Back to Journals » International Journal of General Medicine » Volume 14
Association of Normal-Range Hemoglobin A1c Value During Midpregnancy with Adverse Birth Outcomes
Authors Zhang L, Zhai R, Huo Z, Wei Z, Zhang Z, Wei R, Man D
Received 1 April 2021
Accepted for publication 10 June 2021
Published 30 June 2021 Volume 2021:14 Pages 3049—3057
DOI https://doi.org/10.2147/IJGM.S313952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lihua Zhang,1,2 Ruixia Zhai,1 Zhiyu Huo,1 Zhenyan Wei,1 Ziheng Zhang,2 Ruirui Wei,1 Dongmei Man1,2
1Department of Obstetrics, Affiliated Hospital of Jining Medical University, Jining, Shandong, People’s Republic of China; 2College of Clinical Medicine, Jining Medical University, Jining, Shandong, People’s Republic of China
Correspondence: Dongmei Man Email [email protected]
Background: The midpregnancy normal-range HbA1c value and adverse birth outcomes were controversial. To address this lack of data, we examined the associations between midpregnancy normal-range HbA1c value and adverse birth outcomes.
Objective: To evaluate whether an association exists between the midpregnancy normal-range HbA1c value and adverse birth outcomes.
Materials and Methods: A total of 8389 women in their midpregnancy with normal gestational HbA1c value from the Affiliated Hospital of Jining Medical University in China participated in this study from January to December 2019. Subjects were stratified on the basis of their midpregnancy HbA1c value, and multivariate logistic regression was implemented to investigate the association between different HbA1c values and adverse birth outcomes.
Results: Incidence of preterm birth, macrosomia, and large for gestational age (LGA) for 8389 subjects were 4.8%, 6.3% and 16.5%, respectively. The multivariate logistic regression model demonstrated that the risk of preterm birth (adjusted odds ratio [OR]: 1.71 and 95% confidence interval [CI]: 1.25– 2.34), macrosomia (OR: 1.68 and 95% CI: 1.26– 2.22), and LGA (OR: 1.53 and 95% CI: 1.28– 1.83) increase for every increase of 1% maternal HbA1c. Women with a prepregnancy body mass index (BMI) of < 25 kg/m2 have a stronger correlation with HbA1c values and adverse birth outcomes than women with a prepregnancy BMI of ≥ 25 kg/m2.
Conclusion: Our results indicated that the midpregnancy normal-range HbA1c level within the normal range is associated with adverse birth outcomes. Monitoring and controlling HbA1c may reduce the risk of adverse birth outcomes.
Keywords: hemoglobin A1c, pregnant women, normal-range, midpregnancy, adverse birth outcomes
Introduction
Adverse birth outcomes, including preterm birth, macrosomia, and large for gestational age (LGA), are critical health problems. Fifteen million babies are born with poor birth outcomes annually worldwide. More than a million people die immediately after birth.1–3 These adverse birth outcomes may seriously affect the physical and mental health of pregnant women and neonates, threaten their quality of life, and bring heavy economic burden to the family and society.4,5 Clinical studies have shown that blood glucose values lower than diagnosed diabetes patients are related to adverse pregnancy outcomes.6–8
Hemoglobin A1c (HbA1c) is a substance formed by the reaction between the amino (N) terminal of hemoglobin and hexose that offers an integrated summary of circadian blood glucose value during the preceding two to three months. The consensus panel of International Association of Diabetes and Pregnancy Study Groups recommended that HbA1c ≥ 6.5% may be used for the diagnosis of gestational diabetes mellitus (GDM), with HbA1c ≥ 6.0% indicating a high risk of GDM.9,10
Meanwhile, relatively high but normal HbA1c values may be a potential risk factor for other nondiabetic conditions, such as cancers and brain, kidney, and coronary heart diseases.11–13 Studies have shown that differences in adverse pregnancy outcomes with HbA1c within the normal range are limited and results are inconsistent. A multicenter retrospective study conducted in Guangdong Province in China showed that normal elevated HbA1c values were an independent risk factor for preterm birth, macrosomia, and LGA.14 A previous study showed that a significant correlation existed between HbA1c in the normal range and the risk of macrosomia but was absent with preterm birth and LGA.15 A study conducted at Kaiser Permanente Washington Hospital in 2019 showed that HbA1c within the normal range was not associated with adverse birth outcomes (premature infants, macrosomia, and LGA).16 The value of HbA1c showed a biphasic change during pregnancy, wherein the value was higher in the first and third trimesters but lower during midpregnancy.17 Therefore, our study aims to assess whether the increase in the normal range of HbA1c values of women during midpregnancy is related to the increased risk of adverse birth outcomes.
Materials and Methods
Study Participants
The analysed data were extracted from the medical record information system of the Affiliated Hospital of Jining Medical University in Shandong Province, China. Data on 16,703 pregnant women who gave live birth in our hospital from January to December 2019 were successively collected. We included the following maternal information in this study: HbA1c values during midpregnancy, maternal age, prepregnancy body mass index (BMI), gestational week of delivery, and cesarean section. Neonatal information includes newborn’s gender, birth weight, preterm birth, macrosomia, and LGA. Midwives with experience in the obstetrics department of our hospital were chosen for data entry. All staff members involved in the study were uniformly trained, acquired data were checked, medical records of missing items were retrieved, and medical records for logically incorrect data were recalled for error correction before data entry. Values were retaken from medical records for verification, and 10% of data were randomly selected for verification. This was a retrospective study. The data were anonymous, and the requirement for patient informed consent was therefore waived. Patient data confidentiality was kept and was in compliance with the Declaration of Helsinki. This study was approved by the human ethics committee of the Affiliated Hospital of Jining Medical University (2020C042).
HbA1c Measurement
Blood is drawn in the morning after a fasting period of at least 8 hours. The HbA1c value in the blood is measured using an ARKRAY HA-8180 automatic glycosylated hemoglobin analyzer (HA-8180) with the principle of ion-exchange high-performance liquid chromatography.
Exclusion Criteria
Pregnant women below 18 years old, gestational weeks ≥42 weeks, unspecified gestational weeks, birth weight ≥5000 g, twin and triplet pregnancies, presence of fetal birth defects, gestational diabetes mellitus, prepregnancy diabetes mellitus and patients without data on HbA1c during midpregnancy were excluded from this study. A total of 8389 pregnant women were included in this study (Figure 1).
 |
Figure 1 Flowchart of study population. |
Definition of Variables and Results
- Gestational weeks are determined on the basis of the last menstrual period (LMP) if the first or second-trimester ultrasound agrees with the estimated due date (EDD) within 7 or 14 days, respectively. If the due date differs by more than 7 or 14 days in the first or second trimester, respectively, or if LMP is unknown, then EDD is changed to the date calculated by the earliest available ultrasound.18
- Midpregnancy is within the 14th to 27+6th week of gestation.
- Macrosomia is defined as an estimated fetal weight of more than 4000 g.19
- LGA is determined according to the birth weight with the same gestational age average weight above the 90th percentile.20
- Preterm birth occurs within a gestational age of 28 weeks but less than 37 weeks.21
Statistical Analysis
Mean and standard deviation were used as continuous variables, while number and percentage were utilized as categorical variables. The analysis of variance and chi-square test were applied to determine statistical differences between mean and proportion within the group, respectively. A total of 8389 subjects were grouped into four categories according to the quartile of HbA1c (Q1 – Q4): Q1: ≤4.7% (28 mmol/mol), Q2: 4.8–4.9% (29–30 mmol/mol), Q3: 5.0–5.1% (31–32 mmol/mol), and Q4: 5.2–6.3% (33–46 mmol/mol). Furthermore, the following logistic models were listed: Model I includes two variables (maternal age and prepregnancy BMI) and Model II includes five variables (maternal age, prepregnancy BMI, gestational age at delivery, caesarean section, and sex).
Subgroup analysis was performed using a stratified linear regression model according to prepregnancy BMI (<25 or ≥25 kg/m2) (Figure 2). In addition, HbA1c values ranged from 5.7% to 6.4%, which was defined by the American Diabetes Association as prediabetes because it can identify individuals with high risk of diabetes in the future. We performed a sensitivity analysis to exclude this subset of pregnant women and assess the stability of the results.
 |
Figure 2 Associations between HbA1c level and adverse birth outcomes, stratified by maternal prepregnancy BMI (kg/m2). Abbreviations: OR, odds ratio; LGA, large for gestational age. |
All analyses were performed with the statistical software packages R (http://www.R-project.org, The R Foundation) and Empower Stats (http://www.empowerstats.com; X & Y Solutions, Inc.; Boston, MA, USA). P values < 0.005 (two-sided) were considered statistically significant.
Results
Baseline Characteristics of Selected Participants
A total of 8389 participants were selected for the final data analysis (Figure 1). Characteristics of mothers and newborns are summarized in Table 1. The mean maternal age (mean ± SD) was 29.35 ± 4.66 years; prepregnancy BMI was 22.34 ± 3.48 kg/m2; When HbA1c was measured at (mean ± SD) was 25.31±1.14, median of 25.29 weeks’ gestation, the min-max (14.14–27.99); gestational week of delivery was 39.08 ± 1.37 weeks; incidence of cesarean section was 57.24% (4802/8398), and incidence of boys was 53.83% (4516/8398). The incidence of preterm birth, macrosomia, and LGA were 4.8%, 6.3%, and 16.5%, respectively.
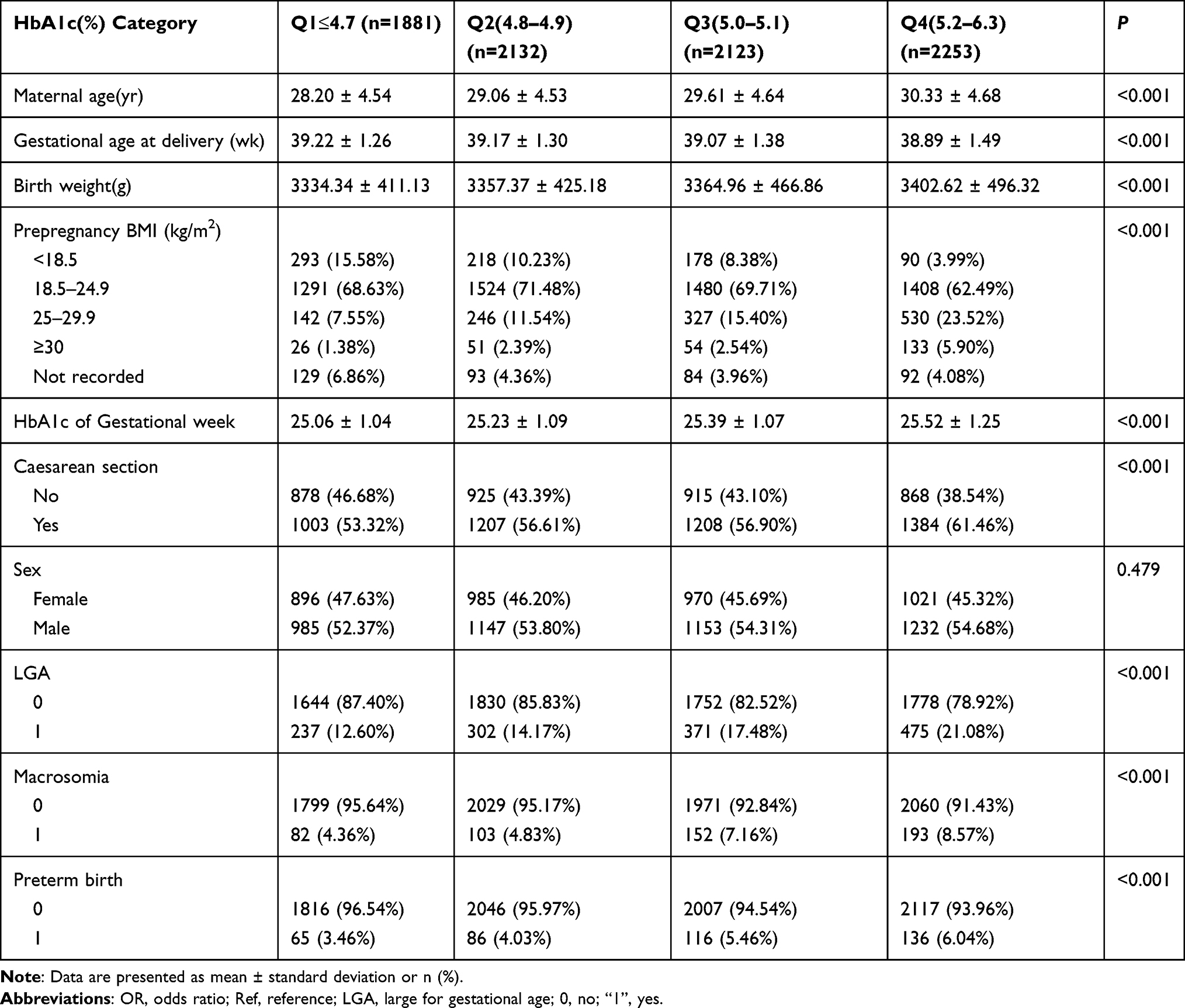 |
Table 1 Characteristics of the Study Population Based on HbA1c (%) (n=8389) |
Univariate Analysis
The results of univariate analyses are listed in Table 2. The results of univariate binary logistic regression showed that HbA1c (%), maternal age, prepregnancy BMI, gestational age at delivery, birth weight, caesarean section, and sex were positively associated with adverse birth outcomes. Participants (8389 pregnant women) were divided into four groups according to the quartile of HbA1c (Q1–Q4). The incidence of preterm birth, macrosomia, and LGA increased significantly with the increase of HbA1c.
 |
Table 2 Univariate Analysis of Adverse Birth Outcomes |
Results of Logistic Regression Analyses
Table 3 shows the associations of the HbA1c value during midpregnancy with adverse birth outcomes. Two adjustment models were constructed to analyze the independent effect of HbA1c on adverse birth outcomes (multivariate binary logistic regression analysis), including effect size (adjusted OR) and 95% CI. The results of the adjustment model I (adjusted according to maternal age and prepregnancy BMI) showed that HbA1c is significantlyand positively correlated with increased risk of preterm birth (adjusted OR: 2.39 and 95% CI: 1.67–3.44), macrosomia (adjusted OR: 1.91 and 95% CI: 1.39–2.63), and LGA (adjusted OR: 1.64 and 95% CI: 1.33–2.02). The results of the adjustment model II (gestational age, cesarean section and neonatal gender were added on the basis of adjusting model I, but the preterm birth model did not include gestational age) demonstrated that HbA1c remains significantly and positively correlated with the increased risk of preterm birth (OR: 2.37 and 95% CI: 1.65–3.41), macrosomia (OR: 2.25 and 95% CI: 1.61–3.13), and LGA (OR: 1.82 and 95% CI: 1.47–2.25).
 |
Table 3 Relationship Between HbA1c and Adverse Birth Outcomes in Different Models |
The relationship between HbA1c and adverse birth outcomes was similar between women with prepregnancy BMIs of ≥25 and <25 kg/m2 but more significant in pregnant women with prepregnancy BMI < 25 kg/m2 (Figure 2).
HbA1c was converted from a continuous variable to a categorical variable (quartiles of HbA1c) for the sensitivity analysis. The P value for the trend of HbA1c with categorical variables in the fully adjusted model was consistent with the result when HbA1c was a continuous variable. Additionally, the trend of the effect size in different HbA1c groups was nonequidistant. The positive correlation between HbA1c during pregnancy and adverse birth outcomes after excluding prediabetic pregnant women demonstrated no significant change (HbA1c value was 5.7–6.4%) (Schedule 1)
Discussion
This study primarily aimed to investigate the relationship between HbA1c and adverse birth outcomes during midpregnancy. We found that elevated HbA1c values during midpregnancy are associated with increased risk of preterm birth, macrosomia, and LGA. HbA1c and adverse birth outcomes were significant in women with a prepregnancy BMI of <25 kg/m2.
HbA1c can be used as a clinical test index, an independent GDM predictor, and in association with other standard diagnostic tests for GDM diagnosis.22–24 Many recent reports on the relationship between HbA1c and adverse pregnancy outcomes in women with GDM confirmed that a correlation exists between the HbA1c value and adverse pregnancy outcomes.10,25,26
Ho et al enrolled 1989 pregnant Taiwanese women,25 the results showed that the midpregnancy HbA1c value was significantly associated with increased risks of preterm delivery and macrosomia (the odds ratio [OR] ranges were 1.31–5.16 and 2.22–27.86). In a study by Iwama and colleagues,27 the adjusted odds ratios per 1% (11 mmol/mol) increase in HbA1c level were 1.30 (95% CI: 1.12–1.50) for preterm birth, 1.95 (95% CI: 1.42–2.70) for macrosomia, 1.15 (95% CI: 1.04–1.28) for LGA. A longitudinal study conducted in New Zealand showed that high HbA1c level below the diagnostic criteria of GDM in pregnant women were associated with preterm birth and LGA, but not with macrosomia17 Hence, the influence of HbA1c values of pregnant non-GDM women on adverse birth outcomes remains unclear. Differences between the results of previous studies and our findings may be due to the following reasons. First, monitoring of HbA1c at different gestational periods (early and midterm) showed that significant differences exist in HbA1c values among the three gestational periods. Second, subjects belonged to different ethnic groups. Finally, differences in HbA1c estimation and standardized methods may affect their results.
The subclinical grouping showed that women with BMI < 25 kg/m2 showed a more significant relationship with preterm birth, macrosomia, and LGA than women with BMI ≥ 25 kg/m2. The relationship between HbA1c and adverse birth outcomes was similar between women with prepregnancy BMI of ≥25 and <25 kg/m2 but more significant in pregnant women with prepregnancy BMI < 25 kg/m2. Among them, the OR of preterm birth (2.39 and 95% CI: 1.67–3.44) in BMI ≥ 25 kg/m2, which is consistent with the results of Bi, et al [1]. The macrosomia (OR: 2.37 and 95% CI: 1.59–3.55) and LGA (OR: 2.05 and 95% CI: 1.60–2.64) results are inconsistent, which may be related to their small sample size.
Some research results show that28,29 pregnant women who are underweight before pregnancy will significantly increase the risk of preterm birth, and obesity will slightly increase the risk of preterm birth. A large cohort study of 536,098 Chinese pregnant women in rural China showed that the prevalence of underweight individuals significantly increased and both extremely high and low maternal prepregnancy BMI values have a significant association with adverse pregnancy outcomes.30 This is also consistent with the results of our study. Pre-pregnancy BMI <25 kg/m2 and the higher incidence of preterm birth may be due to the poor nutritional status of pregnant and lying-in women. Women lacking certain nutrients were susceptible to chronic infection and inflammation, which led to an increased risk of PTB. The mechanism by which macrosomia and LGA were more likely to occur with BMI less than 25 kg/m2 before pregnancy was still unclear, and further research was needed to clarify the mechanism in future work.
The following are the limitations of this study. First, this study is a single-center retrospective investigation because only Chinese subjects were included; therefore, universality and extrapolation of findings are impossible. Second, relative data may be inaccurate because some birth weights were only accurate for percentiles rather than individuals. Third, HbA1c values were collected at different times; hence, the comparison of the association between HbA1c and adverse birth outcomes through a control cohort is infeasible. Fourth, the populations we currently include were all tested for HbA1c in the second trimester, and cannot be extrapolated to those who have not tested HbA1c.
Conclusion
Elevated normal-range HbA1c values during midpregnancy are positively correlated with the risk of adverse birth outcomes even within the normal range. Elevated HbA1c values may increase the risk of adverse birth outcomes.
Acknowledgments
The authors thank all the staff members of the Affiliated Hospital of Jining Medical University in China.
Funding
This study was supported by the Research Fund for Academician Lin He New Medicine in China (Grant no. JYHL2019FMS14) and Scientific Research Foundation of Doctor in Jining Medical University.
Disclosure
The authors declare no conflicts of interest.
References
1. Tsegaye B, Kassa A. Prevalence of adverse birth outcome and associated factors among women who delivered in Hawassa town governmental health institutions, south Ethiopia, in 2017. Reprod Health. 2018;15(1):193. doi:10.1186/s12978-018-0631-3
2. Howson CP, Kinney MV, Mc Dougall L, et al.; Born Too Soon Preterm Birth Action Group. Born too soon: preterm birth matters. Reprod Health. 2013;10:S1.
3. Rubens CE, Gravett MG, Victora CG, et al. Global report on preterm birth and stillbirth (7 of 7): mobilizing resources to accelerate innovative solutions (global action agenda). BMC Pregnancy Childbirth. 2010;10(S1):S1–7. doi:10.1186/1471-2393-10-S1-S7
4. Crowther CA, Hiller JE, Moss JR, et al. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N Engl J Med. 2005;352(24):2477–2486. doi:10.1056/NEJMoa042973
5. Yu H, Wang J, Shrestha Y, et al. Importance of early elevated maternal HbA1c levels in identifying adverse fetal and neonatal events. Placenta. 2019;86:28–34. doi:10.1016/j.placenta.2019.07.008
6. Metzger BE, Lowe LP, Sacks DA, et al.; HAPO Study Cooperative Research Group. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008;358:1991–2002.
7. Cho HY, Jung I, Kim SJ. The association between maternal hyperglycemia and perinatal outcomes in gestational diabetes mellitus patients: a Retrospective Cohort Study. Medicine (Baltimore). 2016;95(36):e4712. doi:10.1056/NEJMoa0707943
8. Shobha P, Mathen S, Abraham J. Glycosylated hemoglobin values in nondiabetic pregnant women in the third trimester and adverse fetal outcomes: an Observational Study. J Fam Med Prim Care. 2016;5(3):646–651. doi:10.4103/2249-4863.197313
9. International Expert Committee. International expert committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care. 2009;32(7):1327–1334. doi:10.2337/dc09-9033
10. Metzger BE, Gabbe SG, Persson B, et al.; International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(7):676–682. doi:10.2337/dc09-1848
11. Joshu CE, Prizment AE, Dluzniewski PJ, et al. Glycated hemoglobin and cancer incidence and mortality in the Atherosclerosis in Communities (ARIC) Study, 1990–2006. Int J Cancer. 2012;131(7):1667–1677. doi:10.1002/ijc.27394
12. Li H, Cui Y, Zhu Y, et al. Association of high normal HbA1c and TSH levels with the risk of CHD: a 10-Year Cohort Study and SVM analysis. Sci Rep. 2017;7(1):45406. doi:10.1038/srep45406
13. Ferroni P, Formica V, Della-Morte D, et al. Prognostic value of glycated hemoglobin in colorectal cancer. World J Gastroenterol. 2016;22(45):9984–9993. doi:10.3748/wjg.v22.i45.9984
14. Bi J, Ji C, Wu Y, et al. Association between maternal normal range HbA1c values and adverse birth outcomes. J Clin Endocrinol Metab. 2020;105(6):105. doi:10.1210/clinem/dgaa127
15. Mañé L, Flores-le Roux JA, Benaiges D, et al. Role of first-trimester HbA1c as a predictor of adverse obstetric outcomes in a multiethnic cohort. J Clin Endocrinol Metab. 2017;102(2):390–397. doi:10.1055/s-0038-1675619
16. Chen L, Pocobelli G, Yu O, et al. Early pregnancy hemoglobin A1C and pregnancy outcomes: a Population-Based Study. Am J Perinatol. 2019;36(10):1045–1053. doi:10.1055/s-0038-1675619
17. Hughes RC, Rowan J, Florkowski CM. Is there a role for HbA1c in pregnancy? Curr Diab Rep. 2016;16(1):5. doi:10.1007/s11892-015-0698-y
18. Dall’Asta A, Lees C. Early second-trimester fetal growth restriction and adverse perinatal outcomes. Obstet Gynecol. 2018;131(4):739–740. doi:10.1097/AOG.0000000000002548
19. Araujo Júnior E, Peixoto AB, Zamarian AC, et al. Macrosomia. Best Pract Res Clin Obstet Gynaecol. 2017;38:83–96. doi:10.1016/j.bpobgyn.2016.08.003.
20. Dai L, Deng C, Li Y, et al. Birth weight reference percentiles for Chinese. PLoS One. 2014;9(8):e104779. doi:10.1371/journal.pone.0104779
21. Gupta PC, Subramoney S. Smokeless tobacco use, birth weight, and gestational age: Population Based, Prospective Cohort Study of 1217 women in Mumbai, India. BMJ. 2004;328(7455):1538. doi:10.1136/bmj.38113.687882.EB
22. Punnose J, Malhotra RK, Sukhija K, et al. Glycated haemoglobin in the first trimester: a predictor of gestational diabetes mellitus in pregnant Asian Indian women. Diabetes Res Clin Pract. 2020;159:107953. doi:10.1016/j.diabres.2019.107953
23. Renz PB, Chume FC, Timm JRT, et al. Diagnostic accuracy of glycated hemoglobin for gestational diabetes mellitus: a systematic review and meta-analysis. Clin Chem Lab Med. 2019;57(10):1435–1449. doi:10.1515/cclm-2018-1191
24. Mousavi SN, Kamali K, Mirbazel M, et al. The best cut-off value for HbA1c as a screening tool in Iranian women with gestational diabetes mellitus. J Fam Reprod Health. 2017;11(1):37–42. PMID: 29114267; PMCID: PMC5664988.
25. Ho YR, Wang P, Lu MC, et al. Associations of mid-pregnancy HbA1c with gestational diabetes and risk of adverse pregnancy outcomes in high-risk Taiwanese women. PLoS One. 2017;12(5):0177563. doi:10.1371/journal.pone.0177563
26. Ye M, Liu Y, Cao X, et al. The utility of HbA1c for screening gestational diabetes mellitus and its relationship with adverse pregnancy outcomes. Diabetes Res Clin Pract. 2016;114:43–49. doi:10.1016/j.diabres.2016.02.007
27. Iwama N, Sugiyama T, Metoki H, et al.; Japan Environment and Children’s Study Group. Associations between glycosylated hemoglobin level at less than 24 weeks of gestation and adverse pregnancy outcomes in Japan: the Japan Environment and Children’s Study (JECS). Diabetes Res Clin Pract. 2020;169:108377. doi:10.1016/j.diabres.2020.108377
28. Enomoto K, Aoki S, Toma R, et al. Pregnancy outcomes based on pre-pregnancy body mass index in Japanese women. PLoS One. 2016;11(6):0157081. doi:10.1371/journal.pone.0157081
29. Khatibi A, Brantsaeter AL, Sengpiel V, et al. Prepregnancy maternal body mass index and preterm delivery. Am J Obstet Gynecol. 2012;207(3):
30. Pan Y, Zhang S, Wang Q, et al. Investigating the association between prepregnancy body mass index and adverse pregnancy outcomes: a Large Cohort Study of 536098 Chinese pregnant women in rural China. BMJ Open. 2016;6(7):011227. doi:10.1136/bmjopen-2016-011227
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.