")
Back to Journals » International Journal of Women's Health » Volume 15
Value of Antibody Drug Conjugates for Gynecological Cancers: A Modern Appraisal Following Recent FDA Approvals
Authors McNamara B , Chang Y, Goreshnik A , Santin AD
Received 1 April 2023
Accepted for publication 9 August 2023
Published 28 August 2023 Volume 2023:15 Pages 1353—1365
DOI https://doi.org/10.2147/IJWH.S400537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Blair McNamara, Yifan Chang, Ashley Goreshnik, Alessandro D Santin
Department of Obstetrics, Gynecology, and Reproductive Sciences Yale University School of Medicine, New Haven, CT, 06520, USA
Correspondence: Alessandro D Santin, Obstetrics and Gynecology, Yale University School of Medicine, 333 Cedar Street, PO Box 208063, New Haven, CT, 06520, USA, Tel +1 203-737-4450, Fax +1 203-737-4339, Email [email protected]
Abstract: Antibody drug conjugates (ADCs) are a new class of targeted anti-cancer therapies that combine a monoclonal tumor surface receptor-targeting antibody with a highly cytotoxic molecule payload. They enable delivery of cytotoxic therapy more directly to tumor cells and minimize delivery to healthy tissues. This review summarizes the existing literature about ADC therapies approved for use in gynecologic malignancies, relevant preclinical studies, as well as ongoing clinical trials.
Keywords: antibody-drug conjugate, gynecologic malignancy, chemotherapy, cervical cancer, ovarian cancer, endometrial cancer
Introduction
Gynecologic malignancies are a significant cause of global morbidity and mortality. In the United States (US) alone, it is estimated that there will be 114,810 new cases of uterine, cervix, ovary, vulva, and vaginal cancer in 2023, and 34,020 deaths.1 The mainstays of initial treatment for advanced, recurrent, or metastatic gynecologic malignancy are platinum doublet chemotherapy and cytoreductive surgery. Chemotherapy is given in the neoadjuvant setting prior to surgery, in the adjuvant setting after surgery, concomitant with radiation therapy for sensitization, and in the recurrent setting. It is common for patients with a recurrent gynecologic malignancy to undergo several lines of chemotherapy, moving on to different combinations of cytotoxic therapy, immunotherapy, or targeted drug with each disease progression or relapse.2–5 There remains a significant need for development of novel, effective, targeted therapies for these malignancies.
In recent years, there has been a surge of novel targeted therapies for gynecologic malignancies in preclinical and clinical trials. One such class of targeted therapies with impressive potential is antibody drug conjugates (ADCs). ADCs are composed of a humanized monoclonal antibody specific for a tumor surface antigen, a cleavable or uncleavable linker and a cytotoxic payload; they thus enable a more targeted delivery of tumor-directed therapy, while minimizing off-target toxicity to normal tissues and thus fewer adverse effects than traditional chemotherapy.6
There are now two Food & Drug Administration (FDA)-approved ADCs for treatment of gynecologic malignancies: mirvetuximab soravtansine for folate receptor alpha (FRα) positive, platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer with 1–3 prior systemic regimens, and tisotumab vedotin in previously treated recurrent or metastatic cervical cancer.7,8 There are many ongoing trials of ADCs alone and in combination with established therapies for gynecologic malignancies (Table 1). This review aims to provide a comprehensive overview of the encouraging preclinical and clinical activity of ADCs in gynecologic malignancies.
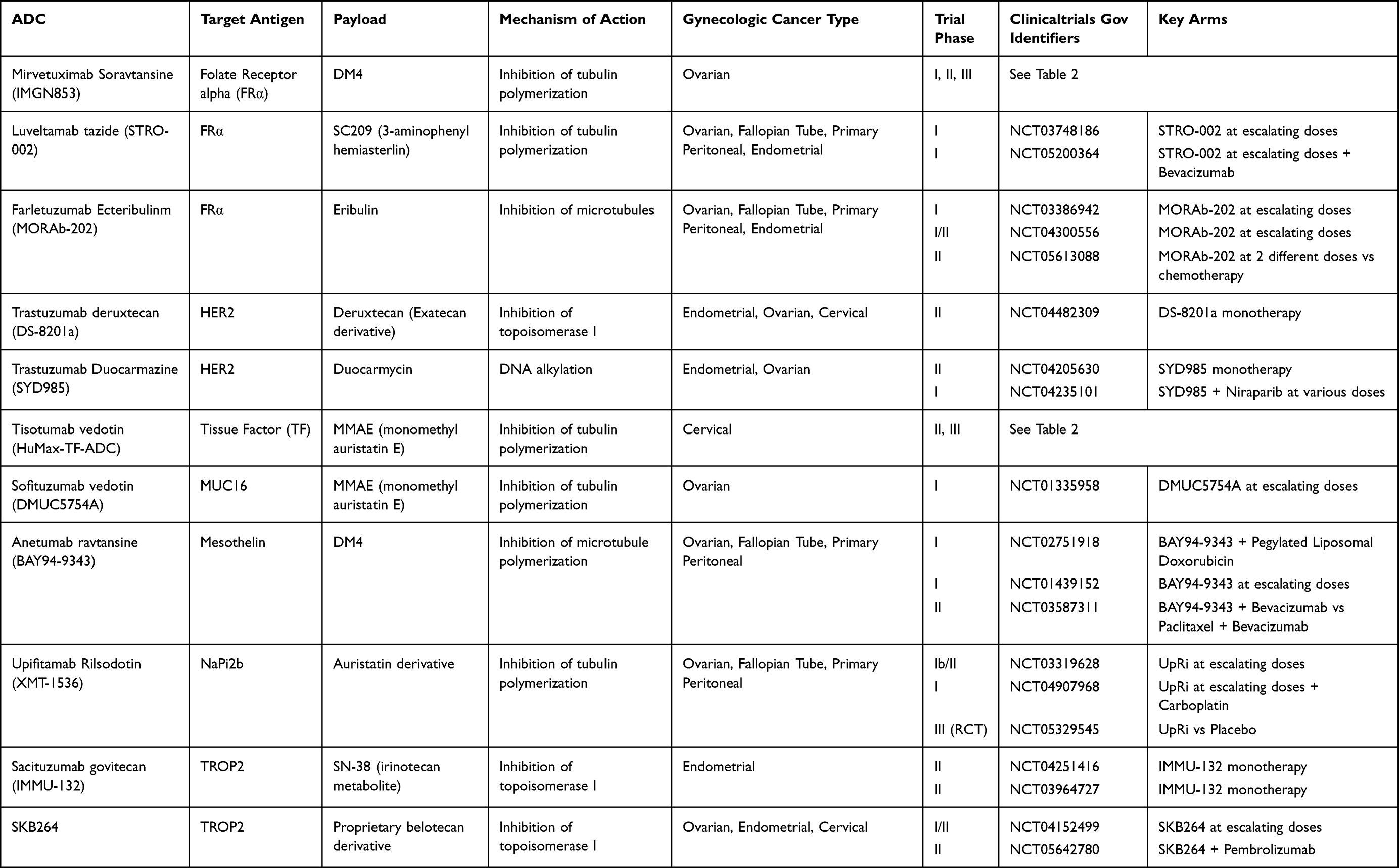 |
Table 1 Summary Table of ADCs in Development for Gynecologic Malignancies |
FDA-Approved ADCs
Tisotumab Vedotin
The first ADC to be FDA approved for gynecologic malignancies was Tisotumab vedotin-tftv, an antibody–drug conjugate comprising tissue factor targeting antibody, a cleavable linker, and a payload of monomethyl auristatin E (MMAE) as a microtubule-disrupting agent. Tisotumab vedotin received accelerated FDA approval in September 2021 for patients with recurrent or metastatic cervical cancer with disease progression after chemotherapy. This decision was supported by findings from the Phase II INNOVA TV 204 trial.7 The trial enrolled 101 patients with recurrent or metastatic cervical cancer who had progression of disease on or after doublet chemotherapy plus bevacizumab before receiving 2 mg/kg every 21 days (maximum 200 mg) of tisotumab vedotin IV until disease progression or unacceptable toxicity. The primary endpoint was ORR, which was 24% (95% CI, 16 to 33) with 7% of patients who had a complete response and 17% with partial responses. The median time to response was 1.4 months (95% CI, 1.1 to 5.1), while the duration of response was 8.3 months (95% CI, 4.2 to not reached). Furthermore, the study noted that target lesions were reduced in 77 (79%) of 97 treated patients with at least one post-baseline scan. With regard to adverse events, 92% of patients experienced TRAEs with 28% of patients experiencing Grade 3 or worse TRAE. Common toxicities included alopecia, conjunctivitis, diarrhea, nausea/vomiting, peripheral neuropathy, and hemorrhagic events. Ocular TRAEs were observed in 53% of patients, with conjunctivitis being the most common. No serous ocular TRAEs occurred, and 86% resolved within 30 days of the last dose. Hemorrhagic adverse events occurred in 39% of patients, however, only 2% were grade 3 events. Overall, 24% of patients had a TRAE leading to dose interruption, and 12% of patients discontinued treatment after a TRAE.7
Advances in metastatic or recurrent cervical cancer were made when pembrolizumab was approved as a first-line treatment for patients with PD-L1 expressing tumors. However, for patients whose tumors do not express PD-L1, there are limited second-line treatment options after disease progression occurs on chemotherapy and bevacizumab. Tisotumab vedotin represents a new option for these patients, and confirmatory randomized control trial comparing tisotumab vedotin vs chemotherapy in recurrent or metastatic cervical cancer is ongoing (INNOVA TV 301 [NCT04697628]) (Table 1 and 2).
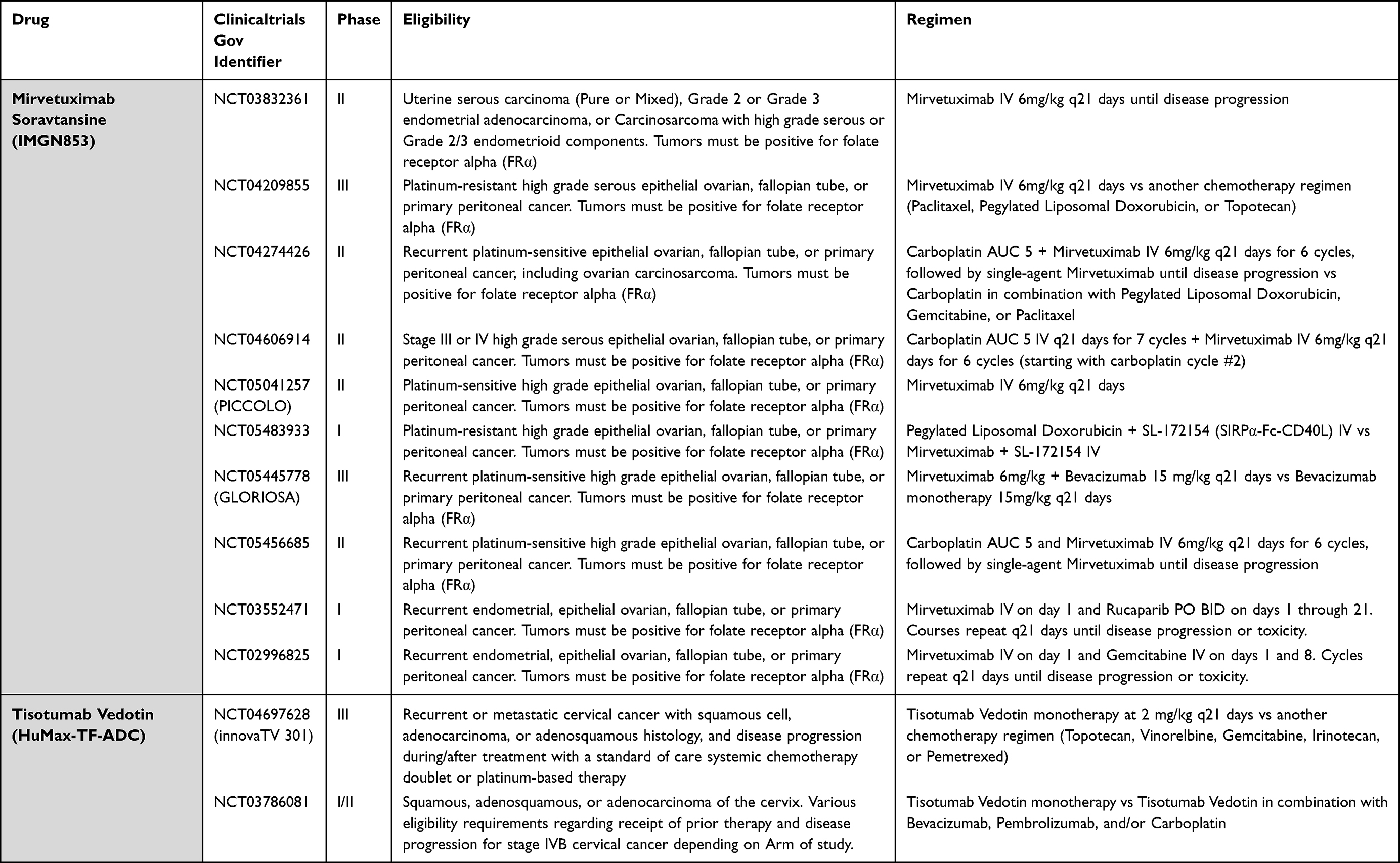 |
Table 2 Ongoing Trials of FDA-Approved ADCs in Gynecologic Malignancies |
Mirvetuximab Soravtansine
The first ADC to be approved for ovarian cancer, Mirvetuximab soravtansine-gynx is an antibody–drug conjugate composed of a folate receptor alpha targeting antibody, a cleavable linker, and a payload of microtubulin destabilizer of maytansinoid DM4. It was granted accelerated FDA approval in November 2022 for patients with folate receptor alpha (FRα) positive, platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer.8 The FDA labeling requires patients to have received up to 3 prior lines of systemic therapy, including bevacizumab.
The FDA approval was supported by findings from the SORAYA trial (NCT04296890).9 This international, single-arm trial enrolled patients with high FRα expression platinum-resistant epithelial ovarian cancer who had received 1–3 prior lines of therapy including bevacizumab. Forty-eight percent of patients were also previously treated with a Poly-ADP Ribose Polymerase inhibitor (PARPi). Confirmed objective response rate (ORR) by investigator was the primary end point, while duration of response was the secondary end point. Patients received single agent mirvetuximab soravtansine at 6 mg/kg every 21 days. Among the 105 patients who were included for efficacy evaluation, ORR was 32.4% (95% CI, 23.6–42.2); there were 5 patients with complete response and 29 with partial response. The medial duration of response was 6.9 months (95% CI, 5.6 to 9.7). Notably, the subgroup analysis demonstrates that mirvetuximab soravtansine was effective regardless of prior PARPi exposure of prior number of lines of therapy. In terms of safety, 86% of patients who received at least one dose of mirvetuximab soravtansine experienced TRAEs, with 28% of patients experiencing at least 1 grade 3 TRAE and 1% experiencing at least 1 grade 4 TRAE. Ocular adverse events were the most common, with 52% of patients experiencing any-grade blurred vision or keratopathy. A 11% of patients had an ocular TRAE that resulted in dose reduction, and 1 required treatment discontinuation. Most of the ocular TRAE were reversible, with 96% of grade 2 or greater ocular events resolved to grade 1 or 0.
Given that a significant percentage of patients with platinum-resistant ovarian cancer were found to have high FRα expression (36% of patients screened for SORAYA trial), the approval of Mirvetuximab soravtansine could fill an unmet need for patients with platinum-resistant ovarian cancer.9
Further study to confirm the efficacy of mirvetuximab soravtansine as a single-agent therapy in platinum-resistant ovarian cancer is underway with the MIRASOL trial (NCT04209855): a randomized, open-label, Phase 3 study comparing mirvetuximab soravtansine with investigator’s choice of standard-of-care chemotherapy in advanced high-grade epithelial ovarian, primary peritoneal or fallopian tube cancers with high FRα expression (Table 2).10
Two additional clinical trials (GLORIOSA [NCT05445778], FORWARD [NCT02606305]) are investigating combination treatment with mirvetuximab soravtansine and bevacizumab in patients with high FRα-expressing platinum-resistant ovarian cancer. In the FORWARD cohort of 94 patients evaluable for efficacy analysis, confirmed ORR in the ITT population was 44% (85% CI, 33 to 54), including 5 patients with complete response and 36 with partial response. The medial duration of response was 9.7 months (95% CI, 6.9 to 14.1), and the median progression-free survival was 8.2 months (95% CI, 6.8 to 10.0).11 The many other Phase 1–3 trials of mirvetuximab soravtansine are summarized in Table 2.
HER2 Targeted Therapies
Human epidermal growth factor receptor-2 (HER2) is encoded by the ERBB2 gene, which when amplified, causes HER2 to be overexpressed in many different solid malignancies. HER2 is a member of the human epidermal growth factor receptor (HER) family of tyrosine kinase receptors. When activated, it dimerizes with other tyrosine kinase receptors in the HER family (HER1/EGFR, HER3, and HER4) and induces signal transduction through the mitogen-activated protein kinase and PI3K signaling cascade.12 This tyrosine kinase activity leads to induction of genes that further promote malignant cellular potential. In gynecologic malignancies, HER2 is most often overexpressed in endometrial cancer (17–30%) and ovarian cancer (5–60%).13–15 Like in many cancers, HER2 has been demonstrated to be a poor prognostic marker in uterine and ovarian cancer.14,16
HER2 has already proven to be a targetable biomarker in gynecologic malignancies—trastuzumab, a monoclonal antibody specific for HER2, is now listed in the National Comprehensive Cancer Network (NCCN) guidelines as the preferred treatment regimen when used in combination with carboplatin-paclitaxel for patients with stage III/IV or recurrent uterine serous carcinoma (USC) with HER2 overexpression.17 At present, there are no FDA approved or standard of care ADCs that utilize trastuzumab as their monoclonal antibody. However, there are several compounds in preclinical development as well as in Phase I/II clinical trials (Table 1).
Trastuzumab Deruxtecan
Trastuzumab deruxtecan (T-DXd or DS-8201a) is one such ADC and is composed of a humanized monoclonal antibody specific for HER2, a cleavable tetrapeptide linker, and a topoisomerase I inhibitor payload. After T-DXd is internalized into tumor cells, the toxic payload, DXd, is released and can permeate through the cell membrane to neighboring tumor cells, regardless of their HER2 status; this feature has resulted in T-DXd demonstrating clinical efficacy in heterogenous HER2 tumors.18
T-DXd’s clinical utility in gynecologic malignancies is being evaluated in a number of ongoing clinical trials (Table 1 and 2). The STATICE trial is a Phase II, multicenter, single-arm study evaluating T-DXd in patients with advanced or recurrent HER2-expressing (ie, 1+, 2+, or 3+) uterine carcinosarcomas (UCS) previously treated with chemotherapy.19 They administered 6.4 or 5.4 mg/kg T-DXd intravenously every 3 weeks until disease progression, unacceptable toxicity, or withdrawal of consent. Trial investigators randomized 32 patients—22 with HER2-high USC, and 10 with HER2-low. The authors report an overall response rate (ORR) of 54.5% (95% CI, 32.2 to 75.6) in the HER2-high cohort, and 70% (95% CI 45.1 to 86.1) in the HER2-low group. Median duration of response (DoR) was 6.9 months in HER2-high group and 8.1 months in HER2-low group. Both groups demonstrated a 100% disease control rate. The study took place across several centers in Japan.
In the US, a Phase I trial (NCT02564900) evaluating T-DXd among HER2-positive solid tumors included 59 patients, 2 patients with endometrial cancer, and one patient with cervical cancer. Patients did very well and had durable disease response rates. Median DoR was reported to be 11.5 (95% CI 7.0 to not met) months, and median PFS was 7.2 months (95% CI 4.8 to 11.1). Patients with HER2-expressing tumors had the most pronounced tumor shrinkage.20
The subsequent Phase II, multicenter, open-label trial (DESTINY-PanTumor02, NCT04482309), has completed enrollment of 268 participants with bladder, biliary tract, cervical, endometrial, ovarian, and pancreatic cancer that express HER2. Primary outcome measures will be ORR, and secondary outcome measures will be DoR, PFS, OS, and safety data. Data collection will be completed June 16, 2023.
T-DXd has shown encouraging preclinical activity in other gynecologic malignancies, such as ovarian carcinosarcoma.21 T-DXd has received FDA approval for use in HER2-positive or HER2-low metastatic breast cancer, HER2 positive gastric cancer, and HER2 mutated non-small cell lung cancer.22–24
Trastuzumab Duocarmazine
Trastuzumab duocarmazine (SYD985) is composed of HER2-directed monoclonal antibody trastuzumab covalently bound to a duocarmycin derivative. This payload is attached via cleavable linker and contains the prodrug seco-duocarmycin-hydroxybenzamide-azaindole (seco-DUBA). DUBA alkylates DNA, resulting in DNA damage and cell death.
In a Phase I dose-expansion clinical trial of trastuzumab duocarmazine in patients with HER2-expressing breast, gastric, urothelial, or endometrial cancer, 146 patients were enrolled, 14 of them with endometrial cancer. Patients were given 1.2 mg/kg of trastuzumab duocarmazine every 3 weeks. Of the 14 patients with endometrial cancer, five (39%, 95% CI 13.9 to 68.4) patients had partial disease responses.25
A Phase II open-label, single-arm study in patients with HER2-expressing recurrent, advanced or metastatic endometrial carcinoma is underway (NCT04205630). Investigators plan to enroll 60 participants with disease progression on or after first-line platinum-based chemotherapy. Patients with 2 or more prior lines of chemotherapy for advanced/metastatic disease are not eligible. Primary outcomes include ORR, PFS, OS, and treatment-emergent adverse events (AEs). HER2 immunohistochemistry (IHC) scores of 1+, 2+, and 3+ are allowed. The primary completion of the study is expected in April 2023 (Table 1).
Trastuzumab duocarmazine has shown preclinical antitumor activity in HER2-expressing epithelial ovarian carcinoma, uterine serous carcinoma, and uterine and ovarian carcinosarcomas.26–28
Folate Receptor Alpha Targeted Therapies
Folate receptor alpha (FRα) is a cell surface glycoprotein that binds and transports folate, a basic component of DNA synthesis and repair, into cells. Given that malignant cells require increased folate to support their rapid division, antifolate therapy has long been a mainstay of cancer-directed therapy.29 Notably, normal tissues have minimal expression of FRα, and it is limited to the apical surfaces of specific cells in the kidney, lung, thyroid, and breast tissues.30 There is an increased cell surface expression of FRα in epithelial malignancies, specifically ovarian and endometrial cancers.31–33 FRα expression is estimated to be 60–100% in non-mucinous ovarian cancers, and 40–90% in endometrial cancers.32,34 Given FRα’s unmatched prevalence and specificity for tumoral cells, it is an attractive biomarker and natural focus of novel and developing ADCs.
Mirvetuximab soravtansine is the most developed and studied FRα-targeting ADC, and received FDA approval for FRα-positive, platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer in November 2022. It is discussed in the above section. The safety and effectivity of several other FRα-targeting ADCs is now being evaluated in patients with gynecologic malignancies in various clinical trials.
Luveltamab Tazide (STRO-002)
Luveltamab tazide (STRO-002) is composed of a high affinity anti-FRα antibody conjugated to a cleavable 3-aminophenyl hemiasterlin linker payload (SC239), which functions as a microtubule stabilizer, preventing microtubule polymerization and thus further cell division. STRO-002 demonstrated promising preclinical effectivity against several ovarian and endometrial cancer cell lines, and early studies suggest potential synergism with other standard therapies such as carboplatin and bevacizumab.35
Luveltamab tazide is currently being evaluated in Phase I clinical trials that include patients with ovarian and endometrial cancer (NCT03748186 and NCT05200364, Table 1). NCT03748186 is a Phase 1 open-label, multicenter, dose-escalation/expansion trial to study its safety, pharmacokinetics, and preliminary efficacy in patients with advanced endometrial or epithelial ovarian, fallopian, or primary peritoneal cancers with progressive or recurrent disease after standard therapy. Ideal drug dosage is being determined, and it is given intravenously every three weeks (dosage range 4.3–5.2mg/kg). As of April 2023, the study is still accruing participants for its dose-expansion arm, with a goal of enrolling 160 participants. Primary outcomes include incidence of AEs, defining the recommended Phase II dose, and ORR in endometrial and ovarian carcinomas. Patients with platinum-refractory disease are excluded. Results are anticipated after August 2024.
NCT05200364 is a Phase 1 open-label multicenter of STRO-002/bevacizumab as combination therapy in patients with advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer. Bevacizumab will be administered at the labeled dose of 15mg/kg IV q3 weeks at the same time as STRO-002 (final dosage to be determined). Primary outcomes are safety and tolerability of the combination, and pharmacokinetics. As of April 2023, the study is still enrolling patients, with a goal of enrolling 58 patients. Results are anticipated after January 2024.
Farletuzumab Ecteribulinm (MORAb-202)
Farletuzumab ecteribulinm (MORAb-202) is composed of a humanized monoclonal antibody targeting FRα linked to a derivative of halichondrin-based microtubule inhibitor eribulin. Eribulin is itself an FDA-approved agent that was first approved for use in patients with metastatic breast cancer in 2010.36 This makes MORAb-202 unique in the ADC space, as most other ADCs have toxic payloads that are not safe for use as monotherapy given their toxicity. Preclinical animal studies of MORAb-202 have shown potent antitumor effect—both direct cytotoxicity as well as bystander effect in patient-derived xenograft (PDX) models with triple-negative breast cancer.37,38
MORAb-202 is currently being evaluated in a Phase II trial of MORAb-202 vs investigator’s choice chemotherapy, in patients with platinum-resistant high grade serous ovarian, peritoneal, or fallopian tube cancer (NCT05613088, Table 1). The investigators plan three experimental cohorts: two different doses of MORAb-202 (specific dosages so far unspecified), and investigator’s choice chemotherapy (either pegylated liposomal doxorubicin or topotecan). The investigators’ primary outcomes are ORR and treatment-related AEs. Secondary outcomes include PFS and OS. Patients with platinum-refractory disease are excluded. The study was initiated on February 1, 2023, and results are anticipated after October 2026.
NCT04300556 is a Phase I/II trial of MORAb-202 in various tumor settings including endometrial and platinum resistant ovarian cancer. Endometrial cancer patients must have relapsed or failed with at least one prior platinum-based chemotherapy or one immunotherapy-based regimen. There is no minimum requirement of FRα expression for participation, but tumor tissue must be available for central testing. Farletuzumab ecteribulin will be administered once every 3 weeks until toxicity, disease progression, or participant withdrawal. Various dosages are being tested to determine the recommended Phase 2 dose.
Human Trophoblast Cell-Surface Marker (Trop-2) Targeted Therapies
Trophoblast cell surface antigen-2 (Trop-2) is encoded by the TACSTD2 gene on chromosome 1p32 and is a 46 kDa transmembrane glycoprotein. Many human tumors of epithelial origin have been found to differentially express Trop-2, and it is known to promote increased proliferation, invasion, and metastasis, although its specific mechanism of action and function remains poorly characterized.39,40 Published studies estimate that Trop-2 is overexpressed in as many as 96% of endometrioid endometrial cancers, and 65% of uterine serous carcinomas.41,42 Trop-2 overexpression has been found to confer worse prognosis in multiple human malignancies, including ovarian cancer.43 Due to its relative overexpression on tumor cells compared to normal tissue cells, Trop-2 has been identified as a potential target for novel cancer immunotherapies.
Sacituzumab Govitecan
Sacituzumab govitecan (IMMU-132) is an ADC comprising an anti-Trop-2 humanized monoclonal antibody hRS7 IgG1k, coupled to a toxic payload SN-38. SN-38 is an active metabolite of irinotecan, a topoisomerase I inhibitor, and is conjugated to the antibody with a hydrolysable linker, CL2A.44,45 When cleaved, SN-38 causes single DNA strand breaks, which develop into double DNA strand breaks if left unrepaired. Apoptosis and cell death ensue.46 Sacituzumab govitecan has now shown considerable promise in early clinical trials for triple-negative breast and urothelial carcinoma; it is now approved by the FDA for use in patients with advanced or metastatic triple-negative breast cancer with two or more prior therapies.47–49
Significant preclinical data suggests that sacituzumab govitecan has utility in epithelial ovarian cancer, and uterine and ovarian carcinosarcomas that express Trop-2.44,50 At present, there are two Phase 2 trials investigating its efficacy that include patients with gynecologic malignancies. NCT03964727 is a Phase 2 open-label study of sacituzumab govitecan in patients with metastatic solid tumors. Allowed tumor types include non-small cell lung cancer, head and neck squamous cell carcinoma, metastatic small cell lung cancer, and endometrial cancer. Patients will receive 10mg/kg of the drug on days 1 and 8 of a 21-day cycle. Patients with endometrial cancer must have progression of disease after platinum-based chemotherapy and anti-PD-(L)1 directed therapy, without more than 3 prior lines of treatment. Patients are excluded if they have received prior topoisomerase I inhibitors. The study is being undertaken at 66 international sites, many of which are still recruiting participants. The study sponsor estimates that it will reach its primary completion in August 2023, and final results are expected after February 2025.
NCT04251416 is a Phase 2 investigator initiated open-label trial for patients with persistent or recurrent endometrial carcinoma regardless of Trop-2 tumoral status. Patients will receive 10mg/kg of sacituzumab govitecan on days 1 and 8 of a 21-day cycle. Primary outcome measures include ORR, OS, PFS, and durable disease control rate. The study is currently recruiting participants, and it is expected to reach its primary completion in February 2024. Survival results are anticipated after February 2026.
SKB264
SKB264 is another novel anti Trop-2 directed ADC. It shares the same monoclonal antibody as IMMU-132 and has 7–8 molecules of a novel toxic payload linked via disulfide bonds. The toxic payload consists of KL610023 (T030), which is a topoisomerase I inhibitor belotecan derivative.51 Preclinical studies have shown promise in Trop-2 positive PDX mouse and monkey models. SKB264 has been shown to have a longer half-life than IMMU-132, with stronger targeting and bystander toxicity.52
NCT04152499 is a Phase 1–2 first-in-human study of SKB264 in patients with locally advanced unresectable/metastatic solid tumors refractory to available standard therapies. Patients with epithelial ovarian cancer, and endometrial carcinoma are included among the list of allowed cancer types. Trop-2 tumoral assessment is not required for enrollment, but the investigators plan to retrospectively assess expression. The Phase 1 component will involve evaluation of dosages from 2 to 12 mg/kg of SKB264 through intravenous infusion (cycle duration is not provided). Investigators aim to assess the ideal drug dosage, maximum tolerated dose, and ORR. The investigators aim to enroll 430 participants and reach primary completion in November 2024. There will be 53 study sites across the US and China.
A second open-label Phase 2 study of SKB264 (NCT05642780) is planned to assess efficacy and safety of SKB264 in combination with pembrolizumab in patients with select solid tumors. Patients with recurrent or metastatic cervical cancer or recurrent ovarian cancer are eligible for participation. Subjects will receive SKB264 as an intravenous infusion on days 1, 15, and 29 of a 42-day cycle, and will receive pembrolizumab as intravenous infusion on day 1 of each 42-day cycle. Primary outcomes include dose limiting toxicities and AEs, as well as ORR. The study is not yet recruiting participants as of April 2023.
NaPi2b Targeted Therapies
NaPi2b is one of a family of epithelial membrane phosphate transporters encoded by the SLC34A2 gene.53 There is evidence that NaPi2b is expressed in high-grade serous epithelial ovarian, fallopian tube, and primary peritoneal cancers, as well as other solid cancer types. It is now known to be absent in normal ovary (ie, benign) epithelium.54 Napi2b is thought to play a role in tumorigenesis from dysregulation of phosphate homeostasis in ovarian, lung, and breast cancers.55 Because of this pathophysiology, Napi2b is an attractive target for ADCs.
Lifastuzumab Vedotin
Lifastuzumab vedotin (LIFA) was the first NaPi2b targeting ADC to be investigated in ovarian cancer. It is comprised of a humanized anti-NaPi2b monoclonal antibody conjugated to monomethyl auristatin E.56 In a Phase 2 open-label trial of patients with platinum-resistant ovarian cancer, LIFA conferred a median PFS of 5.3 months vs 3.1 months with standard-of-care liposomal doxorubicin (p=0.34). Among patients with high-NaPi2b-expressing tumors (as determined on IHC), median PFS was 5.3 vs 3.4 months (p=0.24). While the LIFA cohort experienced a higher ORR (36% vs 14%), no statistically significant improvement in study endpoints such as PFS was noted. LIFA was well tolerated and not increase AEs compared to liposomal doxorubicin.57 Secondary to these discouraging results, the sponsor discontinued LIFA development.55
Upifitamab Rilsodotin
Upifitamab rolsodotin (UpRi, formerly XMT-1536) is a novel NaPi2b-targeting ADC. It is unique in its drug to antibody (DAR) ratio of 10, as well as an auristatin F-HPA toxic payload with only limited diffusion capacity, which serves to control its bystander effect and further limit off-target toxicity.58 UpRi was recently investigated in a Phase 1/1b trial of patients with high grade serous epithelial ovarian, fallopian tube, and primary peritoneal cancers, with favorable safety, tolerability, and efficacy results. This study enrolled 97 patients and administered 36 or 43 mg/m2 up to a maximum dose of ~80 mg intravenous every four weeks. A 64% of patients with known NaPi2b scores were found to have high expression of NaPi2b. Of these NaPi2b-high patients, ORR was 34%, and median duration of response was five months. In the overall population, ORR was 23%. A 28% of patients had to dose-reduce due to adverse effects of the therapy, which were most commonly fatigue, anemia, and thrombocytopenia.59
These encouraging phase 1 efficacy data support the investigation of UpRi clinical benefit in ongoing clinical trials (Table 1): The Phase 2 UPLIFT trial (NCT03319628), UpRi monotherapy in platinum-resistant, high-grade serous ovarian cancer with up to four prior lines of chemotherapy, the Phase 1/2 UPGRADE trial (NCT04907968), which is investigating UpRi in combination with other agents in patients with platinum-sensitive ovarian cancer, and the phase 3 multi-center, randomized, double-blind, placebo-controlled UP-NEXT trial (NCT05329545), evaluating UpRi monotherapy as maintenance vs placebo in patients with recurrent, platinum-sensitive high-grade ovarian cancer with NaPi2b-positive tumors. For the UP-NEXT trial, patients are required to have had 4–8 cycles of platinum-based chemotherapy in their most recent treatment regimen, with stable disease, partial response, complete response, or no evidence of disease. Notably, patients who received prior treatment with mirvetuximab soravtansine will be excluded. The investigators hope to accrue 350 participants across 56 international locations, and estimate primary completion by September 2024, with preliminary results available after March 2025.
Other Targets for Gynecologic Malignancies
Mesothelin
Mesothelin is a cell-surface membrane glycoprotein and normally expressed in mesothelial cells lining the pleura, pericardium and peritoneum. Although mesothelin has restricted expression in normal tissue, it is overexpressed in a number of cancers including up to 70% of ovarian cancer. Mesothelin may be involved in cell adhesion and metastasis, making it an attractive tumor-specific target.60 A number of anti-mesothelin ADCs are under investigation, most notably Anetumab ravtansine (BAY 94-9343), which is composed of a fully humanized anti-mesothelin monoclonal antibody, a disulfide linker and tubulin-inhibitor DM4 as the toxic payload.61
The first-in-human phase 1 study to evaluate for safety and tolerability of anetumab ravtansine included 148 patients with multiple solid tumors, including 21 patients with advanced ovarian cancer. The maximum tolerated and recommended dose for phase 2 study was 6.5 mg/kg every 21 days. This Phase 1 study found the treatment to be relatively well tolerated, with common drug-related AEs including nausea/vomiting, diarrhea, peripheral sensory neuropathy. Ocular AEs were mitigated with strategies previously used for other ADCs and were mostly resolving at the end of treatment. A second phase Ib dose escalation and expansion study investigated the combination of anetumab ravtansine and pegylated-liposomal doxorubicin in platinum-resistant ovarian cancer. In 65 treated patients, the ORR was 27.7% (95% CI, 17.3 to 40.2), including 1 patient with complete response and 17 with partial response. The median duration of response was 7.6 months (95% CI 3.3 to 10.2 months), and medial progression-free survival was 5.0 months (95% CI, 3.2 to 6.0). These results show that ADCs targeting mesothelin may have clinical activity in advanced ovarian cancer.62 Further trials investigating this ADC are ongoing (Table 1).
DMOT4039A is a humanized anti-mesothelin monoclonal antibody conjugated to antimitotic monomethyl auristatin E (MMAE) through a protease-labile valine-citrulline linker. A phase 1 study investigated the use of DMOT4039A in unresectable/metastatic pancreatic cancer or platinum-resistant ovarian cancer. A total of 71 patients were enrolled, 31 of whom had ovarian cancer. The maximum tolerated dose was determined to be 2.4 mg/kg every 21 days. Three out of 10 ovarian cancer patients treated with MTD demonstrated partial responses by RECIST criteria, as well as concurrent decrease in CA125; the median progression-free survival for ovarian cancer patients at the MTD was 4.9 months. The safety profile of DMOT4039A was similar to that of prior agents with microtubule inhibitor payload, and common AEs included gastrointestinal toxicities, fatigue, and cumulative peripheral neuropathy. Interestingly, serum mesothelin levels and immunohistochemistry scores for mesothelin in tissue were not associated with clinical efficacy of DMOT4039A. Further antitumor activity and clinical efficacy remain to be assessed in phase 2 studies.63
BMS-986148 is a mesothelin-targeting ADC that consists of a fully human anti-mesothelin monoclonal antibody conjugated to toxic payload tubulysin through a valine-citrulline linker. The combination of BMS-986148 and the anti-programmed death (PD)-1 drug nivolumab was evaluated in a phase 1/2a trial assessing safety, tolerability and preliminary efficacy in patients with mesothelin-expressing tumors. Clinical activity in either BMS-986148 monotherapy or in combination therapy with nivolumab was observed in 10 of 126 patients, and 2 ovarian cancer patients had confirmed partial response, with duration of response 19.9 and 3.0 months, respectively. The disease-control rate (defined by complete/partial response or stable disease) was 56% in mesothelioma patients and 59% in ovarian cancer patients. The overall safety profile was acceptable, with hepatic TRAEs among most common dose-limiting TRAEs associated with BMS-986148. Ocular AEs were reported in <10% of patients treated with BMS-986148 or combination therapy, and the majority of ocular AEs were low grade.25
MUC16 (CA125)
MUC16 is a type I transmembrane mucin that is frequently overexpressed by ovarian cancers and a precursor of CA125, a commonly used biomarker for recurrent ovarian cancer.64 A number of ADCs target MUC16: DMUC4064A, a humanized anti-MUC16 monoclonal antibody with a protease cleavable linker and monomethyl auristatin E (MMAE) as toxic payload, was studied in a phase 1 dose-escalation study in patients with platinum-resistant ovarian cancer. Notably, DMUC4064A utilizes site-directed conjugation of the antibody to linker-drug, and thus delivers a more homogeneous payload to its targets.65 Prior to the sponsor’s decision to discontinue development on this molecule, which was not due to a safety concern, this clinical trial enrolled 65 patients who received a medial of 5 cycles of treatment. A 85% of patients experienced at least 1 AE related to DMUC4064A, and the most frequent AEs include fatigue, nausea, blurred vision, electrolyte abnormalities and peripheral neuropathy. Of enrolled patients, 43% experienced an ocular AE; however, all were within grade 3. Sixteen patients had a confirmed partial response, and 1 patient (at the dose level of 5.2 mg/kg) experienced a complete response. The overall clinical benefit rate (CR, PR or SD lasting at least 6 months) was 42%, median PFS was 3.9 months (95% CI, 2.6 to 4.9) in the overall trial and 5.3 months (95% CI, 3.9 to 7.4) in the cohort receiving higher treatment dose (5.2 mg/kg). A 58% of patients achieved a reduction of CA125 by over 79%.66
Conclusion
ADCs present the potential for significant, field-defining improvements in the care of gynecologic malignancies, where there exists an ongoing unmet need for well tolerated, novel, and effective therapies. When compared to traditional cytotoxic systemic chemotherapies, ADCs stand to provide significant improvements in specificity, tolerability, and effectivity. As ADCs deliver their toxic payloads directly to tumors that express the specific antigen they are targeting, toxicity to healthy and normal cells is minimized.6 With these therapy advancements, patients may stay healthier and have better quality of lives while on systemic therapy for their gynecologic malignancies. While we currently have limited data on the survival advantages conferred by ADCs to patients with gynecologic malignancies, the recent FDA approvals of tisotumab vedotin and mirvetuximab soravtansine and the many Phase III trials underway with a variety of ADCs suggest that this novel therapeutic approach may represent a promising and efficient tool for targeted gynecologic cancer therapy. ADCs are ushering the treatment of gynecologic malignancies into today’s era of personalized cancer treatment.
Funding
This work did not receive any financial support.
Disclosure
Dr Alessandro Santin reports personal fees from Eisai, Merck, R-Pharm; grants from Merck, R-Pharm, Gilead, ImmunoGen, Boehringer Ingelheim, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
2. Colombo N, Dubot C, Lorusso D, et al. Pembrolizumab for persistent, recurrent, or metastatic cervical cancer. N Engl J Med. 2021;385(20):1856–1867. doi:10.1056/NEJMoa2112435
3. Eskander RN, Sill MW, Beffa L, et al. Pembrolizumab plus chemotherapy in advanced endometrial cancer. N Engl J Med. 2023;388(23). doi:10.1056/NEJMoa2302312
4. González-Martín A, Pothuri B, Vergote I, et al. Niraparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med. 2019;381(25):2391–2402. doi:10.1056/NEJMoa1910962
5. Pujade-Lauraine E, Hilpert F, Weber B, et al. Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: the AURELIA open-label randomized phase III trial. JCO. 2014;32(13):1302–1308. doi:10.1200/JCO.2013.51.4489
6. Birrer MJ, Moore KN, Betella I, Bates RC. Antibody-drug conjugate-based therapeutics: state of the science. J Natl Cancer Inst. 2019;111(6):538–549. doi:10.1093/jnci/djz035
7. Coleman RL, Lorusso D, Gennigens C, et al. Efficacy and safety of tisotumab vedotin in previously treated recurrent or metastatic cervical cancer (innovaTV 204/GOG-3023/ENGOT-cx6): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2021;22(5):609–619. doi:10.1016/S1470-2045(21)00056-5
8. Heo YA. Mirvetuximab soravtansine: first approval. Drugs. 2023;83(3):265–273. doi:10.1007/s40265-023-01834-3
9. Matulonis UA, Lorusso D, Oaknin A, et al. Efficacy and safety of mirvetuximab soravtansine in patients with platinum-resistant ovarian cancer with high folate receptor alpha expression: results from the SORAYA study. J Clin Oncol. 2023. doi:10.1200/JCO.22.01900
10. Moore K, Konecny G, Martin L, et al. MIRASOL: a randomized, open-label, phase 3 study of mirvetuximab soravtansine vs. investigator’s choice of chemotherapy in advanced high-grade epithelial ovarian, primary peritoneal, or fallopian tube cancers with high folate-alpha (FRα) expression (297). Gynecol Oncol. 2022;166:S156–S157. doi:10.1016/S0090-8258(22)01518-9
11. Moore KN, Oza AM, Colombo N, et al. Phase III, randomized trial of mirvetuximab soravtansine versus chemotherapy in patients with platinum-resistant ovarian cancer: primary analysis of FORWARD I. Ann Oncol. 2021;32(6):757–765. doi:10.1016/j.annonc.2021.02.017
12. Citri A, Yarden Y. EGF-ERBB signalling: towards the systems level. Nat Rev Mol Cell Biol. 2006;7(7):505–516. doi:10.1038/nrm1962
13. Diver EJ, Foster R, Rueda BR, Growdon WB. The therapeutic challenge of targeting HER2 in endometrial cancer. Oncologist. 2015;20(9):1058–1068. doi:10.1634/theoncologist.2015-0149
14. Luo H, Xu X, Ye M, Sheng B, Zhu X. The prognostic value of HER2 in ovarian cancer: a meta-analysis of observational studies. PLoS One. 2018;13(1):e0191972. doi:10.1371/journal.pone.0191972
15. Tuefferd M, Couturier J, Penault-Llorca F, et al. HER2 status in ovarian carcinomas: a multicenter GINECO study of 320 patients. PLoS One. 2007;2(11):e1138. doi:10.1371/journal.pone.0001138
16. Morrison C, Zanagnolo V, Ramirez N, et al. HER-2 is an independent prognostic factor in endometrial cancer: association with outcome in a large cohort of surgically staged patients. J Clin Oncol. 2006;24(15):2376–2385. doi:10.1200/JCO.2005.03.4827
17. Fader AN, Roque DM, Siegel E, et al. Randomized phase II trial of carboplatin-paclitaxel compared to carboplatin-paclitaxel-trastuzumab in advanced (stage III-IV) or recurrent uterine serous carcinomas that overexpress Her2/Neu (NCT01367002): updated overall survival analysis. Clin Cancer Res. 2020;26(15):3928–3935. doi:10.1158/1078-0432.CCR-20-0953
18. Ogitani Y, Aida T, Hagihara K, et al. DS-8201a, A novel HER2-targeting ADC with a novel DNA topoisomerase I inhibitor, demonstrates a promising antitumor efficacy with differentiation from T-DM1. Clin Cancer Res. 2016;22(20):5097–5108. doi:10.1158/1078-0432.CCR-15-2822
19. Nishikawa T, Hasegawa K, Matsumoto K, et al. Trastuzumab deruxtecan for human epidermal growth factor receptor 2-expressing advanced or recurrent uterine carcinosarcoma (NCCH1615): the STATICE trial. J Clin Oncol. 2023;41(15):2789–2799. doi:10.1200/JCO.22.02558
20. Tsurutani J, Iwata H, Krop I, et al. Targeting HER2 with trastuzumab deruxtecan: a dose-expansion, phase I study in multiple advanced solid tumors. Cancer Discov. 2020;10(5):688–701. doi:10.1158/2159-8290.CD-19-1014
21. Mauricio D, Bellone S, Mutlu L, et al. Trastuzumab deruxtecan (DS-8201a), a HER2-targeting antibody-drug conjugate with topoisomerase I inhibitor payload, shows antitumor activity in uterine and ovarian carcinosarcoma with HER2/neu expression. Gynecol Oncol. 2023;170:38–45. doi:10.1016/j.ygyno.2022.12.018
22. Narayan P, Osgood CL, Singh H, et al. FDA approval summary: fam-trastuzumab deruxtecan-nxki for the treatment of unresectable or metastatic HER2-positive breast cancer. Clin Cancer Res. 2021;27(16):4478–4485. doi:10.1158/1078-0432.CCR-20-4557
23. The Center for Drug Evaluation and Research. FDA grants accelerated approval to fam-trastuzumab deruxtecan-nxki for HER2-mutant non-small cell lung cancer. FDA; 2022. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-fam-trastuzumab-deruxtecan-nxki-her2-mutant-non-small-cell-lung.
24. US Food and Drug Administration. Office of the Commissioner. FDA approves first targeted therapy for HER2-low breast cancer. US Food and Drug Administration; 2022. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-first-targeted-therapy-her2-low-breast-cancer.
25. Banerji U, van Herpen CML, Saura C, et al. Trastuzumab duocarmazine in locally advanced and metastatic solid tumours and HER2-expressing breast cancer: a phase 1 dose-escalation and dose-expansion study. Lancet Oncol. 2019;20(8):1124–1135. doi:10.1016/S1470-2045(19)30328-6
26. Black J, Menderes G, Bellone S, et al. SYD985, a novel duocarmycin-based HER2-targeting antibody-drug conjugate, shows antitumor activity in uterine serous carcinoma with HER2/Neu expression. Mol Cancer Ther. 2016;15(8):1900–1909. doi:10.1158/1535-7163.MCT-16-0163
27. Menderes G, Bonazzoli E, Bellone S, et al. SYD985, a novel duocarmycin-based HER2-targeting antibody-drug conjugate, shows antitumor activity in uterine and Ovarian carcinosarcoma with HER2/Neu expression. Clin Cancer Res. 2017;23(19):5836–5845. doi:10.1158/1078-0432.CCR-16-2862
28. Menderes G, Bonazzoli E, Bellone S, et al. SYD985, a novel duocarmycin-based HER2-targeting antibody-drug conjugate, shows promising antitumor activity in epithelial ovarian carcinoma with HER2/Neu expression. Gynecol Oncol. 2017;146(1):179–186. doi:10.1016/j.ygyno.2017.04.023
29. Kelemen LE. The role of folate receptor α in cancer development, progression and treatment: cause, consequence or innocent bystander? Int J Cancer. 2006;119(2):243–250. doi:10.1002/ijc.21712
30. Parker N, Turk MJ, Westrick E, Lewis JD, Low PS, Leamon CP. Folate receptor expression in carcinomas and normal tissues determined by a quantitative radioligand binding assay. Anal Biochem. 2005;338(2):284–293. doi:10.1016/j.ab.2004.12.026
31. Senol S, Ceyran AB, Aydin A, et al. Folate receptor α expression and significance in endometrioid endometrium carcinoma and endometrial hyperplasia. Int J Clin Exp Pathol. 2015;8(5):5633–5641.
32. Kalli KR, Oberg AL, Keeney GL, et al. Folate receptor alpha as a tumor target in epithelial ovarian cancer. Gynecol Oncol. 2008;108(3):619–626. doi:10.1016/j.ygyno.2007.11.020
33. Dainty LA, Risinger JI, Morrison C, et al. Overexpression of folate binding protein and mesothelin are associated with uterine serous carcinoma. Gynecol Oncol. 2007;105(3):563–570. doi:10.1016/j.ygyno.2006.10.063
34. O’Shannessy DJ, Somers EB, Smale R, Fu YS. Expression of Folate Receptor-α (FRA) in gynecologic malignancies and its relationship to the tumor type. Int J Gynecol Pathol. 2013;32(3):258. doi:10.1097/PGP.0b013e3182774562
35. Li X, Zhou S, Abrahams CL, et al. Discovery of STRO-002, a novel homogeneous ADC targeting folate receptor alpha, for the treatment of ovarian and endometrial cancers. Mol Cancer Ther. 2023;22(2):155–167. doi:10.1158/1535-7163.MCT-22-0322
36. Cortes J, O’Shaughnessy J, Loesch D, et al. Eribulin monotherapy versus treatment of physician’s choice in patients with metastatic breast cancer (EMBRACE): a phase 3 open-label randomised study. Lancet. 2011;377(9769):914–923. doi:10.1016/S0140-6736(11)60070-6
37. Cheng X, Li J, Tanaka K, et al. MORAb-202, an antibody-drug conjugate utilizing humanized anti-human FRα farletuzumab and the microtubule-targeting agent eribulin, has potent antitumor activity. Mol Cancer Ther. 2018;17(12):2665–2675. doi:10.1158/1535-7163.MCT-17-1215
38. Furuuchi K, Rybinski K, Fulmer J, et al. Antibody-drug conjugate MORAb-202 exhibits long-lasting antitumor efficacy in TNBC PDx models. Cancer Sci. 2021;112(6):2467–2480. doi:10.1111/cas.14898
39. Goldenberg DM, Stein R, Sharkey RM. The emergence of trophoblast cell-surface antigen 2 (TROP-2) as a novel cancer target. Oncotarget. 2018;9(48):28989–29006. doi:10.18632/oncotarget.25615
40. Trerotola M, Cantanelli P, Guerra E, et al. Upregulation of Trop-2 quantitatively stimulates human cancer growth. Oncogene. 2013;32(2):222–233. doi:10.1038/onc.2012.36
41. Bignotti E, Ravaggi A, Romani C, et al. Trop-2 overexpression in poorly differentiated endometrial endometrioid carcinoma: implications for immunotherapy with hRS7, a humanized anti-trop-2 monoclonal antibody. Int J Gynecol Cancer. 2011;21(9):1613–1621. doi:10.1097/IGC.0b013e318228f6da
42. Varughese J, Cocco E, Bellone S, et al. Uterine serous papillary carcinomas overexpress human trophoblast-cell-surface marker (Trop-2) and are highly sensitive to immunotherapy with hRS7, a humanized anti-Trop-2 monoclonal antibody. Cancer. 2011;117(14):3163–3172. doi:10.1002/cncr.25891
43. Bignotti E, Todeschini P, Calza S, et al. Trop-2 overexpression as an independent marker for poor overall survival in ovarian carcinoma patients. Eur J Cancer. 2010;46(5):944–953. doi:10.1016/j.ejca.2009.12.019
44. Perrone E, Lopez S, Zeybek B, et al. Preclinical activity of sacituzumab govitecan, an antibody-drug conjugate targeting trophoblast cell-surface antigen 2 (Trop-2) linked to the active metabolite of irinotecan (SN-38), in ovarian cancer. Front Oncol. 2020;10:118. doi:10.3389/fonc.2020.00118
45. Bardia A, Messersmith WA, Kio EA, et al. Sacituzumab govitecan, a Trop-2-directed antibody-drug conjugate, for patients with epithelial cancer: final safety and efficacy results from the phase I/II IMMU-132-01 basket trial. Ann Oncol. 2021;32(6):746–756. doi:10.1016/j.annonc.2021.03.005
46. Cardillo TM, Govindan SV, Sharkey RM, et al. Sacituzumab govitecan (IMMU-132), an anti-trop-2/SN-38 antibody-drug conjugate: characterization and efficacy in pancreatic, gastric, and other cancers. Bioconjug Chem. 2015;26(5):919–931. doi:10.1021/acs.bioconjchem.5b00223
47. Furlanetto J, Marmé F, Loibl S. Sacituzumab govitecan: past, present and future of a new antibody–drug conjugate and future horizon. Future Oncol. 2022;18(28):3199–3215. doi:10.2217/fon-2022-0407
48. Syed YY. Sacituzumab Govitecan: first Approval. Drugs. 2020;80(10):1019–1025. doi:10.1007/s40265-020-01337-5
49. Bardia A, Hurvitz SA, Tolaney SM, et al. Sacituzumab govitecan in metastatic triple-negative breast cancer. N Engl J Med. 2021;384(16):1529–1541. doi:10.1056/NEJMoa2028485
50. Lopez S, Perrone E, Bellone S, et al. Preclinical activity of sacituzumab govitecan (IMMU-132) in uterine and ovarian carcinosarcomas. Oncotarget. 2020;11(5):560–570. doi:10.18632/oncotarget.27342
51. Lee JH, Lee JM, Kim JK, et al. Antitumor activity of 7-[2-(N-isopropylamino)ethyl]-(20S)-camptothecin, CKD602, as a potent DNA topoisomerase I inhibitor. Arch Pharm Res. 1998;21(5):581–590. doi:10.1007/BF02975379
52. Cheng Y, Yuan X, Tian Q, et al. Preclinical profiles of SKB264, a novel anti-TROP2 antibody conjugated to topoisomerase inhibitor, demonstrated promising antitumor efficacy compared to IMMU-132. Front Oncol. 2022;12:951589. doi:10.3389/fonc.2022.951589
53. Marks J. The role of SLC34A2 in intestinal phosphate absorption and phosphate homeostasis. Pflugers Arch Eur J Physiol. 2019;471(1):165–173. doi:10.1007/s00424-018-2221-1
54. Levan K, Mehryar M, Mateoiu C, Albertsson P, Bäck T, Sundfeldt K. Immunohistochemical evaluation of epithelial ovarian carcinomas identifies three different expression patterns of the MX35 antigen, NaPi2b. BMC Cancer. 2017;17(1). doi:10.1186/s12885-017-3289-2
55. Banerjee S, Drapkin R, Richardson DL, Birrer M. Targeting NaPi2b in ovarian cancer. Cancer Treat Rev. 2023;112:102489. doi:10.1016/j.ctrv.2022.102489
56. Moore KN, Birrer MJ, Marsters J, et al. Phase 1b study of anti-NaPi2b antibody-drug conjugate lifastuzumab vedotin (DNIB0600A) in patients with platinum-sensitive recurrent ovarian cancer. Gynecol Oncol. 2020;158(3):631–639. doi:10.1016/j.ygyno.2020.05.039
57. Banerjee S, Oza AM, Birrer MJ, et al. Anti-NaPi2b antibody–drug conjugate lifastuzumab vedotin (DNIB0600A) compared with pegylated liposomal doxorubicin in patients with platinum-resistant ovarian cancer in a randomized, open-label, phase II study. Ann Oncol. 2018;29(4):917–923. doi:10.1093/annonc/mdy023
58. Mosher R, Poling L, Qin L, Bodyak N, Bergstrom D. Abstract B119: relationship of NaPi2b expression and efficacy of XMT-1536, a NaPi2b targeting antibody-drug conjugate (ADC), in an unselected panel of human primary ovarian mouse xenograft models. Mol Cancer Ther. 2018;17(1_Supplement):B119. doi:10.1158/1535-7163.TARG-17-B119
59. Richardson D, Hamilton E, Barve M, et al. Updated results from the phase 1 expansion study of upifitamab rilsodotin (UpRi; XMT-1536), a NaPi2b-directed dolaflexin Antibody Drug Conjugate (ADC) in ovarian cancer (076). Gynecol Oncol. 2022;166:S48. doi:10.1016/S0090-8258(22)01294-X
60. Rump A, Morikawa Y, Tanaka M, et al. Binding of ovarian cancer antigen CA125/MUC16 to mesothelin mediates cell adhesion *. J Biol Chem. 2004;279(10):9190–9198. doi:10.1074/jbc.M312372200
61. Hassan R, Blumenschein GR, Moore KN, et al. First-in-human, multicenter, phase I dose-escalation and expansion study of anti-mesothelin antibody–drug conjugate anetumab ravtansine in advanced or metastatic solid tumors. J Clin Oncol. 2020;38(16):1824–1835. doi:10.1200/JCO.19.02085
62. Santin AD, Vergote I, González-Martín A, et al. Safety and activity of anti-mesothelin antibody–drug conjugate anetumab ravtansine in combination with pegylated-liposomal doxorubicin in platinum-resistant ovarian cancer: multicenter, Phase Ib dose escalation and expansion study. Int J Gynecol Cancer. 2022. doi:10.1136/ijgc-2022-003927
63. Weekes CD, Lamberts LE, Borad MJ, et al. Phase I study of DMOT4039A, an antibody–drug conjugate targeting mesothelin, in patients with unresectable pancreatic or platinum-resistant ovarian cancer. Mol Cancer Ther. 2016;15(3):439–447. doi:10.1158/1535-7163.MCT-15-0693
64. Yin BWT, Lloyd KO. Molecular cloning of the CA125 ovarian cancer antigen: IDENTIFICATION AS A NEW MUCIN, MUC16*. J Biol Chem. 2001;276(29):27371–27375. doi:10.1074/jbc.M103554200
65. Ohri R, Bhakta S, Fourie-O’Donohue A, et al. High-throughput cysteine scanning to identify stable antibody conjugation sites for maleimide- and disulfide-based linkers. Bioconjug Chem. 2018;29(2):473–485. doi:10.1021/acs.bioconjchem.7b00791
66. Liu J, Burris H, Wang JS, et al. An open-label phase I dose-escalation study of the safety and pharmacokinetics of DMUC4064A in patients with platinum-resistant ovarian cancer. Gynecol Oncol. 2021;163(3):473–480. doi:10.1016/j.ygyno.2021.09.023
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.