Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Association of CLTA-4 Gene Polymorphisms with Diabetes Mellitus: A Study Based on the Han Population of Northern China
Received 16 May 2022
Accepted for publication 15 August 2022
Published 3 September 2022 Volume 2022:15 Pages 2705—2712
DOI https://doi.org/10.2147/DMSO.S374451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Dongyue Ren,1 Lin He,2 Xiaoling Pang1
1Department of Emergency, the Fourth Affiliated Hospital of China Medical University, Shenyang, People’s Republic of China; 2Good Clinical Practice Institution, the Fourth Affiliated Hospital of China Medical University, Shenyang, People’s Republic of China
Correspondence: Xiaoling Pang, Department of Emergency, the Fourth Affiliated Hospital of China Medical University, No. 4 Chongshan East Road, Huanggu District, Shenyang, 110032, People’s Republic of China, Tel +86-18900913992, Email [email protected]
Objective: This study aimed to investigate the association of CLTA-4 gene polymorphism with Type 1 and 2 diabetes mellitus (DM) (T1DM and T2DM) in the Han population of northern China.
Methods: A total of 234 Chinese Han DM patients and 187 non-diabetic subjects were included in the study. Two gene polymorphisms of the CLTA-4, including CTLA-4+49A/G (rs231775) and CTLA4-318C/T (rs5742909), were studied using polymerase chain reaction-restriction endonuclease fragment length polymorphism (PCR-RFLP) analysis. Chi-square analysis and Student’s t-test were performed to determine the distribution of the gene polymorphism and alleles at the locus of CTLA4-318C/T and CTLA4+49A/G among T1DM and T2DM patients with or without diabetic ketosis (DK), diabetic nephropathy (DN) or autoantibodies (Ab).
Results: Our results indicated that the distribution frequencies of genotypes and alleles at the CTLA-4+49A/G and CTLA4-318C/T loci of T1DM patients were not significantly different from those of the controls. However, the distribution frequencies of genotypes and alleles at the CTLA-4+49A/G loci of T2DM patients were significantly different from the controls (P=0.024 for genotypes and P=0.004 for A and G alleles). Besides, the A and G alleles at the CTLA4-318C/T loci of T2DM DK+ patients showed significantly different distribution frequencies compared to those of the T2DM DK patients (P=0.001).
Conclusion: Our data suggest that the gene polymorphisms of CTLA-4, including CTLA-4+49A/G and CTLA4-318C/T, are important predictors of DM. CTLA-4 may be a susceptibility gene for T2DM. Patients with T2DM carrying the T allele at the CTLA4-318 C/T locus are more predisposed to diabetic ketosis.
Keywords: diabetes mellitus, gene polymorphism, CTLA-4, diabetic ketosis, diabetic nephropathy, autoantibodies
Introduction
Diabetes mellitus (DM) is a highly prevalent disease characteristic of elevated glucose level as a result of dysregulated metabolism. There are currently 285 million people with diabetes worldwide, and nearly 500 million people is expected to develop diabetes by 2030.1 The chronic vascular complications of diabetes pose a great threat to patients’ lives and impose a heavy economic burden. The World Health Organization estimated that the economic loss due to diabetes in China has amounted to $557.7 billion between 2005 and 2015.2
The etiology of diabetes is yet to be fully understood. It is now recognized that diabetes is not a disease of a single cause, but a syndrome of multiple causes, among which are genetic, autoimmune and environmental factors.3,4 There are two major subtypes of diabetes mellitus: type 1 and type 2 diabetes. Type 1 diabetes results from cell-mediated autoimmune destruction of β-cells, causing decreased insulin production.5 Type 2 diabetes is characteristic of progressive loss of islet function and insulin resistance in peripheral tissues, eventually requiring insulin therapy. Therefore, immunological factors are extremely important in the pathogenesis of both type 1 and 2 diabetes.6
The capability of some pancreatic β-cells to secrete insulin is lost by the time diabetes develops symptoms, therefore prediction and prevention of diabetes are very important.5 It is helpful to know the genetic profile of diabetes to prevent it. Understanding the genetic underpinnings of DM is critical to develop effective treatments of the disease.7 A recent study suggested that CTLA-4, a costimulatory molecule that activates T cells, might be one of the candidate biomarkers related to DM susceptibility.8 CTLA-4 consists of four exons and three introns and is located on the long arm of chromosome 2q33. Similar to CD28, CTLA-4 also belongs to the immunoglobulin superfamily, but has a higher affinity to B7 molecule expressed on the antigen-presenting cells (APCs) than CD28, making CTLA-4 a potent suppressor of T-cells.9
CTLA-4 has multiple polymorphic loci. The exon 1+49 A/G polymorphism is the sole polymorphism that alters the major amino acid sequence of CTLA4.10 An in vitro study showed that exon +49 A/G mutations in CTLA-4 caused abnormal glycosylation of the endoplasmic reticulum (ER), resulting in decreased cell surface expression.11 In contrast, the CTLA-4 promoter −318 C/T polymorphism is associated with higher promoter activity, which increases CTLA-4 expression and thus decreases T-cell activity, and this polymorphism could be protective against the pathogenesis of autoimmune diseases.12
In this study, we applied PCR-RFLP method13 to detect the gene polymorphisms of promoter exon −318C/T and +49A/G of CTLA-4, and demonstrated the correlation between the gene polymorphisms of −318C/T and +49A/G of CTLA-4 and type 1 and 2 diabetes in Han population in northern China, which provides a new molecular epidemiological basis for the genetic study of diabetes and for predicting the development and genotyping of DM. Our data suggest that the CTLA-4 polymorphisms are important predictors of DM and CTLA-4 may be a susceptibility gene for type 2 diabetes. Patients with type 2 diabetes carrying the T allele at the CTLA4-318 C/T locus are more predisposed to diabetic ketosis. Our study provides a new valuable genetic diagnostic tool for stratifying patients with type 2 diabetes.
Materials and Methods
Study Subjects
In total, 234 Chinese Han diabetic patients who were hospitalized from November 2008 to August 2010 were enrolled in the study. The participants included 13 cases of type 1 diabetes, 221 cases of type 2 diabetes, 26 cases of type 2 diabetes with diabetic ketosis, 53 cases of diabetic nephropathy, 26 patients with positive antibodies to any of DAD65, IAA and IA-2 antibodies, and 107 patients with negative antibodies. In total, 187 non-diabetic subjects who underwent health checkups at a medical examination center were enrolled as controls. Diagnosis of diabetes was made referring to the 1999 WHO diagnostic criteria for diabetes and the Chinese population diagnostic criteria for diabetes of our diabetes association in October 1999. The study was approved by the Ethics Committee of the Fourth Affiliated Hospital of China Medical University. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
All subjects were not related to each other and had no family history of hereditary immune diseases or other autoimmune diseases. The subjects were sex- and age-matched.
PCR-RFLP
Peripheral venous blood of 2 mL was collected and stored in −20 °C until further use. Genomic DNA extraction was performed using the TIANGEN DNA extraction kit in accordance with manufacturer’s recommendations. PCR was performed using the following primers: CTLA4+49A/G (rs231775): forward, 5-GCTCTACTTCCT-GAAGACCT-3; reverse, 5-AGTCTCACT-CACCTTTGCAG-3. CTLA4-318C/T (rs5742909): forward, 5-AAATGAATTGGACTGGATGGT-3; reverse, 5-TTACGAGAAAGGAAGCCGTG-3. The annealing temperature for rs231775 and rs5742909 were 58°C and 56°C, respectively, and the product lengths were 162 and 247 bp, respectively. The following conditions were used for PCR: Pre-denaturation: 95°C for 5 minutes; Denaturation: 95°C for 30 seconds; Annealing: 30 seconds; Extension: 72°C for 30 seconds; Repeat for 30 cycles; Extension: 72°C for 5 minutes.
PCR products underwent electrophoresis using 1% agarose gel and the target bands were purified using the AXYGEN kit. The representative gel images for CTLA-4-318C/T and CTLA-4+49A/G detection are shown in Supplementary Figures S1 and S2. The restriction endonucleases, reaction conditions and fragment lengths of each SNP are shown in Table 1. PCR products containing AG and CT were selected for recovery using the AXYGEN kit and sent to TaKaRa for sequencing. The results of sequencing were compared with those of enzymatic determination to confirm the reliability of the enzymatic results. Representative sequencing results of the CTLA-4+49A/G and CTLA-4-318C/T loci are shown in Supplementary Figures S3 and S4.
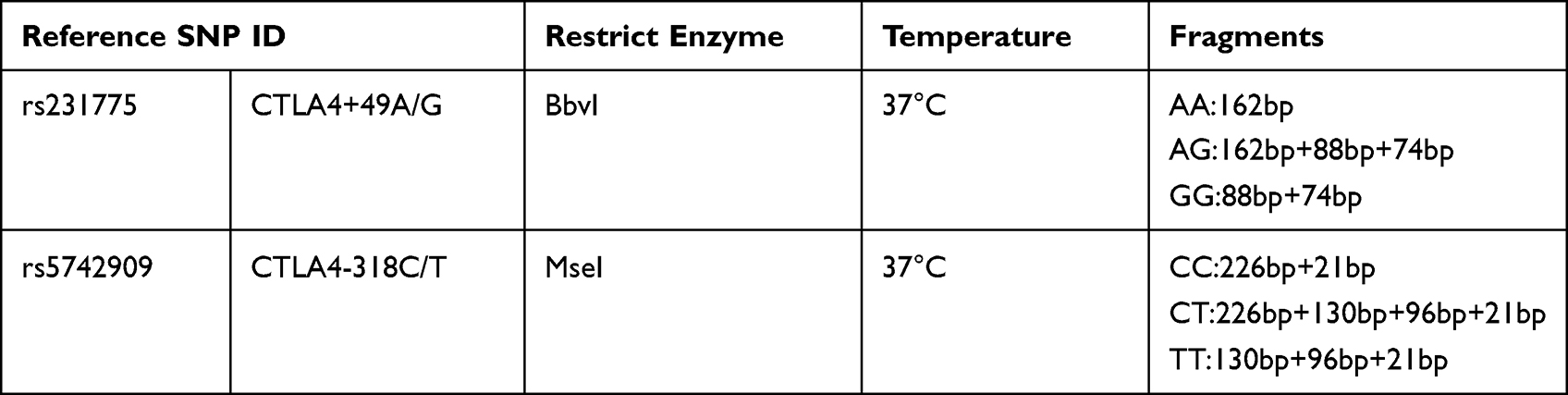 |
Table 1 Conditions for PCR-RFLP |
Statistical Analysis
SPSS16.0 software package was used for data analysis. The comparison of alleles and genotypes was performed by chi-square and Student’s t-tests. The genetic equilibrium coincidence was analyzed using the Hardy–Weinberg equilibrium method. Differences with P<0.05 were determined to be statistically significant.
Results
Study Design and Participants Characteristics
In this study, we enrolled a total of 234 Chinese Han DM patients and 187 non-diabetic healthy subjects. The differences in terms of age and gender between the diabetic group and the control group were not statistically significant and were comparable. The clinical characteristics of the two groups are shown in Table 2. The Hardy–Weinberg equilibrium test was performed on the genotype frequencies of the two loci in the control group, and the equilibrium test was met at both loci (P>0.05), indicating that the sampling was representative of the population (Table 3).
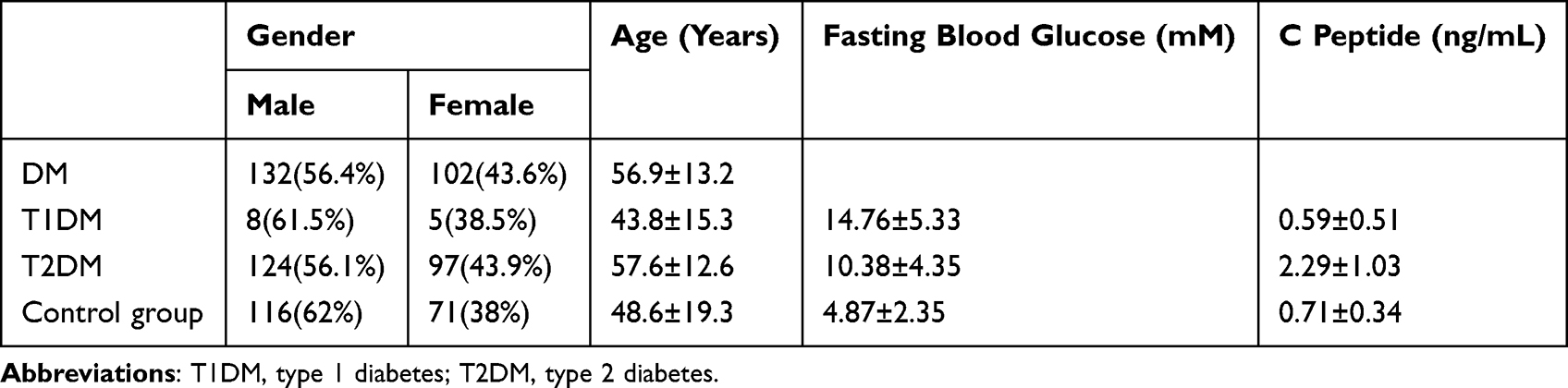 |
Table 2 Participants’ Clinical Characteristics |
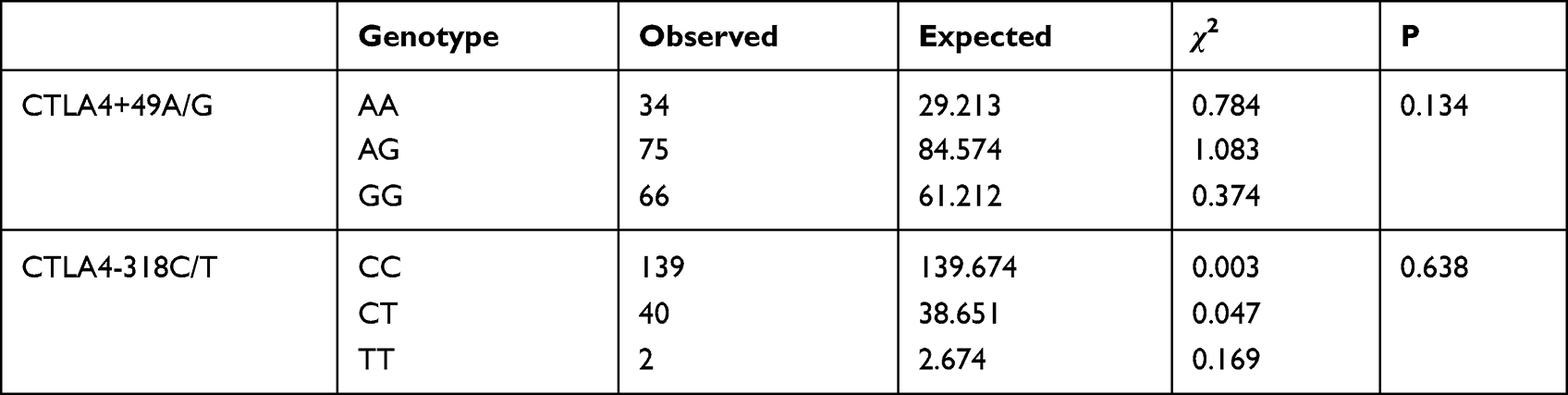 |
Table 3 Hardy–Weinberg Equilibrium Test for CTLA-4+49A/G and −318C/T Gene Polymorphisms |
Genotypes and Allele Frequency Distribution of CTLA-4+49A/G and −318C/T Loci in DM Patients Compared to Control Subjects
The frequency distributions of CTLA-4+49A/G genotype and A and G alleles were not significantly different between T1DM patients and control subjects (P>0.05, Table 4). However, the frequency distribution of CTLA4+49A/G genotype and alleles between T2DM patients and normal controls were statistically significant (P<0.05, OR=1.487, 95% confidence interval 1.116–1.981 for genotypes; and P<0.05, OR=1.55, 95% confidence interval 1.15–2.091 for alleles) (Table 5).
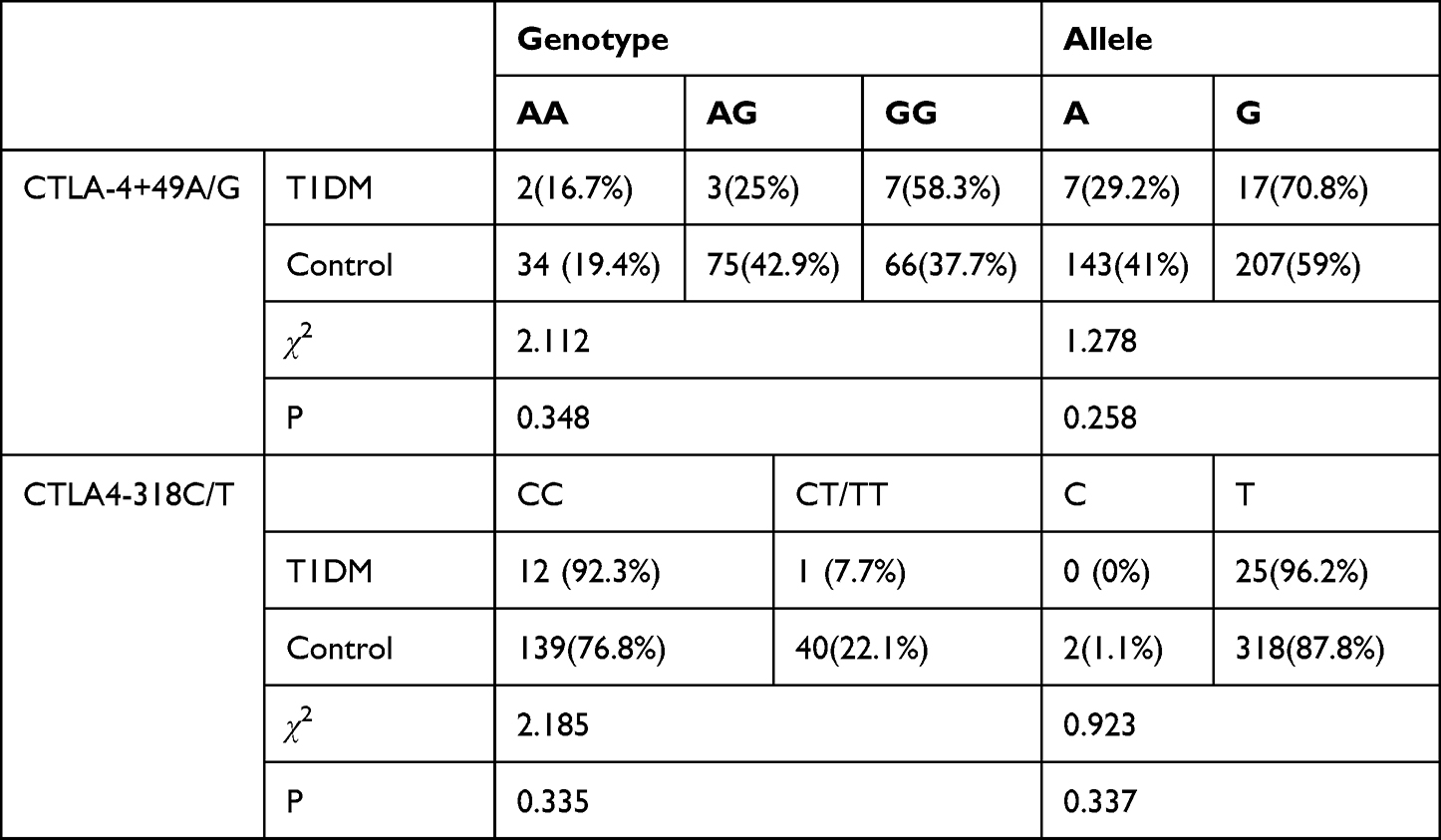 |
Table 4 Distribution of the CTLA-4 Polymorphisms in Patients with Type 1 Diabetes and Controls |
 |
Table 5 Distribution of the CTLA-4 Polymorphisms in Patients with Type 2 Diabetes and Controls |
Our analysis also indicated that at the CTLA4-318C/T locus, no significant differences were seen for the genotype and allele frequency distribution of T1DM or T2DM patients compared to healthy controls (Tables 4 and 5).
CTLA-4 Polymorphisms in T2DM Patients with or without Diabetic Ketosis
Table 6 summarizes the frequency distribution of CTLA-4-318C/T and +49A/G genotypes and alleles of T2DM patients with (DK+) or without (DK-) diabetic ketosis. Our results indicated that CTLA-4+49A/G and −318C/T genotypes both showed no significant differences in terms of genotype distribution frequency between the DK+ and DK- groups (P>0.05). CTLA-4+49A/G also showed no significance in the A and G allele distribution (P>0.05). However, in terms of CTLA4-318C/T, C and T allele frequencies were significantly different between the two groups, and T allele frequencies were higher in DK+ patients than in DK- patients in T2DM (P<0.05, OR=0.334, 95% confidence interval 0.166–0.671).
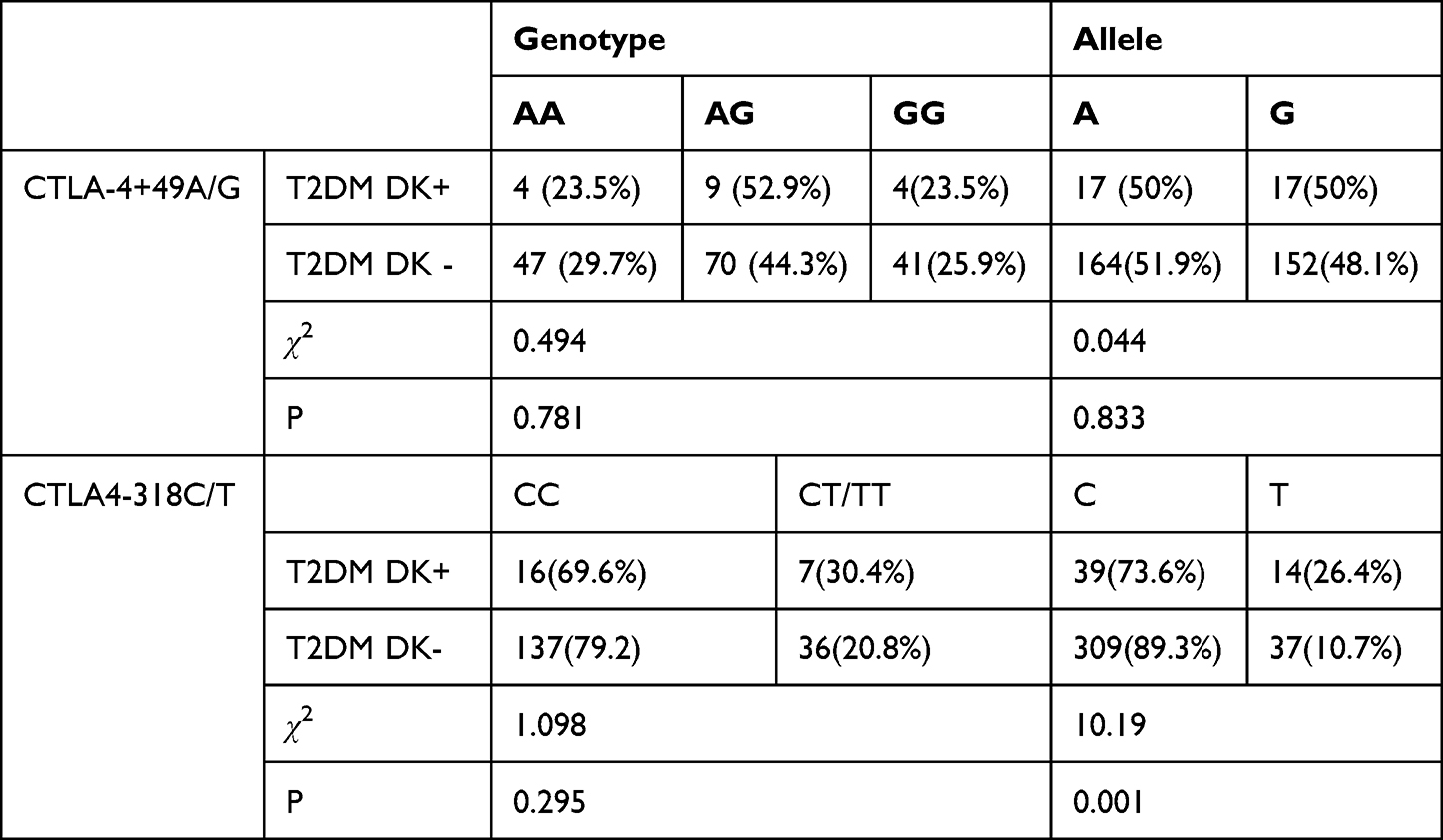 |
Table 6 Distribution of the CTLA-4 Polymorphisms in Type 2 Diabetes Patients with DK+ and DK |
CTLA-4 Polymorphisms in T2DM Patients with or without Diabetic Nephropathy
Table 7 summarizes the frequency distribution of CTLA-4-318C/T and +49A/G genotypes and alleles of T2DM patients with (DN+) or without (DN-) diabetic nephropathy. It turned out that CTLA-4+49A/G and −318C/T genotypes both showed no significant differences in terms of genotype and allele distribution frequency between the DN+ and DN- groups (P>0.05).
 |
Table 7 Distribution of the CTLA-4 Polymorphisms in Type 2 Diabetes Patients with DN+ and DN |
Association of Antibody Positivity Rate with CTLA-4 Polymorphisms in T2DM Patients
Table 8 summarizes the frequency distribution of CTLA-4-318C/T and +49A/G and genotypes and alleles of T2DM patients with (Ab+) or without (Ab-) antibody positivity. Our analysis suggested that CTLA-4+49A/G and −318C/T genotypes both showed no significant differences in terms of SNPs distribution frequency between the Ab+ and Ab- groups (P>0.05).
 |
Table 8 Distribution of the CTLA-4 Polymorphisms in Type 2 Diabetes Patients with Ab+ and Ab |
Discussion
Recent studies have found that there are many important risk loci that are closely associated with the development of diabetes, among which CTLA-4 has been identified as a susceptibility gene for T1DM.8,9 Studies correlating CTLA-4 polymorphisms with T1DM have been carried out among different populations in several countries. It has been shown that the occurrence of T1DM in Korean, Portuguese, Chilean, and Azerbaijani people is not significantly associated with CTLA-4+49 A/G gene polymorphism;14–16 whereas in European, Chinese, African, Iranian, Croatian, Polish, Finnish, Belgian, Estonian, Tunisian, and Egyptian people there is a significant association, where the GG genotype of the CTLA-4+49 locus is a risk factor for T1DM.17,18 In contrast, there are contradictory studies in Japan, with some studies showing that CTLA-4 exon 1+49 GG genotype is closely associated with type 1 diabetes and others showing no association between the two.19 The present study showed that the AA genotype of the CTLA-4 exon 1+49 locus was strongly associated with the development of T2DM, but not with T1DM, which is inconsistent with the previous findings. This discrepancy may stem from the relatively small patient number and hence suboptimal representation of T1DM patient population. However, it was found that DM patients with the G allele at the CTLA-4+49 locus were more likely to develop T1DM,18 while those with the A allele were more likely to develop T2DM.20 No association was found between the CTLA-4+49A/G polymorphism and DK and DN in the study.
The CTLA-4-318C/T gene polymorphism and T1DM have been relatively rarely studied. In our study, no correlation was found between CTLA-4-318C/T gene polymorphism and T1DM. The CTLA-4-318C/T gene polymorphism was not found to correlate with diabetic nephropathy in T2DM neither in the study. However, T2DM patients with a T allele at CTLA-4 promoter −318 were found to be predisposed to DK. This could potentially provide a new predictive basis for ketosis-prone diabetes (KPD).
Approximately 10% of the patients with T2DM have autoantibodies in their body fluids at the time of diagnosis, particularly GAD65,21 and these patients are insulin resistant, with gradually decreasing islet function as the disease progresses and eventually requiring insulin therapy. The presence of islet-specific antibodies in latent autoimmune diabetes in adults (LADA) is similar to that of T1DM, but its symptoms are similar to those of T2DM.22 Some studies have shown that the GG or AG type of CTLA-4+49 is a susceptibility gene for LADA and can be used to diagnose and differentiate LADA from T2DM.23 No relevant comparison was made in this study because the number of LADA patients was too small, which is a limitation of our study. Similarly, our study included a relatively small number of patients with T1DM, which could limit the rigor of comparison among patients with different genotypes. Further, more comprehensive analysis of the CTLA-4 polymorphism in patients with different diseases using Hardy–Weinberg equilibrium test and multivariate logistic regression analysis could likely enhance our understanding of the pathogenetic role of the CTLA-4 polymorphism. At last, there has also been no study on the frequencies of the polymorphisms among Chinese Han population, therefore the representation of the study sample pool to the general population should also be verified in the future once relevant data become available.
Conclusion
Using PCR-RFLP analysis, we showed that CTLA4 gene polymorphism is closely linked to the pathogenesis of diabetes. The frequency distribution of CTLA4+49A/G genotype and alleles between T2DM patients and normal controls were statistically significant. T2DM patients carrying the T allele at the CTLA4-318 C/T locus are more predisposed to DK. In terms of CTLA4-318C/T, C and T allele frequencies were significantly different between the two groups, and T allele frequencies were higher in DK+ patients than in DK- patients in T2DM. Further studies are warranted to investigate how genetic and environmental factors affect the pathogenesis of DM to provide a basis for early diagnosis, genotyping and treatment of DM.
Funding
The study was supported by the Overseas Training Project of the Education Department of Liaoning Province, China (2019GJWZC03); Science and Technology Research Project of the Education Department of Liaoning Province, China (LK201654).
Disclosure
The authors declare that they have no competing interests.
References
1. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14. doi:10.1016/j.diabres.2009.10.007
2. Cheng TO. Diabetes epidemic in China and its economic impact. Int J Cardiol. 2011;149:1–3. doi:10.1016/j.ijcard.2011.01.009
3. Ozougwu J, Obimba K, Belonwu C, Unakalamba C. The pathogenesis and pathophysiology of type 1 and type 2 diabetes mellitus. J Physiol Pathoph. 2013;4:46–57. doi:10.5897/JPAP2013.0001
4. Xie W, Burke B. Nuclear lamins and diabetes mellitus. STEMedicine. 2020;2:e73. doi:10.37175/stemedicine.v2i5.73
5. Eizirik DL, Pasquali L, Cnop M. Pancreatic β-cells in type 1 and type 2 diabetes mellitus: different pathways to failure. Nat Rev Endocrinol. 2020;16:349–362. doi:10.1038/s41574-020-0355-7
6. Aylward A, Chiou J, Okino M-L, Kadakia N, Gaulton KJ. Shared genetic risk contributes to type 1 and type 2 diabetes etiology. Hum Mol Genet. 2018. doi:10.1093/hmg/ddy314
7. Dajani R, Li J, Wei Z, et al. Genome-wide association study identifies novel type II diabetes risk loci in Jordan subpopulations. PeerJ. 2017;5:e3618. doi:10.7717/peerj.3618
8. Borysewicz-Sańczyk H, Sawicka B, Wawrusiewicz-Kurylonek N, et al. Genetic Association Study of IL2RA, IFIH1, and CTLA-4 polymorphisms with autoimmune thyroid diseases and type 1 diabetes. Front Pediatr. 2020;8. doi:10.3389/fped.2020.00481
9. Chikuma S. CTLA-4, an essential immune-checkpoint for T-cell activation. In: Emerging Concepts Targeting Immune Checkpoints in Cancer and Autoimmunity; 2017:99–126.
10. Hosseini A, Gharibi T, Marofi F, Babaloo Z, Baradaran B. CTLA-4: from mechanism to autoimmune therapy. Int Immunopharmacol. 2020;80:106221. doi:10.1016/j.intimp.2020.106221
11. Mäurer M, Loserth S, Kolb-Mäurer A, et al. A polymorphism in the human cytotoxic T-lymphocyte antigen 4 (CTLA4) gene (exon 1+ 49) alters T-cell activation. Immunogenetics. 2002;54:1–8. doi:10.1007/s00251-002-0429-9
12. Gunavathy N, Asirvatham A, Chitra A, Jayalakshmi M. Association of CTLA-4 and CD28 gene polymorphisms with type 1 diabetes in South Indian population. Immunol Invest. 2019;48:659–671. doi:10.1080/08820139.2019.1590395
13. Gorgi Y, Sfar I, Abdallah TB, et al. Ctla-4 exon 1 (+ 49) and promoter (− 318) gene polymorphisms in kidney transplantation. Transplant Proc. 2006;38:2303–2305. doi:10.1016/j.transproceed.2006.06.132
14. Lee YH, Choi SJ, Ji JD, Song GG. No association of polymorphisms of the CTLA-4 exon 1 (+ 49) and promoter (−318) genes with rheumatoid arthritis in the Korean population. Scand J Rheumatol. 2002;31:266–270. doi:10.1080/030097402760375142
15. Angel B, Balic I, Santos JL, Codner E, Carrasco E, Pérez-Bravo F. Associations of the CTLA-4 polymorphisms with type 1 diabetes in a Chilean population: case-parent design. Diabetes Res Clin Pract. 2009;85:e34–e6. doi:10.1016/j.diabres.2009.05.019
16. Almasi S, Aliparasti MR, Aliasgarzadeh A, et al. Investigation of CTLA-4-318C/T gene polymorphism in cases with type 1 diabetes of Azerbaijan, Northwest Iran. Immunol Lett. 2015;166:134–139. doi:10.1016/j.imlet.2015.05.021
17. Mojtahedi Z, Omrani GR, Doroudchi M, Ghaderi A. CTLA-4+ 49 A/G polymorphism is associated with predisposition to type 1 diabetes in Iranians. Diabetes Res Clin Pract. 2005;68:111–116. doi:10.1016/j.diabres.2004.08.008
18. Mosaad YM, Elsharkawy AA, El-Deek BS. Association of CTLA-4 (+ 49A/G) gene polymorphism with type 1 diabetes mellitus in Egyptian children. Immunol Invest. 2012;41:28–37. doi:10.3109/08820139.2011.579215
19. Mochizuki M, Amemiya S, Kobayashi K, et al. Association of the CTLA-4 gene 49 A/G polymorphism with type 1 diabetes and autoimmune thyroid disease in Japanese children. Diabetes Care. 2003;26:843–847. doi:10.2337/diacare.26.3.843
20. Haller K, Kisand K, Nemvalts V, Laine AP, Ilonen J, Type UR. 1 diabetes is insulin− 2221 MspI and CTLA‐4+ 49 A/G polymorphism dependent. Eur J Clin Invest. 2004;34:543–548. doi:10.1111/j.1365-2362.2004.01385.x
21. Hinke SA. Diamyd, an alum-formulated recombinant human GAD65 for diabetes and the prevention of autoimmune diabetes. Curr Opin Mol Ther. 2008;10:1–10.
22. Mollo A, Hernandez M, Marsal JR, et al. Latent autoimmune diabetes in adults is perched between type 1 and type 2: evidence from adults in one region of Spain. Diabetes Metab Res Rev. 2013;29:446–451. doi:10.1002/dmrr.2411
23. Dong F, Yang G, Pan H-W, et al. The association of PTPN22 rs2476601 polymorphism and CTLA-4 rs231775 polymorphism with LADA risks: a systematic review and meta-analysis. Acta Diabetol. 2014;51:691–703. doi:10.1007/s00592-014-0613-z
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Polymorphisms in Antioxidant Enzyme-Encoding Genes with Diabetic Nephropathy in a Group of Saudi Arabian Patients with Type II Diabetes Mellitus
Albeladi FI, Mostafa MM, Zayed MA, Atta H
International Journal of General Medicine 2022, 15:5919-5928
Published Date: 1 July 2022
Association Between ALDH2 Polymorphisms and the Risk of Diabetes Mellitus in Hypertensive Patients
Zeng M, Liu Y, Xie Y
International Journal of General Medicine 2023, 16:5719-5727
Published Date: 6 December 2023
Non-Invasive Diagnosis and Monitoring of Diabetic Nephropathy: Assessment of Renal Function and Fibrosis by Diffusion Kurtosis Imaging
Yuan JL, Hu LA, Wang XY, Shi ZY, Chen T, Huang XZ, Wu Y, Cai QJ, Yang ZX, Chen XY, Yuan L, Zhang Y
International Journal of General Medicine 2025, 18:4011-4026
Published Date: 21 July 2025