")
Back to Journals » Journal of Inflammation Research » Volume 16
Association of Neutrophil to High-Density Lipoprotein Cholesterol Ratio with Cardiac Ultrasound Parameters and Cardiovascular Risk: A Cross-Sectional Study Based on Healthy Populations
Authors Pan X, Zhang X, Ban J, Yue L, Ren L, Chen S
Received 27 January 2023
Accepted for publication 21 April 2023
Published 27 April 2023 Volume 2023:16 Pages 1853—1865
DOI https://doi.org/10.2147/JIR.S406102
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam D Bachstetter
Xiaoyu Pan,1,2 Xueqing Zhang,2 Jiangli Ban,2 Lin Yue,3 Lin Ren,2 Shuchun Chen1,2
1Department of Internal Medicine, Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 2Department of Endocrinology, Hebei General Hospital, Shijiazhuang, Hebei, People’s Republic of China; 3Department of Endocrinology, the Third Hospital of Shijiazhuang, Shijiazhuang, Hebei, People’s Republic of China
Correspondence: Shuchun Chen, Department of Internal Medicine, Hebei Medical University, People’s Republic of China, Tel +86 31185988406, Email [email protected]
Background: Neutrophils and high-density lipoprotein cholesterol (HDL-C) are significantly linked to cardiovascular disease (CVD). This study investigates the correlation of neutrophil count to HDL-C ratio (NHR) with cardiac ultrasound parameters and cardiovascular risk in healthy populations.
Materials and Methods: Firstly, NHR was calculated based on neutrophils and HDL-C. Then, the differences in basic clinical characteristics and cardiac ultrasound parameters were compared between the high and low NHR groups, males and females. Subsequently, cardiovascular risk was predicted according to the Chinese 10-year ischemic cardiovascular disease (ICVD) risk assessment tool for people aged 35– 60 years. Finally, the correlation between NHR and cardiac ultrasound parameters and cardiovascular risk was calculated.
Results: A total of 3020 healthy participants, 1879 males and 1141 females, were included. Participants in the high NHR group had significantly increased Aorta (AO), Left Atrium (LA), Right Atrium (RA), Right Ventricle (RV), End Systolic Diameter of Left Ventricle (ESD), End Diastolic Diameter of Left Ventricle (EDD), Main Pulmonary Artery (MPA), Right Ventricular Outflow Tract (RVOT), Interventricular Septum (IVS), Left Ventricular Posterior Wall (LVPW), and cardiovascular risk and decreased E/A values compared to those in the low NHR group. The same results were found in males participants compared to females. A total of 1670 participants underwent ICVD risk assessment tool. Cardiovascular risk was significantly higher in those with high NHR and in males than in those with low NHR and in females. Correlation analysis showed that NHR was positively correlated with AO, LA, RA, RV, ESD, EDD, MPA, RVOT, IVS, LVPW and cardiovascular risk, and negatively correlated with E/A values.
Conclusion: Our study demonstrates that NHR is significantly associated with cardiac ultrasound parameters and cardiovascular risk in healthy populations. NHR may serve as a useful indicator for the early diagnosis and treatment of cardiovascular disease among healthy populations.
Keywords: neutrophils, high-density lipoprotein cholesterol ratio, cardiovascular risk, cardiac ultrasound, cardiovascular disease
Introduction
The largest cause of morbidity and mortality in the world is cardiovascular disease (CVD), which places a significant burden on the healthcare system.1 Atherosclerosis, which is the primary cause of CVD, is influenced by lipids and inflammation.2,3 A lipoprotein called low-density lipoprotein (LDL), which transports cholesterol into peripheral tissue cells, can oxidize to form oxidized LDL, which, when present in excess, increases the risk of atherosclerosis.4 High-density lipoprotein HDL-cholesterol (HDL-C), on the other hand, acts as a preventative measure against atherosclerosis by moving cholesterol from bodily tissues to the liver, lowering the level of free cholesterol in plasma HDL, and minimizing the deposition of cholesterol in tissues.5
Acute cardiovascular events are brought on by the rupture or erosion of unstable atheromatous plaques in the coronary arteries, which causes acute myocardial ischemia or necrosis due to total or incomplete blockage of the coronary lumen and causes a considerable rise in mortality. Neutrophils play a significant part in this process by attracting pro-inflammatory cells and releasing cytokines.6,7 Increased peripheral blood neutrophil levels are linked to both unfavorable cardiovascular outcomes and atherosclerosis. Additionally, by preventing the production of neutrophil inflammatory factors, HDL-C may provide additional protection against acute cardiovascular events.8 As a result, both low HDL-C and increased neutrophils are harmful CVD risk factors. The neutrophil counts to HDL-C ratio (NHR) is a brand-new measure for lipid metabolism and inflammation. NHR is linked to poor cardiovascular outcomes and cardiovascular mortality after coronary surgery, according to recent research.9,10 However, no studies have examined the relationship between NHR and cardiovascular risk or events in individuals without a history of CVD. One of the popular techniques for determining cardiovascular risk is the Chinese 10-year ischemic cardiovascular disease (ICVD) risk assessment tool, which evaluates a patient’s likelihood of experiencing their first fatal cardiovascular event within the next 10 years based on six variables: age, body mass index (BMI), smoking, blood glucose, systolic blood pressure, and total cholesterol level. The relationship between NHR and the ICVD risk has not yet been studied and reported.11,12 Previous studies have shown that some novel biomarkers for predicting cardiovascular events, such as high-sensitivity C-reactive protein, fibrinogen, lipoprotein-associated phospholipase A2, matrix metalloproteinases, myeloperoxidase, and endothelin-1, are not yet widely used in clinical practice due to the complexity of the tests.13 NHR is more readily available than these indicators and better reflects the inflammatory status of the body, so it can be widely application.
The only device that can repeatedly show the structures inside the heart chambers, the heart’s pulse, and the flow of blood while causing no harm to the body is cardiac ultrasonography. Myocardial thickness and chamber volume can be directly measured, and myocardial mobility and heart function can be seen. Because cardiovascular disease is a chronic, progressive condition, there may be extended stretches during its early stages when there are no readily apparent clinical symptoms, delaying early diagnosis and treatment of the condition. Cardiac ultrasound is a very suitable method for early CVD screening in high-risk populations because it reflects the anatomy and function of the heart at an early stage. Due to its simplicity and accessibility, recent research have demonstrated that NHR can be utilized as a CVD prediction tool, however there have been no investigations on the relationship between NHR and heart anatomy and function.14 A better method for the early detection and prevention of CVD may therefore result from investigating the association between NHR and cardiac ultrasound parameters.
We investigated the relationship between NHR and cardiac ultrasound parameters, as well as NHR and cardiovascular risk predicted by the ICVD risk assessment tool, in an outpatient-based cross-sectional study that included a healthy physical examination population, in order to propose novel clinical concepts and strategies for the prevention and diagnosis of CVD.
Materials and Methods
Study Participants
Clinical records were obtained from all populations attending the Hebei General Hospital physical examination center from June 2022 to July 2022 and were evaluated retrospectively. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Ethics Committee (approval number: 2020–27).
The inclusion criteria for patients were as follows: (a) age ≥ 18 years; (b) consent to participate in the trial; (c) no previous history of chronic disease and medication use. Exclusion criteria were as follows: (a) coronary artery disease; (b) hypertension; (c) history of cardiac surgery or coronary stenting; (d) history of other diseases affecting the structure or function of the heart. Finally, a total of 3020 healthy individuals were recruited for this study.
Information and Data Collection
All participants’ basic information was collected, including gender, age, height, weight, waist circumference, hip circumference, tobacco and alcohol use, and blood pressure. Blood samples were collected from all participants at least 8 hours of fasting and included triglycerides (TG), total cholesterol (TC), HDL-C, low-density lipoprotein cholesterol (LDL-C), alanine aminotransferase (ALT), aspartate aminotransferase (AST), uric acid (UA), fasting blood glucose (FBG), and blood count. All indicators were measured by professionals using a fully automated biochemical analyzer under the same experimental conditions.
The cardiac ultrasound (GE Vivid E9, USA) was performed by the same group of trained physicians according to the same criteria in all participants. Cardiac ultrasound indices included Aorta (AO), Left Atrium (LA), Right Atrium (RA), Right Ventricle (RV), End Systolic Diameter of Left Ventricle (ESD), End Diastolic Diameter of Left Ventricle (EDD), Main Pulmonary Artery (MPA), Right Ventricular Outflow Tract (RVOT), Interventricular Septum (IVS), Left Ventricular Posterior Wall (LVPW), Ejection Fraction (EF), Fractional Shortening (FS) and calculated E/A values.
Calculation of Parameters
BMI = weight (kg)/height (m)2. The formula for calculating NHR is the ratio of neutrophil count (×109/L) to HDL-C (mmol/L).
Assessment of Cardiovascular Risk
The Chinese 10-year ICVD risk assessment tool evaluates the risk of a first fatal cardiovascular event in the next 10 years based on six factors: age, smoking, BMI, systolic blood pressure (SBP), TC, and diabetes as independent variables. The system calculates risk for participants aged 35 to 60 years to predict future cardiovascular risk.
Statistical Analysis
All data were analyzed and visualized using GraphPad Prism 8.01 software. Data satisfying a normal distribution are expressed as mean ± standard deviation and vice versa as median (25th percentile, 75th percentile). Differences between groups were tested by independent samples t-test. If the data did not meet a normal distribution, Mann–Whitney U analysis was used to compare differences between groups. Spearman or Pearson correlation analysis was used to determine the correlation between variables. Differences between groups were considered statistically significant when P<0.05.
Results
Clinical Characteristics of All Participants
A total of 3020 healthy participants were included in the study according to the inclusion and exclusion criteria (Figure 1). In total, there were 1879 men and 1141 women with a average age of 59.23 years and a average BMI of 24.45 kg/m2. The average NHR was 2.63, and all populations were divided into high and low NHR groups (n=1510/group) based on the median.
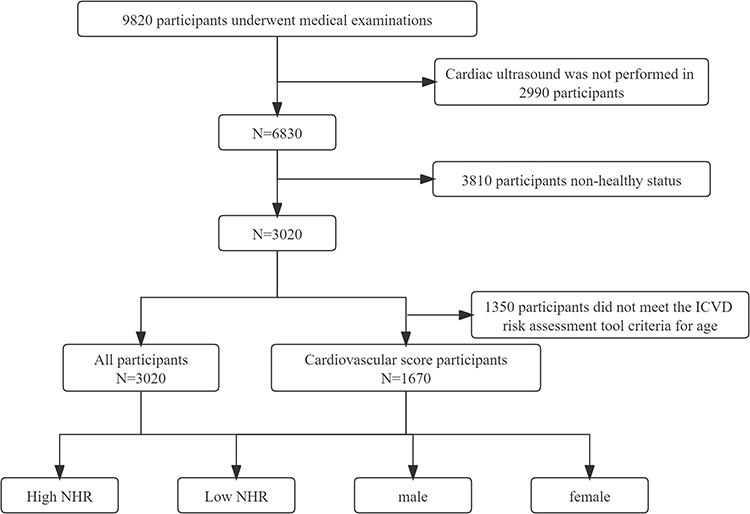 |
Figure 1 Flow chart of this cross-sectional study. Abbreviations: ICVD, ischemic cardiovascular disease; NHR, neutrophils count to high density lipoprotein ratio. |
Clinical Characteristics of Participants in High and Low NHR Groups
The high NHR group was older, had higher BMI, waist and hip circumference, and similarly had higher SBP and DBP compared to the low NHR group (Figure 2A-F). HDL-C and TC were higher in the low NHR group, while TG and LDL-C were higher in the high NHR group (Figure 2G-J). UA, blood cell count, FBG, and ALT were all higher in the high NHR group compared to the low NHR group, while AST was not significantly different (Figure 2K-R). Comparison of tobacco and alcohol use between the two groups showed that participants in the high NHR group had higher rates of tobacco and alcohol use (Figure 2S).
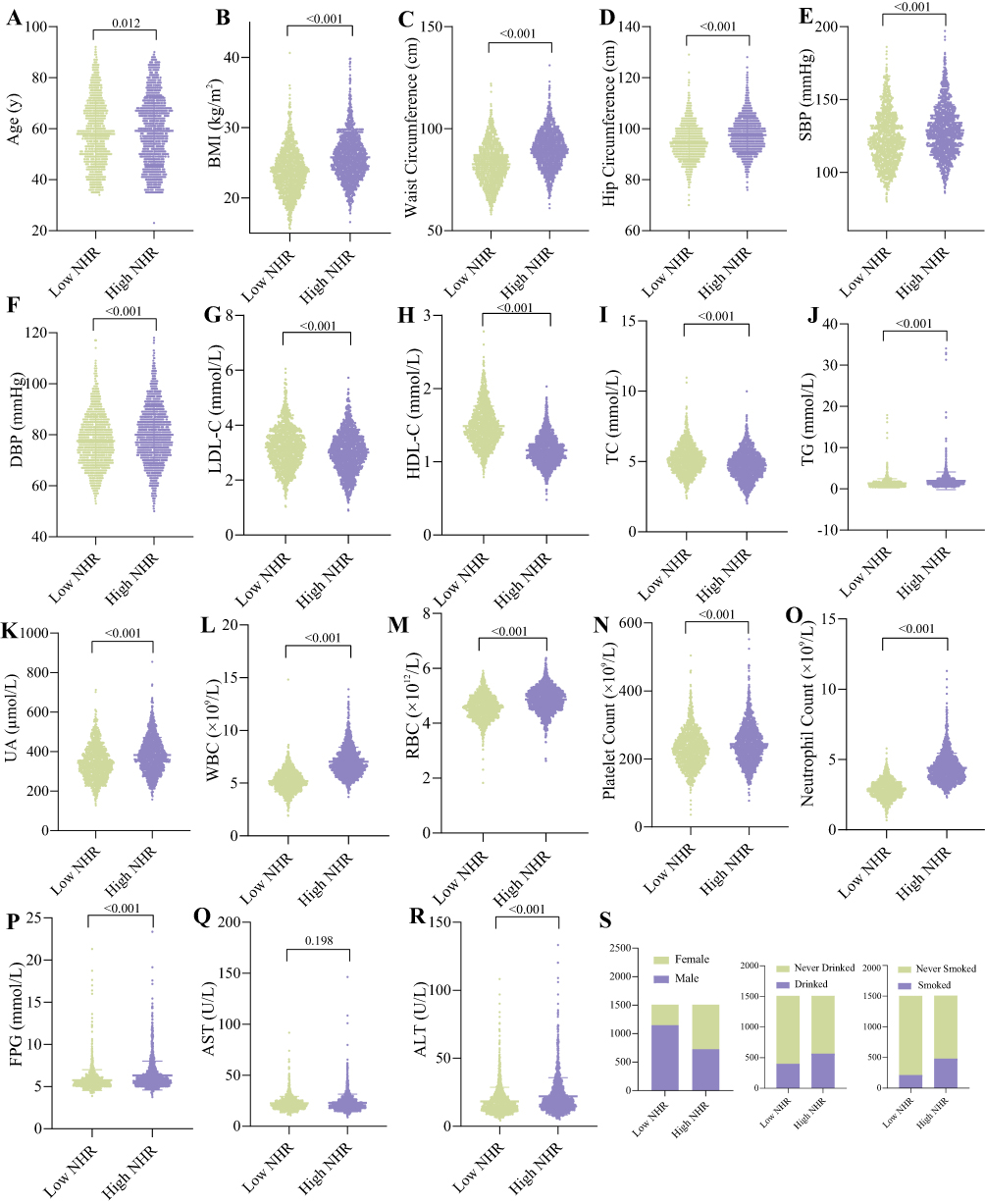 |
Figure 2 Clinical characteristics of participants in high and low NHR groups. (A) Age. (B) BMI. (C) Waist Circumference. (D) Hip Circumference. (E) SBP. (F) DBP. (G) LDL-C. (H) HDL-C. (I) TC. (J) TG. (K) UA. (L) WBC. (M) RBC. (N) Platelet Count. (O) Neutrophil Count. (P) FBG. (Q) ALT. (R) AST. (S) Tobacco and alcohol use rates and gender distribution. Abbreviations: BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TC, total cholesterol; TG, triglyceride; UA, uric acid; WBC, white blood cell; RBC, red blood cell; FBG, fasting blood glucose; ALT, alanine aminotransferase; AST, aspartate aminotransferase; NHR, neutrophils count to high density lipoprotein ratio. |
Comparison of Cardiac Ultrasound Parameters Between High and Low NHR Groups
Participants in the high NHR group had greater AO, LA, RA, RV, ESD, EDD, MPA, RVOT, IVS, and LVPW compared with those in the low NHR group (P<0.001) (Figure 3A-J). EF and FS were not significantly different between the two groups (P>0.05) (Figure 3K and L). E/A reflects early diastolic impairment, and the results of this study showed that participants in the high NHR group had lower E/A values than those in the low NHR group (p<0.001) (Figure 3M and N).
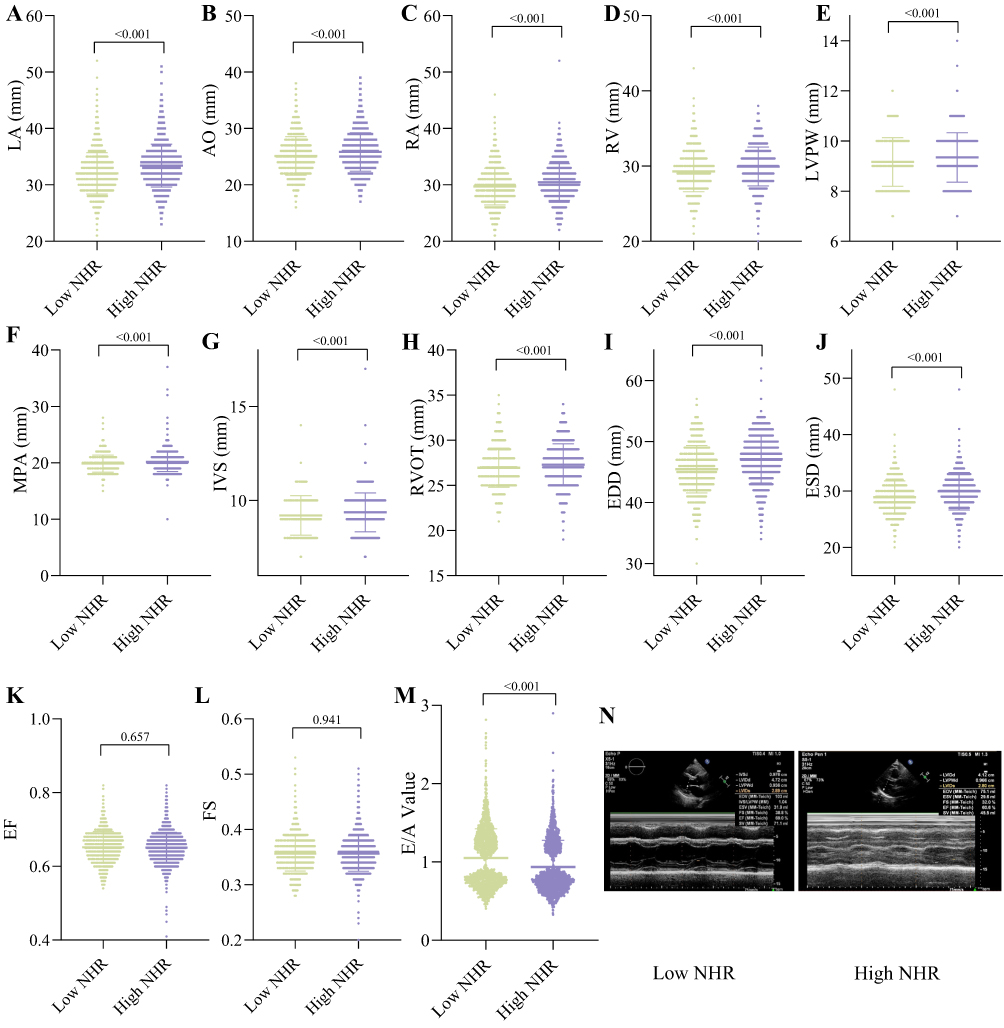 |
Figure 3 Comparison of cardiac ultrasound parameters between high and low NHR groups. (A) LA. (B) AO. (C) RA. (D) RV. (E) LVPW. (F) MPA. (G) IVS. (H) RVOT. (I) EDD. (J) ESD. (K) EF. (L) FS. (M) E/A Value. (N) Representative cardiac ultrasound images. Abbreviations: LA, Left Atrium; AO, Aorta; RA, Right Atrium; RV, Right Ventricle; LVPW, Left Ventricular Posterior Wall; MPA, Main Pulmonary Artery; IVS, Interventricular Septum; RVOT, Right Ventricular Outflow Tract; EDD, End Diastolic Diameter of Left Ventricle; ESD, End Systolic Diameter of Left Ventricle; EF, Ejection Fraction; FS, Fractional Shortening. |
Clinical Characteristics of Male and Female Participants
Compared to female participants, male individuals were older and had higher BMI, waist and hip circumference, and similarly, higher SBP and DBP (Figure 4A-F). HDL-C, LDL-C and TC were higher in women, while TG was higher in men (Figure 4G-J). Compared to females, males had higher UA, blood counts, FBG, AST, and ALT, except for platelet counts (Figure 4K-R). NHR was significantly higher in male participants than in females, and the same trend was observed for tobacco and alcohol use (Figure 4S and T).
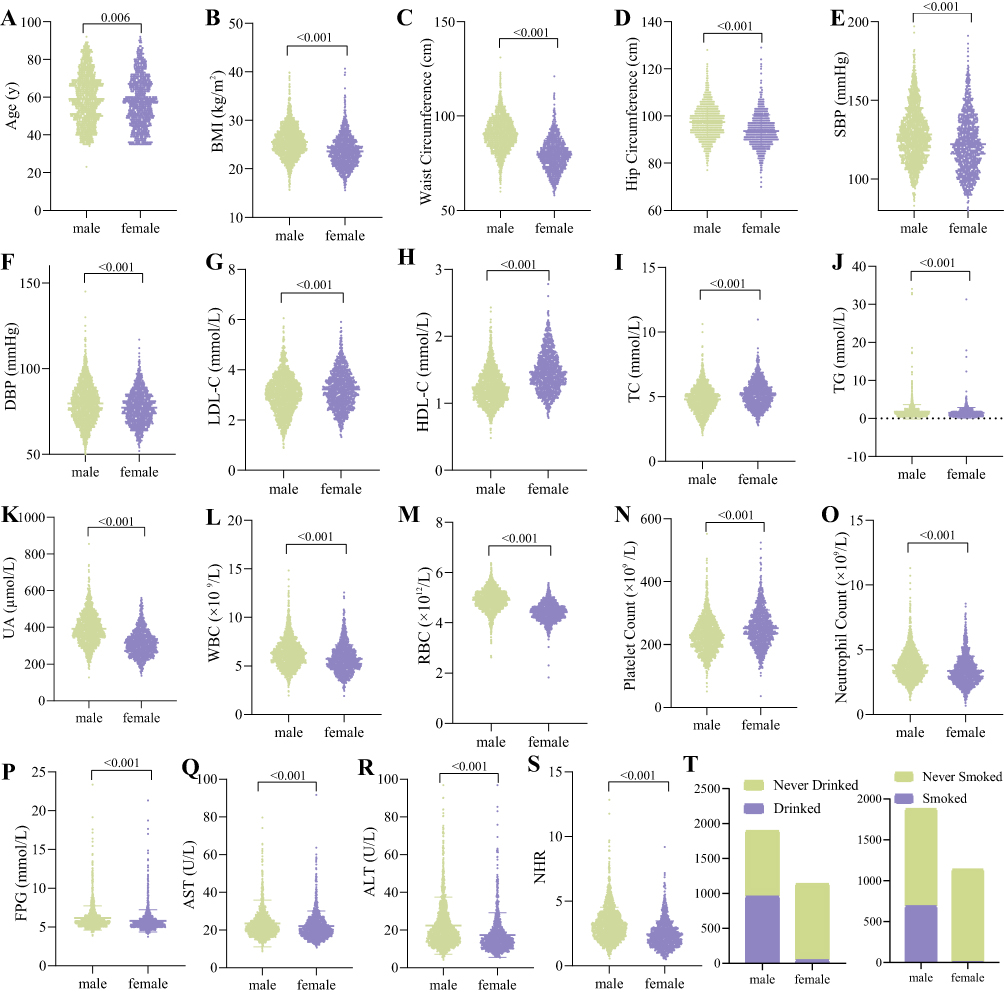 |
Figure 4 Clinical characteristics of male and female participants. (A) Age. (B) BMI. (C) Waist Circumference. (D) Hip Circumference. (E) SBP. (F) DBP. (G) LDL-C. (H) HDL-C. (I) TC. (J) TG. (K) UA. (L) WBC. (M) RBC. (N) Platelet Count. (O) Neutrophil Count. (P) FBG. (Q) AST. (R) ALT. (S) NHR. (T) Tobacco and alcohol use rates. Abbreviations: BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TC, total cholesterol; TG, triglyceride; UA, uric acid; WBC, white blood cell; RBC, red blood cell; FBG, fasting blood glucose; ALT, alanine aminotransferase; AST, aspartate aminotransferase; NHR, neutrophils count to high density lipoprotein ratio. |
Comparison of Cardiac Ultrasound Parameters Between Male and Female Participants
Male participants had greater AO, LA, RA, RV, ESD, EDD, MPA, RVOT, IVS, and LVPW compared with females (P<0.001) (Figure 5A-J), and similarly EF and FS between the two groups were greater in males than in female participants (P<0.01) (Figure 5K and L). However, E/A values were greater in female participants than in males (p<0.001) (Figure 5M and N).
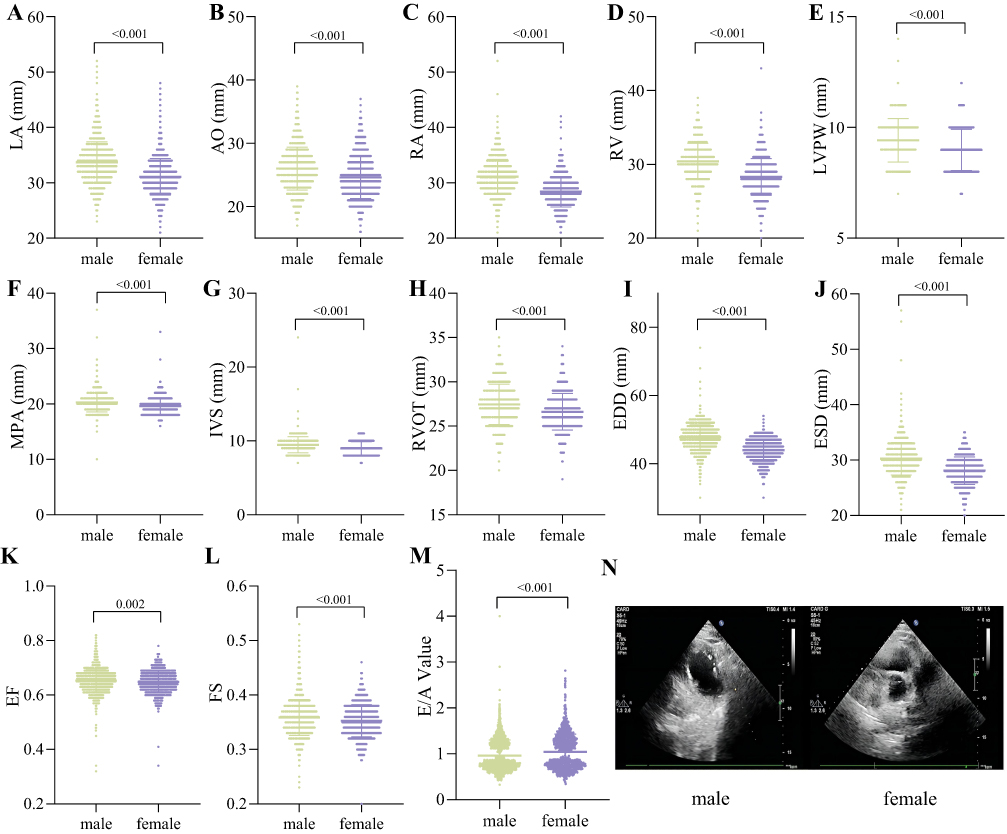 |
Figure 5 Comparison of cardiac ultrasound parameters between male and female participants. (A) LA. (B) AO. (C) RA. (D) RV. (E) LVPW. (F) MPA. (G) IVS. (H) RVOT. (I) EDD. (J) ESD. (K) EF. (L) FS. (M) E/A Value. (N) Representative cardiac ultrasound images. Abbreviations: LA, Left Atrium; AO, Aorta; RA, Right Atrium; RV, Right Ventricle; LVPW, Left Ventricular Posterior Wall; MPA, Main Pulmonary Artery; IVS, Interventricular Septum; RVOT, Right Ventricular Outflow Tract; EDD, End Diastolic Diameter of Left Ventricle; ESD, End Systolic Diameter of Left Ventricle; EF, Ejection Fraction; FS, Fractional Shortening. |
Cardiovascular Risk Assessment
A total of 1670 participants were included in the ICVD risk assessment tool for scoring, including 1000 males and 670 females. The average age was 48.61 years, average BMI was 24.82 kg/m2, and average NHR was 2.86. Other indicators such as blood pressure, FBG, lipids, UA, ALT and AST were within the median normal range (Table 1). Participants in the high NHR group and males had higher risk scores based on the ICVD risk assessment tool compared to those in the low NHR group and females (Figure 6A and B).
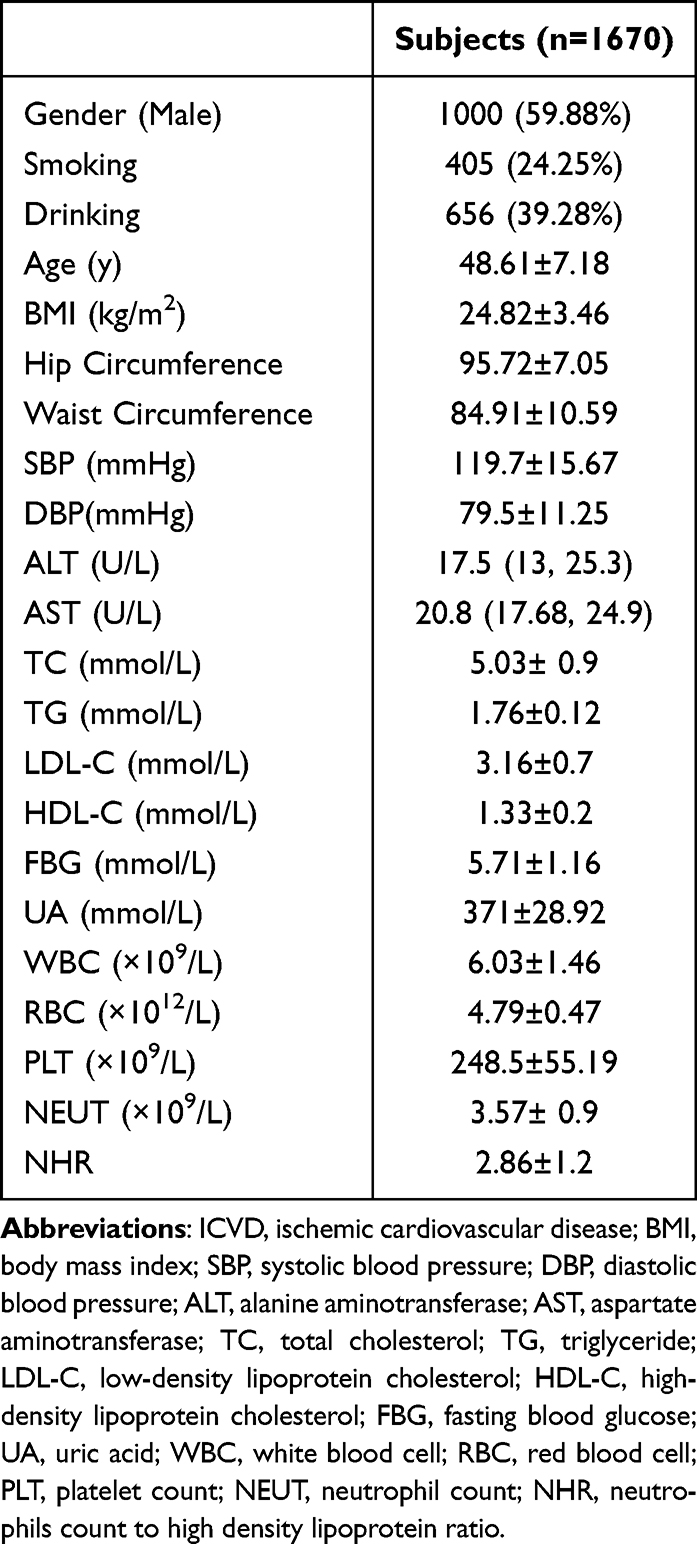 |
Table 1 Clinical Characteristics of All Participants Who Were Scored by ICVD Risk Assessment Tool |
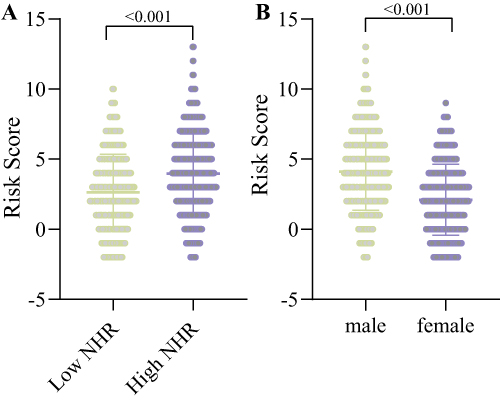 |
Figure 6 Cardiovascular risk assessment. (A) Comparison of cardiovascular risk scores between the low NHR and high NHR groups. (B) Comparison of cardiovascular risk scores in males and females. |
Correlation Between NHR and Cardiac Ultrasound Parameters
In all participants, correlation analysis showed that NHR was significantly and positively correlated with AO, LA, RA, RV, ESD, EDD, MPA, RVOT, IVS, and LVPW, and NHR was also positively correlated with cardiovascular risk in participants (p<0.001). However, there was a significant negative correlation between NHR and E/A values (P<0.001).
In male participants, NHR was weakly correlated with LA (P=0.0043) and RVOT (P=0.0304), while NHR was significantly positively correlated with cardiovascular risk (P<0.001). Similarly, there was a significant negative correlation between NHR and E/A values (P<0.001). Among female participants, there was a negative correlation between NHR and E/A values (P=0.0398), while there was no significant correlation between NHR and other cardiac ultrasound parameters and risk scores (P>0.05) (Table 2).
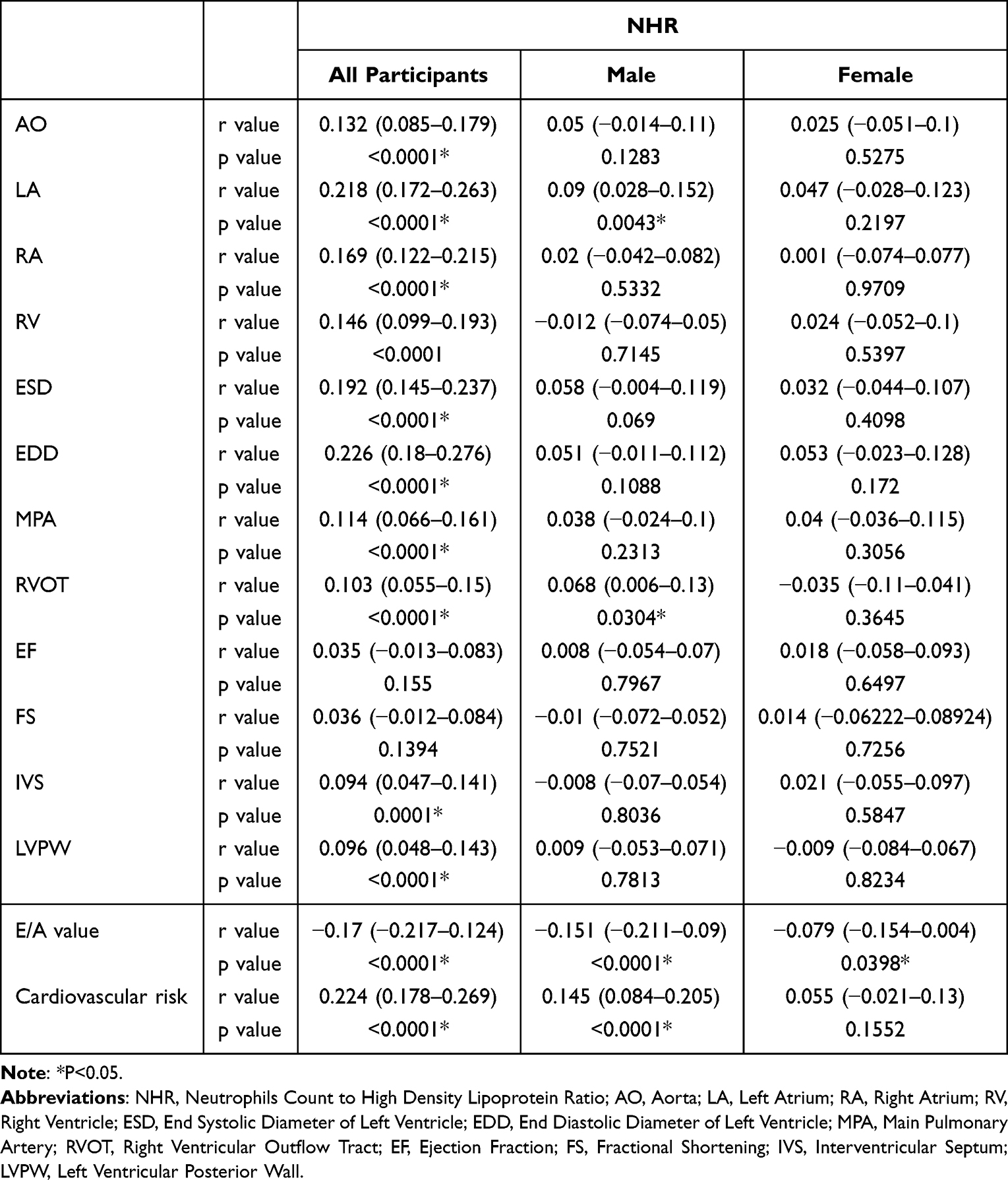 |
Table 2 Correlation Between NHR and Cardiac Ultrasound Index |
Discussion
In this cross-sectional investigation, we looked at the link between NHR and cardiac ultrasonography measures, as well as NHR and cardiovascular risk in a group of 3020 healthy people. Our study’s key findings were as follows: (1) There was a significant difference in cardiac ultrasound parameters between individuals with high and low NHR. (2) Male and female cardiac ultrasound parameters differed significantly. (3) The NHR and cardiac ultrasound parameters showed a strong connection. (4) There was a significant correlation between NHR and cardiovascular risk, as determined by the ICVD risk assessment tool, in both males and all participants.
NHR is a new lipid biomarker capable of quantifying inflammation and lipid levels.15,16 As a result, a rise in NHR can indirectly reflect increasing levels of inflammation and lower anti-inflammatory capacity in the body. This study found that those with high NHR had greater BMI, waist circumference, hip circumference, BP, FBG, non-HDL-C, and UA levels than those with low NHR. Male participants had higher levels of these markers than females because they had higher NHR levels. These findings imply that an increase in NHR may indicate metabolic disruptions and elevated levels of inflammation in vivo, both of which are risk factors for CVD. As a result, the relationship between NHR and CVD is receiving increasing attention.
According to studies, neutrophils contribute to the development of atherosclerosis and are strongly correlated with the frequency of unfavorable cardiovascular events.17 Furthermore, in acute cardiovascular events, the high number of neutrophil aggregates allows for enhanced expression of local inflammatory mediators and cell adhesion molecules, increasing inflammation and exacerbating the condition. HDL-C promotes endothelial function and blood viscosity while also being anti-atherosclerotic.17–19 Previous research has found that HDL-C and neutrophils can regulate each other’s functions.20 As a result, there is a significant correlation between NHR and cardiovascular risk when previous research are combined. In this study, the ICVD risk assessment tool was used to forecast the frequency of initial cardiovascular events during a 10-year period in a group that was generally healthy. Our study discovered a positive relationship between NHR and cardiovascular risk in healthy persons with high NHR. This relationship was also shown in the male population but not in the female population and may be associated with lower NHR, lower BMI, and lower cardiovascular risk in non-menopausal women. Previous research has demonstrated that NHR can be used as a prognostic marker in patients with cardiovascular disease, and the findings of this study imply that NHR can also be used to predict cardiovascular risk in healthy people.
The risk of cardiovascular events is very closely linked to changes in heart shape and function. A substantial positive connection between a number of cardiac ultrasound parameters and cardiovascular risk was found in our prior work.21 We aimed to investigate the association between NHR and cardiac ultrasound parameters in the current investigation. The findings suggested a link between high NHR and early structural alterations in the heart since the high NHR population had higher levels of AO, LA, RA, RV, ESD, EDD, MPA, RVOT, IVS, and LVPW than the low NHR population. E/A values were lower in the high NHR population compared to the low NHR population, and EF and FS did not change significantly between the two groups, suggesting that cardiac systolic function was not yet impaired, but diastolic function may have decreased to some extent. The above results are consistent with the criteria for preclinical stage cardiac lesions, implying that increased NHR seems to be associated with early structural and functional cardiac damage. However, the mechanism by which NHR leads to structural changes and dysfunction of the heart is not clear. It may be explained that NHR is an indicator of inflammation and that elevated NHR can cause abnormal cellular metabolism and oxidative stress thus triggering cardiomyocyte hypertrophy or even death.7,22,23 In addition, the aggregation of neutrophils and their secretion of cytokines, and the decrease in HDL-C, which diminishes the anti-inflammatory effect in vivo, together contribute to microvascular dysfunction.24,25 Cardiomyocyte death, hypertrophy and extracellular matrix remodeling, as well as microvascular dysfunction, ultimately affect cardiac structure and function. The correlation analysis showed that NHR was significantly positively correlated with AO, LA, RA, RV, ESD, EDD, MPA, RVOT, IVS, and LVPW, and negatively correlated with E/A values, further suggesting the correlation between NHR and structural and functional cardiac impairment. However, this correlation was significantly weaker in the gender subgroup analysis, which may be related to the higher NHR correlation in the male population compared to the female population and the lower cardiovascular risk in non-menopausal women. Meanwhile, in the gender subgroup analysis, males had higher AO, LA, RA, RV, ESD, EDD, MPA, RVOT, IVS, and LVPW, and lower E/A values than females, which may be associated with greater BMI and higher NHR in males. Therefore, the significant correlation between NHR and cardiac ultrasound parameters and cardiovascular risk based on healthy population provides a new idea for early diagnosis and intervention of CVD and improves the diagnosis and treatment system of CVD.
This study has several limitations. Firstly, the cross-sectional study limits the persuasiveness of our study and does not lead to causal conclusions. Secondly, this study is based on a single center, so multicenter and large-scale studies are needed to validate the findings of this study. And third, compared with the ICVD risk assessment tool, SCORE2 appears to be a better predictor of the total burden of cardiovascular disease, especially in younger adults, and thus warrants the next step of a study comparing the advantages and disadvantages of the two scoring systems. Finally, the ICVD risk assessment tool is only a predictive tool for cardiovascular risk and does not fully reflect the true incidence of cardiovascular events, so long-term follow-up is needed to validate this conclusion.
Conclusion
Increased NHR was linked to cardiac structural and functional impairment in healthy populations, but these correlations were noticeably weaker in the analysis of the gender subgroup. NHR and cardiovascular risk showed a significant positive correlation, which was also seen in the male participants but not the female ones.
Data Sharing Statement
Data supporting the results of this study are available upon reasonable request from the first author.
Ethics Approval and Consent to Participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Hebei General Hospital (Date May 8, 2020/No. 202027).
Funding
No funding was received to assist with the preparation of this article.
Disclosure
The authors declare that they have no competing interests.
References
1. Pan X, Chen S, Chen X, et al. Effect of high-fat diet and empagliflozin on cardiac proteins in mice. Nutr Metab. 2022;19(1):69. doi:10.1186/s12986-022-00705-0
2. Engelen SE, Robinson AJB, Zurke YX, Monaco C. Therapeutic strategies targeting inflammation and immunity in atherosclerosis: how to proceed? Nat Rev Cardiol. 2022;19(8):522–542. doi:10.1038/s41569-021-00668-4
3. Halasz G, Piepoli MF. Focus on Atherosclerosis and Lipids. Eur J Prev Cardiol. 2021;28(8):799–802. doi:10.1093/eurjpc/zwab090
4. Drexel H, Larcher B, Mader A, et al. The LDL-C/ApoB ratio predicts major cardiovascular events in patients with established atherosclerotic cardiovascular disease. Atherosclerosis. 2021;329:44–49. doi:10.1016/j.atherosclerosis.2021.05.010
5. Casula M, Colpani O, Xie S, Catapano AL, Baragetti A. HDL in Atherosclerotic Cardiovascular Disease: in Search of a Role. Cells. 2021;10(8):1869. doi:10.3390/cells10081869
6. Santoro L, Ferraro PM, Nesci A, et al. Neutrophil-to-lymphocyte ratio but not monocyte-to-HDL cholesterol ratio nor platelet-to-lymphocyte ratio correlates with early stages of lower extremity arterial disease: an ultrasonographic study. Eur Rev Med Pharmacol Sci. 2021;25(9):3453–3459. doi:10.26355/eurrev_202105_25826
7. Jiang M, Sun J, Zou H, et al. Prognostic Role of Neutrophil to High-Density Lipoprotein Cholesterol Ratio for All-Cause and Cardiovascular Mortality in the General Population. Front Cardiovasc Med. 2022;9:807339. doi:10.3389/fcvm.2022.807339
8. Chen H, Xiong C, Shao X, et al. Lymphocyte To High-Density Lipoprotein Ratio As A New Indicator Of Inflammation And Metabolic Syndrome. Diabetes Metab Syndr Obes. 2019;12:2117–2123. doi:10.2147/DMSO.S219363
9. Ozgeyik M, Ozgeyik MO. Long-term Prognosis after Treatment of Total Occluded Coronary Artery is well Predicted by Neutrophil to High-Density Lipoprotein Ratio: a Comparison Study. Kardiologiia. 2021;61(7):60–67. doi:10.18087/cardio.2021.7.n1637
10. Liu SL, Feng BY, Song QR, Zhang YM, Wu SL, Cai J. Neutrophil to high-density lipoprotein cholesterol ratio predicts adverse cardiovascular outcomes in subjects with pre-diabetes: a large cohort study from China. Lipids Health Dis. 2022;21(1):86. doi:10.1186/s12944-022-01695-x
11. Li Y, Liu J, Zhou B, et al. Reducing the 10-year risk of ischemic cardiovascular disease to receive early cardiovascular benefits from bariatric surgery for obesity in China. Front Cardiovasc Med. 2022;9:978682. doi:10.3389/fcvm.2022.978682
12. Yang L, Fish AF, Zhu Y, et al. Sex differences in 10-year ischemic cardiovascular disease risk prediction in Chinese patients with prediabetes and type 2 diabetes. BMC Cardiovasc Disord. 2019;19(1):301. doi:10.1186/s12872-019-1232-y
13. Tibaut M, Caprnda M, Kubatka P, et al. Markers of Atherosclerosis: part 2 - Genetic and Imaging Markers. Heart Lung Circ. 2019;28(5):678–689. doi:10.1016/j.hlc.2018.09.006
14. Chen Y, Jiang D, Tao H, Ge P, Duan Q. Neutrophils to high-density lipoprotein cholesterol ratio as a new prognostic marker in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention: a retrospective study. BMC Cardiovasc Disord. 2022;22(1):434. doi:10.1186/s12872-022-02870-9
15. Liu Z, Fan Q, Wu S, Wan Y, Lei Y. Compared with the monocyte to high-density lipoprotein ratio (MHR) and the neutrophil to lymphocyte ratio (NLR), the neutrophil to high-density lipoprotein ratio (NHR) is more valuable for assessing the inflammatory process in Parkinson’s disease. Lipids Health Dis. 2021;20(1):35. doi:10.1186/s12944-021-01462-4
16. Kou T, Luo H, Yin L. Relationship between neutrophils to HDL-C ratio and severity of coronary stenosis. BMC Cardiovasc Disord. 2021;21(1):127. doi:10.1186/s12872-020-01771-z
17. Chen G, Yang N, Ren J, et al. Neutrophil Counts to High-Density Lipoprotein Cholesterol Ratio: a Potential Predictor of Prognosis in Acute Ischemic Stroke Patients After Intravenous Thrombolysis. Neurotox Res. 2020;38(4):1001–1009. doi:10.1007/s12640-020-00274-1
18. Ossoli A, Pavanello C, Giorgio E, Calabresi L, Gomaraschi M. Dysfunctional HDL as a Therapeutic Target for Atherosclerosis Prevention. Curr Med Chem. 2019;26(9):1610–1630. doi:10.2174/0929867325666180316115726
19. Fan LL, Liu L, Wang CY, Guo T, Luo H. A novel nonsense mutation of ABCA8 in a patient with reduced HDL-c levels and atherosclerosis. QJM. 2022;115(5):321–322. doi:10.1093/qjmed/hcac009
20. Huang JB, Chen YS, Ji HY, et al. Neutrophil to high-density lipoprotein ratio has a superior prognostic value in elderly patients with acute myocardial infarction: a comparison study. Lipids Health Dis. 2020;19(1):59. doi:10.1186/s12944-020-01238-2
21. Pan X, Chen X, Ren L, Li Z, Chen S. Correlation between Cardiac Ultrasound Index and Cardiovascular Risk in Healthy Obese and Overweight Populations. Int J Clin Pract. 2022;2022:2235994. doi:10.1155/2022/2235994
22. Jialal I, Jialal G, Adams-Huet B, Ramakrishnan N. Neutrophil and monocyte ratios to high-density lipoprotein-cholesterol and adiponectin as biomarkers of nascent metabolic syndrome. Horm Mol Biol Clin Investig. 2020;41(2). doi:10.1515/hmbci-2019-0070
23. Chen T, Chen H, Xiao H, et al. Comparison of the Value of Neutrophil to High-Density Lipoprotein Cholesterol Ratio and Lymphocyte to High-Density Lipoprotein Cholesterol Ratio for Predicting Metabolic Syndrome Among a Population in the Southern Coast of China. Diabetes Metab Syndr Obes. 2020;13:597–605. doi:10.2147/DMSO.S238990
24. El Kazzi M, Rayner BS, Chami B, Dennis JM, Thomas SR, Witting PK. Neutrophil-Mediated Cardiac Damage After Acute Myocardial Infarction: significance of Defining a New Target Cell Type for Developing Cardioprotective Drugs. Antioxid Redox Signal. 2020;33(10):689–712. doi:10.1089/ars.2019.7928
25. Tenekecioglu E, Yilmaz M, Demir S, et al. HDL-cholesterol is associated with systemic inflammation in cardiac syndrome X. Minerva Med. 2015;106(3):133–141.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.