Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Association of Red Cell Index and Adverse Hospitalization Outcomes in Chronic Obstructive Pulmonary Disease Patients with Acute Exacerbation: A Retrospective Cohort Study
Authors Yuan F ![]() , Shui W, Xing Y, Niu Y, Zhang X, Zhang C
, Shui W, Xing Y, Niu Y, Zhang X, Zhang C
Received 13 May 2022
Accepted for publication 22 August 2022
Published 15 September 2022 Volume 2022:17 Pages 2263—2275
DOI https://doi.org/10.2147/COPD.S373114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Fu-zhen Yuan,1 Wei Shui,2 Yan-li Xing,2 Yuan-yuan Niu,2 Xin Zhang,2 Chang-ran Zhang2
1Department of General Practice Medicine, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Department of General Medicine, The Eastern Hospital of the First Affiliated Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China
Correspondence: Chang-ran Zhang, Department of General Medicine, The Eastern Hospital of the First Affiliated Hospital, Sun Yat-sen University, No. 183, Huangpu East Road, Huangpu District, Guangzhou, People’s Republic of China, Tel +86 13711409903, Email [email protected]
Purpose: Previous studies have shown that the red cell index (RCI) can be considered as a simple and useful method to evaluate respiratory function. However, at present its association with adverse hospitalization outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is not fully understood. Our study aimed to examine the relationship between adverse hospitalization outcomes and RCI among AECOPD patients.
Patients and Methods: We performed a retrospective analysis of consecutive patients from January 2015 to October 2021. In this study, RCI was the independent variable, measured at baseline, and adverse hospitalization outcome was the dependent variable. According to the RCI median (RCI=2.221), we divided 377 patients into two roughly equal groups (188 and 189, respectively). Next, the association between RCI and adverse hospitalization outcomes was explored using multivariable logistic regression models. To identify any non-linear relationship, a generalized additive model (GAM) was employed.
Results: With a total of 377 patients with AECOPD, we divided them into two roughly equal groups to compare the clinical factors and RCI levels. The patients in the higher RCI group showed poorer outcome incidence (18 [9.57%] vs 31 [16.40%]; p = 0.049). After accounting for potential confounders, the results showed that RCI was positively associated with adverse hospitalization outcomes (odds ratio [OR] = 1.15, 95% CI: 1.01– 1.32). In addition, a non-linear relationship was detected between RCI and adverse hospitalization outcomes, which had an inflection point of 3.2. There were odds ratios and confidence intervals of 0.8 (0.7– 1.0) and 1.3 (1.2– 1.4) on the left and right sides of the inflection point, respectively.
Conclusion: The RCI and adverse hospitalization outcomes exhibited a non-linear relationship in the AECOPD patients. RCI is strongly positively correlated with adverse hospitalization outcomes when it was greater than 3.2.
Keywords: AECOPD, RCI, worse hospitalization outcomes, non-linearity
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable and treatable chronic lung disease that causes progressive breathing difficulties. According to the World Health Organization, in 2019, 3.23 million people died from COPD globally, accounting for 6% of all global deaths in that year, and over 90% of these deaths occurred in low- and middle-income countries, including China.1 Over the next 40 years, the prevalence of COPD is expected to rise, with more than 5.4 million people likely to die from COPD and related conditions each year by 2060.2–4 AECOPD is defined as ≥2 respiratory symptoms (increased frequency or severity of cough, increased sputum volume or purulent sputum, and wheezing) that cause the patient’s attending physician to change the original treatment.5 It is the most common cause of hospitalization and a significant contributor to mortality among COPD patients.6
The diagnosis of COPD is currently based on a forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) ratio of less than 0.70 as determined by spirometry after bronchodilator use.5 For many years, physical methods have been used to evaluate pulmonary ventilation and respiratory function, such as the vital capacity test.7,8 However, these methods are often susceptible to patient subjective factors, and they are particularly inappropriate for children and bedridden individuals. A blood gas analysis can be used for evaluating the respiratory function of bedridden patients. When using this method, it is crucial to collect arterial blood samples under vacuum conditions and then to perform rapid analysis under vacuum. The results may be affected if the preliminary treatment is not appropriate.9
It is known that increased levels of red blood cells (RBC) and hemoglobin (Hb) can compensate for poor pulmonary function and reflects hypoxia sensitivity.10 These values may therefore be considered an appropriate criterion for evaluating respiratory function.11 In COPD patients, lymphocytes (Lym) are the main inflammatory cells in the central airways and lung parenchyma, which is correlated with the number of alveolar injuries and the extent of airway obstruction.12 Platelets (PLT) and their functional consequences in COPD are of interest. There has been previous evidence that platelets and platelet activation influence bronchoconstriction, bronchial reactivity, inflammation, and remodeling in the airways in animals.13 Guang et al have been demonstrated that lymphocytes and platelets can be used to measure blood cell proliferation as a baseline.11 Now, the red blood cell index (RCI) is being used, and it’s based upon platelet count, lymphocyte count, hemoglobin and red blood cells count. The formula for calculating RCI is as follows: (RBC × Hb)/(Lym × PLT).11 RCI is inversely proportional to pulmonary function in theory, and it can be used to measure pulmonary function.11,14 However, its association with poorer outcomes among AECOPD patients is not fully understood.
This study aimed to investigate the association between adverse hospitalization outcomes and RCI in patients with AECOPD.
Patients and Methods
Study Population
Patients with AECOPD who were admitted in the First Affiliated Hospital of Sun Yat-sen University from January 2015 to October 2021 were retrospectively and consecutively enrolled in this study.
The patients were included this study if they met the following criteria: 1) the diagnosis of COPD was made by a pulmonary specialist based on past smoking history, clinical evaluation, and pulmonary function testing which showed air flow obstruction even when taken with bronchodilators (forced expiratory volume in 1 second to forced vital capacity of less than 0.70);5,15 2) AECOPD is defined as an acute worsening of respiratory symptoms such as dyspnea, cough, and sputum volume or purulence;5 and 3) age ≥40 years. In cases where a patient had been admitted to the hospital multiple times, only the first admission was recorded. The following patients were excluded: 1) other respiratory diseases, such as bronchiectasis, lung cancer, asthma, tuberculosis, interstitial lung disease; 2) severe cardiovascular disease, including acute left heart failure; 3) septic shock; 4) diseases of the blood system, including chronic lymphocytic leukemia, multiple myeloma, myelofibrosis etc. Finally, a total of 377 patients were included in the study (Figure 1).
 |
Figure 1 Flowchart of the study participants. Abbreviation: AECOPD, acute exacerbation of chronic obstructive pulmonary disease. |
This study was conducted in accordance with the Declaration of Helsinki, and the protocol was reviewed and approved by the institutional review board of the First Affiliated Hospital of Sun Yat-sen University.
Data Collection
We collected demographic and clinical data from electronic medical records, including sex, age, BMI, drinking history, smoking history, comorbidities, length of hospital stay, and vital capacity parameters from the last stable period in the last two years (FEV1/FVC, FEV1% Pred, FEV1 and FVC). We collected the blood count and other inflammatory parameters at the time of admission before administering antibiotics and steroids. Additionally, blood samples were collected for analysis of arterial blood gas (PaO2, PaCO2 and pH value). In this study, smoking was categorized into three classes: never-smoker (never smoked in their lifetime), current smoker (smoked in the past year) and ever-smoker (smoked sometime in their lifetime, but not currently). The RCI of each subject was calculated and analyzed. The formula for calculating RCI was as follows: (RBC × Hb)/(Lym × PLT).11 Each participant’s clinical outcomes were recorded. Patients who met any of these three criteria were considered to have a poor hospitalization outcome: requiring invasive ventilator, intensive care unit (ICU) admission, or death in hospital.
Statistical Analysis
Continuous variables are presented as mean ± SDs (normal distribution) or medians and IQRs (skewed distribution), while categorical variables are presented as number (%). One-Way Anova tests (normal distribution), Kruskal–Wallis H (skewed distribution) test and chi-square tests (categorical variables) were used to determine any statistical differences between the means and proportions of the groups.
Firstly, a univariate model was used to evaluate whether the RCI and other biochemical variables were associated with adverse hospitalization outcomes. Secondly, to determine the relationship between adverse hospitalization outcomes and the RCI, a smooth curve was fitted. Once non-linearity was detected, the inflection point was calculated using the recursive algorithm, then a two-piecewise linear regression on either side of the inflection point was constructed. We then compared the two-piecewise linear regression model and one-line model. The optimal fitting model was determined according to the p-value of logarithmic likelihood ratio test. If the P value of less than 0.001 for the log-likelihood ratio test indicates that the two-side linear regression was more appropriate for fitting the association between RCI and adverse outcomes, because it can accurately reflect the relationship between them. Thirdly, multivariate logistic regression models were used to examine whether RCI had an independent effect on adverse hospitalization outcomes. We used the following principles to determine whether the potential confounders were adjusted: reported as relevant or used in previous studies14,16 (especially in the study about predictor of AECOPD) and the potential confounders effect estimates individually changed by at least 10%.17 A total of three models were established: the crude model did not adjust other covariates; model 1 adjusted for age, sex, BMI and smoking status; model 2 further adjusted for comorbidities (including hypertension, diabetes, congestive heart failure, coronary artery disease, chronic kidney disease and arrhythmia), therapy in stable stage, inflammatory parameters (including PCT, CRP, LDH), FEV1/FVC, and PaCO2. Finally, we performed subgroup analysis using the stratified linear regression model. Interactions were evaluated using likelihood ratio tests. Since 18.8% of patients were missing BMI and 34% were missing CRP, we used multiple imputations (MIs), based on five replications and a chained equation approach method in the R MI procedure.18,19 Then, the regression coefficients and standard error of five regression models were combined.20
All analyses were performed using Empower (R) (http://www.empowerstats.com, X&Y Solutions, Inc., Boston, MA) and R (http://www.R-project.org, The R Foundation). A p-value of <0.05 was considered statistically significant.
Results
Baseline Characteristics of the Study Subjects and Univariate Analyses
According to the RCI median (RCI=2.221), we divided the 377 patients into two equal groups: RCI<2.221 was defined as the lower RCI group (n=188), while RCI≥2.221 was defined as the higher RCI group (n=189). The clinical characteristics of participants are listed in Table 1. We found no significant differences between the two groups in terms of age, sex, and BMI. Compared with the lower RCI group, the RCI (4.7 ± 2.4 vs 1.4 ± 0.5, p < 0.001), red blood cell (4.7 ± 0.7 vs 4.4 ± 0.8, p < 0.001), hemoglobin (136.1 ± 16.8 vs 127.7 ± 22.8, p < 0.001), CRP (16.8 [4.6,56.4] vs 6.0 [2.0,39.0], p = 0.001), LDH (231.7 ± 116.9 vs 215.2 ± 83.0, p = 0.017), length of stay (10.2 ± 5.7 vs 9.5 ± 11.1, p < 0.001), poorer outcome (31 [16.4%] vs 18 [9.6%], p = 0.049) levels in the higher RCI group were higher. Inversely, compared with the lower RCI group, the lymphocytes (0.9 ± 0.4 vs 1.7 ± 0.6, p < 0.001) and platelet (188.9 ± 60.5 vs 276.6 ± 101.6, p < 0.001) levels in the higher RCI group were lower. In addition, higher PaCO2 (59.7 ± 20.3 vs 49.3 ± 16.7, p < 0.001) and lower FEV1 (0.7 ± 0.3 vs 0.8 ± 0.3, p = 0.028), FEV1%Pred (32.9±14.8 vs 34.7 ± 13.6) were observed among the AECOPD patients with higher RCI. However, there was no significant difference between the two groups in terms of FEV1/FVC ratio and PaO2. The results show that RCI may have an association with pulmonary function. RCI has a positive correlation with COPD severity. In the univariate analyses (Table 2), the outcome variable was associated with diastolic blood pressure (DBP), lymphocytes, red blood cell, hemoglobin, RCI, length of stay, Require NIMV, pH, and PaCO2.
 |
Table 1 Baseline Characteristics of Participants |
 |
Table 2 The Results of Univariate Analysis |
Relationship Between RCI and Adverse Hospitalization Outcomes
We developed three models to control other potential confounding variables and assess the independent effects of RCI on adverse hospitalization outcomes (Table 3). We first treated RCI as a continuous variable. After adjusted sex, age, BMI, smoking status, comorbidities, therapy in stable stage, CRP, PCT, LDH, FEV1/FVC and PaCO2, each 1-unit increase in RCI was associated with a 15% (OR=1.15; 95% CI: 1.01–1.32) increased risk of adverse clinical outcomes. We also treated RCI as a categorical variable (lower and higher groups) for sensitivity analysis. In the crude model, compared to the lower RCI group reference, the OR for the higher RCI group (OR=1.85; 95% CI: 1.00–3.44) was significantly higher. After accounting for sex, age, BMI and smoking status in model 1, the RCI remained independently related to the poor hospitalization outcome, the higher RCI group (OR=1.90; 95% CI: 1.00–3.59). After further adjustment for comorbidities, therapy in stable stage, inflammatory parameters, FEV1/FVC and PaCO2, compared with the lower RCI group, the risk of poorer clinical outcome in the higher RCI group was increased by 77% (OR=1.77, 95% CI: 0.82–3.84), although this was not statistically significant.
 |
Table 3 Association Between RCI and Adverse Hospitalization Outcomes in AECOPD Patients |
Since 69 (377) patients were missing BMI and 127 (377) patients were missing CRP, we used multiple imputation for missing data. Five datasets were created and analyzed together (Tables S1–S5).
Non-Linearity of RCI and Adverse Hospitalization Outcomes
As RCI was a continuous variable, it was necessary to explore whether there was a non-linear relationship between RCI and adverse hospitalization outcomes (Table 4, Figure 2). The smooth curve showed a nonlinear relationship (adjusted for age, sex, BMI, smoking status, comorbidities CRP, PCT, LDH, FEV1/FVC and PaCO2) between the RCI and adverse hospitalization outcomes. We calculated the inflection point as 3.2 by using two-piecewise linear regression model. The effect size, 95% CI and P value for the right side of the inflection point (RCI ≥3.2) were of 1.3, 1.2 to 1.4 and P value of <0.001, respectively. However, the relationship could not be observed on the left side of the inflection point (RCI < 3.2) (OR = 0.8, 95% CI: 0.7–1.0, P = 0.058). This result suggested a threshold effect on the independent association between the RCI and adverse hospitalization outcomes.
 |
Table 4 The Results of Two-Piecewise Linear Regression Model |
 |
Figure 2 General additive model demonstrate the relationship between RCI and the risk of adverse hospitalization outcomes. A nonlinear relationship between the two was detected after adjusting for sex; age; BMI; smoking history; comorbidities (including diabetes, hypertension, arrhythmia, congestive heart failure, chronic kidney disease and coronary artery disease), therapy in stable stage, PCT, LDH, CRP, FEV1/FVC and PaCO2. The red line represents the best-fit line, and the blue lines are 95% confidence intervals. Abbreviations: RCI, red cell index; BMI, body mass index; PCT, procalcitonin; CRP, C-reactive protein; LDH, lactic dehydrogenase; FVC, forced vital capacity; FEV1, forced expiratory volume in 1s; PaCO2, partial pressure of carbon dioxide in arterial blood. |
Subgroup Analysis
We used stratification variables in the subgroup analysis, including sex, age, BMI, smoking history, diabetes, hypertension, arrhythmia, congestive heart failure, chronic kidney disease, coronary artery disease and PaCO2 (Table 5). In the stratified analysis, the association between the RCI and adverse hospitalization outcomes was similar for most strata (P > 0.05). A significant interaction was observed only for age (P = 0.0003). The RCI had a positive correlation with adverse hospitalization outcomes among patients younger than 75 (OR=1.60, 95% CI: 1.23–2.07).
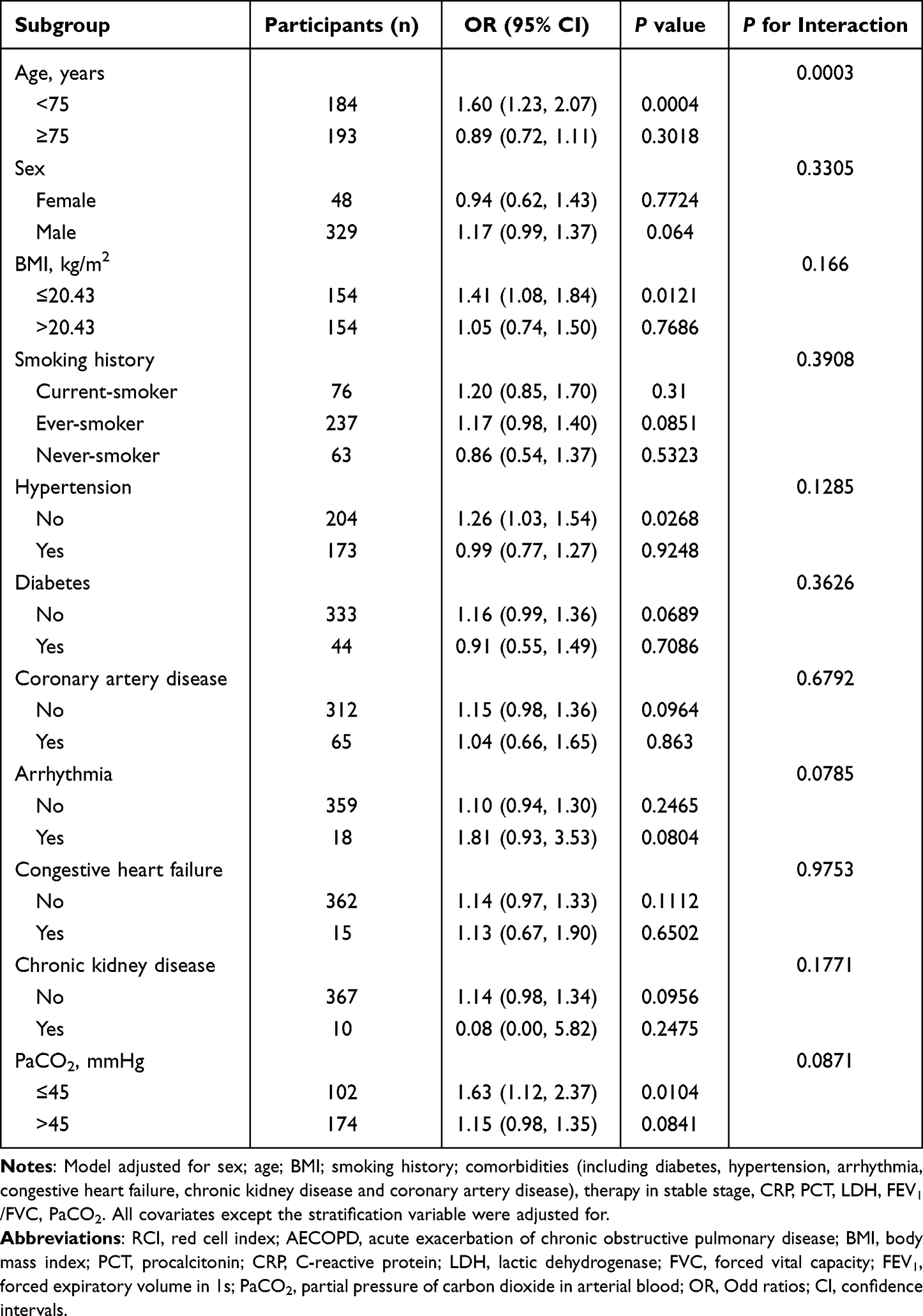 |
Table 5 Subgroup Analyses of the Association Between RCI and Adverse Hospitalization Outcomes in AECOPD Patients |
Discussion
Based on our population-based retrospective cohort study, we drew the following conclusions: (1) After adjusting for potential confounding variables, we found a positive correlation between RCI and adverse hospitalization outcomes among the AECOPD patients. (2) Our analysis results revealed non-linearity between RCI and adverse hospitalization outcomes. We found that the trend of the effect sizes on the left and right sides of the inflection point was inconsistent [right (OR=1.3, 95% CI: 1.2–1.4, P < 0.001); left (OR=0.8, 95% CI: 0.7–1.0, P=0.058)]. This result suggested a threshold effect on the independent association between RCI and incident of adverse hospitalization outcomes. Interestingly, we found that RCI had a positive correlation with adverse hospitalization outcomes among patients younger than 75.
Hemoglobin is a special protein in red blood cells that transports oxygen. In people with COPD, hemoglobin abnormalities, such as anemia and polycythemia, are common.21,22 Due to hypoxia’s promotion of erythropoiesis, COPD has long been associated with secondary polycythemia.10 There is evidence that polycythemia can lead to cor-pulmonale and pulmonary hypertension, which are associated with a poor prognosis.23 In the present study, we also observed higher erythrocyte and hemoglobin levels in the higher RCI group in patients with AECOPD. However, the anemia prevalence rate reported in recent study was shown to be more frequent in COPD patients occurring in 7.5–17% of patients.24 RBC count and hemoglobin level are known to reflect hypoxia susceptibility. A reduction in respiratory function suggested chronic hypoxic conditions, which in turn result in an increase in RBC count and hemoglobin concentration. It is unclear how lymphocytopenia affects chronic inflammatory diseases, but it is associated with a poor prognosis for acute inflammatory diseases.25 Additionally, lymphocytopenia has been linked to all-cause mortality among COPD patients.26,27 Similarly, Acanfora’s study also found an association between a low relatively lymphocyte count and high mortality among elderly patients with COPD.28 An immune response characteristic of lymphocytes is likely to explain lymphocyte influence on COPD. In our study, we also identified a lower lymphocyte count in the high RCI group than in the low RCI group in patients with AECOPD. Lymphocytes are responsible for this immunopathology, which is regulated by targeted immune responses in human lymphocytes. In addition, lymphocyte counts below 1500 is often a sign of malnutrition, Collins et al explained the correlation between malnutrition and COPD severity.29 Platelets modulate inflammatory response.25 While platelet counts in COPD patients have not been studied extensively, thrombocytopenia has been reported in AECOPD patients, and has been associated with poor outcomes and increased mortality.30 Consistent with these findings, we also found lower platelet counts in the higher RCI group than in the lower RCI group in patients with AECOPD. Since lymphocytes and platelets tend to be little affected by other factors, thus they are used as benchmarks for measuring the total permeability of a blood cell.
RCI is a new and composite index. An advantage of this index is that in the context of acute exacerbation of COPD, it acts as a comprehensive indicator, combining association of single hemoglobin, platelet, lymphocyte, and RBC. Recent studies have reported that RCI reflects respiratory function. Patients with higher RCI level are prone to have lower FEV1/FVC and higher PaCO2 values. In the present study, lower FEV1 (0.7±0.3 vs 0.8±0.3, p=0.028) were observed among AECOPD patients with higher RCI. This suggested that RCI was related to lung function to some extent. However, perhaps due to the limited sample size of this study, there was no significant difference between the two groups in terms of FEV1/FVC ratio and FEV1% predicted. Blood gas analysis can also be used to assess a patient’s respiratory function. However, arterial blood gas analysis is a technically complex process, and puncturing the arterial vessel may cause hematoma and other complications, which results in low patient compliance. Moreover, the analysis may require several attempts before success, making it a less than ideal method for clinical practice. Recently, a cohort study of 415 patients with AECOPD in Asia, Australia, and New Zealand found low compliance with blood gas testing, especially in Southeast Asia.31 In contrast, RCI, which is based on complete blood count parameters, is easier to obtain and use to evaluate respiratory function in patients with AECOPD.
In this study, we are the first to investigate the relationship between RCI and adverse hospitalization outcomes in patients with AECOPD. Previously, RCI was considered an efficient index for evaluating lung function based on the results of complete blood counts. As compared with the healthy control group, both the COPD and elderly groups showed significantly higher positive rates of abnormally elevated RCI.11 As shown in Table 1, the RCI was higher in people who had never smoked. However, as one possible explanation for this, we found that the non-smokers were older and more of them had hypertension, suggesting that these people may be in poor health and were thus not capable of smoking, thus their lung function was also poor and RCI was higher.
Subgroup analysis is a crucial aspect of a scientific study. We used sex, age, BMI, smoking history, hypertension, diabetes, arrhythmia, congestive heart failure, chronic kidney disease, coronary artery disease and PaCO2 as the stratification variables, of which only age had an interaction. Due to the lack of similar findings in previous studies, we were unable to explain why the linearly increasing correlation between RCI and adverse hospitalization outcomes occurred only among patients younger than 75. Future studies in other settings are needed to confirm this finding.
Our study has some strengths. (1) We used the generalized additive model (GAM) to clarify the nonlinear relationship between RCI and adverse hospitalization outcomes. There are obvious advantages to GAM in handling non-linear relationships, in handling smoothing factors, as well as fitting a regression curve. Therefore, we can use GAM to better understand the actual relationship between exposures and outcomes. (2) As an observational study, our results may be susceptible to potential confounders. In order to reduce residual confounding, we used strict statistical adjustment methods. (3) By handling the target independent variable as both a continuous and categorical variable, we were able to reduce the contingency and enhance the robustness of the results. (4) Using effect modifier factor analysis improves the use of data. In the subgroup analysis, a positive association was observed between RCI and adverse hospitalization outcomes in patients younger than 75. (5) We had the positive finding that when RCI was greater than 3.2, for every unit increase in RCI, the incidence of adverse hospital outcomes increased by 30%. The clinical significance of this observation is that the association between RCI and adverse hospital outcomes was only apparent when RCI reaches a certain threshold.
However, our study also has some limitations. First, our research had a small sample size. The data in Table 1 indicate that the majority of our study population is male, which may influence the observation of the relationship between RCI and adverse hospitalization outcomes in female AECOPD patients. Researchers have previously found that male and female patients have significant differences regarding disease severity, prognosis, and comorbidities.32,33 COPD has traditionally been seen as a disease of older men, but in recent years its prevalence among female patients has steadily increased. Future studies are needed to focus more on women with COPD. Second, we excluded patients with other respiratory diseases such as asthma, patients with sepsis shock, and patients with diseases of the blood system from analysis; therefore, these findings cannot be extrapolated to these people. Third, the BMI and CRP covariate data were respectively missing for 18.8% and 34% of the participants. However, we used MIs to address the problem of missing data, and the results were robust. Fourth, RCI is currently used only in Chinese patients with COPD. In order to investigate the mechanisms of RCI in the progression of COPD, we must conduct prospective cohort studies in different ethnic populations. Finally, this is a retrospective study with all the inherent limitations of retrospective studies. Further exploration and confirmation of our conclusions is necessary.
Conclusion
In conclusion, the present study showed a non-linear relationship between RCI and adverse hospitalization outcomes. The RCI was strongly positively related to adverse hospitalization outcomes when the RCI is greater than 3.2. Considering that this is a retrospective study, in the future we must conduct well-designed and large-scale longitudinal studies to confirm our results, and explore the predictive role of RCI in patients susceptible to unfavorable evolution.
Abbreviations
AECOPD, acute exacerbation of chronic obstructive pulmonary disease; COPD, chronic obstructive pulmonary disease; RCI, red cell index; Hb, hemoglobin; RBC, red blood cells; PLT, platelet; Lym, lymphocyte; BMI, body mass index; PCT, procalcitonin; CRP, C-reactive protein; LDH, lactic dehydrogenase; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; FEV1%Pred, forced expiratory volume in 1 second in percent of the predicted value; PaO2, partial pressure of oxygen in arterial blood; PaCO2, partial pressure of carbon dioxide in arterial blood; NIMV, noninvasive mechanical ventilation; ICU, intensive care unit; MIs, multiple imputations.
Data Sharing Statement
Due to patient privacy concerns, all data generated and analyzed during this study cannot be made publicly available, but they can be accessed by reasonable request from the author.
Ethics Approval and Informed Consent
The study was approved by the Ethics Review Committee of the First Affiliated Hospital of Sun Yat-sen University in April 2022 ([2022]-179). Because the present study was a retrospective design with anonymized data and patients’ privacy were not violated, the Investigational Ethical Review Board agreed exemption applications of informed consent.
Acknowledgments
The authors would like to thank all the study participants and the First Affiliated Hospital of Sun Yat-sen University for their contributions to the collection of data.
Author Contributions
Fu-zhen Yuan and Chang-ran Zhang: study conception, design, collection of data, analysis, interpretation of results, figure design, writing the article draft, reviewing the article, and editing. Wei Shui, Yan-li Xing, Yuan-yuan Niu, Xin Zhang: study design, collection of data, analysis, interpretation of results and article draft writing. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
Authors declare that they received no external funding for the study.
Disclosure
No competing interests are declared by the authors.
References
1. World Health Organization. World Health Organization (WHO) Website. Available from: https://www.who.int/zh/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
2. World Health Organization. World health statistics 2021: a visual summary. Available from: https://www.who.int/data/stories/world-health-statistics-2021-a-visual-summary.
3. Lopez AD, Shibuya K, Rao C, et al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006;27(2):397–412. doi:10.1183/09031936.06.00025805
4. Fitzmaurice C, Abate D, Abbasi N, Global Burden of Disease Cancer Collaboration. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: a systematic analysis for the global burden of disease study. JAMA Oncol. 2019;5(12):1749–1768. doi:10.1001/jamaoncol.2019.2996
5. Global Initiative for Chronic Obstructive Lung. Global strategy for diagnosis, management, and prevention of COPD; 2022. Available from: https://goldcopd.org/.
6. Nguyen PL, Uddin MM, Mir T, et al. Trends in incidence, and mortality of acute exacerbation of chronic obstructive pulmonary disease in the United States Emergency Department (2010–2018). COPD. 2021;18(5):567–575. doi:10.1080/15412555.2021.1979500
7. Hage JJ, Brinkman RJ. Andreas Vesalius’ understanding of pulmonary ventilation. Respir Physiol Neurobiol. 2016;231:37–44. doi:10.1016/j.resp.2016.05.015
8. Elojeimy S, Cruite I, Bowen S, Zeng J, Vesselle H. Overview of the novel and improved pulmonary ventilation-perfusion imaging applications in the Era of SPECT/CT. AJR Am J Roentgenol. 2016;207(6):1307–1315. doi:10.2214/AJR.15.15071
9. Baird G. Preanalytical considerations in blood gas analysis. Biochem Med (Zagreb). 2013;23(1):19–27. doi:10.11613/BM.2013.005
10. Xu L, Chen Y, Xie Z, et al. High hemoglobin is associated with increased in-hospital death in patients with chronic obstructive pulmonary disease and chronic kidney disease: a retrospective multicenter population-based study. BMC Pulm Med. 2019;19(1):174. doi:10.1186/s12890-019-0933-4
11. Guang Y, Jie Z, Feng D, Hui L. Surrogate scale for evaluating respiratory function based on complete blood count parameters. J Clin Lab Anal. 2018;32(5):e22385. doi:10.1002/jcla.22385
12. Gao S, Chen J, Xie J, Wang J. The effects of BAFF on T lymphocytes in chronic obstructive pulmonary disease. Respir Res. 2020;21(1):66. doi:10.1186/s12931-020-01333-z
13. Kornerup KN, Page CP. The role of platelets in the pathophysiology of asthma. Platelets. 2007;18(5):319–328. doi:10.1080/09537100701230436
14. Huang Y, Wang J, Shen J, et al. Relationship of red cell index with the severity of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2021;16:825–834. doi:10.2147/COPD.S292666
15. Rivas-Ruiz F, Redondo M, Gonzalez N, et al. Appropriateness of diagnostic effort in hospital emergency room attention for episodes of COPD exacerbation. J Eval Clin Pract. 2015;21(5):848–854. doi:10.1111/jep.12390
16. Lu FY, Chen R, Li N, et al. Neutrophil-to-lymphocyte ratio predicts clinical outcome of severe acute exacerbation of COPD in frequent exacerbators. Int J Chron Obstruct Pulmon Dis. 2021;16:341–349. doi:10.2147/COPD.S290422
17. Romskaug R, Skovlund E, Straand J, et al. Effect of clinical geriatric assessments and collaborative medication reviews by geriatrician and family physician for improving health-related quality of life in home-dwelling older patients receiving polypharmacy: a cluster randomized clinical trial. JAMA Intern Med. 2020;180(2):181–189. doi:10.1001/jamainternmed.2019.5096
18. White IR, Royston P, Wood AM. Multiple imputation using chained equations: issues and guidance for practice. Stat Med. 2011;30(4):377–399. doi:10.1002/sim.4067
19. Austin PC, White IR, Lee DS, van Buuren S. Missing data in clinical research: a tutorial on multiple imputation. Can J Cardiol. 2021;37(9):1322–1331. doi:10.1016/j.cjca.2020.11.010
20. Beesley LJ, Bondarenko I, Elliot MR, Kurian AW, Katz SJ, Taylor JM. Multiple imputation with missing data indicators. Stat Methods Med Res. 2021;30(12):2685–2700. doi:10.1177/09622802211047346
21. Cote C, Zilberberg MD, Mody SH, Dordelly LJ, Celli B. Haemoglobin level and its clinical impact in a cohort of patients with COPD. Eur Respir J. 2007;29(5):923–929. doi:10.1183/09031936.00137106
22. Vasquez A, Logomarsino JV. Anemia in chronic obstructive pulmonary disease and the potential role of iron deficiency. COPD. 2016;13(1):100–109. doi:10.3109/15412555.2015.1043519
23. Vlahakos V, Marathias K, Lionaki S, Loukides S, Zakynthinos S, Vlahakos D. The paradigm shift from polycythemia to anemia in COPD: the critical role of the renin-angiotensin system inhibitors. Expert Rev Respir Med. 2022;16(4):391–398. doi:10.1080/17476348.2022.2045958
24. Trudzinski FC, Jorres RA, Alter P, et al. Associations of oxygenated hemoglobin with disease burden and prognosis in stable COPD: results from COSYCONET. Sci Rep. 2020;10(1):10544. doi:10.1038/s41598-020-67197-x
25. Sahin F, Kosar AF, Aslan AF, Yigitbas B, Uslu B. Serum biomarkers in patients with stable and acute exacerbation of chronic obstructive pulmonary disease: a comparative study. J Med Biochem. 2019;38(4):503–511. doi:10.2478/jomb-2018-0050
26. Cao Y, Xing Z, Long H, et al. Predictors of mortality in COPD exacerbation cases presenting to the respiratory intensive care unit. Respir Res. 2021;22(1):77. doi:10.1186/s12931-021-01657-4
27. Liu J, Liu J, Zou Y. Relationship between neutrophil-lymphocyte ratio and short-term prognosis in the chronic obstructive pulmonary patients with acute exacerbation. Biosci Rep. 2019;39:5. doi:10.1042/BSR20190675
28. Acanfora D, Scicchitano P, Carone M, et al. Relative lymphocyte count as an indicator of 3-year mortality in elderly people with severe COPD. BMC Pulm Med. 2018;18(1):116. doi:10.1186/s12890-018-0685-6
29. Collins PF, Stratton RJ, Elia M. Nutritional support in chronic obstructive pulmonary disease: a systematic review and meta-analysis. Am J Clin Nutr. 2012;95(6):1385–1395. doi:10.3945/ajcn.111.023499
30. Rahimi-Rad MH, Soltani S, Rabieepour M, Rahimirad S. Thrombocytopenia as a marker of outcome in patients with acute exacerbation of chronic obstructive pulmonary disease. Pneumonol Alergol Pol. 2015;83(5):348–351. doi:10.5603/PiAP.2015.0056
31. Kelly AM, Holdgate A, Keijzers G, et al. Epidemiology, treatment, disposition and outcome of patients with acute exacerbation of COPD presenting to emergency departments in Australia and South East Asia: an AANZDEM study. Respirology. 2018;23(7):681–686. doi:10.1111/resp.13259
32. Grabicki M, Kuznar-Kaminska B, Rubinsztajn R, et al. COPD course and comorbidities: are there gender differences? Adv Exp Med Biol. 2019;1113:43–51. doi:10.1007/5584_2018_160
33. Souto-Miranda S, van ‘t Hul AJ, Vaes AW. Differences in pulmonary and extra-pulmonary traits between women and men with chronic obstructive pulmonary disease. J Clin Med. 2022;11:13. doi:10.3390/jcm11133680
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Relationship Between Prognostic Nutritional Indexes and the Clinical Outcomes of Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Yuan FZ, Xing YL, Xie LJ, Yang DL, Shui W, Niu YY, Zhang X, Zhang CR
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1155-1167
Published Date: 12 June 2023