Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Association of ADIPOQ Single-Nucleotide Polymorphisms with the Two Clinical Phenotypes Type 2 Diabetes Mellitus and Metabolic Syndrome in a Kinh Vietnamese Population
Authors Truong S, Tran NQ ![]() , Ma PT, Hoang CK
, Ma PT, Hoang CK ![]() , Le BH, Dinh T, Tran L, Tran TV
, Le BH, Dinh T, Tran L, Tran TV ![]() , Gia Le LH, Vu HA, Mai TP
, Gia Le LH, Vu HA, Mai TP ![]() , Do MD
, Do MD ![]()
Received 12 November 2021
Accepted for publication 11 January 2022
Published 3 February 2022 Volume 2022:15 Pages 307—319
DOI https://doi.org/10.2147/DMSO.S347830
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Steven Truong,1,* Nam Quang Tran,2,3,* Phat Tung Ma,2,3 Chi Khanh Hoang,3 Bao Hoang Le,3 Thang Dinh,3 Luong Tran,3 Thang Viet Tran,2,3 Linh Hoang Gia Le,4 Hoang Anh Vu,4 Thao Phuong Mai,5 Minh Duc Do4
1Department of Biological Engineering, Massachusetts Institute of Technology, Cambridge, MA, USA; 2Department of Endocrinology, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 3Department of Endocrinology, University Medical Center, Ho Chi Minh City, Vietnam; 4Center for Molecular Biomedicine, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 5Department of Physiology-Pathophysiology-Immunology, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam
*These authors contributed equally to this work
Correspondence: Minh Duc Do
Center for Molecular Biomedicine, University of Medicine and Pharmacy at Ho Chi Minh City, 217 Hong Bang, District 5, Ho Chi Minh City, 700000, Vietnam
, Tel +84 932999989
, Email [email protected]
Purpose: Genetic factors play an important role in the development of type 2 diabetes mellitus (T2DM) and metabolic syndrome (MetS). However, few genetic association studies related to these disorders have been performed with Vietnamese subjects. In this study, the potential associations of ADIPOQ single nucleotide polymorphisms (SNPs) with T2DM and MetS in a Kinh Vietnamese population were investigated.
Patients and Methods: A study with 768 subjects was conducted to examine the associations of four ADIPOQ SNPs (rs266729, rs1501299, rs3774261, and rs822393) primarily with T2DM and secondarily with MetS. The TaqMan SNP genotyping assay was used to determine genotypes from subjects’ DNA samples.
Results: After statistical adjustment for age, sex, and body mass index, the ADIPOQ SNP rs266729 was found to be associated with increased risk of T2DM under multiple inheritance models: codominant (OR = 2.30, 95% CI = 1.16– 4.58), recessive (OR = 2.17, 95% CI = 1.11– 4.26), and log-additive (OR = 1.32, 95% CI = 1.02– 1.70). However, rs1501299, rs3774261, and rs822393 were not associated with risk for T2DM. Additionally, rs266729, rs3774261, and rs822393 were statistically associated with MetS, while rs1501299 was not. Haplotype analysis showed a strong linkage disequilibrium between the SNP pairs rs266729/rs822393 and rs1501299/rs3774261, and the haplotype rs266729(G)/rs822393(T) was not statistically associated with MetS.
Conclusion: The results show that rs266729 is a lead candidate SNP associated with increased risk of developing T2DM and MetS in a Kinh Vietnamese population, while rs3774261 is associated with MetS only. Further functional characterization is needed to uncover the mechanism underlying the potential genotype–phenotype associations.
Keywords: genetic association, Kinh Vietnamese, metabolic syndrome, type 2 diabetes mellitus
Corrigendum for this paper has been published
Introduction
Metabolic syndrome (MetS) is characterized by a cluster of symptoms comprising of glucose intolerance, dyslipidemia, hypertension, and central obesity. Although definitions of MetS differ, it generally relates to insulin resistance or hyperinsulinemia.1–4 Diabetes is a chronic metabolic disorder characterized by elevated levels of blood glucose, also known as hyperglycemia. Type 2 diabetes mellitus (T2DM) - with the distinct etiologies of insulin deficiency, insulin resistance, or both - accounts for approximately 90% of all cases of diabetes.5,6 T2DM and MetS are common disorders that share a similar insulin resistance pathophysiology. Additionally, the two conditions are often the result of obesity and sedentary lifestyle. Several studies have shown that subjects with MetS are highly likely to develop type 2 diabetes.7,8 In tandem, T2DM and MetS are significant healthcare burdens contributing to morbidity and mortality globally, mainly through cardiovascular complications.9–11
Although environmental factors play an important part in the pathogenesis of these disorders, Asian individuals have been shown to have significant genetic predispositions to T2DM and MetS.12,13 However, to date, no studies have examined the Vietnamese population, which totals more than 100 million inhabitants. This apparent lack of representation in genome research exacerbates health disparities,14–16 underscoring the value of studying a Vietnamese sample population.
The ADIPOQ gene encodes adiponectin, an adipokine that regulates metabolic processes. Overall, serum adiponectin concentration correlates with heightened insulin sensitivity and improved islet β‐cell function.17–20 Conversely, low levels of adiponectin is associated with the development of MetS and T2DM.21,22 Therefore, this study examined the potential associations of four single-nucleotide polymorphisms (SNPs) located in the ADIPOQ gene (rs266729, rs1501299, rs3774261, and rs822393) with T2DM and MetS in a Kinh Vietnamese population. While ADIPOQ SNPs have been reported to be associated with MetS and T2DM in South Asian, East Asian, and Caucasian populations,23–25 this is the first study to investigate this association within the context of a Kinh Vietnamese population. The ADIPOQ SNPs in this study were chosen on the basis that previous studies have shown varying associations with T2DM and MetS, particularly among ethnically different populations. For example, studies have suggested that the ADIPOQ SNP rs266729 is associated with T2DM and MetS in East Asian populations and could be a functional SNP; meta-analysis supports this theory.26–28 As rs266729 is located in the SP1-binding site of the ADIPOQ gene, it has been hypothesized that the G allele of rs266729 disrupts SP1-binding and consequently yields lower adiponectin expression in the body.29,30 This hypothesis is supported by the work of Smetnev et al, who showed that in a population of Russian individuals, the G/G genotype of rs266729 results in lower levels of serum adiponectin compared to the C/C and C/G genotypes.31 However, two different studies performed on European populations did not find rs266729 to be associated with T2DM.32,33
Additionally, 21 relevant studies of the ADIPOQ SNP rs1501299 have presented conflicting data on its association with T2DM; a meta-analysis by Han et al concluded that rs1501299 is not associated with T2DM risk, but this study did not consider inter-ethnic differences.26 Similarly, rs3774261 confers differing risk of T2DM between ethnicities; it is associated with T2DM in Han Chinese and South Indian populations but not in white and black American populations.34–36 Inter-ethnic differences are also evident with rs822393, which was shown by Ramya et al to confer a two-fold greater risk of T2DM in a population of South Indian individuals, while Yao et al found no such association in a population of ethnic Han northeast Chinese individuals.34,35
These discrepancies in T2DM and MetS risk from the ADIPOQ SNPs rs266729, rs1501299, rs3774261, and rs822393 point to potential inter-ethnic differences in genetic predisposition to the diseases. Thus, it is imperative to study the association of these SNPs with T2DM and MetS in a previously unstudied population, the Kinh Vietnamese.
Materials and Methods
Subject Recruitment
A total of 768 subjects who were all self-identified as Kinh Vietnamese were randomly recruited for this study. The study’s protocol was approved by the institutional review board of the University of Medicine and Pharmacy at Ho Chi Minh City (HEC/IRB number 350/HĐĐĐ-ĐHYD), and informed written consent was obtained from all study subjects. T2DM subjects were selected if they had history of T2DM or were newly diagnosed with T2DM based on the American Diabetes Association 2020 criteria.5 Among T2DM patients, further MetS diagnosis was made using the criteria provided by the Executive Summary of The Third Report of The National Cholesterol Education Program Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults.2 Patients were diagnosed with MetS when they had at least three among five following criteria: waist circumference over 40 inches (101 cm) (for men) or 35 inches (89 cm) (for women), blood pressure over 130/85 mmHg or currently on hypertension treatment, fasting triglyceride levels over 150 mg/dl or currently on triglyceride-lowering treatment, fasting high-density lipoprotein (HDL) cholesterol levels less than 40 mg/dl (for men) or 50 mg/dl (for women), and fasting blood sugar (FPG) over 100 mg/dl or currently on diabetes treatment.
Exclusion criteria for T2DM cases were the following: (i) type 1 diabetes, (ii) liver dysfunction, (iii) use of substances affecting plasma glucose levels, and (iv) endocrine diseases that heighten plasma glucose levels. Control subjects were recruited among regular health checkup visitors to the hospital with the following exclusion criteria: (i) previous history of diabetes of any type, (ii) use of substances that affect plasma glucose levels, (iii) pregnancy, (iv) cancer, and (v) any other diseases which affect blood glucose levels. After selection, 376 subjects with T2DM were recruited and, of these, 239 participants fulfilled the criteria for MetS.
Clinical and Laboratory Measurements
All subjects underwent a detailed physical examination and answered a survey soliciting information about their health as it pertained to the study. Anthropometric measurements included weight, height, waist circumference, hip circumference, systolic and diastolic blood pressure. Demographic information included age, sex, and duration of T2DM since diagnosis (for T2DM cases). Medication information, such as antihypertensive, antidiabetic, and lipid-lowering agents, was also documented.
Fasting (minimum 8 hours) blood samples were collected. Biochemical analyses were performed immediately using the Beckman Coulter AU2700 Chemistry Analyzer for FPG, HbA1c, total serum cholesterol, HDL cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides, and creatinine levels.
Genotyping
The remaining blood samples were stored at −20°C until extracted for genomic DNA using the QiAmp DNA Blood Mini Kit (QIAGEN, Hilden, Germany). SNP genotyping was performed using the TaqMan SNP genotyping assay (Thermo Fisher Scientific, Waltham, MA, USA) consisting proper forward, reverse primers, and fluorescently named MGB™ probes (FAM and VIC) to identify the alleles. PCR reactions were carried out using the 7900HT Fast Real-Time PCR System in separate 384-wells (Thermo Fisher Scientific, Waltham, MA, USA). PCR reactions were performed according to manufacturer’s protocols in a total volume of 25 μL (12.5 μL of TaqMan universal PCR Master Mix, 0.625 μL of TaqMan assay, and 6.875 μL of milli-Q water and 5 μL of DNA) for each SNP (rs266729, rs1501299, rs3774261, and rs822393). The thermal cycles consisted of 63°C for 1 min and 95°C for 3 min, followed by 40 cycles at 95°C for 15 sec and 63°C for 40 sec. Sample genotyping was identified based on the fluorescence signal detected.
Statistical Analyses
For continuous variables, the distributions for baseline clinical measurements for case and control groups were compared using Student’s independent two-tailed t-test. The use of the statistical test was based on the data’s normality, as assessed by visual inspection and the Shapiro Wilk test for normality. The sex distribution in case and control groups was assessed using the Chi-Square test for independence. The ANOVA one-way test was used to investigate the differences of baseline clinical characteristics between genotypes for rs266729 and rs3774261.
Genotype frequencies were tested for Hardy-Weinberg equilibrium (HWE) using the goodness-of-fit χ2 test. The web tool SNPstats was used to test for the association of the ADIPOQ SNPs rs266729, rs1501299, rs3774261 and rs822393 to T2DM and MetS under different inheritance models: codominant, dominant, recessive and log-additive.37 Age, sex, and body mass index (BMI) were used as covariates for statistical adjustment in the models. Odds ratios (OR) were calculated with 95% confidence interval (CI). Haplotype frequency, linkage disequilibrium for each pair of alleles and the association between haplotypes and T2DM/MetS were analyzed using the Python SciKit-Allel package.38 Two-sided P-values <0.05 were considered statistically significant.
Results
Clinical and Biochemical Characteristics of Study Subjects
Baseline demographic and clinical measurements for T2DM, MetS, and control subjects are presented in Table 1. For T2DM, statistically significant differences were found between the T2DM and T2DM-control group for age, BMI, waist circumference, waist-to-hip ratio (WHR), HbA1c, FPG, systolic blood pressure (SBP), triglyceride levels, total cholesterol, HDL cholesterol, and LDL cholesterol (P<0.05). On the other hand, there were no statistically significant differences between the two groups for diastolic blood pressure (DBP), serum creatinine levels, and sex.
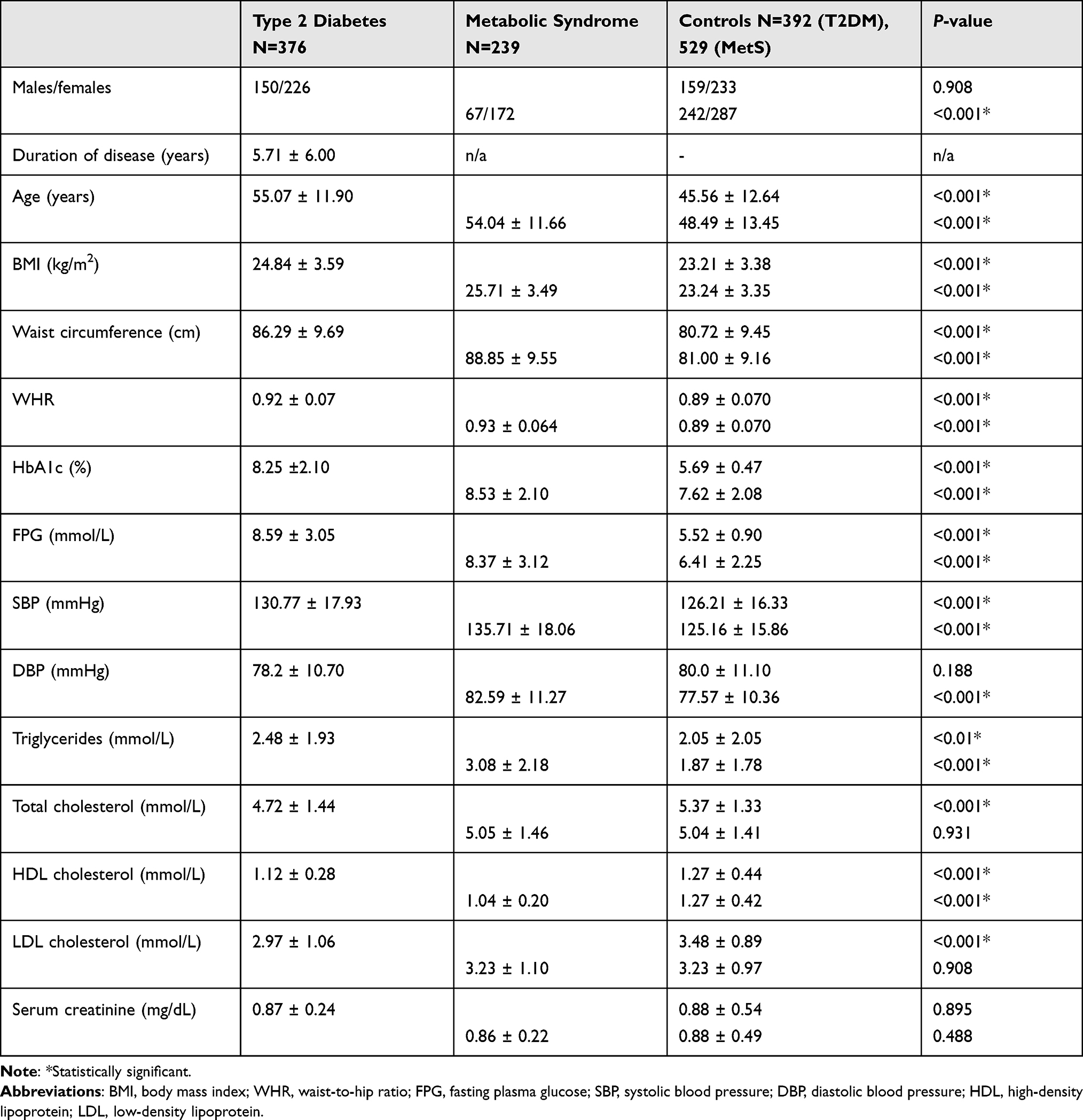 |
Table 1 Baseline Clinical and Biochemical Characteristics of the Studied Population |
For MetS, statistically significant differences were found between the MetS and MetS-control group for age, BMI, WHR, HbA1c, FPG, SBP, DBP, triglyceride levels, and HDL cholesterol. However, no statistically significant differences were found for total cholesterol, LDL cholesterol, and serum creatinine.
Association of ADIPOQ SNPs with Type 2 Diabetes Mellitus
Genotype distributions for the SNPs rs266729, rs1501299, rs3774261, and rs822393 were all under HWE in the studied population, which includes T2DM, T2DM-control, MetS, and MetS-control groups (all P-values > 0.05) (Supplementary Table 1). Multiple inheritance models were used to assess statistically significant associations between genotypes and T2DM status: codominant (Supplementary Table 2), dominant (Supplementary Table 3), recessive (Supplementary Table 4), and log-additive (Supplementary Table 5). ORs were calculated with 95% confidence intervals (CI). To account for covariate effects, statistics were adjusted for age, sex, and BMI.
Only the SNP rs266729 showed a statistically significant association between genotypes and T2DM. The SNP showed statistically significant associations in three inheritance models: codominant (OR = 2.30, 95% CI = 1.16–4.58, P = 0.049), recessive (OR = 2.17, 95% CI = 1.11–4.26, P = 0.022), and log-additive (OR = 1.32, 95% CI = 1.02–1.70, P = 0.034) (Table 2). However, in the dominant inheritance model, the G allele for rs266729 did not conferred risk of T2DM (OR = 1.27, 95% CI = 0.93–1.74, P = 0.13). On the other hand, rs1501299, rs3774261 and rs822393 did not show statistically significant associations with T2DM in all the inheritance models (Supplementary Tables 2–5).
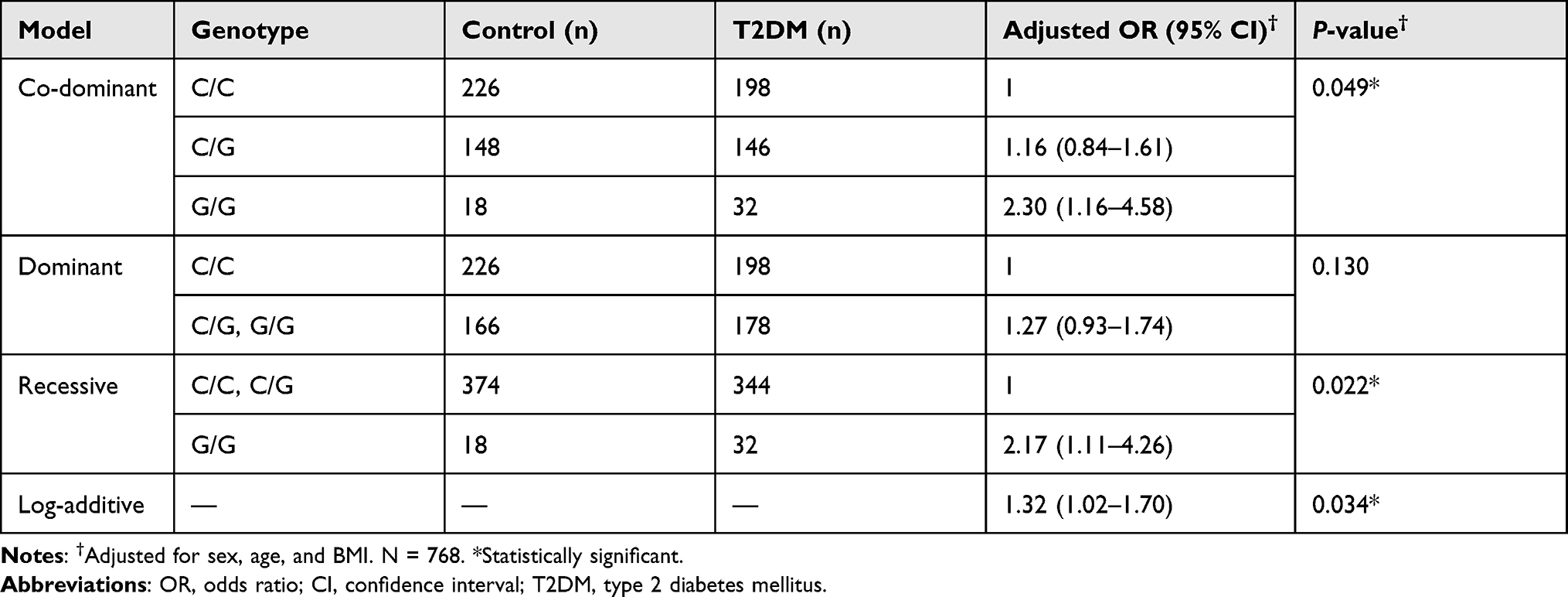 |
Table 2 The Association of rs266729 with T2DM |
Association of rs3774261 with MetS
Because ADIPOQ regulates metabolism and lipid levels, the potential associations between the four ADIPOQ SNPs and MetS were also investigated. Using the same methodology as described above, statistically significant associations of rs3774261 with MetS were detected under different inheritance models (Table 3). On the other hand, rs266729 and rs822393 were found to be associated with MetS under the recessive inheritance model (Table 4 and Supplementary Table 8). However, rs1501299 did not have statistically significant associations with MetS under any of the inheritance models (Supplementary Tables 6–9).
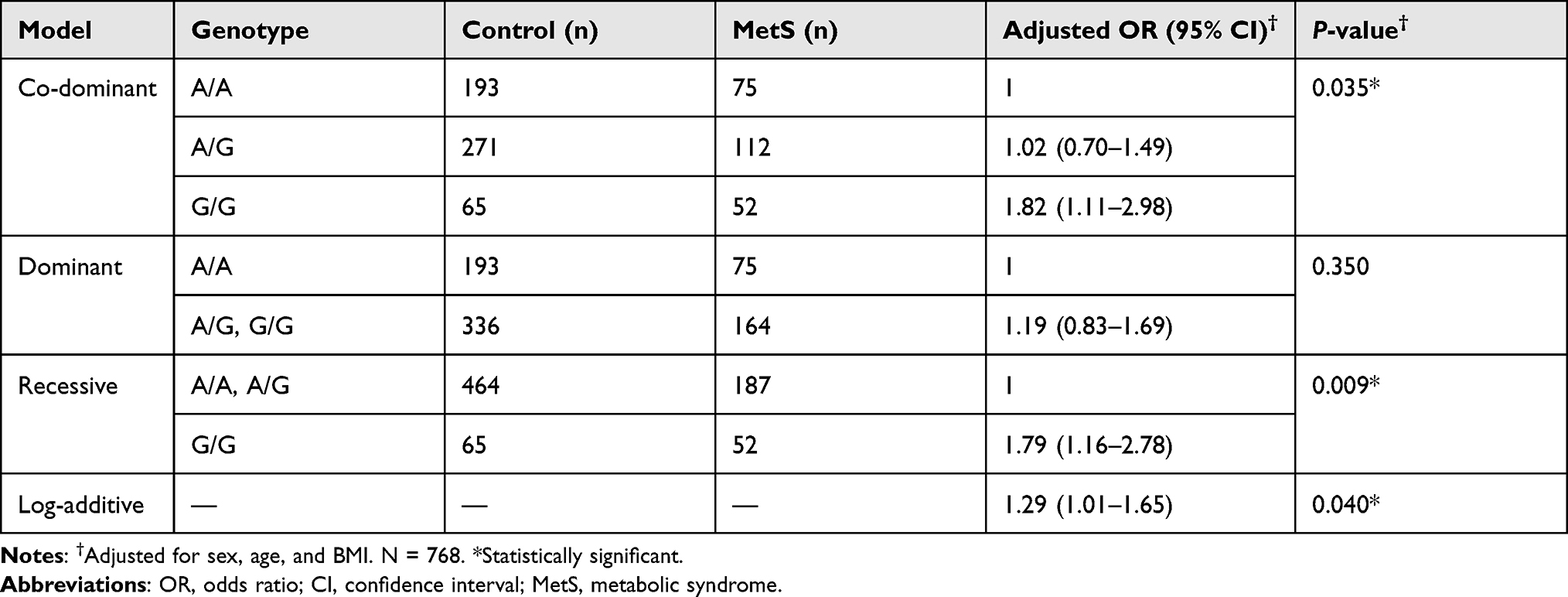 |
Table 3 The Association of rs3774261 with MetS |
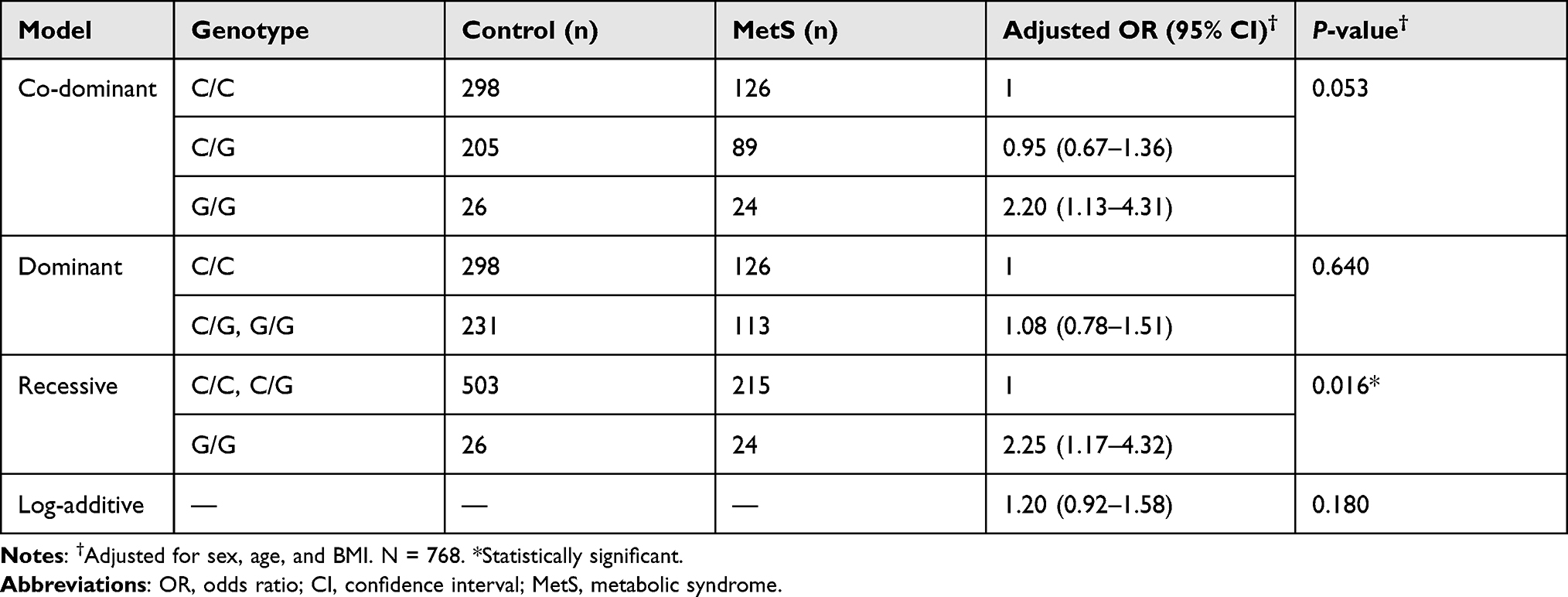 |
Table 4 The Association of rs266729 with MetS |
Haplotype Analysis
Among the four SNPs examined in this study, strong linkage disequilibrium between the SNP pairs rs266729/rs822393 and rs1501299/rs3774261 was observed (Figure 1). Due to the borderline statistical associations between rs266729 and rs822393 with MetS, the haplotype rs266729/rs3774261 was further examined for association with MetS. However, the rs266729(G)/rs822393(T) haplotype was not found to be statistically associated with MetS (Table 5).
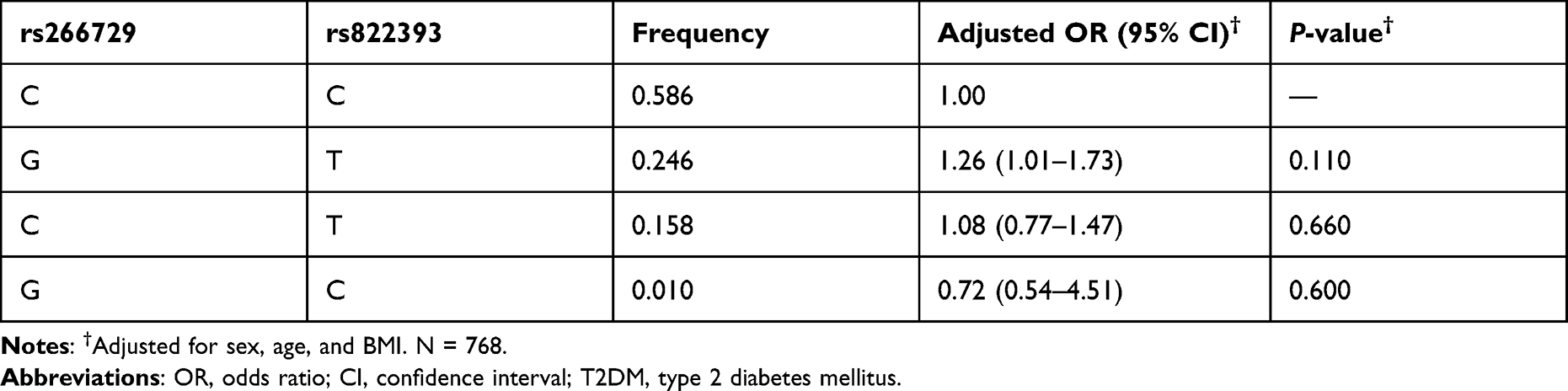 |
Table 5 The Association of Haplotype rs266729/rs822393 with MetS |
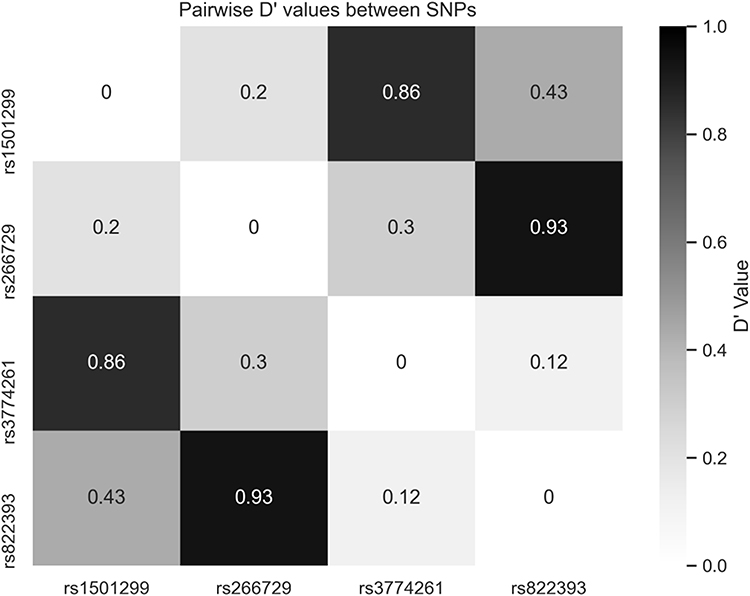 |
Figure 1 Linkage disequilibrium between allele pairs of rs266729, rs1501299, rs3774261, and rs822393. |
Association of rs266729 and rs3774261 with Subjects’ Characteristics
As rs266729 was associated with T2DM, and rs3774261 was associated with MetS, the rs266729 genotypes (CC, CG, GG) and rs3774261 genotypes (GG, GA, AA) were further analyzed with respect to subjects’ clinical and biochemical characteristics. In T2DM and MetS case and respective control subjects, there were no statistical differences observed in BMI, WHR, HbA1c, FPG, or triglyceride levels between rs266729 CC, CG, GG genotypes (Table 6) and rs3774261 GG, GA, AA genotypes (Table 7).
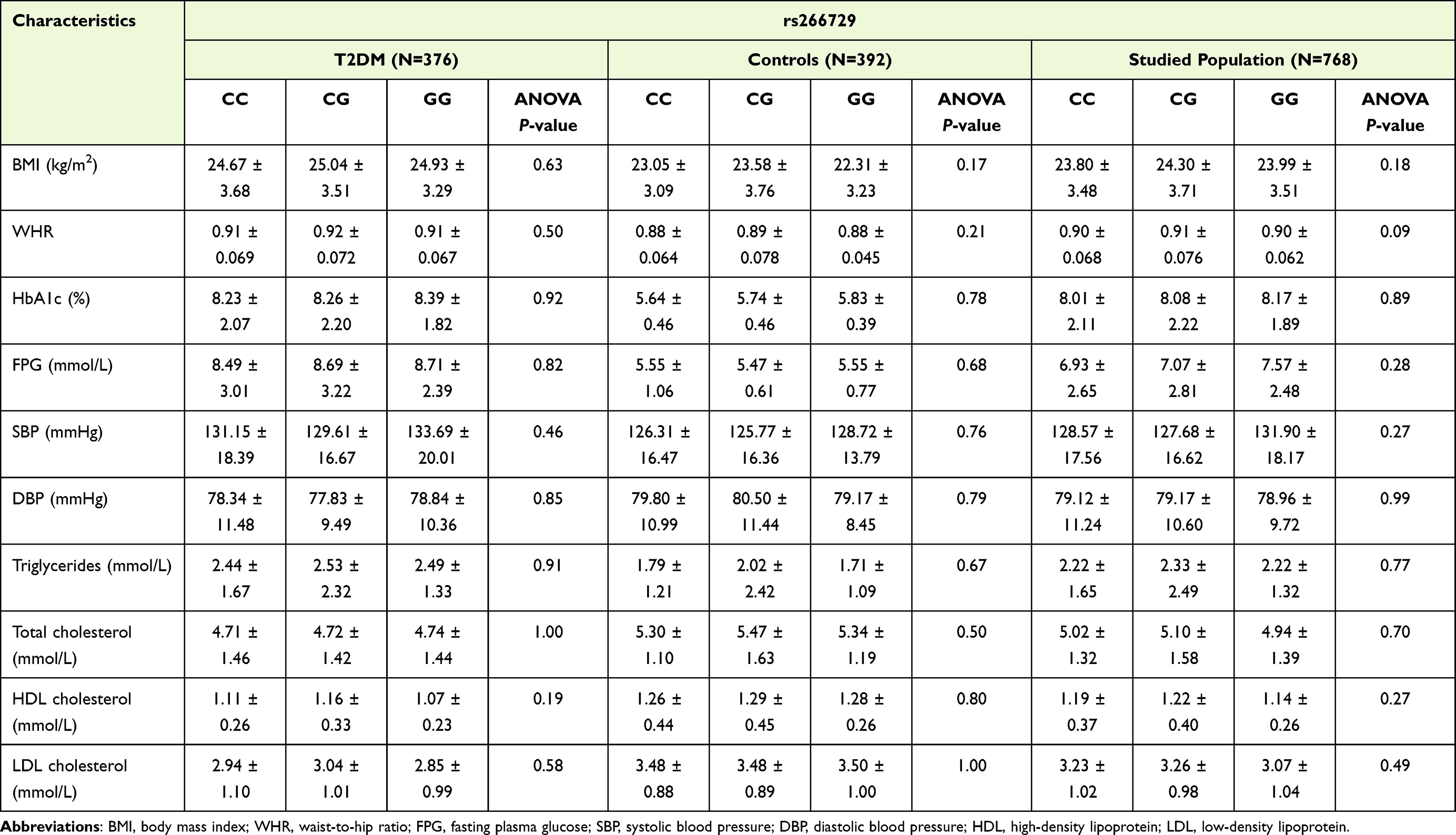 |
Table 6 The Association of rs266729 with Clinical and Biochemical Characteristics in T2DM and Control Subjects |
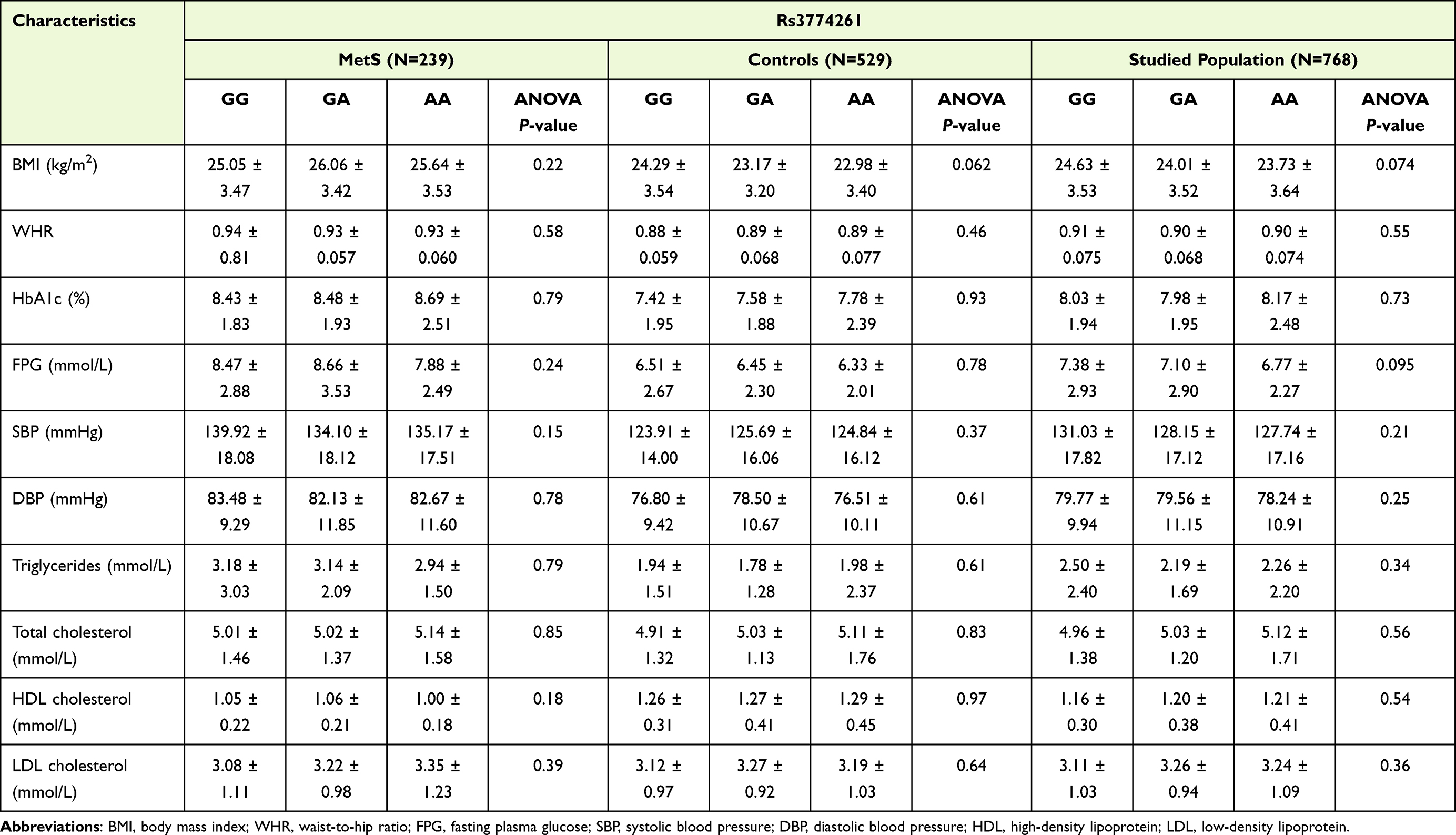 |
Table 7 The Association of rs3774261 with Clinical and Biochemical Characteristics in MetS and Control Subjects |
Discussion
T2DM and MetS are polygenic disorders that present heavy healthcare burdens worldwide. Multiple risk loci of these disorders have been identified through genome-wide association studies.39,40 Among contributing genetic factors, the ADIPOQ gene has been reported to be highly associated with T2DM, MetS, and obesity in various study populations.25,41–43
The results of this study show strong associations between the promoter variants rs266729 to T2DM and rs3774261 to MetS. This finding corroborates with the well-documented effect of rs266729 on T2DM risk in East Asian populations.26 The finding that rs3774261 is associated with MetS but not T2DM is quite a novel finding, with only one previous study reporting this association in a population of elderly Han Chinese.44 This result emphasizes the importance of investigating previously unstudied populations.
Another interesting observation is that rs1501299 was not found to be associated with either T2DM or MetS in the studied Kinh Vietnamese population. Contrary to this observation, this variant has been found to have close associations with the obesity and T2DM phenotypes in several studies of African, Asian, and Caucasian populations.45–48 Notably, rs1501299 showed a contradicting protective role against obesity in a Tunisian population.49 These findings once again highlight the important potential effects of ethnicity on genetic studies, emphasizing the unique genetic characteristics of the Kinh Vietnamese in terms of genetic variation and disease association.50–53
It has been shown that adiponectin concentration is highly heritable and can be regulated by ADIPOQ genetic variants.54 The associations between ADIPOQ SNPs and major adverse phenotypes, such as diabetes, obesity, MetS, and even coronary heart disease, are considered to be the result of hypoadiponectinemia, given the important role of adiponectin in regulating metabolism and anti-inflammatory functions. Apart from the disruption of SP1-binding in the promoter region by rs266729, the association of rs3774261 with hypoadiponectinemia is still not well understood. Interestingly, this variant has been shown to be associated with eating behavior and can affect the results of nutritional intervention.55,56 Additionally, the lack of linkage disequilibrium between the SNP pairs rs266729 and rs3774261 suggests that these two SNPs may regulate the adiponectin level by independent mechanisms.
On the other hand, the pair rs266729 and rs822393 was found to be in strong linkage disequilibrium. In this study, no association between the rs266729(G)/rs822393(T) haplotype and MetS was observed. However, both rs266729 and rs822393 have been shown to be significantly associated with hypoadiponectinemia in the literature.36 Altogether, the data suggest that these SNPs may regulate adiponectin levels by the same mechanism, and the combination of rs266729(G)/rs822393(T) may have compounding effects on serum adiponectin levels in the studied population. The comparison of clinical and biochemical parameters between rs266729 genotypes in T2DM and rs3774261 in MetS group showed no statistical differences. This observation is consistent with previous studies in which ADIPOQ SNPs were not statistically associated with biochemical parameters except for insulin concentration and homeostasis model assessment index for insulin resistance.57,58
Nevertheless, the present study carries several limitations. First, the adiponectin level was not measured due to the lack of reliable facilities; hence, the associations between the SNPs and adiponectin levels were not elucidated. Second, the small sample size may affect the study’s statistical power. However, future meta-analyses and studies building on the present study will help reconcile the numerous inconsistent findings in the literature for the ADIPOQ SNPs studied.
Conclusions
To our knowledge, this is the first study of its kind performed with a population of Kinh Vietnamese individuals, underscoring its importance in the wider context of genomics research. Nonetheless, additional replication or further expanded studies with larger sample sizes are required to form stronger conclusions. Future functional studies are also needed to understand the biology underlying these potential genotype–phenotype associations. Also, going forward, additional variants should be investigated to pinpoint the differences in genetic predispositions to T2DM and MetS between populations globally.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request: please contact [email protected].
Ethical Statement
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Ethics Committee of the University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam (FWA registered number: FWA00023448). Approval number: 350/HĐĐĐ-ĐHYD on May 26th, 2020 and informed consent was taken from all individual participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the MIT UROP Program’s Peter J. Eloranta Research Fellowship and the National Foundation for Science & Technology Development (NAFOSTED), grant number 108.01-2019.319. We thank Christine Mendonca and the Joslin Diabetes Center DRC Core for their assistance in genotyping samples.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–1645. doi:10.1161/CIRCULATIONAHA.109.192644
2. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA. 2001;285(19):2486–2497. doi:10.1001/jama.285.19.2486
3. Bloomgarden ZT. American Association of Clinical Endocrinologists (AACE) consensus conference on the insulin resistance syndrome: 25–26 August 2002, Washington, DC. Diabetes Care. 2003;26(4):1297–1303. doi:10.2337/diacare.26.4.1297
4. Alshammary AF, Alharbi KK, Alshehri NJ, Vennu V, Ali Khan I. Metabolic syndrome and coronary artery disease risk: a meta-analysis of observational studies. Int J Environ Res Public Health. 2021;18(4):1773. doi:10.3390/ijerph18041773
5. American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S14–S31. doi:10.2337/dc20-S002
6. Ali Khan I. Do second generation sequencing techniques identify documented genetic markers for neonatal diabetes mellitus? Heliyon. 2021;7(9):e07903. doi:10.1016/j.heliyon.2021.e07903
7. Huang PL. A comprehensive definition for metabolic syndrome. Dis Model Mech. 2009;2(5–6):231–237. doi:10.1242/dmm.001180
8. Garvey WT, Ryan DH, Henry R, et al. Prevention of type 2 diabetes in subjects with prediabetes and metabolic syndrome treated with phentermine and topiramate extended release. Diabetes Care. 2014;37(4):912–921. doi:10.2337/dc13-1518
9. Saklayen MG. The global epidemic of the metabolic syndrome. Curr Hypertens Rep. 2018;20(2):12. doi:10.1007/s11906-018-0812-z
10. Cho NH, Shaw J, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
11. Lin X, Xu Y, Pan X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10(1):14790. doi:10.1038/s41598-020-71908-9
12. Rhee EJ. Diabetes in Asians. Endocrinol Metab Seoul Korea. 2015;30(3):263–269. doi:10.3803/EnM.2015.30.3.263
13. Pang Y, Lv J, Kartsonaki C, et al. Metabolic risk factors, genetic predisposition, and risk of severe liver disease in Chinese: a prospective study of 0.5 million people. Am J Clin Nutr. 2021;114(2):496–504. doi:10.1093/ajcn/nqab099
14. Haga SB. Impact of limited population diversity of genome-wide association studies. Genet Med. 2010;12(2):81–84. doi:10.1097/GIM.0b013e3181ca2bbf
15. Landry LG, Ali N, Williams DR, Rehm HL, Bonham VL. Lack of diversity in genomic databases is a barrier to translating precision medicine research into practice. Health Aff Proj Hope. 2018;37(5):780–785. doi:10.1377/hlthaff.2017.1595
16. Wojcik GL, Graff M, Nishimura KK, et al. Genetic analyses of diverse populations improves discovery for complex traits. Nature. 2019;570(7762):514–518. doi:10.1038/s41586-019-1310-4
17. Abbasi F, Chu JW, Lamendola C, et al. Discrimination between obesity and insulin resistance in the relationship with adiponectin. Diabetes. 2004;53(3):585–590. doi:10.2337/diabetes.53.3.585
18. Yamauchi T, Kamon J, Waki H, et al. The fat-derived hormone adiponectin reverses insulin resistance associated with both lipoatrophy and obesity. Nat Med. 2001;7(8):941–946. doi:10.1038/90984
19. Xia JY, Holland WL, Kusminski CM, et al. Targeted induction of ceramide degradation leads to improved systemic metabolism and reduced hepatic steatosis. Cell Metab. 2015;22(2):266–278. doi:10.1016/j.cmet.2015.06.007
20. Berg AH, Combs TP, Du X, Brownlee M, Scherer PE. The adipocyte-secreted protein Acrp30 enhances hepatic insulin action. Nat Med. 2001;7(8):947–953. doi:10.1038/90992
21. Matsuzawa Y, Funahashi T, Kihara S, Shimomura I. Adiponectin and metabolic syndrome. Arterioscler Thromb Vasc Biol. 2004;24(1):29–33. doi:10.1161/01.ATV.0000099786.99623.EF
22. Wang Y, Meng RW, Kunutsor SK, et al. Plasma adiponectin levels and type 2 diabetes risk: a nested case-control study in a Chinese population and an updated meta-analysis. Sci Rep. 2018;8. doi:10.1038/s41598-017-18709-9
23. Peters KE, Beilby J, Cadby G, et al. A comprehensive investigation of variants in genes encoding adiponectin (ADIPOQ) and its receptors (ADIPOR1/R2), and their association with serum adiponectin, type 2 diabetes, insulin resistance and the metabolic syndrome. BMC Med Genet. 2013;14:15. doi:10.1186/1471-2350-14-15
24. Palit SP, Patel R, Jadeja SD, et al. A genetic analysis identifies a haplotype at adiponectin locus: association with obesity and type 2 diabetes. Sci Rep. 2020;10(1):2904. doi:10.1038/s41598-020-59845-z
25. Zhou JM, Zhang M, Wang S, et al. Association of the ADIPOQ rs2241766 and rs266729 polymorphisms with metabolic syndrome in the Chinese population: a meta-analysis. Biomed Environ Sci. 2016;29(7):505–515. doi:10.3967/bes2016.066
26. Han LY, Wu QH, Jiao ML, et al. Associations between single-nucleotide polymorphisms (+45T>G, +276G>T, −11377C>G, −11391G>A) of adiponectin gene and type 2 diabetes mellitus: a systematic review and meta-analysis. Diabetologia. 2011;54(9):2303–2314. doi:10.1007/s00125-011-2202-9
27. Gong M, Long J, Liu Q, Deng HC. Association of the ADIPOQ rs17360539 and rs266729 polymorphisms with type 2 diabetes: a meta-analysis. Mol Cell Endocrinol. 2010;325(1–2):78–83. doi:10.1016/j.mce.2010.05.007
28. Gao M, Ding D, Huang J, Qu Y, Wang Y, Huang Q. Association of genetic variants in the adiponectin gene with metabolic syndrome: a case-control study and a systematic meta-analysis in the Chinese population. PLoS One. 2013;8(4):e58412. doi:10.1371/journal.pone.0058412
29. Berg AH, Combs TP, Scherer PE. ACRP30/adiponectin: an adipokine regulating glucose and lipid metabolism. Trends Endocrinol Metab. 2002;13(2):84–89. doi:10.1016/s1043-2760(01)00524-0
30. Tong G, Wang N, Leng J, et al. Common variants in adiponectin gene are associated with coronary artery disease and angiographical severity of coronary atherosclerosis in type 2 diabetes. Cardiovasc Diabetol. 2013;12:67. doi:10.1186/1475-2840-12-67
31. Smetnev S, Klimushina M, Kutsenko V, et al. Associations of SNPs of the ADIPOQ gene with serum adiponectin levels, unstable angina, and coronary artery disease. Biomolecules. 2019;9(10):537. doi:10.3390/biom9100537
32. Chiodini BD, Specchia C, Gori F, et al. Adiponectin gene polymorphisms and their effect on the risk of myocardial infarction and type 2 diabetes: an association study in an Italian population. Ther Adv Cardiovasc Dis. 2010;4(4):223–230. doi:10.1177/1753944710371483
33. Gable DR, Matin J, Whittall R, et al. Common adiponectin gene variants show different effects on risk of cardiovascular disease and type 2 diabetes in European subjects. Ann Hum Genet. 2007;71(Pt 4):453–466. doi:10.1111/j.1469-1809.2006.00340.x
34. Yao M, Wu Y, Fang Q, Sun L, Li T, Qiao H. Association of ADIPOQ variants with type 2 diabetes mellitus susceptibility in ethnic Han Chinese from northeast China. J Diabetes Investig. 2016;7(6):853–859. doi:10.1111/jdi.12535
35. Ramya K, Ayyappa KA, Ghosh S, Mohan V, Radha V. Genetic association of ADIPOQ gene variants with type 2 diabetes, obesity and serum adiponectin levels in south Indian population. Gene. 2013;532(2):253–262. doi:10.1016/j.gene.2013.09.012
36. Rasmussen-Torvik LJ, Pankow JS, Jacobs DR, Steinberger J, Moran A, Sinaiko AR. The association of SNPs in ADIPOQ, ADIPOR1, and ADIPOR2 with insulin sensitivity in a cohort of adolescents and their parents. Hum Genet. 2009;125(1):21–28. doi:10.1007/s00439-008-0595-4
37. Solé X, Guinó E, Valls J, Iniesta R, Moreno V. SNPStats: a web tool for the analysis of association studies. Bioinforma Oxf Engl. 2006;22(15):1928–1929. doi:10.1093/bioinformatics/btl268
38. Miles A, Ralph P, Rae S, Pisupati R. Cggh/Scikit-Allel: V1.3.2. Zenodo; 2020. doi:10.5281/zenodo.3976233
39. Xue A, Wu Y, Zhu Z, et al. Genome-wide association analyses identify 143 risk variants and putative regulatory mechanisms for type 2 diabetes. Nat Commun. 2018;9(1):2941. doi:10.1038/s41467-018-04951-w
40. Lind L. Genome-wide association study of the metabolic syndrome in UK biobank. Metab Syndr Relat Disord. 2019;17(10):505–511. doi:10.1089/met.2019.0070
41. Dong Y, Huang G, Wang X, Chu Z, Miao J, Zhou H. Meta-analysis of the association between adiponectin SNP 45, SNP 276, and type 2 diabetes mellitus. PLoS One. 2020;15(10):e0241078. doi:10.1371/journal.pone.0241078
42. Alimi M, Goodarzi MT, Nekoei M. Adiponectin gene polymorphisms and risk of type 2 diabetes: an updated evidence for meta-analysis. Diabetol Metab Syndr. 2021;13(1):133. doi:10.1186/s13098-021-00749-x
43. Torres-Castillo N, Campos-Perez W, Rodriguez-Echevarria R, Rodriguez-Reyes SC, Martinez-Lopez E. A metabolically unhealthy phenotype is associated with ADIPOQ genetic variants and lower serum adiponectin levels. Lifestyle Genom. 2020;13(6):172–179. doi:10.1159/000510021
44. Wang Q, Ren D, Bi Y, et al. Association and functional study between ADIPOQ and metabolic syndrome in elderly Chinese Han population. Aging. 2020;12(24):25819–25827. doi:10.18632/aging.104203
45. Ogundele OE, Adekoya KO, Osinubi AAA, Awofala AA, Oboh BO. Association of adiponectin gene (ADIPOQ) polymorphisms with measures of obesity in Nigerian young adults. Egypt J Med Hum Genet. 2018;19(2):123–127. doi:10.1016/j.ejmhg.2017.08.005
46. Karmelić I, Lovrić J, Božina T, et al. Adiponectin level and gene variability are obesity and metabolic syndrome markers in a young population. Arch Med Res. 2012;43(2):145–153. doi:10.1016/j.arcmed.2012.02.004
47. Apalasamy YD, Rampal S, Salim A, Moy FM, Bulgiba A, Mohamed Z. Association of ADIPOQ gene with obesity and adiponectin levels in Malaysian Malays. Mol Biol Rep. 2014;41(5):2917–2921. doi:10.1007/s11033-014-3147-0
48. Dolley G, Bertrais S, Frochot V, et al. Promoter adiponectin polymorphisms and waist/hip ratio variation in a prospective French adults study. Int J Obes. 2008;32(4):669–675. doi:10.1038/sj.ijo.0803773
49. Boumaiza I, Omezzine A, Rejeb J, et al. Association between eight adiponectin polymorphisms, obesity, and metabolic syndrome parameters in Tunisian volunteers. Metab Syndr Relat Disord. 2011;9(6):419–426. doi:10.1089/met.2011.0035
50. Thao MP, Tuan PVA, Linh LGH, et al. Association of HLA-B*38:02 with antithyroid drug-induced agranulocytosis in Kinh Vietnamese patients. Int J Endocrinol. 2018;2018:7965346. doi:10.1155/2018/7965346
51. Tran TT, Mai TP, Tran HCB, et al. Association between AGT M235T and left ventricular mass in Vietnamese patients diagnosed with essential hypertension. Front Cardiovasc Med. 2021;8:608948. doi:10.3389/fcvm.2021.608948
52. Do MD, Mai TP, Do AD, et al. Risk factors for cutaneous reactions to allopurinol in Kinh Vietnamese: results from a case-control study. Arthritis Res Ther. 2020;22(1):182. doi:10.1186/s13075-020-02273-1
53. Do MD, Le LGH, Nguyen VT, et al. High-resolution HLA typing of HLA-A, -B, -C, -DRB1, and -DQB1 in Kinh Vietnamese by using next-generation sequencing. Front Genet. 2020;11:383. doi:10.3389/fgene.2020.00383
54. Cesari M, Narkiewicz K, De Toni R, Aldighieri E, Williams CJ, Rossi GP. Heritability of plasma adiponectin levels and body mass index in twins. J Clin Endocrinol Metab. 2007;92(8):3082–3088. doi:10.1210/jc.2007-0403
55. Rohde K, Keller M, Horstmann A, et al. Role of genetic variants in ADIPOQ in human eating behavior. Genes Nutr. 2015;10(1):449. doi:10.1007/s12263-014-0449-8
56. de Luis Roman DA, Primo D, IZaola O, Gómez E, López JJ. Adiponectin gene variant rs3774261, effects on lipid profile and adiponectin levels after a high polyunsaturated fat hypocaloric diet with Mediterranean pattern. Nutrients. 2021;13(6):1811. doi:10.3390/nu13061811
57. Warodomwichit D, Shen J, Arnett DK, et al. ADIPOQ Polymorphisms, Monounsaturated Fatty Acids, and Obesity Risk: The GOLDN Study Obesity. 2009;17(3):510-517. doi:10.1038/oby.2008.583
58. Melistas L, Mantzoros CS, Kontogianni M, Antonopoulou S, Ordovas JM, Yiannakouris N. Association of the +45T>G and +276G>T polymorphisms in the adiponectin gene with insulin resistance in nondiabetic Greek women Eur J Endocrinol. 2009;161(6):845-852. doi:10.1530/EJE-09-0492
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.