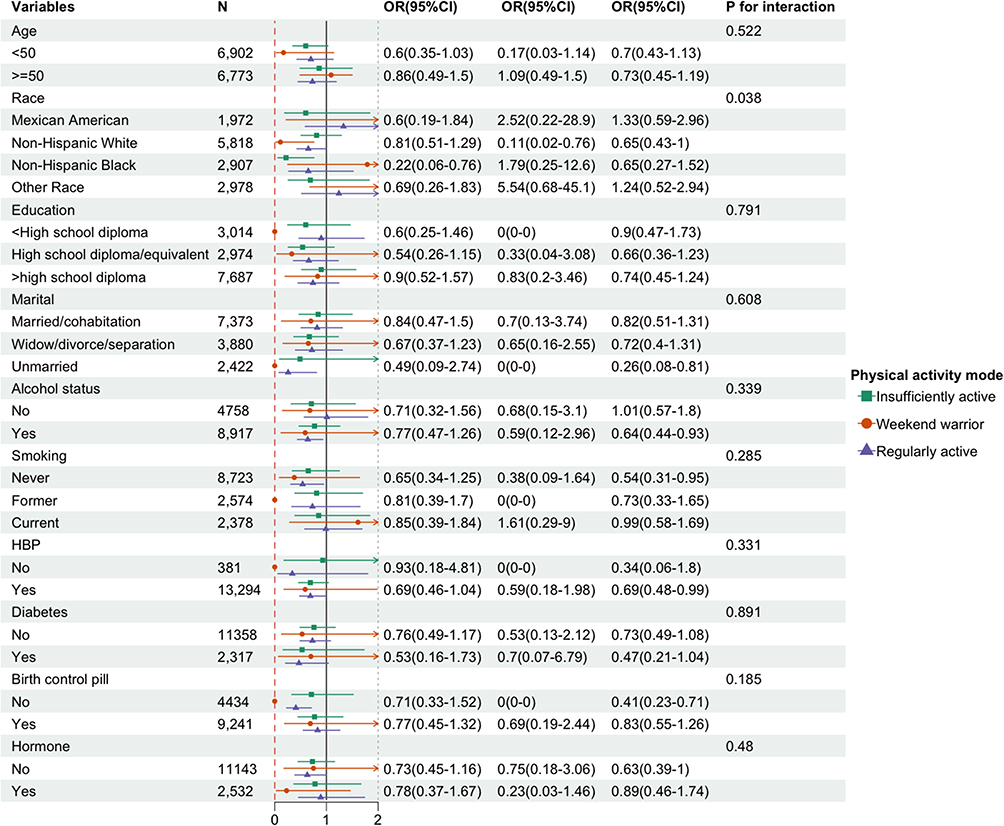 |
Figure 3 Subgroup analyses assessing the associations between PA patterns and GC. |
In the PSM sensitivity analysis of GC participants, baseline characteristics were well balanced between the matched groups, with no significant differences observed for any variable before or after matching (all p > 0.05), indicating that the matching effectively reduced confounding bias (Supplementary Table S2). Post-matching multivariable logistic regression analysis (Supplementary Table S3), adjusted for age, race/ethnicity, education level, marital status, PIR, smoking status, alcohol consumption, hypertension, diabetes, oral contraceptive use, and hormone therapy, showed that, compared with the Inactive PA group, the Insufficiently Active PA group was significantly associated with a lower risk of GC (OR = 0.62, 95% CI: 0.39–0.96, p = 0.034). Associations for the WW PA pattern (OR = 2.01, 95% CI: 0.76–5.93, p = 0.20) and Regularly Active PA groups (OR = 0.69, 95% CI: 0.48–1.01, p = 0.055) with GC risk were not statistically significant. These findings suggest that, after controlling for multiple potential confounders, certain levels of PA may serve as independent protective factors, and this association remained robust in the post-matching sensitivity analysis.
Discussion
In this cross-sectional study using data from NHANES 2007–2018, we investigated the association between different PA patterns and the risk of GC, including CC, UC, and OC. Participants were categorized into regularly active, WW, and inactive groups based on PA frequency and duration. Our findings showed that the regularly active PA pattern was significantly associated with a lower risk of GC, even after adjusting for multiple demographic and lifestyle confounders. In contrast, the WW PA pattern did not demonstrate a statistically significant association with cancer risk, which may be partly attributable to the wide confidence intervals and limited statistical power in this subgroup. In addition, restricted cubic spline analysis revealed a nonlinear inverse relationship between PA duration and GC risk. The protective association was most evident within a PA range of approximately 51 to 1130 minutes per week. This indicates that both insufficient and extremely high levels of activity may have fewer clear benefits. Subgroup analysis further suggested that the association between PA patterns and GC risk may differ by race/ethnicity, emphasizing the need for tailored public health recommendations and interventions that consider population diversity.
Accumulating evidence suggests that approximately 30–50% of cancers can be prevented through healthy lifestyle behaviors, particularly PA and vaccination.17 A U.S.-based study reported that lack of regular recreational PA was associated with a higher incidence of CC.18 Similarly, Jie Xing et al19 found that increasing daily PA duration or distance may help reduce the risk of HPV infection and cervical cancer. In a dose-response analysis, women in the highest PA tertile (≥72 MET-hours/week) had significantly lower odds of CC (OR = 0.61; 95% CI: 0.38–0.98; p-trend = 0.03) compared to those in the lowest tertile (<38.5 MET-hours/week).20 Leisure-time PA (LTPA) has also been associated with a 20% reduction in EC risk.21 Modeling studies in five Nordic countries suggested that adequate PA could potentially prevent up to 11,000 cancer cases, including EC, over a 30-year period.22 However, findings have not been entirely consistent. For instance, a Japanese cohort study reported no significant association between several hours of exercise and EC risk,23 possibly due to limitations in PA assessment tools. Regarding OC, regular vigorous activity during early life has been linked to delayed menarche, earlier menopause, shortened menstrual cycles, and increased anovulation—all of which are considered protective factors.24 A Mendelian randomization study found suggestive evidence that higher levels of overall accelerations in PA were associated with a lower risk of endometrioid OC (OR = 0.18; 95% CI: 0.05–0.64; p = 0.008).25 Moreover, high-intensity PA was linked to a 26% reduction in OC-specific mortality and a 24% reduction in all-cause mortality (HR = 0.74; 95% CI: 0.56–0.98 and HR = 0.76; 95% CI: 0.58–0.98, respectively).26 A recent study in China also demonstrated an inverse association between habitual PA and OC risk, highlighting the importance of promoting LTPA in cancer prevention efforts.27 However, not all studies reached consistent conclusions. For example, Anne Grundy et al28 reported that the association between moderate-to-vigorous PA and OC risk remains inconclusive. These inconsistencies underscore the need for high-quality prospective cohort studies and mechanistic investigations to further elucidate the preventive potential of PA in GC and to guide more targeted public health interventions.
Persistent infection with human papillomavirus (HPV) is recognized as the primary etiological factor for cervical cancer.29 Physical inactivity has been shown to significantly increase the risk of HPV infection, whereas moderate PA may reduce HPV acquisition and persistence.30 Additionally, obesity has been consistently associated with an elevated risk of CC.31,32 Given that PA can reduce adiposity and improve metabolic profiles, it may indirectly lower carcinogenic potential. Exercise interventions have been reported to decrease circulating levels of free estrogens and progestogens,33 thereby suppressing abnormal endometrial proliferation. Furthermore, insulin-like growth factor 1 (IGF-1) plays a critical role in the autocrine and paracrine regulation of ectopic endometrial cell growth and maintenance.34 Overexpression of IGF-1 receptor (IGF1R) and activation of the AKT signaling pathway have been implicated in the early stages of endometrial hyperplasia and the pathogenesis of type I EC.35 Exercise-induced weight loss has been shown to significantly lower circulating insulin and IGF-1 levels, thereby inhibiting cell proliferation signaling pathways such as PI3K/Akt/mTOR.36 Moreover, regular PA helps mitigate chronic low-grade inflammation,37 reducing oxidative stress and mutagenic events that contribute to carcinogenesis. In terms of OC, early-life hormonal fluctuations, particularly in progesterone and androgen levels, are thought to influence disease etiology.38 PA may suppress the hypothalamic–pituitary–ovarian (HPO) axis, leading to decreased ovarian hormone production.39 These mechanisms help contextualize our findings: the protective effects of regularly active PA on gynecologic cancer are supported by well-established metabolic, hormonal, and inflammatory pathways. In contrast, evidence on the biological mechanisms underlying the WW pattern is currently limited, and our study did not observe a significant association, highlighting the need for further research on how infrequent, concentrated exercise might influence gynecologic cancer risk.
This study has several notable strengths. First, it is based on a nationally representative sample from the NHANES, enhancing the external validity and generalizability of the findings. Second, multivariable-adjusted analyses consistently revealed a significant inverse association between regular PA patterns and the risk of GC, with evidence supporting a dose–response relationship. However, several limitations should be acknowledged. Due to the cross-sectional nature of the study, causal inferences cannot be established. The analysis was limited to the three most common gynecologic cancers (cervical, uterine, and ovarian cancers), as NHANES does not provide data on less prevalent cancers such as vulvar or vaginal cancer. Both PA and cancer diagnosis were self-reported, which may introduce recall bias and misclassification. Additionally, other lifestyle factors such as diet and sleep patterns were not included in the analysis, potentially resulting in residual confounding. The small number of WW pattern participants and the low incidence of gynecologic cancer in this group limit the precision of estimates and the strength of conclusions for this subgroup. Observed associations should be interpreted cautiously, and further studies with larger sample sizes are needed to confirm these findings. Moreover, future research should adopt objective measures of PA to reduce bias, and investigation into specific barriers to sustaining regular PA may provide valuable insights for developing targeted prevention strategies.
Conclusion
This study, based on nationally representative NHANES data, evaluated the associations between PA patterns—including the WW pattern—and the risk of three major GC. Regular PA may be associated with a reduced risk of GC in a dose–response manner, whereas current evidence remains insufficient to establish a clear association for the WW pattern. These findings underscore the importance of sustained PA for primary GC prevention. Given the small number of WW participants, further longitudinal and mechanistic studies are needed to confirm these results and inform targeted PA recommendations, particularly for individuals with limited time for regular exercise. From a public health perspective, promoting consistent PA remains a key strategy for cancer prevention, with tailored interventions necessary for those unable to maintain regular activity.
Data Sharing Statement
The datasets generated during and analyzed during the current study are available in the NHANES repository (https://www.cdc.gov/nchs/nhanes/index.htm).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank all contributors to the National Health and Nutritional Examination Survey (NHANES) data that were used in this analysis.
Funding
The research of our article was funded by the Chinese Medicine Research Program of Guangxi Province (2022JJA140848); The National Natural Science Foundation of China (82160919); The National Natural Science Foundation of China (82360950).
Disclosure
The authors declare no competing interests in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Piechocki M, Koziołek W, Sroka D, et al. Trends in incidence and mortality of gynecological and breast cancers in Poland (1980-2018). Clin Epidemiol. 2022;14:95–114. doi:10.2147/CLEP.S330081
3. Zhu X, Xuan F, Yu S, Qiu Z, Lou Y, Qiu Z. Quantitative analysis of trends and inequalities in disease burden and care quality of gynecological cancers, 1990-2021. Eur J Cancer Prev. 2025. doi:10.1097/CEJ.0000000000000978
4. Yang C, Zou J, Luo X, et al. Health inequality and improvement gap in the prevalence of gynecological cancers among perimenopausal women globally, 1990-2019. BMC Public Health. 2025;25(1):590. doi:10.1186/s12889-025-21807-3
5. Tan N, Wu Y, Li B, Chen W. Burden of female breast and five gynecological cancers in China and worldwide. Chin Med J. 2024;137(18):2190–2201. doi:10.1097/CM9.0000000000003293
6. Kushi LH, Doyle C, McCullough M, et al. American cancer society guidelines on nutrition and physical activity for cancer prevention: reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin. 2012;62(1):30–67. doi:10.3322/caac.20140
7. Liu F, Han X, Cheng Y, et al. Association of physical activity level and all-cause mortality among stroke survivors: evidence from NHANES 2007-2018. Environ Health Prev Med. 2025;30:27. doi:10.1265/ehpm.24-00322
8. Chen P, Zhu L, Mou Y, Zhao S, Huang G. The association between glycated hemoglobin, physical activity and infertility: a multiple logistic regression and mediation analysis based on the NHANES database. Front Endocrinol. 2025;16:1495470. doi:10.3389/fendo.2025.1495470
9. Liu W, An J, Jiao C, Zhi L, Guo J, Sun L. The association between physical activity and risk for breast cancer in US female adults: a cross-sectional study based on NHANES 2011-2020. Eur J Surg Oncol. 2024;50(12):108647. doi:10.1016/j.ejso.2024.108647
10. O’Donovan G, Sarmiento OL, Hamer M. The rise of the “Weekend warrior”. J Orthop Sports Phys Ther. 2018;48(8):604–606. doi:10.2519/jospt.2018.0611
11. Wang K, Xia F, Li Q, Luo X, Wu J. The associations of weekend warrior activity patterns with the visceral adiposity index in US adults: repeated cross-sectional study. JMIR Public Health Surveill. 2023;
12. Xu S, Zhao C, Hu L. Association of accelerometer-derived physical activity pattern with depression: weekend warrior or regular activity? J Affect Disord. 2025;381:92–99. doi:10.1016/j.jad.2025.04.016
13. Fu K, Wang J, Pan H, Huang L, Li X. Weekend warrior and the risk of specific disease: a meta-epidemiology study. BMC Public Health. 2025;25(1):1414. doi:10.1186/s12889-025-22667-7
14. National Health Commission PRC. Ministry of Education, Ministry of Science and Technology, National Administration of Traditional Chinese Medicine. Easures for the Ethical Review of Life Science and Medical Research Involving Humans: GUO WEI KE JIAO FA. Beijing: National Health Commission. 2023.
15. Chen Z, Xin J, Jia J, Tu J, Li X. The association between weekend warrior physical activity pattern and anxiety: evidence from a U.S. population-based study. BMC Psychiatry. 2025;25(1):168. doi:10.1186/s12888-025-06612-x
16. Chen C, Zheng M, Dong X, et al. Association of dietary inflammatory index with gynecological cancers in NHANES 2011-2018. Front Nutr. 2025;12:1560987. doi:10.3389/fnut.2025.1560987
17. Kruk J, Aboul-Enein BH, Gołębiewska ME, Duchnik E, Czerniak U, Marchlewicz M. Physical activity and cancer incidence and mortality: current evidence and biological mechanisms. Cancers. 2025;17(9):1410. doi:10.3390/cancers17091410
18. Szender J, Cannioto R, Gulati N, et al. Impact of physical inactivity on risk of developing cancer of the uterine cervix: a case-control study. J Lower Genital Tract Disease. 2016;20(3):230–233. doi:10.1097/lgt.0000000000000210
19. Xing J, Zhu T, Zhang J, Yang W, Yu A-J. Association between prestored smartphone monitored physical activity and the risk of HPV infection and cervical cancer. Asian Pac J Cancer Prev. 2022;23(10):3393–3404. doi:10.31557/APJCP.2022.23.10.3393
20. Lee JK, So KA, Piyathilake CJ, Kim MK. Mild obesity, physical activity, calorie intake, and the risks of cervical intraepithelial neoplasia and cervical cancer. PLoS One. 2013;8(6):e66555. doi:10.1371/journal.pone.0066555
21. Saint-Maurice PF, Sampson JN, Michels KA, et al. Physical activity from adolescence through midlife and associations with body mass index and endometrial cancer risk. JNCI Cancer Spectr. 2021;5(4):pkab065. doi:10.1093/jncics/pkab065
22. Andersson TML, Engholm G, Lund A-SQ, et al. Avoidable cancers in the Nordic countries-the potential impact of increased physical activity on postmenopausal breast, colon and endometrial cancer. Eur J Cancer. 2019;110:42–48. doi:10.1016/j.ejca.2019.01.008
23. Miyata H, Shirai K, Muraki I, Iso H, Tamakoshi A. Associations of body mass index, weight change, physical activity, and sedentary behavior with endometrial cancer risk among Japanese women: the japan collaborative cohort study. J Epidemiol. 2021;31(12):621–627. doi:10.2188/jea.JE20200145
24. Wang T, Jake-Schoffman DE, Townsend MK, Vinci C, Willett WC, Tworoger SS. Early life physical activity and risk of ovarian cancer in adulthood. Int J Cancer. 2021;149(12):2045–2051. doi:10.1002/ijc.33760
25. Wang J, Zhao H, Zhu J, Jiang M. Causal effects of physical activity on the risk of overall ovarian cancer: a Mendelian randomization study. Digit Health. 2023;9:20552076231162988. doi:10.1177/20552076231162988
26. Zhou Y, Chlebowski R, LaMonte MJ, et al. Body mass index, physical activity, and mortality in women diagnosed with ovarian cancer: results from the Women’s Health Initiative. Gynecol Oncol. 2014;133(1):4–10. doi:10.1016/j.ygyno.2014.01.033
27. Lee AH, Su D, Pasalich M, Wong YL, Binns CW. Habitual physical activity reduces risk of ovarian cancer: a case-control study in southern China. Prev Med. 2013;57:Suppl:S31–S33. doi:10.1016/j.ypmed.2012.11.009
28. Grundy A, Ho V, Abrahamowicz M, et al. Lifetime recreational moderate-to-vigorous physical activity and ovarian cancer risk: a case-control study. Int J Cancer. 2020;146(7):1800–1809. doi:10.1002/ijc.32513
29. Cohen PA, Jhingran A, Oaknin A, Denny L.Cervical cancer. Lancet. 2019;393(10167):169–182. doi:10.1016/S0140-6736(18)32470-X
30. Li Y, Liu M, Huang P, et al. The lifestyle factors of physical activity and diet balance associated with HPV infection in China: the cross-sectional study. Front Oncol. 2022;12:1043937. doi:10.3389/fonc.2022.1043937
31. Urbute A, Frederiksen K, Thomsen LT, Kesmodel US, Kjaer SK. Overweight and obesity as risk factors for cervical cancer and detection of precancers among screened women: a nationwide, population-based cohort study. Gynecol Oncol. 2024;181:20–27. doi:10.1016/j.ygyno.2023.12.002
32. Maruthur NM, Bolen SD, Brancati FL, Clark JM. The association of obesity and cervical cancer screening: a systematic review and meta-analysis. Obesity. 2009;17(2):375–381. doi:10.1038/oby.2008.480
33. Kossman DA, Williams NI, Domchek SM, Kurzer MS, Stopfer JE, Schmitz KH. Exercise lowers estrogen and progesterone levels in premenopausal women at high risk of breast cancer. J Appl Physiol. 2011;111(6):1687–1693. doi:10.1152/japplphysiol.00319.2011
34. Blontzos N, Mavrogianni D, Ntzeros K, et al. Differential expression of insulin growth factor 1 (IGF-1) isoforms in different types of endometriosis: preliminary results of a single-center study. Biomolecules. 2023;14(1):7. doi:10.3390/biom14010007
35. McCampbell AS, Broaddus RR, Loose DS, Davies PJA. Overexpression of the insulin-like growth factor I receptor and activation of the AKT pathway in hyperplastic endometrium. Clin Cancer Res. 2006;12(21):6373–6378.
36. Xie L, Wang W. Weight control and cancer preventive mechanisms: role of insulin growth factor-1-mediated signaling pathways. Exp Biol Med. 2013;238(2):127–132. doi:10.1177/1535370213477602
37. Gleeson M. Immune function in sport and exercise. J Appl Physiol. 2007;103(2):693–699.
38. Gong -T-T, Wu Q-J, Vogtmann E, Lin B, Wang Y-L. Age at menarche and risk of ovarian cancer: a meta-analysis of epidemiological studies. Int J Cancer. 2013;132(12):2894–2900. doi:10.1002/ijc.27952
39. Cano Sokoloff N, Misra M, Ackerman KE. Exercise, training, and the hypothalamic-pituitary-gonadal axis in men and women. Front Horm Res. 2016;47:27–43. doi:10.1159/000445154
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Port Site Metastasis After Minimally Invasive Surgery in Gynecologic Malignancies: Two Case Reports and a Review of the Literature
Yu N, Zhou T, Sun H, Fu P, Liu R
International Journal of Women's Health 2023, 15:579-588
Published Date: 12 April 2023
Value of Antibody Drug Conjugates for Gynecological Cancers: A Modern Appraisal Following Recent FDA Approvals
McNamara B, Chang Y, Goreshnik A, Santin AD
International Journal of Women's Health 2023, 15:1353-1365
Published Date: 28 August 2023
BRCA2, PALB2, RECQL4 Germline Pathogenic Variants, and Somatic TP53 Mutation in Triple Metachronous Malignancies: A Case Report and Literature Review
Liu Y, Yang H, Fu X, Zhong L, Xu P, Fang F, Liu Y, Li Q, Yan Y, Wei S, Wang J, Zhang C
International Medical Case Reports Journal 2024, 17:23-29
Published Date: 10 January 2024