Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Association Between Triglyceride to High-Density Lipoprotein Cholesterol Ratio and Insulin Resistance in Mongolian Adults
Authors Narkhajid G ![]() , Oyuntugs B, Yagaantsetseg A, Bolormaa E, Anuurad E, Enkhmaa B, Berglund L
, Oyuntugs B, Yagaantsetseg A, Bolormaa E, Anuurad E, Enkhmaa B, Berglund L ![]() , Bayasgalan T
, Bayasgalan T ![]()
Received 20 January 2025
Accepted for publication 1 May 2025
Published 23 May 2025 Volume 2025:18 Pages 1711—1719
DOI https://doi.org/10.2147/DMSO.S518509
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Galsanjigmed Narkhajid,1,* Byambasukh Oyuntugs,1 Altangerel Yagaantsetseg,2 Enkhtuvshin Bolormaa,3 Erdembileg Anuurad,4 Byambaa Enkhmaa,5 Lars Berglund,5 Tumenbayar Bayasgalan2,*
1Department of Endocrinology, School of Medicine, Mongolian National University of Medical Sciences, Ulaanbaatar, 13270, Mongolia; 2Postgraduate Training Institute, Mongolian National University of Medical Sciences, Ulaanbaatar, 14210, Mongolia; 3Intermed Hospital, Ulaanbaatar, Mongolia; 4Office of Research, School of Medicine, University of California – Davis, Sacramento, CA, 95817, USA; 5Department of Internal Medicine, School of Medicine, University of California – Davis, Davis, CA, USA
*These authors contributed equally to this work
Correspondence: Tumenbayar Bayasgalan, Postgraduate Training Institute, Mongolian National University of Medical Sciences, S. Zorig Street, Sukhbaatar District, 1st Khoroo, Ulaanbaatar, 14210, Mongolia, Tel +976 96664800, Email [email protected]
Introduction: While the Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) is widely used to identify insulin resistance, its clinical utility can be cumbersome. An alternative, the triglyceride-to-high-density lipoprotein cholesterol (TG/HDL) ratio, offers simplicity but may exhibit variability across different populations. This study aimed to investigate its association with HOMA-IR adjusting for waist circumference among Mongolian adults.
Materials and Methods: This cross-sectional study, conducted at the Mongolian National University of Medical Sciences Hospital, included 365 participants over 35 who participated in health check-up examinations (mean age 46.8 ± 8.8 years, 37.0% male). Waist circumference was categorized into tertiles. Associations between the TG/HDL ratio and HOMA-IR were meticulously assessed within the waist circumference tertiles (0– 33.3%, 33.4– 66.6%, and 66.7– 100%), ensuring a comprehensive understanding of the data.
Results: A significant positive correlation (r = 0.391, p = 0.019) was observed between the TG/HDL ratio and HOMA-IR levels in all participants. Analyses by waist circumference tertiles revealed a progressively stronger correlation (ranging from r = 0.241 to 0.469) with increasing waist circumference (p < 0.05). The diagnostic accuracy of the TG/HDL ratio in identifying insulin resistance was assessed using HOMA-IR thresholds of 2.0 and 2.5, yielding AUC values of 0.693 and 0.746, respectively. When considering waist circumference thresholds (> 90 cm for men and > 80 cm for women), TG/HDL ratio thresholds of 1.2 (sensitivity 56%, specificity 90%) in men and 0.69 (sensitivity 46%, specificity 80%) in women were identified.
Conclusion: The study indicates that the TG/HDL ratio, adjusted for waist circumference, could be a useful marker for insulin resistance in Mongolian adults, supporting its potential in clinical practice.
Keywords: insulin resistance, TG/HDL ratio, HOMA-IR, waist circumstance
Introduction
In Mongolia, the prevalence of type 2 diabetes (T2DM) was 3.1% in 1999.1 Twenty years later, a nationwide study conducted in the exact geographical locations using the same methods as the previous research revealed a significant increase in the prevalence of T2DM to 10.0%.2 The increase in the prevalence of T2DM is driven mainly by factors such as obesity, unhealthy lifestyles, and genetic susceptibility.3,4 Moreover, the emergence of metabolic syndrome, strongly associated with insulin resistance, appears to be more pronounced in Mongolian populations compared to other Asian countries.5 As a result, addressing insulin resistance becomes paramount for alleviating the burden of obesity-related health issues in Mongolia.
While the hyperinsulinemic-euglycemic clamp test remains the gold standard,6 the Homeostasis Model Assessment for Insulin Resistance (HOMA-IR) method is a widely used alternative to detect insulin resistance in clinical settings.7 However, both methods have limitations and can be resource-intensive, requiring resources unavailable in primary and secondary hospitals in Mongolia. Hence, investigators have diligently pursued more accessible markers for discerning insulin resistance, with the triglyceride-to-high-density lipoprotein cholesterol (TG/HDL) ratio emerging as a promising candidate.8–11 For instance, studies conducted in China and South Korea have highlighted the potential utility of the TG/HDL ratio in assessing insulin resistance within their respective populations.9–11 Moreover, the method is demonstrated to be both reliable and cost-effective.9,12,13
In Mongolia, previous studies have not evaluated insulin resistance at the population level using the HOMA-IR method or established cut-off points. As a result, the utility of the triglyceride-to-HDL cholesterol (TG/HDL) ratio as an estimator of insulin resistance remains limited because well-defined HOMA-IR cut-off values are lacking. To lay the groundwork for a nationwide study aimed at establishing HOMA-IR cut-off values and identifying predictors within the Mongolian population, we conducted this study to investigate the relationship between the TG/HDL ratio and HOMA-IR. We included waist circumference in our analysis due to its strong association with insulin resistance, which improved our ability to estimate insulin resistance.
Materials and Methods
Data Source and Study Population
The study was conducted at the Mongolian National University of Medical Sciences Hospital from June to September 2019. The study comprised individuals aged 35 and above who underwent health check-up examinations voluntarily. Exclusion criteria included prevalent diabetes (both type 1 and type 2), other comorbid endocrine disorders, malignancies, renal failure, cerebrovascular diseases, acute medical conditions, individuals utilizing insulin mimetics and lipid-lowering drugs, as well as pregnant participants, leaving a total of 365 eligible individuals included in the study. All participants provided informed consent, and the Ethical Committee of the Mongolian National University of Medical Sciences approved the study.
Variables and Measurements
The questionnaire gathered demographic information such as age and education, along with lifestyle factors including diet, physical activity, smoking, and alcohol consumption. It was designed based on Mongolia’s established guidelines for managing type 2 diabetes mellitus. Dietary intake was evaluated following WHO recommendations. As detailed below, anthropometric measurements and laboratory data (fasting blood glucose, insulin, and lipid profiles) were obtained. Following the recommendations of the World Health Organization, individuals consuming fewer than five servings of fruits and vegetables per week were classified as insufficient.
Anthropometric Measurements
Participants underwent height, weight, and waist circumference measurements following the established study protocols. Body weight was measured to the nearest 0.01 kg standing using a TANITA® BC-541 (Tanita Corporation, Japan) bioelectrical impedance analysis tool scale. Height was measured to the nearest 0.1 m using a stadiometer, with individuals standing with closed feet and without shoes. Waist circumference was measured at the narrowest circumference between the lower costal border and the iliac crest; following a normal exhalation, the arms remained relaxed at the sides. Body mass index (BMI) was calculated by squaring the height in meters and dividing it by the weight in kilograms. Individuals were classified as obese if their BMI exceeded 30 kg/m2. In addition, we assessed waist circumference, considering values greater than 80 cm for women and greater than 90 cm for men as indicative of central obesity.14 Blood pressure measurements were conducted in triplicate following established guidelines, and an average reading exceeding 140/90 mmHg was used to identify individuals with hypertension.
Biochemical Measurements
To achieve the most accurate results during their hospital visit, participants were required to follow strict dietary guidelines for 24 hours beforehand, which included abstaining from alcohol and avoiding high-fat, high-glucose foods. Blood samples collected after an overnight fasting period of 8 to 12 hours were used to measure blood glucose, insulin, triglycerides, low-density lipoprotein (LDL), high-density lipoprotein (HDL), and total cholesterol levels, as in previous studies.5,9,11 Triglyceride (TG) values were converted to millimoles per liter (mmol/L) and subsequently utilized to determine the TG/HDL ratio.15 The HOMA-IR index was calculated using the following formula: HOMA-IR index = (INS0 [IU/L] × G0 [mmol/L]) / 22.5.5 We utilized HOMA-IR thresholds of 2.0 and 2.5, commonly applied in Asian populations, to assess the diagnostic accuracy of the TG/HDL ratio in relation to waist circumference tertiles, which may be a more relevant variable for evaluating insulin resistance.16–18
Statistical Analysis
The general characteristics of the study population were summarized using means and standard deviations (SD) for normally distributed variables, and medians with ranges (minimum to maximum) for non-normally distributed variables, after assessing normality. Categorical variables were expressed as percentages with corresponding numbers. Waist circumference was categorized into tertile groups (0–33.3%, 33.4–66.6%, and 66.7–100%) based on its sex-specific distributions (Figure S1). We used the one-way ANOVA, Kruskal–Wallis, or Chi-square test, where appropriate, to assess group differences. Spearman correlation test was used to investigate the associations between variables. Association between the TG/HDL ratio and HOMA-IR were assessed within waist circumference tertiles. Furthermore, the Receiver Operating Characteristic (ROC) curve was used to determine the diagnostic accuracy of the TG/HDL ratio in this study.
We used IBM SPSS V.28.0 (IBM, Chicago, IL) for all statistical analyses, and a statistical significance level was set at p < 0.05 for all tests.
Results
The mean age of participants was 46.8 ± 8.8 years, with 37.0% being male. Participant characteristics by tertiles of waist circumference are shown in Table 1. This table revealed a significant association between waist circumference and various metabolic parameters. Specifically, individuals with the highest waist circumference tertile exhibited markedly elevated insulin levels, along with other metabolic indicators such as increased blood pressure and adverse lipid profiles, compared to those with the lowest waist circumference tertile. Notably, in the lowest waist circumference tertile, the mean insulin level was 10.0 ± 6.6 µU/mL. In the middle group, it measured 12.2 ± 6.8 µU/mL, and in the highest waist circumference group, it reached 16.4 ± 12.1 µU/mL. These observations suggest a robust association between higher waist circumference and increased insulin resistance within the highest waist circumference group. Importantly, these findings were statistically significant, underscoring the significance of waist circumference in this population as a predictor of insulin resistance.
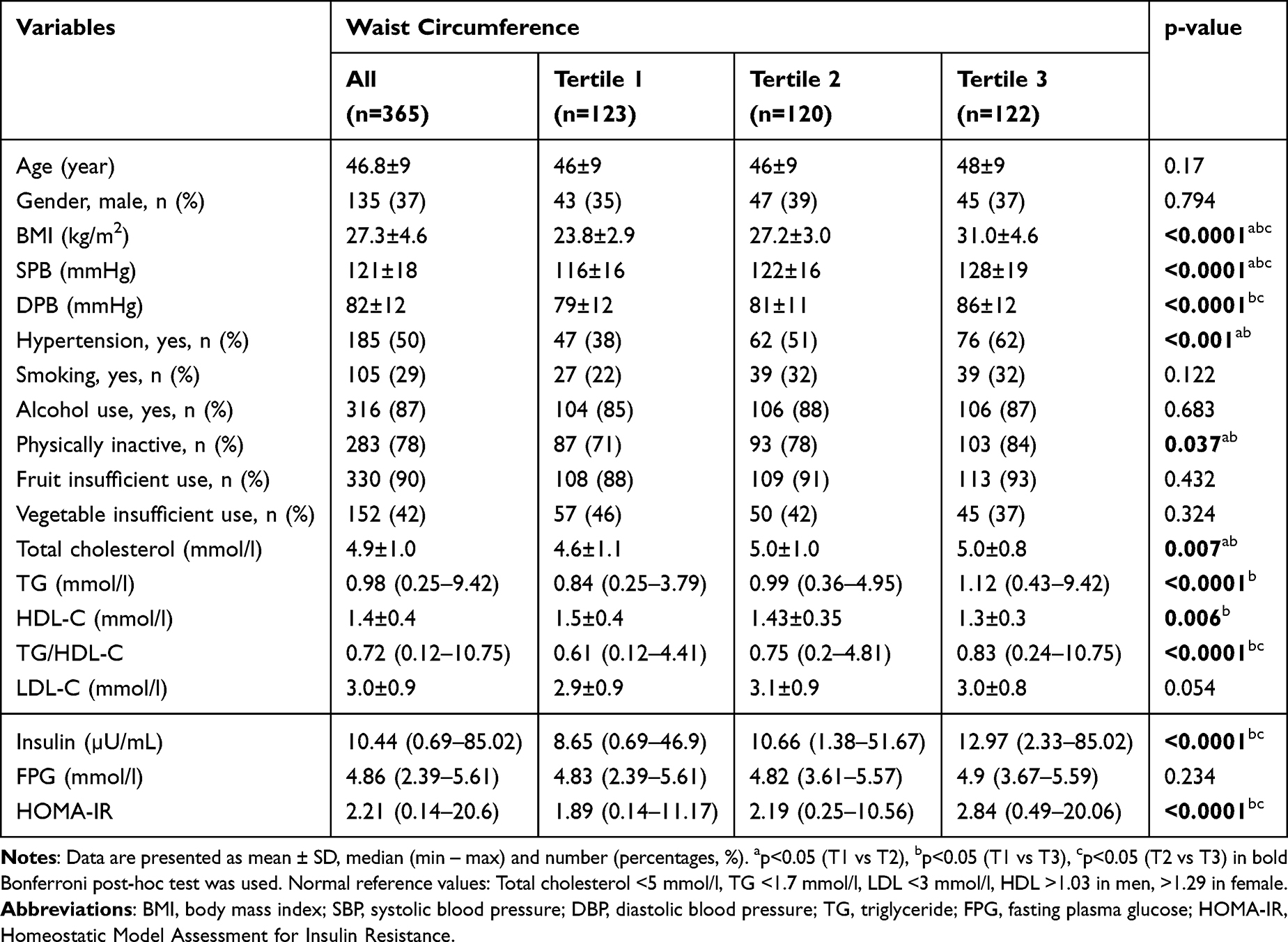 |
Table 1 Characteristics of the Study Population |
As illustrated in Figures 1 and 2, a notable pattern becomes evident, as both HOMA-IR and TG/HDL ratio levels consistently increased as waist circumference increased, suggesting a positive association between HOMA-IR and waist circumference. These findings underscore that individual with larger waist circumferences exhibit heightened insulin resistance. Furthermore, there was a significant, positive correlation between the TG/HDL ratio and HOMA-IR levels (r = 0.391, p = 0.019) in all participants. When subgroup analyses were conducted based on waist circumference tertiles, it became evident that an increase in waist circumference was linked to a more robust correlation between the TG/HDL ratio and HOMA-IR levels. Thus, the correlation coefficient between the TG/HDL ratio and HOMA-IR increased from 0.241 (p=0.007) in tertile 1 to 0.336 (p=0.0001) in tertile 2 and to 0.469 (p=0.0001) in tertile 3 of waist circumference.
 |
Figure 1 HOMA-IR across waist circumference tertiles. |
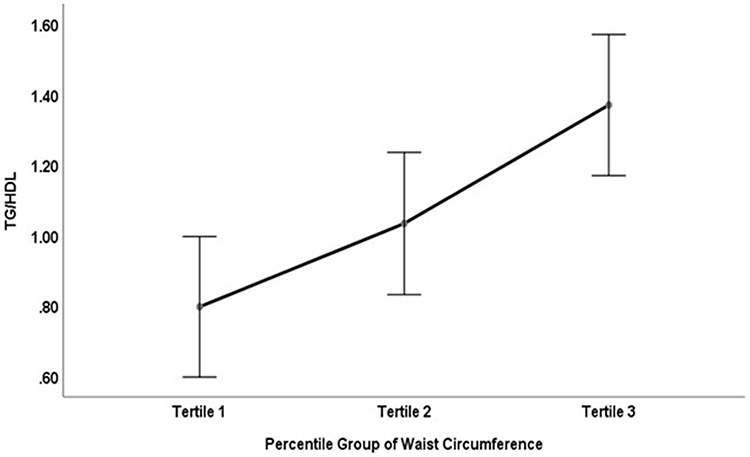 |
Figure 2 TG/HDL ratio across waist circumference tertiles. |
To assess the diagnostic accuracy of the TG/HDL ratio in identifying individuals with insulin resistance, we examined the thresholds of 2.0 and 2.5 for HOMA-IR levels, as depicted in Figure 3.19,20 These thresholds yielded AUC values of 0.693 and 0.746, respectively. Additionally, when using waist circumference thresholds above 90 and 80 cm for men and women, respectively, the threshold for the TG/HDL ratio was 1.2 for men (with a sensitivity of 56% and specificity of 90%) and 0.69 for women (with a sensitivity of 46% and specificity of 80%).
 |
Figure 3 Diagnostic Accuracy of TG/HDL in Relation to HOMA-IR Cut-offs of 2.0 (Top) and >2.5 (Bottom). |
In additional analysis, we conducted multivariate regression to examine the associations of TG/HDL ratio and waist circumference with HOMA-IR. The results indicated that both TG/HDL (1-SD increase: β [95% CI] = 0.261 [0.132–0.389]) and waist circumference (1-SD increase: β [95% CI] = 0.412 [0.276–0.549]) were significantly and independently associated with HOMA-IR. Furthermore, in univariate analysis, the association between TG/HDL (1-SD increase: β [95% CI] = 0.499 [0.375–0.623]) was stronger than that of waist circumference (1-SD increase: β [95% CI] = 0.397 [0.269–0.525]) with HOMA-IR.
Discussion
In this study, we investigated the potential utility of the TG/HDL ratio as an indicator of insulin resistance among Mongolian adults. The absence of established HOMA-IR cut-off values to define insulin resistance within the Mongolian population made any direct correlations between TG/HDL and insulin resistance challenging. Consequently, we sought to establish an association between TG/HDL and insulin resistance beyond any correlation with HOMA-IR by examining its relationship with other relevant indicator, such as waist circumference.
Our results demonstrate a significant association between the TG/HDL ratio and HOMA-IR. Furthermore, HOMA-IR levels exhibited a positive relationship with waist circumference, with the strength of the association between TG/HDL and HOMA-IR intensifying as waist circumference increased. These findings suggest that the TG/HDL ratio can indicate HOMA-IR, particularly among individuals with central obesity. However, it is essential to acknowledge that the TG/HDL ratio may not be employed as a standalone method to assess insulin resistance among Mongolian adults due to the absence of established cut-off values for HOMA-IR and waist circumference within this population. Therefore, while our study identifies the TG/HDL ratio as a promising tool, it also underscores the importance of a comprehensive assessment considering multiple factors, including waist circumference. This approach may contribute to a more thorough understanding of insulin resistance assessment among the Mongolian population and guide interventions.
Previous studies have extensively investigated the TG/HDL ratio as a valuable tool for assessing insulin resistance. For instance, a study involving 13,908 participants reported a correlation between the TG/HDL ratio and insulin resistance.21 Numerous population-based cohort studies have also supported the ratio’s predictive capacity for diabetes risk. For instance, Zheng et al identified the ratio as a predictor of diabetes risk in the Chinese elderly population,22 a conclusion independently reached by Cheng et al in a different cohort.23
Nevertheless, it’s essential to acknowledge the presence of heterogeneity in the relationship between the TG/HDL ratio and insulin resistance among different populations. In studies involving African descent19 and Southeast Asians20 populations, the TG/HDL ratio did not correlate with insulin resistance. These heterogeneous findings suggest that the effectiveness of the TG/HDL ratio as a marker for insulin resistance may be population-specific. In this study, we observed a significant association between the TG/HDL ratio and insulin resistance among Mongolian adults, suggesting the TG/HDL ratio may be a valuable indicator for evaluating insulin resistance, especially in individuals with existing insulin resistance or those susceptible to its development.
Previous research has reported a range of AUC values for the TG/HDL ratio concerning insulin resistance, from 0.69 to 0.77.20 Studies employing more sophisticated models, such as insulin-stimulated glucose disposal, demonstrated a robust correlation with the TG/HDL ratio. For instance, in Mohd Nor et al study among obese adolescents, a negative correlation between the TG/HDL ratio and insulin-stimulated glucose disposal (r = −0.416) was observed, alongside an AUC of 0.715,24 further reinforcing the potential of the TG/HDL ratio as a valuable marker for assessing insulin resistance.18,25,26 These data underscore the promise of the TG/HDL ratio as a valuable tool for evaluating insulin resistance. Moreover, our study indicated even higher diagnostic accuracy when analyzing the TG/HDL ratio with population-specific insulin resistance cut-offs derived from the widely used method, such as HOMA-IR.
Our study has shed light on the potential of enhancing insulin sensitivity by incorporating waist circumference measurements into insulin resistance assessment tools like HOMA-IR. Thus, we observed a significant association between the TG/HDL ratio and insulin resistance. Moreover, TG/HDL ratio and waist circumference were directly correlated, and these two parameters exhibited a robust association with HOMA-IR. Notably, previous studies have emphasized the importance of this relationship. For instance, Oliveira et al demonstrated that for every 1 cm increase in waist circumference, there was a corresponding 0.04 increase in the TG/HDL ratio.27 Furthermore, when the TG/HDL ratio exceeded 2.73, it was associated with a 10 cm increase in waist circumference, resulting in a substantial 4% increment in the TG/HDL ratio.28 While more research is warranted, these insights have the potential to inform the development of more comprehensive and precise insulin resistance assessment tools relevant to populations and settings, ultimately contributing to guide interventions and improve health outcomes.
This study presents several important limitations that must be recognized. Although the sample size is one such limitation, we conducted a robust post-hoc power analysis that confirmed the adequacy of our sample. The analysis revealed that our study possessed strong statistical power (over 80%) to detect significant differences in key variables, including HOMA-IR and the TG/HDL ratio adjusted for waist circumference, using G*Power. This reinforces the credibility of our findings despite concerns regarding sample size. Moreover, while the absence of nationally recognized reference measurements for HOMA-IR and waist circumference in the Mongolian population posed challenges, our results clearly demonstrate that the TG/HDL ratio serves as a significant indicator of insulin resistance. When adjusted for waist circumference, this metric provides valuable insights that can pave the way for future research in the Mongolian context. Our findings lay a critical groundwork for advancing the understanding of insulin resistance within this population.
Conclusion
The study suggests that the TG/HDL ratio, when paired with waist circumference measurements, may serve as a helpful marker for insulin resistance in Mongolian adults. It identified specific TG/HDL ratio thresholds that could aid in detecting at-risk individuals. However, more research is needed to confirm these results using nationwide HOMA-IR cut-offs.
Ethical Statements
- Approval of the research protocol: the protocol for this study has been approved by the Medical Research Ethical Committee at the Mongolian National University of Medical Sciences, on May 24, 2019 (approval No. 2019/D-06), and it conforms to the provisions of the Declaration of Helsinki (as revised in Fortaleza, Brazil, October 2013).
- Informed Consent: All informed consent was obtained from participants in Mongolian language.
- Approval date of Registry and the Registration No. of the study/trial: N/A
- Animal Studies: N/A
Acknowledgments
The authors would like to express their gratitude to Temuulen Tsedensodnom, Oyudari Sodnombileg, and Maral Boldbaatar for the assistance provided in data collection for the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Seed grant awards jointly funded this study for international activities from the Science and Technology Development Foundation of the Mongolian National University of Medical Sciences and the Global Affairs, University of California--Davis, Davis, USA. The funders had no role in study design, data collection and analysis, publication decisions, or manuscript preparation.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Suvd J, Gerel B, Otgooloi H, et al. Glucose intolerance and associated factors in Mongolia: results of a national survey. Diabet Med. 2002;19(6):502–508. doi:10.1046/j.1464-5491.2002.00737.x
2. Dayan A, Erkhembayar R, Luvsandavaajav O, Mukhtar Y, Enkhtuvshin B, Tumenbayar B. Prevalence of type 2 diabetes in Mongolia: results from population-based survey compared with 1999 study. Diabetes Metab Syndr Obes. 2023;16:1833–1846. doi:10.2147/DMSO.S413320
3. National Centre for Public Health (2020). Fourth national steps survey on the prevalence of non-communicable disease and injury risk factors-2019. Ulaanbaatar: National center for public health, Mongolia. Available from: https://extranet.who.int/ncdsmicrodata/index.php/catalog/836/related-materials.
4. Munkhtulga L, Nakayama K, Utsumi N, et al. Identification of a regulatory SNP in the retinol-binding protein 4 gene associated with type 2 diabetes in Mongolia. Hum Genet. 2007;120(6):879–888. doi:10.1007/s00439-006-0264-4
5. Shiwaku K, Nogi A, Kitajima K, et al. Prevalence of the metabolic syndrome using the modified ATP III definitions for workers in Japan, Korea, and Mongolia. J Occup Health. 2005;47(2):126–135. doi:10.1539/joh.47.126
6. DeFronzo RA, Tobin JD, Andres R. Glucose clamp technique: a method for quantifying insulin secretion and resistance. Am J Physiol. 1979;237(3):E214–E223. doi:10.1152/ajpendo.1979.237.3.E214
7. Tang Q, Li X, Song P, Xu L. Optimal cut-off values for the homeostasis model assessment of insulin resistance (HOMA-IR) and pre-diabetes screening: developments in research and prospects for the future. Drug Discov Ther. 2015;9(6):380–385. doi:10.5582/ddt.2015.01207
8. Tahapary DL, Pratisthita LB, Fitri NA, et al. Challenges in the diagnosis of insulin resistance: focusing on the role of HOMA-IR and Tryglyceride/glucose index. Diabetes Metab Syndr. 2022;16(8):102581. doi:10.1016/j.dsx.2022.102581
9. Zhang L, Chen S, Deng A, et al. Association between lipid ratios and insulin resistance in a Chinese population. PLoS One. 2015;10(1):e0116110. doi:10.1371/journal.pone.0116110
10. Song Q, Liu X, Wang A, et al. Associations between non-traditional lipid measures and risk for type 2 diabetes mellitus in a Chinese community population: a cross-sectional study. Lipids Health Dis. 2016;15(1):70. doi:10.1186/s12944-016-0239-y
11. Kim JS, Kang HT, Shim JY, Lee HR. The association between the triglyceride to high-density lipoprotein cholesterol ratio with insulin resistance (HOMA-IR) in the general Korean population: based on the national health and nutrition examination survey in 2007-2009. Diabet Res Clin Pract. 2012;97(1):132–138. doi:10.1016/j.diabres.2012.04.022
12. Zhou M, Zhu L, Cui X, et al. The triglyceride to high-density lipoprotein cholesterol (TG/HDL-C) ratio as a predictor of insulin resistance but not of β cell function in a Chinese population with different glucose tolerance status. Lipids Health Dis. 2016;15(1):104. doi:10.1186/s12944-016-0270-z
13. Gong R, Luo G, Wang M, Ma L, Sun S, Wei X. Associations between TG/HDL ratio and insulin resistance in the US population: a cross-sectional study. Endocr Connect. 2021;10(11):1502–1512. doi:10.1530/EC-21-0414
14. World Health Organization, 2011. Waist circumference and waist-Hip ratio: report of a WHO expert consultation, Geneva. 2008.
15. Ren X, Chen ZA, Zheng S, et al. Association between Triglyceride to HDL-C Ratio (TG/HDL-C) and insulin resistance in Chinese patients with newly diagnosed type 2 diabetes mellitus. PLoS One. 2016;11(4):e0154345. doi:10.1371/journal.pone.0154345
16. Singh Y, Garg MK, Tandon N, Marwaha RK. A study of insulin resistance by HOMA-IR and its cut-off value to identify metabolic syndrome in urban Indian adolescents. J Clin Res Pediatric Endocrinol. 2013;5:245–251.
17. Yun K-J, Han K, Kim MK, et al. Insulin resistance distribution and cut-off value in Koreans from the 2008-2010 Korean national health and nutrition examination survey. PLoS One. 2016;11(4):e0154593. doi:10.1371/journal.pone.0154593
18. Lee CH, Shih AZ, Woo YC, et al. Optimal cut-offs of homeostasis model assessment of insulin resistance (HOMA-IR) to identify dysglycemia and type 2 diabetes mellitus: a 15-year prospective study in Chinese. PLoS One. 2016;11(9):e0163424. doi:10.1371/journal.pone.0163424
19. Sumner AE, Harman JL, Buxbaum SG, et al. The triglyceride/high-density lipoprotein cholesterol ratio fails to predict insulin resistance in African-American women: an analysis of Jackson heart study. Metab Syndr Relat Disord. 2010;8(6):511–514. doi:10.1089/met.2010.0028
20. Mostafa SA, Davies MJ, Morris DH, et al. The association of the triglyceride-to-HDL cholesterol ratio with insulin resistance in White European and South Asian men and women. PLoS One. 2012;7(12):e50931. doi:10.1371/journal.pone.0050931
21. Azarpazhooh MR, Najafi F, Darbandi M, Kiarasi S, Oduyemi T, Spence JD. Triglyceride/high-density lipoprotein cholesterol ratio: a clue to metabolic syndrome, insulin resistance, and severe atherosclerosis. Lipids. 2021;56(4):405–412. doi:10.1002/lipd.12302
22. Zheng D, Li H, Ai F, et al. Association between the triglyceride to high-density lipoprotein cholesterol ratio and the risk of type 2 diabetes mellitus among Chinese elderly: the Beijing longitudinal study of aging. BMJ Open Diabetes Res Care. 2020;8(1):e000811. doi:10.1136/bmjdrc-2019-000811
23. Cheng C, Liu Y, Sun X, et al. Dose-response association between the triglycerides: high-density lipoprotein cholesterol ratio and type 2 diabetes mellitus risk: the rural Chinese cohort study and meta-analysis. J Diabetes. 2019;11(3):183–192. doi:10.1111/1753-0407.12836
24. Mohd Nor NS, Lee S, Bacha F, Tfayli H, Arslanian S. Triglyceride glucose index as a surrogate measure of insulin sensitivity in obese adolescents with normoglycemia, prediabetes, and type 2 diabetes mellitus: comparison with the hyperinsulinemic-euglycemic clamp. Pediatr Diabetes. 2016;17(6):458–465. doi:10.1111/pedi.12303
25. Gayoso-Diz P, Otero-González A, Rodriguez-Alvarez MX, et al. Insulin resistance (HOMA-IR) cut-off values and the metabolic syndrome in a general adult population: effect of gender and age: EPIRCE cross-sectional study. BMC Endocr Disord. 2013;13(1):47. doi:10.1186/1472-6823-13-47
26. Moon S, Park JH, Jang EJ, et al. The cut-off values of surrogate measures for insulin sensitivity in a healthy population in Korea according to the Korean national health and nutrition examination survey (KNHANES) 2007-2010. J Korean Med Sci. 2018;33(29):e197. doi:10.3346/jkms.2018.33.e197
27. Oliveira AM, Almeida M, Almeida M, et al. Is triglyceride to high-density lipoprotein cholesterol ratio a surrogate for insulin resistance in youth? Health. 2013;5(03):481–485. doi:10.4236/health.2013.53066
28. Nie G, Hou S, Zhang M, Peng W. High TG/HDL ratio suggests a higher risk of metabolic syndrome among an elderly Chinese population: a cross-sectional study. BMJ Open. 2021;11(3):e041519. doi:10.1136/bmjopen-2020-041519
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of HOMA-IR with Ovarian Sensitivity Index in Women Undergoing IVF/ICSI: A Retrospective Cohort Study
Li Y, Jiang Y, Zhang S, Liu H, Zhang C
Diabetes, Metabolic Syndrome and Obesity 2023, 16:309-320
Published Date: 2 February 2023