Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Association Between Weight Change During Adulthood and Chronic Kidney Disease: Results from a National Survey 2011–2018
Received 9 September 2023
Accepted for publication 12 November 2023
Published 23 November 2023 Volume 2023:16 Pages 3817—3826
DOI https://doi.org/10.2147/DMSO.S435886
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Xuemei Gong,1,2 Xiaoxi Zeng,1,3 Ping Fu1,2
1Department of Nephrology, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Division of Nephrology, Kidney Research Institute, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 3West China Biomedical Big Data Center, West China Hospital, Sichuan University, Chengdu, People’s Republic of China
Correspondence: Ping Fu, Division of Nephrology, Kidney Research Institute, West China Hospital, Sichuan University, Guo Xue Lane 37, Chengdu, 610041, People’s Republic of China, Tel/Fax +862885422335, Email [email protected]
Purpose: This study aimed to investigate the intricate relationship between weight change patterns and the onset of chronic kidney disease (CKD). Although obesity is recognized as a predisposing factor for CKD, the dynamics of weight fluctuation and its impact on CKD development are not well-defined. By analyzing data from the National Health and Nutrition Examination Survey (NHANES) spanning 2011 to 2018, we sought to elucidate the association between weight trajectories and CKD risk.
Patients and Methods: We included participants aged ≥ 40 years, employing body mass index (BMI) measurements at three life stages—baseline, age 25, and a decade preceding baseline—to categorize weight change patterns. Logistic regression was employed to evaluate the association of these patterns with CKD onset, adjusting for potential confounders.
Results: The study encompassed 12,284 participants, with 2893 individuals diagnosed with CKD. Transitioning from normal weight to obesity and staying obese throughout adulthood were found to increase the risk of developing CKD. These associations remained consistent after adjusting for covariates but were statistically insignificant after adjusting for comorbidities. Notably, individuals transitioning from obesity to normal weight from age 25 to baseline and from 10 years before baseline to baseline demonstrated significant correlations with CKD but not between age 25 and 10 years before baseline.
Conclusion: Obesity, weight gain throughout adulthood, and weight loss in middle-to-late adulthood are associated with an increased risk of CKD. This emphasizes the importance of long-term weight change patterns and maintaining a healthy weight throughout adulthood.
Keywords: body weight changes, body mass index, adulthood, chronic kidney diseases, national health and nutrition examination survey
Introduction
Chronic kidney disease (CKD) is a serious and widespread public health problem, with its associated morbidity and mortality contributing significantly to worldwide disease burdens.1 For efficacious management and intervention of CKD, pinpointing modifiable risk factors remains paramount. Obesity has emerged as a prominent contributor to CKD, with extensive research exploring its association with body mass index (BMI), a widely utilized obesity measure. Notably, elevated BMI correlates with an amplified CKD risk, independent of confounders like hypertension and type 2 diabetes (T2D).2–4 Yet, the nuanced interplay between obesity and CKD is intricate, epitomized by certain investigations unveiling an obesity-related paradox in CKD and end-stage renal disease (ESRD) cohorts.5 Previous research primarily relied on isolated BMI measurements, disregarding the dynamic nature of weight changes that lead to BMI fluctuations over time. Hence, it is crucial to consider long-term weight change patterns when investigating the obesity-CKD connection.
Although a handful of studies have delved into the impact of BMI changes on CKD occurrence and progression, their findings have been inconsistent.6–9 Some indicate weight gain as a CKD risk factor,7,9 whereas others suggest that weight reduction might accelerate CKD’s evolution to ESRD.8 However, these analyses occasionally suffer from limited statistical robustness, predominantly accentuating ephemeral weight shifts spanning years. Weight, in reality, can exhibit substantial variations across adulthood stages. The propensity for weight gain is often pronounced in early adulthood, with a plateau or decrement manifesting in subsequent life phases.10 Precociously acquired obesity or weight gain, in contrast to its later onset, correlates with escalated risks of various health issues, including cardiovascular disease,11 non-alcoholic fatty liver disease,12 diabetes,13,14 and all-cause mortality.11
Understanding the impact of weight fluctuation and BMI changes on CKD is pivotal for recommending patient-centric solutions. With a considerable fraction of patients with CKD grappling with obesity, weight regulation becomes indispensable. Although advocacy for maintaining a salubrious BMI spectrum is well-established,15 the blueprint for optimal BMI modulation in CKD contexts is debatable. Our investigation harnesses data from the National Health and Nutrition Examination Survey (NHANES) database, integrating baseline weight measurements with self-reported weights at age 25 and 10 years before baseline. This methodology facilitates a comprehensive probe into weight trajectories from young adulthood to mid-life and late adulthood stages and their bearing on CKD susceptibility.
Materials and Methods
Study Population
Data were obtained from NHANES designed to assess population health and nutrition. This encompassed chronic disease information, nutritional status, lifestyle habits, and environmental exposure data gathered through interviews, physical assessments, and laboratory analyses. Our analysis involved participants from NHANES spanning 2011 to 2018 who were aged 40 or older. Inclusion criteria required data on weight at baseline, at age 25, and 10 years before baseline, alongside serum creatinine and urine albumin-to-creatinine data. Consequently, 12,284 participants were retained for our analysis (as depicted in Figure 1).
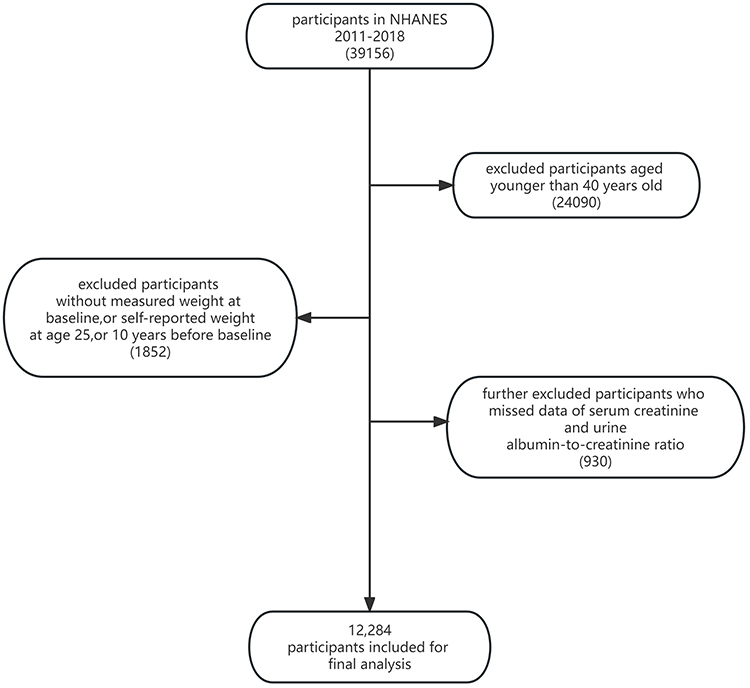 |
Figure 1 Flow chart of inclusion and exclusion of study participants. |
Assessment of Weight Change and Covariates
Weight data at age 25 and 10 years before the baseline NHANES survey were recall-collected during the baseline surveys. Height and baseline weight were measured in a mobile physical examination. We subsequently derived BMI values at three distinct life stages: age 25, 10 years before baseline, and baseline surveys. The formula employed was weight (kg) divided by the square of height (m2). Based on these BMI values, participants were categorized into: underweight (<18 kg/m2) and normal weight (18–25 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30.0 kg/m2).
Based on a recent study by Chen et al,11 we then assessed weight change over three periods: (1) BMI changes from age 25 years to 10 years before baseline, approximating weight change from young to middle adulthood; (2) BMI changes from 10 years before baseline to baseline, approximating weight change from midlife to late adulthood; (3) BMI changes from age 25 years to baseline, approximating weight change during the entire adulthood period. Then we defined four weight change patterns for each interval: (1) stable non-obese (maintaining a BMI of <30.0 kg/m2), (2) obese to non-obese (changing from BMI ≥30.0 kg/m2 to <30.0 kg/m2), (3) non-obese to obese (changing from BMI <30.0 kg/m2 to ≥30.0 kg/m2), and (4) stable obese (maintaining a BMI of ≥30.0 kg/m2).
Additionally, key variables potentially influencing the correlation between BMI transitions and CKD were extracted, including demographic information such as sex, age, race/ethnicity, education level, family poverty income ratio, smoking status, and physical activity level. We also collected self-reported baseline history of comorbidities including chronic bronchitis, emphysema, chronic obstructive pulmonary disease (COPD), diabetes mellitus (DM), cardiovascular disease (CVD), and stroke. Furthermore, the following parameters were obtained from blood tests: total cholesterol, triglycerides, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, fasting glucose, serum creatinine, blood urea nitrogen, and urine albumin-to-creatinine ratio.
Outcome Variables
The primary outcome was weighted prevalence of CKD in the overall population and different strata, defined as the presence of impaired kidney function (estimated glomerular filtration rate [eGFR] <60 mL/min/1.73 m2) or albuminuria (urine albumin-to-creatinine ratio ≥30 mg/g). The eGFR was calculated from serum creatinine, using the chronic kidney disease epidemiology collaboration equation 2021,16 and albuminuria data were extracted from laboratory results.
Statistical Analysis
We employed a descriptive analysis, considering the intricate survey design parameters of NHANES, including sample weights, clustering, and stratification. Data metrics are presented as either mean (standard deviation) or frequency (percentage), contingent on suitability. Baseline characteristics were compared among weight change patterns in the three intervals using the Rao–Scott χ2 test for categorical variables and the Wilcoxon rank-sum test adjusted for sampling weights for continuous variables. Multivariable logistic regression models were utilized to establish odds ratios (ORs) and corresponding 95% confidence intervals (CIs) for CKD risk concerning BMI at each time point and weight change patterns in the three intervals. Firstly, we examined the relations between BMI at each time point and CKD risk, using normal weight as the reference group. In our analysis, Model 1 was not adjusted for any covariates. Model 2 accounted for adjustments in covariates such as sex, age, race/ethnicity, educational level, family income-poverty ratio, smoking status, and physical activity level. Ultimately, Model 3 further refined the adjustments to include potential mediating comorbidities, such as hypertension, diabetes, and cardiovascular disease. Subsequently, employing a consistent methodology, we meticulously examined the associations between the four weight change patterns across the three intervals and CKD.
Subgroup analyses were conducted based on sex (male vs female), age (<60, 60–80, and >80 years), and leisure physical activity (0 times/week, 1–2 times/week, and ≥3 times/week).
To ensure the robustness of our findings, we conducted a series of sensitivity analyses. Firstly, the Multiple Imputation by Chained Equations package in R was utilized to address missing data, resulting in a rigorously imputed dataset. This dataset facilitated a re-examination of the association between variations in BMI and CKD incidence. Secondly, we performed a complete case analysis by omitting cases with missing covariate information to verify the consistency of our results. Thirdly, we refined our classification of weight-change patterns, stratifying participants into quintiles based on the percentage of absolute body weight fluctuation over three distinct intervals: ≥10% weight loss, 5–10% weight loss, ≤5% weight change, 5–10% weight gain, and ≥10% weight gain. This new categorization was then employed to reevaluate the relationship between BMI change and CKD.
For all statistical evaluations, tests were two-tailed, with the threshold of significance firmly established at P < 0.05. These analyses were diligently performed using R software, version 4.3.0 (R Core Team, Vienna, Austria).
Results
Baseline Characteristics and Weight-Change Patterns
In this cohort analysis of 12,284 participants, the trajectory of BMI was ascending throughout all recorded intervals, signaling an escalating trend in obesity prevalence. Specifically, BMI increased from 24.3 (4.6) at age 25 to 28.3 (6.4) at 10 years before baseline, escalating further to 30 (7) at the baseline survey. This trend illustrates an average weight gain of 15 kg from age 25 to the baseline, with an 11-kg increment from age 25 to 10 years before baseline and a 4-kg increase in the subsequent decade approaching baseline. Regarding weight change patterns from age 25 to baseline, most (58%) of the population successfully maintained a non-obese status, whereas a significant contingent (33%) experienced a transition from non-obesity to obesity. A minute fraction (1.3%) exhibited a reversal from obesity to non-obesity. Furthermore, 7.6% of the cohort consistently presented with obesity across the observed timeframe. Examining the period from age 25 to 10 years before baseline, 68% of participants retained a stable normal weight. A minority (8.1%) remained persistently obese, 23% transitioned from non-obesity to obesity, and a mere 0.8% reversed from an obese to a non-obese state (as elucidated in Supplementary Table 1). In the period from 10 years before baseline to baseline, 25% of individuals remained consistently obese, with 16% transitioning from non-obese to obese states (detailed in Supplementary Table 2).
As depicted in Table 1, we profiled the health-related characteristics of the participants, stratified by their weight trajectory from age 25 until the study baseline. This stratification elucidated notable differences among the cohorts. Compared with the participants with stable non-obesity, individuals in the other trajectories were, on average, younger, possessed lower educational achievements, and reported diminished household incomes. Particularly, the subgroup with persistent obesity exhibited the highest prevalence of DM. In contrast, individuals transitioning from an obese to a non-obese category demonstrated increased frequencies of several health conditions, including hypertension, cardiovascular diseases, cerebrovascular accidents, chronic bronchitis, COPD, and CKD. Baseline characteristics of the participants for the other two time intervals are presented in Supplementary Tables 1 and 2.
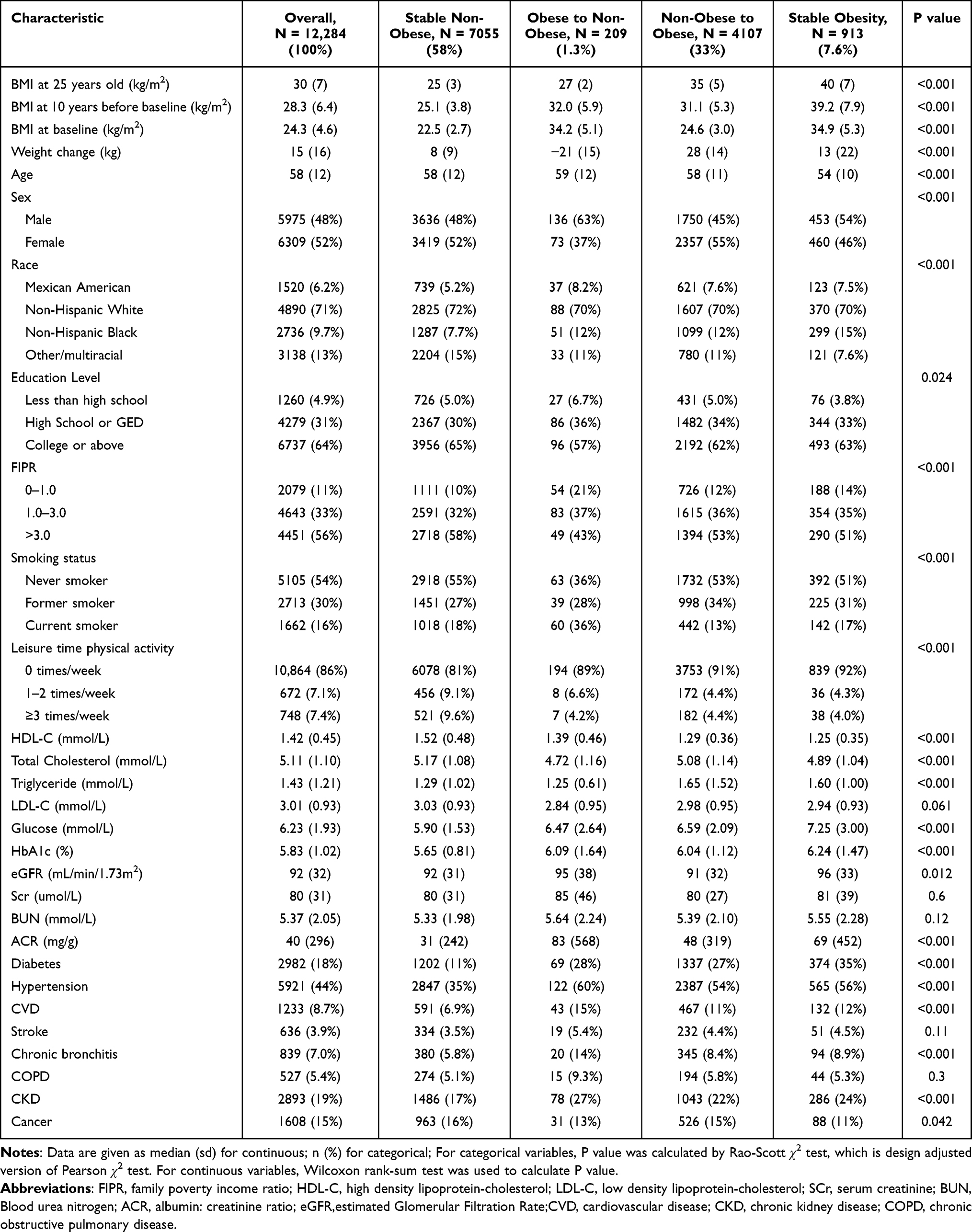 |
Table 1 Baseline Characteristics of Study Participants in the NHANES 2011–2018 According to Weight Change Patterns from Age 25 Years to Baseline |
Associations of Weight and Weight-Change Patterns with Chronic Kidney Disease
Among the 12,284 study participants, 2893 were diagnosed with CKD. To elucidate the influence of BMI on CKD risk, we systematically examined this association at three separate time intervals (Supplementary Table 3), using the normal weight group as the reference. In Model 1, overweight individuals had a relative risk of 1.4 (95% CI: 1.17–1.66) 10 years before baseline. Contrastingly, obesity presented a more pronounced risk at different time points: 1.52-fold (95% CI: 1.33–1.73) at baseline, 1.91-fold (1.61–2.26) 10 years before the baseline, and 1.38-fold (1.14–1.68) at age 25. Notably, underweight individuals did not manifest a significant association with CKD when benchmarked against individuals with normal weight. After adjusting for covariates such as sex, age, education, income, smoking, and physical activity, the observed relationships paralleled those from Model 1. However, a nuanced adjustment that factored in comorbidities in Model 3 rendered the observed correlations statistically non-significant.
Figure 2 offers a comprehensive visual representation of the relationship between weight-change patterns over the three periods and CKD using the stable normal-weight group as the benchmark. In the unadjusted model, both the transitions, from non-obese to obese as well as stable obese groups, showed a significant association with increased CKD risk over all three periods. From age 25 to baseline, transitioning from a non-obese to obese status was linked to an OR of 1.39 (95% CI: 1.24–1.56), whereas the stable obese group revealed an OR of 1.52 (95% CI: 1.23–1.88). Between age 25 and 10 years before the baseline, the ORs were 1.62 (95% CI: 1.41–1.86) and 1.57 (95% CI: 1.28–1.94) for the transitioning from a non-obese to obese status and stable obese groups, respectively. From 10 years before baseline to baseline, the corresponding ORs stood at 1.29 (95% CI: 1.09–1.54) and 1.65 (95% CI: 1.47–1.85). Moreover, the group transitioning from obesity to a non-obese status presented a robust link with CKD at specific intervals. Specifically, there was an 80% elevated risk from age 25 to baseline (OR=1.80, 95% CI: 1.21–2.69) and a 97% heightened risk in 10 years before baseline (OR=1.97, 95% CI: 1.55–2.50). Notably, this association was not consistently observed from age 25 to 10 years before the baseline, with an OR of 1.53 (95% CI: 0.90–2.60). Model 2, even after covariate adjustments, mirrored these findings. The transition from a non-obese to obese status and sustained obesity remained significantly associated with CKD across all intervals. Remarkably, when juxtaposed with the stable non-obese cohort, maintaining obesity was pinpointed as the strongest predictor for CKD onset. In the intricately adjusted Model 3, which incorporated baseline comorbidities like diabetes, cardiovascular diseases, and hypertension, the associations between various BMI-change patterns and CKD were found to be weakened and statistically insignificant (Supplementary Table 4).
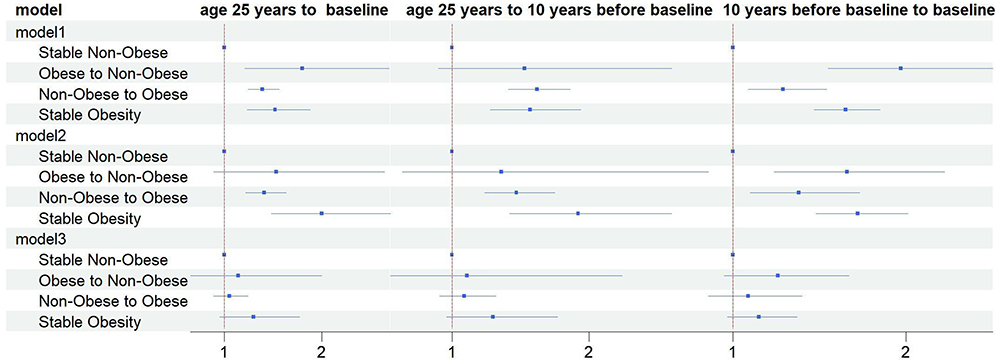 |
Figure 2 Odds Ratios (95% Confidence Intervals) for the association between weight change patterns and CKD risk across adulthood. |
Subgroup stratification by sex demonstrated consistent patterns. However, a distinct stratification by sex within the older subgroup, those aged ≥80 years, did not exhibit a clear link between weight change and CKD, indicating potential variances attributable to aging. Regarding physical activity levels, an absence of regular exercise amplified the detrimental effects of weight escalation on renal function, predominantly evident in the cohorts with obesity. On the brighter side, sustained physical activity appeared to temper the adverse ramifications of obesity on renal health, as evidenced by our findings, which pinpointed the shift from obesity to non-obesity as a protective factor against CKD onset (Supplementary Table 5).
Lastly, in sensitivity analyses, both imputations and complete-case analyses consistently confirmed our primary findings, as detailed in Supplementary Tables 6 and 7. Moreover, when classifying participants according to the percentage variation in absolute body weight, weight reductions of 5–10% and over 10% were profoundly linked to an augmented CKD risk from 10 years before baseline to baseline, even after adjusting for covariates and comorbidities. This further reinforces the notion that, during middle-to-late adulthood, weight loss emerges as a salient risk factor for CKD (Supplementary Table 8).
Discussion
Using a large, nationally representative sample of middle-aged and older adults, we aimed to determine the association between long-term weight change and CKD. Our data clearly indicate that obesity is a significant and robust risk factor for CKD, as is marked weight gain over time. Crucially, the observed association persisted even after accounting for a range of potential confounders. Notably, a transition from an obese to a normal weight status during mid-to-late adulthood was associated with CKD risk, at times exceeding the risks associated with consistent obesity. This trend was not evident in the earlier stages of adulthood. Our findings, therefore, underscore a complex and stage-specific interplay between weight dynamics and CKD risk, suggesting that the timing of weight change may have substantial implications for renal health outcomes.
Numerous studies have documented non-linear (U- or J-shaped) associations between BMI and CKD,4,17–20 with higher BMI being a known risk factor for ESRD.17 This concurs with our findings and is supported by Mendelian randomization studies indicating an inverse relationship between high BMI and renal function, independent of diabetic status.3 Current evidence suggests that metabolic abnormalities,21 chronic inflammation,22 and increased risk of hypertension or diabetes23 are implicated in the connection between excess body weight and CKD. Additionally, the direct impacts of obesity on renal structure or function can lead to renal damage and lower glomerular filtration rates.24 Despite this, our covariate-adjusted analyses did not corroborate an increased risk of CKD with overweight status, as has been stated in some previous reports.25 This variance may be attributable to methodological differences and sample size discrepancies among studies. Intriguingly, the “obesity paradox”—improved survival rates in patients with obesity with ESRD—persists in the literature, challenging conventional understanding of obesity’s role in chronic illnesses.5 Despite rigorous adjustment for confounders, the paradoxical protective effect of higher BMI in ESRD suggests a complex interplay between obesity, inflammation, and hemodynamic stability.5 Emerging experimental and clinical research suggests that obesity and elevated adiposity may confer a protective advantage in contexts marked by systemic inflammation and hemodynamic instability.26 This hypothesis is bolstered by evidence demonstrating that individuals who are underweight or malnourished are at a higher risk for negative health outcomes.27,28 The observed “obesity paradox” may also reflect a non-causal association, where BMI variations are secondary to changes in health status rather than directly contributing to ESRD outcomes. Current insights stem predominantly from observational studies; hence, causal interpretations remain speculative, necessitating further research for a comprehensive elucidation.
Our study underscores the importance of evaluating weight trajectories over absolute weight values, acknowledging that both weight gain and loss are pertinent to CKD risk. The trajectory and timing of weight-changes can influence disease outcomes.29–31 Previous studies have also suggested that weight-changes can affect the occurrence or progression of CKD.6,8,9,32–34 However, inconsistent conclusions have been also reported in this regard. Ku et al, for example, examined weight-changes in adults with CKD and their association with mortality following the initiation of dialysis therapy. They found that significant weight loss in pre-dialysis stages has been associated with increased mortality post-dialysis initiation.6 Conversely, among participants without CKD at baseline, another study revealed that weight gain exceeding 10% (RR: 1.43; 95% CI: 1.07–1.90) and increase in waist circumference exceeding 15% (RR: 1.37; 95% CI: 1.01–1.85) were associated with higher risk of CKD incidence.35 Research has also shown that rapid weight gain and loss are associated with a high risk of adverse outcomes.7 Although a significant association between mid-to-late-life weight loss and CKD emerged, earlier studies have connected weight loss in older adults with increased mortality,11,36,37 possibly confounded by smoking habits or pre-existing conditions.38 Consequently, interpretations of weight loss as a CKD correlate must be approached with caution, given the potential reverse causality from undiagnosed diseases at baseline. Unfortunately, this study’s design precludes the ability to differentiate whether weight loss is a precursor or a consequence of ill health. Furthermore, weight reduction in middle-aged and older adults may reflect a state of protein-energy wasting and nutritional deficits, which have been implicated in exacerbating outcomes for patients with CKD—an imbalance between lean and fat mass is especially prognostic of adverse events.7 Weight loss might also indicate a more severe underlying disease state or enhanced inflammatory processes, potentially signaling an accelerated progression toward ESRD.39 It should be noted that this study did not capture data on the intent behind weight loss, which is relevant given that some studies have observed that purposeful weight loss through interventions designed to increase muscle mass and decrease fat can decelerate the emergence and progression of CKD.40,41 This observation supports the hypothesis that selective reduction in specific fat compartments and preservation of lean body mass might have differential effects on morbidity and mortality.42 Lastly, although BMI is ubiquitously utilized as an obesity metric, it fails to provide an accurate assessment of body fat distribution—a factor that may be more decisive than overall mass in contributing to vascular complications associated with CKD.43
Our study, though informative, presents several non-negligible limitations warranting cautious interpretation of the results. Primarily, the inherent design of this observation study constrains our capacity to establish causative determinations between BMI fluctuations and CKD. Additionally, our reliance on self-reported historical weight data introduces the potential for recall bias, with inaccuracies possibly arising from participants’ imperfect recollections or societal influences, including normative biases or stigma. Furthermore, the analysis did not adjust for a spectrum of variables potentially influencing weight loss, encompassing nutritional practices, pathological weight loss secondary to illness (cachexia), or medication effects. Consequently, the posited correlations between weight trajectory and CKD risk may not fully account for these confounding factors, possibly diminishing the inferred associations’ strength.
Conclusions
Despite these constraints, our investigation reveals a compelling link between BMI variation patterns and the risk of CKD, highlighting a notably heightened risk in individuals with consistent obesity or those experiencing weight gain throughout adulthood, as well as those with weight loss in middle-to-late adulthood. The relationship between weight dynamics and CKD underscores the complex nature of obesity-related risk factors and suggests that weight management across the lifespan could play a pivotal role in CKD prevention and control. Future research endeavors should aim to elucidate the intricate mechanisms underpinning these associations and assess the impact of targeted weight management interventions on the progression and prevention of CKD.
Abbreviations
CKD, Chronic kidney disease; NHANES, National Health and Nutrition Examination Survey; BMI, Body mass index; ESRD, End-stage renal disease; FIPR, Family poverty income ratio; COPD, Chronic obstructive pulmonary disease; DM, Diabetes mellitus; CVD, Cardiovascular disease; eGFR, estimated Glomerular Filtration Rate; ORs, Odds ratios; CIs, Confidence intervals.
Institutional Review Board Statement
Ethical review and approval were exempted for this study as it made use of publicly accessible data sourced from the National Health and Nutrition Examination Survey (NHANES) database. Authorization for the use of the NHANES database was granted by the National Center for Health Statistics (NCHS) in the United States. The study protocols underwent approval by the NCHS Research Ethics Review Committee, and all participants in the NHANES survey provided informed consent.
Acknowledgments
We thank the National Health and Nutrition Examination Survey participants and staff and the National Center for Health Statistics for their valuable contributions, and thank Editage for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Bikbov B, Purcell CA, Levey AS. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;395(10225):709–733. doi:10.1016/S0140-6736(20)30045-3
2. Zhu P, Herrington WG, Haynes R, et al. Conventional and genetic evidence on the association between adiposity and CKD. J Am Soc Nephrol. 2021;32(1):127–137. doi:10.1681/ASN.2020050679
3. Kjaergaard AD, Teumer A, Witte DR, et al. Obesity and kidney function: a Two-Sample Mendelian Randomization Study. Clin Chem. 2022;68(3):461–472. doi:10.1093/clinchem/hvab249
4. Foster MC, Hwang S-J, Larson MG, et al. Overweight, obesity, and the development of stage 3 CKD: the Framingham Heart Study. Am J Kidney Dis. 2008;52(1):39–48. doi:10.1053/j.ajkd.2008.03.003
5. Naderi N, Kleine C-E, Park C, et al. Obesity paradox in advanced kidney disease: from bedside to the bench. Prog Cardiovasc Dis. 2018;61(2):168–181. doi:10.1016/j.pcad.2018.07.001
6. Ku E, Kopple JD, Johansen KL, et al. Longitudinal weight change during CKD progression and its association with subsequent mortality. Am J Kidney Dis. 2018;71(5):657–665. doi:10.1053/j.ajkd.2017.09.015
7. Ryu H, Hong Y, Kang E, et al. Rapid weight change over time is a risk factor for adverse outcomes in patients with predialysis chronic kidney disease: a Prospective Cohort Study. J Ren Nutr. 2021;31(6):569–578. doi:10.1053/j.jrn.2021.01.026
8. Toda A, Hara S, Tsuji H, et al. Effects of body weight change on development of chronic kidney disease in obese metabolic phenotypes. Nephron. 2022;146(5):449–456.
9. Ryu S, Chang Y, Woo H-Y, et al. Changes in body weight predict CKD in healthy men. J Am Soc Nephrol. 2008;19(9):1798–1805. doi:10.1681/ASN.2007121286
10. Sheehan TJ, DuBrava S, DeChello LM, et al. Rates of weight change for black and white Americans over a twenty year period. Int J Obes Relat Metab Disord. 2003;27(4):498–504. doi:10.1038/sj.ijo.0802263
11. Chen C, Ye Y, Zhang Y, et al. Weight change across adulthood in relation to all cause and cause specific mortality: prospective cohort study. BMJ. 2019;367:l5584. doi:10.1136/bmj.l5584
12. Wang L, Yi J, Guo J, et al. Weigh change across adulthood is related to the presence of NAFLD: results from NHANES III. J Transl Med. 2023;21(1):142. doi:10.1186/s12967-023-04007-8
13. Power C, Thomas C. Changes in BMI, duration of overweight and obesity, and glucose metabolism: 45 years of follow-up of a birth cohort. Diabetes Care. 2011;34(9):1986–1991. doi:10.2337/dc10-1482
14. Lamichhane AP, Couper D, Jenkins GP, et al. Longitudinal associations between body mass index during young adulthood, subsequent weight change, and incident diabetes during mid- and older-adulthood in non-Hispanic white and African American Populations: the Atherosclerosis Risk in Communities Study. Metab Syndr Relat Disord. 2020;18(7):313–320. doi:10.1089/met.2020.0005
15. Stevens PE, Levin A. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013;158(11):825–830. doi:10.7326/0003-4819-158-11-201306040-00007
16. Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med. 2021;385(19):1737–1749. doi:10.1056/NEJMoa2102953
17. C-y H, McCulloch CE, Iribarren C, et al. Body mass index and risk for end-stage renal disease. Ann Intern Med. 2006;144(1):21–28. doi:10.7326/0003-4819-144-1-200601030-00006
18. Chang AR, Grams ME, Ballew SH, et al. Adiposity and risk of decline in glomerular filtration rate: meta-analysis of individual participant data in a global consortium. BMJ. 2019;364:k5301. doi:10.1136/bmj.k5301
19. Betzler BK, Sultana R, Banu R, et al. Association between body mass index and chronic kidney disease in Asian populations: a participant-level meta-analysis. Maturitas. 2021;154:46–54. doi:10.1016/j.maturitas.2021.09.005
20. Garofalo C, Borrelli S, Minutolo R, et al. A systematic review and meta-analysis suggests obesity predicts onset of chronic kidney disease in the general population. Kidney Int. 2017;91(5):1224–1235. doi:10.1016/j.kint.2016.12.013
21. Sharma I, Liao Y, Zheng X, et al. New pandemic: obesity and associated nephropathy. Front Med. 2021;8:673556. doi:10.3389/fmed.2021.673556
22. Brennan E, Kantharidis P, Cooper ME, et al. Pro-resolving lipid mediators: regulators of inflammation, metabolism and kidney function. Nat Rev Nephrol. 2021;17(11):725–739. doi:10.1038/s41581-021-00454-y
23. Tonneijck L, Muskiet MHA, Smits MM, et al. Glomerular hyperfiltration in diabetes: mechanisms, clinical significance, and treatment. J Am Soc Nephrol. 2017;28(4):1023–1039. doi:10.1681/ASN.2016060666
24. Henegar JR, Bigler SA, Henegar LK, et al. Functional and structural changes in the kidney in the early stages of obesity. J Am Soc Nephrol. 2001;12(6):1211–1217. doi:10.1681/ASN.V1261211
25. Khedr A, Khedr E, House AA. Body mass index and the risk of progression of chronic kidney disease. J Ren Nutr. 2011;21(6):455–461. doi:10.1053/j.jrn.2010.12.001
26. Park J, Ahmadi S-F, Streja E, et al. Obesity paradox in end-stage kidney disease patients. Prog Cardiovasc Dis. 2014;56(4):415–425. doi:10.1016/j.pcad.2013.10.005
27. Stack AG, Murthy BVR, Molony DA. Survival differences between peritoneal dialysis and hemodialysis among “large” ESRD patients in the United States. Kidney Int. 2004;65(6):2398–2408. doi:10.1111/j.1523-1755.2004.00654.x
28. Kalantar-Zadeh K, Streja E, Molnar MZ, et al. Mortality prediction by surrogates of body composition: an examination of the obesity paradox in hemodialysis patients using composite ranking score analysis. Am J Epidemiol. 2012;175(8):793–803. doi:10.1093/aje/kwr384
29. Park SY, Wilkens LR, Maskarinec G, et al. Weight change in older adults and mortality: the Multiethnic Cohort Study. Int J Obes. 2018;42(2):205–212. doi:10.1038/ijo.2017.188
30. Myrskylä M, Chang VW. Weight change, initial BMI, and mortality among middle- and older-aged adults. Epidemiology. 2009;20(6):840–848. doi:10.1097/EDE.0b013e3181b5f520
31. Ingram DD, Mussolino ME. Weight loss from maximum body weight and mortality: the third national health and nutrition examination survey linked mortality file. Int J Obes. 2010;34(6):1044–1050. doi:10.1038/ijo.2010.41
32. Ku E, Kopple JD, McCulloch CE, et al. Associations between weight loss, kidney function decline, and risk of ESRD in the Chronic Kidney Disease in Children (CKiD) Cohort Study. Am J Kidney Dis. 2018;71(5):648–656. doi:10.1053/j.ajkd.2017.08.013
33. Yun H-R, Kim HW, Chang TI, et al. Increased risk of chronic kidney disease associated with weight gain in healthy adults: insight from metabolic profiles and body composition. Front Med. 2021;8:705881. doi:10.3389/fmed.2021.705881
34. Zhang H-S, An S, Ahn C, et al. Obesity measures at baseline, their trajectories over time, and the incidence of chronic kidney disease: a 14 year cohort study among Korean adults. Nutr, Metab Cardiovasc Dis. 2021;31(3):782–792. doi:10.1016/j.numecd.2020.10.021
35. Chung HF, Al Mamun A, Huang MC, et al. Obesity, weight change, and chronic kidney disease in patients with type 2 diabetes mellitus: a longitudinal study in Taiwan: 2. J Diabetes. 2017;9(11):983–993. doi:10.1111/1753-0407.12514
36. Pan X-F, Yuan J-M, Koh W-P, et al. Weight change in relation to mortality in middle-aged and elderly Chinese: the Singapore Chinese Health Study. Int J Obes. 2019;43(8):1590–1600. doi:10.1038/s41366-018-0259-y
37. Cheng FW, Gao X, Jensen GL. Weight change and all-cause mortality in older adults: a meta-analysis. J Nutr Gerontol Geriatr. 2015;34(4):343–368. doi:10.1080/21551197.2015.1090362
38. Karahalios A, English DR, Simpson JA. Change in body size and mortality: a systematic review and meta-analysis. Int J Epidemiol. 2017;46(2):526–546. doi:10.1093/ije/dyw246
39. Amdur RL, Feldman HI, Gupta J, et al. Inflammation and progression of CKD: the CRIC Study. Clin J Am Soc Nephrol. 2016;11(9):1546–1556. doi:10.2215/CJN.13121215
40. Look AHEAD Research Group. Effect of a long-term behavioural weight loss intervention on nephropathy in overweight or obese adults with type 2 diabetes: a secondary analysis of the Look AHEAD randomised clinical trial. Lancet Diabetes Endocrinol. 2014;2(10):
41. Moncrieft AE, Llabre MM, McCalla JR, et al. Effects of a multicomponent life-style intervention on weight, glycemic control, depressive symptoms, and renal function in low-income, minority patients with type 2 diabetes: results of the community approach to lifestyle modification for diabetes randomized controlled trial. Psychosomatic Med. 2016;78(7):851–860. doi:10.1097/PSY.0000000000000348
42. Simonsen MK, Hundrup YA, Obel EB, et al. Intentional weight loss and mortality among initially healthy men and women. Nutr Rev. 2008;66(7):375–386. doi:10.1111/j.1753-4887.2008.00047.x
43. Lee SW, Son JY, Kim JM, et al. Body fat distribution is more predictive of all-cause mortality than overall adiposity. Diabetes Obes Metab. 2018;20(1):141–147. doi:10.1111/dom.13050
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.